
Successfully Integrating PAP Technology in the Clinic · Successfully Integrating PAP Technology in...
71
Successfully Integrating PAP Technology in the Clinic Loretta Colvin, APRN-BC Nurse Practitioner Clayton Sleep Institute
Transcript of Successfully Integrating PAP Technology in the Clinic · Successfully Integrating PAP Technology in...
Successfully Integrating PAP
Technology in the ClinicLoretta Colvin, APRN-BC
Nurse Practitioner
Clayton Sleep Institute

Objectives
• Review PAP technology options
• Identify PAP comfort technology
• Understand variations in technology
options available

Conflict of Interest
• I have no conflicts of interest to disclose
My Plans
• Discuss brands common in my practice
• Focus on newer model features
• Discuss adherence reports and
interpretation later today

Cheat Sheet

Be Prepared

Assess Equipment
When to Assess Equipment
• New set-ups
• Replacement equipment
• Yearly follow-up
• Any complaints
Look, listen and feel

Look at Equipment
• Machine
– Settings: do they match orders?
– Capabilities: brand, model, AHI & leak
• Disposables
– Mask: style, condition
– Tubing: style, condition
– Humidifier chamber: setting & condition
– Filters: condition, large/fine particle
• Data transfer (modem, card)

Listen to Equipment
• Machine noise
– Is it REALLY loud?
• Leak noise
– Machine, humidifier, tubing
– Connections and ports
– Look for holes!

“Feel” the Equipment
• Check pressure with manometer
– Verify against pressure setting
– BEWARE of
• Auto-ramp
• Pressure relief (ex: EPR)
• Bilevel or advanced modality
• Altitude (manual adjustment)
• Check heat plate
– Water level unchanged after use
– Is humidifier turned on? (zero=off)

Altitude Adjustment
• Auto-adjustment altitude– ResMed S8, S9, Airsense 10 (up to 8,000 ft)
– Respironics System One, M-series pro and auto (up to 10,000 ft)
– Fisher&Paykel Icon premo & auto, SleepStyle 608 (up to 9,000 ft)
• Manual adjustment altitude
– Respironics System One, M-series & Legacy plus
• 1:0-2500 ft, 2:2500-5000, 3:5000-7500
– F&P Icon novo and sleep style (other than 608)
• 1:0-3000, 2:3000-6000, 3:6000-9000
? ? X??

Case Examples
Assess Equipment!

Pressure Manometer
• ResMed S9 CPAP
• Ordered at 10 cm per titration study
• 4 cm on manometer
• Auto ramp @ 4 cm
• 7 cm on manometer
• EPR @ 3 = 3 cm reduction
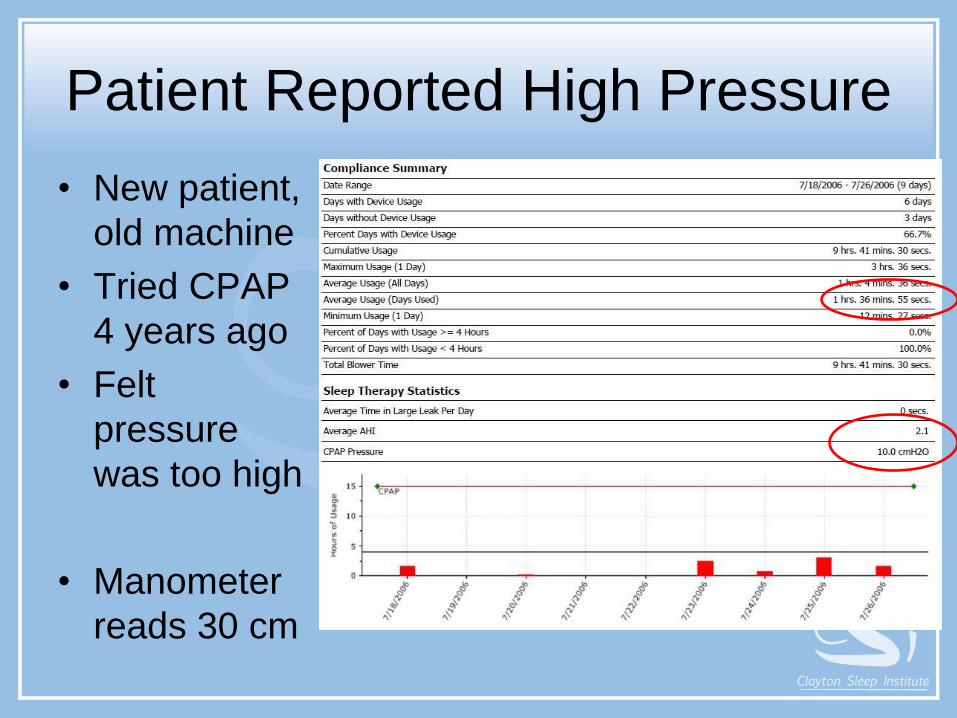
Patient Reported High Pressure
• New patient,
old machine
• Tried CPAP
4 years ago
• Felt
pressure
was too high
• Manometer
reads 30 cm

New Machine at Correct Pressure

Patient Reported OSA Symptoms
• Patient moved to Denver from Texas
• Since move, feels OSA symptoms have returned despite
CPAP use
• Machine set at 9 cm

Re-Assessment
• Re-titration – 9 cm optimal (current setting)
• F/u after study – OSA symptoms persist
• What next?
• Manometer – blowing 6
• Has RemStar M-series PLUS machine
that does NOT auto-adjust altitude1 = 0 - 2500 ft, 3 = 5000 – 7500 ft (Denver 5280)

Report Indicates Leak
• Staff insist patient wearing
machine several hours nightly
• Patient was instructed to bring
ALL supplies and machine to
clinic
• CPAP placed on patient
• Machine REALLY loud

Patient Reports Loud Machine
• Limited hand mobility affects ability to
properly close humidifier lid

Extra Credit
• Patient returns for yearly f/u
• Started CPAP in 2008 – history of nightly usage
• What happened?

Answer
• 2008 recall on certain M-
series models-humidifier only
• Call Respironics customer
support with machine serial #

Comfort FeaturesHumidification & Pressure Relief

Humidification Audience Poll
• Does heated humidification increase
adherence to therapy?
Yes
No
Unsure

Humidification
• Across studies, results are inconsistent for: – Adherence, preference, side effects
– Subgroups w/oronasal symptoms may benefit
• AASM guidelines (2009)
– Standard recommendation
• Am College of Physicians (ACP - 2013)
– Insufficient evidence, inconsistent findings
• It is a comfort feature covered by Medicare
• Commonly ordered at onset of new therapy
Sawyer A et al 2011. Sleep Medi Review 15:343-356. Wickwire E et al, 2013. Chest 144(2):680-693.
Epstein L et al 2009. J Clin Sleep Med 5(3):263-276. Qaseem, A et al 2013. Ann Intern Med 159:471-483.

Extra Credit
• Humidification comes standard with PAP
therapy order?
Yes
No
Unsure

Humidifiers and Orders
• Humidifier is a separate HCPCS code,
technically requires separate order
• F&P and ResMed AirSense 10 use integrated
humidifier, cannot actually be “detached”.
• Medicare pays outright for humidifier, even if
patient returns machine for non-usage
• Some insurance may not actually cover
humidifier

Humidification Fine Tuning
• Heated Tubing
– Integrated circuit
• Beware – varied settings for tubing heat
vs. humidifier heat, brands vary
• Note – DME must provide tubing ($)
– Added circuit
• Insulated tubing
– “cozy”

Humidification OptionsMachine Chamber
Attachment
Chamber
Heater
Heated
Tubing
Patient
Controlled
Heated Tubing
System OneRespironics
Detachable 0-5regular tubing
“classic”/“system one”
1-3 heated tubing
Preheat option
0-5≥ 60 series
Note – if heated tubing
connected, the 0-5 dial
controls tubing, not heat
plate
+
If granted access
S9ResMed
Detachable 0-6Preheat option
60 - 86°controls tubing/chamber
+
AirsenseResMed
Integrated 0-8Preheat option
Auto controls tubing/chamber
Manual 60-86°separate chamber control
+
Icon Fisher & Paykel
Integrated 0-7No preheat option
Boost
L-M-H
+Advanced mode only,
push and hold chamber temp to
access thermometer icons
Note – heated tubing must be attached and “clicked in” to
activate heated tubing controls (when patient accessible)

Special Notes

Examples
Humidification Discussion
• Post-menopausal women
• Teenagers
• Dry climate
• Oro-nasal symptoms at baseline
• Anxious
• Elderly
• Long-haul truck drivers

Pressure Relief Audience Poll
• Pressure relief increases adherence to
PAP therapy
Yes
No
Unsure

Pressure Relief
• Across studies, findings are inconsistent – Benefit, no benefit, mixed results
– Published studies may not reflect all algorithms
– Sub-groups with poor adherence may find benefit
• AASM Guidelines (2009)
– Consensus recommendation
• Am College of Physicians (ACP 2013)
– Low quality evidence (discusses C-flex only)
Sawyer A et al 2011. Sleep Medi Review 15:343-356. Wickwire E et al, 2013. Chest 144(2):680-693.
Epstein L et al 2009. J Clin Sleep Med 5(3):263-276. Qaseem, A et al 2013. Ann Intern Med 159:471-483.

Pressure Relief (cont)
• Each manufacturer uses different proprietary
algorithm, goes through FDA approval
process
• Designed to selectively reduce pressure
• Use selectively in patients, not in all patients
• Know your machines and the varied
algorithms. Watch your detailed reports.
• Consider an “add on” if issues present later

Pressure Relief • F&P Sensawake
– Clinician sets low pressure
– Senses “wake” to drop pressure
• ResMed EPR– 1–3 cm pressure
– Easy-breathe bilevels only
• Respironics ‘flex”– Flex 1-3 refers to relative
drop
– Cflex+: 2 cm drop from baseline on exhalation (“mini-bilevel”)
ResMed – EPR
Respironics – cflex, cflex+ (and aflex, biflex)
Fisher & Paykel – Sensawake

Special Notes

Discussion
• Pressure relief requires a prescription
Yes
No
Unsure
• Patients should have uncontrolled access?

Discussion (cont)
It depends on your DME and your preference:
• Icon (sensawake)– Comes activated “out of the box”
– DME must turn OFF (!)
• SystemOne (flex/flex+) and S9/AirSense 10 (EPR)– Clinician must activate at set-up
• Patient access – Always (older machines)
– Clinician controlled
– Varies by device
Pressure Relief Discussion
• Lab-initiated feature
– Do you script for machine by brand?
• Provider scripted @ initiation
– When ?
• Add on feature
– When ?
• Replacement machines

Leak and AHI
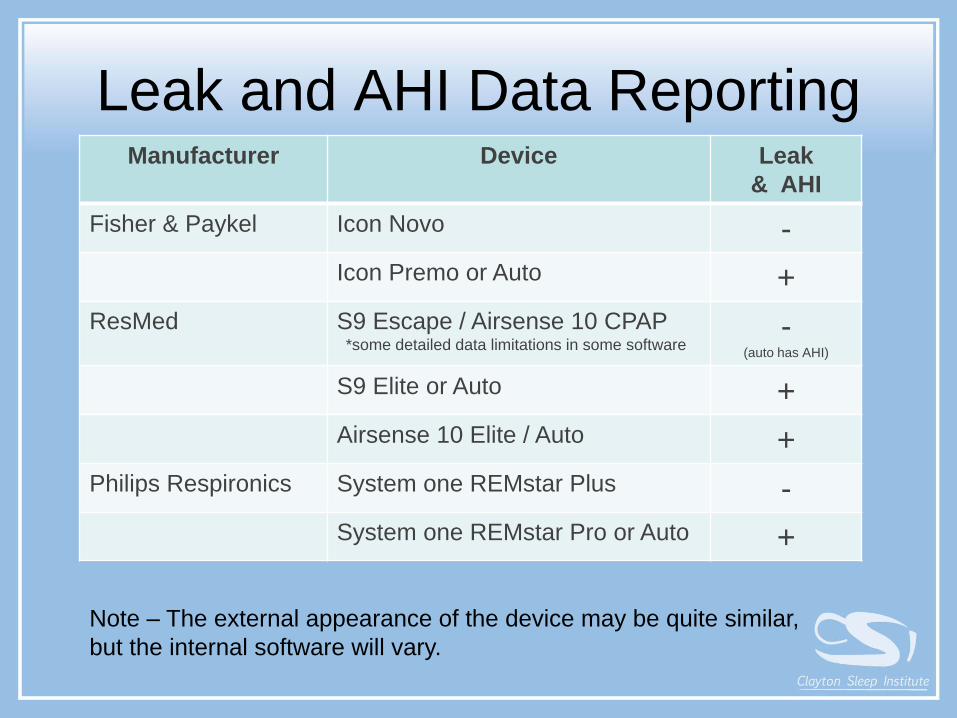
Leak and AHI Data Reporting Manufacturer Device Leak
& AHI
Fisher & Paykel Icon Novo -
Icon Premo or Auto +
ResMed S9 Escape / Airsense 10 CPAP*some detailed data limitations in some software
-(auto has AHI)
S9 Elite or Auto +
Airsense 10 Elite / Auto +
Philips Respironics System one REMstar Plus -
System one REMstar Pro or Auto +
Note – The external appearance of the device may be quite similar,
but the internal software will vary.

Leak
Leak Audience Poll
• A leak > 24 L / min is considered a high
leak
Yes
No
Unsure

Leak
• Total leak (> 40 – 50 L/min generally concerning)– All the leak reported, including normal leak from mask
– Intentional (mask) + unintentional (seals)
– “abnormal” leak depends on mask and pressure
– Respironics • Black: Large Leak (LL) – approx 2X expected leak detected > 1.5
minutes
– Fisher & Paykel
• Excessive leak (>24 L/min generally high)– Leak above what is expected for mask selected on
machine
– Intentional leak only
– Must have right mask selected for calculation to work
– Resmed
Intentional
Leak
Unintentional
Leak

Leak References
• Each mask
manufacturer
can provide
you with mask
leak guides
• You may find
one in your
lab

AHI

AHI – Audience Poll
• An AHI > 10 on a detailed report indicates
in-lab titration must be performed
Yes
No
Unsure
Extra Credit
• AHI of zero indicates effective therapy
Yes
No
Unsure

•AHI and Leak = 0
•REMstar System One Plus in Encore Anywhere
•No AHI detection
•No leak report statistics
AHI and Leak Data

Leak and AHI Detection
• If leak not resolved, AHI detection can be unreliable
• Use particular caution when monitoring aPAPAHI (ie – no in-lab titration for reference)
• You will either get both measures, or you will get neither
• May add noise, detectable by some patients switching machines
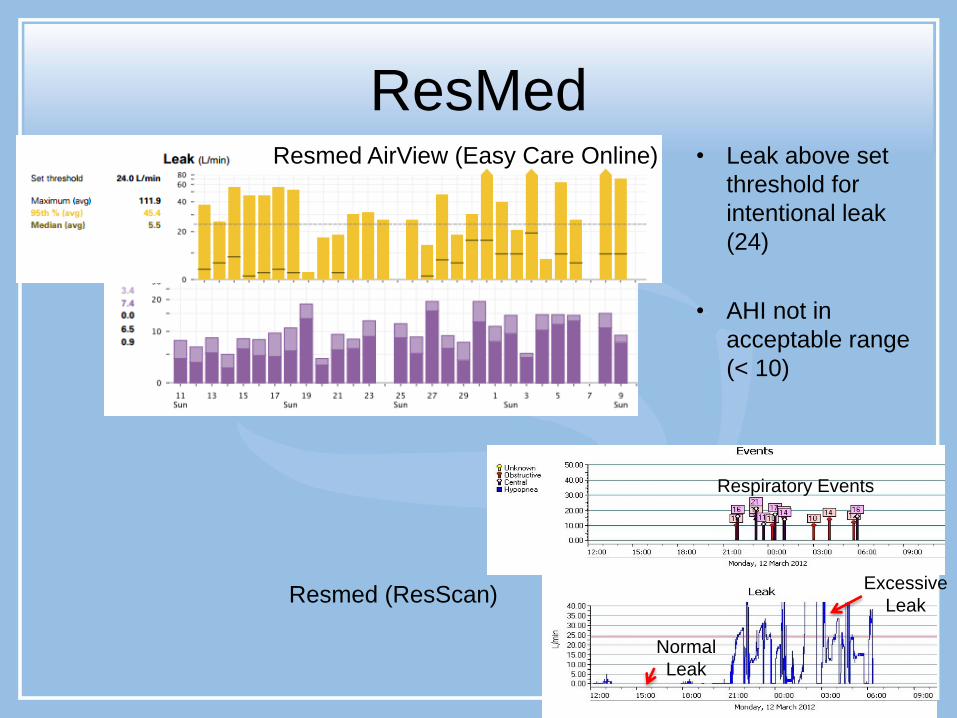
• Leak above set
threshold for
intentional leak
(24)
• AHI not in
acceptable range
(< 10)
ResMed
Resmed (ResScan)
Normal
Leak
Excessive
Leak
Respiratory Events
Resmed AirView (Easy Care Online)

• Leak is horrible
• > 80 L/min (!)
• AHI wide
variation
• Undetectable AHI
is unusual
F&P Icon Leak and AHI

DOT Driver

Daily Details DOT Driver
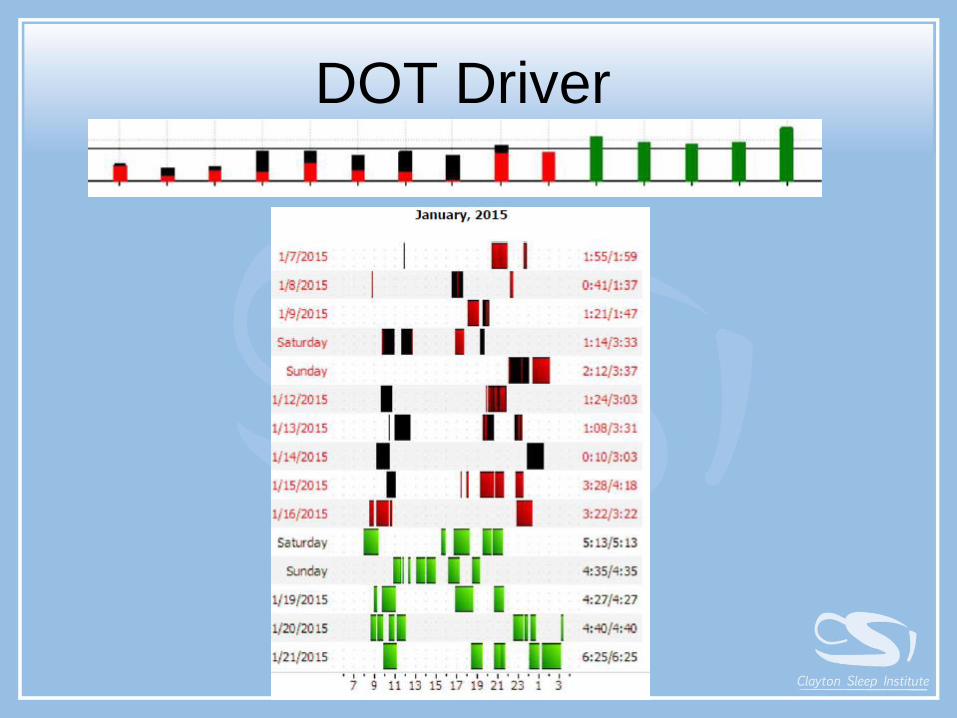
DOT Driver

AHI Detection - Group Discussion
• Do you script for AHI detection?
– When
• Do you script by manufacturer?
– When
• Examples
– No REM or no supine observed at optimal
– Monitoring for centrals in certain scenarios• Idiopathic centrals on HST with limited in-lab
titration option due to insurance or deductible

Tips (and a little soapbox)

Equipment Assessment Tips
• Use a manometer
• Train scheduling staff to advise patient to
bring machine and ALL equipment
– Modem does not always mean data available
• Have a cheat sheet to help find settings
• Have power cords for all machines
• Keep spare cards for all machines in clinic

Download Tips
• Have backup PC based software for all
manufacturers
– Encore Pro, ResScan, InfoSmart
– Keep version updated, centralize data storage
• Have a cheat sheet to help “break into”
machines for pressure changes
Assessment Tips
• Double check the DME
– Check settings vs. orders
– Check for pressure relief
– Check the basics (humidifier)
– Set expectations (ex: AHI detection)
• Always “dig deeper”
– Use detailed reports when there’s a problem

“I’m Using My Machine”
• Assess technology– Was download done correctly? (ex: wrong dates)
– Was card inserted in machine?
– View machine screens to double check
• Assess patient– Clinical improvement?
– Describe the machine/mask? (ex: color)
– Would they over-estimate usage? (DOT, insurance)
• CPAP self-monitoring assessment– Log, patient data access (machine, online)

ResMed S9
• Card holds
only 6 mo
data

A Note on Mouth Breathing
• OSA patients do not remain mouth breathers….
• Patient preference for FFM initially– Coach patient to consider alternatives to FFM
• Clinician preference • Tech preference during titration
• DME preference for aPAP with higher max pressure
• Alternatives • Humidification helpful in many patients
• Chin strap an option, a good “trainer”
• Routine “practice” with PAP

A Note on Claustrophobia
Not all claustrophobics are the same
• Eye crowding, smothering, head straps, small spaces…
Mask style
• Some like smaller, away from eyes (pillows)
• Some want less “intense” pressure (nasal, FFM)
• Some want strapless (dental appliance – pillow combo)
• Unique: away from eyes, no pillows (whole face mask)
Pressure
• Air hunger – raise ramp or auto-PAP min
• Pressure intolerance – reduce pressure for comfort
• Teach them the ramp (don’t assume they know it!)
GIVE THEM TIME AT HOME http://ainsleyrae.blogspot.com/2014_06_01_archive.html

23:00 pm 2:30 am
3:00 am 6:30 pm
A Note About Oximetry
• Verify the patient using their PAP when
oximetry performed

Leak Trouble-shooting
• Look at download (when leak available)
– Constant
• Very poor mask fit, defect/hole, removal
• Turned on but not on patient(!)
– Fluctuating
• Patient: mouth opening, positional, removal
• Equipment:
– aPAP pressure changes without proper mask fitting
– mask change, old seals
– Examples (next slide)

Leak Examples
50 L/min
Insomnia – leaves machine running when OOB
Lost seal after first night
Not wearing (DOT)

Cost Containment
RESmart (3B Medical)
• Lost cost tubing
• Durability concerns
• Low cost machines
• Download
challenges

“I Want a Smaller Machine”
http://mytranscend.blogspot.com/2011/04/w
e-know-it-looks-strange-why-transcend.html
• Questions to discuss
– Will there be humidification?
– Do you require adherence monitoring?
• Insurance
• DOT
– Financial considerations with 2nd machine
Questions


















