Survival and event history analysis - Day 6. Competing...
43
Det Sundhedsvidenskabelige Fakultet Survival and event history analysis Day 6. Competing risks Section of Biostatistics
Transcript of Survival and event history analysis - Day 6. Competing...

Det Sundhedsvidenskabelige Fakultet
Survival and event history analysisDay 6. Competing risks
Section of Biostatistics

Two-state life-death model: one type of event that eventuallywill happen to everyone
Alive Dead-h(t)
The transition rate from state “Alive” to “Dead” is the hazardrate
h(t) ≈ Pr(Dead at time t + dt|Alive at time t)
dt
for small dt.
The survival probability is
S(t) = Pr(Still alive at time t) = exp
(−∫ t
0h(s)ds
)

Examples of hazards
0 5 10 15 20 25 30 35
A
Years
0 20 40 60 80 100
B
Years
0 20 40 60 80
C
Months

Hazard and survival

Hazards are rates not risks (probabilities)Hazard ratios cannot generally be extended to acorresponding ratio of survival or event probabilities (risks).
Pr(Individual 1 dead before time t)
Pr(Individual 2 dead before time t)=
Pr(T1 ≤ t)
Pr(T2 ≤ t)6= hindividual 1(t)
hindividual 2(t)
The hazard ratio is 4 in both plots:
0 2 4 6 8 10
0.0
0.2
0.4
0.6
0.8
1.0
Time
Ris
k (p
roba
bilit
y) o
f dea
th
0 2 4 6 8 10
0.0
0.2
0.4
0.6
0.8
1.0
Ris
k (p
roba
bilit
y) o
f dea
th

Competing risks“All-cause mortality” or “event-free survival” is not always therelevant concept.• In the study of survival after surgery for malignant
melanoma we studied “death from any cause”.Researchers may be interested in assessing factors thatimpact the rate and risk of death from malignantmelanoma, while death from other causes is of secondaryinterest.• In the PBC liver trial we studied “transplant-free
survival” (time to failure of medical treatment defined aseither transplant or death). Here researchers may wantto investigate factors that relate to the rate and/orprobabilty of having a liver transplant instead of thecomposite outcome including also death.

Independent right-censoringSome individuals are incompletely observed. Examples ofpossible causes of termination of follow-up in a study oftime-to-cancer
• End of study• Emigration (loss to follow-up)• Death in traffic accident• Death from thrombosis
Censoring must be independent of the time to cancer.• Violated if the most severly ill patients are censored and
only the healthiest are observed• Censoring by being alive when the study ends can
typically be taken to be independent, but for subjectslost to follow-up, one may be more suspicious

Competing events and right-censoring
The occurrence of a competing event may change the rate foror preclude events of the type of interest (i.e., the event is notindependent censoring)
• Our aim is to estimate population quantities correctlybased on data where there are independent censoringsand possibly competing events• In the survival model we deal with censorings and
estimate the population survival S(t)• In the competing risks model, we want to estimate the
probability of seeing a cause l event in an uncensoredpopulation (in the presence of other events)

Competing risks
An individual can die from K different causes of death
Alive
Dead from cause K
������3
�������7
SSSSSSSw
Dead from cause 2
Dead from cause 1
.
.
.
hK (t)
h1(t)
h2(t)

Cause-specific hazards
Alive
Dead cause K
���3-����7
SSSSw
Dead cause 2
Dead cause 1
...
Transition form the state “Alive” to the state “Dead fromcause l” is governed by the cause-specific hazard hl(t).
hl(t) ≈Pr(Dead from cause l at time t + dt|Alive at time t)
dt
for small dt.
Cause-specific hazards give a local description of themechanisms by which subjects may fail.

Cause-specific hazards and survival
The overall mortality rate is
h(t) = h1(t) + . . .+ hK (t)
and the survival probability is
S(t) = exp
(−∫ t
0h(s)ds
)= exp
(−∫ t
0h1(s) + . . .+ hK (s)ds
)The survival probability depends on all cause-specific hazards.

Inference for cause-specific hazards
Standard methods for inference on the hazard are valid alsofor cause-specific hazards.
When estimating cause-specific hazards for cause l , we treatdeaths from causes other than l as censorings, and proceed“as usual”
• Cox regression for cause-specific hazards• Model checking can be done as for all-cause mortality• Nelson-Aalen estimate for the cumulated hazard

Mortality hazard after m. melanoma operationmelanoma <- read.csv2("http://publicifsv.sund.ku.dk/~frank/data/melanoma.csv")library(survival)
# All-cause mortality ratecox.overall <- coxph(Surv(days, status!=2)~sex+age, data=melanoma)summary(cox.overall)$conf.int
## exp(coef) exp(-coef) lower .95 upper .95## sex 1.74091 0.5744122 1.087201 2.787678## age 1.02676 0.9739379 1.010685 1.043090
# Melanoma deathcox.melanoma <- coxph(Surv(days, status==1)~sex+age, data=melanoma)summary(cox.melanoma)$conf.int
## exp(coef) exp(-coef) lower .95 upper .95## sex 1.818949 0.5497680 1.0764804 3.073512## age 1.016679 0.9835944 0.9995631 1.034089
# Non-melanoma deathcox.other <- coxph(Surv(days, status==3)~sex+age, data=melanoma)summary(cox.other)$conf.int
## exp(coef) exp(-coef) lower .95 upper .95## sex 1.446435 0.6913551 0.4949803 4.226780## age 1.078759 0.9269908 1.0341484 1.125295

Nonparametric hazard estimation
(Cause-specific) hazard rates hl(t) are difficult to estimatedirectly, but the cumulative hazard Hl(t) =
∫ t0 hl(s)ds can be
estimated easily by the Nelson-Aalen estimator.
The hazard can then be approximated by the “local slope” ofthe cumlative hazard.
In R, the Nelson-Aalen estimator can be estimated by thecommand survift and plotted bykmplot(.,fun="cumhaz") from the timereg package.
This is true for all-cause mortality rates as well as forcause-specific rates.

Melanoma data : Cause-specific Nelson-Aalenlibrary(timereg)par(mfrow=c(1,2)) # Plot 1 row, 2 columnsna.melanoma <- survfit(Surv(days, status==1)~sex, data=melanoma)kmplot(na.melanoma, fun="cumhaz", main="Melanoma death")
na.melanoma <- survfit(Surv(days, status==3)~sex, data=melanoma)kmplot(na.melanoma, fun="cumhaz", main="Non-melanoma death")
0 1000 2000 3000 4000 5000
0.0
0.1
0.2
0.3
0.4
0.5
0.6
Melanoma death
sex=0sex=1
0 1000 2000 3000 4000 5000
0.00
0.05
0.10
0.15
0.20
Non−melanoma death
sex=0sex=1

Survival after bone marrow transplant1715 leukemia patients recieved a bone marrow transplant(International Bone Marrow Transplant Registry). At the endof the follow-up period (median 37.2 months)• 311 patients relapsed• 557 patients died in remission• 847 patients still alive and in remission (right-censored)
Death
Completeremisson
Relapse

Survival after bone marrow transplant
Information on• time from transplant to event or censoring (months)• event : 0=censoring; 1=relapse; 2=death in remission• donor : 1=HLA identical sibling (n=1224); 2=HLA
matched unrelated (n=383); 3=HLA mismatchedunrelated (n=108)• stage : 1=early; 2=intermediate; 3=advanced stage at
transplantation
Purpose: comparison of relapse and death in remissionbetween patients with different donor types.

bmt <- read.csv2("http://publicifsv.sund.ku.dk/~frank/data/bmt1715.csv")par(mfrow=c(1,2)) # Plot 1 row, 2 columnsna1 <- survfit(Surv(time, event==1)~donor, data=bmt)kmplot(na1, fun="cumhaz", main="Relapse", lty=1, add.legend=FALSE, conf.int=FALSE,
xlab="Time since transplant (months)", ylab="Cumulative hazard")legend("bottomright", inset=.05,lty=1, col=1:3, title="HLA",
legend=c("identical sibling","matched unrelated", "mismatched unrelated"))na2 <- survfit(Surv(time, event==2)~donor, data=bmt)kmplot(na2, fun="cumhaz", main="Death in remission", lty=1, add.legend=FALSE, conf.int=FALSE,
xlab="Time since transplant (months)", ylab="Cumulative hazard")legend("right", inset=.05,lty=1, col=1:3, title="HLA",
legend=c("identical sibling","matched unrelated", "mismatched unrelated"))
0 20 40 60 80
0.0
0.1
0.2
0.3
Relapse
Time since transplant (months)
Cum
ulat
ive
haza
rd
HLA
identical siblingmatched unrelatedmismatched unrelated
0 20 40 60 80
0.0
0.2
0.4
0.6
0.8
1.0
1.2
Death in remission
Time since transplant (months)
Cum
ulat
ive
haza
rd
HLA
identical siblingmatched unrelatedmismatched unrelated

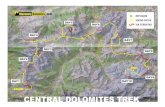
Survival after bone marrow transplantThe “local slope” of the cumulative hazard approximates thehazard.
The plots suggest that• Patients with HLA mismatched unrelated donors have
lower relapse rate than patients with HLA identicalsibling donors.• Little sign of a difference in relapse rates between HLA
matched unrelated donors and HLA identical siblingdonors• HLA identical sibling donors have lower treatment related
mortality rate than HLA matched unrelated donors• HLA matched unrelated donor patients have lower
treatment related mortality rate than patients with HLAmismatched unrelated donors

Cause-specific risks
Cause-specific hazards describe the rates of the mechanimsdriving the events. One might also be interested in the risk(probability) of a specific cause of death over a time period• What is the risk of having a liver transplantation within a
year for a CyA treated PBC patient with albumin 40g/L?• What fraction of the melanoma patients will die from the
disease within 2 years after tumour removal?• What is the probability of recurrence of the leukemia
within 8 months for a patient recieving HLA identicalbone marrow transplant from a sibling?
These questions relate to risks rather than rates and are notlocal, but cumulated over time.

Cause-specific risksThe cumulative incidence function for cause l is theprobability of death from cause l before time t
Fl(t) = Pr(Dead from cause l time ≤ t) =
∫ t
0S(s)hl(s)ds
where S(t) = exp(−∫ t0 h1(s)− . . .− hK (s)ds
).
Note that the cumulative incidence for cause l depends onthe cause-specific hazard rates of all causes through thesurvival function S(t).
The survival probability is the probability of not having diedfrom any of the risks
S(t) = 1− F1(t)− . . .− FK (t)

Nonparametric cumulative incidence estimation
The overall survival function S(t) can be estimated by theKaplan-Meier estimator S(t) for death from any case.
The cumulative incidence
Fl(t) = Pr(Dead from cause l time ≤ t) =
∫ t
0S(s)hl(s)ds
can be estimated by plugging in the estimated S(t) and thejumps of the Nelson-Aalen estimate Hl(t).
The estimator is called the Aalen-Johansen estimator.

The Aalen-Johansen estimator can be estimated by prodlimwith Hist() instead of Surv()
aj1 <- prodlim(Hist(time, event)~1, data=bmt) # Hist() instead of Surv()par(mfrow=c(1,2))plot(aj1, cause=1, plot.main="Relapse") # Plot cause 1plot(aj1, cause=2, plot.main="Death in remisson") # Plot cause 2
Relapse
Time
Cum
ulat
ive
inci
denc
e
0 20 40 60 80
0 %
25 %
50 %
75 %
100
%
1715900 732 573 398 274 165 85 36 10 1Subjects:
Death in remisson
TimeC
umul
ativ
e in
cide
nce
0 20 40 60 80
0 %
25 %
50 %
75 %
100
%1715900 732 573 398 274 165 85 36 10 1Subjects:
Independent censoring should be labelled 0.

Relapse
Time
Cum
ulat
ive
inci
denc
e
0 20 40 60 80
0 %
50 %
100
%
1715900 732 573 398 274 165 85 36 10 1Subjects:
Death in remisson
Time
Cum
ulat
ive
inci
denc
e
0 20 40 60 80
0 %
50 %
100
%
1715900 732 573 398 274 165 85 36 10 1Subjects:
summary(aj1, times=c(20,80)) # CIF and 95%CI at specific times
###### ----------> Cause: 1#### time n.risk n.event n.lost cuminc se.cuminc lower upper## 1 20 714 0 0 0.157 0.00907 0.139 0.175## 2 80 18 0 0 0.221 0.01226 0.197 0.245###### ----------> Cause: 2#### time n.risk n.event n.lost cuminc se.cuminc lower upper## 1 20 714 0 0 0.325 0.0116 0.303 0.348## 2 80 18 0 0 0.346 0.0122 0.322 0.370

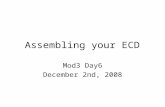
Probability (risk) of relapse (left) and treatment related death(right) after bone marrow transplant according to HLA match
par(mfrow=c(1,2))aj <- prodlim(Hist(time, event)~donor, data=bmt)plot(aj, cause=1, plot.main="Relapse",
legend.legend=c("identical sibling","matched unrelated", "mismatched unrelated"))
plot(aj, cause=2, plot.main="Death in remission",legend.legend=c("identical sibling","matched unrelated", "mismatched unrelated"))
Relapse
Time
Cu
mu
lative
in
cid
en
ce
0 20 40 60 80
0 %
25
%5
0 %
75
%1
00
%
donor1224 735 609 488 340 239 148 80 34 10 11: 383 132 103 68 43 25 10 3 0 0 02: 108 33 20 17 15 10 7 2 2 0 03:
identical siblingmatched unrelatedmismatched unrelated
Death in remission
Time
Cu
mu
lative
in
cid
en
ce
0 20 40 60 80
0 %
25
%5
0 %
75
%1
00
%
donor1224 735 609 488 340 239 148 80 34 10 11: 383 132 103 68 43 25 10 3 0 0 02: 108 33 20 17 15 10 7 2 2 0 03:
identical siblingmatched unrelatedmismatched unrelated

0 20 40 60 80
0.0
0.1
0.2
0.3
Relapse
Time since transplant (months)
Cum
ulat
ive
haza
rd
HLA
identical siblingmatched unrelatedmismatched unrelated
0 20 40 60 80
0.0
0.2
0.4
0.6
0.8
1.0
1.2
Death in remission
Time since transplant (months)
Cum
ulat
ive
haza
rd
HLA
identical siblingmatched unrelatedmismatched unrelated
Time since transplant (months)
Cum
ulat
ive
inci
denc
e
0 20 40 60 80
0 %
25 %
50 %
75 %
100
%
Relapse
HLA
identical siblingmatched unrelatedmismatched unrelated
Time since transplant (months)
Cum
ulat
ive
inci
denc
e
0 20 40 60 80
0 %
25 %
50 %
75 %
100
%
Death in remission
HLA
identical siblingmatched unrelatedmismatched unrelated

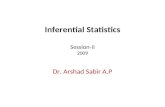
Hazard and risk for relapse and treatmentrelated mortalityThe plots on the previous slide show the cumulative hazards(upper row) and cumulative incidences (lower row) accordingto HLA match.
1 Does recieving bone marrow from an HLA matchedunrelated compared to form a HLA identical siblingdonor increase or decrease the hazard for relapse ?
2 Does recieving bone marrow from an HLA matchedunrelated compared to from a sibling donor increase ordecrease the risk of relapse ?
3 Relate the two answers above to each other and totreatment related mortality
4 Would you choose a HLA mismatched unrelated or aHLA identical sibling donor if you had the choice?

Gray’s test
We can test if the cumulative incidence is equal in groups(e.g., treatment, donor match) with the nonparametric Gray’stest.• Gray’s test is used for checking if cumulative incidence
curves are the same at all time points t• Can test the equivalence of the cumulative incidence
between groups for each cause (i.e., we can perform onetest per cause)• Gray’s test is an extension of the log-rank test to the
competing risks setting (without competing risks thetests are identical)

Gray’s test in R
library(cmprsk)cuminc(bmt$time, bmt$event, bmt$donor)
## Tests:## stat pv df## 1 11.76072 0.002793773 2## 2 161.28025 0.000000000 2## Estimates and Variances:## $est## 20 40 60 80## 1 1 0.16893575 0.21016909 0.24535186 0.24535186## 2 1 0.14424091 0.16423335 0.17798257 NA## 3 1 0.06706941 0.07914268 0.07914268 0.07914268## 1 2 0.23916032 0.25170457 0.25788874 0.25788874## 2 2 0.50704439 0.53328371 0.54932447 NA## 3 2 0.69146531 0.69146531 0.69146531 0.69146531#### $var## 20 40 60 80## 1 1 0.0001212894 0.0001569526 0.0002271119 0.0002271119## 2 1 0.0003532375 0.0004393534 0.0006124871 NA## 3 1 0.0006129920 0.0007467670 0.0007467670 0.0007467670## 1 2 0.0001544662 0.0001636895 0.0001739834 0.0001739834## 2 2 0.0007176358 0.0007810226 0.0009844068 NA## 3 2 0.0021786565 0.0021786565 0.0021786565 0.0021786565

Cause-specific risks
Without competing risks the cumulative incidence is
F (t) = Pr(T ≤ t) = 1− S(t) = 1− exp
(−∫ t
0h(s)ds
)but with competing risks this relation no longer holds. Instead
Fl(t) =
∫ t
0S(s)hl(s)ds ≤ 1− exp
(−∫ t
0hl(s)ds
)The size of the difference depends on the strength of therates for the causes other than l .
Conclusion: When calculating cumulative incidences (risks,probailities) we cannot treat competing events as censorings.

Quantities like
exp
(−∫ t
0hl(s)ds
)estimated by the Kaplan-Meier estimator where events fromcompeting causes are treated as censorings are hard tointerpret
It estimates the survival probability in a world where all othercauses have been removed without changing the mortalityrate for cause l .
Do not use Kaplan-Meier for one cause when estimatingsurvival in the presence of competing risks

Cause-specific hazards and cumulative incidences
• Cumulative incidences Fl (risks, probailities)I Are not local in time but cumulated and we cannot treat
competing events as censorings.• The cause-specific hazards hl(t)
I Are local in time and calculated conditional on beingalive at time t. Therefore we can treat competing eventsas censorings.
I When assessing the local strength of a cause in the shortinterval [t, t + dt), the other causes need not be takeninto account (we are conditioning on no death from anycause before time t)

Censoring or competing risk?
We wish to estimate the population parameters S(t), Fl(t)and hl(t) based on censored data.
• Independent censoringI Individuals censored at time t should not be a biased
sample of those at risk at time tI The extra information that the subject is not only alive,
but also uncensored at time t does not change thefailure rate
• The complete non-censored population must bewell-defined. Everyone will experience an event if we waitlong enough.

Cause-specific hazards regressionTreat competing events as censorings and fit a model (e.g.Cox) for each cause• Easy to fit. Just treat competing events as censorings.• Describes the mechanism driving the events• We can estimate the cumulative incidence for cause l by
estimating all cause-specific hazards and plugging theminto the formula
Fl(t|X = x)
= Pr(Death from cause l at time ≤ t given covariates x)
=
∫ t
0S(s|x)hl(s|x)ds
=
∫ t
0exp
(−∫ s
0h1(u|x) + . . .+ hK (u|x)du
)hl(s|x)ds

library(riskRegression)bmt$donor <- factor(bmt$donor)bmt$stage <- factor(bmt$stage)csc1 <- CSC(Hist(time,event)~donor+stage, data=bmt)csc1
## CSC(formula = Hist(time, event) ~ donor + stage, data = bmt)#### Right-censored response of a competing.risks model#### No.Observations: 1715#### Pattern:#### Cause event right.censored## 1 311 0## 2 557 0## unknown 0 847###### ----------> Cause: 1#### Call:## survival::coxph(formula = survival::Surv(time, status) ~ donor +## stage, x = TRUE, y = TRUE)#### n= 1715, number of events= 311#### coef exp(coef) se(coef) z Pr(>|z|)## donor2 -0.05941 0.94232 0.14998 -0.396 0.6920## donor3 -0.90361 0.40511 0.36068 -2.505 0.0122 *## stage2 0.74655 2.10971 0.14840 5.031 4.89e-07 ***## stage3 2.07002 7.92497 0.13394 15.455 < 2e-16 ***## ---## Signif. codes: 0 '***' 0.001 '**' 0.01 '*' 0.05 '.' 0.1 ' ' 1#### exp(coef) exp(-coef) lower .95 upper .95## donor2 0.9423 1.0612 0.7023 1.2643## donor3 0.4051 2.4685 0.1998 0.8214## stage2 2.1097 0.4740 1.5773 2.8219## stage3 7.9250 0.1262 6.0952 10.3041#### Concordance= 0.718 (se = 0.015 )## Likelihood ratio test= 209.4 on 4 df, p=<2e-16## Wald test = 244.4 on 4 df, p=<2e-16## Score (logrank) test = 316 on 4 df, p=<2e-16######## ----------> Cause: 2#### Call:## survival::coxph(formula = survival::Surv(time, status) ~ donor +## stage, x = TRUE, y = TRUE)#### n= 1715, number of events= 557#### coef exp(coef) se(coef) z Pr(>|z|)## donor2 0.89384 2.44449 0.09506 9.403 < 2e-16 ***## donor3 1.15925 3.18753 0.13416 8.641 < 2e-16 ***## stage2 0.51135 1.66754 0.09903 5.164 2.42e-07 ***## stage3 0.76171 2.14193 0.11561 6.588 4.45e-11 ***## ---## Signif. codes: 0 '***' 0.001 '**' 0.01 '*' 0.05 '.' 0.1 ' ' 1#### exp(coef) exp(-coef) lower .95 upper .95## donor2 2.444 0.4091 2.029 2.945## donor3 3.188 0.3137 2.451 4.146## stage2 1.668 0.5997 1.373 2.025## stage3 2.142 0.4669 1.708 2.687#### Concordance= 0.662 (se = 0.011 )## Likelihood ratio test= 204.1 on 4 df, p=<2e-16## Wald test = 219.3 on 4 df, p=<2e-16## Score (logrank) test = 241.2 on 4 df, p=<2e-16

The output from the CSC() function from the packageriskRegression reveals no evidence for a difference inrelapse-specific hazard between patients with HLA mathcedbone marrow from a siblibng or an unrealted donor with thesame disease stage (p=0.69).
We can draw predicted cumulative incidence curves forspecific choices of covariates with the functionplotPredictEventProb() from the pec package.

Predicted cumulative incidence, Stage 3 patientslibrary(pec)nd <- data.frame(donor=factor(c("1","2","3"), levels=levels(bmt$donor)),
stage=factor("3", levels=levels(bmt$stage)))plotPredictEventProb(csc1, newdata=nd, cause=1, col=1:3)legend("topleft", inset=.05, lty=1, col=1:3,
c("HLA identical sibling donor, stage 3","HLA matched unrelated donor, stage 3","HLA mismathced unrelated donor, stage 3"))
Time
Eve
nt p
roba
bilit
y
0 20 40 60 80
0.00
0.25
0.50
0.75
1.00
HLA identical sibling donor, stage 3HLA matched unrelated donor, stage 3HLA mismathced unrelated donor, stage 3

Predicted cumulative incidence, Stage 1 patientsnd <- data.frame(donor=factor(c("1","2","3"), levels=levels(bmt$donor)),
stage=factor("1", levels=levels(bmt$stage)))plotPredictEventProb(csc1, newdata=nd, cause=1, col=1:3)legend("topleft", inset=.05, lty=1, col=1:3,
c("HLA identical sibling donor, stage 1","HLA matched unrelated donor, stage 1","HLA mismathced unrelated donor, stage 1"))
Time
Eve
nt p
roba
bilit
y
0 20 40 60 80
0.00
0.25
0.50
0.75
1.00
HLA identical sibling donor, stage 1HLA matched unrelated donor, stage 1HLA mismathced unrelated donor, stage 1

Cumulative incidences from cause-specific Coxmodels• The Cox model imposes a simple structure between
covariates and rates (cause-specific hazards)• Due to the complicated relationship between rates and
risks in a competing risks model, the simple relationshipin the Cox model does not carry over to the cumulativeincidences
Pr(Death from cause l at time ≤ t given covariates x)
=
∫ t
0exp
(−
K∑k=1
∫ s
0h0k(u)e
βTk xdu
)h0l(s)e
βTl xds
• The way in which a covariate affects a rate can be verydifferent from the way in which it affects thecorresponding risk: this will depend on how it affects therates for the competing causes.

Direct cumulative incidence regression
• Hard to evaluate the effect of covariates on thecumulative incidence because of the complex relationbetween hazards and risk in competing risks models• Cumulative incidence function (CIF) regression models
estimate the effect of covariates on the cumulativeincidence directlyI Fine & Gray’s regression modelI Proportional odds / logistic risk regression

Summary• In studies of all-cause mortality, there is a one-to-one
correspondance between rates (hazard) and risk(probability of event). One may be obtained from theother.• Without competing events, e.g. in studies of all-cause
mortality, the cumulative incidence can be calculated as1 minus the Kaplan-Meier curve• In studies where the event will not happen to everyone in
the population, this is no longer the case• With competing risks, using “1-Kaplan-Meier for a single
cause” is upwards biased and should not be used forestimating risks• The magnitude of the bias depends on the frequency of
the competing events

Summary
• A rather simple, unbiased estimator for the risk exists -the “Aalen-Johansen” estimator• Effects of covariates on rates (cause-specific hazards)
may be (qualitatively) different from their effects on therisks (cumulative incidences)• Rates may be analysed using standard hazard-based
methods from survival analysis (Nelson-Aalen, Cox,...)• Risks may be analyzed by “plugging in” results from such
hazard models

Summary
• Cause-specific hazards are easy to estimate (e.g., Coxregression)• Cause-specific hazards are driving the underlying
dynamics• Can be hard to say what the effect on the risk of an
event is from the cause-specific hazards• Cumulative incidences are easy (easier?) to interpret
Both cause-specific hazards and cumulative incidencefunctions are useful and needed for a complete description inthe competing risks setting.
“Rates are good for etiological questions and risks forprediction” (Koller et. al., Stat.Med., 2012)