
Sudden Cardiac Death in the Older Athlete · REVIEW TOPIC OF THE WEEK Sudden Cardiac Death in the...
10
REVIEW TOPIC OF THE WEEK Sudden Cardiac Death in the Older Athlete Sumeet S. Chugh, MD,* Joseph B. Weiss, MDy ABSTRACT The overwhelming majority of sports-related sudden deaths occur among those older than 35 years of age. Because increasing numbers of older people are participating in organized endurance and competitive sporting events, the inci- dence of sports-related sudden death in older adults is expected to rise. Older athletes will approach clinical cardiologists for advice regarding their fitness for participation. It is important to recognize both that strenuous exercise is associated with a transient elevation in risk of sudden cardiac death and that appropriate training substantially reduces this risk. The approach to pre-participation screening for risk of sudden death in the older athlete is a complex issue and at present is largely focused on identifying inducible ischemia due to significant coronary disease. In this brief review, we summarize the current state of knowledge in this area with respect to epidemiology, mechanisms, and approaches to risk stratifi- cation, as viewed from the perspective of the consulting clinical cardiologist. (J Am Coll Cardiol 2015;65:493–502) © 2015 by the American College of Cardiology Foundation. T he legend of the first marathon runner, Pheidippides, embodies the popular notion that endurance athletics increase the risk of death. An Athenian messenger approximately 40 years of age, he is fabled to have run from Mara- thon to Athens in 490 B.C., perishing on arrival after proclaiming the Greek victory over the Persians. The beneficial, health-promoting effects of habitual phys- ical and sports activity are undeniable. However, a “sports paradox” exists: some people, most often those not habituated to exercise, experience sports activity–related cardiac arrests, usually associated with underlying heart disease. Middle-aged and older athletes are at significantly higher risk for sudden cardiac death (SCD) compared with younger athletes and are more vulnerable to misconceptions regarding the cardiovascular effects of sports. The burden of SCD during sports needs further evaluation but prob- ably constitutes a small proportion (5% to 6%) of sud- den deaths in the general population (1,2). However, from a societal perspective, sports-related SCD can have a disproportionate impact. People who engage in athletic activity are ostensibly healthier than most and therefore considered least likely to experi- ence a cardiac arrest. The media attention on sports- related SCD tends to exaggerate the sports paradox and obscure the global health benefits of regular exer- cise. In addition to being cardiologists, both authors of this review are dedicated long-distance runners who seek to put the clinical risks and benefits of aer- obic exercise in scientific balance. A leisure athlete is “an individual, usually middle- aged or elderly ($35 years), who participates in a variety of informal recreational sports, on either a regular or an inconsistent basis, which do not require systematic training or the pursuit of excellence” (3). For the purpose of this review, the term “older athlete” includes all athletes older than 35 years of age participating in sports at a competitive or masters level or as a leisure activity. Both clinical cardiol- ogists and their patients will benefit from a balanced approach to education, risk stratification, and exer- cise prescription for the middle-aged and older athlete. The goal of this review is to put forth such an approach on the basis of a current and compre- hensive assessment of previously published studies. From *The Heart Institute, Cedars-Sinai Medical Center, Los Angeles, California; and the yDivision of Cardiology, Warren Alpert Medical School of Brown University, Providence, Rhode Island. Both authors have reported that they have no relationships relevant to the contents of this paper to disclose. Listen to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Valentin Fuster. You can also listen to this issue’s audio summary by JACC Editor-in-Chief Dr. Valentin Fuster. Manuscript received August 12, 2014; revised manuscript received October 9, 2014, accepted October 21, 2014. JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 65, NO. 5, 2015 ª 2015 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION ISSN 0735-1097/$36.00 PUBLISHED BY ELSEVIER INC. http://dx.doi.org/10.1016/j.jacc.2014.10.064
Transcript of Sudden Cardiac Death in the Older Athlete · REVIEW TOPIC OF THE WEEK Sudden Cardiac Death in the...

J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 5 , N O . 5 , 2 0 1 5
ª 2 0 1 5 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N DA T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 4 . 1 0 . 0 6 4
REVIEW TOPIC OF THE WEEK
Sudden Cardiac Death in the Older Athlete
Sumeet S. Chugh, MD,* Joseph B. Weiss, MDyABSTRACT
Fro
Me
rel
Lis
Yo
Ma
The overwhelming majority of sports-related sudden deaths occur among those older than 35 years of age. Because
increasing numbers of older people are participating in organized endurance and competitive sporting events, the inci-
dence of sports-related sudden death in older adults is expected to rise. Older athletes will approach clinical cardiologists
for advice regarding their fitness for participation. It is important to recognize both that strenuous exercise is associated
with a transient elevation in risk of sudden cardiac death and that appropriate training substantially reduces this risk. The
approach to pre-participation screening for risk of sudden death in the older athlete is a complex issue and at present is
largely focused on identifying inducible ischemia due to significant coronary disease. In this brief review, we summarize
the current state of knowledge in this area with respect to epidemiology, mechanisms, and approaches to risk stratifi-
cation, as viewed from the perspective of the consulting clinical cardiologist. (J Am Coll Cardiol 2015;65:493–502)
© 2015 by the American College of Cardiology Foundation.
T he legend of the first marathon runner,Pheidippides, embodies the popular notionthat endurance athletics increase the risk
of death. An Athenian messenger approximately40 years of age, he is fabled to have run from Mara-thon to Athens in 490 B.C., perishing on arrival afterproclaiming the Greek victory over the Persians. Thebeneficial, health-promoting effects of habitual phys-ical and sports activity are undeniable. However,a “sports paradox” exists: some people, most oftenthose not habituated to exercise, experience sportsactivity–related cardiac arrests, usually associatedwith underlying heart disease. Middle-aged and olderathletes are at significantly higher risk for suddencardiac death (SCD) compared with younger athletesand are more vulnerable to misconceptions regardingthe cardiovascular effects of sports. The burden ofSCD during sports needs further evaluation but prob-ably constitutes a small proportion (5% to 6%) of sud-den deaths in the general population (1,2). However,from a societal perspective, sports-related SCD canhave a disproportionate impact. People who engagein athletic activity are ostensibly healthier than
m *The Heart Institute, Cedars-Sinai Medical Center, Los Angeles, Califo
dical School of Brown University, Providence, Rhode Island. Both auth
evant to the contents of this paper to disclose.
ten to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Vale
u can also listen to this issue’s audio summary by JACC Editor-in-Chief D
nuscript received August 12, 2014; revised manuscript received October 9
most and therefore considered least likely to experi-ence a cardiac arrest. The media attention on sports-related SCD tends to exaggerate the sports paradoxand obscure the global health benefits of regular exer-cise. In addition to being cardiologists, both authorsof this review are dedicated long-distance runnerswho seek to put the clinical risks and benefits of aer-obic exercise in scientific balance.
A leisure athlete is “an individual, usually middle-aged or elderly ($35 years), who participates in avariety of informal recreational sports, on either aregular or an inconsistent basis, which do not requiresystematic training or the pursuit of excellence”(3). For the purpose of this review, the term “olderathlete” includes all athletes older than 35 years ofage participating in sports at a competitive or masterslevel or as a leisure activity. Both clinical cardiol-ogists and their patients will benefit from a balancedapproach to education, risk stratification, and exer-cise prescription for the middle-aged and olderathlete. The goal of this review is to put forth suchan approach on the basis of a current and compre-hensive assessment of previously published studies.
rnia; and the yDivision of Cardiology, Warren Alpert
ors have reported that they have no relationships
ntin Fuster.
r. Valentin Fuster.
, 2014, accepted October 21, 2014.

FIGURE 1 Relationship Betwe
120
100
80
60
40
20
015 20 25 30
Num
ber o
f Spo
rts-
Rela
ted
SDs
Distribution by age of sports-rel
and among young competitive a
showing that the vast majority o
permission from Marijon et al. (
ABBR EV I A T I ON S
AND ACRONYMS
CAC = coronary artery calcium
CAD = coronary artery disease
MET = metabolic equivalent
MI = myocardial infarction
RV = right ventricular
SCD = sudden cardiac deat
Chugh and Weiss J A C C V O L . 6 5 , N O . 5 , 2 0 1 5
Sudden Death in the Older Athlete F E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2
494
CURRENT BURDEN AND
FUTURE PROJECTIONS
The overwhelming majority of sports-relatedsudden deaths occur among those 35 years ofage or older (4) (Figure 1). Because many suchdeaths are unwitnessed, the magnitude ofthe problem is difficult to ascertain. Retro-spective studies of athletes who participate
in marathons yield estimates of 0.8 to 2 SCDs per100,000 marathon runners (4–11). More comprehen-sively, a prospective 5-year study of sports-relatedSCD in the general population of France reported anannual incidence of 4.6 sports-related SCDs per1 million residents of France (4). Most of these eventsoccurred in older male athletes, with only 6% (50 of820) of all cases of sports-related SCDs in young,competitive athletes. When placed in the context ofthe overall burden of SCD in the general population(600 to 900 per million), sports-related SCDs consti-tute a small subset. Some have reasoned that theabsolute burden of sports-related SCD is small andtherefore of modest clinical significance. For recrea-tional joggers, however, the annual incidence of SCDis significantly higher: 13 SCDs per 100,000 joggersper year (8).
Several additional factors contribute to the clinicaland public health importance of SCD in the older
h
en Age and Sports-Related Sudden Deaths
35 40 45 50 55 60 65 70 75Age, Years
ated sudden deaths (SDs) in the overall population (blue)
thletes (red) in a nationwide, 5-year study in France,
ccurred in those 35 years of age and older. Reprinted with
4).
athlete. The number of older Americans is steadilyincreasing and is expected to double by 2035, reach-ing 70 million. By 2040, 21% of the U.S. populationwill be older than 65 years of age (currently 13.7%)(12). As the population ages, a burgeoning subgroupof older athletes is participating in leisure and orga-nized sports. The popularity of endurance sports,especially running, is significantly on the rise in theUnited States. For example, there are approximately20,000,000 participants in foot races in the UnitedStates annually. Of these, 54% are older than 35 yearsof age and 57% are male. The number of participantshas been growing steadily for the past 15 years (13)(Figure 2). These trends are driven by the growingawareness of the health benefits of exercise activitybut are matched by increasing levels of cardiovascu-lar risk among aspiring older athletes. According torecently published studies, the overwhelming ma-jority of sports-related SCDs have occurred in men,with a 9:1 ratio of men to women experiencing SCDduring sports (11). Potential explanations includelower participation rates for women in marathons orsimilar events. Because women tend to developatherosclerosis about 10 years later than men, theparticipation rate of women at risk may be evenlower. As the demographics of endurance athleticschange along with the population, we anticipate thatincreasing numbers of older women will pursueendurance athletics. However, women clearly enjoythe advantage of a lower likelihood of overall SCD,and the possibility remains that they have a specialadvantage during physical activity.
EVIDENCE FOR TRANSIENT ELEVATION IN
RISK WITH EXERCISE, COUNTERED BY A
PROTECTIVE EFFECT OF REGULAR EXERCISE
Several now-classic studies showed an increasedrisk of SCD and myocardial infarction (MI) duringstrenuous exercise. Siscovick et al. (7) interviewedthe spouses of 133 men with SCD without knownprior heart disease and reported a significant in-crease in relative risk with exercise, but this effectstrongly depended on the habitual exercise level.Among sedentary people, the relative risk of SCDduring exercise was increased 56-fold comparedwith other times. This contrasted strikingly with thelower relative risk during exercise of 5 for menwith the highest level of habitual activity. Despitethe residual 5-fold increased risk of SCD duringvigorous activity, men with the highest habituallevel of physical activity had a substantially lowerrelative risk (0.4) of global SCD compared withsedentary controls.

FIGURE 2 Increasing Numbers of U.S. Athletes Complete Running Races
57%
43%
44%
56%
45%
55%53%
47%
2000
58%
42%
1995
32%
68%
20,000,000
10,000,000
01990 2005 2010 2011 2012 2013
1990Female
Male
1995 2000 2005 2010 2011 2012 20131,199,200 2,215,500 3,619,600 4,494,400 6,929,000 7,685,700 8,699,000 10,844,200
6,835,000 8,180,8006,288,3006,071,0004,947,6004,998,4004,708,0003,597,800
Male Female
75%
25%
52%
48%
Between 1990 and 2013, the number of participating athletes who completed running
races in the United States increased significantly to w20 million per year; 54% were
older than 65 years of age, and 57% were male. Reprinted with permission from State
of the Sport (13).
FIGURE 3 The Greater the Frequency of Weekly Exertion,
the Greater the Reduction in Relative Risk of MI
107
19.4
8.6
2.4
180
160
140
120
100
Rela
tive
Risk
of O
nset
of M
I
Frequency of Physical Exertion per Week
80
60
40
20
00 1-2 3-4 ≥5
A clear dose-response effect of exertion on the relative risk
of MI was demonstrated. Modified with permission from
Mittleman et al. (14). MI ¼ myocardial infarction.
J A C C V O L . 6 5 , N O . 5 , 2 0 1 5 Chugh and WeissF E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2 Sudden Death in the Older Athlete
495
This “paradox of exercise” was confirmed by 2other important epidemiological studies: one study ofexercise-related MI, the most common substrate forSCD, and a second study of exercise-related SCD.Mittleman et al. (14) reported an overall increasedrelative risk of MI during exercise of 5.9. They alsofound an extraordinary 50-fold difference betweensedentary patients (relative risk of MI associatedwith exertion of 107) and active patients (relativerisk: 2.4). They showed a clear dose-response effect,and the greater the frequency of weekly exertion, thegreater the reduction in relative risk of MI (Figure 3).Although SCD was not evaluated, the congruenceof their findings with those of Siscovick et al. (7)for SCD is striking. A third prospective analysis,conducted by Albert et al. (10) from the PhysiciansHealth Study, showed very similar findings. Theoverall relative risk of SCD within 30 min of vigorousexercise was 16.9. For those who exercised less thanonce per week, the relative risk was 74.1; for thosewho exercised $5 times per week, the relative riskwas 10.9. These 3 seminal studies confirm boththe increased risk of MI and SCD associated withexercise and the beneficial effect of regular exerciseto reduce this risk.
The magnitudes of the risk reduction attributedto frequent exercise are impressive, in the range of7- to 10-fold lowered risk for exercise-associated SCDand 50-fold reduction for exercise-associated MI. Theglobal mortality benefits of exercise, we reiterate, faroutweigh the increased risk (Table 1). Multiple studiesconfirm a dose-related beneficial impact of regularexercise on global cardiovascular risk, which is inde-pendent of sex, ethnicity, and probably of age. Themagnitude of the risk reduction is comparable to orexceeds that of statin therapy and extends beyondcardiovascular risk to cancer. Moderate exercise(30 min of moderate activity 5 times per week) re-duces cardiovascular risk by 20%, and high levelsof exercise (30 min of vigorous activity 5 times perweek) reduce cardiovascular risk by 30% to 40% (15).These benefits are enhanced by the observed addi-tional impact of regular exercise on the risk of cancer.Over an 8-year period, regular high levels of exercisein healthy people were associated with a 70% reduc-tion in age-adjusted all-cause mortality in men andan 80% reduction in women (16).
POTENTIAL MECHANISMS OF
EXERCISE-INDUCED SCD
In older athletes, coronary artery disease (CAD) isthe most common cause of sports-related SCD, iden-tified in more than 80% of cases. The remaining
sports-related cases of SCD are attributable to anumber of other problems, such as hypertrophic car-diomyopathy, arrhythmogenic right ventricular (RV)dysplasia, myocarditis, valvular heart disease, and asmall but distinct subgroup of unexplained SCD(11,17–19). For the cases with significant associated

TABLE 1 A Long-Term Protective Effect of
Regular Exercise Counters the Transient Risk of Exercise
In sedentary people, the relative risk of sudden death during exerciseincreases by 56-fold
For those habituated to regular exercise, this risk increases by only5-fold
Regular exercise of mild to moderate intensity provides a 7-fold to10-fold risk reduction for sudden cardiac death and a 50-foldrisk reduction for myocardial infarction
Leisure running, even 5 to 10 min per day at slow speeds (<6 miles/h),is associated with substantial mortality benefits
Chugh and Weiss J A C C V O L . 6 5 , N O . 5 , 2 0 1 5
Sudden Death in the Older Athlete F E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2
496
CAD, the mechanism of sudden death is incompletelyunderstood. Although ischemic ventricular arrhythmiais the final common pathway, the triggers have yet tobe established. Hypothetical mechanisms include sym-pathetic activation, electrolyte and metabolic factors,activation of the hemostatic system, and hemody-namic effects on vulnerable coronary plaque. Exercise-related sympathetic activity may sensitize vulnerablemyocardium to ischemia and arrhythmia. Prolongedexercise produces electrolyte abnormalities that mayalso contribute. It is striking that the overwhelmingmajority of sudden deaths occu in the final quartile ofmarathons and that marathons are associated withgreater risk than half-marathons (9,11). Both findingssupport an electrolyte/metabolic contribution to risk ofSCD. One recent retrospective study also raised thequestion of whether heat stroke is an underdiagnosedcause of death in long-distance races (20).
FIGURE 4 Comparison of Plaque Rupture With Exertion and at Rest
Plaque Rupture With Exertion
VasaVasorum
Necrotic Co
HP
Th
L
Plaque rupture with exertion (left) is characterized by a relatively thin fi
midcap. In contrast, plaque rupture at rest (right) is depicted at the junct
from Burke et al. (21). HP ¼ hemorrhage into plaque; L ¼ lumen; Th ¼
Postmortem studies strongly support roles forplaque rupture, hemostasis, and thrombosis. In acomparative pathological study of plaque mor-phology in men whose death was temporally linkedto physical or emotional stress versus men who diedat rest (21), acute plaque rupture was evident at au-topsy in 68% of the stress-related deaths comparedwith 23% of the deaths at rest (p < 0.001). Similarly,hemorrhage into the plaque was found in 71% ofstress-related SCDs compared with 41% of SCDs at rest(p ¼ 0.007). Stress-related plaque rupture occurred inthe central, thin-capped plaque, while plaque rupturethat occurred at rest was found in the shoulders ofplaque (Figure 4). Increased subjacent vasa vasorumwas identified as a likely source of underlying hem-orrhage in stress-related plaque rupture, whereasplaque rupture at rest was remote from the vasavasorum. On this basis, the authors suggest that he-modynamic factors contribute to stress-related pla-que rupture as the substrate for sports-related SCD.How habitual exercise confers protection againstplaque rupture is not known, but both hemodynamicand tissue effects are potential contributors.
POTENTIAL HAZARDS AT THE HIGH END
OF THE EXERCISE SPECTRUM
Although high levels of habitual exercise clearlyreduce all-cause mortality, the benefits at the highestlevels of exercise may come at a price. Emerging
Plaque Rupture at Rest
re
L
HPTh
Fibrous Cap
brous cap, relatively numerous vasa vasorum, and rupture in the
ion of the fibrous cap and the arterial wall. Reprinted with permission
thrombus.
J A C C V O L . 6 5 , N O . 5 , 2 0 1 5 Chugh and WeissF E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2 Sudden Death in the Older Athlete
497
evidence proposes 2 adverse cardiovascular conse-quences of exercise at the high end: 1) accumulationof coronary artery calcium (CAC) with myocardialfibrosis; and 2) RV fibrosis secondary to episodicvolume/pressure overload. Mohlenkamp et al.(22) quantified CAC, as measured by computed to-mography, and late gadolinium enhancement, asmeasured by magnetic resonance imaging, formyocardial fibrosis in 108 apparently healthy, expe-rienced male marathon runners older than 50 yearsof age (22). Higher levels of accumulation of CAC werefound in runners matched to controls on the basis ofthe Framingham risk score. However, accumulation ofCAC was not significantly different from that ofage-matched controls. Therefore, marathon runnershad lower Framingham risk profiles, without lowerCAC scores. Among 102 marathon runners, 12% had
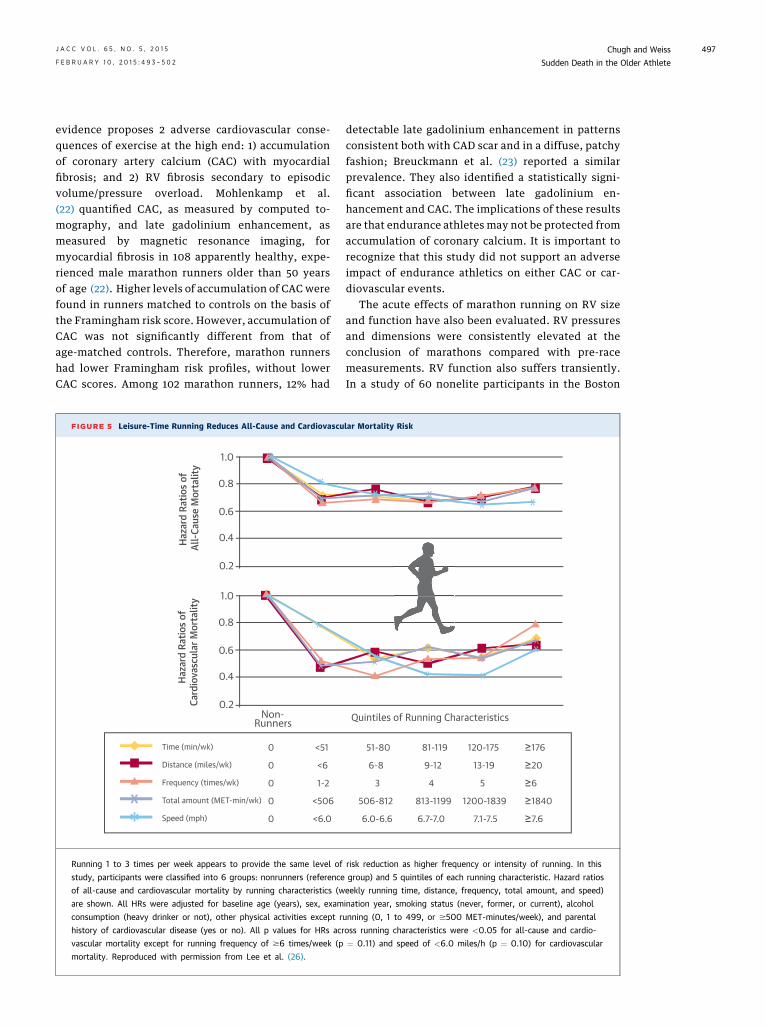
FIGURE 5 Leisure-Time Running Reduces All-Cause and Cardiovascu
0.2
0.4
0.6
0.8
1.0
0.2
0.4
0.6
0.8
1.0
X
X
X
X*
*
H
azar
d Ra
tios o
f C
ardi
ovas
cula
r Mor
talit
y H
azar
d Ra
tios o
f Al
l-Cau
se M
orta
lity
X
*
Time (min/wk)
Distance (miles/wk)
Frequency (times/wk)
Total amount (MET-min/wk)
Speed (mph)
0 <51
0 <6
0 1-2
0 <506
0 <6.0
**
Non-Runners
Running 1 to 3 times per week appears to provide the same level of
study, participants were classified into 6 groups: nonrunners (reference
of all-cause and cardiovascular mortality by running characteristics (w
are shown. All HRs were adjusted for baseline age (years), sex, exam
consumption (heavy drinker or not), other physical activities except r
history of cardiovascular disease (yes or no). All p values for HRs acr
vascular mortality except for running frequency of $6 times/week (p
mortality. Reproduced with permission from Lee et al. (26).
detectable late gadolinium enhancement in patternsconsistent both with CAD scar and in a diffuse, patchyfashion; Breuckmann et al. (23) reported a similarprevalence. They also identified a statistically signi-ficant association between late gadolinium en-hancement and CAC. The implications of these resultsare that endurance athletes may not be protected fromaccumulation of coronary calcium. It is important torecognize that this study did not support an adverseimpact of endurance athletics on either CAC or car-diovascular events.
The acute effects of marathon running on RV sizeand function have also been evaluated. RV pressuresand dimensions were consistently elevated at theconclusion of marathons compared with pre-racemeasurements. RV function also suffers transiently.In a study of 60 nonelite participants in the Boston
lar Mortality Risk
X XX
X
X
XX
X
** *
*
Quintiles of Running Characteristics
51-80 81-119 120-175 ≥176
6-8 9-12 13-19 ≥20
3 4 5 ≥6
506-812 813-1199 1200-1839 ≥1840
6.0-6.6 6.7-7.0 7.1-7.5 ≥7.6
* * * *
risk reduction as higher frequency or intensity of running. In this
group) and 5 quintiles of each running characteristic. Hazard ratios
eekly running time, distance, frequency, total amount, and speed)
ination year, smoking status (never, former, or current), alcohol
unning (0, 1 to 499, or $500 MET-minutes/week), and parental
oss running characteristics were <0.05 for all-cause and cardio-
¼ 0.11) and speed of <6.0 miles/h (p ¼ 0.10) for cardiovascular

Chugh and Weiss J A C C V O L . 6 5 , N O . 5 , 2 0 1 5
Sudden Death in the Older Athlete F E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2
498
Marathon (mean age of 41 years), Neilan et al.(24) found approximately 2-fold elevations ofN-terminal pro–B-type natriuretic peptide and in-creased cardiac troponin T levels in 60%, with 40%exceeding the threshold usually used to diagnoseMI. The increased levels of biomarkers correlatedwith impaired left ventricular diastolic function,increased pulmonary artery pressures, and RV dys-function. One of the more remarkable findingsin this study pertains to the role of training in rela-tion to these markers of myocardial injury anddysfunction. Virtually all indexes of RV functionand the pulmonary artery pressures were moreseverely affected in the least well-trained athletescompared with the best. La Gerche et al. (25)comparing marathon runners with ultraenduranceathletes, confirmed the findings of transient RVdysfunction. They observed elevations of cardiactroponin T, B-type natriuretic peptide, and RV vol-umes with declines in RV function immediatelyafter these endurance events. They also found thatrelease of cardiac troponin T strongly correlated witha decline in RV ejection fraction, particularly inultra-triathletes (r ¼ 0.746; p ¼ 0.003). Although the
CENTRAL ILLUSTRATION The Balance Between Risk of SuTilted in Favor of Regular Sports Activity
MECHANISMS• Coronary plaque rupture• Rare disorders• RV remodeling• Myocardial fibrosis
Transient SCD Risk(Sports Paradox)
Sport-naïveHabituated
Older Ath
Chugh, S.S. et al. J Am Coll Cardiol. 2015; 65(5):493–502.
The consulting cardiologist can assist with stepwise screening, especially
both of which have the potential to further decrease risk. RV ¼ right ve
acute effects all reversed in the days after the events,they found late gadolinium enhancement in 12.8% ofthe athletes, which correlated with a modest reduc-tion in resting RV ejection fraction (47.1 � 5.9% vs. 51.1� 3.7%). The authors hypothesize that extremeendurance athletics is associated with repeated RVinsult, injury, and fibrosis that can evolve late into asubstrate for ventricular arrhythmia. It should benoted that this has not been documented as a cause ofsports-related SCD on an epidemiological basis. Froma public health perspective, we emphasize thatalthough these findings raise some concerns about thebenefits of endurance athletics at the high end, theydo not undermine the substantial benefits of regularexercise on all-cause mortality in the vast majority ofolder athletes (Figure 5) (26).
CLINICAL APPROACH TO RISK
STRATIFICATION FOR SCD IN
OLDER ATHLETES: GREATEST UTILITY
IN THE SPORT-NAÏVE ATHLETE
The growing popularity of endurance athletics in anaging population will result in a larger pool of older
dden Death and Benefits of Sports in the Older Athlete:
40-60% MORTALITY• Dose related• Any age• Even moderate activity
HOW TO MITIGATE RISK
• Gradual in activity• Aspirin
Protective Effectof Regular Activity
athleteathlete
For significant in activity level
lete
3-STEP SCREENING• Patient questionnaire• Physician evaluation• Maximal stress testing
in the sport-naïve athlete, and encourage gradual increase in activity,
ntricular; SCD ¼ sudden cardiac death.

FIGURE 6 American Heart Association/American College of Sports Medicine Health/Fitness Facility Pre-Participation Screening Questionnaire
Assess your health needs by marking all true statements.
You should be able to exercise safely without consulting your healthcareprovider in almost any facility that meets your exercise program needs.
If you marked 2 or more of the statements in this section, consult yourhealthcare provider before engaging in exercise. You might benefit by
using a facility with a professionally qualified exercise staff to guide your exercise program.
If you marked any of the statements in this section, consult your healthcareprovider before engaging in exercise. You may need to use a facility with a
medically qualified staff.
None of the above is true.
Other health issues:You have musculoskeletal problems.You have concerns about the safety of exercise.You take prescription medication(s).You are pregnant.
HistoryYou have had:
A heart attackHeart surgeryCardiac catheterizationCoronary angioplasty (PCTA)
Heart valve diseaseHeart failureHeart transplantationCongenital heart disease
Pacemaker/implantable cardiac defibrillator/rhythm disturbance
SymptomsYou experience chest discomfort with exertion.You experience unreasonable breathlessness.You experience dizziness, fainting, blackouts.You take heart medications.
Cardiovascular risk factorsYou are a man older than 45 years.
You smoke.Your blood pressure is >140/90.You don’t know your blood pressure.
You don’t know your cholesterol level.You have a close blood relative who had a heart attack before age 55(father or brother) or age 65 (mother or sister).You are diabetic or take medicine to control your blood sugar.You are physically inactive (ie, you get <30 minutes of physical activityon atleast 3 days per week).
Your blood cholesterol level is >240 mg/dl.
You are >20 pounds overweight.
You are a woman older than 55 years or you have had a hysterectomy or you are postmenopausal.
PCTA ¼ percutaneous transluminal coronary angioplasty. Reproduced with permission from Balady et al. (29).
TABLE 2 Recommended Criteria for Identification of the
High-Risk Athlete During Evaluation by the Physician
10-year risk of coronary artery disease >5% (Framingham risk score)
Total cholesterol level >320 mg/dl or low-density lipoproteincholesterol level >240 mg/dl
Diabetes mellitus with microalbuminuria
Strong family history of sudden cardiac death or premature (ageyounger than 50 years) coronary artery disease in a first-degreerelative
Body mass index >28 kg/m2
J A C C V O L . 6 5 , N O . 5 , 2 0 1 5 Chugh and WeissF E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2 Sudden Death in the Older Athlete
499
athletes. This is, of course, very good news, becauseregular exercise has enormous proven potentialto reduce cardiovascular morbidity and mortality.Therefore, there is a growing need to provide prac-tical, clinically relevant advice to minimize the asso-ciated risk. Among older athletes, the primary riskfor sports-related SCD is CAD with acute plaquerupture. This risk is low for most endurance events,such as the marathon. Indeed, an epidemiologicalstudy has argued credibly that marathons reducethe death toll because the average number of race-associated SCDs is about one-half the number ofdeaths that would typically result from motor vehicleaccidents if the race route were not closed to traffic(9). However, the risk associated with trainingis approximately 5-fold greater. Accordingly, weobserve that cardiologists can intervene most effec-tively by advising noncompetitive or pre-competitiveathletes. Because the most common substrate forrisk is (by far) CAD, the main objective of pre-
participation screening of the older athlete isruling out significant occult CAD. We considered 3published documents for pre-participation screeningof the older athlete in developing recommendationsfor risk stratification of the older athlete: 1) recom-mendations from a working group of the AmericanHeart Association and allied organizations (3); 2) theAmerican College of Sports Medicine guidelines (27);and 3) the European Association for CardiovascularPrevention and Rehabilitation guidelines (28).

FIGURE 7 A Suggested 3-Step Screening Process for
Significant Occult Coronary Artery Disease in the Older Athlete
Assessment of Risk(self or by non-physician)
Negative
Negative
Negative
Positive
Positive
Positive
Screening by Physician(History, Physical Exam,
Risk factors, Resting ECG)
Maximalexercise testing
Eligible forexercise training
Furtherevaluation
Three levels are recommended for cardiovascular evaluation in older athletes, depending
on the individual’s risk factors and intended physical activity. ECG ¼ electrocardiography.
Modified from Borjesson et al. (28).
FIGURE 8 A Grade
3/week
<3 METS, 50-7Max predicted
Balancing the risk of
be addressed throug
rather than the inten
heart rate; METS ¼ m
Chugh and Weiss J A C C V O L . 6 5 , N O . 5 , 2 0 1 5
Sudden Death in the Older Athlete F E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2
500
AUTHORS’ RECOMMENDATIONS FOR
RISK STRATIFICATION IN THE
ASYMPTOMATIC PATIENT
Because there is a significant amount of informationcommon to the 3 guidelines and none of the
d Approach to Exercise Conditioning in the Older Athlete
0% HR
3-6 METS, 50-70%Max predicted HR
>6 METS, 70-85%Max predicted HR
5/week
3→5/week
sudden cardiac death with the protective effect of regular activity can
h screening of the older athlete and by emphasis on the frequency,
sity, of the activity level, which should be increased gradually. HR ¼etabolic equivalents.
approaches have been tested prospectively, we sug-gest a succinct, 3-step process (Central Illustration):
1. Assess risk using the American Heart Associationpre-participation questionnaire (29) (Figure 6),which is a useful initial screening tool for com-pletion by the patient that is designed to elicitevidence of known risk factors. If any are detected,evaluation by a physician is recommended. If thepatient is in the cardiologist’s office, then onecould move directly to step 2.
2. Perform a physician-led evaluation comprising acareful clinical history (including family historythat can uncover familial conditions, such as longQT syndrome), physical examination, and estima-tion of the absolute 10-year risk of CAD usingthe Framingham risk score (30). Any criterion lis-ted in Table 2 indicates a high-risk profile.
3. Use maximal exercise stress testing as a discrimi-nator when the risk profile is high and the gapbetween habitual physical activity and intendedlevel of activity is large (Figure 7). If maximalexercise electrocardiography is unsuitable for agiven patient, we suggest single-photon emissioncomputed tomography or stress echocardiographyas appropriate alternatives. This applies to sed-entary patients achieving <2 metabolic equiv-alents (MET)-h/week. For active patients alreadyachieving >2 MET-h/week, low-intensity activitymay be appropriate without this evaluation pro-cess. Routine use of stress testing in healthy,asymptomatic athletes is not recommended. Judi-cious use of resting 12-lead electrocardiogramand echocardiogram may be indicated and insome cases may result in diagnosis of previouslyunrecognized conditions, such as hypertrophiccardiomyopathy or arrhythmogenic RV dysplasia.Physical activity is important to manage, andpotentially to restrict, in aspiring athletes, whomay have conditions such as uncontrolled hyper-tension and active myocarditis.
PRE-PARTICIPATION SCREENING IN THE
OLDER ATHLETE: FUTURE CONSIDERATIONS
Stress testing is most likely to identify those withsubocclusive CAD. However, plaque rupture, which isconsidered to be an important mechanism of SCD inthe older athlete, can occur among coronary lesionsthat bring about mild to moderate coronary stenoses.Therefore, imaging of coronary plaque to identifylesions vulnerable to rupture has significant potentialto enhance risk stratification. Although there is aconspicuous lack of studies that specifically evaluate

J A C C V O L . 6 5 , N O . 5 , 2 0 1 5 Chugh and WeissF E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2 Sudden Death in the Older Athlete
501
SCD as an outcome, plaque characteristics clearlydetermine the risk of acute coronary syndrome andmajor adverse cardiovascular events (31). Increasedcoronary artery calcification, as measured by com-puted tomography, is a strong predictor of incidentCAD beyond standard risk factors, with a 10-foldincreased risk in those with coronary calcium scores>300 (32). However, any additions to the risk strati-fication armamentarium of the older athlete shouldrequire assessment of SCD as the outcome and carefulconsideration of cost versus benefit.
STRATEGIES TO MITIGATE RISK
IN THE SPORT-NAÏVE ATHLETE:
AUTHORS’ SUGGESTIONS
We propose that gradually increasing the level ofhabitual activity has the greatest potential to renderexercise safe while improving all-cause mortality.The increased risk associated with a sedentary life-style identifies this group as high risk, and gradedtraining can in theory reduce the risk of sports-relatedSCD by a factor of 10 to 50 (7,10). Although specific,universally applicable recommendations for reducingrisk through graded conditioning are difficult to pro-vide, we propose a few principles. First, frequency ofphysical activity (rather than intensity) should beemphasized at the outset. Exercise intensity is usu-ally defined by either METs or heart rate in relation tothe maximum predicted heart rate and the numberof sessions per week (Figure 8). An initial period oflow-intensity exercise (<3 METs, or increase in heartrate to 50% to 70% of maximum predicted) performed3 times a week attenuates the risk and may rendermoderate or higher intensity exercise safer (Figure 8).Each stage should ideally be covered in 6 to 8 weeksor longer, on the basis of the patient’s overall fit-ness and conditioning level. This graded approachobviates the risk of high-intensity exercise performedby poorly conditioned athletes.
In our opinion, the decision regarding cholesterol-lowering therapy, such as statins, should be drivenby standard recommendations (33). For many, life-style alterations associated with sports activity mayobviate the need for such drugs. Statins may, in the-ory, contribute to coronary plaque “stabilization,” butany modest beneficial effects could be offset by the
statin-induced muscle fatigue or myopathy reportedamong 10% to 25% of patients in clinical practice (34),which is particularly relevant during exercise trainingadaptation (35). Low-dose aspirin (75–100 mg) mayhave a modest contribution to primary prevention ofcardiovascular disease (36), but we propose that theoverall mortality benefit is likely to exceed the riskin asymptomatic middle-aged and older athletes.
CONCLUSIONS
The increased risk of sports-related SCD in olderathletes is real, but it is balanced by the benefitsof fitness. However, as the population ages andendurance athletics gain in popularity, the popula-tion at risk is growing. Unlike in younger athletes,CAD is the predominant cause of SCD in older ath-letes. On a population basis, the risk associatedwith sporting events is much lower than the riskassociated with training or leisure athletics. In mul-tiple studies, low levels of habitual exercise are avery strong risk factor for sports-related SCD.Therefore, cardiologists should advise appropriatelygraded athletic training as the safest, most effectivecourse. Both American and European societiesrecommend screening for occult CAD by question-naire along with risk stratification on the basis ofCAD risk profiles. Maximal stress testing for a high-risk subset may be beneficial in appropriate pa-tients. However, a negative stress test may notidentify all patients at risk for SCD. In the future,imaging of the coronary plaque may enhance pre-participation screening for occult CAD. It is impor-tant to remember that reductions in cardiovascularand all-cause mortality associated with moderate-intensity exercise performed $3 times per week arein the range of 40% to 60%. On balance, the healthbenefits of regular exercise heavily outweigh therisks of SCD in older athletes, especially in those whotrain appropriately.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Sumeet S. Chugh, Cedars-Sinai Medical Center,Advanced Health Sciences Pavilion, Suite A3100, 127South Vicente Boulevard, Los Angeles, Califor-nia 90048. E-mail: [email protected].
RE F E RENCE S
1. Berdowski J, de Beus MF, Blom M, et al.Exercise-related out-of-hospital cardiac arrest inthe general population: incidence and prognosis.Eur Heart J 2013;34:3616–23.
2. Reddy PR, Reinier K, Singh T, et al. Physicalactivity as a trigger of sudden cardiac arrest: theOregon Sudden Unexpected Death Study. Int JCardiol 2009;131:345–9.
3. Maron BJ, Araujo CGS, Thompson PD, et al.,World Heart Federation; International Federationof Sports Medicine; American Heart AssociationCommittee on Exercise, Cardiac Rehabilitation,
Chugh and Weiss J A C C V O L . 6 5 , N O . 5 , 2 0 1 5
Sudden Death in the Older Athlete F E B R U A R Y 1 0 , 2 0 1 5 : 4 9 3 – 5 0 2
502
and Prevention. Recommendations for prepar-ticipation screening and the assessment of car-diovascular disease in masters athletes: anadvisory for healthcare professionals from theworking groups of the World Heart Federation, theInternational Federation of Sports Medicine, andthe American Heart Association Committee onExercise, Cardiac Rehabilitation, and Prevention.Circulation 2001;103:327–34.
4. Marijon E, Tafflet M, Celermajer DS, et al.Sports-related sudden death in the generalpopulation. Circulation 2011;124:672–81.
5. Maron BJ, Poliac LC, Roberts WO. Riskfor sudden cardiac death associated with mara-thon running. J Am Coll Cardiol 1996;28:428–31.
6. Ragosta M, Crabtree J, Sturner WQ, et al.Death during recreational exercise in the Stateof Rhode Island. Med Sci Sports Exerc 1984;16:339–42.
7. Siscovick DS, Weiss NS, Fletcher RH, et al. Theincidence of primary cardiac arrest during vigorousexercise. N Engl J Med 1984;311:874–7.
8. Thompson PD, Funk EJ, Carleton RA, et al.Incidence of death during jogging in Rhode Islandfrom 1975 through 1980. JAMA 1982;247:2535–8.
9. Redelmeier DA, Greenwald JA. Competingrisks of mortality with marathons: retrospectiveanalysis. BMJ 2007;335:1275–7.
10. Albert CM, Mittleman MA, Chae CU, et al.Triggering of sudden death from cardiac causes byvigorousexertion.NEngl JMed2000;343:1355–61.
11. Kim JH, Malhotra R, Chiampas G, et al., RaceAssociated Cardiac Arrest Event Registry (RACER)Study Group. Cardiac arrest during long-distancerunning races. N Engl J Med 2012;366:130–40.
12. Administration on Aging, Administration onCommunity Living, U.S. Department of Health andHuman Services. A profile of older Americans2013. 2013. Available at: http://www.aoa.acl.gov/Aging_Statistics/Profile/2013/docs/2013_Profile.pdf.Accessed November 17, 2014.
13. State of the Sport - Part III: U.S. Race Trends.RunningUSA.July9,2014.Available at: http://www.runningusa.org/2014-state-of-the-sport-part-III-us-race-trends. Accessed November 14, 2014.
14. Mittleman MA, Maclure M, Tofler GH, et al.Triggering of acute myocardial infarction by heavyphysical exertion. Protection against triggeringby regular exertion. Determinants of MyocardialInfarction Onset Study Investigators. N Engl J Med1993;329:1677–83.
15. Shiroma EJ, Lee IM. Physical activity andcardiovascular health: lessons learned from
epidemiological studies across age, gender, andrace/ethnicity. Circulation 2010;122:743–52.
16. Blair SN, Kohl HW III, Paffenbarger RS Jr., et al.Physical fitness and all-cause mortality. A pro-spective study of healthy men and women. JAMA1989;262:2395–401.
17. Corrado D, Migliore F, Basso C, et al. Exerciseand the risk of sudden cardiac death. Herz 2006;31:553–8.
18. Maron BJ, Epstein SE, Roberts WC. Causes ofsudden death in competitive athletes. J Am CollCardiol 1986;7:204–14.
19. Waller BF, Roberts WC. Sudden death whilerunning in conditioned runners aged 40 years orover. Am J Cardiol 1980;45:1292–300.
20. Yankelson L, Sadeh B, Gershovitz L, et al.Life-threatening events during endurance sports:is heat stroke more prevalent than arrhythmicdeath? J Am Coll Cardiol 2014;64:463–9.
21. Burke AP, Farb A, Malcom GT, et al. Plaquerupture and sudden death related to exertion inmen with coronary artery disease. JAMA 1999;281:921–6.
22. Mohlenkamp S, Lehmann N, Breuckmann F,et al., Marathon Study Investigators; HeinzNixdorf Recall Study Investigators. Running:the risk of coronary events: prevalence andprognostic relevance of coronary atheroscle-rosis in marathon runners. Eur Heart J 2008;29:1903–10.
23. Breuckmann F, Mohlenkamp S, Nassenstein K,et al. Myocardial late gadolinium enhancement:prevalence, pattern, and prognostic relevance inmarathon runners. Radiology 2009;251:50–7.
24. Neilan TG, Januzzi JL, Lee-Lewandrowski E,et al. Myocardial injury and ventricular dysfunctionrelated to training levels among nonelite partici-pants in the Boston Marathon. Circulation 2006;114:2325–33.
25. La Gerche A, Burns AT, Mooney DJ, et al.Exercise-induced right ventricular dysfunction andstructural remodelling in endurance athletes. EurHeart J 2012;33:998–1006.
26. Lee DC, Pate RR, Lavie CJ, et al.Leisure-time running reduces all-cause andcardiovascular mortality risk. J Am Coll Cardiol2014;64:472–81.
27. ACSM’s Guidelines for Exercise Testing andPrescription. 9th edition. In: Pescatello LS,Arena R, Riebe D, et al. editors. Philadelphia, PA:Lippincott Williams & Wilkins, 2013.
28. Borjesson M, Urhausen A, Kouidi E, et al.Cardiovascular evaluation of middle-aged/ senior
individuals engaged in leisure-time sport activ-ities: position stand from the sections of exercisephysiology and sports cardiology of the EuropeanAssociation of Cardiovascular Prevention andRehabilitation. Eur J Cardiovasc Prev Rehabil 2011;18:446–58.
29. Balady GJ, Chaitman B, Driscoll D, et al.Recommendations for cardiovascular screening,staffing, and emergency policies at health/fitnessfacilities. Circulation 1998;97:2283–93.
30. Grundy SM, Pasternak R, Greenland P, et al.AHA/ACC scientific statement: assessmentof cardiovascular risk by use of multiple-risk-factor assessment equations: a statement forhealthcare professionals from the AmericanHeart Association and the American Collegeof Cardiology. J Am Coll Cardiol 1999;34:1348–59.
31. Stone GW, Maehara A, Lansky AJ, et al.,PROSPECT Investigators. A prospective natural-history study of coronary atherosclerosis. N EnglJ Med 2011;364:226–35.
32. Detrano R, Guerci AD, Carr JJ, et al. Coronarycalcium as a predictor of coronary events in fourracial or ethnic groups. N Engl J Med 2008;358:1336–45.
33. Stone NJ, Robinson JG, Lichtenstein AH,et al., American College of Cardiology/AmericanHeart Association Task Force on PracticeGuidelines. 2013 ACC/AHA guideline on thetreatment of blood cholesterol to reduceatherosclerotic cardiovascular risk in adults: areport of the American College of Cardiology/American Heart Association Task Force onPractice Guidelines. J Am Coll Cardiol 2014;63:2889–934.
34. Cohen JD, Brinton EA, Ito MK, et al. Under-standing Statin Use in America and Gaps in PatientEducation (USAGE): an internet-based surveyof 10,138 current and former statin users. J ClinLipidol 2012;6:208–15.
35. Mikus CR, Boyle LJ, Borengasser SJ, et al.Simvastatin impairs exercise training adaptations.J Am Coll Cardiol 2013;62:709–14.
36. Vandvik PO, Lincoff AM, Gore JM, et al.,American College of Chest Physicians.Primary and secondary prevention of cardiovas-cular disease: antithrombotic therapy and pre-vention of thrombosis, 9th ed: American Collegeof Chest Physicians evidence-based clinicalpractice guidelines. Chest 2012;141 2 Suppl:e637S–68S.
KEY WORDS athletics, endurance,exercise, risk stratification


















