Susceptibility to Pain During Coronary Angioplasty: Usefulness of Pulpal … · 2017. 2. 2. ·...
7
JACC Vol. 28, No, 4 October 1996:903-9 903 Susceptibility to Pain During Coronary Angioplasty: Usefulness of Pulpal Test COLOMBA FALCONE, MD, CARLA AUGUADRO, MD, RENATO SCONOCCHIA, MD, ORONZO CATALANO, MD, MICHAEL OCHAN, MD, LUIGI ANGOLI, MD, CARLO MONTEMARTINI, MD Pavia, Italy Objectives.This study in patients with coronaryartery disease (CAD)sought to 1) determine the dental pain threshold and reaction to tooth pulp stimulation; 2) correlate the clinical, ergometricand angiographicfeaturesofpatientswithandwithout pain during percutaneous transluminal coronary angioplasty (PTCA)to pulpal test response; 3) verifywhether reactivityto dental pulp stimulation could help to identi~ patients particu- larly prone to perceivingangina duringmyocardialischemia. Background. Silentmyocardialischemiais frequentlyobserved in patients with CAD.Higher pain thresholds have been docu- mentedin asymptomaticsubjects,suggestinga generalizedhypo- sensitivityto pain. Methods.Eighty-sixconsecutivemale patients with reproduc- ibleexercise-inducedmyocardialischemiaand CADdocumented byangiographyunderwentPTCA.Apulpal test wasperformedin all patients by means of an electrical tooth pulp stimulator. Results. Seventy-onepatients (82.6%)with and 15 (17.4%) without angina during daily life were studied, Duringthe pulpal test, 57patients (66.2%)reporteddental pain,whereas29 (33,7%) wereasymptomatic,evenat maximalstimulationof 500MA.The study cohort was classified into two groups according to the presence (58 patients [group1]) or absence(28patients [group 2]) of angina during myocardial ischemia induced by PTCA. Silentmyocardialischemiaisfrequentlyobservedin patients withcoronaryarterydisease(CAD)bothduringdailylifeand duringstressortests(l-5). Someinvestigatorshavereported that the absenceof symptomsis frequentlyassociatedwith ischemiaofshorterdurationandsmallerextension;however, acuteischemiaduringmyocardialinfarctionandangioplasty- inducedcoronaryocclusionmayalsonot be associatedwith anginalpain(6–9).Variousmechanismshavebeenproposed to explainthe absenceof anginaduringmyocardial ischemia. Theendogenousopioidsystemseemsalsotoplayanimportant roleinpainmodulation(10–15).Ageneralizedhyposensitivity From the Department of Cardiology,UniversityHospital,IRCCS Pol. San Matteo, Pavia, Italy. ManuscriptreceivedOctober 23, 1995;revisedmanuscriptreceivedMay 2, 1996,acceptedMay 13, 1996. Address for correspondence:Dr. ColombaFalcone, Department of Cardi- ology,IRCCS Po]. San Matteo, PiazzaleGolgi 1, 27100Pavia,Italy. 01996 by the AmericanCollegeof Cardiology Publishedby ElsevierScienceInc. Ergometric variables, extent of CAD, presence of ST segment elevationduring PTCA,number of inflations,inflation time and maximalinflationpressureweresimilarin the twopatient groups. Dental pain was provokedby pulpal test in 81%of patients with and36%ofpatientswithoutsymptomsduringPTCA(p = 0.0004). The absenceof dental pain evenat maximaltooth pulp stimula- tion (500MA)wasobservedin 11(18.9%)patients in group1and 18 (64.2%)in group 2. Patients whowere asymptomaticduring PTCA had a higher mean dental pain threshold, lower mean threshold reaction and lowermean maximalreaction than those whoweresymptomaticduring both PTCAand the pulpal test. Conclusions, Acorrelationbetweenthe prevalenceofsymptoms during pulpal test, daily life, exercise-inducedmyocardialisch- emia and PTCAwas found.A higher dental pain threshold and lowerreactivitycharacterized those subjects who were prone to silent ischemiabothduringdailylifeand duringPTCA.Ergomet- ric variables, extent of CADand techniquesused during PTCA wereunrelatedto the tendencyto perceivepain duringmyocardial ischemia.Responseto the pulpal test and the presenceof symp- tomsduringdailylifewerehighlyrelated to the presenceofangina during PTCA. (JAm Coil Cardiol 1996;28:903-9) to differentpainfulstimulihasbeenreportedinasymptomatic patients,andahigherpainthresholdhasbeendemonstrated in suchsubjectsbymeansofvariousstimulating techniques. This result suggeststhat the lack of symptomsmay be partly explainedbyindividual differences in painthreshold(16-19). Dental pulp stimulationmay be used to test the pain thresholdin humans(19–24).Theelectricalpulpstimulation and consequentpain are very brief (a few seconds)and produceno tissuedamage.Becausethe test current can be increasedprogressively, thepulpaltestallowsquantificationof the pain thresholdand avoidsinterferencefrom superficial sensations thatcouldbetriggeredbyothermethods.Thisstudy in patientswith CAD soughtto 1) determinedental pain thresholdand reactionto toothpulpstimulation; 2) correlate the clinical,ergometricandangiographic featuresof patients withandwithoutsymptomsduringangioplastywiththepulpal test response;3) verify whether reactivityto dental pulp stimulationcouldhelptoidentifypatientsparticularlyproneto 0735-1097/96/$15.00 PH SO735-1097(96)OO252-5
Transcript of Susceptibility to Pain During Coronary Angioplasty: Usefulness of Pulpal … · 2017. 2. 2. ·...

JACC Vol. 28, No, 4October 1996:903-9
903
Susceptibility to Pain During Coronary Angioplasty: Usefulness ofPulpal Test
COLOMBA FALCONE, MD, CARLA AUGUADRO, MD, RENATO SCONOCCHIA, MD,
ORONZO CATALANO, MD, MICHAEL OCHAN, MD, LUIGI ANGOLI, MD,
CARLO MONTEMARTINI, MD
Pavia, Italy
Objectives.This studyin patients with coronaryartery disease(CAD)sought to 1) determine the dental pain threshold andreaction to tooth pulp stimulation; 2) correlate the clinical,ergometricand angiographicfeaturesofpatientswithandwithoutpain during percutaneous transluminal coronary angioplasty(PTCA)to pulpal test response;3) verifywhether reactivitytodental pulp stimulation could help to identi~ patients particu-larly prone to perceivingangina during myocardialischemia.
Background.Silentmyocardialischemiais frequentlyobservedin patients with CAD.Higher pain thresholds have been docu-mentedin asymptomaticsubjects,suggestinga generalizedhypo-sensitivityto pain.
Methods.Eighty-sixconsecutivemale patients with reproduc-ible exercise-inducedmyocardialischemiaand CADdocumentedbyangiographyunderwentPTCA.A pulpal test wasperformedinall patients by means of an electrical tooth pulp stimulator.
Results. Seventy-onepatients (82.6%)with and 15 (17.4%)withoutangina during daily lifewere studied,Duringthe pulpaltest, 57patients (66.2%)reporteddental pain,whereas29 (33,7%)wereasymptomatic,evenat maximalstimulationof 500MA.Thestudy cohort was classified into two groups according to thepresence (58 patients [group1]) or absence (28patients [group2]) of angina during myocardial ischemia induced by PTCA.
Silentmyocardialischemiais frequentlyobservedin patientswithcoronaryarterydisease(CAD)bothduringdailylifeandduringstressortests (l-5). Someinvestigatorshavereportedthat the absenceof symptomsis frequentlyassociatedwithischemiaof shorterdurationand smallerextension;however,acute ischemiaduringmyocardialinfarctionand angioplasty-inducedcoronaryocclusionmay also not be associatedwithanginalpain (6–9).Variousmechanismshavebeen proposedto explainthe absenceof anginaduringmyocardialischemia.Theendogenousopioidsystemseemsalsoto playanimportantroleinpainmodulation(10–15).A generalizedhyposensitivity
From the Department of Cardiology,UniversityHospital, IRCCS Pol. SanMatteo, Pavia,Italy.
ManuscriptreceivedOctober 23, 1995;revisedmanuscriptreceivedMay 2,1996,acceptedMay 13, 1996.
Address for correspondence:Dr. ColombaFalcone, Department of Cardi-ology,IRCCS Po]. San Matteo, PiazzaleGolgi 1, 27100Pavia,Italy.
01996 by the AmericanCollegeof CardiologyPublishedby ElsevierScienceInc.
Ergometric variables, extent of CAD,presence of ST segmentelevationduring PTCA,number of inflations,inflation time andmaximalinflationpressureweresimilarin the twopatient groups.Dental pain was provokedby pulpal test in 81%of patients withand 36%ofpatientswithoutsymptomsduringPTCA(p = 0.0004).The absenceof dental pain evenat maximaltooth pulp stimula-tion (500MA)wasobservedin 11(18.9%)patients in group1 and18 (64.2%)in group 2. Patients whowere asymptomaticduringPTCA had a higher mean dental pain threshold, lower meanthreshold reactionand lowermean maximalreaction than thosewhoweresymptomaticduring both PTCAand the pulpal test.
Conclusions,Acorrelationbetweenthe prevalenceofsymptomsduring pulpal test, daily life, exercise-inducedmyocardialisch-emia and PTCAwas found.A higher dental pain threshold andlowerreactivitycharacterizedthose subjectswhowere prone tosilent ischemiabothduringdailylifeand duringPTCA.Ergomet-ric variables, extent of CADand techniquesused during PTCAwereunrelatedto the tendencyto perceivepain duringmyocardialischemia.Responseto the pulpal test and the presenceof symp-tomsduringdailylifewerehighlyrelated to thepresenceofanginaduring PTCA.
(JAm Coil Cardiol 1996;28:903-9)
to differentpainfulstimulihasbeenreportedin asymptomaticpatients,anda higherpainthresholdhasbeendemonstratedinsuchsubjectsbymeansofvariousstimulatingtechniques.Thisresult suggeststhat the lack of symptomsmay be partlyexplainedbyindividualdifferencesin pain threshold(16-19).
Dental pulp stimulationmay be used to test the painthresholdin humans(19–24).The electricalpulp stimulationand consequentpain are very brief (a few seconds)andproduceno tissuedamage.Becausethe test current can beincreasedprogressively,thepulpaltestallowsquantificationofthe pain thresholdand avoidsinterferencefrom superficialsensationsthatcouldbe triggeredbyothermethods.Thisstudyin patientswith CAD sought to 1) determinedental painthresholdand reactionto toothpulpstimulation;2) correlatethe clinical,ergometricand angiographicfeaturesof patientswithandwithoutsymptomsduringangioplastywiththe pulpaltest response;3) verifywhether reactivityto dental pulpstimulationcouldhelpto identifypatientsparticularlyproneto
0735-1097/96/$15.00PH SO735-1097(96)OO252-5

904 FALCONEETAL. JACCVol.28,No.4PULPALTESTFORPAINDURINGPTCA October1996:903-9
AbbreviationsandAcronymsCAD = coronaryarterydiseaseECG = electrocardiogram,electrocardiographicEST = exercisestresstestPTCA= percutaneoustransluminalcoronary
angioplastyRPP = rate-pressureproduct
experienceanginalpain duringepisodesof myocardialisch-emia.
MethodsPatientselection.Eighty-sixconsecutivemalepatientswho
underwentpercutaneoustransluminalcoronaryangioplasty(PTCA)forclinicalindicationswereenrolledin thestudy.Theinclusioncriteriawerereproducibleexercise-inducedmyocar-dial ischemia;CADdocumentedby angiography;PTCAsuc-cessfullyperformedin at leastone vessel;presenceof trans-mural myocardial ischemia (electrocardiographic[ECG]changes)provokedbyPTCAin areasthatwerenot involvedinpreviousmyocardialinfarction;dentalformulasuitableforthepulpaltest, as indicatedby a previousdentalcheckup.
The studyincluded71patientswithand 15withouthistoryof angina.Thirty-sevenpatientshad a previousmyocardialinfarction>6 weeksbeforethe study(2 of 37 patientsweresymptomlessduringthe acuteevent).One-vesseldiseasewasdocumentedat angiographyin 62 patientsand multivesseldiseasein 24.Thedilatedvesselwasthe leftanteriordescend-ingcoronaryarte~ in50patientsandthe rightcoronaryarteryin36.Mean(tSD) ejectionfractioncalculatedbythestandardarea–lengthmethodwas61.7* 11.1%,meanleftventricularend-diastolicpressure 17.8 * 9.9 mm Hg, and mean end-diastolicvolume 127.6 t 50.7 ml. Patients with valvulardisease,bundlebranchblock,congestiveheartfailure,systemichypertension,diabetes,peripheralneuropathyor clinicalcon-ditionsthat didnot permittempora~withdrawalof antiangi-naltherapywereexcludedfromthestudy.Allpatientsenrolledunderwentthe followingtests: bicycleexercisestress test(EST),pulpaltest,coronaryangiographyandPTCA.Thetestswere performedat pharmacologicwashout;calciumchannelblockingagentsand nitrateswere suspended48 h beforethetests.No patientreceivedbeta-adrenergicblockingagentsordigitalis.Written informedconsentwas obtained from allpatientsfor each test. The studywas approvedby the ethicscommitteeof the hospital.
Exercisestresstest. A multistagebicycleergometricstresstest wasperformed1 to 7 daysbeforePTCA,in the supinepositionwith an initialwork load of 25 W and subsequentstepwiseincrementsof 25 W every 3 min at a pedalingfrequencyof 60 rpm.A 12-leadstandardECG wasrecordedbeforethe test,everyminuteduringexercise,at peakexerciseand everyminuteduringrecovery.LeadsD3,V5and Vcjwere
monitoredcontinuouslythroughoutthe test and displayedonan oscilloscope.Bloodpressurewasmeasuredby meansof astandardsphygmomanometerat baselineand at 3-reininter-vals duringexerciseand recovery.During the test, patientswere askedabout the presenceof chestpain or discomfort.Whenpresent,it wasquantifiedon a scalefrom 1 to 10andtimed in seconds.The test was stoppedwhen moderatetosevereangina,dyspnea,exhaustion,majorarrhythmiasor STsegmentdepression>3 mm occurred.A positiveECG re-sponsewasdefinedas the occurrenceof at least 1 mmflatordownslopingST segmentdepressionfor a durationof 0.08safter the J point.Ischemiathresholdwasdefinedas l-mmSTsegmentdepression.Rate-pressureproduct(RPP)(Heartrate[beats/rein]X systolicbloodpressure[mmHg])wascalculatedat baseline,at ischemiaand pain thresholdsand at peakexercise.
Pulpaltest. An electricaltoothpulpstimulator,commonlyused in dentistryfor diagnosisof pulp disease,was used todeterminedentalpainthreshold.Thetoothpulptesterutilizedforthisstudywasthesameasthatusedpreviously(19);it isanelectronicdevicethatdeliversa square-shapedcurrentimpulse(plateau70 ms) of increasingintensity.The stimulatorwasappliedto the tooththrougha metalcylinderandwasdesignedto delivera currentimpulseof increasingintensityfrom10to500mA.As the test currentincreased,a numberfromOto 9wasdisplayedon the instrument.All patientshad previouslyundergonea dentalcheckupto excludetooth fractures,abra-sions,caries,fillingsor markedperiodontaldisease.The testwasperformedon at leasttwohealthyupperincisorsand oneinferiorincisor.Theaverageofthemeasurementsforthe threeteethwasused.Patientswereinstructedto raisetheirhandsatthe occurrenceof pain or when they wanted the test to bestopped.Dental pain thresholdwas definedas the minimalcurrentintensitylevelthat elicitedanypulp sensation(10 to500mA; 1 to 9 on the tester).The highestintensitycurrent(500mA;9 on the tester)wasappliedin allpatients.Duringthe test, patientswere asked to grade the intensityof painexperienced(reaction)on a scale from 1 to 10; thresholdreaction(mean pain intensityat dentalpain threshold)andmaximalreaction(painintensityat maximalstimulation)weredeterminedin all patients.The lackof sensationat maximalstimulationwas definedas reactionO.Pulpal test was per-formedat rest andundercomfortableconditions1daybeforePTCAin the morningbetween9 and 11AM.The cardiologistwho performedPTCA (L.A. or C.M.) was blinded to theresponseto the pulpaltest.
Coronaryarteriography.Arteriographywasperformedus-ing the Sonestechnique,with multipleviewsof each vesselbeingfilmed1 to 15daysbeforecoronaryangioplasty.Signif-icantCADwasconsideredpresentwhen >50% lumendiam-eter stenosiswas found in a major coronaryvessel.Leftventriculographywas performedbefore coronaryarteriogra-phy in the 30°rightanteriorobliqueprojection.Ventricularvolumesandejectionfractionswerecalculatedbythe standardarea-lengthmethod.
—.

JACCVol.28,No.4October1996:903-9
FALCONE ET AL. 905PULPALTESTFORPAINDURING PTCA
Percutaneoustransluminalcoronary angioplasty.Coro-nary angioplastywas performedin all our patientsby thefemoralapproach,between9 and 11AM.Theprocedureis thesame as that describedin a previousstudy(25).Duringtheprocedure,the patientswere askedabout the occurrenceofsymptomsand, if present,theywerereportedon a graduatedlinearscale(1 to 10).Onsetof ST segmentdisplacementandany variationswere carefullyobservedand independentlyestimatedby two cardiologists(C.F., C.A.).Coronaryangio-plastywasperformedonlyin a singlevesselin each patient;successfulangioplastywasdefinedas a diametergainof 20%withoutcomplications.
Statisticalanalysis,Resultsare presentedas meanvalue*SD. Statisticalsignificancewastestedby meansof one-wayanalysisofvariance,the contrastmethodandlinearregressionanalysisusing the computerizedSPSS program (StatisticalPackagefor the SocialSciences).TheMann-Whitneytestwasused for two independentnonparametricsamples;p <0.05wasconsideredstatisticallysignificant.
ResultsClinicalfeatures. Of the 86 studypatients,71 (82.6%)
reportedanginaduringdailylife(7 on effort,4 at rest and 60mixed;meananginalpain intensity5.2 t 2.6),and 15(17.4%)had silentischemia(3 had a historyof syncope,3 had silentpostinfarctionmyocardialischemia,and 9 were referredbe-causeof silentmyocardialischemiadiscoveredduringa rou-tinecheckup).AllpatientshadmyocardialischemiaduringtheEST:32 patients(37.2%)referredfor angina(meananginalpain intensityat peak exercisewas 4.0 t 2.8),whereas54(62.8%)wereasymptomatic.TheRPPat baseline,at ischemiathresholdand at peak exercisewas 9,292f 2,199,19,601t5,623and 21,786t 5,685beats/reinX mm Hg, respectively.Fifty-sevenpatients(66.2%)reporteddentalpain duringthepulpal test (mean dental pain threshold5.7 f 2.0, meanthresholdreaction3.4 i 1.5,mean maximalreaction5.3 *2.7),whereas29(33.7%)wereasymptomatic(thresholdOandreactionOto pulpaltest) even at maximalstimulation(500mA).No significantvariationsin controlheart rate andbloodpressurewereobservedduringthe procedure.
Thestudycohortwasclassifiedintotwogroupsaccordingtothe occurrenceof anginaduringmyocardialischemiainducedbycoronaryangioplasty:Group1included58patients(67.4%,mean age53.8t 8.6years)withanginalsymptoms,Group2included28 patients (32.5%,mean age 59.2 * 7.0 years)withoutsymptomsduringcoronaryocclusion.The character-isticsof the groupsare summarizedin Table1.
Percutaneous transluminal corona~ angioplasty.Thenumber of inflations,inflationtime and maximalinflationpressurewere similar in Groups 1 and 2 (p = NS). Nostatisticaldifferencesin mean baselineheart rate and bloodpressurewere observed.Meanheart rate and bloodpressurevaluesduringPTCAwere alsosimilarbetweenpatientswithandwithoutsymptoms.OnsetofECGchangeswasobservedatsimilarinflationpressuresin both groups(3.9 f 1.0atm for
Table 1. Clinical Characteristics and Test Results in Symptomatic(Group 1) and AsymptomaticPatients (Group 2) DuringPercutaneous Transluminal CoronaryAngioplasty
Group1 Group2@= 58) (n= 28) pValue
ClinicalfeaturesAge(yr)HistoryofanginaAnginalpainintensityPreviousMI
CoronaryangiographyOne-vesseldiseaseMrdtivesseldiseaseEjectionfraction(%)LVEDV(ml)LVEDP(mmHg)
PTCABaselineHR(beats/rein)BaselineBP(mmHg)HRduringFTCA(beatshnirr)BPdoringPTCA(nunHg)No.ofirrtlationsInflationtime(s)Maxinflationpressure(atm)STsegmentelevation(mm)
ESTPtswithanginalpainArrgirralpainintensityPtswithoutangkdpainBaselineRPP(beatahnirr
XmmHg)IscherniathresholdRPP(beats/
rninXnunHg)PainthresholdRPP(beata/mirr
XnunHg)PeakexerciseRPP(Lreata/nrin
XnrrnHg)STsegmentdepression(mm)
PulpaltestPtssymptomaticduringpulpal
testPtsasymptomaticat 500MA
53.818.655(94.8%)5g ~ 24
25(43%)
43(74.1%)15(25.8%)
61.1* 12.2117L 1818.2* 10.5
68* 15~~ ~ 2Q80.1t 19
143.3* 16.52.4t 1.880~ 285.2t 2.02.7* 1.2
22/32(68.7%)22? 2.9
36/54(66.6%)9,182t 2,077
19,308t 5,927
59.2* 7.0 0.0116(57.1%)<0.05
37 ~ 2,3 0.00312(42.8%) NS
19(67.8%) NS9(32.1%) NS
61.8t 9.9 NS133? 81 NS15.9? 9.7 NS
73~ ‘2Q NS131? 19 NS847~ 178 NS
147.8t 10.6 NS3.3f 1.9 NSM ~ M NS50 ~ 29 NS2,9Y1,4 NS
10/32(31.2%)<0.051.5t 2.6 NS
18/54(33.3%)<0.059,619t 2,404 NS
20,000t5,836 NS
19,861.1k 6,527.218,562t 6,199.7 NS
20,92Q~ 5,457 22,325?6,285 NS
1.9t 1.4 2.1* 1.8 NS
47/58(81%) 10/28(35.7%)0.0W4
11(18.9%) 18(64.2%) 0.001
Datapresentedaremeanvalue~ SDornumber(%)ofpatients(Pts).BP=bloodpressure;EST= exercisestresstest; HR = heart rate; LVEDP= leftventricularend-diastolicpressure;LVEDV= left ventricularend-diastolicvolume;Max= maximal;MI = myocardialinfarction;PTCA= percutaneouscoronaryangioplasty;RPP= rate-pressureproduct.
Group 1 vs. 4.1 t 0.4 atm for Group 2). All patientshadtransmuralischemiaas an inclusioncriterion;the presenceofSTsegmentelevationwassimilarin the twogroups,andECGchangeslastedan averageof 29 t 12s in Group 1 and 23 *14 s in Group 2 (p = NS). Anginalpain duringPTCAwasprovokedin 57(80.2%)of71patientswithand 1(6.6%)of 15withoutsymptomsduringdailylife.PTCA-relatedanginalpainappeared in the symptomaticpatients at maximalballoondilation(meananginalpain intensity6 t 2.17).Anginalpainappeared37 f 35.7s fromthe start of inflation.Absenceofanginalpain duringPTCA-inducedmyocardialischemiawasobservedin 10(17.5’%)of57patientswithsymptomsat pulpal

906 FALCONE ET AL.PULPAL TEST FOR PAIN DURING PTCA
JACC Vol. 28, No. 4October 1996:903-9
10 p=o.ocwm
8 T
6
4
2
nI
p=o.mi
I I
p=o.0001
r-< T
.meandentalpalnthreshold meanthresholdreaction meanmaximalreaction
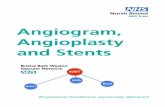
Figure1. Pulpaltestresponseinpatientswith(openbars)andwithout(solidbars)symptomsduringPTCA.Asymptomaticpatientshadasignificantlyhighermeandentalpainthreshold,lowermeanthresholdreactionandlowermeanmaximalreactionthansymptomaticpatients.
test. A positivecorrelationbetween anginalpain intensityduringdailylifeand PTCAwasalsofound(p = 0.005)(Table1).
Exercisestresstest. Of 32patientswhoweresymptomaticduringthe EST,22(68.7%)alsoreportedanginalpainduringPTCA,whereasthe remaining10(31.2%)wereasymptomaticduringPTCA.Of 54 patientswithoutsymptomsduringtheEST,18(33.3%)remainedasymptomatic,whereas36(66.6%)reportedpainduringPTCA.The intensityof anginalpainandST segmentdisplacementinducedby EST were similarinpatients in both groups.The RPP at baseline,at ischemiathresholdand at peakexercisealsodidnot differbetweenthetwogroups.In patientswithsymptomsduringbothPTCAandEST, the pain thresholdrate-pressureproductwassimilartothat in patientswithout symptomsduring PTCA but withsymptomsduringEST. Patientswith and withoutsymptomsduring EST did not differwith regard to the extent anddistributionof CAD(Table1).
Pulpaltest. Dentalpainwasprovokedbypulpaltest in 47(81%)of 58symptomaticand 10(35.7%)of 28asymptomaticpatientsduringPTCA(chi-square16.93,p = 0.0004).Absenceof pain duringpulpaltest, evenat maximaltoothpulpstimu-lation, was observed in 11 (18.9%) symptomaticand 18(64.2%) asyrnptomaticpatients during PTCA (Table 1).AsymptomaticpatientsduringPTCA who had pain duringdentalpulpstimulationhad a highermeandentalpainthresh-old, lowermean thresholdreactionand lowermeanmaximalreaction(7.3f 2, 1.9 t 0.9and 2.4 t 1.2,respectively)thanpatientssymptomaticbothduringPTCAandpulpaltest(5.3i1.9,p = 0.0006;3.7 * 1.4,p = 0.0001;6.1 * 2.6,p = 0.0000,respectively,allbythe Mann-Whitneytest)(Fig.1).Therewasalsoa correlationbetweenthe prevalenceofsymptomsduringdailylife, exercise-inducedmyocardialischemia,pulpal testandPTCA;14(93.3%)of 15patientswithoutsymptomsand56(78.8%)of71withsymptomsduringdailylifewereasymptom-atic and symptomaticduringpulpaltest, respectively.Signifi-
10
8
6
4
2
0-
p=O.0016
m
p=o.0001
p=o.Oooo
3meandentalpainthreshold meanthresholdreaction meanmaximalreaction
Fignre2.Pulpaltestresponseinpatientswith(openbars)andwithout(solidbars)symptomsduringdailylife.Asymptomaticpatientsshoweda significantlyhighermeandentalpainthreshold,lowermeanthresh-oldreactionandlowermeanmaximalreactionat pulpaltestthansymptomaticpatients.
cant differencesin mean dentalpain threshold(8.7 * 1.3vs.6.5 t 2.3,p = 0.0016,Mann-Whitneytest), mean thresholdreaction(0.3 f 0.8vs.2.6 * 1.9,p = 0.0000,Mann-Whitneytest)and meanmaximalreaction(0.5* 1.8vs.3.9~ 3.3,p =0.0001,Mann-Whitneytest)betweenasymptomaticandsymp-tomatic patients during daily life were observed(Fig. 2).Twenty-sixpatients(81.2%)whoreportedanginaduringESTalso had dental pain during tooth pulp stimulation;of 54asymptomaticpatients during EST, 23 (42.5%)were alsoasymptomaticduringpulpaltest. Of 58 symptomaticpatientsduringPTCA,22(37.9%)werealsosymptomaticduringESTandpulpaltest;of 28asymptomaticpatientsduringPTCA,12(42.8%)werealsoasymptomaticduringEST and pulpaltest.Of 31patientswithsilentischemiaduringESTand symptomsduringpulpaltest, 25 (80.6%)reported anginalpain duringPTCA.
A multipleregressionmodelwasconstructedto assesstherelativeimportanceof the variables(age,anginaduringdailylife and pulpal test responsiveness)that were significantlydifferentbetweenthe twogroupsofpatientsforpredictingtheoccurrenceof anginaduringPTCA-inducedtransmuralisch-emia.Thismodelshoweda strongerstatisticalpowerforpulpaltest stimulationresults.Dentalpainthreshold,thresholdreac-tion and,aboveall,maximalreactioncouldexplain-30!%to35%of the observedvariabilityin the presenceor absenceofanginaduringPTCA-inducedmyocardialischemia(adjustedcoefficientof determinationwas, respectively,0.29,0.33and0.36,p = 0.0000).Theinclusionin themodelofthepatientageincreasedthepredictivepowerto 38$Z0to 49Y0(adjustedR2=0.39,0.47and 0.48,respectively,p = 0.000,0.0004and 0.000,respectively).
Angiography.Extentof coronaryartery disease,ejectionfraction, left ventricular end-diastolicpressure and end-diastolicvolumewere similarin the two groupsof patients(Table1).
.————.—. ——.-——

JACC Vol. 28, No. 4October 1996:903-9
FALCONE ET AL. 907PULPAL TEST FOR PAIN DURING PTCA
DiscussionA highincidenceof anginalsymptomsbothin dailylifeand
during PTCA despite a low prevalenceof angina duringexercise-inducedmyocardialischemiawas observedin ourcohortwithCAD.Significantdifferencesin dentalpainthresh-old and reactionwere observedbetweenpatientswith andwithoutsymptomsduringdailylifeandPTCA.Theprevalenceof pain duringpulpaltest correlateswith the prevalenceofanginaboth duringdailylife and PTCA-inducedmyocardialischemia.
Silent ischemiaduring PTC4 ESTand daily life. Theprevalenceof silentmyocardialischemiavariesfrom 16%to47% during PTCA and from 32% to 70% during EST(5,24,26-34).In our cohort,63%of patientswereasymptom-aticduringEST,and only32.5Y0didnot reportanginaduringPTCA. The variablesof the inflationprocedurewere notcorrelatedwiththe tendencyto perceivepainduringmyocar-dialischemiainducedbycoronaryocclusion.Thus,durationorintensityof ischemiaand left ventriculardysfunctionare notabsolutefactors in determiningthe occurrenceof angina,althoughit hasbeenreported(6,8,9)that the absenceof painis frequentlyassociatedwith myocardialischemiaof shorterdurationand smallerextent.The higherprevalenceof silentischemiaduringexercisecouldprobablybe explainedby thegreater activationof the sympatheticsystem,resultingfromphysicalstress.Previousstudies(35,36)have demonstratedthat activationof the baroceptorreflexarchbypressoragentscaninducehyperalgesiain rats,and stimulationof the cardio-pulmonaryvagalafferentscouldberesponsiblefortheabsenceof pain in humansduringmyocardialischemia.Shepset al.(37)suggestedthat the stimulationofbaroceptorsmaymodifythe perceptionof anginalpain.In fact, theyfounda positivecorrelationbetween rest blood pressure and an index ofischemicpain perception (37). It has also been reported(38-40) that the pain thresholdin subjectswith essentialhypertensionwas higherthan in age-matchednormotensivepatients. In our cohort the blood pressurevaluesat peakexercisewere higher than during balloon occlusion.Thisfindingmightconfirmthe role of the baroceptorregulatorysystemin the greater prevalenceof silent ischemiaduringexercise.The strongerischemicstimulusduringballooncoro-naryocclusionmayhavebeenthe causeof our patientsbeingasymptomaticduringexercisebut otherwiseproneto perceivepain.Twenty-twoofthepatientswhoweresymptomaticduringPTCA reported pain duringEST, and 18 of those withoutsymptomsduringPTCAwere also asymptomaticon EST.Astrongcorrelationbetweentheprevalenceofsymptomsduringdailylifeandduringprovokedmyocardialischemiawasfound.In fact, the majorityof symptomaticpatientsduringdailylifealso had anginal symptomsduring PTCA. Moreover,theintensityofanginabothduringdailylifeandESTwashigherinsymptomaticthanasymptomaticpatientsduringPTCA.There-fore,individualdifferencesin sensitivityto painand,aboveall,an individualvariabilityin pain perceptionmightexplainin
part the presenceor absenceof anginaduring myocardialischemia.
Pulpal test responseand anginalpain perception.Symp-tomaticpatientsduringmyocardialischemiadifferfromthosewith silent ischemiain reactivityto pain. Various studies(17-19,41,42)havedemonstratedthat in patientswith silentmyocardialischemia,themeanpainthresholdandtoleranceinresponseto electricalskinstimulationand forearmischemiaare significantlyhigherthan in thosewith symptomaticisch-emia.Toothpulpstimulationhasalsobeenusedto determinepain thresholdin humans,and a fair reproducibilityof pulpaltest resultswasfoundin all studiesusingthe sametechnique(43-45).In a previousstudythatweperformedinpatientswithCAD (19), tooth pulp stimulationshowedsignificantdiffer-encesin dentalpain thresholdand reactionbetweenpatientswith and withoutanginaduringmyocardialischemia.Mostpatientswith silentischemiaduringEST did not have painduringpulpaltest,evenat the highestintensityof testcurrent.Likewise,80.4%of patientswho were symptomaticduringexercisealsoreportedpainduringdentalpulpstimulation(19).In the presentstudya correlationwasfoundbetweendentalpain threshold,reactionto pulpaltest and angina.A higherdentalpain thresholdand a lowermaximalreactionto pulpstimulationwere observedamongasymptomaticthan symp-tomaticpatientsduringdailylifeand PTCA.Dentalpainwasevokedbytoothpulpstimulationin 8170of symptomaticand36.8%of asymptomaticpatientsduringPTCA-inducedmyo-cardialischemia.Patientswith symptomsduringPTCA hadsignificantlya lowermeandentalpain thresholdand a highermeanthresholdreactionandmeanmaximalreactionat pulpaltest than did asymptomaticpatients during PTCA. Theseresultssuggestthat in patientsproneto pain,the pulpaltest isableto confirmthissusceptibility,whereasin thosewhoshowa variablereactivityto variouspainfulstimuli,the pulpaltesthas the same probabilityto evoke pain. Thus, individualdifferencesin painperceptionseemto be an importantfactorin determiningsusceptibilityto pain.
Previousstudieshavedemonstratedthat psychologicalfea-tures may modulatethe cardiovascularand neurohumoralresponsesto noxiousstimuliproducingdiscomfort.Personalitytraits, emotionalstate, environmentor psychologicalstress,social factors, degree of physicalconditioning,amount ofexerciseand timeof dayhaveall been proposedas havingarole in painperception(38).Differentmechanismshavebeensuggested(10,19,38,49)to explainthehyposensitivityto paininresponseto ditlerenttechniquesof painstimulation:inadequatestimulus,a defectin peripheralpain perception,a defectincentralpainsensationtransmission,a disturbanceincentraJpainmodulation,damageto the cardiacnociceptivepathwaybypre-viousinfarctionorneuropathyandtheinvolvementoftheendog-enousanalgesicsystem.Manycentraland peripheralmediatorshavebeen recognizedas importantfactorsin the modulationof pain, such as endorphins(higherbeta-endorphinplasmalevelsboth at baselineand during stress have been docu-mentedin asymptomaticpatients),metenkephalin,serotonin,

908 FALCONE ET AL.PULPAL TEST FOR PAIN DURING PTCA
catecholamines,gamma-aminobutyricacid and adenosine(14,15,25).
A generalizedaltered perceptionof noxiousstimuliinelderlypatientshasbeen reported;in factageseemsto be anindependentrisk factor for silentmyocardialischemia(46-48). Our asymptomaticpatientsundergoingPTCAwere onaverageolder than our symptomaticpatients;moreover,theinclusionof patient age in the multipleregressionmodelincreased the predictivityfor the presence or absenceofsymptomsfrom3070to 35’%oto 3870to 49Y0.
Variabilityin responseto painfulstimuli.An intragroupvariabilityin responseto variouspainfulstimuliwasobservedin our patients.A similaroverlapin pain thresholdbetweensymptomaticand asymptomaticpatientswithCADwasprevi-ously found (19,49);moreover,patients with documentedCADmayhavebothsymptomaticandasymptomaticischemicepisodes(4,6-8,17-19,49-51).Varyingconcentrationsofbeta-endorphinsin plasma,cerebrospinalfluid and intersynapticfluidmayunderliethevaryingindividualsensitivityto pain.Acircadianvariationin pain thresholdhas been also reported(12);inpatientswithvariabieresponsestopainfulstimuli,boththe circadianbeta-endorphinsecretionand the responsetovariousstressorsmayundergoperiodicvariations(52,53).Agreater instabilityin beta-endorphinplasma levels amongsymptomaticpatientshasbeenobserved(25).In fact,a signif-icantreductionin beta-endorphinplasmalevelsduringangio-plasty has been documentedin patients with symptoms,whereaspatientswith silent ischemiashowedmore stablevaluesduringthe procedure(25).A greateror lesservariationin beta-endorphinplasmalevelsmightexplainthe presenceorabsenceofanginaduringdifferentischemicepisodesoccurringin the same patient. In the present cohort,only 1590werealwaysasymptomatic(duringdailylife,EST,PTCAandpulpaltest), and this groupprobablyrepresentstrulyasymptomaticpatients. In contrast, 25.5% of our patients were alwayssymptomatic,andthustheycanbe consideredtrulysymptom-atic.In betweenthesetwogroupswasa continuousspectrumof patientswhowere sometimessymptomaticand sometimesasymptomatic.
Conclusions.Our resultsdemonstratethe presenceof anindividualprofilefor pain perception.A positivecorrelationbetweenthe responseto the pulpaltest and the presenceofanginaduringmyocardialischemiain patientsprone to painwasdocumented.In fact,a higherdentalpainthresholdandalowerdentalpainreactioncharacterizedthesubjectswhowereprone to silent ischemia.Therefore,pulpal stimulation—acommon,simple,briefandsafeprocedureusedin dentistrytodeterminetoothviability-mayfindusefulapplicationin car-diologybyidentifyinga subgroupofpatientsat relativelyhighrisk of symptomlessacute ischemicevents.Patientswith ahigher pain threshold and lower reactivityon pulpal testconstitutea subgroupthat shouldbe the focusof particularattentionduringfollow-up.These patientswith even severeCADmanifestminimalsymptoms,thuslackingthe usefulnessof anginaas a warning.In contrast,patientswitha lowdentalpain thresholdand highreactivityto dentalpulp stimulation
JACC Vol. 2S,No. 4October 1996:903–9
mayreceiveadequateattentionandworkupbythecardiologistbecausetheir diseaseis more associatedwith angina]pain,forcingthemto seekregularcare.
1
2,
3
4,
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
ReferencesCohn PF. Severeasymptomaticcoronaryartery disease:a diagnostic,prognosticandtherapeuticpuzzle.AmJ Med1977;62:565-8.ColeJP,EllestadMH.Significanceofchestpainduringtreadmillexercise:correlationwithcoronaryevents.AmJ Cardiol1978;41:227–32.SchangSJ Jr, PepineCJ.TransientasymptomaticSTsegmentdepressionduringdailyactivity.AmJ Cardiol1977;39:396-402.SelwynAP.TransientSTsegmentdepressionas a markerof myoeardialischemiaduringdaifylife.AmJ Cardiol1984;54:1195-200.FalconeC, De ServiS, PomaE, et al. Clinicalsignificanceof exercise-inducedsilentmyocardialischemiainpatientswithcoronaryarterydisease.J AmCoilCardiol1987;9,2:295-9.DeanfieldJE, MaseriA, SelwynA, et al. Myocardialischemiaduringdailylife in patientswithstableangina:its relationto symptomsandheart ratechanges.Lancet1983;2:753-8.MaseriA, ChierchiaS, DaviesG, GlazierJJ. Mechanismsof ischemiccardiacpain and silentmyocardialischemia.Am J Med 1985;79Suppl3A:7-11.CecchiA,DovelliniEV,MarchiF,PucciP,SantoroGM,FazziniPF.Silentmyoeardialiscfremiaduringambulatoryelectrocardiographicmonitoringinpatientswitheffortangina.J AmCoilCardiol1983;1:934-9.ChierchiaS,LazzariM,FreedmanSB,BmnelliC,MaseriA.Impairmentofmyoeardialperfusionand finrctionduringpainlessmyocardialischemia.J AmCoilCardiol1983;1:924-30.FieldsHL,BasbaumALEndogenouspaincontrolmechanisms.In:WallPD,MelzackZ, editors.Textbookof Pain.Edinburgh:ChurchillLivingstone,1984:143-52.FieldsHL. An endorphin-mediatedanalgesiasystem:experimentalandclinicalobservation.In: MartinJB,ReichlinS,BickKL,editors.Neurose-cretionandBrainPeptides:ImplicationsforBrainfunctionandNeurologicalDisease.NewYork:RavenPress,1981:199-203.BasbaumAI,FieldsHL.Endogenonspaincontrolmechanism:reviewandhypothesis.ArmNeurol1978;4:451-62.WatkinsLR,MayerD. Organizationof endogenousopiateandnonopiatepaincontrolsystem.Science1982;216:1185-92.FatconeC, SpecchiaG, RondanelliR, et al. Correlationbetweenbeta-endorphinplasmalevelsand anginalsymptomsin patientswithcoronaryarterydisease.J AmCoilCardiol1988;11:719–23.ShemDS.AdamsRF.HinderliterAL.et al.Endorohinsarerelatedtouainperceptionin coron~ arterydisease.’,%rrJ Cardi~l1987;59:523-7.‘
16.CohnPF. Sifentmyocardialischemiain patientswitha defectiveangirralwarningsystem.AmJ Cardiol1980;45:697-702.
17.DrosteC, RoskmanH. Experimentalpainmeasurementin patientswithasymptomaticmyocardialischemia.J AmCoilCardiol1983;1:940–5.
18.GlazierJJ, ChierchiaS, BrownMJ,MaseriA. Importanceof generalizeddefectiveperceptionof painfulstimulias a cause of silent myocardialischemiain chronicstableanginapectoris.AmJ Cardiol1986;58:667-72.
19.FalconeC,SconoccbiaR,GuastiL,CodegaS,MontemartiniC,SpeccbiaG.Dentalpainthresholdandanginapectorisin patientswithcoronaryarterydisease.J AmCoilCardiol1988;12:348-52.
20.AndersonSA,EricsonT, HolmgrenE, LinquistG. Electroacupuncture:effectonpainthresholdmeasuredwithelectricalstimulationoftooth.BrainRes1973;63:393-6.
21.ChapmanCR,WilsonME,GehrigJD.Comparativeeffectsofacupunctureandtranscutaneousstimulationontheperceptionofpainfuldentalstimuli.Pain1976;2:265-83.
22.AzeradJ, WodaA. Sensationevokedbybipolarintrapulparstimulationinman.Pain1977;4:145-52.
23.KemppainemP,Pertovaara& HuopaniemiT,et al.Modificationofdentalpainandcutaneousthermalsensitivitybyphysicalexerciseinman.BrainRes1985;360:33-40.
24.WohlgelemterD, JaffeCC,CabinHS,YeatmanLA, ClemanM. Silentmyocardialischcmiaduringcoronaryocclusionproducedbyballooninfla-tion:relationto regionalmyocardialdysfunction.J AmCoilCardiol1987;10:491-8.

JACC Vol. 28, No. 4October 1996:903-9
FALCONE ET AL. 909PULPAL TEST FOR PAIN DURING PTCA
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
FalconeC, GuastiL, OchanM, et al. Beta-endorphinsduringcoronaryangioplastyinpatientswithsilentorsymptomaticmyocardialischemia.JAmCoilCardiol1993;22:1614-20.MizutaniM,FreedmanSB,BarnsE, OgasawaraS,BaileyBP,BernsteinL.STmonitoringfor myocardialischemiaduringand after coronaryangio-plasty,AmJ Cardiol1990;66:389-93.SerruysPW,WijnsW,VanDeBrandM,et al.Leftventricularperformance,regionalbloodflow,wallmotion,andlactatemetabolismduringtransluminalangioplasty.Circulation1984;1:25-36.GriffinB,TimmisAD,CrickJCP,SowtonE. Theevolutionof myocardialischemiaduringpercutaneoustransluminalcoronaryangioplasty.EurHeartJ 1987;8:347-53.LabovitzAJ,LewenMK,KernM,VandormaelM,DeligonalU, KennedyHL.Evaluationof leftventricularsystolicanddiastolicdysfunctionduringtransientmyocardialischemiaproducedbyangioplasty.J AmCoilCardiol1987;10:4:748-55.SpecchiaG,FalconeC,TortoriciM,et al.SilentischerrriaduringPTCA:itsrelationshipwithexercise-inducedsilentischemiaandthe possibleroleforbeta-endorphins.In:KellerrnannJJ,BraunwaldE,editors.SilentMyocardialIschemia:A CriticalAppraisal.Karger:Basel,1990:165-75.WeinerD, RyanT, McCabeC, et al. Significanceof sifentmyocardialischemiaduringexercisetestingin patientswithcoronaryarterydisease.AmJ Cardiol1987;59:725-9.GasparettiCM, BurweOLR, Beller GA. Prevalenceof and variablesassociatedwithsilentischemiaonexercisethallium-201stresstesting.J AmCoilCardiol1990;16:115-23.OuyangP, ShapiroEP,ChandraNC,GottliebSH,ChewPH,GottliebSO.An angiographicand functionalcomparisonof patientswithsilent andsymptomatictreadmillischemiaearlyafter myocardialinfarction.AMJCardiol1987;59:730-4.HechtHS,ShawRE, BruceT, MylerRK.Silentischemia:evaluationbyexerciseandredistributiontomographicthallium-201myocardialimaging.JAmCOOCardiol1989;14:895-900.RandichA, MaixnerW. Interactionsbetweencardiovascularand painregulatorysystems.NeurosciBiobehavRev1984;8:343-67.RandichA, Maimer W. The role of sinoaorticand cardiopulmonarybaroreceptorreflexarcsin nociceptionand stress-inducedanalgesia.AnnNYAcadSci1986;467:385-401.ShepsDS,MaixnerW, HinderliterAL, et al. The relationshipbetweensystolicbloodpressure,ventricularvohrmeandischemicpainperceptioninpatientswithanginapectoris:a potentialroleforbaroceptors.IsrJ MedSci1989;25:482-7.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
ShepsDS,MaixnerW,HinderliterAL.Mechanismsin painperceptioninpatientswithsilentmyocardialischemia.AmHeartJ 1990;11:983-7.ZamirN,ShuberE.Alteredpainperceptioninhypertensivehumans.BrainRes1980;201:471-4.GhioneS, RosaC, MezzasalmaL, PanattoniE. Arterialhypertensionisassociatedwithhypalgesiain humans.Hypertension1989;12:491-7.LarrgerA, O’ConnorP. Centralmodulationofpainperceptionin patientswithsilentmyocardialischemia.AmJ Cardiol1994;74:182-4.Droste C, RoskammH. Pain measurementand pain modificationbynaloxonein patientswith asymptomaticmyocardialischemia.In: Rut-ishauserW, RoskammH, editors.SilentMyocardialIschemia.Berlin:Springer-Verlag,1984:14-23.GhioneS, Rosa C, PanattoniE, Nuti M, MezzasalmaL, GiulianoG.Comparisonof sensoryand pain thresholdin tooth pulpstimulationinnormotensiveman and essentialhypertension.J Hypertens1985;3Suppl3:s113-5.RosaC,VignocchiG,PanattoniE,RossiB,GhioneS.Relationshipbetweenincreasedbloodpressureand hypoalgesia:additionalevidencefor theexistenceof an abnormalityof painperceptionin arterialhypertensioninhumans.J HumHyperten1994;8:119-26.PapiF, GhioneS,RosaC,DelSeppiaC,LuschiP.Exposureto oscillatingmagneticfieldsinfluencessensitivityto electricalstimuli.ILExperimentsonhumans.Bioelectromagnetics1995;16:295-300.HarkinsSW,ChapmanCR.Detectionanddecisionfactorsin painpercep-tioninyoungandelderlymen.Pain1976;2:253-64.MillerPF, ShepsDS,BragdonEE, et al. Agingand pain perceptioninischemicheartdisease.AmHeartJ 1990;120:22-30.HarkinsSW,PriceDP, MartelliM. Effectsof age on pain perception:therrnonociception.J Gerontol1986;41:58-63.DrosteC, GreerdeeMW,RoskammH. A defectiveanginapectorispainwarningsystem:experimentalfindingsof ischemicandelectricalpaintest.Pain1986;26:199-209.LewisT, PickeringGW,RothschildP. Observationuponmuscularpaininintermittentclaudication.Heart1931;15:360-83.BuchsbaumMS,DavisGC,CoppolaR,NaberD.Opiatepharmacologyandindividualdifferences.II. Somatosensoryevokedpotential.Pain 1981;10:367-77.WatkinsLR,MayerD. Organizationof endogenousopiateandnonopiatepaincontrolsystem.Science1982;216:1185-92.YaksaTL.Spinalopiateanalgesia:characteristicsandprinciplesof action.Pain1981;11:293-346.







![ASD 903: Standards For Elevated Heliport · 2017-09-29 · ASD 903 (2006) (English): Standards For Elevated Heliport. ASD903 DRZ/SEPT2005 AIRPORT STANDARDS DIRECTIVE 903 [ASD 903]](https://static.fdocuments.in/doc/165x107/5f030d9c7e708231d4074d5d/asd-903-standards-for-elevated-heliport-2017-09-29-asd-903-2006-english.jpg)