Successful Treatment of Renal Abscess with Percutaneous Needle Aspiration in a Diabetic Patient with...
6
©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc. MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016 RENAL FAILURE Vol. 25, No. 4, pp. 653–657, 2003 CASE REPORT Successful Treatment of Renal Abscess with Percutaneous Needle Aspiration in a Diabetic Patient with End Stage Renal Disease Undergoing Hemodialysis I-Kuan Wang, M.D., Yu-Ming Chen, M.D., Ph.D., Yung-Chang Chen, M.D., Ji-Tseng Fang, M.D., * and Chiu-Ching Huang, M.D. Department of Nephrology, Chang Gung Memorial Hospital, Chang Gung University, Taiwan ABSTRACT Renal abscesses in patients with end stage renal disease are quite rare, and mis- diagnosis or delaying in diagnosis is frequent. This report examines a case of renal abscess in a patient with end stage renal disease on maintenance hemodialysis and diabetes mellitus, which presented with a prolonged fever. An infected diabetic foot was impressed initially. Purulent urine, pyuria, bacteriuria, and bacteremia were noted after admission. Renal abscess was diagnosed by percutaneous needle aspiration under computerized tomography guidance. The patient was treated with parenteral antibiotics and percutaneous aspiration of the abscess. Follow- up ultrasonography showed renal abscess resolution. This case demonstrated that nephrectomy was not required in selected uremic patients with renal abscess. Key Words: Chronic renal failure; Dialysis; Urinary tract infection; Renal abscess. *Correspondence: Ji-Tseng Fang, M.D., Department of Nephrology, Chang Gung Memorial Hospital, 5, Fu-Shin Street, Kweishan, Taoyuan, 333, Taiwan, Republic of China; Fax: 886-3-328-2173; E-mail: [email protected]. 653 DOI: 10.1081/JDI-120022558 0886-022X (Print); 1525-6049 (Online) Copyright & 2003 by Marcel Dekker, Inc. www.dekker.com Ren Fail Downloaded from informahealthcare.com by The University of Manchester on 11/30/14 For personal use only.
-
Upload
chiu-ching -
Category
Documents
-
view
215 -
download
0
Transcript of Successful Treatment of Renal Abscess with Percutaneous Needle Aspiration in a Diabetic Patient with...

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
RENAL FAILURE
Vol. 25, No. 4, pp. 653–657, 2003
CASE REPORT
Successful Treatment of Renal Abscess with Percutaneous
Needle Aspiration in a Diabetic Patient with End Stage
Renal Disease Undergoing Hemodialysis
I-Kuan Wang, M.D., Yu-Ming Chen, M.D., Ph.D.,
Yung-Chang Chen, M.D., Ji-Tseng Fang, M.D.,*
and Chiu-Ching Huang, M.D.
Department of Nephrology, Chang Gung Memorial Hospital,
Chang Gung University, Taiwan
ABSTRACT
Renal abscesses in patients with end stage renal disease are quite rare, and mis-
diagnosis or delaying in diagnosis is frequent. This report examines a case of renal
abscess in a patient with end stage renal disease on maintenance hemodialysis and
diabetes mellitus, which presented with a prolonged fever. An infected diabetic
foot was impressed initially. Purulent urine, pyuria, bacteriuria, and bacteremia
were noted after admission. Renal abscess was diagnosed by percutaneous needle
aspiration under computerized tomography guidance. The patient was treated
with parenteral antibiotics and percutaneous aspiration of the abscess. Follow-
up ultrasonography showed renal abscess resolution. This case demonstrated that
nephrectomy was not required in selected uremic patients with renal abscess.
Key Words: Chronic renal failure; Dialysis; Urinary tract infection; Renal
abscess.
*Correspondence: Ji-Tseng Fang, M.D., Department of Nephrology, Chang Gung
Memorial Hospital, 5, Fu-Shin Street, Kweishan, Taoyuan, 333, Taiwan, Republic of China;
Fax: 886-3-328-2173; E-mail: [email protected].
653
DOI: 10.1081/JDI-120022558 0886-022X (Print); 1525-6049 (Online)
Copyright & 2003 by Marcel Dekker, Inc. www.dekker.com
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
30/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
INTRODUCTION
Renal abscess is uncommon; its onset and clinical course are insidious, its symp-toms are highly variable, and unrecognized and untreated, it results in considerablemorbidity and mortality.[1–5] The diagnosis of renal abscess in patients with end stagerenal disease (ESRD) is frequently delayed because the urine-deprived urinary tractsare ignored as potential infection sites.[6] Renal abscess treatment in ESRD patientsfrequently requires nephrectomy.[6–8] This report investigates a diabetic patient withESRD on maintenance hemodialysis, which had a renal abscess and was successfullytreated with percutaneous aspiration and parenteral antibiotics.
CASE REPORT
A 65-year-old female patient was admitted to our hospital with a 2-day fever asher chief complaint. She had been on hemodialysis for three years for her ESRD, andwas anuric with a urinary amount of a few milliliters per day. The underlyingetiology of ESRD was diabetic nephropathy. She also had a 24-year history oftype 2 Diabetes Mellitus (DM) with insulin control, and an 8-year history of hyper-tension with medical treatment. The patient had in fact been admitted to our hospitaltwice for an infected left diabetic foot, 3 and 2 months prior to the current admis-sion. Wound cultures during previous admission yielded Staphylococcus aureus.There were no symptoms of dysuria, urinary frequency, urinary urgency, nausea,vomiting, or flank pain prior to her current admission; her body weight was 90 kgand height 152 cm. Blood pressure was 103/85mmHg, pulse rate 91/min, respiratoryrate 18/min, and body temperature 38.9�C. Physical examination showed a smallwound associated with surrounding erythematous swelling, and local heat at the leftfifth toe. There was no tenderness at the costovertebral angle. Laboratory datashowed hemoglobin 10.9 gm/dL, WBC 9400/mm3, segment 89%, Band 2%, mono-cyte 2%, and lymphocyte 7%. Blood chemistry tests showed creatinine 8.1mg/dLand Ac sugar 394mg/dL. The left diabetic foot was treated with cefazolin andgentamicin for a suspected infection. Dark red purulent urine was noted on thesecond hospitalization day. Urinalysis displayed 12–14 red blood cells per highpower field, protein 500mg/dL, and >100 white blood cells per high power field.Blood cultures and a urine culture yielded E. Coli, sensitive to gentamycin, amikacin,aztreonam, and ceftriaxone. The fever persisted despite improvement of the erythe-matous swelling of the left foot. A renal echo revealed a 4.8 cm hypoechoic renalmass with an irregular wall, and abdominal computerized tomography (CT) showeda 5.0 cm low-attenuation mass, both at the right kidney’s lower pole (Fig. 1).Percutaneous needle aspiration and biopsy under CT guidance were performed onthe 15th hospitalization day. Aspiration yielded 15 cc of dark red purulent material.Percutaneous drainage was not performed due to the small amount of pus. Septicshock immediately developed after the procedure, and the antibiotic regimen waschanged to ceftriaxone and gentamycin. The hemodynamic stabilized the followingday. The biopsy result was negative for malignancy. An aspirate culture yieldedE. coli with the same sensitivity as the previous blood and urine cultures. The anti-biotic regimen was changed to amikacin on the 22nd hospitalization day because of
654 Wang et al.
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
30/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
the persistent fever, which later subsided. The patient was discharged on the 31sthospitalization day and had an uneventful followed-up at the outpatient department.
DISCUSSION
Uremic patients have compromised immune systems and an increased infectionfrequency. Infection is a major cause of mortality and morbidity in hemodialysispatients.[9] The incidence of urinary tract infections in ESRD patients ranges from0.2 to 1.1 episodes per 100 patient-months.[10] Azotemia, infrequent voiding, lowurinary flow rates, and urinary concentration defects have all been reported asleading to bacteriuria.[11] Urinary tract infections were in fact the second mostimportant source of bacteremia, with gram-negative bacilli, mainly E. coli, almostalways being the causative microorganisms.[5,12]
Renal abscess is uncommon, with major risk factors including renal stones,urinary tract obstruction, and DM.[2–4,7,13] Enteric aerobic gram-negative bacilli,including E. coli, Klebsiella species, and Proteus species are commonly responsiblefor this infection.[4,5,7,14] The risks of urinary tract infection and renal abscessincreased in the current report’s patient since she had DM and had been anuric.
The symptoms of urinary tract infections in ESRD patients are no different topatients without renal failure, except a greater frequency of gross hematuria.[12]
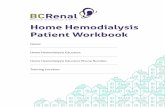
Figure 1. CT scan showing a low-attenuation mass with an irregular wall (arrow) in the right
kidney’s lower pole.
Renal Abscess in ESRD Patient 655
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
30/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
As the presenting symptoms are vague and nonspecific, a delay of weeks or monthsmay occur before a renal abscess diagnosis is made.[1–8] The typical renal abscesspresentation includes fever, chills, and flank or abdominal pain. Dysuria is notnecessarily present, although leukocytosis is generally present and the urinalysis isoften abnormal with bacteriuria, pyuria, proteinuria, or hematuria. Bacteremia isfrequently present in renal abscess patients.[1–5,7]
Computerized tomography and ultrasonography are used to establish a renalabscess diagnosis. Fowler et al. reported that ultrasonography and CT identified92% and 96% of abscesses, respectively.[4] CT scan findings commonly include asoft tissue mass of central attenuation, an inflammatory wall with a slightly higherattenuation coefficient on unenhanced views, a ring sign (a ring of increased densityin the abscess wall after injection of contrast material), obliteration of surroundingtissue planes, ipsilateral enlargement of the kidney or psoas muscle, thickening ofGerota’s fascia and gas or air fluid level within the lesion.[14] These signs are notspecific for renal abscess, and the ring sign could not be demonstrated in the currentreport’s patient, because of renal dysfunction. Percutaneous needle aspiration shouldbe performed under sonographic or CT guidance to make a definite diagnosis.
The choice of antibiotics for treatment of urinary tract infections in ESRDpatients is complicated, and the efficacy of many of these drugs depends on theconcentration achieved in the urine. Patients with reduced renal excretory functionor oligoria may be unable to achieve an adequate urine or tissue drug level.Ampicillin, trimethoprim-sulfamethoxazole, cephalosporin, semisynthetic penicillin,and aminoglycoside have been used previously.[12,15] Renal abscess treatmentincludes medical therapy, percutaneous aspiration, and surgery.[1–5,7,16] Smallabscesses (less than 3 cm) in immunocompetent patients can be treated with anti-biotics alone,[13,16] although larger abscesses (greater than 3 cm) require percuta-neous drainage or surgery. Treatment of renal abscesses in patients with renaldysfunction is more complicated, and nephrectomy is required.[6–8] Mortality ofthese patients is high—3 of 5 patients with polycystic kidney disease undergoinghemodialysis died in a previous report.[8] The current study’s patient with DMand ESRD on maintenance hemodialysis had a renal abscess, and was successfullytreated with antibiotics and percutaneous aspiration alone.
In conclusion, although renal abscesses in ESRD patients are rare, the possibi-lity should never be excluded when making a diagnosis. Because the urinary tract isnonfunctional, it is often disregarded as a potential infection site. The most impor-tant step in renal abscess diagnosis is to remember that the condition exists.Nephrectomy may be unnecessarily in certain patients who responded to medicaltherapy and abscess aspiration.
REFERENCES
1. Sheinfeld, J.; Erturk, E.; Spataro, R.F.; Cockett, A.T.K. Perinephric abscess:current concepts. J. Urol. 1987, 137, 191–194.
2. Anderson, K.A.; Mcaninch, J.W. Renal abscess: classification and review of40 cases. Urology 1980, 16, 333–338.
656 Wang et al.
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
30/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
3. Morgan, W.R.; Nyberg, L.M. Perinephric and intrarenal abscesses. Urology1985, 26, 529–536.
4. Fowler, J.E.; Perkins, T. Presentation, diagnosis, and treatment of renalabscesses: 1972–1988. J. Urol. 1994, 151, 847–851.
5. Dembry, L.M.; Andriole, V.T. Renal and perirenal abscesses. Infect. Dis. Clin.North Am. 1997, 11, 663–680.
6. Lees, J.A.; Falk, R.M.; Stone, W.J.; Mcdougal, W.S. Pyocystitis, pyonephrosis,and perinephric abscess in end stage renal disease. J. Urol. 1985, 134, 716–719.
7. Deyoe, L.A.; Cronan, J.J.; Lambiase, R.E.; Dorfman, G.S. Percutaneousdrainage of renal and perirenal abscesses: results in 30 patients. Am. J.Roentgenol. 1990, 155, 81–83.
8. Sweet, R.; Keane, W.F. Perinephric abscess in patients with polycystic kidneydisease undergoing chronic dialysis. Nephron 1979, 23, 237–240.
9. Lazarus, J.M. Complications in hemodialysis: an overview. Kidney Int. 1980,18, 783–796.
10. Kessler, M.; Hoen, B.; Mayeux, D.; Hestin, D.; Fontenaille, C. Bacteremia inpatients on chronic hemodialysis. Nephron 1963, 64, 95–100.
11. Goldblum, S.E.; Reedm, W.P. Host defenses and immunologic alterationsassociated with chronic hemodialysis. Ann. Intern. Med. 1980, 93, 597–613.
12. Rault, R. Symptomatic urinary tract infection in patients on maintenancehemodialysis. Nephron 1984, 3, 82–84.
13. Siegel, J.F.; Smith, A.; Moldwin, R. Minimally invasive treatment of renalabscess. J. Urol. 1996, 155, 52–55.
14. Gerzof, S.H.; Gale, M.E. Computerized tomography and ultrasonography fordiagnosis and treatment of renal and retroperitoneal abscesses. Urol. Clin.North Am. 1982, 9, 185–193.
15. Bennett, W.M.; Craven, R. Urinary tract infections in patients with severe renaldisease. JAMA 1976, 236, 946–948.
16. Rives, R.K.; Harty, J.I.; Amin, M. Renal abscess: emerging concepts ofdiagnosis and treatment. J. Urol. 1980, 124, 446–447.
Renal Abscess in ESRD Patient 657
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
30/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
The
Uni
vers
ity o
f M
anch
este
r on
11/
30/1
4Fo
r pe
rson
al u
se o
nly.