Suicide and Self Harm – Mental Wellbeing in Young People Shona Straiton & Morna Johnston
Suicide and Self-harm in Gloucestershire
Alice Walsh
Acting Director of Public Health

Contents of presentation • Definitions
• Contributory factors
• Addressing the issue (nationally & locally)
• Patterns of suicide in Gloucestershire
• Suicide in Children and Young People
• Preventing suicide – what the evidence says
• Self harm / patterns of self harm in Gloucestershire
• Suicide – precipitating events (triggers)
• Suicide prevention model
• Conclusions

Definition
Suicide – intentionally ending one’s life
• Coroner pronouncement, clear evidence
• Official statistics: suicides and open verdicts (undetermined injuries)
Self-harm – intentionally damaging or injuring one’s body
• Coping with distress
• Different degrees of risk to life

Contributory Factors in suicide
Varied and complex – no single preventive measure. Factors include:
• Gender
• Age
• Mental illness
• Physically disabling/painful illnesses
Substance misuse
Job loss
Imprisonment
Debt
Living alone/social exclusion/isolation
Family breakdown & conflict/family

Addressing the Issue of Suicide National :
• Suicide Prevention Strategy 2012 with twin objectives:
• Reduction in suicide rate in general population
• Better support for people bereaved/affected by suicide
Local:
• Gloucestershire Suicide Prevention Strategy 2011-15
• Gloucestershire Health and Wellbeing Strategy
• Gloucestershire Mental Health & Wellbeing Strategy

Governance Structure 1. Gloucestershire Suicide prevention Partnership Forum (GSPPF)
-Key stakeholders across statutory and VCS
-Develop and deliver strategy and action plan
-Task & Finish Groups
2. Gloucestershire Mental Health Local Implementation Team/Gloucestershire Mental Health and Wellbeing Partnership
-Gloucestershire Mental Health and Wellbeing Strategy
-Receives report of GSPPF
3. Joint Commissioning Partnership
-Receives report of Mental Health LIT/Mental Health & Wellbeing Partnership
4. Health and Wellbeing Board
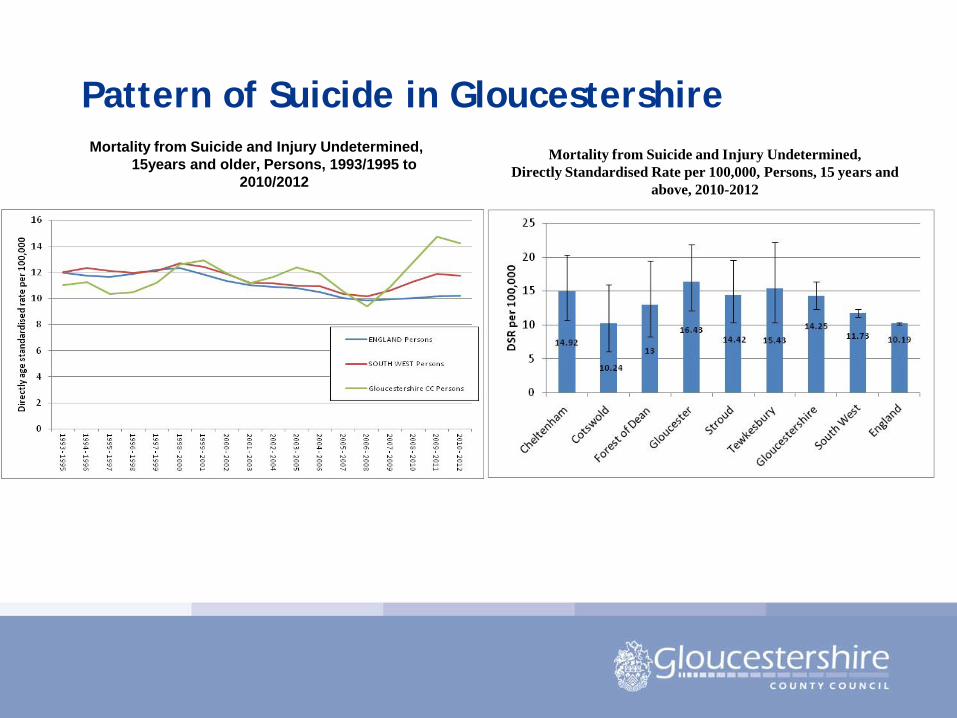
Pattern of Suicide in Gloucestershire Mortality from Suicide and Injury Undetermined,
15years and older, Persons, 1993/1995 to 2010/2012
Mortality from Suicide and Injury Undetermined, Directly Standardised Rate per 100,000, Persons, 15 years and
above, 2010-2012

Pattern of Suicide in Gloucestershire (2009-2012) (1)
Suicides and Injury Undetermined in Gloucestershire by Age Band, 2009-2012
Suicide Methods in Gloucestershire, 2009-2012
Pattern of Suicide in Gloucestershire (2009-2012) II
Where in Gloucestershire?* • 60% occur at home
‘Hotspot’ areas include: • Rivers
• canals
• multi storey car parks
• railway tracks
• stations
• 66.3% did not have any known previous contact with mental health services
• 31% had a lifetime history of self harm
• 74% no previous suicide attempt
NB: Coroners comments:
• 72% not related to mental illness
*2008-2010 time period

Suicides in Young People (I) Max. two or three annually – six deaths in a year in the past,
Four suspected suicides in 2012
Child Death Review Process (deaths in children up to 18 years in 2012 & 2013:
Information from most recent 7 deaths from the Child Death Review Process (CDRP) (up to 18 years) shows:
• 6 were male
• Family discord / relationship problems and bullying were thought to be factors in 57% of deaths
• A few were known to MH services –note CDRP did not think mental illness was a factor in these specific deaths

Suicides in Young People (Jan 2008-Jan 2013)(2) Other important factors (across SW region):
• Concerns in various settings about emotional or mental health
• Evidence for low self-worth
• Relationship difficulties
• Previous threat of self-harm or suicidal ideation
• Previous self-harm
• Being known to police/courts/social care
• Internet searches for suicide methods
• Some discussion within their peer group about suicide
• Triggering event – family row, worsening of relationship difficulties

‘Near Misses’ in Young People
Monitoring by C&YP T&F Group following 2012 deaths – of 15 incidents since then:
• No obvious gender differences
• 87% attempted hanging/strangulation
• One third under 15 years
• 60% had not presented to mental health services
• Other factors: child protection concerns, family discord, sibling history of suicide, previous admission for overdose/self-harm

Preventing Suicide – What the evidence says
• Broad international consensus that many suicides are preventable at a population level
• No clear ways to predict and prevent suicidal behaviour at individual level
Most effective strategies:
• combine with wider work addressing social and other determinants of poor health
• Build population resilience and social connectedness in communities
• Increase individual resilience across the life course

Examples of Action to prevent suicide by CYP T&F Group • Working with schools providing resources and sources of
support
• Developing curriculum resources (Key Stage 4 resources and ‘Safe, healthy relationship’ curriculum (Key Stage 1-5)
• Resources for professional (little Red Book)
• Developing referral pathways for all professionals
• Surveillance – through On Line Pupil Survey
• Developing Suicide prevention ‘app’ focussing on CYP
• Expand Youth Mental Health First Aid Training
• PH Campaign May 2014

Suicide methods most amenable to intervention
• Hanging/strangulation in CJS & in-patient settings
• Self Poisoning
• Deaths at high risk locations
• Deaths on the rail or underground networks
Local work:
• 2g NHSFT – constantly implementing measures to prevent suicide
• CCG; GHFT & 2g NHSFT – reviewing self harm clinical pathways
• ‘Hotspots’ multi-agency T&F Group established under GSPPF

Self Harm – All Ages
• Common – often hidden problem
• Admission data shows tip of the iceberg
• Increased risk of suicide (3-4% of self harm admissions will die of suicide in 10-12 years)
• Rates higher in females
• Across all ages and social classes, some high risk groups
• Incidence increasing over last 20 years

Patterns of Self Harm in Gloucestershire County self harm rates are significantly worse than English average
Districts comparisons with England average:
• Gloucester, Cheltenham & Stroud = significantly worse
• Cotswold, FOD = significantly better
• Gloucestershire has shown sustained increase in admissions since 2005
• Mostly (60%) female; 85% by poisoning
• Age: Peak in teenagers, secondary peak in late 20’s and 40’s
• Deprivation: 49% from most deprived deciles in county

Suicide - Precipitating Events (Triggers)
• Risk Factors e.g: MH problems / gender / family problems / substance misuse
• Warning Signs: e.g: Hopelessness / feeling trapped/ social withdrawal / no sense of purpose etc.
• Tipping Point: e.g: relationship ending/loss of status/ debilitating physical illness/ abused bullying etc.
• Imminent Risk: e.g: Expressed intent to die; plan in mind; access to lethal means; impulsive, aggressive behaviour
Source: Department of Health and Ageing, Australian Government
Suicide prevention model Evidence suggests suicide prevention model should include
activities aimed at:
• The broader population
• Specific ‘at risk’ groups
• Individuals who may be at risk
And informed by knowledge of:
• Risk and protective behaviours (individual; social & contextual)
• Resilience and vulnerability
• Impact of interaction of personal factors, life events, including MH
• Warning signs and tipping points

Conclusion (1)
• Causes of suicide are varied and complex
• Rates of suicide & self harm are increasing nationally, regionally and locally
• Most not in contact with MH services in 12 months before death
• No single preventative factor – evidence strongly suggests association with unemployment
• No clear ways to predict and prevent suicidal behaviour at individual level
• Interventions need to address wider determinants & be wide ranging
Conclusion (2)
• Increasing demand for CYP MH services generally is challenging supply and is being explored
• Need to build population resilience across life course
• Intervening at an individual level is more challenging
• There is local awareness of issues
• Work is underway and monitored within existing partnership structures