Sue Hayward Chief Nursing and Midwifery Officer Waikato ... · 2 Contents 1 Introduction 4 1.2...
20
Sue Hayward Chief Nursing and Midwifery Officer Waikato District Health Board
Transcript of Sue Hayward Chief Nursing and Midwifery Officer Waikato ... · 2 Contents 1 Introduction 4 1.2...

Sue Hayward
Chief Nursing and Midwifery Officer
Waikato District Health Board

2
Contents
1 Introduction 4
1.2 Vision 4
1.2 Waikato DHB’s strategic imperatives 4
2 Accountability 5
3 Expectations 6
3.1 Midwifery clinical decision-making and documentation 7
3.2 Partnership care 8
3.3 Bedside handover 9
3.4 Intentional Rounding 9
3.5 Releasing Time to Care 9
3.6 Assignment workload manager 9
3.7 Professional development framework 10
4 Summary 11
5 Strategic aims 12
Strategic aim 1 12
Strategic aim 2 13
Strategic aim 3 14
Strategic aim 4 15
Professional development framework for midwifery 16
Professional development framework for moving into designated senior midwifery roles 17
Role expectations for designated senior midwifery roles 18
Reference list 20

3
People at heartTe iwi Ngakaunui
Give and earn respect – Whakamana
Listen to me; talk to me – Whakarongo
Fair play – Mauri Pai
Growing the good – Whakapakari
Stronger together – Kotahitanga
Values
Pae taum
ata Ratonga a iwi Manaaki
H
aum
aru
Effective and efficient care and services
People centred services
A centre of excellence in learning,
training, research,
and innovation
Safe, quality health
services for all
Health equity for high need
populations
Productive partnerships
Whanaketang
a
O
rang
a
VisionHealthy people. Excellent care
MissionEnable us all to manage our health and wellbeing
Provide excellent care through smarter, innovative delivery
Waikato DHB Strategy

4
1 Introduction1.2 VisionThe vision, Healthy People, Excellent Care has been set by the Waikato District Health Board (Waikato DHB) and Executive Group following engagement and consultation with wider groups. This is the vision when working at the Waikato DHB we all work towards achieving. The skills and knowledge midwives hold and use in care delivery contribute to achieving this vision. Commitment to working together with other members of the health care team in a manner that women and their families find acceptable will make this vision achievable.
1.2 Waikato DHB’s strategic imperativesEach midwife must use their knowledge and skills whether as a beginner or experienced practitioner, in a way that supports and improves maternity care and the clients’ experience. To guide in prioritising where care delivery is to be focused:
• Achieving health equity for high needs population
• Ensuring quality health services for all
• Providing people centred care
• Delivering effective and efficient care and services
• Becoming a centre of excellence in teaching training and research
• Developing productive partnerships
The four midwifery strategic aims (pages 12-15) align with the DHBs strategic imperatives. These aims provide the direction for the next five years. The actions needed to achieve the aims can be utilised by midwives either individually or as part of the wider team. Utilising these provides a mechanism to support individual accountability with evidence informing performance reviews and the setting of objectives. The DHB imperatives inform the direction and activities of the DHB, the midwifery strategic aims indicate how they can be achieved. Midwifery practice contributes to and influences the success of each of the DHB imperatives.

5
2 AccountabilityEach midwife is accountable for their practice, they are also accountable as members of the health care team to know and understand how they influence achievements both clinically and organisationally. Accountability is the requirement to demonstrate and take responsibility for performance; this is both as an individual and as part of a health care team. In order to ensure understanding of accountability the following describes the principles and supporting structures:
• Expectations are clarified and understood: Midwifery at Waikato 2017-2021, position descriptions and the professional development frameworks all describe levels of expectations and minimum requirements of midwifery roles.
• Decisions are transparent and rational: policies governing practise, professional behaviours and evidenced based clinical protocols are in place and accessible e.g. policies housed on the DHBs intranet site, Lippincott Clinical Procedures etc.
• Feedback is the expected norm: yearly performance appraisals support and provide ongoing guidance and real time feedback should be given by managers and peers.
• Responsibility is understood and accepted: each midwife must be cognisant of their scope of practice: Position Descriptions indicate levels of authority and participation in the Quality Leadership Programme is encouraged to provide evidence of how responsibility is demonstrated.
• Continuous improvement is in place: utilising, engaging with and driving changes and improvement through the Quality and Patient Safety agenda as well as Releasing Time to Care ensures that individuals and teams are accountable for outcome aligned to practice and organisational design.
Each identified senior midwifery role is allocated key activities to achieve the strategic imperatives with these also aligning with accountabilities.
Waikato DHB is committed to a Just Culture. The DHB is supporting this through the designing of safe systems, managing behavioural choices and creating a learning culture. It is the balancing of the need to learn from mistakes and the need to take disciplinary action that will promote organisational and individual accountability through just and fair consequences.

6
3 ExpectationsEach midwife must be cognisant of their scope of practice as defined by the Midwifery Council of New Zealand (MCNZ), work within the MCNZ Code of Conduct and understand how to develop therapeutic relationships without breaching professional boundaries. www.midwiferycouncil.health.nz/midwives
Delivering care in a culturally competent manner is an absolute expectation, indicating an understanding commitment and active engagement with patients/service users and colleagues. Building on this, cultural humility as described by Trevalon & Murray-Garcia (1998) further supports lifelong commitment to self-evaluation and understanding how relational dynamics that occur between the midwife and women can affect how the health care delivered is accepted.
The following outlines expectations placed on midwives relating to quality of care, providing women centred care, providing effective care delivery processes, remaining current in knowledge, advancing practice and working in partnership with women and their families and our health colleagues. Minimum standards of care, knowledge acquisition, career progression and importantly the manner in which care is delivered are described, and are to be considered standards that are not negotiable.
Supporting these expectations, education and learning required to keep midwives clinically sound and opportunities to extend the way individual midwives may aspire to achieve, are provided via the Professional Development Unit. The Nursing and Midwifery Directorate is committed to the use of Practice Development methodology as it brings together sustainable evidenced, approaches to deliver measurable outcomes that make a difference in practice and can add to the body of knowledge. Practice Development methodologies support the transfer of many types of knowledge from learning to practice. Adopting person centred active learning; it is a facilitated process that makes use of critical reflection and generative discussion.
Midwives employed by Waikato DHB work in primary, secondary and tertiary maternity settings and contribute to the maternity client’s journey through her pregnancy, birth and postnatal experience. Midwives care for women and their babies holistically in whatever setting.
Specific workforce challenges exist for the acute services in which secondary/tertiary midwives practice at Waikato DHB. The fast turnover of clients coupled with high acuity pose particular challenges around recruitment and retention. Midwives contributed to a profile to celebrate their work setting.
Reducing client/patient/service user harm and suffering is the ultimate aim for all health workers. The Nursing and Midwifery Directorate has chosen the overarching framework Compassionate Connected Care (3Cs) as a way to equip midwives with the understanding of how midwifery care and organisational requirements can be merged and support the DHBs strategic imperatives. This framework described by Dempsey Wojciechowski, McConville and Drain,(2014) integrates the clinical, operational, cultural and behavioural aspects of care delivery and provides a way to work so all aspects of organisational requirements are met, while addressing the challenges faced to reduce client suffering or harm.
As described by Dempsey et al inherent suffering is often not preventable as this occurs because of the diagnosis and sometimes then by the treatment which can be painful or uncomfortable and generally causes a disruption to normal life. It is the avoidable suffering midwives can reduce, as this

7
Clinical excellenceConnecting clinical
excellence with outcomes
Operational efficiencyConnecting efficiency
with quality
Caring behaviourConnecting
engagement with action
Organisational cultureConnecting mission, vision and value with
engagement
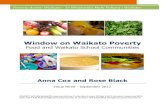
Compassionate connected care
Table 1:JONA Vol 44 no.10 (2014)
is associated with unmanaged pain, medication error, hospital acquired pressure injury (rare, but occurring in maternity), a fall or being treated without dignity and respect.
The domains of the 3Cs (Table 1) provides a visualisation of how each component can be supported by connecting actions with outcomes.
Clinical excellence links to outcomes, operational efficiency and quality, caring behaviours to the service user’s experience and culturally to the DHBs vision Healthy People Excellent Care. The central component is; all care is delivered with compassion, with an understanding of what outcomes (goals) are being aimed for, being aware of how the care will be perceived by the woman, keeping quality at the forefront and knowing that by doing this the DHBs values are supported.
The Compassionate Connected Care framework guides the systems and process needed to support the work of midwives. These systems and processes are not an addition to midwifery work but should be viewed as essential and integrated structures allowing midwifery to be delivered effectively during the peaks and troughs of clinical demand.
The programmes of work and models of care delivery that support midwives and are expected to be utilised are described next:
3.1 Midwifery clinical decision-making and documentation The midwife bases her clinical decision-making upon making an assessment, plan interventions required, followed by an evaluation of the effectiveness of the intervention. The midwife enables the client to set her own goals and document these in the appropriate documentation, e.g. birth plan, care plan. Midwives fully utilise the documents specified in the setting where they work. For example, in the inpatient setting the antenatal – or postnatal care plan will reflect the midwifery assessment and supports the planning and intervention stage. The evaluation of the care delivered, outcomes and any escalation undertaken are always documented in the clinical notes.

8
3.2 Partnership care
Supporting clinical excellence and operational efficiency the model of clinical service delivery within inpatient wards is “Partnership Care”. This model while still having elements of allocation has the midwives and nurses on each shift working in defined teams caring for a group of clients. The teams can consist of a mix of Registered Midwife, Registered Nurse, Enroled Nurse, Health Care Assistants. At the very minimum each team must:
• introduce themselves to their clients
• equitable work load in terms of acuity, (this is not necessarily the same as numbers)
• some knowledge of all the clients their team is caring for
• have planned support for high intensity interventions/procedures
• team based or ward based huddles
• staggered meal relief.
The teams must work in a culture that encourages case discussions and joint decision making around complex care planning and use opportunities that are presented to share knowledge. Working in Partnership Care permits the midwife/nurse to seek advice from colleagues when confronted with any aspect of clinical care that may need clarifying, or require a higher knowledge level or skill than they have at that point in time.

9
3.3 Bedside handoverThe DHB’s policy is set out in the Clinical Handover (Bedside Handover) for Nursing and Midwifery procedure.
Supporting caring behaviour and engagement, this hand over process is to be carried out between shifts over the 24 hour period. Bedside handover actively includes the client and her Lead Maternity Carer if present using the Situation, Background, Assessment, Recommendation and Response (SBARR) communication tool to ensure a cohesive handover of information occurs. The client being part of the handover must be given the opportunity to participate and confirm that the information is correct.
3.4 Intentional Rounding The DHB’s policy is set out in the Interntional Rounding procedure.
Supporting all four domains of the CCC (3Cs) framework, Intentional Rounding is the process used to ensure every patient regardless of their acuity is seen and interacted with on a regular basis. Utilising Intentional Rounding in the maternity service allows clients the comfort and confidence that they will be seen at the very least every two hours. While essential aspects of care such as managing pain, assisting with personal needs and positioning are always to be addressed, other areas related to the client’s clinical needs are also included. Documented activities are noted in the care plan and evaluation of the care delivered is documented in the clinical notes.
3.5 Releasing Time to Care (RTC)Supporting all four domains of the CCC (3CS) framework, Releasing Time to Care (RTC) is a series of processes that enable midwives to create a working environment that is efficient, streamlined and gives more time to focus on midwifery care. The RTC methodology helps support quality and patient safety initiatives, whether local or global, provide the mechanism that improves audit results while giving midwives on the floor the opportunity to drive the changes needed in order to improve their practice environment and safety for women and their babies.
Every midwife must at the very least be aware of what activities are occurring within productives in their area, and for those with the increased enthusiasm and ability to drive change then engagement is most welcomed.
3.6 Assignment workload manager
Supporting operational efficiency and clinical excellence, Assignment Workload Manager (AWM) is the acuity tool the Waikato DHB is utilising that measures the work of midwives and nurses and then translate to rostering the right skill mix and number to match patient demand (i.e. numbers acuity and dependency). Entering the data while a CMM responsibility is delegated to appropriate midwives/nurses on each shift, and as such learning how to do this is essential. Understanding how the data is entered and how the calculations are created increases individual midwife/nurse’s opportunity to influence how this tool can be used in order to smooth out staffing variances, allocate the right team of staff to the acuity of inpatients rather than to number of patients, plan activity associated with high intensity treatments and planning breaks.

10
3.7 Professional development frameworkEvery midwife must be aware of the Career Path framework and the minimum standards of knowledge and skills in practice expected of them dependent on years of practise. Achieving these and being engaged in quality and patient safety activities promotes a confident and competent midwifery workforce able to deliver the clinical care required to meet the needs of the maternity population.
Participating in the Quality and Leadership Programme (QLP)For Waikato DHB employees, more information is available in the Developing Our Staff section of the staff intranet.QLP provides the evidence midwives and their managers can use both as a way of advancing careers and receiving monetary acknowledgment of the contribution the midwife makes to client care. While participation in the QLP is not compulsory, for appointment to a senior midwifery role the minimum requirement for interview is achievement to the leadership domain on the QLP.

11
4 SummaryEvery midwife working within the Waikato DHB is accountable for their own practise, responsible for understanding their scope as described by the Midwifery Council of NZ, expected to work in a caring compassionate manner and at the very least understand how their contributions to client safety and outcomes are connected to their own personal values, the clinical areas values and those of the DHB.
Midwives are a highly valuable component in the delivery of maternity care, and integral to the clinical team. Midwives are encouraged and to be congratulated when they lead where they stand.
The Nursing and Midwifery Directorate is in place and committed to support midwives to achieve the best outcomes possible for their clients, to provide advice and opportunities to extend and expand knowledge and skill acquisition during their career.

12
STRATEGIC AIM 1:Lead and apply a strong midwifery culture which harnesses and values the contribution of midwives
Key objectives Outcome measures
Facilitate and apply leadership competencies for senior midwives that meet organisational requirements
• Organisations vision and values are demonstrated in the care environment
• Visibility and presence of midwives exist within all patient and staff safety forums
• Competencies have been identified and inserted in position descriptions
• Senior midwives are responsive to KPIs and data from audit to drive ongoing quality improvements
• PDU activities align with leadership development
Midwifery contribution to quality and patient safety will be demonstrated
• Releasing Time to Care series is implemented in a way that will show an increase in direct client care
• The skill mix for each ward/department is defined and matches patient demand (throughput) and predicted acuity or dependency
• Hand Hygiene audits reflect best practise and meeting target
• Culturally competent midwifery workforce as per the Midwifery Council statement in order to meet the needs of our Maori and culturally diverse population
5 Strategic aimsThe following four strategic aims are specific to midwifery while supporting the DHB strategic imperatives. The objectives and outcome measures indicate what we are to achieve and how success will be viewed.

13
STRATEGIC AIM 2:Build workforce capability, readiness and capacity
Key objectives Outcome measures
Ensure a continuation of advanced roles and midwifery-led services to meet organisation requirements
• Each service has identified the roles required to provide safe care presently and into the near future
• Advanced roles have clear quality assurance frameworks e.g. credentialing, QLP
• Senior and advanced midwifery roles can describe their contribution to the model of care for improving population health outcomes
Establish the ‘entry workforce’ numbers, type and processes needed to sustain the midwifery workforce
• Evidence of collaboration with Wintec to ensure student numbers and quality reflect the population need
• A sustainable process that achieves intakes of an agreed number of midwifery graduates to maintain the employed midwifery workforce
• Employed graduate midwives are supported through preceptorship, education and mentoring. Graduate LMCs are supported when they access the secondary care facility
• Midwifery workforce reflects the demographics of our population

14
STRATEGIC AIM 3:Midwifery uses and contributes to the delivery of effective health care based in research and acknowledged best practice
Key objectives Outcome measures
Develop, influence and implement processes that ensure maternity and newborn service users will receive safe and effective care
• Patient safety programmes have been implemented inclusive of:
- Releasing Time to Care
- Falls Minimisation
- Early Deterioration Detection System (ADDS) (Obstetric Early Warning Score, Primary Maternity ADDS and Newborn observation chart)
- Care Standards
- Organisational Audits
- Role imperatives
- Hand Hygiene practices
- Medication Safety
- Hospital acquired pressure ulcers
- Utilisation of evidence based midwifery procedures
• Risk minimisation is evident
• Midwives participate in research that contribute to the body of knowledge and inform midwifery practice
Demonstrate that midwifery practice is based in contemporary best practice
• Education plans are linked to learning needs assessments and workforce design. Training resources have been made available to primary maternity providers and NGOs
• Staff has access to policies and procedures that are up to date, consistent across the DHBs and based on evidence
• Results from patient safety programme reflect acceptable outcomes as per national and international benchmarking
• Implement culture of learning (based on DEU principles1) as the preferred midwifery student learning experience
• Integrate the use of virtual health delivery into learning programmes
1E.g. dedicated preceptor, increased in-practice presence from DHB and Wintec etc.

15
STRATEGIC AIM 4:Improve care coordination across the health continuum to enhance timely access to health care for the Waikato population
Key objectives Outcome measures
In collaboration with key stakeholders, develop and implement primary- and rural midwifery strategies to meet key requirements of communities and new models of care
• Develop and implement integrated rural – and primary maternity models of care in conjunction with LMCs and key stakeholders to enable sustainability of service delivery and founded on continuity of care and the needs of women
• Develop processes that support ambulatory care and avoid unnecessary hospital admissions during pregnancy
• Develop a sustainable and flexible midwifery workforce
• Build and strengthen alliances across and within the maternity sector, including education, NGOs, primary, secondary and tertiary care
• Virtual Health Strategy and its delivery are integrated into models of care
• Developing models of service delivery that are inclusive of virtual health technologies
Implement smooth patient journeys across health settings
• Midwifery led discharge is utilised from postnatal inpatient secondary care
• Midwifery led clinics developed and implemented with evidence of quality service delivery
• Inter/intra- hospital transfer/retrievals occur in a timely and safe way
• Two-way communication between maternity services and LMCs occur in a timely, appropriate and effective way
• Virtual health technologies are increasingly explored to support clinical care delivery

16
Professional development framework for midwifery
PR
OF
ES
SIO
NA
L D
EV
ELO
PM
EN
T F
RA
ME
WO
RK
FO
R M
IDW
IVE
SP
RO
FE
SS
ION
AL
DE
VE
LOP
ME
NT
FR
AM
EW
OR
K F
OR
MID
WIV
ES
Clin
ical
ex
celle
nce
Con
nect
ing
clin
ical
ex
celle
nce
with
ou
tcom
es
Op
erat
iona
l ef
ficie
ncy
Con
nect
ing
effic
ienc
y w
ith
qual
ity
Car
ing
beh
avio
urC
onne
ctin
g en
gage
men
t with
ac
tion
Org
anis
ing
cu
lture
Con
nect
ing
mis
sion
, vis
ion
and
valu
e w
ith
enga
gem
ent
Compassi
onat
e co
nnec
ted
care
………
lead
ersh
ipM
idw
ife
confi
den
tM
idw
ife
com
pet
ent
Mid
wife
Tikanga Māori
Tikanga Māori
Tika
nga
Māo
ri Tikanga Māori
CM
S- la
ctat
ion/
dia
bete
s/ b
erea
vem
ent
Lact
atio
n C
onsu
ltant
Com
plex
car
e sp
ecia
list
Rev
iew
ers
/ ass
esso
rs (
MSR
/ Q
LP)
Con
fere
nce
pres
enta
tions
Flig
ht m
idw
ife/ l
ead
prec
epto
rsC
ham
pion
s –
prot
ocol
/Au
dits
/
Res
earc
h m
idw
ifeN
Z Q
& S
rep
Mid
/cou
ncil
role
s-
advi
sors
/Exp
ert
witn
ess
Reg
iona
l rol
es (
nzco
m c
hair,
m
idla
nd s
ubgr
oup
mem
ber chai
r)M
ento
rsR
evie
wer
s / a
sses
sors
( M
SR /
QLP
)C
ham
pion
s ( R
TC/S
mok
ing/
slee
p/in
fect
ion
cont
rol/Q
& R
/FV
)
Cha
mpi
ons
LMC
- w
ith e
xper
ienc
e in
fina
nce/
team
and
bus
ines
s m
anag
emen
tSh
ift c
oord
inat
orAC
MM
CM
M MM AD
OM
Cha
mpi
ons
-FV/
Smok
ing/
Q &
RU
nit t
each
ing-
info
rmal
or
form
alPr
ecep
tor
Con
fere
nce
pres
ente
rQ
LP C
oach
and
or A
sses
sor
NLS
inst
ruct
or ,
Chi
ldbi
rth e
duca
tor
Mid
wife
pro
gram
me
coor
dina
tor (
pepi
pods
)Ed
ucat
or /t
utor
s

17
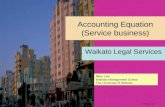
Professional development framework for moving into designated senior midwifery roles
PR
OF
ES
SIO
NA
L D
EV
ELO
PM
EN
T F
RA
ME
WO
RK
FO
R M
OV
ING
IN
TO
DE
SIG
NAT
ED
SE
NIO
R M
IDW
IFE
RY
RO
LES
PR
OFE
SS
ION
AL
DE
VE
LOP
ME
NT
UN
IT
Man
agem
ent
• Le
ads
out c
hang
e pr
oces
ses
and
qual
ity in
itiat
ives
• C
oord
inat
es s
hifts
an
d su
ppor
ts C
MM
• A
ctiv
e an
d ef
fect
ive
prec
epto
r
• P
artic
ipat
es in
ap
prai
sals
• In
volv
ed in
R
elea
sing
Tim
e to
C
are
QLP
Lea
ders
hip
Pos
t Gra
duat
e C
ertifi
cate
and
Pos
t Gra
duat
e D
iplo
ma
Clin
ical
• Id
entifi
ed a
s a
clin
ical
reso
urce
• Is
a c
ham
pion
for
a qu
ality
initi
ativ
e
• P
uts
chan
ge
proc
esse
s in
to
prac
tice
• P
artic
ipat
es
in p
olic
y an
d pr
oced
ure
deve
lopm
ent
Ed
ucat
ion
• Id
entifi
ed a
s a
reso
urce
for
supp
ortin
g/de
liver
ing
clin
ical
ed
ucat
ion
• A
ctiv
e an
d ef
fect
ive
prec
epto
r
• V
iew
ed a
s an
edu
catio
n ch
ampi
on fo
r ch
ange
pro
cess
es
• In
volv
ed in
R
elea
sing
Tim
e to
C
are
Res
earc
h an
d
qua
lity
• A
ctiv
ity d
eliv
erin
g w
ork
base
d te
achi
ng u
sing
re
sear
ch to
un
derp
in s
essi
ons
• Id
entifi
ed a
s an
ef
fect
ive
cham
pion
su
ppor
ting
qual
ity
and
chan
ge
proc
esse
s
• In
volv
ed in
R
elea
sing
Tim
e to
C
are
• In
volv
ed in
aud
its
Productive partnerships
A centre of excellence in learning, training, research and innovation
Effective and efficient care and services
People centred services
Safe, qualtiy health services for all
Health equity for high need populations
Harness and value midwifery contribution
Contribute to seamless continuum of care
Build workforce capability
Deliver effective, evidence based care
Dis
tric
t Hea
lth B
oard
Chi
ef N
ursi
ng a
nd M
idw
ifery
Offi
cer
Hea
lthy
Peo
ple
– E
xcel
lent
Car
e
Str
ateg
ic In
tent
Hea
lth o
f al
l New
Zea
land
ers

18
Role expectations for designated senior midwifery roles
RO
LE E
XP
EC
TAT
ION
S –
DE
SIG
NAT
ED
SE
NIO
R M
IDW
IFE
RY
RO
LES
PR
OFE
SS
ION
AL
DE
VE
LOP
ME
NT
UN
IT
Man
agem
ent
MM
• E
ffici
ent a
nd e
ffect
ive
oper
atio
nal
man
agem
ent o
f a s
ervi
ce(s
) •
Lead
ing
peop
le, s
yste
ms,
pro
cess
es a
nd
resp
onse
s to
faci
litat
e se
rvic
e de
liver
y •
Bus
ines
s, fi
nanc
ial,
hum
an re
sour
ce
plan
ning
and
man
agem
ent
• C
ontr
ibut
es to
the
deve
lopm
ent o
f or
gani
satio
nal s
trat
egic
dire
ctio
n
CM
M
• P
rovi
de c
linic
al le
ader
ship
with
in a
defi
ned
care
are
a •
Man
age
syst
ems,
pro
cess
es a
nd
reso
urce
s to
ena
ble
mid
wiv
es to
mee
t ne
eds
of p
atie
nts
• M
ay h
ave
budg
et h
oldi
ng re
spon
sibi
lity
• P
rom
otes
a q
ualit
y pr
actic
e en
viro
nmen
t th
at s
uppo
rts
dem
onst
ratio
n of
co
mpe
tenc
y an
d en
able
s sa
fe, e
ffect
ive
and
ethi
cal m
idw
ifery
pra
ctic
e
AC
MM
• S
uppo
rtiv
e ro
le to
CM
M; c
ontin
uing
clin
ical
co
ordi
natio
n an
d ex
pert
ise
to e
nabl
e an
ef
fect
ive
and
effic
ient
pra
ctic
e en
viro
nmen
t.•
Pro
vide
s cl
inic
al le
ader
ship
for
staf
f and
as
sist
s w
ith c
oach
ing
and
prof
essi
onal
su
perv
isio
n
Clin
ical
CM
S
• Fo
cus
on c
are
deliv
ery
acro
ss th
e co
ntin
uum
of
care
, pro
vidi
ng s
peci
alis
t m
idw
ifery
car
e an
d ex
pert
ise
in th
e m
anag
emen
t of a
de
fined
pat
ient
/clie
nt g
roup
•
Res
earc
hing
, eva
luat
ion,
de
velo
ping
and
im
plem
entin
g st
anda
rds
of m
idw
ifery
pra
ctic
e in
sp
ecifi
c ar
ea o
f pra
ctic
e •
Lead
s th
e de
velo
pmen
t of
path
way
s, p
roto
cols
and
gu
idel
ines
in th
e sp
ecifi
c ar
ea o
f pra
ctic
e
Clin
ical
Mid
wife
ry
Co
ord
inat
or
• C
oord
inat
es p
eopl
e,
syst
ems
and
reso
urce
s fo
r a
shift
or
grou
p to
ens
ure
serv
ice
deliv
ery
is m
et
• M
ay c
ontr
ibut
e to
coa
chin
g an
d su
perv
isio
n of
sta
ff •
Pro
mot
es a
qua
lity
envi
ronm
ent t
hat s
uppo
rts
and
faci
litat
es im
prov
ed
patie
nt o
utco
mes
and
ex
perie
nce
Ed
ucat
ion
ME
• C
ontr
ibut
e to
the
stra
tegi
c di
rect
ion
of m
idw
ifery
ed
ucat
ion
• Fo
cus
on s
kill
deve
lopm
ent a
nd e
duca
tion
of
mid
wiv
es w
ithin
clin
ical
are
as to
mee
t the
nee
ds
of c
lient
s•
Faci
litat
e le
arni
ng, d
evel
opm
ent a
nd d
eliv
ery
of
educ
atio
n in
clin
ical
and
cla
ssro
om s
ettin
gs•
Dev
elop
com
pete
ncy
and
capa
bilit
y of
the
mid
wife
ry w
orkf
orce
• P
rom
ote
an e
nviro
nmen
t tha
t con
trib
utes
to
on-g
oing
dem
onst
ratio
n an
d ev
alua
tion
of
com
pete
ncie
s•
Inte
grat
e ev
iden
ce b
ased
theo
ry a
nd b
est
prac
tice
into
edu
catio
n ac
tiviti
es
Mid
wife
C
oo
rdin
ato
r
• D
evel
op, i
mpl
emen
t and
coo
rdin
ate
spec
ific
clin
ical
, edu
catio
n an
d qu
ality
pro
gram
mes
ac
ross
Wai
kato
DH
B to
refle
ct s
trat
egic
di
rect
ion
• E
nsur
e pr
ogra
mm
es c
ontin
ue to
mee
t the
M
CN
Z ac
cred
itatio
n st
anda
rds
and/
or H
WN
Z re
quire
men
ts
• R
evie
w, i
mpl
emen
t and
eva
luat
e pr
ogra
mm
e ch
ange
s ba
sed
on re
gion
al a
nd/o
r na
tiona
l ch
ange
s •
Con
trib
ute
to s
ubm
issi
ons
on c
onsu
ltatio
n do
cum
ents
impa
ctin
g on
pro
fess
iona
ls,
prog
ram
mes
and
/or
heal
th o
f New
Zea
land
ers
Res
earc
h an
d Q
ualit
y
Mid
wife
Res
earc
her
• Le
ads
and
unde
rtak
es
mid
wife
ry o
r po
pula
tion
heal
th re
sear
ch a
nd
deve
lopm
ent a
ctiv
ity
usin
g ac
cept
ed re
sear
ch
met
hodo
logy
, loc
ally,
re
gion
ally
and
/or
natio
nally
• P
rom
otes
a re
sear
ch
envi
ronm
ent t
hat s
uppo
rts
and
faci
litat
es re
sear
ch
min
dedn
ess
and
rese
arch
ut
ilisat
ion
• S
uppo
rts
and
eval
uate
s pr
actic
e th
roug
h re
sear
ch
activ
ities
and
app
licat
ion
of e
vide
nce
base
d kn
owle
dge
Mid
wife
Co
nsul
tant
• P
rovi
des
prof
essi
onal
m
idw
ifery
adv
ice,
le
ader
ship
and
con
sulta
ncy
• In
crea
ses
effe
ctiv
enes
s of
pa
tient
car
e de
liver
y •
Lead
s qu
ality
impr
ovem
ent
• D
evel
ops
and
mai
ntai
ns
fram
ewor
ks fo
r po
licy
and
educ
atio
n•
Faci
litat
es m
idw
ifery
inpu
t in
to p
olic
y de
velo
pmen
t

19

Reference list:Demsey,C., Wojciechowski,S.,McConville,E.,& Drain,M. (2014) Reducing patient suffering through Compassionate Connected Care. Journal Nursing Administration, Oct; 44(10) 517-524.
Trevalon,M.,& Murray-Garcia,J.(1998). Cultural Humility versus Cultural Competence. Journal of Health Care for the Poor and Underserved, 9(2), 117-119
C1724HWFTM05/17