
Sum Scores & Components’ Scores Chronic Scores Acute Rejection Scores Lillian W. Gaber University...
49
Sum Scores & Components’ Scores Chronic Scores Acute Rejection Scores Lillian W. Gaber University of Tennessee
-
date post
19-Dec-2015 -
Category
Documents
-
view
268 -
download
0
Transcript of Sum Scores & Components’ Scores Chronic Scores Acute Rejection Scores Lillian W. Gaber University...
Sum Scores & Components’ ScoresChronic Scores
Acute Rejection Scores
Lillian W. GaberUniversity of Tennessee
•Inclusive but in the mean time selective of the examined lesions •Weigh lesions according to their importance
•Simplify the schema•less features to assess•Conspicuous lesions
Too Many or Less Features to Evaluate
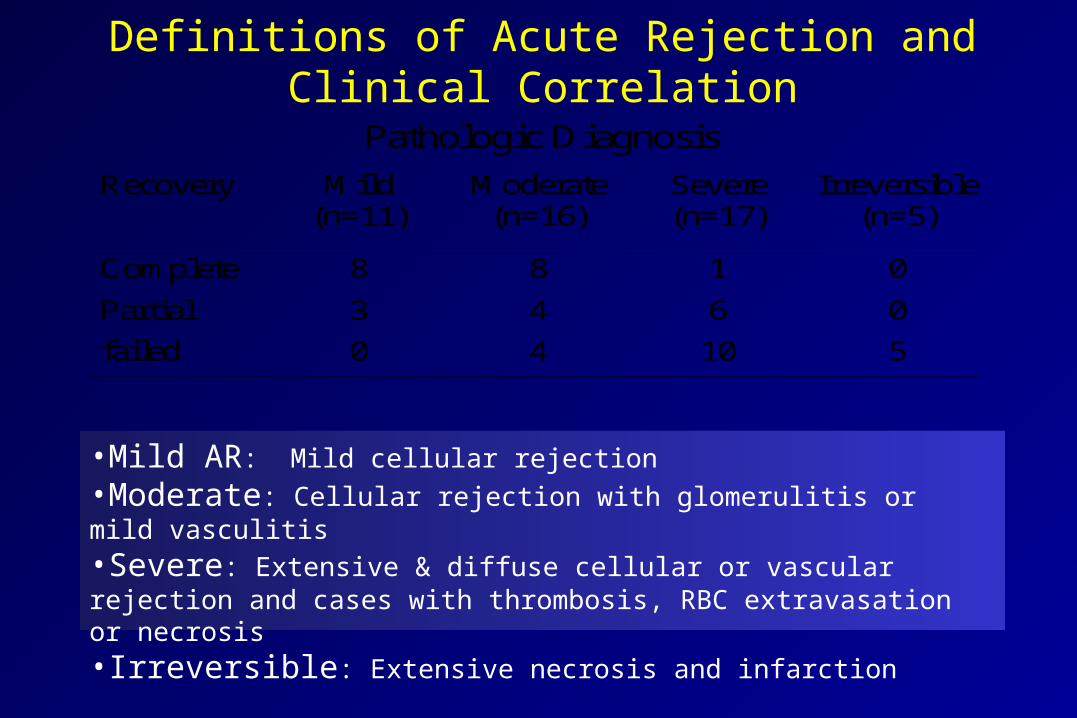
Definitions of Acute Rejection and Clinical Correlation
Pathologic Diagnosis
Recovery Mild(n=11)
Moderate(n=16)
Severe(n=17)
Irreversible(n=5)
Complete 8 8 1 0
Partial 3 4 6 0
failed 0 4 10 5
•Mild AR: Mild cellular rejection•Moderate: Cellular rejection with glomerulitis or mild vasculitis•Severe: Extensive & diffuse cellular or vascular rejection and cases with thrombosis, RBC extravasation or necrosis•Irreversible: Extensive necrosis and infarction
Banfi et al; 1981
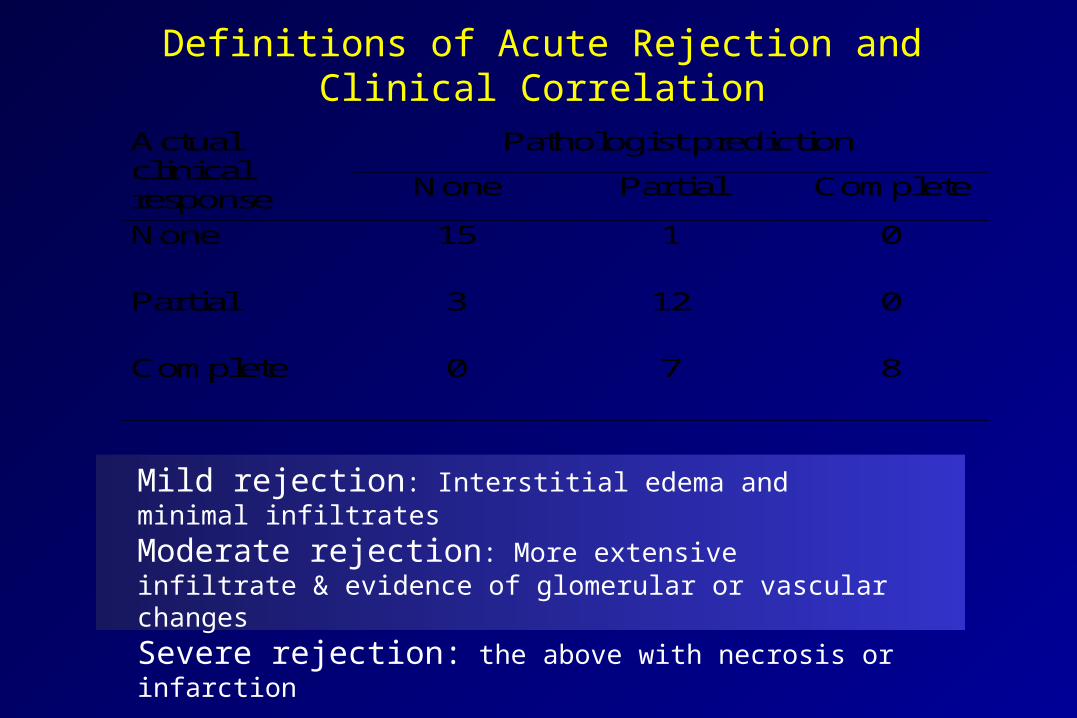
Definitions of Acute Rejection and Clinical Correlation
Pathologist predictionActualclinicalresponse None Partial Complete
None 15 1 0
Partial 3 12 0
Complete 0 7 8
Mild rejection: Interstitial edema and minimal infiltrates
Moderate rejection: More extensive infiltrate & evidence of glomerular or vascular changes
Severe rejection: the above with necrosis or infarction
Finkelstein et al, 1976
Early Studies with Semiquantitative Data
• Hsu et al- University of Toronto (1976)– Chronic lesions, fibrinoid vascular deposits and obliterative endarteritis correlate
with creatinine rise at 1-3 mo post biopsy
• Klaer et al- Aarhus Denmark (1980)– Glomeurlar or arterial thrombosis and infarction correlate with graft loss
• Banfi et al- Milan (1981)– Glomerular necrosis, intimal arteritis, arterial fibrinoid necrosis and PTC
congestion predicted elevation of the 2-mo postbiopsy creatinine
• Durand et al, France (1983)– Arterial and tubular lesions were the strongest predictors of adverse outcome
• Parfrey et al, McGill University (1984)– Interstitial hemorrhage was the strongest predictor for graft failure. Intimal arteritis
and glomerulitis strengthened the prognosis
Acute Rejection Index(0-36)
• Glomerular endothelial swelling
• Endothelial and mesangial proliferation
• Glomerular Leukocytes
• Glomerular necrosis
• Interstitial edema
• Interstitial inflammation
• Swelling of the vascular endothelium and edema
• Mural vascular inflammation
• Mural vascular necrosis
Finkelstein&Kashgarian 1976
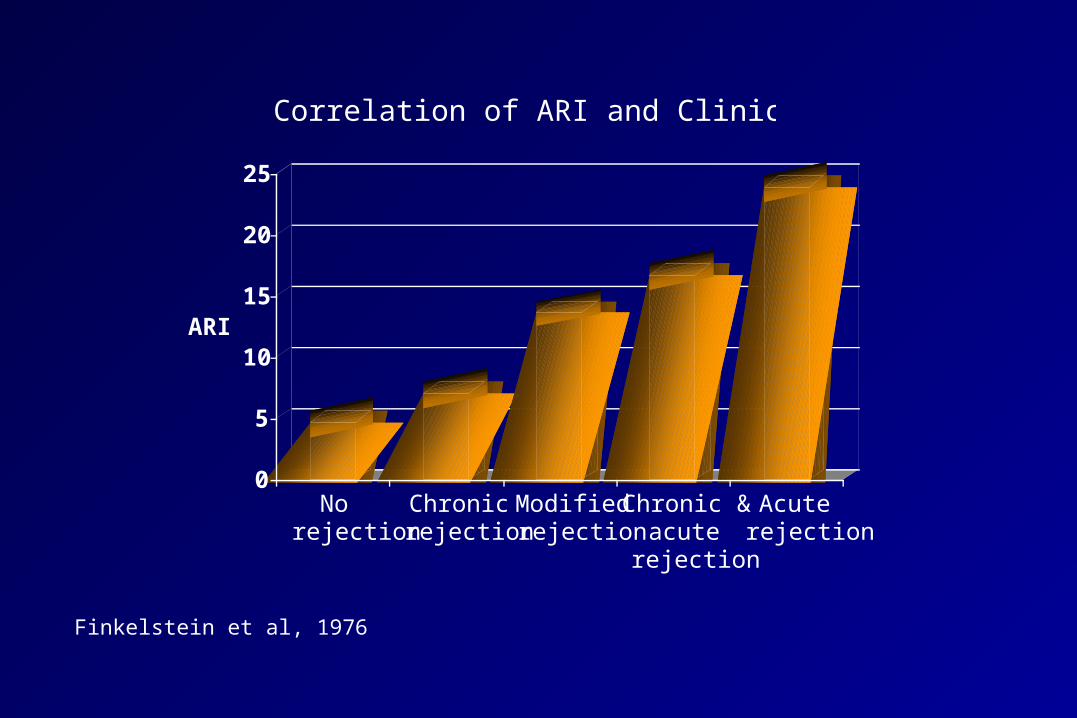
0
5
10
15
20
25
ARI
Norejection
Chronicrejection
Modifiedrejection
Chronic ´
rejection
Acuterejection
Correlation of ARI and Clinical Diagnosis
Finkelstein et al, 1976
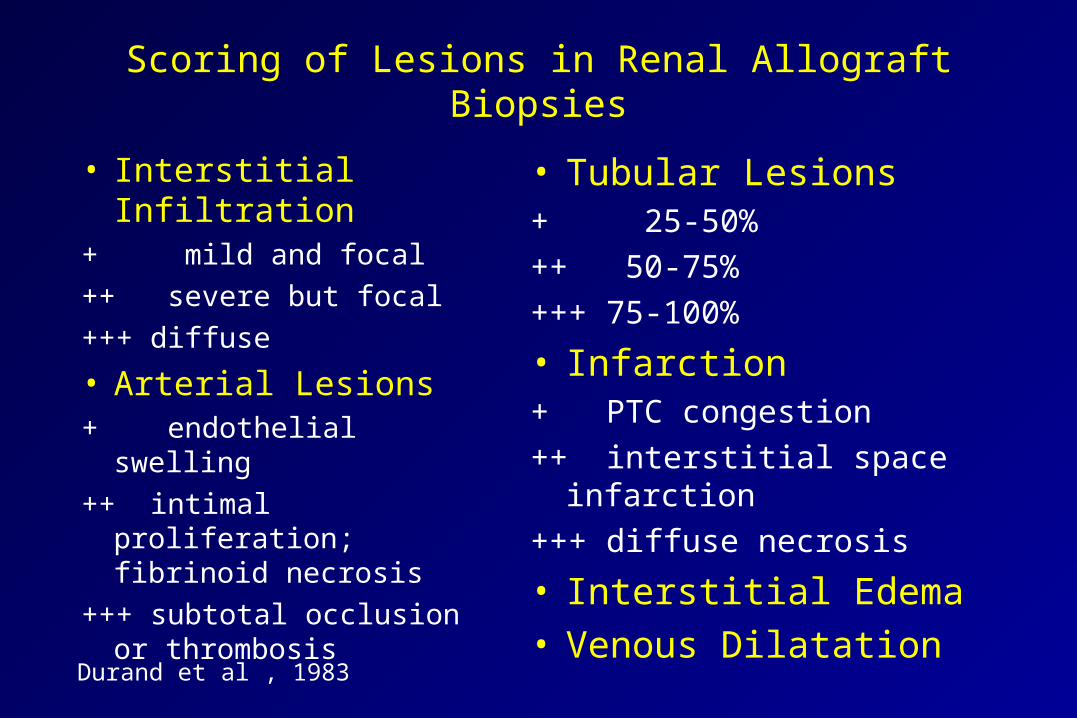
Scoring of Lesions in Renal Allograft Biopsies
• Interstitial Infiltration+ mild and focal
++ severe but focal
+++ diffuse
• Arterial Lesions+ endothelial swelling
++ intimal proliferation; fibrinoid necrosis
+++ subtotal occlusion or thrombosis
• Tubular Lesions+ 25-50%
++ 50-75%
+++ 75-100%
• Infarction+ PTC congestion
++ interstitial space infarction
+++ diffuse necrosis
• Interstitial Edema• Venous Dilatation
Durand et al , 1983
Durand et al , 1983
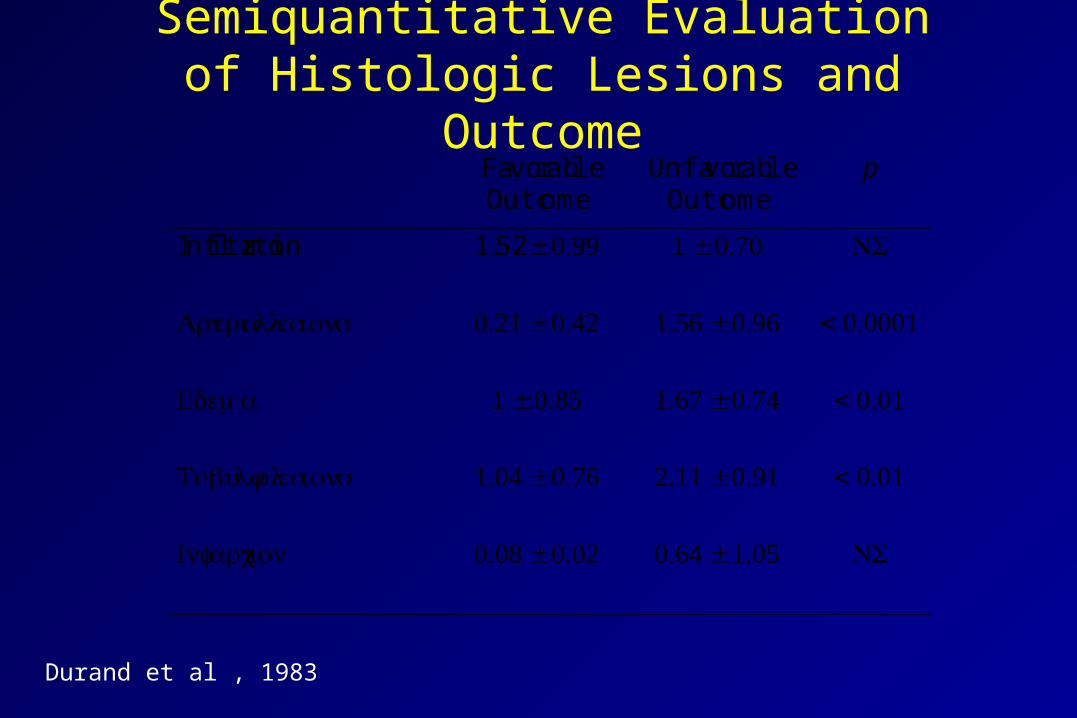
Semiquantitative Evaluation of Histologic Lesions and Outcome
FavorableOutcome
UnfavorableOutcome
p
Infiltration 1.52 ± 0.99 1 ± 0.70 NS
Arterial lesions 0.21 ± 0.42 1.56 ± 0.96 < 0.0001
Edema 1 ± 0.85 1.67 ± 0.74 < 0.01
Tubular lesions 1.04 ± 0.76 2.11 ± 0.91 < 0.01
Infarction 0.08 ± 0.02 0.64 ± 1.05 NS
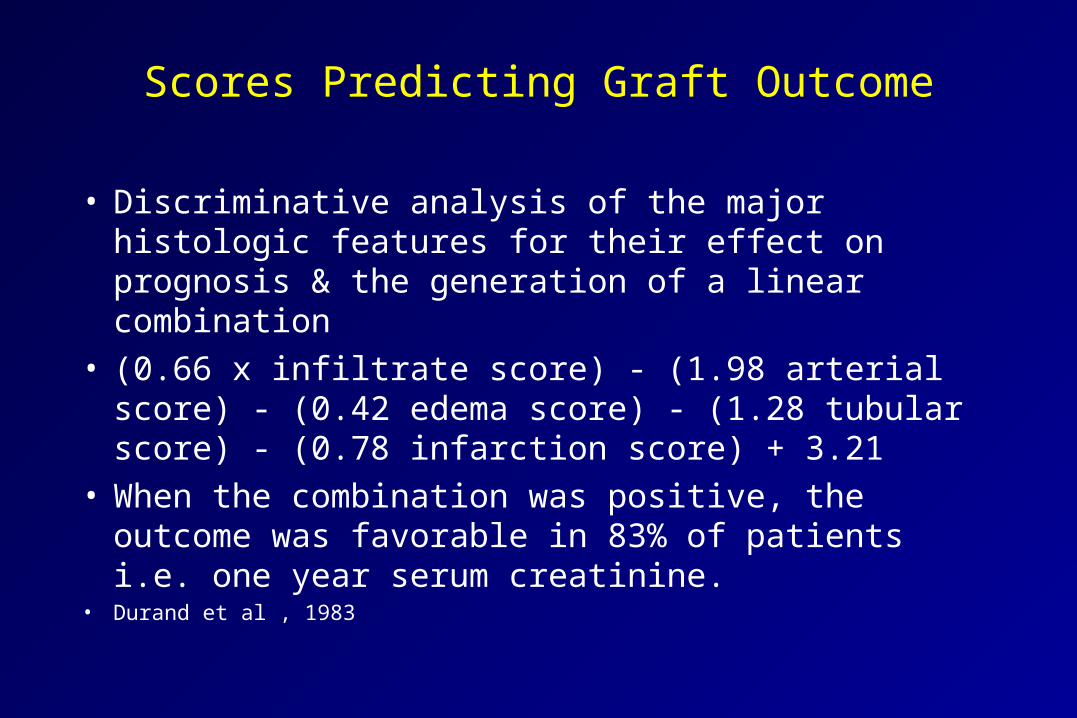
Scores Predicting Graft Outcome
• Discriminative analysis of the major histologic features for their effect on prognosis & the generation of a linear combination
• (0.66 x infiltrate score) - (1.98 arterial score) - (0.42 edema score) - (1.28 tubular score) - (0.78 infarction score) + 3.21
• When the combination was positive, the outcome was favorable in 83% of patients i.e. one year serum creatinine.
• Durand et al , 1983
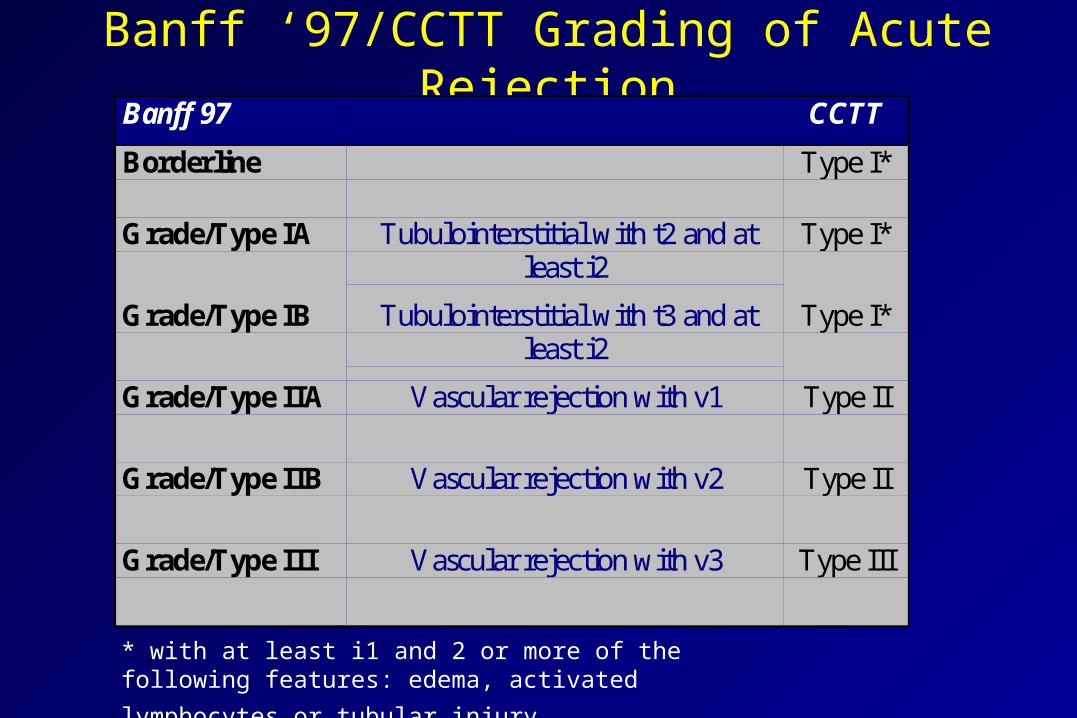
Banff ‘97/CCTT Grading of Acute RejectionBanff 97 CCTT
Borderline Type I*
Grade/Type IA Tubulointerstitial with t2 and atleast i2
Type I*
Grade/Type IB Tubulointerstitial with t3 and atleast i2
Type I*
Grade/Type IIA Vascular rejection with v1 Type II
Grade/Type IIB Vascular rejection with v2 Type II
Grade/Type III Vascular rejection with v3 Type III
* with at least i1 and 2 or more of the following features:
edema, activated lymphocytes or tubular injury
Questions!
• Is the current grading of rejection clinically relevant?• Do Grades and scores correlate with clinical severity?• Are grades/scores helpful in managing patients outside of
study protocols?• How were scores used in clinical trials and investigative
research?• Is there a need to modify the current scores, and if so
how to do it?
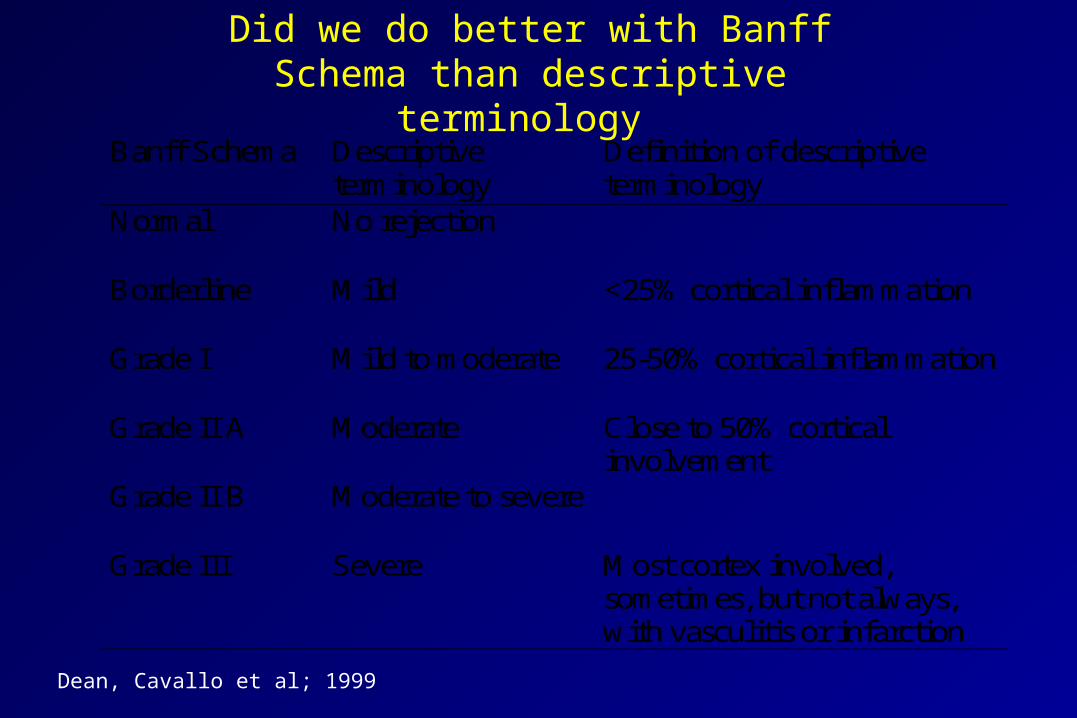
Did we do better with Banff Schema than descriptive terminology
Banff Schema Descriptiveterminology
Definition of descriptiveterminology
Normal No rejection
Borderline Mild <25% cortical inflammation
Grade I Mild to moderate 25-50% cortical inflammation
Grade II A Moderate Close to 50% corticalinvolvement
Grade II B Moderate to severe
Grade III Severe Most cortex involved,sometimes, but not always,with vasculitis or infarction
Dean, Cavallo et al; 1999
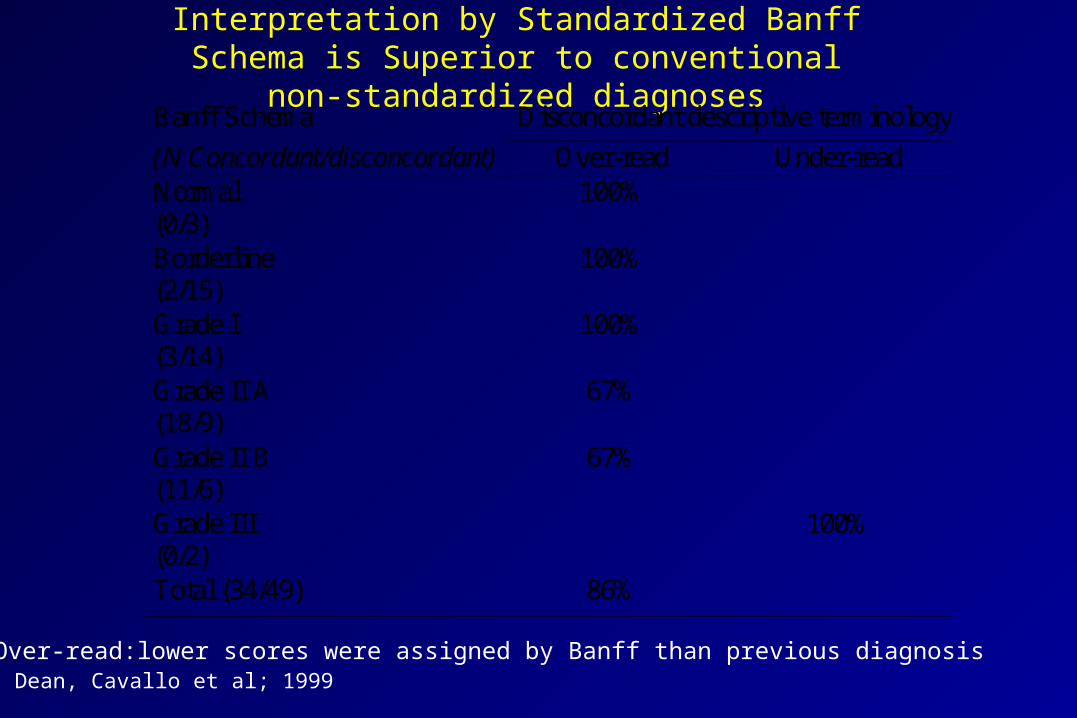
Interpretation by Standardized Banff Schema is Superior to conventional non-standardized diagnoses
Banff Schema Disconcordant descriptive terminology
(N Concordant/disconcordant) Over-read Under-readNormal(0/3)
100%
Borderline(2/15)
100%
Grade I(3/14)
100%
Grade II A(18/9)
67%
Grade II B(11/6)
67%
Grade III(0/2)
100%
Total (34/49) 86%
Dean, Cavallo et al; 1999Over-read:lower scores were assigned by Banff than previous diagnosis
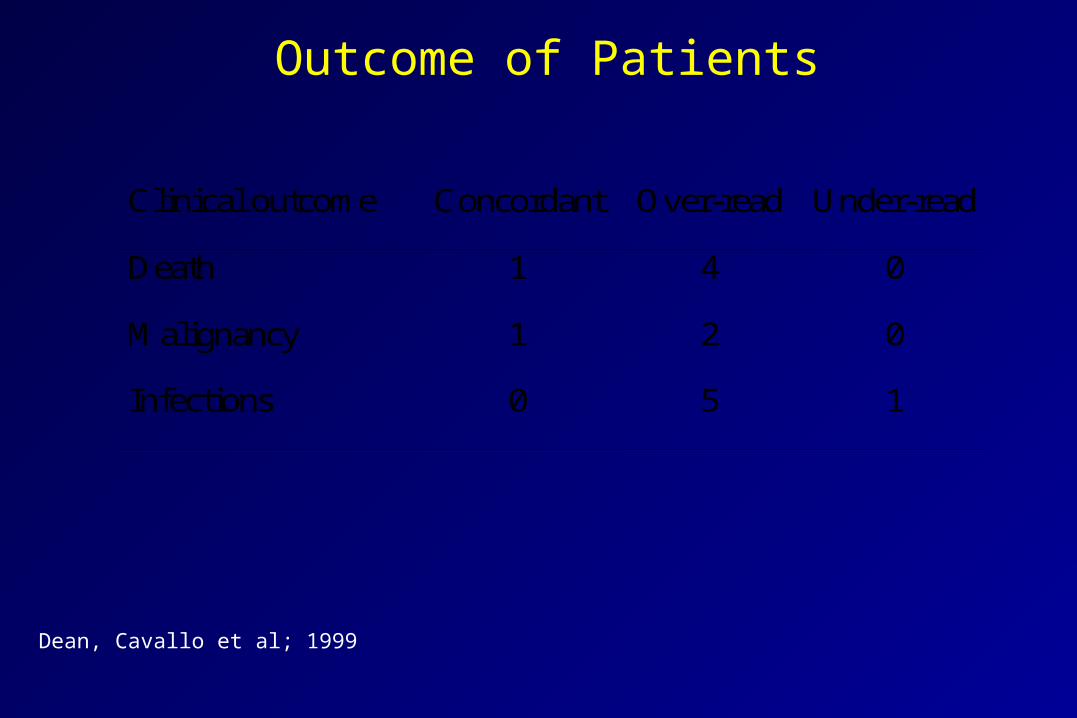
Outcome of Patients
Clinical outcome Concordant Over-read Under-read
Death 1 4 0
Malignancy 1 2 0
Infections 0 5 1
Dean, Cavallo et al; 1999
CCTT Analysis of Morphologic Correlates to Clinical Severity of Acute Rejection
• Morphologic features that significantly correlated with clinical severity of rejection– Type II rejection
– Tubular injury
– Endothelialitis
– Interstitial hemorrhage
– Interstitial edema
– Glomerulitis
– Activated lymphocytes
– Tubulitis
Vascular Scores
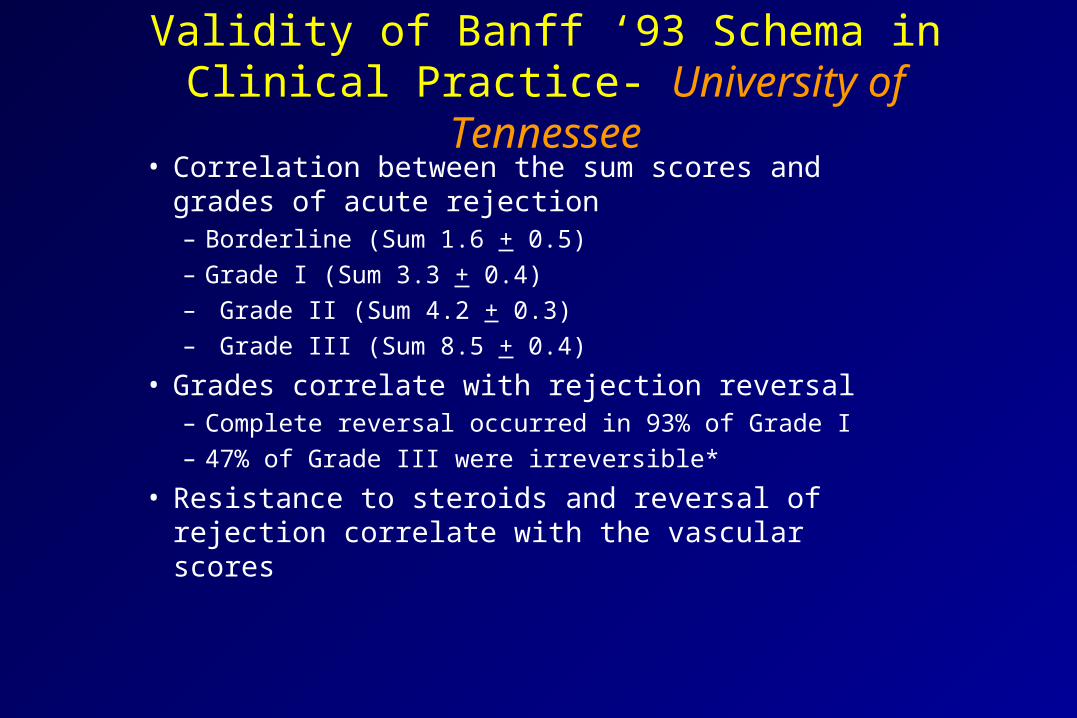
Validity of Banff ‘93 Schema in Clinical Practice- University of Tennessee
• Correlation between the sum scores and grades of acute rejection – Borderline (Sum 1.6 + 0.5)– Grade I (Sum 3.3 + 0.4)– Grade II (Sum 4.2 + 0.3)– Grade III (Sum 8.5 + 0.4)
• Grades correlate with rejection reversal– Complete reversal occurred in 93% of Grade I – 47% of Grade III were irreversible*
• Resistance to steroids and reversal of rejection correlate with the vascular scores
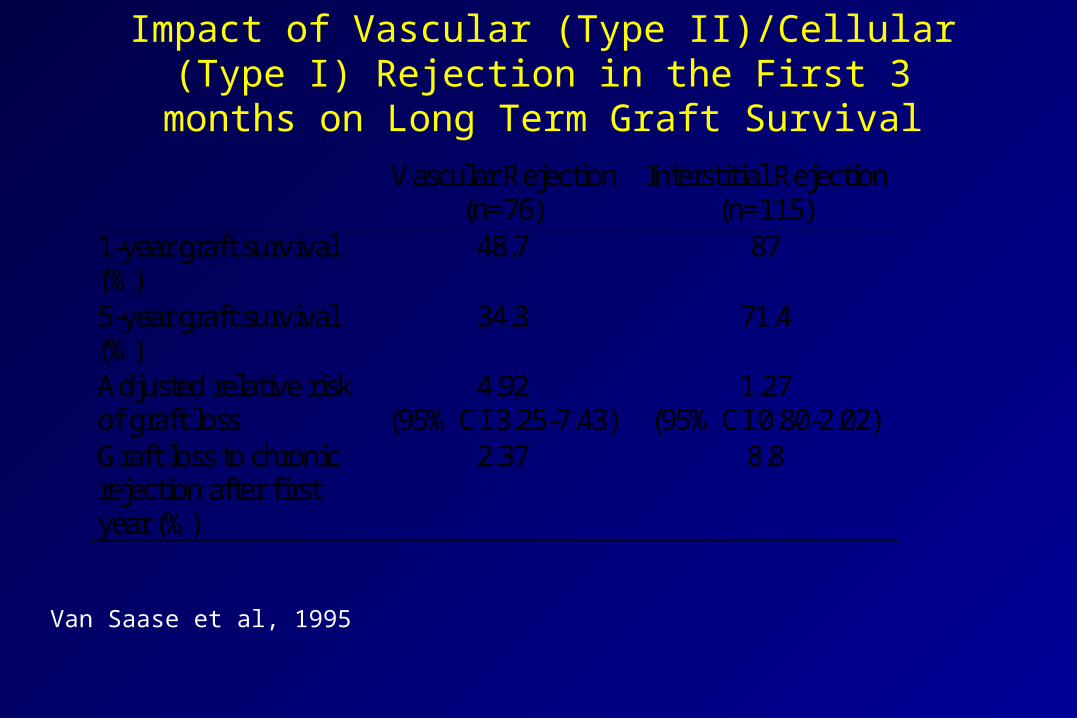
Impact of Vascular (Type II)/Cellular (Type I) Rejection in the First 3 months on Long Term Graft Survival
Vascular Rejection(n=76)
Interstitial Rejection(n=115)
1-year graft survival(%)
48.7 87
5-year graft survival(%)
34.3 71.4
Adjusted relative riskof graft loss
4.92(95% CI 3.25-7.43)
1.27(95% CI 0.80-2.02)
Graft loss to chronicrejection after firstyear (%)
2.37 8.8
Van Saase et al, 1995

Divergent graft survival between tubulointerstitial rejection and rejection with fibrinoid necrosis
CCTT Response to Therapy(%)
MeanSerum
Creatinine
GraftFailure
(%)Steroid OKT3/ATG 6-mo 1 year
Type I 45 65 2.3 + 0.2 21
Type II 19* 61 2.5 + 0.2 28
Type III 0 0 6.7 100
Nickeleit, Colvin et al, 1998
* P= 0.03 versus Type I
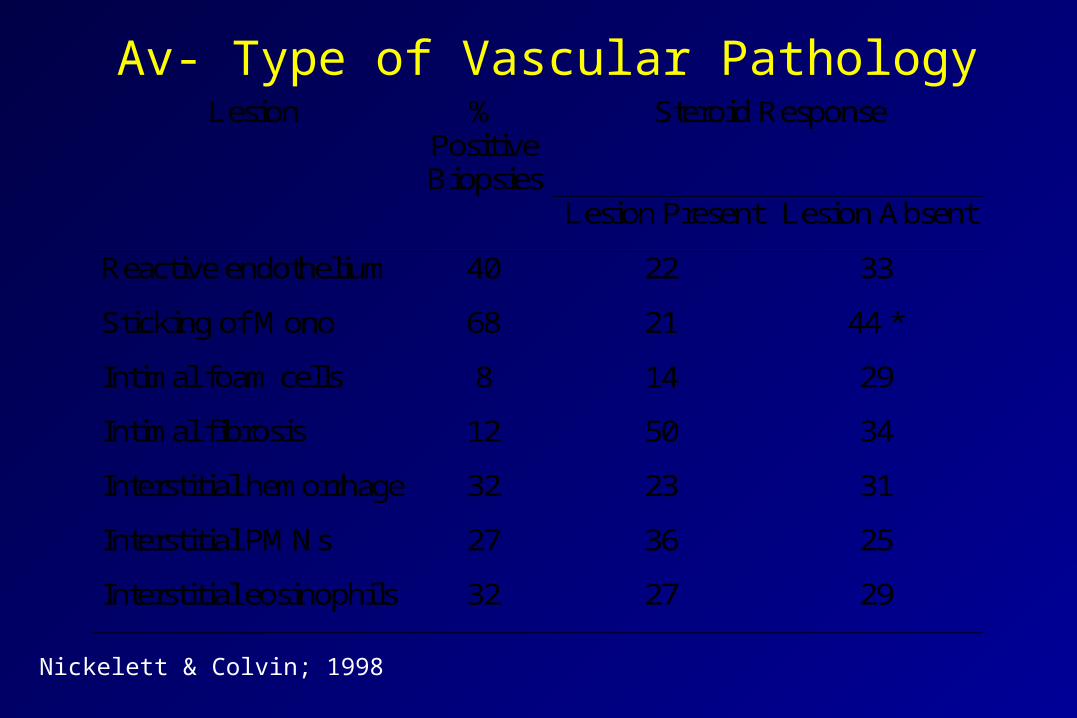
Av- Type of Vascular PathologyLesion %
PositiveBiopsies
Steroid Response
Lesion Present Lesion Absent
Reactive endothelium 40 22 33
Sticking of Mono 68 21 44 *
Intimal foam cells 8 14 29
Intimal fibrosis 12 50 34
Interstitial hemorrhage 32 23 31
Interstitial PMNs 27 36 25
Interstitial eosinophils 32 27 29
Nickelett & Colvin; 1998
Vascular Pathology and Rejection Outcome
• Number of arteries with lesions did not correlate with steroid responsiveness or the 12-month creatinine
• Of the different types of lesions, reactive endothelium and sticking of mononuclear cells correlated with steroid resistance
Nickelett & Colvin; 1998
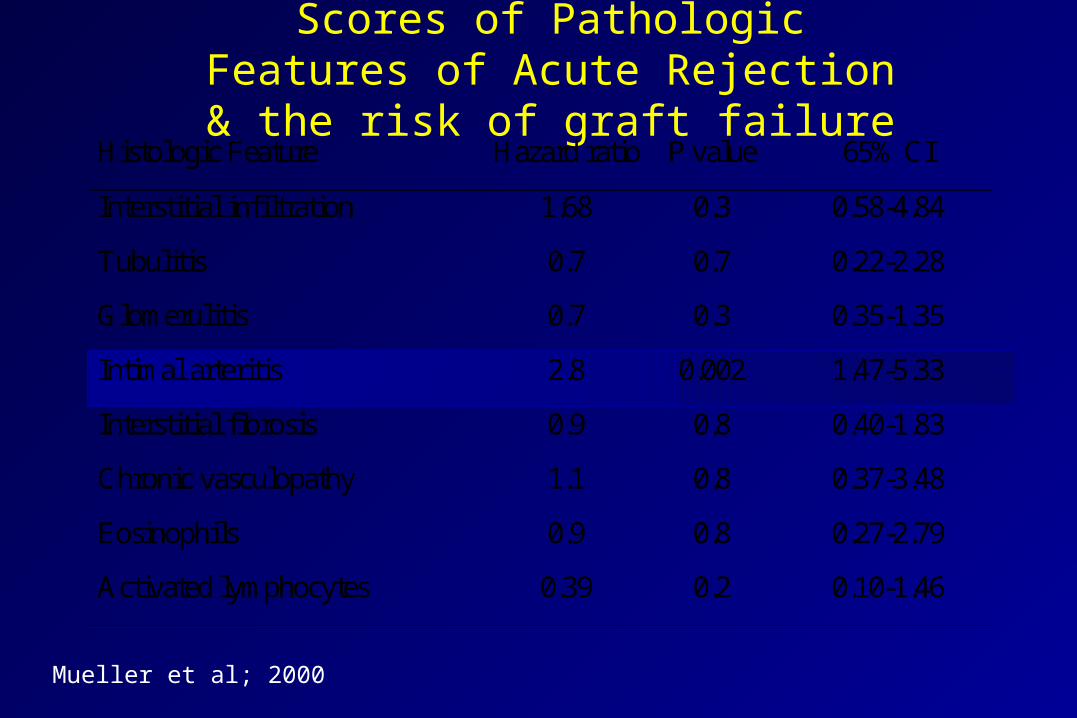
Scores of Pathologic Features of Acute Rejection & the risk of graft failure
Histologic Feature Hazard ratio P value 65% CI
Interstitial infiltration 1.68 0.3 0.58-4.84
Tubulitis 0.7 0.7 0.22-2.28
Glomerulitis 0.7 0.3 0.35-1.35
Intimal arteritis 2.8 0.002 1.47-5.33
Interstitial fibrosis 0.9 0.8 0.40-1.83
Chronic vasculopathy 1.1 0.8 0.37-3.48
Eosinophils 0.9 0.8 0.27-2.79
Activated lymphocytes 0.39 0.2 0.10-1.46
Mueller et al; 2000
Vascular Scores
• The most significant determinant of steroid response, rejection reversal and kidney function at one year
• Vascular rejection is a predictor of chronic rejection• Number of arteries to be examined?• Isolated vascular rejection?• V1-2 rejection and severe tubulo-interstitial rejection?• Lumen compromise and severity of rejection?• Sticky mononuclear cells and endothelial edema?• Fibrinoid vascular necrosis! Rejection or no rejection?
Interstitial scores
Interstitial infiltratesThreshold for Acute Rejection
• i1 in Banff identified as 10-25% of parenchyma involved• Type I rejection Banff requires at least i1• CCTT specified greater than 5% inflammation in the
renal cortex
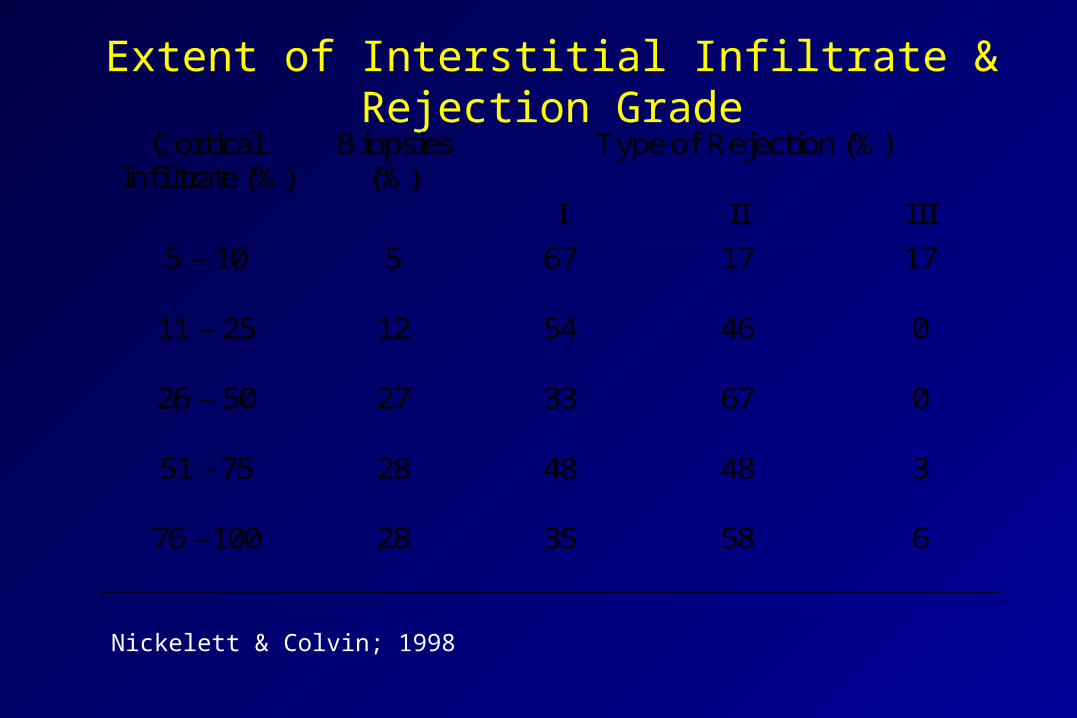
Extent of Interstitial Infiltrate & Rejection GradeCortical
Infiltrate (%)Biopsies
(%)Type of Rejection (%)
I II III
5 – 10 5 67 17 17
11 – 25 12 54 46 0
26 – 50 27 33 67 0
51 - 75 28 48 48 3
76 - 100 28 35 58 6
Nickelett & Colvin; 1998
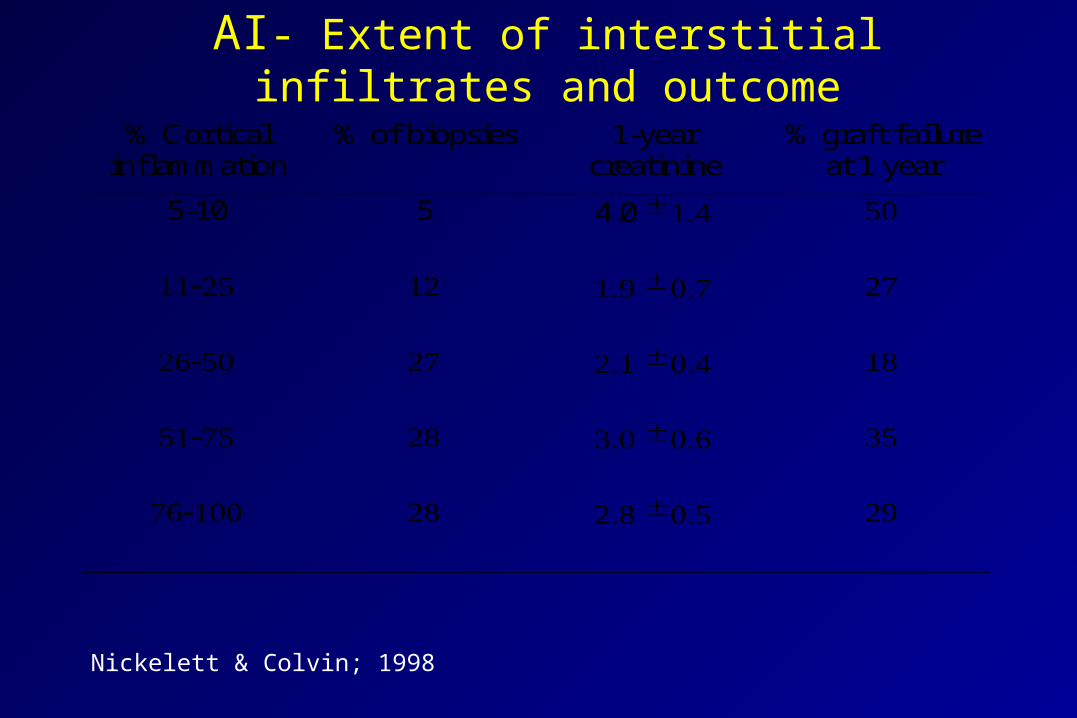
AI- Extent of interstitial infiltrates and outcome
% Corticalinflammation
% of biopsies 1-yearcreatinine
% graft failureat 1 year
5-10 5 4.0 ± 1.4 50
11-25 12 1.9 ± 0.7 27
26-50 27 2.1 ± 0.4 18
51-75 28 3.0 ± 0.6 35
76-100 28 2.8 ± 0.5 29
Nickelett & Colvin; 1998
Interstitial inflammation/infiltration Variables
• Cell Types in the interstitial infiltrates– Activated lymphocytes
– Monocytes
– Plasma cells
– Eosinophils
• Surface area involved• Edema
Tubular Injury Scores
Acute tubular injury• CCTT group identified tubular injury as a significant
parameter in determining severity of acute rejection • Tubulitis scores tended to be higher in patients with OKT3
failure, and identified higher T scores for partially reversed and irreversible rejection compared to completely reversed rejection- UT
• Mild or moderate tubulitis (Banff 97 IA) have better prognosis than acute cellular rejection with severe tubulitis (Banff 97 IB). No differences between acute rejection with t3 (Banff IB) and rejection with mild vasculitis v 1(Banff IIA) in terms of rejection reversal, 12-month creatinine or graft loss. Randhawa, AST 2000
Scores for Tubulitis
• Post rejection biopsy scores• Severe tubulitis with very mild inflammation• Acute tubular necorsis + tubulitis
Acute Glomerulitis Scores
Glomerulitis
• Kashgarian recognized the significance of endothelial swelling and glomerular inflammation alongside with vascular pathology
• Scores for G were higher in the irreversible and partially reversible rejection, and in steroid resistant rejection. Higher glomerular scores for patients with recurrent rejections (NS). UT
• Glomeruliits more in first rejection, patients with delayed graft function and has worse outcome than G0 rejection. Racusen AST, 2000
• Glomerulitis distinguished patients with Bo that progressed to rejection
Glomerulitis Scores
• Glomerulitis and Antibody-mediated rejection• Glomerular necorsis and thrombosis in TMA• Is it a sign of a unique or a severe rejection?
Scores and Sum Consensus
Sum scores in Clinical Practice
• Excellent correlation between grades of rejection and response to therapy, outcome parameters
• Although scores in most cases correlate the grade of rejection, they are not to be used for therapeutic decisions
• Incorporation of scores in the reports is optional, but highly recommended for data accession and retrieval in academic centers
• Inclusion of scores and sum of rejection is encouraged – Forces compulsive and methodical analysis of the morphologic
features
– Easy method to scan the pathology report for rejection severity in the different compartments
Sum Scores in Clinical Trials
• It is strongly recommended for clinical trials for meaningful statistical analysis of morphologic features
• Potential application in clinical trials– Fibrosis at 6 mo-2 years is an appropriate surrogate endpoint in
chronic rejection trials
– Not necessary for inclusion, but they may be important to thoroughly compare both arms in a study
– Endpoint analysis
– Control sample size and followup period
Vascular scores
• Need 4 arteries to increase the sensitivity for the detected of intimal arteritis
• Number of arteries affected by inflammation does not impact therapy response or graft survival
• Adhesion of mononuclear cells to activated endothelium correlates with steroid failure. Should we add suspicious for acute vascular rejection or include it with Type IIA. Type IB and IIA act similarly!
Glomerulitis
• Underdiagnosed entity• Highly associated with Ab-mediated rejection and feature
of borderline progressing to acute rejection. May identify a subset of acute rejection. May be the predecessor for chronic transplant glomerulopathy
• Should we use CD68?
Tubulitis
• Rejection with severe tubulitis acts similar to mild vascular rejection
Interstitial Inflammation
• Continue to specify and flag cell types• Mononuclear cell score?
Chronicity scores• Interstitial fibrosis
– Recommend evaluation by trichrome/sirius red
– Morphometric assessment for studies is recommended
• Chronic transplant vasculopathy– Types
• Inactive sclerosing transplant vasculopathy
• Proliferative sclerosing vasculopathy
• Foam cell
– Elastic stains or conventional stains adequate?
• Chronic rejection with TV is more aggressive. Socres for RTV may need to be adjusted?
• Glomerular pathology specify obsolescent/solidified/FSGS
C4D Staining
• Do we need to incorporate in the sum?• What is the value to be assigned?
Sum Scores
• Not ideal to represent the rejection severity or reflect on the pathogenesis of rejection. Linear parameter and does not take into account the varying relative strength of its components in the assessment of rejection severity
• Design a more mathematically correct parameter?• Combined clinical and Morphological index?
Scoring of lesions in renal allograft biopsies: Durand et al
• Interstitial Infiltration+ mild and focal
++ severe but focal
+++ diffuse
• Arterial Lesions+ endothelial swelling
++ intimal proliferation; fibrinoid necrosis
+++ subtotal occlusion or thrombosis
• Tubular Lesions+ 25-50%
++ 50-75%
+++ 75-100%
• Infarction+ PTC congestion
++ interstitial space infarction
+++ diffuse necrosis
• Interstitial Edema• Venous Dilatation
Durand et al , 1983
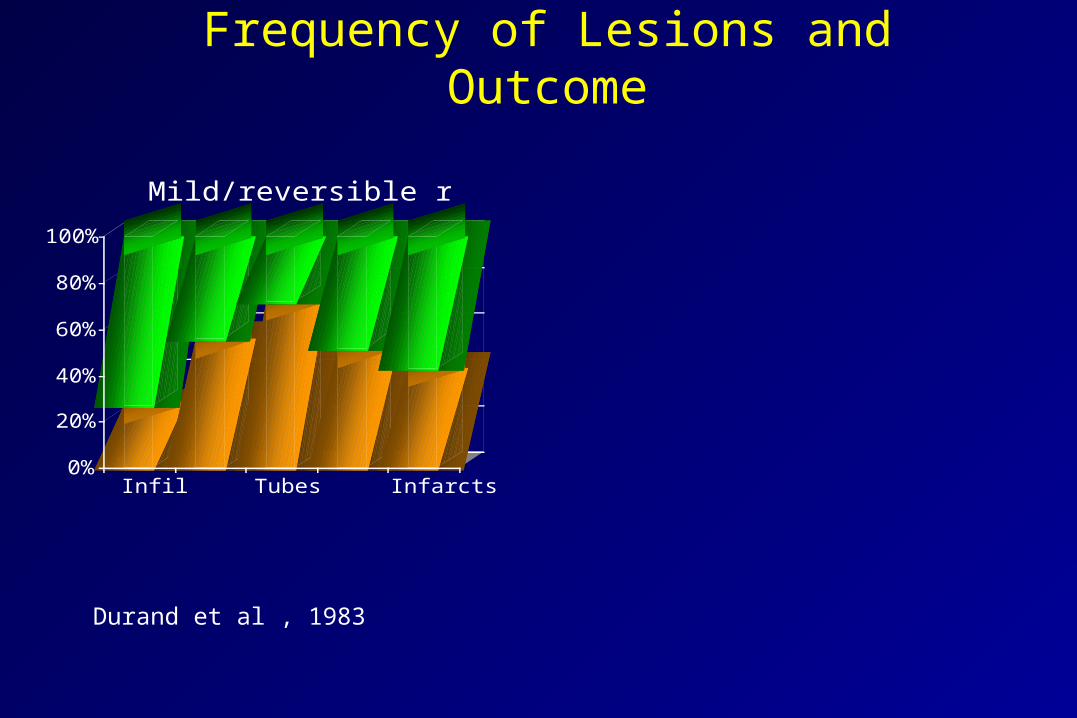
Frequency of Lesions and Outcome
0%
20%
40%
60%
80%
100%
Infil Tubes Infarcts
Mild/reversible rejection
Durand et al , 1983
Durand et al , 1983
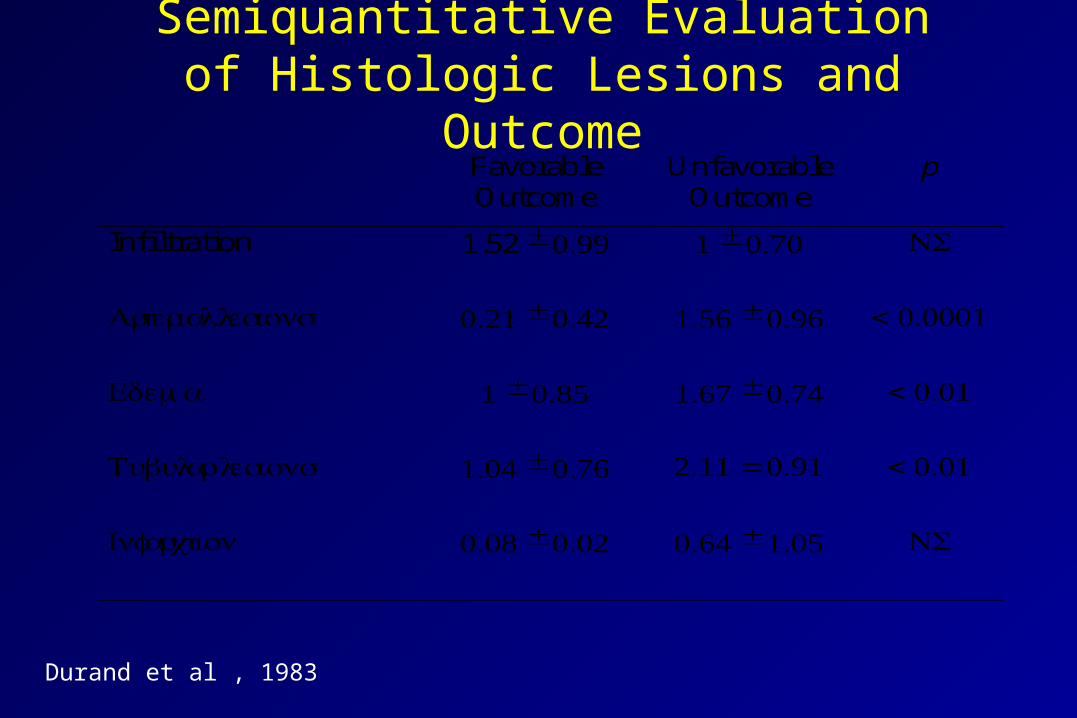
Semiquantitative Evaluation of Histologic Lesions and Outcome
FavorableOutcome
UnfavorableOutcome
p
Infiltration 1.52 ± 0.99 1 ± 0.70 NS
Arterial lesions 0.21 ± 0.42 1.56 ± 0.96 < 0.0001
Edema 1 ± 0.85 1.67 ± 0.74 < 0.01
Tubular lesions 1.04 ± 0.76 2.11 = 0.91 < 0.01
Infarction 0.08 ± 0.02 0.64 ± 1.05 NS
Scoring of lesions in renal allograft biopsies: Durand et al
• Discriminative analysis of the major histologic features for their effect on prognosis lead to the generation of a linear combination
• (0.66 x infiltrate score) - (1.98 arterial score) - (0.42 edema score) - (1.28 tubular score) - (0.78 infarction score) + 3.21
• when the combination was positive, the outcome was favorable in 83% of patients i.e. one year serum creatinine.
• Durand et al , 1983


















