
suPrAPubic Tube (sPT) PlAcemenT DurinG rObOT...
3
18 Video Article -Point of Technique ABSTRACT Robot-assisted laparoscopic prostatectomy (RALP) is a widely accepted surgery for the treatment of localized prostate cancer. The benefits of this procedure compared to open prostatectomy have been described in the literature include: decreased blood loss, shorter convalescence, earlier return of continence and improved cosmesis1-3. Overall, recovery is generally uneventful and smooth however patients do complain about discomfort secondary to their urethral catheter (UC). UC is traditionally used during the postoperative course after robot-assisted laparoscopic prostatectomy (RALP) for bladder drainage presumably to bridge the anastomotic line through cross-healing thus preventing a urethrovesical anastomotic stricture. However catheter associated discomfort, specifically meatal irritation and penile pain are common postoperative complaints expressed by the patient.4,5 The use of a percutaneous suprapubic tube (SPT) has been proposed as an alternative to a UC for postoperative drainage after RALP.6,7 Accordingly our experiences, the SPT is well tolerated by patients and associated with minimal penile pain compared to the UC. In this article, surgical technique of suprapubic tube placement (SPT) during RARP is explained. Key Words: Suprapubic tube (spt) placement, Robotic surgery, Prostate cancer, Quality of life SUPRAPUBIC TUBE (SPT) PLACEMENT TECHNIQUE Following a one-layer running urethrovesical anastomosis with a 3-0 barbed –continued suture (V-Loc TM ), bladder is filled with 300 mL of saline via the UC to inspect for possible urine leak and to distend the bladder for identification of the optimal insertion site for the SPT (Figure 1). The midline SPT placement site is identified by measur- ing a 2 centimeter distance cephalad to the pubic symphysis. Application of pressure by the bedside assistant over the potential placement site aids in the alignment of the anterior abdominal wall incision-site with the optimal bladder insertion-site. A one centimeter incision is made in the skin overlying the insertion sight and a spiked introducer (Lawrence Supra-Foley Introducer®, Utah Medical Products Inc., Midvale, UT, USA) is placed through the anterior abdominal wall under direct vision and then advances into the bladder with the assistance of the console surgeon pushing up on the distended bladder (Figure 2). The trocar is removed and through the sheath a 16 French catheter is inserted into the bladder and the balloon inflated with 10 milliliters of sterile water (Figure 3). Correspondence Address Asim Ozayar Ankara Ataturk Training and Research Hospital, Department of Urology, Bilkent, 06800 Ankara, Turkey Phone: +90 505 502 54 98 E-mail: [email protected] Received : 27 December 2015 Accepted : 28 December 2015 ROBOTICS, LAPAROSCOPY & ENDOSURGERY R o b o t i c s , L a p a r o s c o p y a n d E n d o s u r g e r y www.robotictimes.org Video of this article can be accessed on www.robotictimes.org 1 Department of Urology, Ankara Ataturk Training and Research Hospital, Ankara, Turkey 2 Department of Urology, University of Texas Southwestern Medical Center, Dallas, Texas, USA Asim Ozayar 1 , Jeffrey A. Cadeddu 2 SUPRAPUBIC TUBE (SPT) PLACEMENT DURING ROBOT-ASSISTED LAPAROSCOPIC PROSTATECTOMY
Transcript of suPrAPubic Tube (sPT) PlAcemenT DurinG rObOT...

18
Vid
eo A
rtic
le -P
oin
t of
Tech
niq
ue
AbsTrAcTRobot-assisted laparoscopic prostatectomy (RALP) is a widely accepted surgery for the treatment of localized prostate cancer. The benefits of this procedure compared to open prostatectomy have been described in the literature include: decreased blood loss, shorter convalescence, earlier return of continence and improved cosmesis1-3. Overall, recovery is generally uneventful and smooth however patients do complain about discomfort secondary to their urethral catheter (UC).
UC is traditionally used during the postoperative course after robot-assisted laparoscopic prostatectomy (RALP) for bladder drainage presumably to bridge the anastomotic line through cross-healing thus preventing a urethrovesical anastomotic stricture. However catheter associated discomfort, specifically meatal irritation and penile pain are common postoperative complaints expressed by the patient.4,5 The use of a percutaneous suprapubic tube (SPT) has been proposed as an alternative to a UC for postoperative drainage after RALP.6,7 Accordingly our experiences, the SPT is well tolerated by patients and associated with minimal penile pain compared to the UC.
In this article, surgical technique of suprapubic tube placement (SPT) during RARP is explained.
Key Words: Suprapubic tube (spt) placement, Robotic surgery, Prostate cancer, Quality of life
suPrAPubic Tube (sPT) PlAcemenT Technique
Following a one-layer running urethrovesical anastomosis with a 3-0 barbed –continued suture (V-LocTM), bladder is filled with 300 mL of saline via the UC to inspect for possible urine leak and to distend the bladder for identification of the optimal insertion site for the SPT (Figure 1).
The midline SPT placement site is identified by measur-ing a 2 centimeter distance cephalad to the pubic symphysis. Application of pressure by the bedside assistant over the potential placement site aids in the
alignment of the anterior abdominal wall incision-site with the optimal bladder insertion-site. A one centimeter incision is made in the skin overlying the insertion sight and a spiked introducer (Lawrence Supra-Foley Introducer®, Utah Medical Products Inc., Midvale, UT, USA) is placed through the anterior abdominal wall under direct vision and then advances into the bladder with the assistance of the console surgeon pushing up on the distended bladder (Figure 2).
The trocar is removed and through the sheath a 16 French catheter is inserted into the bladder and the balloon inflated with 10 milliliters of sterile water (Figure 3).
Correspondence Address
Asim Ozayar
Ankara Ataturk Training and Research Hospital, Department of Urology, Bilkent, 06800 Ankara, Turkey
Phone: +90 505 502 54 98 E-mail: [email protected]
Received : 27 December 2015Accepted : 28 December 2015
Robotics, LapaRoscopy & EndosuRgERyRobo
tics,
Laparoscopy and Endosurgery
www.robotictimes.org
Video of this article can be accessed on www.robotictimes.org
1 Department of Urology, Ankara Ataturk Training and Research Hospital, Ankara, Turkey2 Department of Urology, University of Texas Southwestern Medical Center, Dallas, Texas, USA
Asim Ozayar1, Jeffrey A. Cadeddu2
suPrAPubic Tube (sPT) PlAcemenT DurinG rObOT-AssisTeD lAPArOscOPic PrOsTATecTOmY
19Robotics, Lap and Endosurg 2(1): 18-20, 2016
Suprapubic Tube (SPT) Placement During Robot-Assisted Laparoscopic Prostatectomy
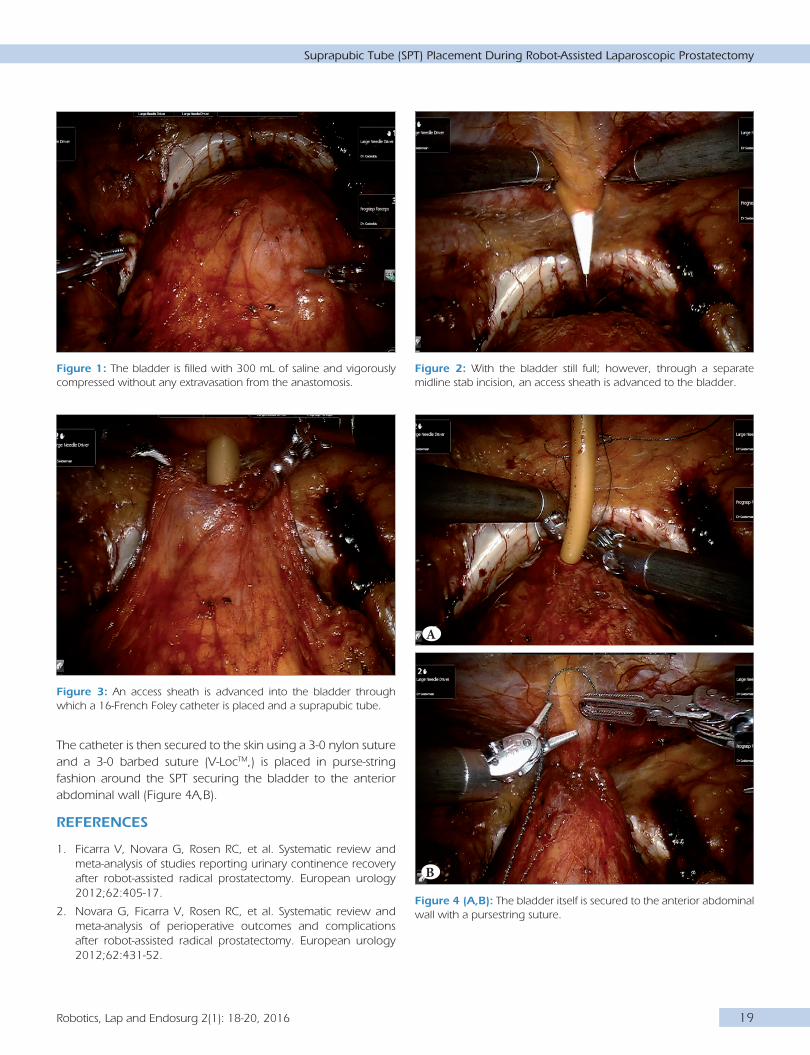
The catheter is then secured to the skin using a 3-0 nylon suture and a 3-0 barbed suture (V-LocTM,) is placed in purse-string fashion around the SPT securing the bladder to the anterior abdominal wall (Figure 4A,B).
references
1. Ficarra V, Novara G, Rosen RC, et al. Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. European urology 2012;62:405-17.
2. Novara G, Ficarra V, Rosen RC, et al. Systematic review and meta-analysis of perioperative outcomes and complications after robot-assisted radical prostatectomy. European urology 2012;62:431-52.
figure 4 (A,b): The bladder itself is secured to the anterior abdominal wall with a pursestring suture.
figure 1: The bladder is filled with 300 mL of saline and vigorously compressed without any extravasation from the anastomosis.
figure 3: An access sheath is advanced into the bladder through which a 16-French Foley catheter is placed and a suprapubic tube.
figure 2: With the bladder still full; however, through a separate midline stab incision, an access sheath is advanced to the bladder.
A
B

20 Robotics, Lap and Endosurg 2(1): 18-20, 2016
Ozayar A and Cadeddu JA
3. Trinh QD, Sammon J, Sun M, et al. Perioperative outcomes of robot-assisted radical prostatectomy compared with open radical prostatectomy: results from the nationwide inpatient sample. European urology 2012;61:679-85.
4. Lepor H, Nieder AM, Fraiman MC. Early removal of urinary catheter after radical retropubic prostatectomy is both feasible and desirable. Urology 2001;58:425-9.
5. Woldu SL, Weinberg AC, Bergman A, et al. Pain and analgesic use after robot-assisted radical prostatectomy. Journal of endourology / Endourological Society 2014;28:544-8.
6. Krane LS, Bhandari M, Peabody JO, Menon M. Impact of percutaneous suprapubic tube drainage on patient discomfort after radical prostatectomy. European urology 2009;56:325-30.
7. Sammon JD, Trinh QD, Sukumar S, et al. Long-term follow-up of patients undergoing percutaneous suprapubic tube drainage after robot-assisted radical prostatectomy (RARP). BJU Int 2012;110:580-5.


















