Surgery GI bleeding
82
GASTROINTESTINAL BLEEDING NUR JASHIMAH IDAYU JAMALUDIN TAN LAY TENG MOHD HANAFI RAMLEE 1/81
description
Transcript of Surgery GI bleeding

GASTROINTESTINAL
BLEEDING
NUR JASHIMAH IDAYU JAMALUDINTAN LAY TENG
MOHD HANAFI RAMLEE
1/81

CONTENTS
• Anatomy• Definition• Epidemiology• Clinical features• Aetiology• History & Examination• Investigation• Management
2/81

• FOREGUTAbdominal esophagus
• MIDGUT Major duodenal papilla • HINDGUT Junction B/w prox 2/3 and distal 1/3 of tranverse colon
Major duodenal papilla
Junction B/w prox. 2/3 and distal 1/3
of tranverse colon.
Midway of anal canal
ANATOMY OF GIT
3/81

ARTERIAL SUPPLY
• Mostly by anterior branch of abdominal aorta
Celiac trunk - Foregut
• left gastic artery
• splenic artery
• common hepatic artery
Superior Mesenteric
Artery - Midgut• inferior
pancreaticoduodenal artery
• jejunal and ileal arteries
• middle colic artery
• right colic artery
• ileocolic artery
Inferior Mesenteric
Artery - Hindgut
• sigmoid arteries
• superior rectal artery
• Left colic artery
4/81

PORTAL VEIN
Union of splenic vein and sup. Mesentric
vein• Tributaries ; -right and left
gastric veins -cystic veins -para umbilical veins• Portal vein drains to
inferior vena cava (systemic system) through hepatic vein
5/81

PORTAL-SYSTEMIC ANASTOMOSES• Lower 3rd of esophagus
Left gastric veinAzygos vein
• Anal canalSuperior rectal veinInferior rectal vein
• Umbilicus Paraumbilical veinSuperficial vein of
anterior abdominal wall• Bare area of liver
Vein in liverDiaphragmatic/
phrenic vein• Retroperitoneal organs
Colic veinLumbar/renal vein
6/81

INTRODUCTION
• Gastrointestinal bleeding describe every form of haemorrhage in the GIT, from the pharynx to the rectum.
• Can be divided into 2 clinical syndromes:-- upper GI bleed (pharynx to ligament of Treitz)- lower GI bleed (ligament of Treitz to rectum)
LIGAMENT OF TREITZ
7/81

UPPER GASTROINTESTINAL BLEEDING
8/81

EPIDEMIOLOGY
• Upper GI bleed remains a major medical problem.
• About 75% of patient presenting to the emergency room with GI bleeding have an upper source.
• In-hospital mortality of 5% can be expected.
• The most common cause are peptic ulcer, erosions, Mallory-Weiss tear & esophageal varices.
9/81

CLINICAL FEATURES
• Haematemesis : vomiting of blood whether fresh and red or digested and black.
• Melaena : passage of loose, black tarry stools with a characteristic foul smell.
• Coffee ground vomiting : blood clot in the vomitus.
• Hematochezia : passage of bright red blood per rectum (if the haemorrhage is severe).
10/81

CLINICAL FEATURES
• Haematemesis without malaena is generally due to lesions proximal to the ligament of Treitz, since blood entering the GIT below the duodenum rarely enters the stomach.
• Malaena without haematemesis is usually due to lesions distal to the pylorus
• Approximately 60mL of blood is required to produced a single black stool.
11/81
AETIOLOGY
Oesophagus-Oesophageal varices-Oesophageal CA-Reflux oesophagitis-Mallory-Weiss syndrome
-Haemophilia-Leukemia-Thrombocytopenia-Anti-coagulant therapy
Stomach-Gastric ulcer-Erosive gastritis-Gastric CA-gastric lymphoma-gastric leiomyoma-Dielafoy’s syndrome
Duodenum-Duodenal ulcer-Duodenitis-Periampullary tumour-Aorto-duodenal fistula
LOCAL
GENERAL
12/81

13/81

OESOPHAGEAL VARICES• Abnormal dilatation of
subepithelial and submucosal veins due to increased venous pressure from portal hypertension (collateral exist between portal system and azygous vein via lower oesophageal venous plexus).
• Most commonly : lower esophagus.14/81

Esophageal varices: a view of the everted
esophagus and gastroesophageal junction, showing
dilated submucosal veins (varices).
15/81

OESOPHAGEAL VARICES: PORTAL HYPERTENSION
PRE HEPATIC• Portal
vein thrombosis
• Splenic vein thrombosis
INTRA HEPATIC
• Cirrhosis• Schistos
omiasis• Sarcoido
sis• Myelopro
liferative disorder
• Congenital hepatic fibrosis
POST HEPATIC
• Budd-chiari syndrome
• Right heart failure
• Constrictive pericarditis
• Veno-occlusive disease
16/81

OESOPHAGEAL VARICES: PATHOPHYSIOLOGY
Portal venous hypertension
Resistance to flow in portal venous system
Pressure
Portal systemic shunting(Abnormal venous communication between portal system
and systemic venous circulation)
Appearing of large submucosal veins at lower end of oesophagus and gastric fundus
Haemorrhage due to intravariceal pressure17/81

OESOPHAGEAL VARICES• Sudden onset• Painless• Large volume of blood• Dark red• History of (alcoholic) liver
disease• Physical findings of portal
hypertension – ascites, splenomegaly
18/81
OESOPHAGEAL VARICES• Management
- blood transfusion- endoscopic variceal injection with sclerosant or banding.- sengstaken tube
19/81

MALLORY-WEISS TEAR• Longitudinal tears at the
oesophagogastric junction.• may occur after any event that provokes
a sudden rise in intragastric pressure or gastric prolapse into the esophagus.
Clinical features:- An episode of haematemesis
following retching or vomiting.- melaena- hematochezia- syncope- abdominal pain.
Precipitating factors:- hiatus hernia- retching & vomiting- straining- hiccuping- coughing- blunt abdominal trauma - cardiopulmonary resuscitation 20/81
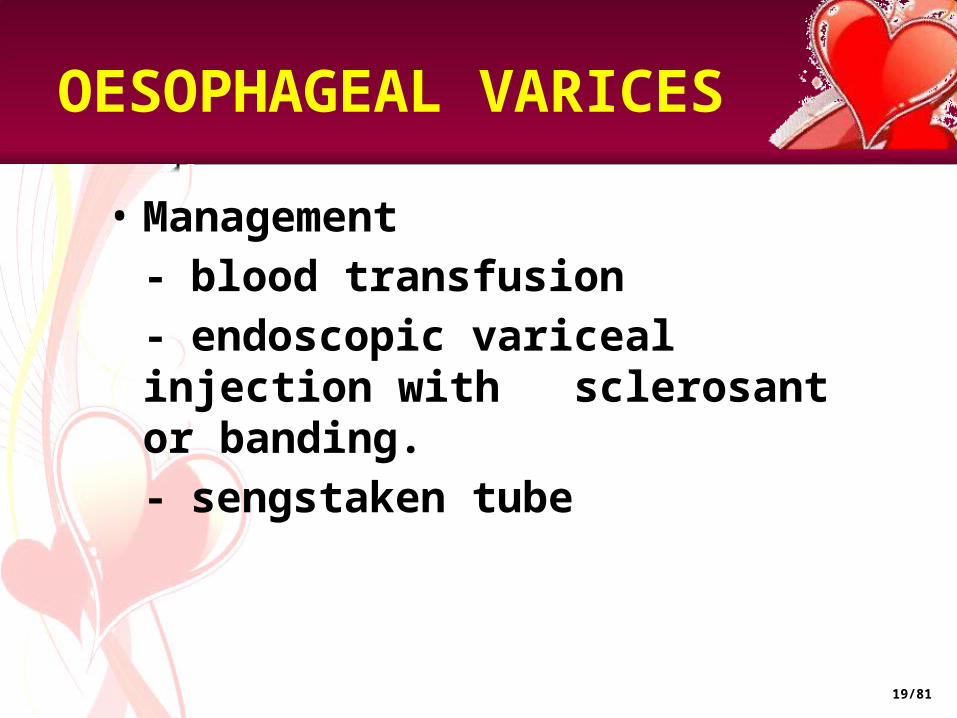
MALLORY-WEISS TEAR: MANAGEMENT
- Bleeding from MWTs stops spontaneously in 80-90% of patients - A contact thermal modality, such as multipolar electrocoagulation (MPEC) or heater probe, with or without epinephrine injection, is typically used to treat an actively bleeding - Epinephrine injection -reduces or stops bleeding via a mechanism of vasoconstriction and tamponade - Endoscopic band ligation - Endoscopic hemoclipping
21/81

ESOPHAGEAL CANCER• 8th most common cancer seen
throughout the world.• 40% occur in the middle 3rd of
the oesophagus and are squamous carcinomas.
• adenoCA (45%) occur in the lower 3rd of the oesophagus and at the cardia.
• Tumours of the upper 3rd are rare (15%) 22/81

ESOPHAGEAL CANCER
-more common in men.-risk factor:
- tobacco smoking- heavy alcohol intake- plummer-vinson syndrome- achalasia- coeliac disease- tylosis- diet deficient in vitamins
high dietary carotenoids & vitamin C possibly decrease the risk.
- arise in the columnar lined epithelium of the lower
oesophagus.- risk factor:
- long-standing GORD- barrett’s
oesophagus- tobacco smoking
ADENOCARCINOMASQUAMUS CELL CARCINOMA
23/81

ESOPHAGEAL CANCER: CLINICAL FEATURES
1) Dysphagia- progressive & unrelenting- initially there is difficulty in swallowing solids, but eventually dysphagia for liquids also occur.
2) Odynophagia- retrosternal pain on swallowing.
3) Regurgitation4) Aspiration pneumonitis5) Weight loss6) Anorexia7) Anemia8) Lassitude
24/81

ESOPHAGEAL CANCER: TNM STAGING
1. Tumour confined to submucosa2. Tumour extends into muscularis propria3. Tumours extend outside muscle layer4. Tumour invades adjacent structures
5. Lymph node metastases to paraoesophageal, cardia or left gastric regions.
o. No other metastatic spread1. Lymph node metastases to all other areas.
Metastases to liver, lung, brain, bone, etc.
T
N
M
25/81

PEPTIC ULCER• gastric ulcer & duodenal
ulcer• Caused by imbalance
between secretion of acid and pepsin, and mucosal defence mechanism.
-Helicobacter pylori infection-Zollinger-ellison syndrome-NSAIDs-others: stress, smoking,alcohol, steroid
- epigastric pain- haematemesis- Melaena- heartburn
AETIOLOGY
SIGNS & SYMPTOMS
26/81

PEPTIC ULCER: PATHOGENESIS
Predisposing factors including H.pylori infection of mucosa
Acid-pepsin attack and/or breach of mucosal protection
Acute inflammation resolution
Destruction of mucosa
Mucosal ulceration mucosal regeneration
Extension through submucosal & muscular layers causing deep ulceration
Perforation erosion of major granulation tissue blood vessel formed & attemps repair
Peritonitis massive haemorrhage chronic & relapsing
ulceration27/81

Feature Gastric ulcer Duodenal ulcer
Onset Soon after eating 2-3 hours after eating
Relieving factor vomiting Eating
Precipitating factor
eating Missing a meal, anxiety, stress
Duration of attack
A few weeks A month or two
PEPTIC ULCER
28/81

PEPTIC ULCER: COMPLICATION
• Haemorrhage- posterior duodenal ulcer erode the gastroduodenal artery- lesser curve gastric ulcers erode the left gastric artery
• Perforation- generalized peritonitis- signs of peritonitis
• Pyloric obstruction- profuse vomiting, LOW, dehydrated, weakness, constipation
29/81

PEPTIC ULCER: TREATMENT
• Antacid – aluminium/Mg hydroxide, Mg Trisiclate• Mucosal protective agents – sucralfate• Prostaglandin analogues – misoprostol• H2 receptor antagonist – cimetidine & ranitidine• Proton pump inhibitor – omeprazole & lansoprazole
• H.pylori eradication- triple
therapy :metronidazole,amoxycilin,erythromycin
• surgery should be done if -failed medical treatment-vagotomy, gastrectomy, pyloroplasty 30/81

EROSIVE GASTRITIS
• Acute mucosal inflammatory process
• Accompanied by hemorrhage into the mucosa and sloughing of the superficial epithelium (erosion).
31/81

EROSIVE GASTRITIS: AETIOLOGY
- NSAIDs- alcohol- smoking- chemotherapy- uraemia- stress - ischaemia and shock- suicide attempts - mechanical trauma- distal gastrectomy
32/81

EROSIVE GASTRITIS: CLINICAL FEATURES
- asymptomatic- epigastric pain with nausea & vomiting- haematemesis and melaena- fatal blood loss
It is one of the major causes of haemetemesis, particularly in alcoholic!
33/81

GASTRIC CANCER
- adenomatous polyps- leiomyoma- neurogenic tumour- fibromata- lipoma
- gastric adenocarcinoma (90%)- lymphomas- smooth muscle tumour
BENIGN GASTRIC NEOPLASM
GASTRIC CARCINOMA
34/81

GASTRIC CANCER
• 60-80 years age group.• Male:female , 2:1
- diet- H.pylori infection- gastric polyps- gastroenterostomy- chronic gastric ulcer disease- chronic atrophic gastritis- intestinal metaplasia- gastric dysplasia- host factors
AETIOLOGICAL FACTOR
35/81

GASTRIC CANCER: TNM STAGING
T1 tumour extends to lamina propria or submucosa.
T2 tumour extend into muscleT3 tumour extend into serosaT4 tumour invades adjacent structures
N0 no lymph node involvementN1 fewer than 7 lymph node involved by tumourN2 7-15 lymph node involved by tumourN3 more than 15 lymph node involved by tumour
M0 no metastasesM1 metastases present
T
N
M
36/81

GASTRIC CANCER
Early signs -Indigestion -Flatulence -DyspepsiaLate signs - LOW -anemia -dysphagia -vomiting -epigastric/back pain - epigastric mass -sign of metastases (jaundice, ascites, diarrhoea, intestinal obstruction)
• Radical total gastrectomy• Palliative resection• Palliative bypass
CLINICAL FEATURESTREATMENT
37/81

DIEULAFOY’S DISEASE
• Rare – erosion of mucosa overlying artery in stomach causes necrosis arterial wall & resultant hemorrhage.
• Gastric arterial venous abnormality
• covered by normal mucosa
• profuse bleeding coming from an area of apparently normal mucosa.
38/81

DUODENITIS
- aspirin, - NSAIDs- high acid secretion
- Symptoms are similar to peptic ulcer disease
- stomach pain- bleeding from the intestine- nausea & vomiting- LOA- intestinal obstruction(rare)
AETIOLOGY
CLINICAL FEATURE
39/81

DUODENITIS
- endoscopy, may
be some redness and nodules in the wall of the small intestine.
- Sometimes, it can be more severe and there may be shallow, eroded areas in the wall of the intestine, along with some bleeding
-stop all medications that can make things worse (aspirin & NSAIDS)
-H2 receptor blockers (ranitidine/cimetidine) or proton pump inhibitors (omeprazole) reduce the acid secretion by the stomach
INVESTIGATION MANAGEMENT
40/81

HISTORY TAKING
- when?- have u vomited blood/passed black tarry stools?- had both haematemesis & malaena?- have u had, bleeding from the nose? Bloody expectoration? A dental extraction?
- what is the color, the appearance of the vomited blood?- red? Dark red? Brown? Black?- ‘coffee ground appearance?- bright red & frothy?- what is the color of the stool? Bright red? Black tarry?
- have u vomited blood only once/several times?- has the bleeding been abrupt/massive?- have u had >1 black, tarry stool within a 24-h period?- for how long have the tarry stools persisted?
MODE OF ONSET
CHARACTER
EXTENT AND RATE
41/81
- retching & severe nonbloody vomiting?- lightheadedness? Nausea? Thirst? Sweating?- faintness when lying down/when standing/syncope?- following the haemorrhage did you have diarrhea?
- aspirin? anticoagulant therapy? iron preparation?- age of the patient?- what is your smoke/alcohol intake?
- have there been similar episode in the past? When? Diagnosis?- were u hospitalized on this occasion? Did u receive a transfusion?- are there any other members of your family who have intestinal disease/bleeding tendency/peptic ulcer/liver disease, History of Malignancy?
OTHER SYMPTOMS
IATROGENIC FACTORS
PREVIOUS EPISODES
FAMILY HISTORY
HISTORY TAKING
42/81

PHYSICAL EXAMINATION:UPPER GI BLEED
Anaemic Bruishing/ Purpura Cachexic Dehydrated Jaundice
Inspection - distension, scar, prominent vein.
Palpation - tenderness, mass/ organomegaly
Percussion - shifting dullness, fluid thrill.
Auscultation - hyperactive bowel sound.
Perianal Skin Lesion Masses Melaena
Supraclavicular LN Cervical LN Axillary LN Inguinal LN
Confusion ( Shock, liver failure….)
Neurological Deficit
GENERAL INSPECTION
ABDOMEN
RECTAL
LYMPH NODES
CNS
43/81

PHYSICAL SIGN
• Clinical shock• Systolic BP < 100mmHg• Pulse rate > 100 bpm• Postural sign: patient place in a
upright position – pulse rate rises 25% or
more- systolic BP alls 20mmHg
or more• Sign of liver disease & portal
hypertension• Sign of GI disease• Sign of bleeding abnormalities• Bloody / black stools on per rectal
examination. 44/81

INVESTIGATIONS
- full blood count – Hb, WCC- liver function test – cirrhosis- coagulation profile- renal profile- RBC morphology- OGDS
- Barium meal / Double-contrast barium meal
- Ultrasound- CT scan
BASELINE INVESTIGATION
IMAGING
45/81

Acute Upper Gastrointestinal Bleed
Resuscitation and Risk Assessment
Routine Blood Test
Endoscopy (within 24 hrs)
Varices Peptic Ulcer No obvious cause
Management Varices
Major SRH Minor SRH Minor Bleed
Major Bleed
Eradicate H.pylori &
Risk Reduction
Endoscopic Treatment
Failure
Surgical
Other colonoscopy or
angiography
OVERVIEW:MANAGEMENT OF UPPER GI BLEED
46/81

RESUSCITATION
• airway and oxygen• Insert 2 large-bore (14-16G) IV cannulate take
blood• IV colloid - crossmatched. • In a dire emergency, give O Rh-ve blood.• haemodynamically stable.• Correct clotting abnormalities• Monitor• Insert urinary catheter and monitor hourly
urine output if shocked.• Consider a CVP line to monitor CVP and guide
fluid replacement.• Organize a CXR, ECG, and check arterial blood
gases in high-risk patient.• Arrange an urgent endoscopy.• Notify surgeon of all severe bleeds on admision.47/81

BLOOD TRANFUSION
– Haemoglobin - May be normal during the acute stages until haemodilution occurs
– Urea and electrolytes - Elevated blood urea suggests severe bleeding
– Cross match for transfusion - Two units of blood are sufficient unless bleeding is extreme.
– If the transfusion is not needed urgently, group the blood and save the serum
– LFT and coagulation profile
1.Systolic BP < 110 mmHg
2.Postural hypotension
3.Pulse > 110/min
4.Haemoglobin <8g/dl
5.Angina or cardiovascular disease with a Haemoglobin <10g/dl
BLOOD TEST INDICATION OF BLOOD TRANSFUSION
48/81

DETECTION & ENDOSCOPIC• Used to detect the site of
bleeding.• May also be used in a therapeutic
capacity (active bleeding from the ulcer, the presence of a visible vessel, adherent clot overlying the ulcer)
• Injection sclerotherapy is used commonly. Other method include the use of heat probes and lasers.
• Angiography in whom endoscopy does not identify the bleeding point. Limitation: can only detect active bleeding of greater than 1mL/min. 49/81

FORREST CLASSIFICATION FOR BLEEDING PEPTIC ULCER
– Ia: Spurting Bleeding– Ib: Non spurting active bleeding– IIa: visible vessel (no active
bleeding)– IIb: Non bleeding ulcer with
overlying clot (no visible vessel)– IIc: Ulcer with hematin covered
base– III: Clean ulcer ground (no clot,
no vessel)
Min
or S
RHM
ajor
SRH
50/81

MANAGEMENT
• H2 receptor antagonist - cimetidine, ranitidine• Proton pump inhibitors – omeprazole, lanzoprazole• H. pylori irradication• Triple regimen – proton pump inhibitor + 2 antibiotics given for 1
week (elimination rate > 90%) e.g. Omeprazol + metronidazole/amoxycillin + clarithromycin
• GU – remove ulcer, gastrin secreting zone – Billroth I gastrectomy• DU – Polya or Billroth II gastrectomy – Vagotomy
MEDICAL
SURGICAL
51/81

UPPER GI BLEED:RISK FACTORS FOR DEATH
1. Advanced AGE2. SHOCK on admission(pulse rate >100 beats/min; systolic
blood pressure < 100mmHg)3. COMORBIDITY (particularly hepatic or renal failure and
disseminated malignancy)4. Diagnosis (worst PROGNOSIS for advanced upper
gastrointestinal malignancy)5. ENDOSCOPIC FINDINGS (active, spurting haemorrhage from
peptic ulcer; non-bleeding visible vessel)6. REBLEEDING (increases mortality 10 fold)
52/81

GASTROINTESTINAL BLEEDING
LOWER
53/81

LOWER GI BLEED: AETIOLOGY
Crohn’s diseaseDiverticula eg:
Meckel’s diverticulum,
Jejujanal diverticulosisBenign neoplasm eg:
Peutz-Jegher’s syndrome
Leiomyoma. Malignant neoplasm eg:
Lymphoma,
Angiodysplasia
Rectal carcinoma and polypsRectal prolapse
Carcinoma of colonPolyps eg:
Familial adenomatous polyposis Diverticular diseaseInflamation
Ischaemic colitisUlcerative colitis
Pseudomembranous colitis Angiodysplasia
HaemorrhoidsFissure-in-anoAnal carcinomaAnal wart
SMALL INTESTINE
RECTUM
COLON
ANUScDNA
PC
PACID
wCHF
54/81

HISTORY TAKING:RECTAL BLEEDING
Blood on its own or streaking the stool:Rectum : polyps or carcinoma, prolapsedAnus : Haemorrhoids, Fissure-in-ano, Anal carcinoma.
Stool mixed with blood:GIT above sigmoid colon. Sigmoid carcinoma or diverticular disease.
Blood separate from the stool:Follows defaecation : Anal condition eg: Haemorrhoids.Blood is passed by itself : Rapidly bleeding carcinoma,
inflammatory bowel disease, diverticulitis, or passed down from high up in the gut.
Blood is on the surface of the stool: suggest a lesion such as polyp or carcinoma further proximally either in the rectum or descending colonBlood on the toilet paper: Fissure-in-ano, Heamorrhoids.Loose, black, tarry, foul smelling stool: from the proximal of DJ flexure
55/81

Bright red/ Fresh blood: Rectum and anus.Dark blood: Upper GIT to above rectum.Drugs eg: iron tablets- appear as greenish black formed stool.
• Discharge apart from blood:--Mucus- irritable bowel syndrome-Copious mucus- villous adenoma, frank cancer of the rectum-Mucus and pus- IBD, diverticular disease
HISTORY TAKING:COLOUR OF BLOOD/DISCHARGE
56/81

Normal bowelIntermittent bouts of constipation interrupted by diarrhoea: Carcinoma or Diverticular disease.Diarrhoea: Inflammatory bowel disease or rectal villous tumour.Tenesmus: Irritable bowel syndrome or abnormal mass of rectum or anal canal (e.g. CA, polyps or thrombosed haemorrhoid)
HISTORY TAKING
ALTER BOWEL HABIT
ANAL PAIN
ITCHINESS
Causes: Allergic, anal warts, anal leak of mucus in haemorrhoid, excessive used of liquid paraffin, generalized disorder. eg: jaundice, diabetes mellitus.
During pregnancy/childbirth: Fissure-in-ano, haemorrhoids.Throbbing, severe pain occur during defaecation: Fissure-in-ano.
57/81
•Previous perianal disease•Inflammatory bowel disease•Peptic ulcer disease•Liver disease•Coagulopathy
HISTORY TAKING
• Laxative agent• Anti-parkinson agent• Anti-coagulant therapy
eg: warfarin• NSAID’s-risk factor of
PUD
• Low fiber diet• Smoking
PREVIOUS HISTORY
•History of malignancy•Familial Adenomatous Polyposis
FAMILY HISTORY
DRUGS HISTORY
SOCIAL HISTORY
58/81

PHYSICAL EXAMINATION:LOWER GI BLEED
Anaemic Bruishing/ Purpura Cachexic Dehydrated Jaundice
Inspection - distension, scar, prominent vein.
Palpation - tenderness, mass/ organomegaly
Percussion - shifting dullness, fluid thrill.
Auscultation - hyperactive bowel sound.
Perianal Skin Lesion Masses Melaena
Supraclavicular LN Cervical LN Axillary LN Inguinal LN
Confusion ( Shock, liver failure….)
Neurological Deficit
GENERAL INSPECTION
ABDOMEN
RECTAL
LYMPH NODES
CNSSAME WITH UPPER GI BLEED
59/81

INVESTIGATION
1. Full Blood Count (FBC)2. BUSE3. Coagulation profile4. Cross-matched (Transfusion)
1. Scintigraphy -Radioactive test using Technetium-99m (99mTc)-
Labelled red cells -diagnose ongoing bleeding at a rate as low as 0.1
mL/min
2. Mesenteric angiography -Can detect bleeding at a rate of more than 0.5 mL/min.
LABORATORY
IMAGING
60/81

IMAGING
3. Helical CT scan• Abdomen and pelvis • Can also be used when routine workup fails to
determine the cause of active GI bleeding • Multiple criteria are used to establish the
bleeding sites: -vascular extravasation of the contrast medium -contrast enhancement of the bowel wall -thickening of the bowel wall -spontaneous hyperdensity of the peribowel fat -vascular dilatations with helical CT.
61/81

IMAGING
4.Colonoscopy• Bleeding slowly or who have already stopped
bleeding.• Biopsy
5.Proctosigmoidoscopy• Exclude an anorectal source of bleeding
6.Oesophagoduodenoscopy (OGDS)• To exclude upper GI bleeding
62/81

IMAGING
7. Double-contrast barium enema
• Elective evaluation of unexplained lower GI bleeding
• Do not use in the acute hemorrhage
phase 8. Small bowel enema• Often valuable in investigation of long-
term, unexplained lower GI bleeding
Example of barium enema study showing ulcerative colitis of the colon
63/81

INTUSSUSCEPTION
• Common in children within 1st year of life
• Symptoms: abdominal pain, red-currant-jelly stool
• Signs: palpable mass at right iliac fossa
• Procedure: Barium enema, laparotomy
64/81
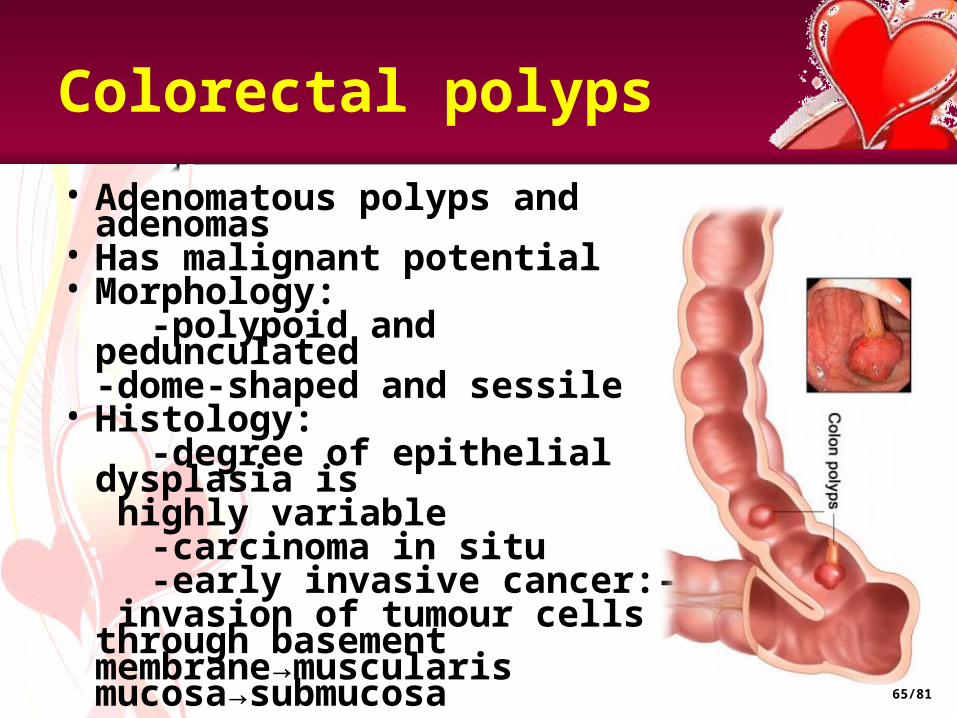
Colorectal polyps
• Adenomatous polyps and adenomas
• Has malignant potential• Morphology: -polypoid and
pedunculated-dome-shaped and sessile
• Histology: -degree of epithelial
dysplasia is highly variable
-carcinoma in situ -early invasive cancer:-
invasion of tumour cells through basement membrane→muscularis mucosa→submucosa
65/81

TYPES OF COLORECTAL POLYPS
1.Tubular adenomas - small pedunculated / sessile lesions
-retain a tubular form similar to normal colonic
mucosa -least potential for malignant transformation
2. Villous adenomas -sessile and frond like lesions -secrete mucus
-more dysplastic -greater potential for malignant change
3. Tubulo-villous adenoma -intermediate between tubular and villous
adenoma -pedunculated, stalk is covered with normal epithelium 66/81

SIGN AND SYMPTOM
• Rectal bleeding• Iron deficiency anaemia• Mucus• Hypokalaemia• Tenesmus• Prolapse• Obstructive symptoms
67/81

FAMILIAL ADENOMATOUS POLYPOSIS
• Autosomal dominant defect in APC gene
• Mid teen years- hundred / more adenomatous polyps
• Average age of 40- colorectal cancer
• Symptoms: -rectal bleeding -diarrhoea • Gardner’s syndrome=
+desmoid tumours + osteomas of mandible & skull
68/81

INVESTIGATION
• Sigmoidoscopy• Colonoscopy -gold standard -visualize, biopsy, remove -disadvantage: full day’s bowel preparation sedation risk of haemorrhage & perforation• CT pneumocolon -elderly / infirm patient -< invasive & not require sedation. -bowel preparation• Double contrast barium enema 69/81
MANAGEMENT
• Subtotal colectomy & ileorectal anastomosis
• Panproctocolectomy & ileotomy / ileal pouch
• Follow-up colonoscopies - an adenomatous polyp is found / a
colorectal cancer has been treated -intervals depend on number, size & pathology of polyps
70/81

ADENOCARCINOMA OF COLON & RECTUM
• Rare < 50 years old, Common > 60 years old
• Common site- sigmoid colon, rectum
• Clinical features: -altered bowel habit &
large bowel obstruction -rectal bleeding -iron deficiency
anaemia -tenesmus -perforation -anorexia & weight loss
71/81
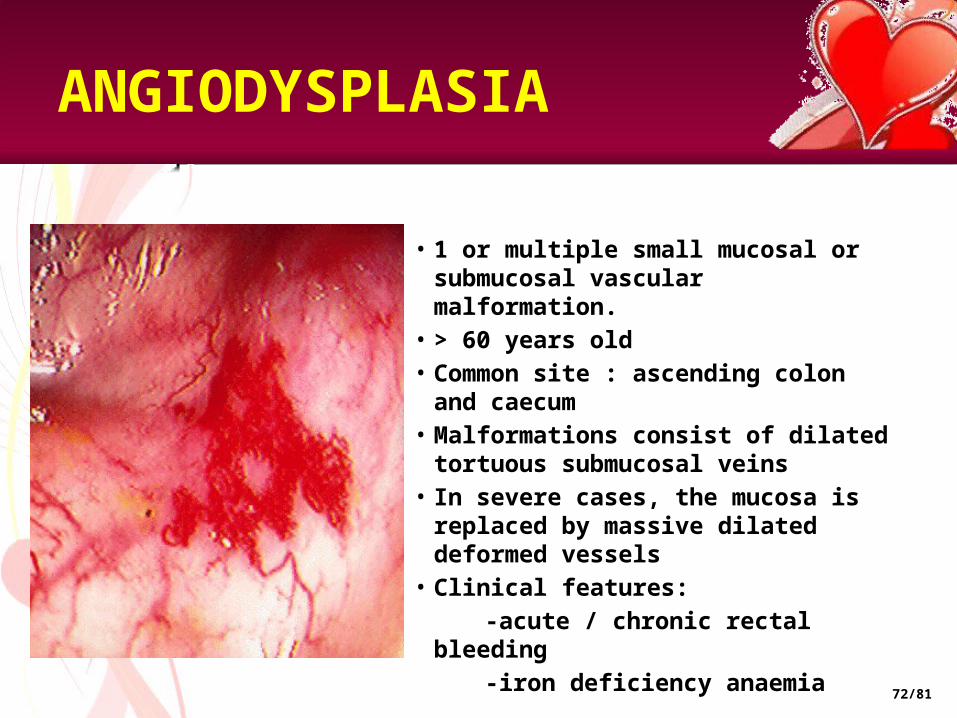
ANGIODYSPLASIA
• 1 or multiple small mucosal or submucosal vascular malformation.
• > 60 years old• Common site : ascending colon
and caecum• Malformations consist of dilated
tortuous submucosal veins• In severe cases, the mucosa is
replaced by massive dilated deformed vessels
• Clinical features: -acute / chronic rectal bleeding -iron deficiency anaemia
72/81

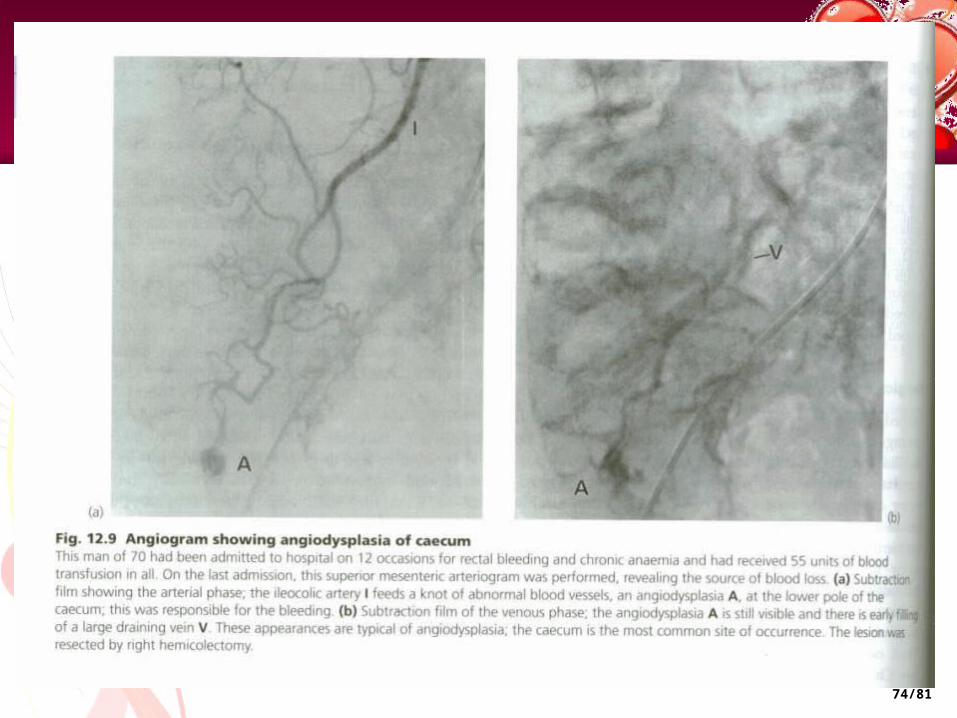
INVESTIGATION
• Colonoscopy -bright red 0.5-1cm diameter
submucosal lesion -small dilated vessels
• Mesenteric angiography
• Radioactive test using technetium-99m –labeled red cells
73/81
74/81

MANAGEMENT
• colonoscopic diathermy
• if patient seriously ill→ catheter is placed in the appendix stump and the colon irrigated progradely with saline or water→ on-table colonoscopy carried out and site of bleeding can be confirmed
75/81

ISCHAEMIC COLITIS
• Elderly• Transient ischaemia of a
segment of a large bowel, followed by sloughing of mucosa
• Common site –splenic flexure• Clinical features: -abdominal pain -rectal bleeding ( dark red) -1-3x over 12 hours• Complication- fibrotic sticture
76/81

HAEMORRHOIDS
• M > F• Female- late pregnancy,
puerperium• Supine lithotomy position- 3 ,7,
11 o’clock positions
• Classification: 1st degree : never prolapse 2nd degree: prolapse during
defaecation but return spontaneously
3rd degree : remain prolapse but can be reduced digitally
4th degree : long-standing
prolapse cannot be reduced
77/81
HAEMORRHOIDS: SIGNS & SYMPTOMS
• Rectal bleeding• Perianal irritation & itching• Mucus leakage• Mild incontinence of flatus • Prolapse• Acute pain• Skin tags at anal margin
78/81

ANAL FISSURE
• Longitudinal tear in mucosa & skin of anal canal
• M > F• Common site: midline in posterior
anal margin• Clinical features: - acute pain during defaecation - fresh bleeding at defaecation
79/81

DIVERTICULAR DISEASE• Rare < 40 years old• F > M• Causes: -Chronic lack of dietary fibre -Genetic• Common site: sigmoid colon• Clinical features: -diverticulosis
(asymptomatic) -chronic grumbling
diverticular pain (chronic constipation & episodic diarrhoea)
80/81

MANAGEMENT
1. Vasoconstrictive agents: vasopressin
2. Therapeutic embolization: -Embolic agents: Autologous clot, Gelfoam, polyvinyl alcohol, microcoils,
ethanolamine, and oxidized cellulose
-Selective angiography
3. Endoscopic therapy: -Diathermy / laser coagulation-Short term control of bleeding during resuscitation
• The bleeding point is localized, perform a limited segmental resection of the small or large bowel
• Poor prognostic features: -age over 60 years -chronic history -relapse on full medical
treatment -serious coexisting
medical conditions -> 4 units of blood
transfusion required during resuscitation
MEDICAL SURGICAL
81/81

THANK YOU FOR YOUR aTTENTIONLUNCH TIME !!!
82/81