
Supplemental Figure 1. Erlotinib does not alter oxygenation of tumors. Tumor pO 2 was measured by...
7
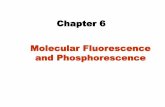
0 10 20 30 40 50 60 0 2 4 6 8 10 12 14 16 Erl 1 Erl 2 Time after erlotinib administration (h) pO2 (mmHg) Supplemental Figure 1. Erlotinib does not alter oxygenation of tumors. Tumor pO 2 was measured by phosphorescence lifetime oximetry at times before erlotinib administration (0h), then at 24h, 48h, and 51h post-erlotinib administration. These timepoints were evaluated because they follow the dosing schedule used for the combination erlotinib/PDT regimen under investigation. Plots represent individual animals. No significant alterations in pO 2 levels were observed at any timepoint post-erlotinib administration.
-
Upload
gordon-nelson -
Category
Documents
-
view
213 -
download
1
Transcript of Supplemental Figure 1. Erlotinib does not alter oxygenation of tumors. Tumor pO 2 was measured by...

0 10 20 30 40 50 600
2
4
6
8
10
12
14
16
Erl 1Erl 2Erl 3
Time after erlotinib administration (h)
pO2
(mm
Hg)
Supplemental Figure 1. Erlotinib does not alter oxygenation of tumors. Tumor pO2 was measured by phosphorescence lifetime oximetry at times before erlotinib administration (0h), then at 24h, 48h, and 51h post-erlotinib administration. These timepoints were evaluated because they follow the dosing schedule used for the combination erlotinib/PDT regimen under investigation. Plots represent individual animals. No significant alterations in pO2 levels were observed at any timepoint post-erlotinib administration.

#
Ctrl
PDT
Ctrl
_x0004_Live Apoptotic
Necrotic0
20
40
60
80
100
120 (-) Erl (+) Erl (ctrl)
1h PDT 1h PDT + Erl
18h PDT 18h PDT + Erl
% T
otal
cells
in p
aren
t pop
ulati
on
Live Apoptotic Necrotic
* *
*
Supplemental Figure 2. Erlotinib increases in vivo tumor cell death at delayed timepoints. In vivo H460 viability, and the presence of necrosis and apoptosis, assessed by flow cytometry (n=4-6). *p<0.05 compared to untreated, #p<0.05 for erlotinib/PDT vs. PDT.

Ctrl
PDT
Ctrl0 0.5 1 1.5 2 2.50
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Ex v
ivo
imag
ing
(FI/
unit
area
)
In vivo imaging (FI/unit area)
r=0.99
Supplemental Figure 3. In vivo imaging of tumor perfusion is well correlated with ex vivo imaging of the excised tumor. In H460 tumors, in vivo imaging of IRDye®800-PEG uptake was compared to images of the same tumors that were taken after their excision. Data are plotted as the average fluorescence (FI) per unit area of the region of interest (ROI). ROI was customized to the dimensions of the tumor for both the in vivo and the ex vivo images.

Ctrl
PDT
Ctrl
10
1
2
3
4
5
6
7
8
9 (-) Erlotinib(+) Erlotinib
hVEG
F (fo
ld ch
ange
vs.
untr
eate
d)
Supplemental Figure 4. VEGF levels decrease in A549 tumors with pre-PDT administration of erlotinib. Relative concentrations of tumor-localized human VEGF (hVEGF) in A549 tumors at 18h after treatment with PDT compared to treatment with erlotinib/PDT (n=6).
BPD-PDT

Ctrl
PDT
Ctrl
Blot:
EGFR
Actin
SVEC A549 H460
Supplemental Figure 5. Western blot analysis shows that EGFR is expressed in each of the cell lines studied. β-actin serves as the internal loading control. SVEC, mouse endothelial cell line; H460/A549, human non-small cell lung carcinoma cell lines.

Ctrl
PDT
Ctrl
Tumor Flank0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8(-) Erlotinib(+) Erlotinib
BPD
Inte
nsity
(FI/u
nit a
rea)
Supplemental Figure 6. BPD levels increase in A549 tumors after Erlotinib administration. In vivo imaging of BPD uptake after triple-dose erlotinib regimen compared to untreated (n=4).

Ctrl
PDT
1 20.010
0.100
1.000
(-) Erlotinib(+) Erlotinib
Surv
ivin
g Fr
actio
n
Controls BPD-PDT
* * #
Supplemental Figure 7. A single-dose of erlotinib augments PDT-induced cytotoxicity. Control conditions indicate the surviving fraction of SVEC endothelial cells that were unilluminated and untreated with erlotinib, or unilluminated and exposed to erlotinib. In parallel, cells that were or were not exposed to erlotinib were treated with 0.8 J/cm2 of BPD-PDT. Surviving fractions are calculated relative to untreated controls (no illumination or erlotinib). Erlotinib incubation was over the 3 hours prior to PDT (simultaneous with incubation in BPD). By paired t-test, *p<0.05 compared to untreated, #p<0.05 for erlotinib/PDT vs. PDT.




![Development of [ C]erlotinib Positron Emission Tomography ...clincancerres.aacrjournals.org/content/clincanres/19/1/183.full.pdf · Imaging, Diagnosis, Prognosis Development of [11C]erlotinib](https://static.fdocuments.in/doc/165x107/5a9efa4b7f8b9a8e178c2b60/development-of-cerlotinib-positron-emission-tomography-diagnosis-prognosis.jpg)












