Surge Hosptials: Providing Safe Care in Emergencies communication in and with surge hospitals .....8...
29
Surge Hospitals: Providing Safe Care in Emergencies
Transcript of Surge Hosptials: Providing Safe Care in Emergencies communication in and with surge hospitals .....8...

SSuurrggee HHoossppiittaallss::
Providing Safe Care in Emergencies

SSuurrggee HHoossppiittaallss::Providing Safe Care in Emergencies

© 2006 by the Joint Commission on Accreditation of Healthcare Organizations
All rights reserved. No part of this publication may be reproduced in any form or by any means without written permission from the publisher.
Requests for permission to reprint: 630/792-5631.
Cover photos courtesy of George Mills.

Table of Contents
Surge Hospitals: Providing Safe Care in Emergencies
Executive Summary ..............................................................................................................................ivIntroduction ..........................................................................................................................................1
Goal of this Publication ..............................................................................................................1Acknowledgments ......................................................................................................................1
Using surge hospitals to respond to emergencies ....................................................................................2Types of surge hospitals ..............................................................................................................2
Shuttered hospitals or closed wards ........................................................................................2Facilities of opportunity ........................................................................................................2Mobile medical facilities ........................................................................................................3Portable facilities ..................................................................................................................3Project ER One....................................................................................................................3
Planning for, establishing, and operating surge hospitals ..........................................................................4Evaluating the options for surge capability ..................................................................................4Design considerations for dual use in existing buildings ..............................................................4Coordinating effects with local, state, and federal emergency management planners ....................4Obtaining needed personnel and supplies ....................................................................................6
Obtaining a sufficient number of staff members ....................................................................6Medical supplies and equipment............................................................................................7
Leaders in charge of establishing and operating surge hospitals ....................................................7The state’s senior medical officer’s role in surge hospitals ......................................................8
Effective communication in and with surge hospitals ..................................................................8Other issues to consider..........................................................................................................................9
Sufficiency of care ......................................................................................................................9Legal and reimbursement issues ................................................................................................10
Ensuring that long-term surge hospitals offer safe care ..........................................................................12Possible development of Joint Commission standards for surge hospitals................................................13Case studies ..........................................................................................................................................14
Case Study 1:“Katrina Clinic,” Houston,Texas..........................................................................14Case Study 2: Dallas Convention Center ..................................................................................15Case Study 3: Basketball arena and field house at Louisiana State University, Baton Rouge............16
Planning for the surge hospital ............................................................................................16Setting up the surge hospital................................................................................................16Treating patients ..................................................................................................................18Some disadvantages ............................................................................................................18
Case Study 4: Empty former retail store in Baton Rouge, Louisiana ..........................................19Establishing the surge hospital..............................................................................................19Treating patients ..................................................................................................................19Lessons learned....................................................................................................................20
Case Study 5:A veterinary hospital in College Station,Texas ....................................................21Lessons learned....................................................................................................................21
Closing Comment ................................................................................................................................22References............................................................................................................................................23
iii

Executive Summary
Surge Hospitals: Providing Safe Care in Emergencies
After Hurricane Katrina slammed into the Gulf Coast in late August 2005 followed closely byHurricane Rita, the health care community quickly mobilized to provide care to thousands of peoplewho were caught in the storms’ paths. Because the hurricanes and subsequent flooding caused the samesort of devastation to many local health care facilities as it did to other types of buildings in the region,the disaster forced many health care organizations to set up temporary facilities called “surge hospitals” inplaces such as shuttered retail stores, athletic arenas, and veterinary hospitals.The surge hospitals, so-calledbecause they are designed to treat a surge in the number of patients needing care, contained triage, treat-ment, and sometimes even surgical capabilities.These temporary facilities were established to serve as astopgap measure to provide medical care until the area’s health care organizations could reopen.Theseverity of the damage that was done to the region’s health care facilities has brought the health carecommunity’s responsibility for planning, building, and operating effective surge hospitals into focus.Asthis disaster has shown, health care organizations may be forced to provide care at surge hospitals for anextended period of time due to the damage sustained to their permanent facilities during catastrophicevents.This reality challenges the Joint Commission to consider implementing a minimum set of stan-dards to ensure that care provided at surge hospitals is safe and of high quality. Should the developmentof these standards move forward, the Joint Commission would seek input from groups that have exten-sive knowledge of surge hospitals, such as the Texas A&M University System Health Science Center.(Representatives of this organization were involved in establishing and operating the surge hospitaldescribed in Case Study 5, which begins on p. 21.)
It is crucial that health care organizations understand what surge hospitals are and how they can plan forand establish them, including whom they should work with to do so. Hurricanes Katrina and Rita haveshown us that having plans to “surge in place,” meaning expanding a functional facility to treat a largenumber of patients after a mass casualty incident, is not always sufficient in disasters because the healthcare organization itself may be too damaged to operate.Where outside of its own walls does a healthcare organization go to expand its surge capacity? Who should be involved in planning, establishing, andoperating surge hospitals? This paper provides the answers to these questions and offers real-life examplesof how surge hospitals were established on the Gulf Coast.
iv

Introduction
Surge Hospitals: Providing Safe Care in Emergencies
A familiar concept to health care organizations,surge capacity is a health care system’s ability toexpand quickly beyond normal services to meetan increased demand for medical care.1 Surgehospitals have been defined as facilities designedto supplement existing hospitals in the case ofan emergency.2
Because many health care organizations’ abilityto surge in place, meaning the capability toexpand the surge capacity of a functioninghealth care facility, is limited, health care organi-zations need to have plans for increasing surgecapacity which include the establishment oftemporary surge hospitals. It is critical thathealth care organizations (in concert with com-munity leadership) initiate pacts with otherorganizations such as medical centers, schools,hotels, veterinary hospitals, and/or conventioncenters to establish locations for the off-sitetriage of patients as well as for acute care duringan emergency. Hospitals and other health careorganizations must develop communitywideresponse plans that integrate their capacities intoa single, organized response. Communicationsand data sharing that link health care organiza-tions to local and state public health agencies arecritical to this process.
In truth, no single model exists for the surgehospital.Today’s health care leaders must exam-ine the various types of surge hospital facilitiesthat have been used to respond to emergencies
and build their plans based on the needs of thecommunity as well as the resources available tothe organization.
Goal of this PublicationThis publication provides information to healthcare planners at the community, state, and feder-al level about what surge hospitals are, the kindof planning they require, how they can be setup, and who should be responsible for theirestablishment and operation.The case studies atthe end of this paper describe how surge hospi-tals along the Gulf Coast were established andoperated, providing a real-life perspective on theimportance of creating safe surge hospitals afterdisasters strike as well as on the challenges thatgo along with providing care under thesemakeshift conditions.
AcknowledgmentsWe would like to extend our gratitude to thefollowing people, both of whom were instrumental in writing this publication:
■ Pam Brick Freelance Writer
■ Paul K. Carlton, Jr., M.D., FACSLt. General, USAF (Ret.)Director, Office of Homeland SecurityTexas A&M University System Health ScienceCenter
1
“Few, if any, hospitals in America today could handle 100 patients suddenly demanding care.There is nometropolitan area, no geographically contiguous area, that could handle 1,000 people suddenly needingadvanced medical care in this country right now.”
Source: U.S. Congress. Senate. Committee on Government Affairs.FEMA’s Role in Managing Bioterrorist Attacks and the Impactof Public Health Concerns on Bioterrorism Preparedness. 107th Cong., 1st sess., July 23, 2001.Testimony of Tara J. O’Toole, M.D.,M.P.H., Johns Hopkins Center for Civilian Biodefense Studies.

Surge Hospitals: Providing Safe Care in Emergencies
Positioning a hospital emergency room near thesite of every potential disaster is impossible, yet apatient with serious injury needs to be trans-ported to surgery within the “golden hour” afterthe injury occurs for the best chances of sur-vival. Health care planners have developed anumber of innovative ways that a surge hospitalcan respond to this need.These solutionsinclude opening shuttered hospitals or closedwards in an existing facility, temporarily usingbuildings in the community to obtain greatersurge capacity, transporting mobile medical facil-ities to the site, installing portable medical orsurgical units near the emergency, and usingthese types of portable facilities to augment hos-pital capacity.Agreements for use of these facili-ties should, if possible, be made in advance toexpedite the delivery of care in a worst-case sce-nario.A description of the different kinds ofsurge hospitals follows.
Types of surge hospitals
Shuttered hospitals or closed wards The Agency for Healthcare Research and Quality(AHRQ), a branch of the U.S. Department ofHealth and Human Services (DHHS), offers guid-ance on using closed hospitals to expand surgecapacity in an emergency.The agency recom-mends two occasions when the use of a shutteredfacility is warranted: mass casualty events and caseswhere quarantines must be instituted to guardagainst transmission of an infectious agent orcommunicable disease.Any institution contem-plating the use of a closed hospital to expandsurge capacity should ideally engage in advanceplanning to thoroughly assess the facility, althoughit must be acknowledged that in many cases theurgency of a situation often calls for swifteraction.The best approach might be for an existinghospital or other health care organization toacquire the shuttered hospital as a satellite of the
medical center so that patient services such aspharmacy and laboratory can be extended to thesatellite.Whether the site is a shuttered hospital,or, as is described in Sidebar 1 below, a closedhospital ward, the first staff to enter the facilityshould be an environmental crew that wouldclean the facility to ensure that the water, air, andgeneral environment are sanitary and adequate fortheir intended use.
Facilities of opportunity “Facilities of opportunity” are nonmedicalbuildings that, because of their size or proximityto a medical center, can be adapted into surgehospitals.These facilities may include sites suchas veterinary hospitals, convention centers, exhi-bition halls, empty warehouses, airport hangars,schools, sports arenas, or hotels. Health careorganizations can designate such nearby build-ings and equip them to handle an overflow ofpatients. Sometimes a medical facility designedfor another purpose, such as a day surgery cen-ter, can quickly adapt into a surge hospital withminimal cost and effort.
2
Using surge hospitals to respond to emergencies
SIDEBAR 1. AN EXAMPLE OF “SURGING IN
PLACE”—OPENING A CLOSED HOSPITAL WARD
Baton Rouge’s largest public health hospital, the200-bed Earl K. Long Medical Center, is a facil-ity that provides care to the indigent: the poor,the uninsured, the frail elderly, and prisonersfrom the city’s four jails.This hospital’s methodof increasing surge capacity to treat victims ofHurricane Katrina was to open several closedwards within the hospital.This step expanded itscapacity by 200 beds, effectively doubling thehospital in size. Jimmy Guidry, M.D., statehealth officer of Louisiana and medical directorfor Louisiana’s Department of Health &Hospitals (DHH), made the decision to openthe wards, using the strategy of “surging inplace” to increase the hospital’s surge capacity.

Surge Hospitals: Providing Safe Care in Emergencies
Mobile medical facilities Another type of surge hospital is the mobile surgehospital, such as an 18-wheeler truck fitted withstate-of-the-art surgical and intensive care unitsthat can rapidly deploy to the scene of an emer-gency.These mobile intensive care units typicallyhave six beds and their surgical units contain pre-op and post-op recovery areas, a centralized nurs-ing station, and clean and soiled utility rooms.Anadditional advantage is that these facilities can beused not only for disaster management but also asportable clinics offering preventive services torural or otherwise underserved areas.These dual-use facilities have been referred to as Thursday hos-pitals because they can be used for patient care inone given location on a certain day of the week(such as on a Thursday) and can be used in otherlocations the rest of the week, while remainingavailable for other purposes of disaster response atall times.
Portable facilities An additional answer to the surge capacity prob-lem is the portable, mobile medical facility thatcan be set up quickly and be ready to be used to provide care in a few hours. Such units, com-monly known as hospitals in a box, are fullyequipped, self-contained, turnkey systemsdesigned to be set up near mass casualty eventsto treat the most severely wounded as soon aspossible. One soon-to-be-available protoype, theAdvanced Surgical Suite for Trauma Casualties(ASSTC), is a highly mobile, lightweight, self-contained surgical facility that has both militaryand civilian uses. It can be set up in less than 30minutes and is stored in a 5ft. x 5ft. x 10ft. box.Supply cabinets in the unit can be stockpiledwith medications and equipment tailored to thespecific situation.
Project ER One Project ER One is a prototypical emergencycare facility developed by Washington HospitalCenter in Washington, D.C., and conceived as achemical- and bioterrorism-ready mass casualtyfacility. Intended as a model for all new emer-gency departments constructed in the nation,ER One features the following emergency-ready elements to enable a rapid response in disaster-stricken communities:
■ Treatment areas designed to thwart cross-contamination and cross-infection
■ Modular scalability to serve many patients ona daily basis and then expand for larger num-bers in minutes
■ An educational training center that can alsoserve as a planning hub for neighboring healthcare organizations and for handling non-conventional threats
■ State-of-the-art computer information systemthat can track patients and patient records inreal time
■ The ability to share encrypted data with sanc-tioned medical, public safety, military, and gov-ernmental agencies
■ A laboratory for research and development inbioterrorism and similar events
ER One embodies the hallmark principles ofthe surge facility, which include dual use, scala-bility, and modularity. During phase one of theproject, design specifications were developed forthe emergency facility at Washington HospitalCenter.The Phase II design study will put thephase one findings into operation at the hospitalcenter.
3

When planning for the potential use of a surgehospital, health care institutions need to considertheir definition of surge capacity as more than justthe number of available hospital beds. Instead,they need to think about their ability to handlea public health emergency by examining twoadditional types of resources inside their institu-tions: staffing and equipment. Organizations alsoneed to investigate pharmaceutical reserves inlocal pharmacies so they can have a ready supplyof needed medications that last until additionalsupplies arrive from the Strategic NationalStockpile (see p. 7 for a detailed description ofthe Strategic National Stockpile). In addition,communications systems and information tech-nology should be in place so that the organiza-tion can communicate with both internal staffand outside agencies.Another fundamental partof the planning process is the connectivity withcommunity leaders and planning organizationsto ensure compatibility with community think-ing and functional initiatives.
Evaluating the options for surge capabilityWhen considering the surge facility optionsavailable to a health care organization, it isimportant to start at the neighborhood level andwork outward. Can any closed wards beopened? Does the organization have a satelliteoutpatient facility that can be converted to inpa-tient use to increase hospital capacity? What arethe closest available large-capacity venues, suchas veterinary hospitals, exhibition halls, orschools that could be used to expand capacity?
Mobile medical facilities and portable surgicalunits can also be attractive candidates to serve assurge facilities; however, a disadvantage of usingthese facilities is their considerable cost. Cash-strapped hospitals and other health care organi-zations may find it difficult to dedicate hugesums of money for infrastructure changes that
may rarely, if ever, be used. For this reason, manyorganizations are looking at ways to retrofit theirexisting buildings to add surge capacity whilecontrolling costs.
Design considerations for dual use inexisting buildingsHealth care facilities that have one purpose, suchas a surgery suite in nonemergency circumstances,but which can be converted to increase surgecapacity in an emergency, are called dual-use facil-ities. Hospitals themselves can be equipped fordual use during a crisis, but the cost of retrofittinga hospital for dual use is prohibitive for manyorganizations.The Joint Commission encourageshealth care organizations undertaking new con-struction to build for dual use. (See Sidebar 2 onpage 5 for information about building considera-tions for dual use facilities.) Health care leadersshould also consider becoming involved in theconstruction and planning of new structures, suchas libraries, civic centers, or community centers sothat these buildings can incorporate dual-use con-cepts into their construction plans.
Coordinating efforts with local, state,and federal emergency managementplanners Hurricanes Katrina and Rita illustrated that stateand local preparedness is a key factor in a suc-cessful response during the first 24–28 hoursafter a disaster.The relationships and agreementsestablished before a disaster occurs are critical toan effective emergency response.
Health care organization leaders should evaluatetheir surge capacity outside of their own institu-tion in the context of their local communities aswell as at the regional level. (See Sidebar 3 onpage 5 for a list of issues that leaders shouldconsider regarding collaborating with otherhealth care organizations during emergencies.)
Planning for, establishing, and operating surge hospitals
Surge Hospitals: Providing Safe Care in Emergencies
4

Surge Hospitals: Providing Safe Care in Emergencies
5
The catastrophe in New Orleans showed thenation nothing if not the reality that disasterscan cripple entire regions. Institutions must putcooperative agreements in place with state andregional partners and also work with federalrepresentatives who can ensure that sufficientresources are available to handle a widespreademergency.
Certain locations in the country are alreadydoing this. For example, New York City under-
stands, because of its recent history and proximi-ty to other states, that a disaster that occurs insidethe city could also impact New York State, NewJersey, and Pennsylvania if the city’s ability torespond to the emergency is overwhelmed bythe severity of the disaster.As a consequence, asignificant amount of regional planning occurs inthat city.
SIDEBAR 2. BUILDING CODE VARIANCES
Disaster planning highlights the need forchanges in building code requirements to meetthe demand for high-volume patient care. Mostof these recommendations could also apply tothe new construction of schools, libraries,hotels, and other buildings in a community.Some of the variances that health care organiza-tions need to consider include the following:■ Wide hallways and stairwells to allow stretch-
ers to pass each other ■ Redundant power, such as a second genera-
tor or a duplicate electrical system that servesas a backup for the primary system
■ “Clean” rooms that contain self-decontami-nating surfaces, negative pressure air–handlingsystems, and controlled pressure, temperature,and humidity
■ Horizontal construction with larger andfaster elevators to avoid bottlenecks whenmoving patients to different floors
■ Multiple patient drop-off entrances to pre-vent traffic jams
■ HEPA filter systems that trap biologicalagents in incoming air and expose them toultraviolet light to render them harmless
■ Storage for medical equipment which pro-tects supplies from biological and radiologicalthreats
■ Docking stations to accomodate 18-wheelerresponse vans that meet all standards of care
SIDEBAR 3. LEADERSHIP ISSUES FOR
COLLABORATING WITH PROXIMATE HEALTH CARE
ORGANIZATIONS
■ What health care organizations are geograph-ically proximate (all types, whether offeringsimilar services or not)?
■ What proximate health care organizationsoffer similar services?
■ What resources (such as supplies, beds, andstaff) might be shared or pooled in an emer-gency response?
■ What might our organization be able to pro-vide for proximate health care organizations?What provisions can we make to offer suchservices/supplies in the event of a disaster oremergency?
■ What in-kind or reciprocal agreements mightwe make with each organization?
■ How will we communicate with proximatehealth care organizations? Who should becontacted at each organization?
■ If care recipients must be evacuated from ourorganization, which neighboring organizationcould receive transferred individuals?
■ What suppliers/vendors does each proximateorganization rely on for materials that mightbe needed in an emergency? What are theirback-up plans for supplies in case of anemergency? Are all of the region’s health careorganizations relying on the same vendors?
Source: Joint Commission on Accreditation ofHealthcare Organizations: Guide to EmergencyManagement Planning in Health Care. Oakbrook Terrace,IL: Joint Commission Resources, 2002.

Surge Hospitals: Providing Safe Care in Emergencies
Obtaining needed personnel and suppliesOne of the key components of an effective healthand medical care response is ensuring an adequatenumber of qualified health care providers who areavailable and willing to serve in a mass casualtyevent. Having sufficient supplies, pharmaceuticals,and equipment is also critical.
Obtaining a sufficient number of staff
membersA model for determining the number of staffneeded for a surge facility is the ModularEmergency Medical Stem (MEMS) designed bythe U.S. Department of Defense.The system isbased on the incident command system, whichis commonly used by the emergency medicalservices community.The system sets up a net-work used to access patient care personnelthrough neighborhood emergency help centersand acute care centers.Activities that can help inthe search for additional qualified personnel in atime of need include the following:
■ Recruiting from retired or currently unem-ployed but qualified volunteer providers with-in the community and state
■ Making use of reserve military medical and nurs-ing providers and other responders, as well as anexpanded group of providers, such as veterinari-ans, dentists and dental auxiliary providers, phar-macists, and health professional students
■ Reallocating providers from nonemergencycare and nonemergency sites to emergencyresponse assignments and from unaffectedregions to affected regions (this will involveidentifying skill sets of each practitioner group[such as paramedics and nurse midwives], so asto optimize reassignment potential)
■ Creating and training a pool of nonmedicalresponders to support health and medical careoperations
■ Making adequate provisions to protectproviders (and their families) who serve inmass casualty event situations to ensure theirwillingness to respond
Perhaps the best known source of supplementarymedical personnel is the Medical Reserve Corps(MRC) Program, which organizes the services ofmore than 27,000 practicing and retired physi-cians, nurses, and other health professionals as wellas ordinary citizens who wish to volunteer incommunity public health efforts and help duringlarge-scale emergencies. Founded by PresidentGeorge W. Bush in 2002 in cooperation with theUSA Freedom Corps, the MRC specializes inidentifying, training, and organizing volunteermedical and public health professionals.
Two additional resources exist for the recruit-ment of medical staff in a worst-case scenario.The first is the National Disaster MedicalSystem (NDMS), established in the 1980s by theU.S. Departments of Health and HumanServices and Veterans Affairs and the FederalEmergency Management Agency. NDMS orga-nizes 7,000 health care volunteers in locallysponsored specialty teams that become federal-ized upon activation.The second resource is thePublic Health Service Commissioned Corpsheaded by the surgeon general.The corps con-sists of roughly 6,000 physicians, nurses, pharma-cists, allied health care workers, dentists, scien-tists, computer specialists, and other officersavailable to offer health care–related expertise intimes of war or national emergencies.
Local medical, nursing, and allied health carestudents can also help provide care in times ofneed. In addition, the American Red Cross,temporary medical staffing agencies, and volun-teer programs, such as AmeriCorps andSeniorCorps, provide medical personnel andvolunteers to health care organizations duringemergencies.
Education of the existing hospital staff is alsoimportant and involves the following areas: bet-ter disaster-response awareness, improved skills,
6

Surge Hospitals: Providing Safe Care in Emergencies
an understanding of roles and responsibilities,more effective communication, and experiencein cooperating with other staff members as wellas personnel from outside agencies and organi-zations during emergencies. Strengtheningemergency training programs fortifies prepared-ness, but the skills most valuable during a disas-ter are those practiced by staff every day.
Medical supplies and equipmentA number of options exist to acquire the neededbeds, medical supplies, and equipment in a time ofcrisis.The Strategic National Stockpile, a programof the Centers for Disease Control and Prevention(CDC), maintains large quantities of medicationsand medical supplies, such as airway maintenance,IV maintenance, and medical surgical items to beused in public health emergencies including infec-tious disease outbreaks, natural disasters, and man-made disasters. Needed medicines and suppliescan be delivered free of charge to any state as partof this program. Each state is then responsible fordistributing supplies to local communities.Torespond to this additional need, the medical centermay need to consider equipment rental or leasingoptions.
The experience of the medical teams that set upthe surge hospitals in Louisiana and Texas fol-lowing the hurricanes was that the StrategicNational Stockpile may not be able to deliverneeded medical goods for several days duringemergencies of extreme magnitude. In suchemergencies, hospitals and medical centers mayhave to order equipment from local suppliers orrequest donated items from physician offices,medical schools, local armories, medical supplyhouses, and other sources.This fact underscoresthe value of establishing partnerships with suchorganizations in advance to accelerate the pro-curement of supplies in an emergency.
Surge facility pharmaceutical procurement canbe more problematic than that of disposableequipment and supplies because of the legalrequirements surrounding the prescription, stor-age, and preparation of medications. Orderingdrugs could pose a problem if the surge facilitydoes not have preexisting contracts with phar-maceutical suppliers. One way of handling thisproblem is to have a sponsoring hospital orother health care organization order medicationsfor the surge hospital.Another option is for ahospital to establish an advance contract with apharmaceutical distributor that would be imple-mented only in an emergency. If possible, thenumber of supplies held in inventory at thesurge hospital should be sufficient to last at leastthree days per patient.
Leaders in charge of establishing andoperating surge hospitals It is vital that the leaders who have integral rolesin establishing and maintaining surge hospitals arevisible within the community and ensure consis-tency in the way surge hospitals operate.Theintent of setting up the surge hospital is todemonstrate to stricken communities that themedical community will continue to take care ofthe ill and injured. In this role, the leaders of thestate are key.Advance planning for emergencyevents is crucial in enabling them to project con-sistency and to protect and enhance the publictrust.To promote visibility, officials must maintaincommunications with the public through personalvisits to the hospital site as well as through mediainterviews and appearances.
Disasters happen locally, requiring a local response.As such, the states within the U.S. have variousdesignated government officials who possess theauthority to call for the establishment of surgehospitals. In Texas, for example, the county judgehas the power to order the creation of a surge
7

Surge Hospitals: Providing Safe Care in Emergencies
hospital. However, if it becomes clear that theemergency will have a statewide effect, the gover-nor takes charge of the effort and delegates theestablishment of surge hospitals to the seniormedical officer in the state, usually the commis-sioner of health or director of the public healthdepartment.This is what occurred as Texas pre-pared for Hurricane Rita.
The state’s senior medical officer’s role
in surge hospitalsThe senior medical officer in the state appointsa medical director of the surge hospital, whothen assembles a set-up team. Sometimes theperson recommended to oversee the creation ofa surge hospital is a physician who has devel-oped a relationship with state officials and hasbecome a trusted advisor.This is the wayRaymond Swienton, M.D., FACEP, was giventhe authority to recommend the sites for andsupervise the opening of the surge hospitals atLouisiana State University (see p. 16) and at anempty former retail store a few blocks from theEarl K. Long Medical Center in Baton Rouge(see p. 19). Swienton is the co-director ofEmergency Management Services of theDisaster Medicine and Homeland SecuritySection, and associate professor, Division ofEmergency Medicine in the Department ofSurgery at the University of Texas SouthwesternMedical Center at Dallas. In addition, Swientonserved as a senior advisor to the State of
Louisiana’s Secretary of Health as well as theState Health Officer and staff. Over the previoustwo years, he has become well known to thesenior state health care leadership by providingdisaster preparedness education and training pro-grams and helping establish these programsstatewide.
Effective communication in and withsurge hospitalsCommunication is often the weakest link inmass casualty incident responses.3 This fact isborne out by the experience of those whoworked in the post-Katrina surge hospitals inLouisiana and Texas.The surge hospital at theempty former retail store site was no exceptionto this rule. Cellular access was sporadic at bestand often not available for an hour or more.Radio communication with arriving buses oremergency services vehicles was essentiallynonexistent. Inside the facility itself, communi-cation posed a separate challenge because of thesize and acoustic environment of the facility.
A redundant communications system thatincludes two telephone systems, two-way radios,more reliable paging systems, and better satellitecommunications needs to be explored to miti-gate the negative effects of poor communicationon patient care.
8

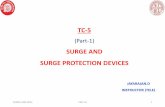
Sufficiency of careIdeally, the goal of the surge facility is to maintainhigh standards of care. In practice, however, medi-cal treatment in a surge hospital may reach onlythe level of sufficiency of care because of the chal-lenging circumstances under which the facilitymust operate. (See figure below for an illustrationof the difference between the standard of care andsufficiency of care.)
In a sufficiency-of-care facility, the medical stafffaces challenges such as limited privacy for patientassessments, crowded conditions, limited access tomedical records, and inadequate access to testingcapabilities. For example, of all the surge hospitalsset up after Hurricane Katrina, the empty formerretail store (see p. 19) veered the furthest from theaccepted standard of care—but it still deliveredsufficient care.The goal of any sufficiency-of-care-
facility is to treat each patient and then transferhim or her to a facility with full capability to treatpatients at an ideal level of care.Again, this is whatoccurred at the empty former retail store site,which remained open for only five days.
The veterinary hospital in College Station,Texas,(see p. 21) was able to deliver a higher quality ofcare because, although it was intended for use asan animal hospital, it contained most of the equip-ment and supplies necessary to treat humanpatients. In addition, electrical power, the watersupply, and the telephone system were all inworking order and it had backup power systems,access to medical gases, and a high standard ofcleanliness.
Any plan for a surge hospital that is envisionedas a sufficiency-of-care site should be part of a
Surge Hospitals: Providing Safe Care in Emergencies
9
Other issues to consider
Standard of care vs. sufficiency of careThe concept of sufficiency of care—medical care that may not be of the same quality as that delivered undernonemergency conditions, but is sufficient for need—is often the reality of surge hospitals because of the diffi-cult circumstances in which care is provided.

Surge Hospitals: Providing Safe Care in Emergencies
community response network.This way, all inva-sive procedures, deliveries, or surgical needs canbe transferred to a standard-of-care-based hospi-tal unless emergent intervention is needed tosave a life. To handle such emergent cases,advanced airway equipment, ventilator support,portable dialysis units, and monitoring capabili-ties should be available on site.
Legal and reimbursement issuesAnytime health care workers perform volunteerservices, they expose themselves to the risk ofhaving claims filed against them by patients whobelieve they have been harmed during the deliv-ery of care.The state and federal governmentshave methods by which the law can be changedto provide some liability protection. During thecrisis in the Gulf Coast, for example, the governorof Louisiana waived the state of Louisiana licens-ing restrictions to allow access to all licensedproviders throughout the U.S.The federal govern-ment also set aside certain national laws so thathealth care workers responding in an emergencycould act as their professional judgment dictatedwhile delivering care without fear of medical lia-bility. For example, the U.S. Department of Health& Human Services afforded liability protection tohealth care workers who volunteered to treat hur-ricane victims.
The Emergency Medical Treatment and ActiveLabor Act (EMTALA), which states that emer-gency rooms must diagnose, treat, and stabilize apatient before being able to transfer him or her,was also waived because, during an emergency,transfer may be the most expedient action. Byprearranged cooperative agreement, particularmedical centers in a community may be desig-nated to accept certain types of patients, such asburn or trauma victims.Therefore, if a burn vic-tim arrived at a surge facility during an emer-gency, the patient would immediately be trans-ferred to the preselected hospital.
A number of recent laws and agreements havemade it easier for medical personnel from otherregions to provide health care assistance toaffected areas.The need to make the best possi-ble use of volunteer health workers in an emer-gency led to the development of the EmergencySystem for Advance Registration of HealthProfessions Volunteers (ESARHPV)4.This act,still in its developmental stages, will enable eachstate and U.S. territory to set up a standardized,volunteer registration system for medical work-ers. Each state’s system is designed to containup-to-date information about a volunteer’sidentity, licensing, credentialing, accreditation,and privileging in hospitals or other medicalorganizations. Such a system will allow eachstate to rapidly identify professional health carevolunteers during mass casualty events and willenable states to share these preregistered andalready credentialed health care workers nation-wide.
The Emergency Management Assistance Compact(EMAC), enacted by Congress in 1996, also facili-tates mutual aid between 49 U.S. states, theDistrict of Columbia, Puerto Rico, and the VirginIslands in times of crisis. EMAC, which is admin-istered by the National Emergency ManagementAssociation, is not an agency of the federal gov-ernment, but is instead an agreement among thestates to provide aid across state lines when anytype of disaster occurs.The governor of the affect-ed state must first declare a state of emergency,and then the state can request the assistance itneeds.This appeal then activates the response fromother EMAC-member states, putting the EMACsystem of coordination and deployment inmotion. EMAC garnered national attention in2004 when four major hurricanes hit the U.S. in asix-week period, triggering what was then thelargest use to date of state-to-state mutual aid inU.S. history.
10

Surge Hospitals: Providing Safe Care in Emergencies
Under the compact, licensed physicians or otherhealth care workers who travel to any of theEMAC member states or territories (once theconditions for providing assistance have beenmet) will have their credentials honored acrossstates lines. EMAC provisions addressing liabilityand workers compensation issues for these per-sonnel alleviate the financial and legal burdensof the responding states.
EMAC enabled a massive deployment of medicalpersonnel and resources in response to HurricanesKatrina and Rita. More than 31,000 workers,including medical personnel, search and rescuestaff, law enforcement officers, waste managementexperts, and fire fighters were dispatched fromdozens of states to Louisiana and Mississippi.
Reimbursement is another issue that the federalgovernment would need to examine so that cer-tain provisions of reimbursement for Medicareand Medicaid might be relieved in a disaster situa-tion. Some of these federal requirements involvecertifying the quality of the facility, the privilegingof its staff, and the upkeep of medical records tosecure reimbursement from the federal govern-ment. Many of these requirements would have tobe set aside so that the health care system doesnot end up with two disasters—one caused by theevent itself, and the other caused by the loss ofrevenue to the health care organizations involvedin providing care.
11

Ensuring that long-term surge hospitals offer safe care
Surge Hospitals: Providing Safe Care in Emergencies
All surge facilities must ensure that the care theyprovide is safe. In addition, certain quality assur-ance processes must be followed in surge hospitalsso that, for example, patients are identified anddrug errors do not occur.The longer a facilityremains operational, the more demands must bemade on both its environment of care and theprocess of care delivery to make sure they are inline with high standards of care.These demandscan ensure that, while expedient care may begiven, substandard care is never allowed.
The possibility of surge hospitals operating on along-term basis adds a third dimension to theconcept of the emergency event itself. Health careorganizations are used to thinking about emer-gency events on two levels of magnitude, eachwith its own response.The first level of emergen-cy can be called the major incident. Examplesinclude a school bus accident with multiple casu-alties, or an industrial explosion producingnumerous burn victims.The local hospital needsto respond by activating its emergency manage-ment plan in order to have enough staff availableto manage the situation; however, this type ofevent is usually short-lived—lasting perhaps 24hours—and the community and its hospital bothremain intact.
The second type of emergency event can be char-acterized as the disaster. For example, HurricaneKatrina was a disaster in Gulf Port and Biloxi,Mississippi, because the health care infrastructurewas damaged as was the infrastructure of thecommunity.The disaster presents as a community-wide problem that can extend for many weeks ormonths and may need extensive state and federalresources to ameliorate the situation.
The third level of emergency, virtually unvisitedby health care planners until recent events thrust
it into view, can be described as the catastrophe:a series of disasters occurring to the same com-munity in a short period of time.What hap-pened in New Orleans after the levees brokewas a catastrophe. First, the hurricane hit, caus-ing serious but manageable damage.Then thelevees broke, flooding the city.As a consequence,the community’s entire infrastructure brokedown: sewer, water, and electrical power were alldisabled.The ability of health care and emergen-cy medical services to respond was totally dis-rupted. Finally, civil disturbance occurred as des-perate people fought to survive.This event wasunprecedented in recent U.S. history and canonly be compared to the San Francisco earth-quake and fire of 1906, which ranks as one ofthe most serious natural disasters of all time.
What happened in New Orleans has forcedhealth care organizations to think about howsurge hospitals can be used on a long-term basisto supply needed medical care. Most pointedly,Charity Hospital, which was significantly dam-aged in the disasters, has prompted the need forpatients who would normally be treated at thehospital to instead seek care at surge hospitals inthe area. The surge hospital that was initiallyestablished in this area (and which will be devel-oped further in two additional phases) could beused by the Federal Emergency ManagementAgency (FEMA) as a model for the nation.
The initial stage of the surge hospital that wasset up after Charity Hospital was severely dam-aged was the tent hospital established onOctober 8, 2005, in the parking lot of the oldCharity Hospital.This surge hospital remainedin place when this publication went to press.The next phase being considered is a hard-sidedshelter system with individual rooms, each withits own bathroom.
12

Surge Hospitals: Providing Safe Care in Emergencies
Louisiana State University (LSU), which operat-ed Charity Hospital, expects to set up a modularcomponent structure over the next six monthsthat has been used nationwide and meets allJoint Commission standards. Such a structuremay represent a permanent solution to the prob-lem of a replacement for hospitals that must berebuilt due to extensive damage from a disaster.This type of premanufactured component con-
struction is assembled on site and is built to lastfor years.Alternatively, the permanent facilitymight evolve into a site that has a main hospitaldowntown with eight satellite offices that couldaccommodate outpatient surgery suites or clinics.These satellites could be converted into surgehospital space within hours. Other options werebeing considered as this paper went to press.
13
Possible development of Joint Commission standards forsurge hospitalsIn the aftermath of the hurricanes that caused significant damage to health care organizations on theGulf Coast, the Joint Commission is considering the development of a set of standards with which surgehospitals would need to comply.These standards would assure the public that the care received in a givensurge hospital—or in the health care system as a whole—is safe. If the development of these standardsmoves forward, the Joint Commission will work with health care organizations that are developing plansfor surge facilities so that these standards can be implemented quickly and with minimal cost.

Surge Hospitals: Providing Safe Care in Emergencies
This section examines several surge hospitals thatwere set up after Hurricanes Katrina and Rita dev-astated the Gulf Coast.They illustrate the variety offorms the concept can take as well as the variety ofresponses medical personnel were able to coordi-nate in response to the recent disasters.
Case Study 1: “Katrina Clinic,” Houston,TexasThe Houston Astrodome served as a shelter formore than 25,000 of the people who fled the leveebreaches that followed Hurricane Katrina’s destruc-tion in New Orleans. In response to this onslaughtof evacuees in crisis, many of whom had lived inappalling conditions for days, Harris CountyHospital District (HCHD) in Houston set up“Katrina Clinic” in Reliant Arena, a building adja-cent to the Houston Astrodome. In partnership withHCHD, physicians and faculty from Baylor Collegeof Medicine (BCM) staffed the clinic with othermedical volunteers from throughout the region.
Three days after the storm hit, Harris County,TexasJudge Robert Eckels and Houston Mayor BillWhite asked George Masi, chief operating officerof the Harris County Hospital District, to coordi-nate a facility that could manage the health needsof the arriving multitudes. The HoustonAstrodome in Reliant Park, in ordinary times usedas a livestock exhibition hall, had been long desig-nated a shelter by local officials involved in disasterplanning.The team from HCHD and its physicianstaff from BCM had roughly 15 hours to preparebefore the first busload of patients arrived.
The set-up team employed stored rods and curtainsused for exhibitions to separate rooms into spacesthat could be used for patient registration, triage,exam rooms, and a pharmacy.Tables, computers,photocopiers, telephones, and full sets of medicalequipment and supplies were deployed fromHCHD and brought to the clinic, which had thebenefit of full electrical power, working toilets, and
potable running water.The team acquired a num-ber of donated X-ray machines from a nationalmedical supply corporation and a major pharma-ceutical company sent a mobile laboratory on an18-wheeler truck.Two national drug store chainsset up pharmacies at the site, one housed in twomobile homes. Many local businesses donated med-ical supplies and the Red Cross provided cots. Forthe most part, the 100,000-square-foot clinic wasprepared to provide care to patients by midnight.
Supervised by medical director Thomas Gavagan,M.D., MPH, vice chair for community health inthe Department of Family and CommunityMedicine at BCM, the clinic processed 150patients per hour over 15 days—or a total of morethan 10,000 people.
Originally equipped with 20 examination rooms,the clinic quickly ballooned to 65 exam rooms.The medical staff members worked 36 hoursstraight after the clinic opened, and were finallyrelieved after a call for medical volunteers producedabout 2,700 responders. For the rest of the time, 25physicians were assigned to work per each 12-hourshift.The staff administered thousands of immu-nizations—10,000 tetanus shots alone—and filled asimilar number of prescriptions.The site remainedan outpatient facility; acutely ill patients were sentto local hospitals for treatment.
Paul Sirbaugh, M.D., Director of PrehospitalMedicine at Texas Children’s Hospital, oversaw aspecial pediatric clinic at the Astrodome so thatchildren could be seen by a physician without having to be separated from their parents. Mentalhealth needs were seen as crucial to the care ofhurricane survivors, so psychiatric staff from BCMstepped in to provide mental health counseling.
The clinic’s medical staff treated patients withbroken bones, chest pain, and withdrawal fromdrug addiction, but most of the patients had
14
Case studies

Surge Hospitals: Providing Safe Care in Emergencies
chronic conditions, such as asthma, diabetes, andhigh blood pressure. One patient presented witha gunshot wound to the arm. On the fourth dayof operation, physicians began to see quite a fewpediatric patients with some type of gastroin-testinal infection that caused diarrhea and vom-iting, presumably from exposure to the contami-nated water in New Orleans.The infection wastransmitted to several hundred people beforephysicians identified the cause as the Norwalkvirus and promptly provided treatment.As thenumber of acute care cases decreased, evacueesat the Astrodome began requesting assistance formore mundane medical needs, such as prescrip-tion eyeglasses or other minor complaints forwhich they could not seek care in New Orleansbecause of a lack of health insurance.
As patients continued to pour into Katrina Clinic,Houston’s mayor requested that a second clinic beopened at the George R. Brown ConventionCenter. Physicians from the University of TexasHealth Science Center in Houston staffed thissite. It processed 500 to 700 evacuees each day, fora total of more than 9,000 patients.
Katrina Clinic remained open for 2½ weeks at acost of $4.1 million.After it closed down, theRed Cross established an outpost at the site todeliver first aid to evacuees.
Thomas Gavagan, M.D., MPH served as the pri-mary source of information for this case study.
Case Study 2: Dallas Convention CenterPhysicians, employees, and students from theUniversity of Texas (UT) Southwestern MedicalCenter at Dallas began gearing up their reliefefforts even before Hurricane Katrina evacueesstarted pouring into Dallas.They established amedical command center at the DallasConvention Center, where they set up a surge
facility.The site for the facility was chosen byofficials from the City of Dallas Office ofEmergency Management and the city fire mar-shal’s office, Dallas Fire-Rescue.
In Dallas, faculty and employees from UTSouthwestern volunteered in large numbers,working at Reunion Arena and the DallasConvention Center to help with the reliefeffort.Volunteers included physicians as well asnurses, pharmacists, respiratory therapists, andallied health care workers.
Kathy J. Rinnert, M.D., MPH, assistant professorof emergency medicine at UT SouthwesternMedical Center in Dallas and attending physi-cian at Parkland Health and Hospital Systemsand Raymond Fowler, M.D., associate professorof emergency medicine at UT SouthwesternMedical Center and deputy medical director foroperations and quality assurance for the DallasArea BioTel (EMS) System, both served as med-ical directors of the site. More than one hundredphysicians from UT Southwestern as well asmedical staff from Parkland Health and HospitalSystems, Children’s Medical Center of Dallas,Methodist Hospital of Dallas, Medical CityHospital, and Baylor Medical Center worked upto 20-hour days to care for the sick and injured.The site was staffed locally with no supportfrom out-of-state medical volunteers. Facilitiesincluded an 11-bed urgent care center and a 20-bed chronic care center.
The 8,200-square-foot surge facility was openfrom September 1 through September 16. Faculty,staff, residents, and medical students treated morethan 4,000 evacuees during the first week alone,and a total of roughly 8,600 patients over the 16days of operation. The medical staff treated notonly patients from the shelter set up at the site,but also those from other shelters and hotels inDallas.Wounds were the principle injuries seen
15

Surge Hospitals: Providing Safe Care in Emergencies
during the first three days, followed by gastroin-testinal disorders, and then acute exacerbations ofchronic medical conditions such as asthma, dia-betes, and cardiovascular problems.
Located one sub-basement level down from themain floor, the facility shared space with an evac-uee shelter ringed by a variety of social serviceagencies, such as the Red Cross, the SalvationArmy, and the Texas State Child ProtectiveServices Agency. Medical equipment, supplies, andpharmaceuticals came from the local medicalcommunity, primarily Children’s Medical Centerand Parkland Health and Hospital Systems, thelargest contributor.Telephones, copiers, faxmachines, and other office equipment were pro-vided by the City of Dallas.
According to Rinnert, the main advantages of asurge facility site such as a convention centerinclude the flexibility of the space, which can becordoned off as circumstances dictate, and theavailability of air conditioning in a climate thatnormally averages more than 100º Fahrenheit inSeptember. Several disadvantages were the austereappearance of the site, which had bare concretefloors and harsh fluorescent lighting, and theabsence of showering facilities. Overall, however,the convention center proved to be a satisfactoryenvironment for a surge facility.
Kathy J. Rinnert, M.D., MPH, served as the pri-mary source of information for this case study.
Case Study 3: Basketball arena andfield house at Louisiana StateUniversity, Baton Rouge
Planning for the surge hospitalWhen Jimmy Guidry, M.D., the state health offi-cer of Louisiana and medical director for theLouisiana Department of Health & Hospitals
(DHH), heard that large numbers of patients hadnot been evacuated from New Orleans hospitalsand nursing homes before Hurricane Katrina hit,he decided that the state needed to have an addi-tional acute care facility in place in Baton Rouge,knowing that existing hospitals would be inundat-ed with patients. Raymond Swienton, M.D.,served as an advisor to Guidry to aid in the selec-tion of the site for this surge hospital. Because of alongstanding relationship between the DHH andLouisiana State University (LSU), Guidry selectedChris Trevino, M.D., director of emergencymedicine at St. Elizabeth’s Hospital in Gonzales,Louisiana, and medical director of emergencymedical services for the state of Louisiana, to over-see the establishment of a surge hospital at theuniversity. Guidry then chose the LSU PeteMaravich Assembly Center (PMAC), a basketballarena, as the site of the surge hospital and LSU’sCarl Maddox Field House, located next door, as aspecial needs shelter.The two sites were chosenbecause of their size and the availability of medicalstaff from LSU.
Guidry selected Walter Cain, M.D., medical direc-tor of LSU’s Fire and Emergency TrainingInstitute and attending physician at Earl K. LongHospital, a part of LSU’s Health Care ServicesDivision, to set up the special needs shelter. Cainthen asked Stephen Barr, assistant technical direc-tor of the LSU Theater, to help convert the fieldhouse into a special-needs hospital, primarily fornursing home patients.
Setting up the surge hospitalThe PMAC began as a medical triage facility,but was soon transformed into a surge hospital.The 800-bed facility at the PMAC became thelargest acute care field hospital to be establishedin the U.S. since the Civil War.
The LSU administration drew on its student gov-ernment to take charge of the volunteer efforts of
16

Surge Hospitals: Providing Safe Care in Emergencies
the students, faculty, and staff.The student leadersset up a volunteer hotline and Web site for volun-teer registration.They handled more than 1,000calls per day from people at LSU who wanted tovolunteer or provide lodging to displaced personsor emergency personnel. Student volunteersstaffed 80 to 90 people per shift to work in bothhospitals.After the schedules were finalized, thestudents called volunteers back to give them theirshift assignments.The student leaders managednonmedical volunteers both at the field house andat the PMAC. Eighty-five nonmedical volunteersworked 12-hour shifts daily. Student volunteersalso helped set up the surge facilities by movingboxes, setting up shelves and tables, and perform-ing other nonmedical tasks. LSU Chancellor SeanO’Keefe met with medical staff daily to assesstheir most pressing needs.
A significant number of health care providersarrived from out of state. For example, the IllinoisMedical Emergency Response Team assisted teamsfrom medical centers in Texas as well as localmedical volunteers from Baton Rouge, especiallythose from St Elizabeth’s Hospital.
The special-needs hospital at the field house tookonly approximately two days to establish becausethe state had experience in creating back-up spe-cial-needs facilities for nursing home patients whohave to be evacuated because of power outagesand other similar problems. Setting up the PMAChad to proceed rapidly because patient arrival wasimminent, so the emergency room at the PMACwas up and running in eight or nine hours.Electricity was in good working order and gener-ator backup was available.
The DHH, through one of its components, theBureau of Emergency Medical Services, wasintimately involved in the emergency room’s setup, providing both paramedics and supplies.Two
years before, Guidry and the rest of the medicalleadership in the state had evaluated what itwould take to set up a field hospital and hadpurchased supplies and equipment through agrant from the U.S. Department of HomelandSecurity. As a result, the state already had a 200-bed hospital and all the supplies associated withit in storage.Training had also been in place. Infact, just a week before, the state held a disasterexercise to prepare for a fictional storm named“Hurricane Pam.”
Private emergency medical service companieslent volunteers and equipment. Trevino alsoobtained assistance from the nursing, respiratorytherapy, and other professional staff at St.Elizabeth’s Hospital to set up and staff thePMAC emergency room. During the first 48hours of operation, the medical and professionalstaff worked straight through, without leavingthe facility, perhaps sleeping for an hour or twoat a time.After the third day, hundreds morevolunteers from other local hospitals arrived tolend a hand, but the huge volume of patientscontinued to demand 12-hour shifts or more.
Large sports arenas typically have sizeable entryports where trucks can easily bring equipmentinto the site.The medical team chose one of thelarger of these ports as a triage center.They setup tables in the port, where physicians and nurs-es could examine the patients coming in byambulance or bus and then send them into thearena on foot or by wheelchair or stretcher.Attimes, convoys of up to 15 ambulances, eachcarrying four patients, would arrive at once.Busloads of 50 patients would also arrive; some-times, only a few on each bus were ill. Healthypassengers who had traveled 60 miles from NewOrleans wanted to exit the bus, use the bath-room, and have something to eat or drinkbefore getting back on the bus to be transferred
17

Surge Hospitals: Providing Safe Care in Emergencies
elsewhere. Patients coming in by helicopterentered at a different port and then weretriaged. In total, both hospitals treated or housedroughly 6,000 patients in addition to the peoplewho simply used the facility as a stopover beforebeing bused to a shelter. Counting those people,both facilities served 15,000 to 20,000 people.
Areas of the PMAC were reserved for laborato-ry, X-ray, electrocardiogram, and ultrasound ser-vices.The staff also arranged for dialysis patientsto be transported to a local dialysis center fortreatment. The hospital even had 80 bedsequipped with a cardiac monitoring system.Asfor meals, one of the larger local church groupscalled Trevino and announced they could pro-vide up to 16,000 cooked meals a day for boththe PMAC basketball arena and the special-needs field house next door. LSU volunteersalso donated food. Meals were provided fourtimes per day so that staff and volunteers couldeat during night shifts.
Security was initially provided by the LSU securi-ty force and was later supplemented by SWATteams and the National Guard. Neither site had amajor security incident, although a potential secu-rity threat occurred when healthy individualsarriving in buses were originally told they couldnot leave the bus unless they were sick.This prob-lem was resolved by allowing everyone off the busto freshen up and have some food and drink.Afterthe riders understood that the facility was a hospi-tal and not a shelter, they returned to their seatson the bus.
Treating patientsAs patients poured into the facilities at LSU, theyquickly filled the basketball arena’s emergencyroom to capacity and spilled over into the fieldhouse for four to five days.The initial surge ofpatients was from hospitals and nursing homes,
but buses full of evacuees soon transported a pop-ulation of all ages to the facilities.The principalcondition treated was the exacerbation of chronicmedical conditions such as diabetes or asthmabecause of dehydration and because patients hadnot been able to take their prescribed medicationsfor several days.Another issue was the fact thatsome patients could not recall the names of themedications they had been taking.The staff alsosaw some cases of trauma and delivered severalbabies who needed resuscitation.At one point, thehospital had 14 ventilatory patients. Because thepatients arrived so early after the disaster, only afew cases of infectious disease, such as abscessesand cellulitis, were seen.
When the patients came in such waves, the pri-mary goal of the medical team was to treat themas quickly as possible.After the first day, the doc-umentation process began to take shape and bythe third day, the site had a full medical recordssystem in place.
As soon as it became apparent that large num-bers of new patients were no longer arrivingfrom New Orleans,Trevino began to close thePMAC facility down, recognizing that, as func-tional as the facility was, it was not optimal forpatient care; however, as of this writing, the LSUfield house remains open as a special-needs shel-ter for nursing home patients.
Some disadvantagesAs a university with more than 30,000 students,LSU presents some disadvantages as a surge hos-pital site. For example, housing a medical facilityat a university can be disruptive to student life.Imagine seeing Blackhawk helicopters full ofevacuated patients landing on the quad. Secondly,sheltering sick patients and medical personnel ona university campus holds the potential for trans-mission of disease. Operationally, it is problematic
18

Surge Hospitals: Providing Safe Care in Emergencies
to expect a university to essentially shut down itseducational function and take over disaster reliefin an emergency. Other venues, such as an expo-sition center similar to the Houston Astrodomeor other multiuse facilities, can more easily cancelevents to gear up for an emergency situationwhile maintaining logistical and infrastructuresupport.
Chris Trevino, M.D., served as the primary sourceof information for this case study.
Case Study 4: Empty former retail storein Baton Rouge, Louisiana
Establishing the surge hospitalPhysicians from the University of Texas (UT)Southwestern University Hospitals took leader-ship positions in providing emergency care andmental health services in the state of Louisianaafter Hurricane Katrina struck the Gulf Coast.UT Southwestern’s Raymond Swienton, M.D.,and William M. Cassidy, M.D., associate profes-sor of medicine at Louisiana State UniversityMedical Center (LSU), chose to locate one ofthe temporary field hospitals in a building thathad formerly housed a large retail store in BatonRouge, Louisiana.They chose the site because itwas located just one half block from LSU’s EarlK. Long Medical Center and because LSU hadbeen in the process of purchasing the property,which was to be torn down to make space forthe construction of new clinics.The locationproved to be desirable in terms of managementof emergencies, medical staffing, and supplies.
Cassidy served as medical director of the facility,but he gave responsibility for the actual set up toSteven Winkler, MHA, former senior director ofrisk management at Baton Rouge GeneralMedical Center, and Monica Nijoka, MHA,BSN, R.N., former vice president of patient care
services at the same medical center.The teamfirst arrived at the site at 4:30 P.M. on Thursday,September 2, 2005. By 7:00 P.M. the next day,they were ready to provide care to patients.
The neglected site was daunting.The floor wasgreasy and layers of dust covered everything.There was virtually no lighting, the telephoneswere out of order, and only one toilet func-tioned.The inside temperature reached 100ºFahrenheit. Over 400 volunteers worked toclean the site, remove trash, fix the plumbing,and install electrical outlets and emergencypower.Winkler and Nijoka designed the layoutof the surge facility and developed a staffingplan for the professional staff.They supervisedinformation systems personnel who installed acomputer system that would allow medical staffto document information in computerizedpatient records.
At the Louisiana Department of Health andHospitals, urgent contracting deals were madewith national vendors to acquire medical sup-plies, medications, beds, and other equipment.These expensive acquisitions were neededbecause the state stockpiles had already beendeployed at the LSU campus sites. The teamobtained the rest of its materials by way ofdonations from local supply houses, physicians’offices, and hospitals. Intravenous (IV) polesnever appeared, so the staff made do by string-ing rope along the ceiling and then using metalchips to hang the intravenous bags from therope.They set up the pharmacy in the areawhere the store’s pharmacy had originally been.
Treating patientsMost patients were assessed at the centralizedtriage station at the PMAC Center on the LSUcampus and then transported to the surge hospi-tal by emergency medical services or bus.
19

Surge Hospitals: Providing Safe Care in Emergencies
Staffing at the site consisted of physicians, nurs-es, technicians, social service workers, and otherhealth care workers from local hospitals, homehealth care agencies, and physicians’ offices.Disaster medical assistance teams (DMATs) fromall parts of the U.S. also descended on the site,with particular assistance from the DMAT inIowa. Most of the professional staff worked in12-hour shifts, while nonmedical volunteers putin shifts that lasted from one to 36 hours.
Volunteer medical workers fulfilled a number ofvital roles, including nursing, pharmacy, registra-tion, central supply, social service, mental health,discharge planning, waste handling, respiratorytherapy, and food service. In addition, a numberof local restaurants, caterers, and church groupssent cooked meals to the site. Several volunteerswere dedicated to the scheduling of professionaland nonprofessional staff and also assisted in thecredentialing of the professional staff. Many localvolunteers also sorted and distributed the donat-ed clothing and toys brought to the site.
The team decided to locate the triage area inwhat had been the oil-change department insidethe store’s automotive service center because itafforded a wide space that could accommodateincoming buses and ambulances.Triage wasdivided into two areas: decontamination/securi-ty and registration/medical triage.The local firedepartment set up portable showers outside ofthe building where patients showered and weregiven clean clothing before entering the build-ing. Most of the clothing worn by patients hadto be destroyed because of contamination fromthe polluted water that had flowed into NewOrleans.After being scanned for weapons byhand-held security wands, patients proceededthrough registration and into medical triage,where physicians, nurses, and paramedics assessedtheir vital signs and general condition.The state
police, National Guard, and a private securityguard firm maintained security at the site.
The surge hospital served about 250 patientsover the course of three days. Like the otherpost-hurricane surge hospitals, this facility main-ly saw patients whose chronic conditions weremade worse by the loss of their prescribeddrugs.Although the medical staff saw some rash-es and infections from exposure to contaminatedwater, their main task was to stabilize thepatients and get them back on their prescribedmedications.The staff maintained paper recordsand computer files on all patients that includedinformation about where they were transferredor discharged.
Lessons learnedIn the confusion that occurred after HurricaneKatrina hit, communications seemed to be theweakest link at the site.The telephone systemtook a long time to be installed and cellularphones were inoperable most of the time.Whencommunications did get through, the informa-tion was often incorrect. For example, the hos-pital team was told that the location would beused heavily to free up space at the two surgefacilities set up at LSU. However, the site wasclosed after three days while the field house atthe university remained operational for weeksafter the event.Twice word came that manymore patients would soon be arriving, but addi-tional patients never arrived. In fact, the hospitalcould have handled many more patients.As aresult, the staff viewed the facility as sound butunderutilized.
Overall, the strongest factor was the spirit ofvolunteerism among the workers.When askedto perform, volunteers and local suppliers couldnot do enough, according to Winkler andNijoka. Only two suppliers refused to send
20

Surge Hospitals: Providing Safe Care in Emergencies
needed provisions, because the hospital couldnot issue purchase order numbers, and had nomeans to ensure payment.
Steven Winkler, MHA, and Monica Nijoka,MHA, BSN, R.N., served as the primary sourcesof information for this case study.
Case Study 5: A veterinary hospital inCollege Station, TexasHurricane Rita also produced an unlikely sitefor a surge facility: the Large-Animal Hospital atthe College of Veterinary Medicine andBiomedical Sciences at Texas A & M University.The university transformed the veterinary hos-pital into a special needs shelter that cared for320 patients—primarily geriatric nursing homepatients, pediatric burn victims, physically handi-capped children, and home health carepatients—from Houston and Galveston.University staff emptied the hospital of all of itsanimals (including 20 horses), then cleaned andsterilized the building and made it ready for usein less than a day under the direction of WilliamMoyer, D.V.M., head of the Department ofLarge Animal Clinical Sciences.At its peak onthe night before the hurricane hit, the facilityhoused about 650 people, including patients,families, and caregivers.The transfers of highacuity patients from less sophisticated sheltersinto this facility and free transfers back and forthbetween the surge hospital and St. JosephHospital, the largest hospital in the area, allowedSt. Joseph Hospital to never exceed 80% occu-pancy.This enabled the standard of care to bemet despite transfers of large numbers ofpatients with critical medical needs.
Paul Carlton, M.D., of the Texas A&M UniversitySystem Health Science Center (HSC), served asthe medical director of this surge hospital.Carlton, a former surgeon general of the U.S.AirForce, worked with HSC staff as well as represen-tatives of the CDC, Public Health Service, andFEMA to establish the facility.The volunteers setup the first 600 bed component before the arrivalof any outside help, and an additional 500 bedsfrom the CDC were added before the storm hit.Thus, the 1,100 bed surge facility was prepared toprovide care prior to Hurricane Rita’s assault.Thestaff included physicians, nurses, medical and vet-erinary students, and many volunteers. Only onemedical procedure had to be done, which was totreat an abscess. At one point, Evelyn Castiglioni,Ph.D., head of the university’s Department ofVeterinary Anatomy and Public Health and anaccomplished harpist, calmed patients with animpromptu concert.The hospital remained openfor six days.
Lessons learnedThe main advantage of converting veterinaryhospitals into surge hospitals is their state ofreadiness.The state-of-the-art facility was a fullyequipped hospital, so no building issues had tobe dealt with.The power system had an emer-gency generator for continuous power if com-mercial power was lost and the building wasplumbed with medical gases and suction so thatportable equipment did not have to be used.Use of this site shows that a veterinary hospitalcan be an ideal model for the surge hospital in acatastrophic situation.
21

Surge Hospitals: Providing Safe Care in Emergencies
Advance planning, coordination of resources, effective communication, and visible leadership are criticalto ensuring that surge hospitals can be set up quickly and can provide care to patients during emergen-cies. Health care organizations must prepare for the possibility that their buildings could be too damagedto function during as well as after a disaster, necessitating the use of surge hospitals—some of which mayneed to operate for months or years until permanent health care organization facilities can be rebuilt. Asthe Joint Commission considers the need for standards to ensure the quality of care being provided atsurge hospitals, health care planners at all levels must familiarize themselves with the challenges associatedwith surge hospitals and must develop thorough plans for their use in emergencies.
22
Closing Comment

References
Surge Hospitals: Providing Safe Care in Emergencies
1. Agency for Healthcare Research and Quality: Surge Capacity—Education and Training for a QualifiedWorkforce. Issue Brief No. 7, Oct. 2004. http://www.ahrq.gov/news/ulp/btbriefs/btbrief7.pdf (accessedNov. 3, 2005).
2. Romano M.:At capacity and beyond. Modern Healthcare p. 16, Sept. 2005.3. Hayes B.E., et al.:A prehospital approach to multiple-victim incidents. Ann Emerg Med 15:458–462,
Apr. 1986.4. Public Law 107–188, 107th Cong., Public Health Security and Bioterrorism Preparedness and Response Act
of 2002, Section 107.
23