
Surgical Treatment of Atrial Fibrillation (A Fib or AF) · PDF fileSurgical Treatment of...
58
Surgical Treatment of Atrial Fibrillation (A Fib or AF) Innovation in Care Sponsored by Florida Hospital East Florida Region June 15, 2016 William H. Johnson, III, M.D. Fellow of American College of Surgeons Atlantic Cardiovascular & Thoracic Surgeons, LLC
Transcript of Surgical Treatment of Atrial Fibrillation (A Fib or AF) · PDF fileSurgical Treatment of...

Surgical Treatment of Atrial Fibrillation
(A Fib or AF)Innovation in Care
Sponsored by Florida Hospital East Florida RegionJune 15, 2016
William H. Johnson, III, M.D.Fellow of American College of SurgeonsAtlantic Cardiovascular & Thoracic Surgeons, LLC

Most common cardiac arrhythmia

What is Atrial Fibrillation?
Irregular beating of the atria
caused by irregular electrical
signals. The atria and the
ventricles lose their synchrony.

• A-Fib affects more than 2.5 million adults
• 80% are older than 65 years old
• The number of AF patients is predicted to
double in the next 40 years

The U.S. Healthcare Burden of Atrial FibrillationFastest Growth Area in Cardiology
$0
$50
$100
$150
$200
$250
$300
0
2
4
6
8
10
12
14
16
18
2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050 Po
ten
tial
Co
st t
o U
.S.
Hea
lth
Sys
tem
Bil
lio
ns
Pro
ject
ed U
.S. A
F P
op
ula
tio
n1
Mil
lio
ns
YearProjected AF Population Estimated Healthcare Costs
1Miyasaka Y, et al. Secular trends in incidence of atrial fibrillation in Olmsted county, Minnesota, 1980 to 2000, and implications on the projections for future prevalence.
Circulation. 2006;114:119-125.2Wu EQ, et al. Economic Burden and Co-Morbidities of Atrial Fibrillation in a Privately Insured Population. Curr Med Res Opin. 2005;21(10):1693-1699.3Ball J, et al. Atrial fibrillation: Profile and burden of an evolving epidemic in the 21st century. Int J Card. 2013;167:1807-1824.
$14,985 Annual Direct + Indirect Costs2
“AF represents an evolving, global epidemic providing considerable challenges
to minimize its impact from an individual to whole society perspective.”3

Convergent Approach Can Help Address An Unmet Need
Colilla S, et al. Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013;doi/10.1016/j.amjcard.2013.05.063.
Jahangir A, et al. Long-term progression and outcomes with aging in patients with long atrial fibrillation: a 30-year follow-up study. Circulation 2007;115:3050-3056.
Amin AN, et al. Hospital readmissions in US atrial fibrillation patients: occurrence and costs. Am J Ther. 2013;20:143-150.
Vaziri S. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Study. Circulation 1994;89;724-730.
Catheter Ablation
Potential U.S. Marketn=290,000
Unmet Potential U.S.
Marketn=4,750,000
Untreatable
Populationn=860,000

A-Fib patients are associatedwith significant mortality andmorbidity

A-Fib patients are at an increasedrisk for:
Stroke
Heart failure
Death

A-Fib patients who are within oneyear of initial onset:
• Almost double the stroke rate of
non-AF patients (23.1% vs 13.3%)
• 3 times more likely to experience
congestive heart failure than non-
AF patients (36.7% vs 10.4%)

A-Fib costs the U.S. $15.7 billion annually treating newly diagnosed A-Fib.
Medicare also spends $8 billion annually treating strokes in patients with A-Fib.

3 Physiologic Consequences of A-Fib
• Abnormal atrial function with stasis of atrial
blood—increased risk of thromboembolism
• Loss of coordinated atrioventricular contractions
(atrial kick), leading to hemodynamic compromise
• Palpitations—can cause significant anxiety and
discomfort

Other Symptoms of A-Fib
Lightheadness
Extreme fatigue
Shortness of breath
Chest pain

Risk Factors in Developing A-Fib
Increased age (80% are >65 years old
Hypertension
Obesity
European ancestry
Diabetes
Heart failure
Ischemic heart disease
Chronic kidney disease
Heavy alcohol use

Classifications of A-Fib
• Paroxysmal – 2 or more episodes
spontaneously terminating within 7 days
• Persistent - >7 days and needs
pharmacologic or electrical conversion
• Longstanding - >1 year duration
• Permanent – decision to not attempt
restoration of sinus rhythm by any
means
A-Fib Treatment Options
• Non-invasive
• Invasive

Non-Invasive Treatments
• Rhythm conversion by medications and/or
cardioversion
• Rate control by medication
• Anticoagulation
• Managing the risk factors

Invasive Treatments
• Catheter ablations
• Open surgical procedures:
Ablations combined with other cardiac
surgical procedures
Stand-alone open surgical procedures
such as the Cox-Maze procedures and
thorascopic pulmonary vein ablations
• Hybrid a-fib ablation—combines elements of
minimally invasive and catheter based
ablations

Longstanding persistent A-Fib is the most difficult to manage (>1 year duration)
This is the most common type of A-Fib treated by invasive measures

A study by Tilz RR, et al, in the JAM Coll Cardiology 2012, Nov 6,60 (19) 1921-9, reviewed the 5year efficacy of catheter ablationfor longstanding persistent A-Fib.

Results: After the first ablation,20.3% were in sinus rhythm.After multiple ablations, 45%were in sinus rhythm.

Because of results like these,there has been a search to finda procedure that can give thehighest conversion rate at onesetting

Indications for Invasive Procedures
• A-Fib patients undergoing elective cardiac
surgery
• Younger patients who have failed all other
attempts at conversion
• Patients with contraindications for
anticoagulation
• Thromboembolism while anticoagulated

Dr. James Cox, a cardiacsurgeon, is considered thefather of open surgicaltreatment for A-Fib

His procedures have evolvedover time, but still requiremajor surgery and CPB

Results of the Cox-Maze IV procedure asdescribed by Damiano and Baily in theMultimedia Manual of CardiothoracicSurgery, Volume 2007, Issue 0723,showed over 90% cure rate of paroxysmaland permanent A-Fib

Because of the complexity andrequirement for CPB, not manypatients wish to go this routefor treatment of their A-Fib

The Hybrid Atrial Fibrillationprocedure combines minimallyinvasive surgery with catheterablation

Multidisciplinary OutcomesSinus Rhythm & Repeat Ablation Procedures
Published Convergent Articles / Presentations
1. Civello, K, et al. HRS Scientific Sessions, May 2012.
2. Gilligan DM, et al. HRS Scientific Sessions. May 2012.
3. Golden K, et al. Boston AF Symposium. January 2012.
4. Golden K, et al. HRS Scientific Sessions. May 2012.
5. Gersak B, et al. JCE. 2012;23:1059-1066.
0%
20%
40%
60%
80%
100%
%SinusRhythm@
1Year
0%
20%
40%
60%
80%
100%
%RepeatPro
cedures@
1Year
Catheter Ablation OutcomesSinus Rhythm & Repeat Ablation Procedures
Published Catheter Ablation Articles / Presentations
1. Packer, et al. ACC Scientific Sessions. March 15, 2010.
2. Weerasooriya R, et al. J Am Coll Cardiol. 2011;57:160-6.
3. Boersma LVA, et al. Circulation. 2012;125(1):23-30.
4. Sorgente A, et al. Am J Cardiol. 2012;109:1179-1186.
5. Packer, et al. ACC Scientific Sessions. March 15, 2010.
6. Tilz RR, et al. J Am Coll Cardiol. 2012; doi:10.1016/j.jacc.2012.04.060.
0%
20%
40%
60%
80%
100%
%SinusRhythm@
1Year
0%
20%
40%
60%
80%
100%%
Re
pe
at
Pro
ced
ure
s @
1 Y
ea
r
1
4
2
3
6
5
2
6
5
4
1
2
5
3
1
4
15
4
2
3
Performance Improvement Indicator: Minimizes Re-hospitalizations
Standardization Drives Consistent Results Across Sites

51%
40%
32%
23%
63%
53%
45%
39%
36%
26%23% 20%
61%
50%46% 45%
88% 87%84%
0%
20%
40%
60%
80%
100%
0 1 2 3 4 5 6
Sin
us
Rh
yth
m
Single Procedure
[Sorgente]
Multiple Procedure (1.5/pt)
[Sorgente]
Single Procedure
[Tilz]
Multiple Procedure (1.9/pt)
[Tilz]
Single Procedure
[Gersak, JCE 2012]
Multiple Procedure (1.09/pt)
[Gersak, Boston AF 2014]
1. Sorgente A, Tung P, Wylie J, Josephson ME. Six year follow-up after catheter ablation of atrial fibrillation: a palliation more than a true cure. Am J Cardiol. 2012;109:1179-1186.
2. Tilz RR, et al. Catheter ablation of long-standing persistent atrial fibrillation: 5-year outcomes of the Hamburg sequential ablation strategy. J Am Coll Cardiol. 2012;
doi:10.1016/j.jacc.2012.04.060.
3. Gersak B, et al. Low rate of atrial fibrillation recurrence verified by implantable loop recorder monitoring following a Convergent epicardial and endocardial ablation of atrial fibrillation.
JCE. 2012;23:1059-1066.
4. Gersak B, et al. Prospective Reveal XT Outcomes for the Convergent Atrial Fibrillation Ablation Procedure. Boston AF Symposium. 2014:Jan 9-11, Orlando, FL.
Performance Improvement Indicator: Sustainable Outcomes
MULTIDISCIPLINARY PROCEDURE
SINGLE CATHETER ABLATIONS
MULTIPLE CATHETER ABLATIONS
YEARS
Multidisciplinary Results monitored
by loop recorders for up to 3 Years

Published and Presented Results
Presented Data
% Persistent/
LongstandingAF
MonitoringLevel
Sinus Rhythm @ MeanFollow up
RedosSerious Adverse
Event Rate
Boedefeld, WM.
Northeast Cardiothoracic Surgical Society 2014
N=224
66%72 hr – 14 day Holters &
Implanted Devices93% @ 1 yr 6% 2.7%
Child N, et al. HRC UK 2014
N=19100% Holters 90% @ 1 yr (9 of 10) 5.3% 15.8%
Mittal S, et al. ESC 2014
N=23 (persistent cohort)100%
EKG, Loop Recorder or
Implanted Devices83% @ 1 yr
Not
reportedNot reported
Pajitnev D, et al. HRS 2014
N=28 Convergent
N=28 Endocardial only ablation
100%
100%
Reveals
72 hr Holters
71% @ 2 yrs
Convergent
36% @ 2 yr
Endocardial-only ablation
0%
0%
3.5% overall
Zembala M, et al. AATS 2014
N=49 100% 7 day Holters 85% @ 1 yr
Not
reportedNot reported
Gersak B, et al.
AF Symposium 2014
N=76
95% All Reveals 84% @ 3 yrs 10% 10.0%
Gilligan D, et al.
JICRM Oct 2013:4(10): 1396-1403
N=42
81% 72 hr Holters 95% @ 1 yr 9% 4.7%
Civello K, et al.
JICRM Sept 2013:4(9): 1367-1373
N=104
73% 72 hr Holters 88% @ 1 yr 2.8% 5.8%

Published and Presented Results (continued)
Presented Data% Persistent/LongstandingAF
MonitoringLevel
Sinus Rhythm @ MeanFollow up
RedosSerious Adverse
Event Rate
Gersak B, et al.
JTCVS Nov 2013: 1-6. Epub
N=73
100% Reveals or 7 day Holters 80% @ 1 yr 4% 11.0%
Thosani AJ, et al.
AER 2013;2(1):65–8
N=43
86% 2 wk Monitors 89% @ 6 mo 0% 0%
Robinson MC, et al.
EP Lab Digest 2012;13(6):34-36
N=42
100% EKG & Holter Monitors 89% @ 13 mo 4.8% 7%
Gersak B, et al.
JCE 2012;23:1059-66
N=50
94% All Reveals 88% @ 1 yr 2% 10.0%
Olson J, et al.
AF Symposium 2012
N=115
83.5% 72 hr Holters 84% @ 11.4 mo 4% 6.1%
Golden K, et al. HRS 2012
N=6188% 72 hr Holters 79% @ 11 mo 8% 3.3%

Hybrid A-Fib Ablation
Minimally invasive surgery plus
catheter ablation

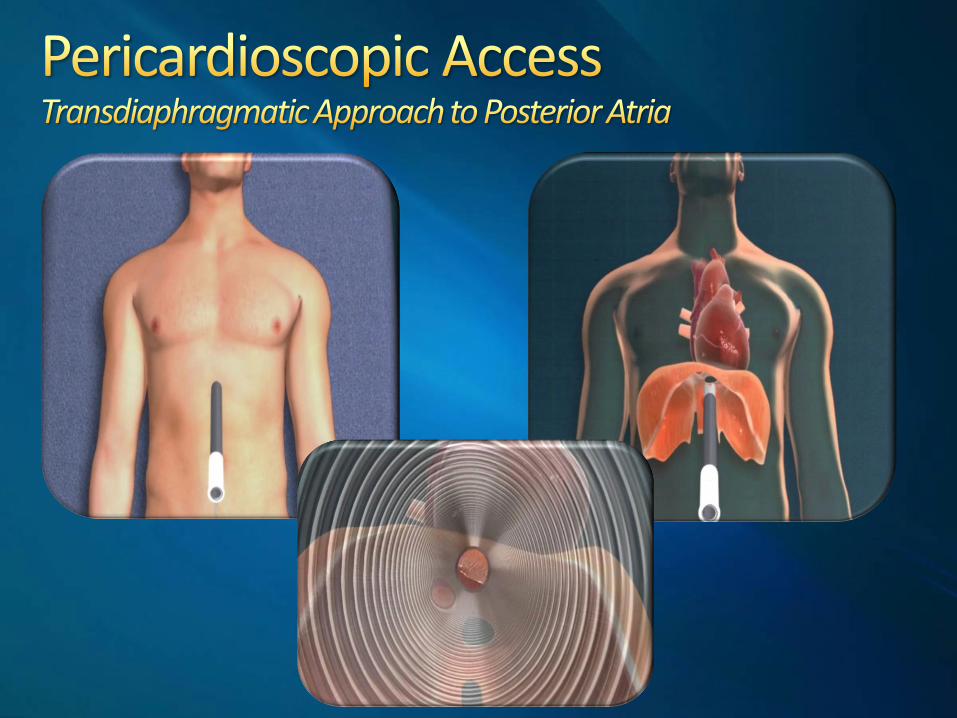
SUBTLE® access enables a transdiaphragmatic approach that provides the ability to access the posterior region of a beating heart. The closed chest approach offers surgeons direct visualization to the posterior of a beating heart through endoscopes, enabling the ability to create bi-atrial, linear lesions without chest incisions or ports.

34
Epicardial ablation to create complete lesionsVacuum contact provides consistent ablationFluid perfusion protects collateral anatomyBipolar electrograms monitor lesion creationControlled energy delivery prevents overheatingDirect visibility (endoscopic)Closed chest epicardial access (SUBTLE®)Posterior electrosilencing
Midline Incision “SUBTLE” Access


• Substrates Located Along
PVs and Posterior LA
• Posterior LA Derives
Embryologically from PVs
• PVI Does Not Address
Reentrant Circuits Outside
the PVs
• Need to Ablate Posterior LA
to Target Regions of
Fibrosis
SUBTLE Access Enables
Visualization & Ablation of
Posterior LA



Catheter Ablation Procedure

Percutaneous Access
Breakthrough Locations @ Pericardial Reflections

Ablating Posterior Left AtriumNo Dissecting of Reflections
Ablating RIPV @ Reflections Ablating Reflections to Complete Isolation of PVs

Pre-Epicardial AblationPost-Epicardial Ablation
Post-Endocardial Ablation

Published Convergent Articles / Presentations1. Civello KC, et al. Combined endocardial and epicardial
ablation for symptomatic atrial fibrillation: Single center experience in 100 consecutive patients. J Innov Card Rhythm Manag. 2013;1-7.
2. Gilligan DM, et al. Multidisciplinary collaboration for the treatment of atrial fibrillation: Convergent procedure outcomes from a single center. J Innov Card Rhythm Manag. 2013;4:1396-1403.
3. Geršak B, et al. European experience of the convergent atrial fibrillation procedure: Multicenter outcomes in consecutive patients. J Thorac Cardiovasc Surg. 2014 Apr;147(4):1411-6..
4. Robinson MC, et al. Maximizing ablation, limiting invasiveness, and being realistic about atrial fibrillation: the convergent hybrid. EP Lab Digest. 2012;13(6):34–6.
5. Gersak B, et al. Low Rate of Atrial Fibrillation Recurrence Verified by Implantable Loop Recorder Monitoring Following a Convergent Epicardial and Endocardial Ablation of Atrial Fibrillation. J Cardiovasc Electrophysiol. 2012 Oct;23(10):1059-66.
6. Olson J, et al. Multicenter Retrospective Outcomes for the Treatment of Atrial Fibrillation Using the Multidisciplinary Convergent Procedure. Boston AF Symposium. January 2012.
7. Golden K, et al. Clinical Outcomes of a new Epicardial/Endocardial ablation procedure (Convergent) for the Treatment of Atrial Fibrillation. HRS Scientific Sessions. May 2012.
8. Zembala M, et al. Minimally invasive hybrid ablation of atrial fibrillation. AATS Scientific Sessions. 2014.

Hybrid Ablations
HUIJIAN J. WANG, M.D., FACC, FHRS
WILLIAM H. JOHNSON, III, M.D., FACS
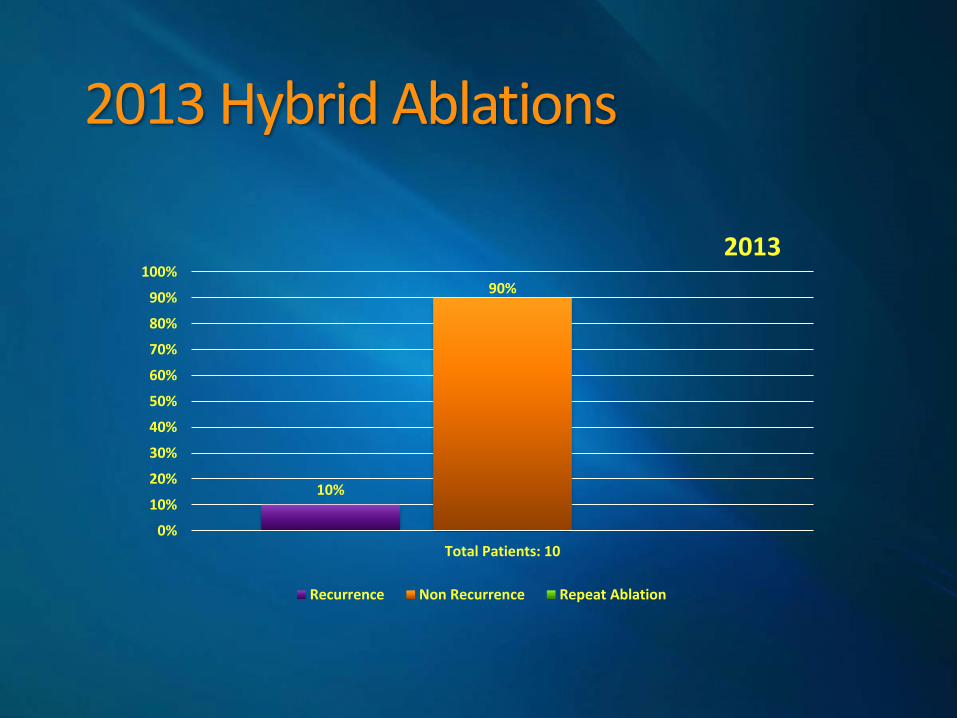
2013 Hybrid Ablations
10%
90%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Total Patients: 10
2013
Recurrence Non Recurrence Repeat Ablation
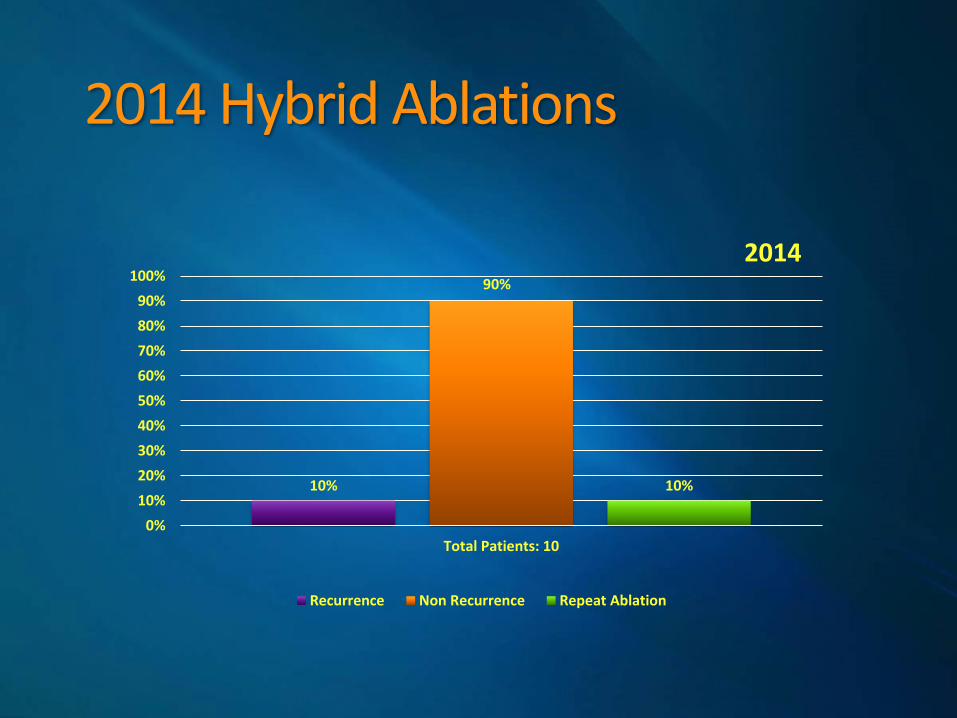
2014 Hybrid Ablations
10%
90%
10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Total Patients: 10
2014
Recurrence Non Recurrence Repeat Ablation

2015 Hybrid Ablations
33.33%
66.66%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Total Patients: 6
2015
Recurrence Non Recurrence Repeat Ablation

2016 Hybrid Ablations
25%
75%
0%
10%
20%
30%
40%
50%
60%
70%
80%
Total Patients: 4
2016
Recurrence Non Recurrence Repeat Ablation

10
10
6
4
1
1
2
1
9
9
4
3
0
1
0
0
0 2 4 6 8 10 12
2013
2014
2015
2016
2013 2014 2015 2016
Had repeat ablation 0 1 0 0
No Recurrence of AtrialFibrillation
9 9 4 3
Had Recurrence ofAtrial Fibrillation
1 1 2 1
Total Patients 10 10 6 4
Hybrid Ablations 2013-2016
16%
81%
3%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Overall Total Patients: 30
2013-2016 Hybrid Ablations Overall Percentage
Recurrence Non Recurrence Repeat Ablation
16%
81%
3%
2013-2016Hybrid Ablations
Recurrence Non Recurrence Repeat Ablation

Ablations, PostopEvaluations & Outcomes
Huijian J. Wang, MD, FACC, FHRS

2013
1st Ablation
63 Y/O W/M 4/12/2013
10/21/2013- 6 months post ablation - Event Recorder showed 3 days with A-Fib 5/05/2014- 1 year post ablation- O.V EKG NSR 52bpm QTC 422msc on Tikosyn. 4/27/2015- 2 years post ablation- Event monitor showed NSR. 4/11/2016- 3 years post ablation- O.V EKG NSR 55bpm QTC stable 463msc on Tikosyn . No recurrence of A-Fib
No Recurrence
72 Y/O W/M 4/19/2013
10/21/2013- OV EKG SR 1st degree AV block HR 80bpm QRS 461ms on Tikosyn 2/17/2014- 10 months post ablation- O.V EKG NSR 76bpm off Tikosyn 9/08/2014- 1 yr 5 mos post ablation- OV EKG NSR 73bpm off Tikosyn 4/06/2015- 2 years post ablation- OV no further episodes of A-Fib, off Tikosyn 12/14/2015- 2 yrs 8 mos post ablation- Still in sinus, No recurrence of A-Fib, off Tikosyn
No Recurrence
68 Y/O W/M 6/4/2013
12/27/2012- A-Fib Ablation 6/04/2013- Hybrid ablation 6/13/2013- OV EKG showed ectopic atrial tachycardia with HR of 158bpm. PT was admitted to hosp for possible cardioversion. 6/14/2013- Successful TEE/ Cardioversion. Put on Tikosyn and Cardizem 9/30/2013- OV EKG showed A-Fib with occasional PVC's HR 94bpm QTC 367. On Tikosyn and Cardizem 10/14/2013- Successful TEE/ Cardioversion, On Tikosyn and Cardizem 12/02/2013- OV EKG showed sinus rhythm with 1st degree heart block HR 81 QTC 452ms. On Tikosyn and Cardizem 4/28/2014- 10 months post hybrid OV EKG showed coarse A-Fib/atrial flutter with HR of 87bpm. Difficult A-Fib case, discussed possible third ablation. PT has not been seen since 4/2014 Recurrence
76 Y/O W/M 6/7/2013
11/11/2013- 5 months post ablation OV EKG showed RBBB HR 62 and QTC 439ms on Tikosyn. D/C Tikosyn at this OV and PT moved to GA. No recurrence of A-Fib
No Recurrence

79 Y/O W/M 7/17/2013
7/30/2013- 13 days post ablation- OV EKG showed A-Fib 8/06/2013- TEE Cardioversion/ On Amiodarone 9/9/2013- OV EKG ventricular paced rhythm 75 bpm. Pacer check showed underlying rhythm of atrial flutter with a rate of 200. On Amiodarone 10/29/2013- OV EKG showed AV paced rhythm HR 60. On Amiodarone 1/24/2014- OV EKG showed AV paced rhythm HR 60, On Amiodarone 5/1/2014- 6 months post ablation -OV EKG showed atrial paced rhythm HR of 60. No recurrence of A-Fib D/C Amiodarone 8/7/2014- 1 year post ablation -PT in NSR, No recurrence of A-Fib 10/06/2014- TEE/ Cardioversion to NSR back on Amiodarone 1/20/2015- OV EKG showed sinus with HR of 61bpm, On Amiodarone 9/1/2015- 2 years post ablation -OV EKG showed SR 60bpm, On Amiodarone 4/26/2016- 2yrs 9mos post ablation- OV EKG showed sinus with RV pacing. Pacer check showed AF<1% & rate response increased. On Amiodarone.
No Recurrence
71 Y/O W/M 7/17/2013
8/8/2013- OV EKG showed AFIB HR of 103bpm, On Tikosyn 2/03/2014- 7 months post ablation OV EKG showed sinus rhythm with RBBB HR of 72m and QTc 488msc. Off Tikosyn- PT to RTC prn No recurrence of A-Fib
No Recurrence
73 Y/O W/M 8/23/2013
11/11/2013- 3 mos post ablation -OV EKG showed sinus with RBBB and QTC 506msc, stable on Tikosyn 2/14/2014- 6 mos post ablation -OV EKG showed sinus with RBBB and QTC 485 msc. Stable. D/C Tikosyn. No recurrence of A-Fib.
No Recurrence
78 Y/O W/F 8/28/2013
9/12/2013- OV EKG showed A-Fib ,HR of 115 bpm, On Amiodarone 2/06/2014- 6 mos post ablation -OV EKG showed sinus with APCs 3/20/2014- 7 mos post ablation -OV EKG showed sinus with HR of 55bpm. D/C Amiodarone. RTC prn No recurrence of A-Fib
No Recurrence
61 Y/O W/M 10/30/20132/10/2014- 4 mos post ablation -OV EKG showed sinus bradycardia with HR 59 QTC 460ms. No recurrence of A-Fib, D/C Tikosyn
No Recurrence
67 Y/O W/M 12/13/2013
4/1/2014- 4 mos post ablation -OV EKG showed sinus rhythm with 1st degree HB HR 71, stable QTC 491ms. D/C Tikosyn 11/19/2014- 11 mos post ablation Event monitor showed NSR HR 81, Off Tikosyn 1/28/2015-1 yr post ablation – OV EKG showed Sinus Rhythm HR 86. No recurrence of A-Fib. Off Tikosyn
No Recurrence

2014
86 Y/O W/M 1/22/2014
1/22/2014- PT became hypotensive with elevation of creatinine post ablation. Cardioversion was preformed but PT had intermittent bradycardia and became hypotensive. When discussed with family they issued a DNR. (Expired 1/25/2014) Deceased
49 Y/O H/M 2/5/2014
12/04/2014- 10 mos post ablation -OV EKG showed sinus rhythm with stable QTC 421 ms and HR of 68bpm. D/C Tikosyn 12/3/2015- 1 yr 10mos post ablation OV EKG showed NSR HR 66bpm, Stable QTC 413ms. Off Tikosyn, No recurrence of A-Fib
No Recurrence
47 Y/O W/M 2/26/2014
3/13/2014- 1 mos post ablation, OV EKG showed sinus rhythm, QTC 472 msec, HR 90. On Tikosyn Pt has not been seen since post proc F/U
No Recurrence
70 Y/O W/M 4/28/2014
5/19/2014- OV EKG showed A-Fib with HR of 86 along with short pauses and LBBB. On Tikosyn 7/29/2014- 3 mos post ablation -OV EKG showed sinus rhythm with LBBB and 1st degree A-V block, stable QTC, On Tikosyn 10/27/2014- 6mos post ablation -OV EKG showed NSR 1st degree AV block and LBBB, QTC stable, D/C Tikosyn 3/26/2015- 11 mos post ablation -OV EKG showed NSR, 1st degree AV block, LBBB, QTC stable, Off Tikosyn 12/17/2015- 1 yr 8 mos post ablation No recurrence of A-Fib
No Recurrence
60 Y/O W/M 5/16/2014
6/23/2014- 1 month post ablation -S/P pacemaker implant, On Tikosyn No recurrence of A-Fib 9/23/2014- 4 mos post ablation -OV EKG showed sinus with HR of 61bpm. D/C Tikosyn 4/30/2015- 11mos post ablation -OV EKG showed SR, HR 65bpm 1st degree AVB. QTc 424 ms. Off Tikosyn 8/11/2015- 1 yr 3 mos post ablation - OV EKG showed SR, Off Tikosyn 2/25/2016- 1yr 9 mos post ablation -OV EKG showed SR HR 67bpm No recurrence of A-Fib, off Tikosyn
No Recurrence
78 Y/O W/F 7/18/2014
8/12/2014- 1 mos post ablation -OV EKG showed sinus with QTC 425msc. She did have VT on Tikosyn and Tikosyn was stopped. 10/21/2014- 3 mos post ablation -OV EKG showed sinus 74 with QTC 426msc. Stable, Off Tikosyn, No recurrence of A-Fib
No Recurrence

66 Y/O W/M 8/1/201411/4/2014- 3mos post ablation -OV EKG showed sinus rhythm with stable QTC 418ms. D/C Tikosyn, No Recurrence of A-Fib
No Recurrence
71 Y/O W/M 8/20/2014
10/30/2014- 2mos post ablation- Event Recorder showed SR, No Recurrence of A-Fib, On Tikosyn 1/29/2015- 5mos post ablation -OV EKG showed SR with HR of 66bpm, D/C Tikosyn 5/28/2015- 9mos post ablation -EKG showed SR, Off Tikosyn, No recurrence of A-Fib
No Recurrence
79 Y/O W/M 9/10/2014
11/11/14- 2mos post hybrid ablation - ICD check showed A-Fib, On Amiodarone 11/26/2014- Successful TEE/ Cardioverion, On Amiodarone 12/1/2014- 3mos post hybrid ablation -OV EKG showed atrial paced rhythm, On Amiodarone 12/11/2014- PPM check showed AFIB, On Amiodarone 1/07/2015- 2nd Cardiac ablation performed 1/19/2015- OV EKG showed Atrial tachycardia with ventricular rate 109. On Amiodarone 2/27/2015- 1 mos post 2nd ablation -OV EKG showed SR with HR 60bpm, On Amiodarone 4/09/2015- 3 mos post 2nd ablation -OV EKG showed A-Fib HR 103 bpm. D/C Amiodarone 5/06/2015- PPM check showed AFL, Back on Amiodarone 10/13/2015- 10mos post 2nd ablation -OV EKG showed AFIB with HR of 97 and PVCs. PT D/C Amiodarone on his own due to cough and wheezing 1/05/2016- 1 year post 2nd ablation -PT still has HR of 106bpm, Now on Cardizem 3/09/2016- 3rd cardiac ablation performed 3/29/2016- 20 days post 3rd ablation -PPM check showed sinus, no A-Fib or AFL. No anti-arrhythmia medications at this time 3 Ablations
55 Y/O W/M 11/14/2014
5/28/2015- 6 mos post ablation- OV to review 5/18/2015 Holter that showed SR/ST with no issues APCs or PVCs, no pauses. 11/20/2015- 1 year post ablation- OV EKG showed SR with HR 71bpm, Off anti-arrhythmics and D/C anticoagulants, No recurrence of A-Fib
No Recurrence
72 Y/O W/M 12/5/2014
5/21/2015- 5mos post ablation- OV to review 4/22/2015 Event recorder that showed SR with average HR 65 bpm, no pauses or atrial/ventricular arrhythmias. D/C Flecanide 9/3/2015- 9 mos post ablation- No recurrence of AFIB. D/C anticoagulants
No Recurrence

2015
67 Y/O W/M 2/4/2015
3/05/2015- 1mos post ablation- OV for F/U and to review EKG in primary cardiologists office that showed ectopic atrial tachycardia/AFL. Was considering cardioversion. PT has not been seen since 03/2015 Recurrence
76 Y/O W/M 3/9/2015
3/18/2015- OV EKG showed SR 64 bpm, QTC 522ms, PT wasn’t tolerating Tikosyn well so D/C 04/23/2015- 1 mos post ablation- OV EKG showed sinus with RBBB. PT now on Amiodarone 10/20/2015- 7 mos post ablation- PT still in SR, D/C Amiodarone, No recurrence of A-Fib
No Recurrence
68 Y/O W/M 3/13/2015
3/30/2015- OV EKG showed SR 61 bpm. On Tikosyn. 6/11/2015- 3 mos s/p ablation- Event monitor showed sinus rhythm bradycardia, 1st degree AV block, PACs, Couplets, Runs and IVCD. No A-Fib7/02/2015- 4 mos post ablation- OV EKG showed sinus with HR of 53bpm and QTc 428msc. D/C Tikosyn 4/05/2016- 1 year post ablation- OV EKG showed A-Fib/ atypical atrial flutter with CL of 240msc. PT refused Tikosyn- consider second ablation 5/4/2016- Second Ablation preformed 5/19/2016- TEE on 5/4/16 showed EF 25%, PT in a Life Vest, S/P second ablation OV EKG showed sinus with HR of 61bpm and QTc 455msc on Tikosyn, F/U in 1 mo
Recurrence/ Repeat Ablation
63 Y/O W/M 5/15/2015
5/27/2015- 12 days post ablation- OV EKG showed AT with VR 100 bpm. On Tikosyn 6/11/2015- Successful TEE/Cardioversion 6/18/2015- OV EKG showed SR 85 bpm, QTC 435ms, On Tikosyn 12/1/2015- 7 mos post ablation- OV EKG showed SR with VR 86bpm, QTC 474ms, On Tikosyn--PT has not been seen since 12/2015
No Recurrence
62 Y/O W/M 6/17/2015
7/01/2015- OV EKG showed SR 61 bpm, On Amiodarone 9/3/2015- 3mos post ablation- OV EKG showed SR/SB 58bpm, D/C Amiodarone 12/28/2015- 6 mos post ablation- OV EKG showed SR 78bpm, off Amiodarone, considering stopping anticoagulant if PT stays in SR 4/21/2016- 10mos post ablation- OV EKG showed sinus with HR of 81bpm, D/C anticoagulant, No recurrence of A-Fib
No Recurrence

86 Y/O W/F 11/20/2015
3/7/2015- 4 mos post ablation- Event monitor showed AFIB, On Amiodarone 04/15/2016- 5 mos post ablation- OV EKG showed sinus with HR of 67bpm, On Amiodarone Recurrence
68 Y/O W/M 12/11/2015
2/15/2016- 2 mos post ablation- Event monitor showed NSR average HR of 77 bpm, No recurrence of AFIB, On Tikosyn 3/10/2016- 3 mos post ablation- OV EKG showed sinus with HR of 73bpm and QTC 445msc. On Tikosyn, No recurrence of AFIB
No Recurrence
2016
82 Y/O W/M 1/13/2016
2/11/2016- 1 mos post ablation- OV EKG showed sinus with HR of 72bpm, On Tikosyn 5/26/2016- 4 mos post ablation- OV EKG showed SR with borderline QTC 468msc, RBBB. D/C Tikosyn, No recurrence of AFIB
No Recurrence
68 Y/O W/M 1/20/2016
2/1/2016- 11 days post ablation- OV EKG showed AFIB HR 80bpm, QTC 425msc, On Amiodarone 2/15/2016- 25 days post ablation- OV EKG showed SR HR of 87bpm and QTC 425msc. On Amiodarone 2/25/2016- 1 month post ablation- OV EKG showed sinus with HR of 88bpm, PVC. On Amiodarone 3/22/2016- 2 mos post ablation- OV EKG showed sinus with HR of 83bpm. On Amiodarone, No recurrence of AFIB
No Recurrence
61 Y/O W/M 1/27/2016
2/11/2016- 15 days post ablation- OV EKG showed sinus with HR of 74bpm, QTc 473msc. . On Tikosyn 5/17/2016- 4 mos post ablation- OV EKG showed sinus with HR of 76bpm, D/C Tikosyn, No recurrence of AFIB
No Recurrence
80 Y/O W/M 4/14/2016
4/28/2016- 14 days post ablation- OV EKG showed atypical atrial flutter Clof360 and QTc 483msc, Stable on Tikosyn 5/2/2016- Successful TEE/ Cardioversion, On Tikosyn 5/23/2016- 1 month post ablation- OV EKG showed sinus HR of 71bpm QTC 448msc, Stable. On Tikosyn
No Recurrence

Thank You


















