Survival Pattern in Patients with Acute Organophosphate Poisoning Receiving Intensive Care
5
Journal of Toxicology CLINICAL TOXICOLOGY Vol. 42, No. 4, pp. 343–347, 2004 Survival Pattern in Patients with Acute Organophosphate Poisoning Receiving Intensive Care U. A. D. D. Munidasa, M.B.B.S., 1,2 I. B. Gawarammana, M.B.B.S., 1,3 S. A. M. Kularatne, M.D., M.R.C.P., 1,3 P. V. R. Kumarasiri, M.Sc., M.D., 1,4 and C. D. A. Goonasekera, M.D., M.R.C.P., Ph.D. 1,2, * 1 Intensive Care Unit, Teaching Hospital, Peradeniya, Sri Lanka 2 Department of Anesthesiology, 3 Department of Medicine, and 4 Department of Community Medicine, Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka ABSTRACT Background. Approximately 35% of patients acutely poisoned with organophosphates (OP) in developing countries like Sri Lanka require intensive care and mechanical ventilation. However, death rates remain high. Objective. To study the outcomes and predictors of mortality in patients with acute OP poisoning requiring intensive therapy at a regional center in Sri Lanka over a period of 40 months. Methods. Retrospective analysis of all intensive care records of patients with acute OP poisoning admitted to the Intensive Care Unit (ICU) between March 1998 and July 2001. Results. During the study period, 126 subjects were admitted to the ICU with acute OP poisoning. Records of 10 patients were lost and those of 37 were incomplete and hence were excluded. All the remaining 71 patients (59 male) had required endotracheal intubation and mechanical ventilation for a period of four (median) days (range 1 – 27) in addition to gastric lavage and standard therapy with atropine and oximes and adequate hydration. Of these 71 patients, 36 (28 male) had died. Life table analysis demonstrated a steep decline in the cumulative survival to 67% during the first three days. Systolic blood pressure of < 100 mmHg and FiO 2 of >40% to maintain a SpO 2 of > 92% within the first 24 h were recognized as poor prognostic indicators among mechanically ventilated patients. Conclusion. Mortality following OP poisoning remains high despite adequate respiratory support, intensive care, and specific therapy with * Correspondence: C. D. A. Goonasekera, Senior lecturer, M.D., M.R.C.P., Ph.D., Department of Anesthesiology, Faculty of Medicine, University of Peradeniya, Peradeniya, Sri Lanka; E-mail: [email protected]. 343 DOI: 10.1081/CLT-120039539 0731-3810 (Print); 1097-9875 (Online) Copyright D 2004 by Marcel Dekker, Inc. www.dekker.com Clinical Toxicology Downloaded from informahealthcare.com by University of Waterloo on 10/28/14 For personal use only.
Transcript of Survival Pattern in Patients with Acute Organophosphate Poisoning Receiving Intensive Care

Journal of Toxicology
CLINICAL TOXICOLOGY
Vol 42 No 4 pp 343ndash347 2004
Survival Pattern in Patients with Acute OrganophosphatePoisoning Receiving Intensive Care
U A D D Munidasa MBBS12 I B Gawarammana MBBS13
S A M Kularatne MD MRCP13
P V R Kumarasiri MSc MD14
and C D A Goonasekera MD MRCP PhD12
1Intensive Care Unit Teaching Hospital Peradeniya Sri Lanka2Department of Anesthesiology 3Department of Medicine and
4Department of Community Medicine Faculty of Medicine
University of Peradeniya Peradeniya Sri Lanka
ABSTRACT
Background Approximately 35 of patients acutely poisoned with organophosphates
(OP) in developing countries like Sri Lanka require intensive care and mechanical
ventilation However death rates remain high Objective To study the outcomes and
predictors of mortality in patients with acute OP poisoning requiring intensive therapy
at a regional center in Sri Lanka over a period of 40 months Methods Retrospective
analysis of all intensive care records of patients with acute OP poisoning admitted to
the Intensive Care Unit (ICU) between March 1998 and July 2001 Results During the
study period 126 subjects were admitted to the ICU with acute OP poisoning Records
of 10 patients were lost and those of 37 were incomplete and hence were excluded All
the remaining 71 patients (59 male) had required endotracheal intubation and
mechanical ventilation for a period of four (median) days (range 1ndash27) in addition to
gastric lavage and standard therapy with atropine and oximes and adequate hydration
Of these 71 patients 36 (28 male) had died Life table analysis demonstrated a steep
decline in the cumulative survival to 67 during the first three days Systolic blood
pressure of lt100 mmHg and FiO2 of gt40 to maintain a SpO2 of gt92 within the
first 24 h were recognized as poor prognostic indicators among mechanically
ventilated patients Conclusion Mortality following OP poisoning remains high
despite adequate respiratory support intensive care and specific therapy with
Correspondence C D A Goonasekera Senior lecturer MD MRCP PhD Department of Anesthesiology Faculty of
Medicine University of Peradeniya Peradeniya Sri Lanka E-mail cgoonasesltlk
343
DOI 101081CLT-120039539 0731-3810 (Print) 1097-9875 (Online)
Copyright D 2004 by Marcel Dekker Inc wwwdekkercom
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
atropine and oximes One-third of the subjects needing mechanical ventilation and
reaching intensive care units die within the first 72 h of poisoning Systolic blood
pressure of less than 100 mmHg and the necessity of a FiO2 gt40 to maintain
adequate oxygenation are predictors of poor outcome in patients mechanically
ventilated in the ICU
Key Words Organophosphate poisoning Mortality Cardiac effects Poor prognostic
indicators
INTRODUCTION
Organophosphates account for 50 of all cases
of acute poisonings and 80 of pesticide poisonings
admitted to hospitals in Sri Lanka (1ndash3) Approxi-
mately 35 of patients with acute OP poisoning re-
quire assisted ventilation (4) Therefore it can be
assumed that one-third of all OP poisoning cases
need intensive care for the purpose of assisted ven-
tilation Studies of mortality among ventilated
patients are scanty in the literature and it is es-
timated to be between 16 and 50 in South Africa
and Sri Lanka respectively (56) At present one-
tenth of admissions to the intensive care units (ICUs)
in Sri Lanka constitute subjects with acute OP poisoning
requiring active treatment particularly ventilator sup-
port (7)
OBJECTIVE
The study was intended to analyze the pattern of
survival and identify the risk factors that may predict
poor outcome in patients requiring ventilatory
support and intensive care following acute organo-
phosphate poisoning
SUBJECTS AND METHODS
This retrospective study included the compre-
hensive medical nursing and intensive care mon-
itoring records of all subjects admitted with acute
organophosphorous poisoning to the Intensive Care
Unit (ICU) of the Teaching Hospital Peradeniya
over a period of 40 months starting from
March 1998
The qualifying case records were identified from
the ICU admission register and traced from the
medical record archives of the hospital We collected
patient information regarding poisoning clinical
features the treatments given parameters monitored
and the outcomes using a data entry form developed
specifically for this study Establishment of the
diagnosis in all cases at inception was based on the
cholinergic clinical features OP smell in gastric
contents history and other circumstantial evidence
such as availability of a poison bottle or a label
found in the vicinity and brought to the hospital by
the relatives The data were analyzed using SPSS
100 statistical software and Epinfo 2001 A life table
was plotted The risk factors predicting mortality
were discerned using odds ratios
RESULTS
During the study period 126 subjects were
admitted to the ICU with acute OP poisoning All
had ingested the poison 112 (97) on suicidal intent
and 4 (3) accidentally Although a specific organo-
phosphorous agent has been identified on circumstantial
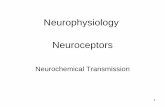
Figure 1 The survival function among patients needing
intensive care therapy and mechanical ventilation following
acute organophosphate poisoning
344 Munidasa et al
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
evidence in 29 (ie a bottle containing the poison was
found on site there were eyewitnesses etc) all cases
were diagnosed on clinical evidence (such as smell
clinical features such as pin point pupils sweating
respiratory difficulty with increased bronchial secre-
tions) as there was no ready analytical diagnostic test
available for use on their biological material All
patients were given atropine and pralidoxime based on
a standard protocol (8)
Records of 10 patients were lost and those of 37
were incomplete and hence were excluded All the
remaining 71 patients (59 male) had required endotra-
cheal intubation and mechanical ventilation for a
period of 4 (median) days (range 1ndash27) in addition
to gastric lavage standard therapy and adequate
hydration Of these 71 patients 36 (28 male) had
died A Kaplan Meier survival curve in this group
showed a cumulative survival of 067 at 3 days and
033 at 16 days from the hour of poisoning and no
mortality subsequently (Fig 1)
Of the 71 mechanically ventilated patients 64 had
recorded clinical information on all parameters that
were used in the analysis to gauge predictors of poor
outcome Twenty-one (33) of the 64 had on average
a systolic blood pressure of less than 100 mmHg despite
adequate hydration with saline and inotropes (Dobut-
amine and Dopamine doses exceeding 10 mgkgmin)
during the first 24 h and 18 of them died In contrast 32 of
the 35 survivors had on average a SBP of gt100 mmHg
during the first 24 h (Table 1)
Systolic blood pressure of less than 100 mmHg
during the first 24 h since admission to the ICU was a
significant predictor of poor outcome Odds ratio was
1745 (95 CI 43ndash7086)
The peripheral SpO2 of those who died and those
who survived were mean (SE) 940 (08) and mean
(SE) 957 (14) respectively and were not signifi-
cantly different However those who died needed a
significantly higher fraction of inspired oxygen (FiO2)
during the first 24 h of poisoning to maintain a
satisfactory peripheral SpO2 ie gt92 The patients
who needed a FiO2 higher than 40 had a higher
risk of death (Table 2) odds ratio was 90 (95 CI
184ndash4403)
DISCUSSION
The estimates of overall mortality following OP
ingestion ranges from 20 to 25 (239ndash11) These
reports consider the delay in discovery and transport
insufficient respiratory management aspiration pneu-
monia and sepsis as attributes to the cause of death in
the most cases
The mortality in mechanically ventilated patients
ranges from 13 to 50 (5612) The recognized
predictors of poor outcome include prolonged QT
interval on the ECG (13) APACHE II score of 26 or
more (14) low-frequency components of blood pres-
sure and heart rate signals on Spectral analysis (12) and
attempted suicide low PaO2 stupor and abnormal
chest X-ray on admission (5) The mortality rate
among the mechanically ventilated patients in our
study was 50 (35 of 71 died) and is similar to other
available data from Sri Lanka (6) In India 35 of the
patients with OP poisoning require assisted ventilation
(4) Assuming that all patients who reached a hospital
before death were intubated and mechanically venti-
lated we can extrapolate that the mortality rate on OP
poisoning with intensive care support facility would
range from 15ndash20 ie one in five patients will die
despite the availability of intensive care in the
developing countries All the patients in our study
had adequate peripheral oxygen saturation maintained
and hence none of the deaths were a direct conse-
quence of intermediate syndrome [ie the respiratory
muscle weakness observed within 6 to 10 days of OP
poisoning (8)] as they were in an ICU and were
mechanically ventilated The survival graph indicates
that by the end of the third day only 67 survived
Death was common in the subjects with hypotension
during the first 24 h and subjects who needed high-
inspired oxygen concentrations to maintain satisfactory
peripheral oxygen saturation
The current study recognizes that measured
systolic blood pressure less than 100 mmHg and the
need for FiO2gt40 to maintain adequate peripheral
Table 1 Average systolic blood pressure of ventilated
patients during the first 24 h
Number of
deaths
Number of
survivors
SBPlt100 mmHg 18 3
SBPgt100 mmHg 11 32
Table 2 The FiO2 of mechanically ventilated patients
Number of deaths Number of survivors
FiO2 gt40 27 21
FiO2 lt40 2 14
Survival Pattern in Patients with Acute OP Poisoning 345
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
oxygen saturation within the first 24 h since poisoning
are predictors of poor outcome in patients mechanically
ventilated in the ICU Although the odds ratios reach a
statistically significant level the wider confidence
internal particularly seen with low blood pressure as
a risk factor suggests that other factors may also be
contributing significantly to mortality For instance the
type of compound ingested the dose retained duration
since poisoning before being brought to intensive care
duration of hypoxia before therapy and the proportion
of poison removed by gastric lavage are other
immeasurable factors that may be making a contribu-
tion in this context The overall mortality is still high
despite institution of prompt ventilatory support in
addition to gastric lavage at inception and standard
therapy with atropine and pralidoxime Higher mortal-
ity rates in ventilated patients warrant research into
other factors which may influence the final outcome
Our observation of low systolic blood pressure and
requirement of FiO2gt40 suggests global impairment
of myocardial function despite adequate hydration
which can lead to reduction of pulmonary and systemic
circulation The most likely reason for myocardial
depression is the direct effect of OP with structural
damage Povoa et al reported focal myocardial
necrosis in a patient who died following ingestion of
OP who also had prolonged QTc (15) However
parasympathetic overactivity hypoxia acidosis and
electrolyte derangement may also depress the myocar-
dium in patients with OP poisoning Chuang et al in
their series of 223 patients reported that 435 had
prolonged QTc interval on the electrocardiography
(ECG) at presentation and these patients had a
significantly higher mortality and a higher rate of
respiratory failure (13) compared with the patients who
did not display QTc prolongation
CONCLUSION
Deaths due to OP poisoning remain high during
the first 72 h despite optimal respiratory care with
mechanical ventilation and oxygen supplementation
A low systolic blood pressure and a requirement of
FiO2gt40 within the first 24 h of OP poisoning are
predictors of mortality Therefore patients with systolic
blood pressure lt100 mmHg and those who need
FiO2gt40 to maintain their SpO2 above 92 should
be considered as at high risk of death and hence treated
in an intensive care environment Cardiovascular
effects of OP seem to be the major contributor for
mortality when temporary respiratory failure of OP
poisoning is controlled by mechanical ventilation
ACKNOWLEDGMENTS
The authors appreciate the help and support
provided by all medical staff and nursing staff of
Peradeniya Teaching Hospital in the clinical manage-
ment of these patients
REFERENCES
1 Goonasekera CDA Wimalaratne H Karalliedde
LD Changing profile of poisoning in a District
Hospital in Sri Lanka Sri Lanka J Med 1999835ndash38
2 Karalliedde L Senanayake N Pattern of acute
poisoning in a medical unit in central Sri Lanka
Forensic Sci Int 1988 36101ndash1043 Jeyaratnam J de Alwis Seneviratne RS
Copplestone JF Survey of pesticide poisoning
in Sri Lanka Bull WHO 1982 60615ndash6194 Goel A Joseph S Dutta TK Organophosphate
poisoning predicting the need for ventilatory
support J Assoc Phys Ind 1998 46786ndash7905 Bardin PG van Eeden SF Joubert JR Intensive
care management of acute organophosphate poi-
soning a 7-year experience in the western Cape S
Afr Med J 1987 72593ndash5976 Rajapakse VP Wijesekera S Outcome of mechan-
ical ventilation in Sri Lanka Ann R Coll Surg Engl
1989 71344ndash3467 Vasanthathilaka VWJK Goonasekera CDA An
audit of admissions to an intensive care unit in a
regional centre in Sri Lanka Ceylon Med J 199742145ndash148
8 Karalliedde L Senanayake N Organophosphorus
insecticide poisoning Br J Anaesth 1989 63736ndash750
9 Wyckoff DW Davies JE Barquet A Davis JH
Diagnostic and therapeutic problems of parathion
poisonings Ann Intern Med 1968 68875ndash88210 Yamashita M Tanaka J Ando Y Human mortality
in organophosphate poisonings Vet Hum Toxicol
1997 3984ndash8511 Abdollahi M Jalali N Sabzevari O Hoseini R
Ghanea T A retrospective study of poisoning in
Tehran J Toxicol Clin Toxicol 1997 35387ndash39312 Yen DH Yien HW Wang LM Lee CH Chan SH
Spectral analysis of systemic arterial pressure and
346 Munidasa et al
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
heart rate signals of patients with acute respiratory
failure induced by severe organophosphate poi-
soning Crit Care Med 2000 282805ndash281113 Chuang FR Jang SW Lin JL Chern MS Chen JB
Hsu KT QTc prolongation indicates a poor
prognosis in patients with organophophate poison-
ing Am J Emerg Med 1996 14451ndash453
14 Lee P Tai DY Clinical features of patients with
acute organophosphate poisoning requiring inten-
sive care Intensive Care Med 2001 27694ndash69915 Povoa R Cardoso SH Luna Filho B Ferreira
Filho C Ferreira M Ferreira C Organophosphate
poisoning and myocardial necrosis Arq Bras
Cardiol 1997 68377ndash380
Submitted October 28 2003Accepted January 29 2004
Survival Pattern in Patients with Acute OP Poisoning 347
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y

atropine and oximes One-third of the subjects needing mechanical ventilation and
reaching intensive care units die within the first 72 h of poisoning Systolic blood
pressure of less than 100 mmHg and the necessity of a FiO2 gt40 to maintain
adequate oxygenation are predictors of poor outcome in patients mechanically
ventilated in the ICU
Key Words Organophosphate poisoning Mortality Cardiac effects Poor prognostic
indicators
INTRODUCTION
Organophosphates account for 50 of all cases
of acute poisonings and 80 of pesticide poisonings
admitted to hospitals in Sri Lanka (1ndash3) Approxi-
mately 35 of patients with acute OP poisoning re-
quire assisted ventilation (4) Therefore it can be
assumed that one-third of all OP poisoning cases
need intensive care for the purpose of assisted ven-
tilation Studies of mortality among ventilated
patients are scanty in the literature and it is es-
timated to be between 16 and 50 in South Africa
and Sri Lanka respectively (56) At present one-
tenth of admissions to the intensive care units (ICUs)
in Sri Lanka constitute subjects with acute OP poisoning
requiring active treatment particularly ventilator sup-
port (7)
OBJECTIVE
The study was intended to analyze the pattern of
survival and identify the risk factors that may predict
poor outcome in patients requiring ventilatory
support and intensive care following acute organo-
phosphate poisoning
SUBJECTS AND METHODS
This retrospective study included the compre-
hensive medical nursing and intensive care mon-
itoring records of all subjects admitted with acute
organophosphorous poisoning to the Intensive Care
Unit (ICU) of the Teaching Hospital Peradeniya
over a period of 40 months starting from
March 1998
The qualifying case records were identified from
the ICU admission register and traced from the
medical record archives of the hospital We collected
patient information regarding poisoning clinical
features the treatments given parameters monitored
and the outcomes using a data entry form developed
specifically for this study Establishment of the
diagnosis in all cases at inception was based on the
cholinergic clinical features OP smell in gastric
contents history and other circumstantial evidence
such as availability of a poison bottle or a label
found in the vicinity and brought to the hospital by
the relatives The data were analyzed using SPSS
100 statistical software and Epinfo 2001 A life table
was plotted The risk factors predicting mortality
were discerned using odds ratios
RESULTS
During the study period 126 subjects were
admitted to the ICU with acute OP poisoning All
had ingested the poison 112 (97) on suicidal intent
and 4 (3) accidentally Although a specific organo-
phosphorous agent has been identified on circumstantial
Figure 1 The survival function among patients needing
intensive care therapy and mechanical ventilation following
acute organophosphate poisoning
344 Munidasa et al
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
evidence in 29 (ie a bottle containing the poison was
found on site there were eyewitnesses etc) all cases
were diagnosed on clinical evidence (such as smell
clinical features such as pin point pupils sweating
respiratory difficulty with increased bronchial secre-
tions) as there was no ready analytical diagnostic test
available for use on their biological material All
patients were given atropine and pralidoxime based on
a standard protocol (8)
Records of 10 patients were lost and those of 37
were incomplete and hence were excluded All the
remaining 71 patients (59 male) had required endotra-
cheal intubation and mechanical ventilation for a
period of 4 (median) days (range 1ndash27) in addition
to gastric lavage standard therapy and adequate
hydration Of these 71 patients 36 (28 male) had
died A Kaplan Meier survival curve in this group
showed a cumulative survival of 067 at 3 days and
033 at 16 days from the hour of poisoning and no
mortality subsequently (Fig 1)
Of the 71 mechanically ventilated patients 64 had
recorded clinical information on all parameters that
were used in the analysis to gauge predictors of poor
outcome Twenty-one (33) of the 64 had on average
a systolic blood pressure of less than 100 mmHg despite
adequate hydration with saline and inotropes (Dobut-
amine and Dopamine doses exceeding 10 mgkgmin)
during the first 24 h and 18 of them died In contrast 32 of
the 35 survivors had on average a SBP of gt100 mmHg
during the first 24 h (Table 1)
Systolic blood pressure of less than 100 mmHg
during the first 24 h since admission to the ICU was a
significant predictor of poor outcome Odds ratio was
1745 (95 CI 43ndash7086)
The peripheral SpO2 of those who died and those
who survived were mean (SE) 940 (08) and mean
(SE) 957 (14) respectively and were not signifi-
cantly different However those who died needed a
significantly higher fraction of inspired oxygen (FiO2)
during the first 24 h of poisoning to maintain a
satisfactory peripheral SpO2 ie gt92 The patients
who needed a FiO2 higher than 40 had a higher
risk of death (Table 2) odds ratio was 90 (95 CI
184ndash4403)
DISCUSSION
The estimates of overall mortality following OP
ingestion ranges from 20 to 25 (239ndash11) These
reports consider the delay in discovery and transport
insufficient respiratory management aspiration pneu-
monia and sepsis as attributes to the cause of death in
the most cases
The mortality in mechanically ventilated patients
ranges from 13 to 50 (5612) The recognized
predictors of poor outcome include prolonged QT
interval on the ECG (13) APACHE II score of 26 or
more (14) low-frequency components of blood pres-
sure and heart rate signals on Spectral analysis (12) and
attempted suicide low PaO2 stupor and abnormal
chest X-ray on admission (5) The mortality rate
among the mechanically ventilated patients in our
study was 50 (35 of 71 died) and is similar to other
available data from Sri Lanka (6) In India 35 of the
patients with OP poisoning require assisted ventilation
(4) Assuming that all patients who reached a hospital
before death were intubated and mechanically venti-
lated we can extrapolate that the mortality rate on OP
poisoning with intensive care support facility would
range from 15ndash20 ie one in five patients will die
despite the availability of intensive care in the
developing countries All the patients in our study
had adequate peripheral oxygen saturation maintained
and hence none of the deaths were a direct conse-
quence of intermediate syndrome [ie the respiratory
muscle weakness observed within 6 to 10 days of OP
poisoning (8)] as they were in an ICU and were
mechanically ventilated The survival graph indicates
that by the end of the third day only 67 survived
Death was common in the subjects with hypotension
during the first 24 h and subjects who needed high-
inspired oxygen concentrations to maintain satisfactory
peripheral oxygen saturation
The current study recognizes that measured
systolic blood pressure less than 100 mmHg and the
need for FiO2gt40 to maintain adequate peripheral
Table 1 Average systolic blood pressure of ventilated
patients during the first 24 h
Number of
deaths
Number of
survivors
SBPlt100 mmHg 18 3
SBPgt100 mmHg 11 32
Table 2 The FiO2 of mechanically ventilated patients
Number of deaths Number of survivors
FiO2 gt40 27 21
FiO2 lt40 2 14
Survival Pattern in Patients with Acute OP Poisoning 345
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
oxygen saturation within the first 24 h since poisoning
are predictors of poor outcome in patients mechanically
ventilated in the ICU Although the odds ratios reach a
statistically significant level the wider confidence
internal particularly seen with low blood pressure as
a risk factor suggests that other factors may also be
contributing significantly to mortality For instance the
type of compound ingested the dose retained duration
since poisoning before being brought to intensive care
duration of hypoxia before therapy and the proportion
of poison removed by gastric lavage are other
immeasurable factors that may be making a contribu-
tion in this context The overall mortality is still high
despite institution of prompt ventilatory support in
addition to gastric lavage at inception and standard
therapy with atropine and pralidoxime Higher mortal-
ity rates in ventilated patients warrant research into
other factors which may influence the final outcome
Our observation of low systolic blood pressure and
requirement of FiO2gt40 suggests global impairment
of myocardial function despite adequate hydration
which can lead to reduction of pulmonary and systemic
circulation The most likely reason for myocardial
depression is the direct effect of OP with structural
damage Povoa et al reported focal myocardial
necrosis in a patient who died following ingestion of
OP who also had prolonged QTc (15) However
parasympathetic overactivity hypoxia acidosis and
electrolyte derangement may also depress the myocar-
dium in patients with OP poisoning Chuang et al in
their series of 223 patients reported that 435 had
prolonged QTc interval on the electrocardiography
(ECG) at presentation and these patients had a
significantly higher mortality and a higher rate of
respiratory failure (13) compared with the patients who
did not display QTc prolongation
CONCLUSION
Deaths due to OP poisoning remain high during
the first 72 h despite optimal respiratory care with
mechanical ventilation and oxygen supplementation
A low systolic blood pressure and a requirement of
FiO2gt40 within the first 24 h of OP poisoning are
predictors of mortality Therefore patients with systolic
blood pressure lt100 mmHg and those who need
FiO2gt40 to maintain their SpO2 above 92 should
be considered as at high risk of death and hence treated
in an intensive care environment Cardiovascular
effects of OP seem to be the major contributor for
mortality when temporary respiratory failure of OP
poisoning is controlled by mechanical ventilation
ACKNOWLEDGMENTS
The authors appreciate the help and support
provided by all medical staff and nursing staff of
Peradeniya Teaching Hospital in the clinical manage-
ment of these patients
REFERENCES
1 Goonasekera CDA Wimalaratne H Karalliedde
LD Changing profile of poisoning in a District
Hospital in Sri Lanka Sri Lanka J Med 1999835ndash38
2 Karalliedde L Senanayake N Pattern of acute
poisoning in a medical unit in central Sri Lanka
Forensic Sci Int 1988 36101ndash1043 Jeyaratnam J de Alwis Seneviratne RS
Copplestone JF Survey of pesticide poisoning
in Sri Lanka Bull WHO 1982 60615ndash6194 Goel A Joseph S Dutta TK Organophosphate
poisoning predicting the need for ventilatory
support J Assoc Phys Ind 1998 46786ndash7905 Bardin PG van Eeden SF Joubert JR Intensive
care management of acute organophosphate poi-
soning a 7-year experience in the western Cape S
Afr Med J 1987 72593ndash5976 Rajapakse VP Wijesekera S Outcome of mechan-
ical ventilation in Sri Lanka Ann R Coll Surg Engl
1989 71344ndash3467 Vasanthathilaka VWJK Goonasekera CDA An
audit of admissions to an intensive care unit in a
regional centre in Sri Lanka Ceylon Med J 199742145ndash148
8 Karalliedde L Senanayake N Organophosphorus
insecticide poisoning Br J Anaesth 1989 63736ndash750
9 Wyckoff DW Davies JE Barquet A Davis JH
Diagnostic and therapeutic problems of parathion
poisonings Ann Intern Med 1968 68875ndash88210 Yamashita M Tanaka J Ando Y Human mortality
in organophosphate poisonings Vet Hum Toxicol
1997 3984ndash8511 Abdollahi M Jalali N Sabzevari O Hoseini R
Ghanea T A retrospective study of poisoning in
Tehran J Toxicol Clin Toxicol 1997 35387ndash39312 Yen DH Yien HW Wang LM Lee CH Chan SH
Spectral analysis of systemic arterial pressure and
346 Munidasa et al
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
heart rate signals of patients with acute respiratory
failure induced by severe organophosphate poi-
soning Crit Care Med 2000 282805ndash281113 Chuang FR Jang SW Lin JL Chern MS Chen JB
Hsu KT QTc prolongation indicates a poor
prognosis in patients with organophophate poison-
ing Am J Emerg Med 1996 14451ndash453
14 Lee P Tai DY Clinical features of patients with
acute organophosphate poisoning requiring inten-
sive care Intensive Care Med 2001 27694ndash69915 Povoa R Cardoso SH Luna Filho B Ferreira
Filho C Ferreira M Ferreira C Organophosphate
poisoning and myocardial necrosis Arq Bras
Cardiol 1997 68377ndash380
Submitted October 28 2003Accepted January 29 2004
Survival Pattern in Patients with Acute OP Poisoning 347
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y

evidence in 29 (ie a bottle containing the poison was
found on site there were eyewitnesses etc) all cases
were diagnosed on clinical evidence (such as smell
clinical features such as pin point pupils sweating
respiratory difficulty with increased bronchial secre-
tions) as there was no ready analytical diagnostic test
available for use on their biological material All
patients were given atropine and pralidoxime based on
a standard protocol (8)
Records of 10 patients were lost and those of 37
were incomplete and hence were excluded All the
remaining 71 patients (59 male) had required endotra-
cheal intubation and mechanical ventilation for a
period of 4 (median) days (range 1ndash27) in addition
to gastric lavage standard therapy and adequate
hydration Of these 71 patients 36 (28 male) had
died A Kaplan Meier survival curve in this group
showed a cumulative survival of 067 at 3 days and
033 at 16 days from the hour of poisoning and no
mortality subsequently (Fig 1)
Of the 71 mechanically ventilated patients 64 had
recorded clinical information on all parameters that
were used in the analysis to gauge predictors of poor
outcome Twenty-one (33) of the 64 had on average
a systolic blood pressure of less than 100 mmHg despite
adequate hydration with saline and inotropes (Dobut-
amine and Dopamine doses exceeding 10 mgkgmin)
during the first 24 h and 18 of them died In contrast 32 of
the 35 survivors had on average a SBP of gt100 mmHg
during the first 24 h (Table 1)
Systolic blood pressure of less than 100 mmHg
during the first 24 h since admission to the ICU was a
significant predictor of poor outcome Odds ratio was
1745 (95 CI 43ndash7086)
The peripheral SpO2 of those who died and those
who survived were mean (SE) 940 (08) and mean
(SE) 957 (14) respectively and were not signifi-
cantly different However those who died needed a
significantly higher fraction of inspired oxygen (FiO2)
during the first 24 h of poisoning to maintain a
satisfactory peripheral SpO2 ie gt92 The patients
who needed a FiO2 higher than 40 had a higher
risk of death (Table 2) odds ratio was 90 (95 CI
184ndash4403)
DISCUSSION
The estimates of overall mortality following OP
ingestion ranges from 20 to 25 (239ndash11) These
reports consider the delay in discovery and transport
insufficient respiratory management aspiration pneu-
monia and sepsis as attributes to the cause of death in
the most cases
The mortality in mechanically ventilated patients
ranges from 13 to 50 (5612) The recognized
predictors of poor outcome include prolonged QT
interval on the ECG (13) APACHE II score of 26 or
more (14) low-frequency components of blood pres-
sure and heart rate signals on Spectral analysis (12) and
attempted suicide low PaO2 stupor and abnormal
chest X-ray on admission (5) The mortality rate
among the mechanically ventilated patients in our
study was 50 (35 of 71 died) and is similar to other
available data from Sri Lanka (6) In India 35 of the
patients with OP poisoning require assisted ventilation
(4) Assuming that all patients who reached a hospital
before death were intubated and mechanically venti-
lated we can extrapolate that the mortality rate on OP
poisoning with intensive care support facility would
range from 15ndash20 ie one in five patients will die
despite the availability of intensive care in the
developing countries All the patients in our study
had adequate peripheral oxygen saturation maintained
and hence none of the deaths were a direct conse-
quence of intermediate syndrome [ie the respiratory
muscle weakness observed within 6 to 10 days of OP
poisoning (8)] as they were in an ICU and were
mechanically ventilated The survival graph indicates
that by the end of the third day only 67 survived
Death was common in the subjects with hypotension
during the first 24 h and subjects who needed high-
inspired oxygen concentrations to maintain satisfactory
peripheral oxygen saturation
The current study recognizes that measured
systolic blood pressure less than 100 mmHg and the
need for FiO2gt40 to maintain adequate peripheral
Table 1 Average systolic blood pressure of ventilated
patients during the first 24 h
Number of
deaths
Number of
survivors
SBPlt100 mmHg 18 3
SBPgt100 mmHg 11 32
Table 2 The FiO2 of mechanically ventilated patients
Number of deaths Number of survivors
FiO2 gt40 27 21
FiO2 lt40 2 14
Survival Pattern in Patients with Acute OP Poisoning 345
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
oxygen saturation within the first 24 h since poisoning
are predictors of poor outcome in patients mechanically
ventilated in the ICU Although the odds ratios reach a
statistically significant level the wider confidence
internal particularly seen with low blood pressure as
a risk factor suggests that other factors may also be
contributing significantly to mortality For instance the
type of compound ingested the dose retained duration
since poisoning before being brought to intensive care
duration of hypoxia before therapy and the proportion
of poison removed by gastric lavage are other
immeasurable factors that may be making a contribu-
tion in this context The overall mortality is still high
despite institution of prompt ventilatory support in
addition to gastric lavage at inception and standard
therapy with atropine and pralidoxime Higher mortal-
ity rates in ventilated patients warrant research into
other factors which may influence the final outcome
Our observation of low systolic blood pressure and
requirement of FiO2gt40 suggests global impairment
of myocardial function despite adequate hydration
which can lead to reduction of pulmonary and systemic
circulation The most likely reason for myocardial
depression is the direct effect of OP with structural
damage Povoa et al reported focal myocardial
necrosis in a patient who died following ingestion of
OP who also had prolonged QTc (15) However
parasympathetic overactivity hypoxia acidosis and
electrolyte derangement may also depress the myocar-
dium in patients with OP poisoning Chuang et al in
their series of 223 patients reported that 435 had
prolonged QTc interval on the electrocardiography
(ECG) at presentation and these patients had a
significantly higher mortality and a higher rate of
respiratory failure (13) compared with the patients who
did not display QTc prolongation
CONCLUSION
Deaths due to OP poisoning remain high during
the first 72 h despite optimal respiratory care with
mechanical ventilation and oxygen supplementation
A low systolic blood pressure and a requirement of
FiO2gt40 within the first 24 h of OP poisoning are
predictors of mortality Therefore patients with systolic
blood pressure lt100 mmHg and those who need
FiO2gt40 to maintain their SpO2 above 92 should
be considered as at high risk of death and hence treated
in an intensive care environment Cardiovascular
effects of OP seem to be the major contributor for
mortality when temporary respiratory failure of OP
poisoning is controlled by mechanical ventilation
ACKNOWLEDGMENTS
The authors appreciate the help and support
provided by all medical staff and nursing staff of
Peradeniya Teaching Hospital in the clinical manage-
ment of these patients
REFERENCES
1 Goonasekera CDA Wimalaratne H Karalliedde
LD Changing profile of poisoning in a District
Hospital in Sri Lanka Sri Lanka J Med 1999835ndash38
2 Karalliedde L Senanayake N Pattern of acute
poisoning in a medical unit in central Sri Lanka
Forensic Sci Int 1988 36101ndash1043 Jeyaratnam J de Alwis Seneviratne RS
Copplestone JF Survey of pesticide poisoning
in Sri Lanka Bull WHO 1982 60615ndash6194 Goel A Joseph S Dutta TK Organophosphate
poisoning predicting the need for ventilatory
support J Assoc Phys Ind 1998 46786ndash7905 Bardin PG van Eeden SF Joubert JR Intensive
care management of acute organophosphate poi-
soning a 7-year experience in the western Cape S
Afr Med J 1987 72593ndash5976 Rajapakse VP Wijesekera S Outcome of mechan-
ical ventilation in Sri Lanka Ann R Coll Surg Engl
1989 71344ndash3467 Vasanthathilaka VWJK Goonasekera CDA An
audit of admissions to an intensive care unit in a
regional centre in Sri Lanka Ceylon Med J 199742145ndash148
8 Karalliedde L Senanayake N Organophosphorus
insecticide poisoning Br J Anaesth 1989 63736ndash750
9 Wyckoff DW Davies JE Barquet A Davis JH
Diagnostic and therapeutic problems of parathion
poisonings Ann Intern Med 1968 68875ndash88210 Yamashita M Tanaka J Ando Y Human mortality
in organophosphate poisonings Vet Hum Toxicol
1997 3984ndash8511 Abdollahi M Jalali N Sabzevari O Hoseini R
Ghanea T A retrospective study of poisoning in
Tehran J Toxicol Clin Toxicol 1997 35387ndash39312 Yen DH Yien HW Wang LM Lee CH Chan SH
Spectral analysis of systemic arterial pressure and
346 Munidasa et al
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
heart rate signals of patients with acute respiratory
failure induced by severe organophosphate poi-
soning Crit Care Med 2000 282805ndash281113 Chuang FR Jang SW Lin JL Chern MS Chen JB
Hsu KT QTc prolongation indicates a poor
prognosis in patients with organophophate poison-
ing Am J Emerg Med 1996 14451ndash453
14 Lee P Tai DY Clinical features of patients with
acute organophosphate poisoning requiring inten-
sive care Intensive Care Med 2001 27694ndash69915 Povoa R Cardoso SH Luna Filho B Ferreira
Filho C Ferreira M Ferreira C Organophosphate
poisoning and myocardial necrosis Arq Bras
Cardiol 1997 68377ndash380
Submitted October 28 2003Accepted January 29 2004
Survival Pattern in Patients with Acute OP Poisoning 347
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y

oxygen saturation within the first 24 h since poisoning
are predictors of poor outcome in patients mechanically
ventilated in the ICU Although the odds ratios reach a
statistically significant level the wider confidence
internal particularly seen with low blood pressure as
a risk factor suggests that other factors may also be
contributing significantly to mortality For instance the
type of compound ingested the dose retained duration
since poisoning before being brought to intensive care
duration of hypoxia before therapy and the proportion
of poison removed by gastric lavage are other
immeasurable factors that may be making a contribu-
tion in this context The overall mortality is still high
despite institution of prompt ventilatory support in
addition to gastric lavage at inception and standard
therapy with atropine and pralidoxime Higher mortal-
ity rates in ventilated patients warrant research into
other factors which may influence the final outcome
Our observation of low systolic blood pressure and
requirement of FiO2gt40 suggests global impairment
of myocardial function despite adequate hydration
which can lead to reduction of pulmonary and systemic
circulation The most likely reason for myocardial
depression is the direct effect of OP with structural
damage Povoa et al reported focal myocardial
necrosis in a patient who died following ingestion of
OP who also had prolonged QTc (15) However
parasympathetic overactivity hypoxia acidosis and
electrolyte derangement may also depress the myocar-
dium in patients with OP poisoning Chuang et al in
their series of 223 patients reported that 435 had
prolonged QTc interval on the electrocardiography
(ECG) at presentation and these patients had a
significantly higher mortality and a higher rate of
respiratory failure (13) compared with the patients who
did not display QTc prolongation
CONCLUSION
Deaths due to OP poisoning remain high during
the first 72 h despite optimal respiratory care with
mechanical ventilation and oxygen supplementation
A low systolic blood pressure and a requirement of
FiO2gt40 within the first 24 h of OP poisoning are
predictors of mortality Therefore patients with systolic
blood pressure lt100 mmHg and those who need
FiO2gt40 to maintain their SpO2 above 92 should
be considered as at high risk of death and hence treated
in an intensive care environment Cardiovascular
effects of OP seem to be the major contributor for
mortality when temporary respiratory failure of OP
poisoning is controlled by mechanical ventilation
ACKNOWLEDGMENTS
The authors appreciate the help and support
provided by all medical staff and nursing staff of
Peradeniya Teaching Hospital in the clinical manage-
ment of these patients
REFERENCES
1 Goonasekera CDA Wimalaratne H Karalliedde
LD Changing profile of poisoning in a District
Hospital in Sri Lanka Sri Lanka J Med 1999835ndash38
2 Karalliedde L Senanayake N Pattern of acute
poisoning in a medical unit in central Sri Lanka
Forensic Sci Int 1988 36101ndash1043 Jeyaratnam J de Alwis Seneviratne RS
Copplestone JF Survey of pesticide poisoning
in Sri Lanka Bull WHO 1982 60615ndash6194 Goel A Joseph S Dutta TK Organophosphate
poisoning predicting the need for ventilatory
support J Assoc Phys Ind 1998 46786ndash7905 Bardin PG van Eeden SF Joubert JR Intensive
care management of acute organophosphate poi-
soning a 7-year experience in the western Cape S
Afr Med J 1987 72593ndash5976 Rajapakse VP Wijesekera S Outcome of mechan-
ical ventilation in Sri Lanka Ann R Coll Surg Engl
1989 71344ndash3467 Vasanthathilaka VWJK Goonasekera CDA An
audit of admissions to an intensive care unit in a
regional centre in Sri Lanka Ceylon Med J 199742145ndash148
8 Karalliedde L Senanayake N Organophosphorus
insecticide poisoning Br J Anaesth 1989 63736ndash750
9 Wyckoff DW Davies JE Barquet A Davis JH
Diagnostic and therapeutic problems of parathion
poisonings Ann Intern Med 1968 68875ndash88210 Yamashita M Tanaka J Ando Y Human mortality
in organophosphate poisonings Vet Hum Toxicol
1997 3984ndash8511 Abdollahi M Jalali N Sabzevari O Hoseini R
Ghanea T A retrospective study of poisoning in
Tehran J Toxicol Clin Toxicol 1997 35387ndash39312 Yen DH Yien HW Wang LM Lee CH Chan SH
Spectral analysis of systemic arterial pressure and
346 Munidasa et al
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y
heart rate signals of patients with acute respiratory
failure induced by severe organophosphate poi-
soning Crit Care Med 2000 282805ndash281113 Chuang FR Jang SW Lin JL Chern MS Chen JB
Hsu KT QTc prolongation indicates a poor
prognosis in patients with organophophate poison-
ing Am J Emerg Med 1996 14451ndash453
14 Lee P Tai DY Clinical features of patients with
acute organophosphate poisoning requiring inten-
sive care Intensive Care Med 2001 27694ndash69915 Povoa R Cardoso SH Luna Filho B Ferreira
Filho C Ferreira M Ferreira C Organophosphate
poisoning and myocardial necrosis Arq Bras
Cardiol 1997 68377ndash380
Submitted October 28 2003Accepted January 29 2004
Survival Pattern in Patients with Acute OP Poisoning 347
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y

heart rate signals of patients with acute respiratory
failure induced by severe organophosphate poi-
soning Crit Care Med 2000 282805ndash281113 Chuang FR Jang SW Lin JL Chern MS Chen JB
Hsu KT QTc prolongation indicates a poor
prognosis in patients with organophophate poison-
ing Am J Emerg Med 1996 14451ndash453
14 Lee P Tai DY Clinical features of patients with
acute organophosphate poisoning requiring inten-
sive care Intensive Care Med 2001 27694ndash69915 Povoa R Cardoso SH Luna Filho B Ferreira
Filho C Ferreira M Ferreira C Organophosphate
poisoning and myocardial necrosis Arq Bras
Cardiol 1997 68377ndash380
Submitted October 28 2003Accepted January 29 2004
Survival Pattern in Patients with Acute OP Poisoning 347
Clin
ical
Tox
icol
ogy
Dow
nloa
ded
from
info
rmah
ealth
care
com
by
Uni
vers
ity o
f W
ater
loo
on 1
028
14
For
pers
onal
use
onl
y