
Supervision, Performance Assessment and Recognition ...
55
i Supervision, Performance Assessment and Recognition Strategy (SPARS) Implementation Guidelines Produced by: Pharmacy Department Ministry of Health Government of Uganda August, 2017
Transcript of Supervision, Performance Assessment and Recognition ...

i
Supervision, Performance Assessment and
Recognition Strategy
(SPARS)
Implementation Guidelines
Produced by: Pharmacy Department
Ministry of Health
Government of Uganda
August, 2017

ii
PREFACE
In 2011, SPARS was adopted by the Ministry of Health (MoH) as a
national strategy to build district level capacity in supply chain
management of medicines and health supplies. Medicines and health
supplies are the second biggest expenditure in the health sector after
human resources and therefore their management is critical in ensuring
effective health service delivery. Experience from the last five years has
shown that the Supervision, Performance, Assessment and Recognition
Strategy (SPARS) can effectively improve facility performance in
managing their essential medicines and health supplies through
sustainably building the health worker skills, knowledge, attitudes, and
practices.
The purpose of these guidelines is to provide district health teams,
implementing partners and donor agencies with a reference manual on
what it takes to comprehensively implement SPARS. The MoH
Pharmacy Department spearheaded development of these guidelines to
facilitate the planning, maintenance of SPARS implementation and to
ensure a quality, standardized approach in implementing this important
district-level capacity building initiative.
I hope you will find these guidelines useful to implement SPARS and to
ensure uniformity in the implementation. Strengthened medicines
management practices in all districts and in all government and private
not for profit health facilities is critical to ensure optimal use of limited
resources and to ensure good health care provision to all people of
Uganda. Implementation of SPARS has proven to make a difference and
with your support we can ensure national coverage.
Morries Seru
Ag. ACHS- Pharmacy
Ministry of Health

iii
ACKNOWLEDGEMENT
The Ministry of Health wishes to thank the following individuals from
the Pharmacy Department and the USAID-supported Uganda Health
Supply Chain (UHSC) project for their invaluable support and
participation in developing these guidelines:
Name Organization
Morries Seru Pharmacy Department
Thomas Obua Pharmacy Department
Dr. Birna Trap Management Sciences for Health, UHSC
Martin Oteba Olowo Management Sciences for Health, UHSC
Denis Okidi Ladwar Management Sciences for Health, UHSC

iv
PREFACE ....................................................................................... i
ACKNOWLEDGEMENT ........................................................... iii
LIST OF ABBREVIATIONS ...................................................... v
BACKGROUND ........................................................................... 1
THE SPARS CONCEPT .............................................................. 2
PURPOSE OF THE GUIDELINES ............................................ 7
SPARS IMPLEMENTATION ..................................................... 7
1. Initial planning with districts .................................................................. 7
2. Selection of Medicines Management Supervisors ................................. 8
3. Roles of SPARS stakeholders ................................................................ 9
4. MMS training and skills development ................................................. 14
5. SPARS performance management ....................................................... 18 6. SPARS data submission and Pharmaceutical Information Portal ........ 21
7. Mitigation of Fraud .............................................................................. 21
8. Good Pharmacy Practice (GPP) certification ....................................... 22
COST OF SPARS IMPLEMENTATION ................................ 23
ANNEX 1: SPARS PERFORMANCE MANAGEMENT
INDICATORS ................................................................................ I
ANNEX 3: MMS MOTORCYCLE AND ACCESSORIES
SPECIFICATIONS ........................................................................ I
ANNEX 4: MMS LAPTOP SPECIFICATIONS ........................ I
ANNEX 5: SHELVE SPECIFICATIONS ................................... I
ANNEX 6: SPARS RECOGNITION SCHEME ...................... IV
a) DHO/ CAO Recognition Scheme......................................................... IV
b) Regional Pharmacist (RP) - Recognition Scheme ................................. V
c) District Medicines Management Supervisors Recognition Scheme ..... VI
d) HSD Medicines Management Supervisors Recognition Scheme ...... VIII
e) Health Facilities Recognition Scheme .................................................. X
TABLE OF CONTENTS

v
LIST OF ABBREVIATIONS
ART Anti- Retroviral Therapy
EMHS Essential Medicines and Health Supplies
Management
HSD Health Sub District
MB Medical Bureau
MMS Medicines Management Supervisor
PFM Pharmaceutical Financial Management
PNFP Private Not for Profit
SPARS Supervision Performance Assessment and
Recognition Strategy
USAID United States Agency for International
Development
1
BACKGROUND
Ensuring the adequate availability and appropriate use of essential
medicines and health supplies (EMHS) is critically important to the
health of the Ugandan people. The Ministry of Health has
prioritized the building of the capacity of health workers in
medicines management as a key strategy to optimize the use of
limited resources, reduce waste and improve health outcomes at all
levels of health care.
Over the past 10 to 15 years, thousands of health facility managers
and other staff have received training on various aspects of supply
chain management of EMHS. However, the change in behavior and
effect was minimal and not sustainable. As a result, the health
sector continued to experience challenges in; quantification
practices, stock and storage management, logistics reporting,
prescribing and dispensing of medicines.
To address these challenges, the Ministry of Health Pharmacy
Department, in collaboration with its partners, developed the
Supervision, Performance Assessment, and Recognition Strategy
(SPARS) to build sustainable EMHS management capacity in
public and private-not-for-profit health facilities throughout the
country. SPARS is a multi-pronged intervention strategy that
combines supervision, on-the-job training and provision of tools
and guidelines with structured performance assessments to identify
and prioritize problems and measure progress with recognition for
improved performance linked to certification for Good Pharmacy
Practices.
SPARS is critically important not only in building the knowledge,
skills and practices of health facility staff, but also for improving
the use of data for decision-making at all levels which is essential
for optimal performance and decision making of the national
supply chain system.

2
THE SPARS CONCEPT
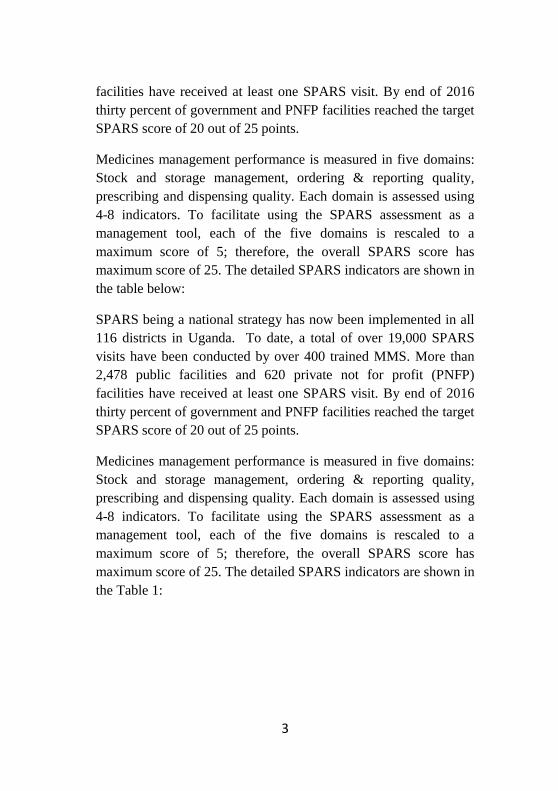
SPARS is based on the best practice of combining different
interventions to increase the likelihood of positive change. The
strategy combines educational, managerial, regulatory, and
recognition interventions with performance assessment to improve
medicines management practices at health facility level. The
education intervention is provided by supervisors who are trained
district staff, called Medicines Management Supervisors (MMS),
providing on-the-job supervision, coaching and mentoring of health
workers. The managerial intervention is the provision of manuals,
guidelines and tools needed to standardize practices and
procedures; and the regulatory intervention is that SPARS prepares
facilities to attain the National Drug Authority’s certification for
Good Pharmacy Practices. Facility performance is assessed by the
MMS through the measurement of 26 medicines management
indicators at each supervisory visit; the results (scores) guide
facility staff on where they need to strengthen their performance
and are used by MMS and District Health Office to target their
support to the facility1. The performance and agreed next steps are
recorded in the supervisory book kept at the facility. The
multipronged SPARS approach is illustrated in Figure 1.
SPARS being a national strategy has now been implemented in all
116 districts in Uganda. To date, a total of over 19,000 SPARS
visits have been conducted by over 400 trained MMS. More than
2,478 public facilities and 620 private not for profit (PNFP)
1 Trap et al (2016). Article 1: Supervision, Performance Assessment, and
Recognition Strategy (SPARS) - a multipronged intervention strategy for strengthening medicines management in Uganda: method presentation and facility performance at baseline. Journal of Pharmaceutical Policy and Practice 9:21
3
facilities have received at least one SPARS visit. By end of 2016
thirty percent of government and PNFP facilities reached the target
SPARS score of 20 out of 25 points.
Medicines management performance is measured in five domains:
Stock and storage management, ordering & reporting quality,
prescribing and dispensing quality. Each domain is assessed using
4-8 indicators. To facilitate using the SPARS assessment as a
management tool, each of the five domains is rescaled to a
maximum score of 5; therefore, the overall SPARS score has
maximum score of 25. The detailed SPARS indicators are shown in
the table below:
SPARS being a national strategy has now been implemented in all
116 districts in Uganda. To date, a total of over 19,000 SPARS
visits have been conducted by over 400 trained MMS. More than
2,478 public facilities and 620 private not for profit (PNFP)
facilities have received at least one SPARS visit. By end of 2016
thirty percent of government and PNFP facilities reached the target
SPARS score of 20 out of 25 points.
Medicines management performance is measured in five domains:
Stock and storage management, ordering & reporting quality,
prescribing and dispensing quality. Each domain is assessed using
4-8 indicators. To facilitate using the SPARS assessment as a
management tool, each of the five domains is rescaled to a
maximum score of 5; therefore, the overall SPARS score has
maximum score of 25. The detailed SPARS indicators are shown in
the Table 1:

4
Figure 1: SPARS intervention elements

5
Table 1: SPARS indicators
Dispensing quality (8) Storage management (6)
1. Dispensing time 2. Packaging material 3. Dispensing equipment 4. Availability of reference materials 5. Services available at the dispensing
area 6. Patient care 7. Labelling 8. Correct filling of dispensing log
18. Cleanliness of the pharmacy & store
19. Hygiene of the pharmacy
20. System for storage of medicines & health supplies
21. Storage conditions
22. Storage practices of medicines
23. One facility-One store-One stock card
Prescribing quality (4) Ordering and reporting quality (3)
9. Rational prescribing 10. Diarrhea 11. Non-pneumonia cough/cold 12. Malaria management
24. Timelines of order and distribution
25. Completeness and accuracy of HMIS105 report
26. Filing
Stock Management (5)
13. Stock card availability 14. Correct filling of stock card 15. Does physical count agree with stock card balance? 16. Is stock book correctly used? 17. Is the calculated Average Monthly Calculation the same as the recorded? ±10%

6
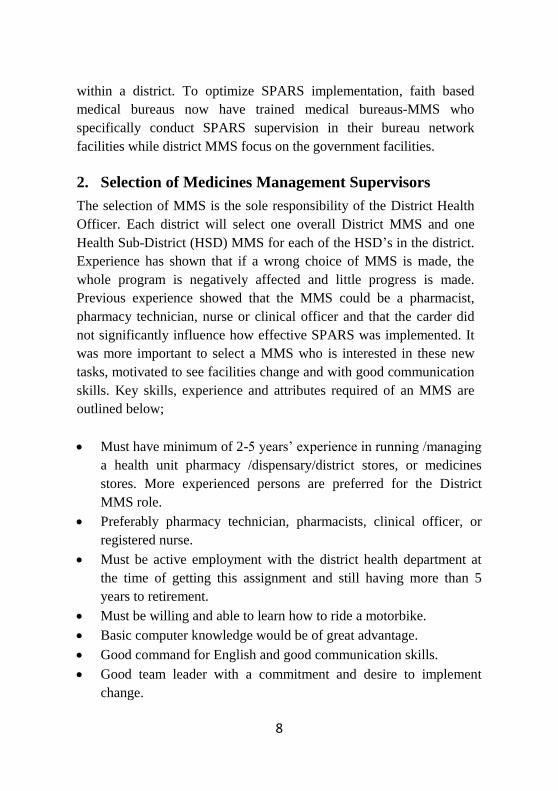
Through SPARS significant improvements are seen in all five domains
of medicines management and in all the indicators. Strongest impact
being at lower level facilities and in the dispensing and prescribing
areas. At the facilities, MMS summarize facility performance in a spider
graph depicting the five domains. The national performance spider
graph as of May 2017 is as shown in figure 2 below.
Figure 2: Impact of SPARS visits depicted in the five
domains of medicines management in Uganda as at May
2017
SPARS visits
Visit 1 Visit 3 Visit 5 Visit Last
Average total SPARS score
11.1 16.3 18.6 19.2

7
PURPOSE OF THE GUIDELINES
Based on the documented effectiveness in improving medicines
management the SPARS strategy was adopted as a national strategy in
2011. These guidelines provides a step by step guide to implementing
partners, district health teams and donor agencies on how to
comprehensively implement SPARS. The guidelines also provides a
detail description of key activities and the costs involved to enable
effective operational planning and budgeting for SPARS
implementation.
SPARS IMPLEMENTATION
The following are key steps for effective implementation of SPARS by
implementing partners.
1. Initial planning with districts
SPARS implementation requires initial planning between
implementing partners and districts to clarify on the roles and
responsibilities of all parties involved. The parties usually include the
District Health Officer and other District Health Team members, the
Chief Administrative Officer, as well as MMS. MMS are District
health staff who are nominated by the District Health Officer to take
on additional responsibility of medicines management supervision and
coordination. For nominated MMS to take on their new role and
responsibilities it is recommended they undergo a two week
examinable MMS training course and be certified as an MMS. The
initial planning stage involves the Implementing Partner agreeing with
Pharmacy Department on specific districts of coverage and SPARS
performance targets. A letter of intent between the District and the
Implementing Partner can then be drawn up with detailed roles and
responsibilities to support SPARS implementation. The district health
system benefits most if SPARS is implemented in all health facilities
8
within a district. To optimize SPARS implementation, faith based
medical bureaus now have trained medical bureaus-MMS who
specifically conduct SPARS supervision in their bureau network
facilities while district MMS focus on the government facilities.
2. Selection of Medicines Management Supervisors
The selection of MMS is the sole responsibility of the District Health
Officer. Each district will select one overall District MMS and one
Health Sub-District (HSD) MMS for each of the HSD’s in the district.
Experience has shown that if a wrong choice of MMS is made, the
whole program is negatively affected and little progress is made.
Previous experience showed that the MMS could be a pharmacist,
pharmacy technician, nurse or clinical officer and that the carder did
not significantly influence how effective SPARS was implemented. It
was more important to select a MMS who is interested in these new
tasks, motivated to see facilities change and with good communication
skills. Key skills, experience and attributes required of an MMS are
outlined below;
Must have minimum of 2-5 years’ experience in running /managing
a health unit pharmacy /dispensary/district stores, or medicines
stores. More experienced persons are preferred for the District
MMS role.
Preferably pharmacy technician, pharmacists, clinical officer, or
registered nurse.
Must be active employment with the district health department at
the time of getting this assignment and still having more than 5
years to retirement.
Must be willing and able to learn how to ride a motorbike.
Basic computer knowledge would be of great advantage.
Good command for English and good communication skills.
Good team leader with a commitment and desire to implement
change.
9
Should be able to pass the MMS exams assessing skills in stock
management, stores management, ordering/reporting, rational
prescribing and dispensing, supervision, communication and
performance assessment.
Should be able to allocate at least 5 days per month for medicines
management supervision activities. The DHO may need to relieve
selected MMS of additional assignments and responsibilities to
ensure they have time for medicines management activities
3. Roles of SPARS stakeholders
SPARS has a wide range of stakeholder from the Ministry of Health
Pharmacy Department to the health facilities. Key responsibilities of
these stakeholders in SPARS implementation are outlined below;
i) MoH Pharmacy Department
Strategic leadership, policy and guidelines formulation, oversight
and coordination to ensure effective and uniform SPARS
implementation and sustainability.
Monitoring, evaluation, tracking and reporting of SPARS
implementation, performance, efficiency and effectiveness at
facility level and by MMS’, districts and Implementing Partners.
Targeted support supervision to identified weak performers to
facilitate SPARS implementation, identify issues and take
necessary corrective actions.
Resource mobilization for supporting gaps identified by SPARS,
Good Pharmacy Practices and supportive supervision such as
appropriate medicines storage infrastructure including cold storage
facilities.
Host and maintain the Pharmaceutical Information Portal in close
collaboration with the Ministry of Health Department of Health
Informatics, optimize data quality and data utilization

10
ii) Regional Pharmacist
Coordinate medicine management activities within a region with
districts and implementing partners
Performance management of SPARS and medicines management
implementation in their region
Capacity building support to MMS in their regions including peer
support to MMS at poor performing facilities.
Regular reporting to Ministry of Heath Pharmacy Department on
medicines situation in their regions and facilities.

11
iii) Implementing partners
Support and manage comprehensive SPARS implementation to all
facilities in supported districts.
Implement and support activities necessary for SPARS set up and
implementation at district level including training of MMS’s in
SPARS, supportive supervision, computer skills information use
and defensive driving.
Support implementation of the recognition scheme and provision of
HMIS tool and equipment to District Health Officers, MMS and
health facilities in supported districts when feasible and doable.
iv) Chief Administrative Officer
Approve assignment of responsibility to district staff nominated as
MMS by the District Health Officer
Maintain custody and ensure proper use and repair of equipment
provided to districts in support of SPARS implementation like;
computers, motorbikes; modems; shelves etc.
Participate in SPARS joint support supervision with implementing
partners.
v) District Health Officer/ District Health Team
Nomination of district staff for assignment of responsibility as
MMS.
Overall supervision and management responsibility for medicines
management activities in the district.
Assess medicines management performance, manage and support
MMS and health facilities EMHS management.
Coordination with higher level Ministry of Health on medicines
management issues.
Participate in the peer support supervision of poor performing
MMS and health facilities.

12
Manage district logistics coordination meetings.
Progress reporting to the district Chief Administrative Officer on
medicines management in the district.
vi) District Medicines Management Supervisors
The District-MMS is the focal person for all medicines management
and logistic activities in the district and will be responsible for SPARS
planning, implementation, reporting and use of information for decision
making. The District-MMS has the following specific roles in SPARS
implementation;
Coordination of medicines management activities within the district
and with regional pharmacists
Focal person for medicines issues within the District Health Team
Work closely with district technical programs officers and focal
persons to ensure coordination of efforts to improve availability of
EMHS.
Coordination, mentorship and supervision of HSD-MMS’s and MB
MMS to improve SPARS implementation and strengthen data
quality.
Coordinate development and management of district medicines
management work plans.
Monthly reporting on medicines situation in the district to the
District Health Officer.
Participate in joint support supervisions with the regional
Pharmacist, & District Health Officer.
Implement SPARS at higher level health facilities.
Coordinate and support other activities such as pharmaceutical
financial management, ART-logistics management supervision and
medicines and therapeutic committees It’s expected that the District
MMS conducts at least 6 supervisions per quarter either to facilities
or to supervise the HSD-MMSs or MB-MMS.
Support district logistics coordination meetings.

13
vii) HSD Medicines Management Supervisors
The HSD MMS on the hand is responsible for medicines management
activities within his designated HSD. The HSD MMS supports the
District MMS in planning and implementation of medicines
management activities within the HSD. The HSD-MMS has the
following specific roles in SPARS implementation;
Responsible for overall SPARS implementation, performance
management and reporting in the HSD of responsibility
Implement SPARS at lower level health facilities in the HSD of
responsibility.
Implement other logistic or medicines management interventions in
the HSD such as pharmaceutical financial management, ART
logistics supervision and Web-based ordering and reporting.
It’s expected that the HSD MMS conducts at least 6 supervisions to
facilities per quarter.
Monthly reporting on medicines situation in the HSD to District-
MMS and the District Health Officer.
Participate in joint support supervisions activities with the District
MMS
Participates in district logistics coordination meetings.
viii) Medical Bureau Medicines Management Supervisors
MB MMS implement medicines management activities within the
network of PNFP facilities. MB MMS are nominated and supported by
the four faith based medical bureaus of: Catholics, Muslims,
Protestants and Orthodox. The MB MMS support facilities across
several districts but report directly to the District MMS in each district.
MB-MMS have the following specific roles in SPARS
implementation;
Act as district focal point for all matters pertaining to medicines in
the district for specific MB PNFP health facilities

14
Develop and manage diocese/ regional medicines management
work plans for PNFP facilities under their responsibility.
Supervision of MB PNFP health facilities in the district in SPARS,
Pharmaceutical Financial Management, ART Test Treat and Track
supervision and other medicines management activities. It’s
expected that the MB MMS also conducts at least 6 supervisions
per quarter to facilities.
Monthly reporting on medicines situation in PNFP facilities to
District MMS and the District Health Officer.
Participate in joint support supervisions activities with the District
MMS.
Participate in district logistics coordination meetings.
ix) Health facility in charge and staff
Identify areas of improvement after each support supervision and
agree on a facility improvement plan by the next visit with the
MMS.
Monitor and track improvements in medicines management.
Use performance information for decision making to improve
practices at facility level.
Regular reporting to the District Health Officer and MMS on
medicines management issues.
Involve all available logistic staff and the In-charge in the
debriefing of SPARS visits.
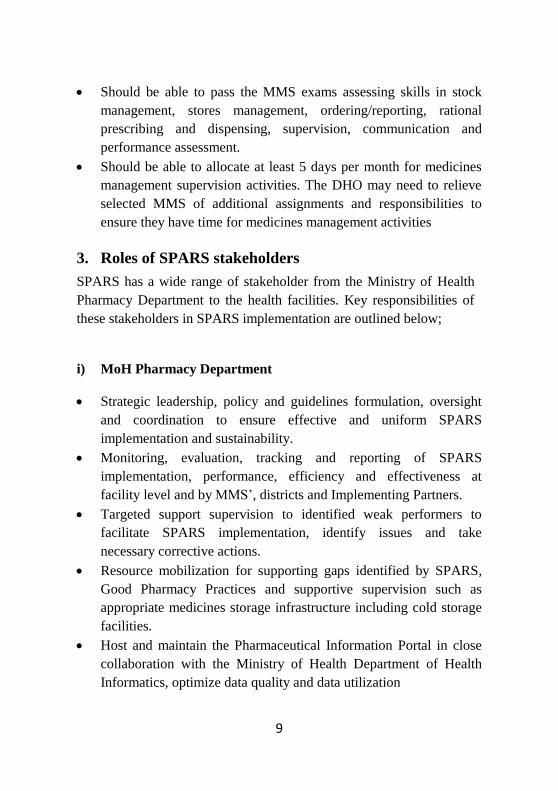
4. MMS training and skills development
All selected MMS must complete a series of training and mentorship
sessions spread out over a period of time that build on each other to
allow efficient and effective SPARS implementation as illustrated in
the diagram below:
15
Figure 3: Capacity building of MMS for SPARS implementation
1. Two week examinable
MMS training course
4. One week examinable defensive
driving course and driving license
test
2. Five day practical field
orientation in SPARS
supervision
5. Regular SPARS facility visits by
MMS
3. Three day computer
training course
6. Five day supportive supervision
training course and other follow up
trainings

16
i) MMS training course
Nominated MMS begin their capacity building by undertaking a 2
week MMS training course conducted by Makerere University,
Pharmacy Department. The course covers a wide range of topics
including; managing medicines, problem solving, communication and
how to mentor health workers and assess performance using the
indicator based SPARS tool. Participants have to pass an exam to
qualify to be a certified MMS. The MMS training course is organized
in close collaboration between the Implementing Partners Ministry of
Health, Pharmacy Department and Makerere University and funded by
the Implementing Partners.
ii) SPARS supervision practical field orientation
Certified MMS receive a 5 days practical field orientation by
experienced MMS or Implementing Partner staff. The focus of this
practical orientation is to mentor and demonstrated data collection
using the indicator based SPARS tool clarifying indicators, hands-on
problem identification, prioritization and improvement planning.
iii) Computer training course
In this course the MMS are provided a netbook to enter the findings
from the SPARS performance assessment and they receive three days
of training in the use of the netbook, entering SPARS performance
data, submitting the data into the pharmaceutical information portal,
and generating SPARS reports. To increase their computer skills, the
MMS’s are provided with flash drives with self-paced learning aids
about various software packages and other technologies2. MMS are
required to undertake certified courses to improve their skills in use of
MS Office Package applications like MS Office and Excel, use of
2 GCFLearnFree.org [Internet]. [Cited 2017 April 8]. Available from:
http://www.gcflearnfree.org/

17
internet and email. The specification for the netbook is attached in
annex 4.
iv) Defensive motorcycle riding course
To facilitate MMS travel to facilities, which are often in rural areas
with uneven dirt roads, they receive 4 stroke motorbikes of 100-125cc,
riding gear (riding boots, jacket, pants and gloves), defensive riding
training, and an examination in motorcycle riding certified by the
Police inspector of vehicles. The defensive riding course is a 6 day
training course. The training mainly covers basic mechanical
maintenance, tactical riding, road safety awareness, off road driving
and defensive driving. Various private firms have the expertise to
deliver defensive motorcycle ridings training. Implementing partners
have usually been the source of funding for the defensive riding
training as well as provision of riding accessories. Once the MMS pass
their defensive riding exam, they are supported to obtain riding
permits which is a requirement for riding motorcycles in Uganda.
Implementing Partners have also had the responsibility of ensuring the
motorcycles provided to the districts are appropriately insured,
serviced and repaired in collaboration with the District Health office.
The specification for the motor bike is attached in annex 3.
v) Supportive supervision training
Applying supportive supervision in contrast to ordinary police-like
supervision is likely to increase SPARS effectiveness. To build
supportive supervision skills the MMS might also be offered a five day
interactive training course conducted by Makerere University focusing
on effective communication, problem identification, data
interpretation, target setting and constructive feedback. The training
utilizes video education as a learning tool where participants appraise
videos of their role plays before and after the supportive supervision
training learning sessions.

18
5. SPARS performance management
Once MMS pass their defensive riding exam, they are ready to provide
regularly SPARS visits to facilities. MMS are expected to supervise
facilities every 60 days till supervision visit 5 and thereafter every 120
days to sustain performance achieved. MMS collect and submit
performance data at each SPARS visit. At minimum MMS should at
least conduct 6 supervisions per quarter.
After a facility has improved and is scoring highly (Usually over 18)
there is normally stagnation in scores. Infrastructural indicators
requiring construction are usually responsible for the stagnation as
they are difficult to change. During this period it’s recommended that
MMS visit the facility less often (2-3 times a year) to sustain SPARS
performance. After the initial five visits the MMS roles should be
refocused to specific logistics challenges that may still be persisting
like ART logistics, stock book use, TB commodity management,
pharmaceutical financial management etc.
In a SPARS longitudinal study that was implemented in 45 out of 112
districts from 2010 to 2013 and included over 6264 SPARS visits, we
found great variation between the SPARS score improvements per visit,
between the annual number of visits implemented by an MMS and days
between SPARS visits to a facility. Based on analysis of the SPARS
implementation data including only the first year and a maximum of the
first five visits to a facility the average improvement in the SPARS
score per visit to a health facility was to 2.3 (-10.7 to 13.9) and the
associated average percentage change in the SPARS score for each visit
23%. We found that a facility on average received a visit every 100
days with a median duration 89 days with an Interquartile range of 61-

19
133 days and that MMS on average annually implemented 28 (2-57)
supervision visits3.
SPARS performance management is monitored in terms of efficiency
and effectiveness. SPARS efficiency refers to number of visits
implemented by the MMS per month and SPARS effectiveness
measure of improvements or impact in SPARS score per visit at
facility level. It’s recommended that each SPARS visit achieves an
improvement of at least 2 score points for the first five visits to the
facility.
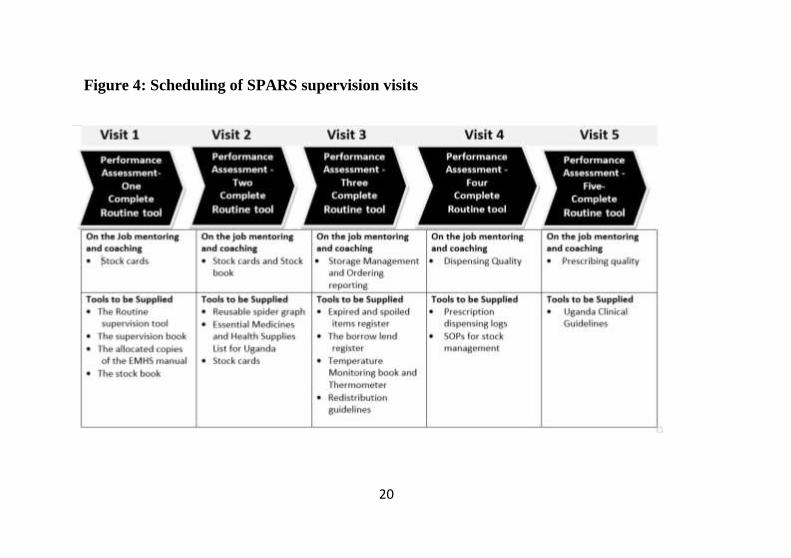
For better impact it’s recommended that MMS focus their mentorships
over five supervisions in specific domains. Recommended focus
domains of SPARS from visit 1 to 5 is outlined below.
3 Trap et al (unpublished).Supervision Performance Assessment and
Recognition Strategy to improve medicines management in Ugandan health
facilities - national longitudinal study.
20
Figure 4: Scheduling of SPARS supervision visits

21
6. SPARS data submission and Pharmaceutical
Information Portal
All SPARS data is submitted to the Pharmaceutical Information Portal
(PIP). The PIP has inbuilt validations that ensure submitted data is
complete and accurate. No SPARS data will be submitted until it
conforms to the data quality requirements of completeness and
accuracy. For example any unfilled mandatory field in the electronic
SPARS tool will prevent the form from being submitted. The PIP also
validates for the interval between the current visit and the last submitted
visit to ensure it conforms to recommended intervals. The current (most
updated) SPARS supervision tool can be obtained from Ministry of
Health Pharmacy Department or online from the PIP at
https://pip.nhdb.ug/. Access permission to the PIP can be obtained from
the Ministry of Health Pharmacy Department who can also in
collaboration with the IP or other interested parties organize PIP
training
The PIP Provides information on how well the five domains and
individual indicators and sub indicators are implemented by each
facility, each district and each region. It also provides a strong
information management system for managers at all levels who have
been trained in the use of the SPARS information and PIP data.
7. Mitigation of Fraud
To minimize the risk of fraud and false claiming of SPARS visits, the
Ministry of Health Pharmacy Department recommends that the District
Health Officer ensures zero tolerance to fraud in implementation of
SPARS and other medicines management activities at district level.
Implementing partners supporting SPARS are advised to conduct 100%
verification of visits through telephone calls and spot checks with
physical audits before any payments are made. Annex 2 details the
SPARS visit verification procedure.

22
8. Good Pharmacy Practice (GPP) certification
The national drug authority is mandated to regularly inspect all
pharmacy outlets to ensure that premises, personnel and practices meet
minimum standards established in the guidelines on suitability of
premises and licensure of pharmacy outlets. The ultimate goal of
improving medicines management at facilities through SPARS is to
ensure facilities adhere to Good Pharmacy Practices standards at all
times. This means that using the SPARS tool, MMS can support the
facility to meet good pharmacy practices standards and pass national
drug authority inspections as there is considerable overlap (73%) in
indicators for SPARS supervision and Good Pharmacy Practices
certification.
By February 2017 about 1200 facilities have been inspected and only
about 60% of the facilities passed good pharmacy practices
certification4. A detailed inspection report is provided which informs on
deficiencies. Some issues require behavioral changes which can be
addressed by the MMS, others will require investments. The Ministry of
Health Pharmacy Department in collaboration with the District Health
Officer will in the coming year take steps to address identified
deficiencies and identified the necessary funding.
4 Trap et al (2016). First regulatory inspections measuring adherence to Good
Pharmacy Practices in the public sector in Uganda: a cross-sectional comparison of performance between supervised and unsupervised facilities Journal of Pharmaceutical Policy and Practice, 9:18

23
COST OF SPARS IMPLEMENTATION
SPARS implementation involves considerable one-off start-up
investments for capacity building and equipment procurement. These
SPARS startup costs include:
1. Training of MMS: This include the initial MMS 2 weeks training
in classes of 25 students, 5 days practical in the field training,
computer training and defensive driving training. The curriculum
and training material for these trainings has been developed and
used for numerous of trainings and experienced trainers are
available. Makerere University has in the past been tasked to
implement these trainings.
2. Motorcycles and accessories: These are critical for MMS to have
the flexibility to reach all facilities within the district for
supervision. Durable off road, high ground clearance 2 strokes 100-
125 cc bikes are recommended (see annex 3 for detail specification
of motorbike and accessories. The Ministry of Health recommends
that these bikes be assessed for replacement after five years given
the rough dirt roads in districts.
3. Computer and internet modems: The netbook and modem allow
the MMS to enter and submit performance assessment data in real
time to the Pharmaceutical Information Portal (PIP), to access
pharmaceutical information and facilitate communication within the
sector and with other MMS’s. Durable and if possible military
grade specifications are recommended for MMS who move with
these computers to the field on their motorbikes (see annex 4 for
recommended specifications). The Ministry of Health also
recommends these computers be regularly serviced and replaced
every five years.
4. Printed materials, tools and equipment: These includes all the
tools and equipment required for effective medicines management
like: supervision books, stock books, standard operating
procedures, dispensing equipment as well as recognition items (see
annex 6 for details of these items)
24
Optional costs:
1. Utility racks/ shelves: This is critical for ensuring good storage
management is achieved at facility stores. To ensure facilities have
a uniform durable brand of shelving Ministry of Health
recommends the shelve specification in annex 5 for procurement.
By end of 2016 about 2/3 of all facilities nationally has been
provided with shelves. Each rack has 5 shelves and HC II are
provided with 1 rack, HC III with 2 racks, HC IV 4 and Hospital
with 8 racks.
2. Supplementary training: These trainings are targeted at improving
MMS supervision effectiveness and MMS taking on additional
roles. This trainings could be supportive supervision,
pharmaceutical financial management training and ARV- logistics
supervision training etc.
3. Good pharmacy practice inspections: In collaboration with the
national drug authority, facilities are required to be inspected
regularly for adherence to good pharmacy practice standards.
Previous good pharmacy practice inspections have been co-funded
by implementing partners and the national drug authority. Cost
involved are per diem for inspector and driver; fuel and the
certificate. Facilities that fail good pharmacy practice inspections
are will have to be supported by the districts and implementing
partners to comply with minimum pharmacy practice standards.
4. Logistics coordination meetings: Coordination is important for
improved medicines management performance at all levels of the
healthcare system. SPARS implementation should provide for
various levels of coordination including regional and national
coordination meetings. These coordination meeting brings together
all medicines management stakeholders at regional and national
level to discuss medicines management performance and make
decisions to improve practices moving forward
5. Central, regional and district level supervision visits: To manage
SPARS implementation, addressing poor performance, follow up
and oversight supportive supervisory visits to the district by

25
Ministry of Health Pharmacy Department, District Health Officer
or regional pharmacists should be facilitated.
Experience from the concluded USAID/ Securing Ugandans’ Right to
Essential Medicines program showed that it costs about 46 USD per
SPARS visit5. The routine costs involved in SPARS implementation
include;
1. MMS supervision costs: The Ministry of Health Pharmacy
department recommends that MMS be facilitated with safari daily
allowance and transport facilitation for their supervision activities.
Only one supervision visit is eligible for reimbursement per day.
Following each supervisory visit and the report submitted into the
PIP the MMS will be facilitated with safari daily allowance and
transport facilitation for their supervision activities. Only one
supervision visit is eligible for reimbursement per day. For MMS
with motorcycles the recommended remuneration per SPARS visit
is 35,000 UGX covering fuel (6000 UGX), Safari Day Allowance
(20,000 UGX), Minor repairs (4000 UGX) and Oil change costs
(5,000).
2. Motorcycles and computer repair and maintenance: To ensure
MMS motorcycles and computers remain functional to support
SPARS implementation, routine repair and maintenance is critical.
The Ministry of Health recommends that the District Heath Officer
approves routine repair of equipment to ensure it’s linked to
performance of medicines management supervisors.
3. Communication expenses: SPARS implementation requires
excellent coordination with health facilities and the District Health
Office by the MMS. Internet connectivity to submit facility
performance assessment tools to the PIP and modem and telephone
5 Trap et al. (unpublished). Costs and Effectiveness of Supervision, Performance
Assessment and Recognition (SPARS) Strategy for Medicines Management in
Uganda

26
time are therefore required. The MMS and District Health Officer
also need to be facilitated monthly with modem time and telephone
time. Ministry of Health Pharmacy department recommends linking
provision of telephone time and modem time to SPARS
performance as per the recognition scheme in annex 6. Table 2
below provides the details of associated unit costs for SPARS
implementation at district level.

27
Table 2: SPARS capacity building and implementation unit costs
Activity/Service/Equipment Supported
Unit cost UGX
Unit cost USD ($1=3500 UGX)
Explanatory notes
One off costs
MMS Trainings
Two weeks SPARS training implemented by Makerere University per MMS
4,300,000 1229 Training implemented by Makerere University in classroom training of 25 participant. Cost includes training, training material, supervisory bags, hotel and meals and certificate
Practical 5 days field orientation per MMS
1,114,286 318 MMS on-the-job-training for 5 days by experienced MMS/ implementing partner officer. Includes 5 day safari day allowance for new MMS within their districts and accommodation and per diem ( for new experienced MMS/ Implementing partner officer &driver for 6 days); fuel (Estimated mileage of 2000 km per district orientation at a cost of 3600 UGX per litre)
Four day net book training per MMS
500,000 143 Course organized by implementing partner assisted by experienced MMS

28
Activity/Service/Equipment Supported
Unit cost UGX
Unit cost USD ($1=3500 UGX)
Explanatory notes
Five days residential course in defensive Motorcycle Riding and license per MMS
2,865,116 819 Implemented at driving ranges in Entebbe using their motorbikes and driving gear
Motorcycles and accessories
One motorcycles 120-125 cc 10,500,000 3,000 Rugged off road bike
Riding Gear (riding suit, Helmet, gloves and riding boots) per MMS
2,300,000 657
Computers and printers
One Laptop 3,750,000 1071 Military grade device. 2-in-1. 360 degree flip from laptop to tablet mode
Printer for District MMS, one per districts
500,000 143 This printer is provided for only the District-MMS, including stationaries, paper and spare tonner etc.
Internet Modem per MMS 100,000 29 Best internet provider in the district preferred
Internet Modem per DHO 100,000 29 Best internet provider in the district preferred

29
Activity/Service/Equipment Supported
Unit cost UGX
Unit cost USD ($1=3500 UGX)
Explanatory notes
Health facility recognition items
Printed materials per facility 600,000 171 Printed materials include; stock cards ,stock books and prescription & dispensing logs, supervision books, EMHS manuals, Uganda clinical guidelines, expiries/ spoiled record book, borrow and lend record book
Tools and equipment per facility
300,000 86 Assorted items (dispensing trays, wall thermometers, notice boards, measuring cylinder, recording books and others)
Optional SPARS implementation costs
Supplementary trainings MMS may receive additional trainings that are targeted at improving supervision effectiveness and preparing MMS to take on additional roles. Trainings include; supportive supervision training & pharmaceutical

30
Activity/Service/Equipment Supported
Unit cost UGX
Unit cost USD ($1=3500 UGX)
Explanatory notes
financial management trainings (conducted Makerere University) and the ART logistics supervision training.
Shelves/ medicines racks including distribution
Each unit costs 280 USD plus 40 USD for distribution. For specification see annex 5
National drug authority good pharmacy practice Inspections
Co-funded by the national drug authority to cover per diem for inspector and driver; fuel and certificate.
Coordination meetings Periodic regional and national SPARS performance and coordination meetings
Support supervision visits Periodic higher level support visits to poor performing regions and districts
Annual running costs
MMS SDA and Fuel per SPARS visit and submitted report
35,000 10 Fixed fee of 35,000 UGX per supervision which includes SDA and fuel

31
Activity/Service/Equipment Supported
Unit cost UGX
Unit cost USD ($1=3500 UGX)
Explanatory notes
Annual Maintenance of Motorbikes (service and repairs)
400,000 114 Major servicing and repair once a year after 30 supervisions.
Annual Internet connectivity per MMS
500,000 143 Annual 12GB internet subscription loaded quarterly based on performance
Annual Internet connectivity per DHO
500,000 143 Annual 12GB internet subscription loaded quarterly based on performance
Annual Telephone air time per District MMS
720,000 206 Coordination telephone airtime loaded quarterly based on performance
Annual Telephone air time per HSD MMS
360,000 103 Coordination telephone airtime loaded
quarterly based on performance
Annual Telephone air time per MMS
360,000 103 Coordination telephone airtime loaded
quarterly based on performance
I
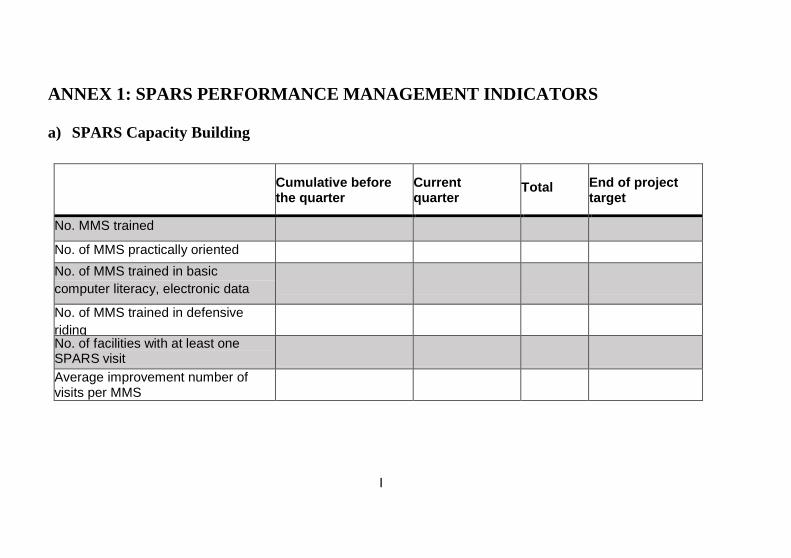
ANNEX 1: SPARS PERFORMANCE MANAGEMENT INDICATORS
a) SPARS Capacity Building
Cumulative before the quarter
Current quarter
Total
End of project target
No. MMS trained
No. of MMS practically oriented
No. of MMS trained in basic
computer literacy, electronic data
collection and submission
No. of MMS trained in defensive
riding
53
20
73
100 No. of facilities with at least one SPARS visit
Average improvement number of visits per MMS

II
b) Efficiency And Effectiveness of SPARS Implementation
i) Frequency of SPARS Visits
No. of visits
No. of facilities
Recommended no. days to next visit
Median no. days between visits
Previous quarter Current quarter
2 60
3 60
4 60
5 60
Average 60
6 120
7 120
8 120
Average 120

III
ii) Spars Score Improvement between Visits
No. of visits
No. of facilities
Recommended improvement
Improvement between visits
Previous quarter Current quarter
Visit 1- Visit 2 2
Visit 2- Visit 3 2
Visit 3- Visit 4 2
Visit 4- Visit 5 2
Visit 5- Visit 6 NA

I
Monthly SPARS supervision visit
verification
Confirm MMS visit by
record in both supervision
and visitors book
MMS visit not
confirmed in both
supervision and
visitors book
No
MMS visit confirmed
in visitors book only
Further telephone
verification for 15
medicines stock cards
balance on day of visit
with record submitted
Do physical SPARS
data audit
At least 12 of 15 (80%) record on
stock card and submitted tool
agree? YesEnd of visit verification
YesMMS visit confirmed by
records in both supervision
and visitor book
No
No
Extract all SPARS reports submitted in PIP for the
Month
Call up supervised persons in submitted SPARS
report
ANNEX 2: MONTHLY SPARS SUPERVISION
VERIFICATION PROCEDURE

I
ANNEX 3: MMS MOTORCYCLE AND ACCESSORIES SPECIFICATIONS
a) MMS Motorcycle specifications
Seating Capacity: 1-2 passengers
Engine: four stroke, 100cc-125cc
Fuel type: Petrol
Fuel tank capacity: 10L or more
Tires with off-road capabilities
Transmission: 5 speed, manual
Starter: Kick and self-starter
High Clearance for off-road purposes
Heavy duty suspension
Mirrors
Turn signals
Brake signal
Running light
Cargo rack
Crash Bars
Tool kit
Full-face helmet

II
b) Motorcycle riding accessories specifications
Item specification
Motorcycle / motor cross riding
boots
Pedal protection, protection of lower leg and angle, easy fit, safety toes
Riding jacket Wind and water tight with protection on shoulder and elbow, reflection material in front and back, pockets inside and outside, removable inner coat.
Riding pants Wind and water tight with protection on knees, adjustable belt and legs with and length.
Riding gloves Strong material , protection on fingers and knots,
locks Chain lock, 2 keys minimum, security lock

I
ANNEX 4: MMS LAPTOP SPECIFICATIONS
Processor Minimum 4 core (1.8Ghz)
Graphics Intel HD graphics or comparable
Memory Minimum 8GB
Display Minimum 11.6" HD (1366x768)
Multi‐touch Multi‐touch display
Storage Minimum 128GB SSD
WLAN & Bluetooth Intel 7260 a/b/g/n + BT4.0 or comparable
Color Black preferred
Camera Yes
Keyboard Keyboard built‐in
Battery (int+ext) Minimum 4‐cell (35wh)
Power Adapter (watt)
Minimum 45W
Preload Windows 8.1 Pro 64
Base Warranty Minimum 1‐year
Durability Military grade device. MIL‐SPEC.
Lock Kingston locks
Carry bag Work‐In case for Chromebooks
Pointing device USB mouse
Design 2‐in‐1. 360 degree flip from laptop to tablet mode

I
ANNEX 5: SHELVE SPECIFICATIONS
Item No Technical Specification Required
A Requirement
Description
A. Style
Number of required shelves
Type Open shelf
Minimum capacity per full set comprising of six shelves)
600kg per full set. (i.e. 100kg/ shelf)
Side anti-way Self-restricting. Only corner clits required to achieve full stability
Forward anti-sway Wall mounting clits 2No
B. Configuration /Appearance
Color white (powder coat Paint finish)
Depth 600mm
Width/length 1200mm
Height 2000mm
Number of shelves Adjustable six (6) shelves per unit.
Shelve level adjustment Increments 38-40mm centers
Ground clearance of bottom most shelf
140-160mm
Height level of top-most shelf 2000mm
Corner Stiffener Triangular corner stiffener plate

II
Item No Technical Specification Required
A Requirement
Assembly method By clipping/slotting. Boltless and Weldless
Shelf separators Not require/ applicable
C. Material Specification
Post
Slotted/Perforated steel, (40x40x2mm thick L shaped cold rolled steel. Slots are on both sides of the angle, spaced at increments of the 38-40mm in the longitudinal plane, and designed to accommodate variety of cross members and facilitate assembly
Spreaders/cross members (lengthwise beams and front to back beams)
Slotted/Perforated steel, 72x33.5x2mm thick L- shaped cold rolled steel. Slots are similar to post slots.
Anti-sway ties Only corner stiffeners required. Shelf MUST be completely stable after assembly without any anti-sway ties.
Shelf Blackboard/chipboard 18mm thick
Wall fixing clits 2 Slotted/Perforated Steel 40x40x2.0L.
Top Corner gussets/plates 4 Stiffener plates to be made of steel triangular, 2.0mm thick with holes to match with bolting/ assembly mechanism
Post shoes/ Footpads /Base plates
Heavy duty
Finishing specification
Stages of finishing including cleaning, rinsing, iron phosphate three rinses and application of final sealer The final sealer to be electrostatically applied Lead – free Powder Epoxy-polyester Coating, Polymerized at 180,

III
Item No Technical Specification Required
A Requirement
Final finish to be resistant to abrasion.
D. Other Requirements
Technical product literature Required and must be provided in English.
Accessories Every fifty complete units to be supplied with necessary assembly accessories and tools
Maintenance Guarantee the availability of maintenance parts in Uganda for a period of 10 years.
Warranty and period
- - As per warranty Letter, agreeing to repair or Replace units that fail in materials or workmanship within the specified warranty period
- - Material defect 5- years Workmanship - 1- year from date of delivery
Sample Successful bidder to provide sample prior to contract signing.
Packaging Bidder defined but every six- shelves unit to be packed in a maximum of two boxes/pieces
Installation Guide lines Must be provided in English.
Installation conference Supplier to Conduct a one-day training session or demonstration (installation conference) at each of the delivery regional offices every time a delivery is made. During this training Review methods and installation procedures related to installation and include at least make one Demonstration of the final product.

IV
ANNEX 6: SPARS RECOGNITION SCHEME
a) DHO/ CAO Recognition Scheme
Achievement Reward
1. At least one MMS in the district should have conducted 7 supervisions or achieved their target for the quarter
Telephone Airtime of 30,000 UGX per quarter
Modem Internet subscription of 1GB per month loaded quarterly
2. 80% of facilities in the district using stock book correctly (with at least 80% score
One off sugar (10kg) and tea leaves (1 Pack of 500g) for DHO and CAO
3. District on average scores at least 20 out of 25 in SPARS
Branded T-Shirts for DHO and CAO
4. 75% of facilities in the district Good Pharmacy Practice certified by the National
Branded wall clock for DHOs and CAO
5. District on average scores 15 out of 20 in ART Test Treat and Track Supervision
Certificate of recognition for excellence in ART logistics management in support of 90-90-90 targets and differentiated service delivery

V
b) Regional Pharmacist (RP) - Recognition Scheme
Achievement Reward
1. At least 80% of MMS in the region achieves their target supervisory visits in the quarter
Modem Internet subscription of 1GB per month for loaded quarterly
2. Regional hospital achieves a score at least 20 out of 25 in SPARS
Branded T-Shirts

VI
c) District Medicines Management Supervisors Recognition Scheme
Achievement Reward
1. New District MMS passes training
course
MMS training certificate
Supervision package (backpack bag, calculator clipboard, pens)
2. New District MMS passes the
defensive motorcycle training
course
Riding license
Defensive motorcycle riding course certificate
Motor cycle/ repair kit
Riding gears
3. New District MMS passes computer
and SPARS Data utilization training
course
Notebook (Laptop)
Modem Internet subscription of 1GB per month loaded for the first quarter
4. Supervision visit conducted and
complete report submitted through
the PIP
Contribution of 35,000 UGX for SDA, fuel and minor repairs paid within 10 days of the new month to the MMS

VII
Achievement Reward
5. District MMS implements at least 7
supervision visits or achieves their
targets for the quarter
Telephone airtime of 30,000 UGX paid quarterly for coordination
Modem Internet subscription of 1GB per month loaded quarterly
6. District MMS conducts at least 2
HSD MMS supervisions or achieved
their target for the quarter
Telephone airtime of 30,000 UGX paid quarterly for coordination
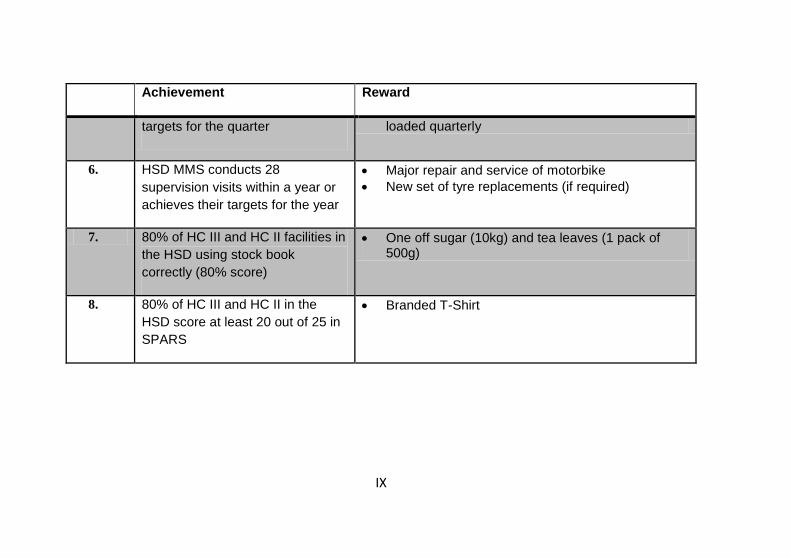
7. District MMS conducts 28
supervision visits within a year or
achieves their targets for the year
Major repair and service of motorbike
New set of tyre replacements (if required)
8. All hospitals and HCIV’s using
stock book correctly (100% score)
One off sugar (10kg) and tea leaves (1 pack of 500g)
9. All hospitals and HCIV’s score at
least 20 out of 25 in SPARS
Branded T-Shirt

VIII
d) HSD Medicines Management Supervisors Recognition Scheme
Achievement Reward
1. New HSD MMS passes training
course
MMS training certificate
Supervision package (Bag, Calculator clipboard, pens)
2. New HSDMMS passes the
defensive motorcycle training
course
Riding license
Defensive motorcycle riding course certificate
Motor cycle and repair kit
Riding gears
3. New HSD MMS passes computer
and SPARS Data utilization
training course
Notebook (Laptop)
Modem Internet subscription of 1GB per month loaded for the first quarter
4. Supervision visit conducted and
complete report submitted through
the PIP
Contribution of 35,000 UGX for SDA, fuel and minor repairs paid within 10 days of the new month to the MMS
5. HSD MMS implements at least 7
supervision visits or achieves their
Telephone airtime of 30,000 UGX paid quarterly for coordination
Modem Internet subscription of 1GB per month
IX
Achievement Reward
targets for the quarter loaded quarterly
6. HSD MMS conducts 28
supervision visits within a year or
achieves their targets for the year
Major repair and service of motorbike
New set of tyre replacements (if required)
7. 80% of HC III and HC II facilities in
the HSD using stock book
correctly (80% score)
One off sugar (10kg) and tea leaves (1 pack of 500g)
8. 80% of HC III and HC II in the
HSD score at least 20 out of 25 in
SPARS
Branded T-Shirt

X
e) Health Facilities Recognition Scheme
Achievement Reward
1. Facility supervised once *One off supply of sugar and tea leaves
Supervision Book
Soft board notice boards, branded
A4 'Cosmic D-ring Insert binder" Box Files (5 files)
Blue and Red pens (12 pens)
Shelve units
Stock cards
Spider graph
2. 100% availability of stock cards Stock Book
Tablet counting Tray Triangular/ Spatula
Casio 12 digit calculator
Masking tape
Pack of permanent markers
MAX-MIN wall thermometer
Temperature monitoring book
Borrow and lend record
Expired medicines register
XI
Achievement Reward
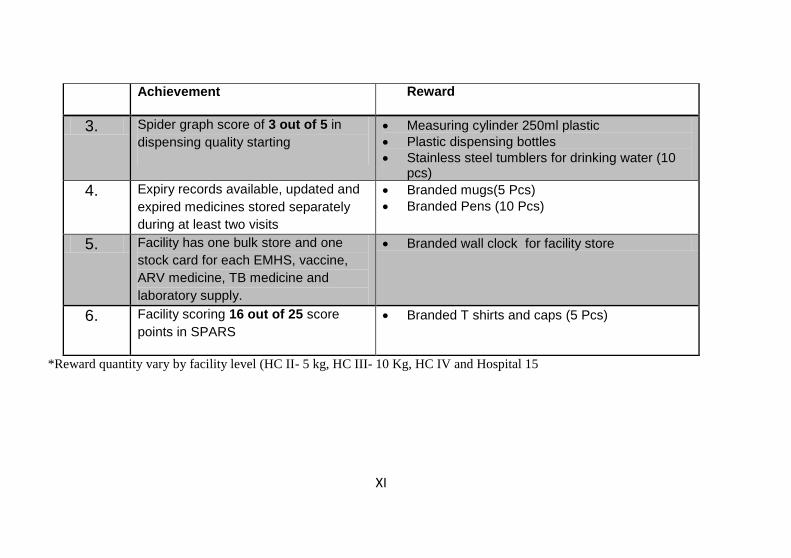
3. Spider graph score of 3 out of 5 in
dispensing quality starting
Measuring cylinder 250ml plastic
Plastic dispensing bottles
Stainless steel tumblers for drinking water (10 pcs)
4. Expiry records available, updated and
expired medicines stored separately
during at least two visits
Branded mugs(5 Pcs)
Branded Pens (10 Pcs)
5. Facility has one bulk store and one
stock card for each EMHS, vaccine,
ARV medicine, TB medicine and
laboratory supply.
Branded wall clock for facility store
6. Facility scoring 16 out of 25 score
points in SPARS
Branded T shirts and caps (5 Pcs)
*Reward quantity vary by facility level (HC II- 5 kg, HC III- 10 Kg, HC IV and Hospital 15
I
Published by Ministry of Health Uganda
with support from USAID/Uganda Health Supply Chain


















