
Successful Clinical Experiences of Using Standardized Nursing Languages T. Heather Herdman, PhD; RN...
25
Successful Clinical Experiences of Using Standardized Nursing Languages T. Heather Herdman, PhD; RN Executive Director NANDA International
-
Upload
homer-allison -
Category
Documents
-
view
214 -
download
0
Transcript of Successful Clinical Experiences of Using Standardized Nursing Languages T. Heather Herdman, PhD; RN...

Successful Clinical Experiences of Using Standardized Nursing Languages
T. Heather Herdman, PhD; RN
Executive Director
NANDA International

Patient Safety
• Patient safety is the number one concern in all delivery of health care
• Assuring patient safety requires, at a minimum:• Competent, intelligent health care professionals• Expertise in critical thinking and clinical judgment• Holistic approach to care that considers the patient’s
priorities, not simply the health care providers’ priorities• Sufficient resources for delivery of care• Patient/family participation in care
Quality of Care
• Institute of Medicine (2001) identified health outcomes of consumers as the most important indicator of quality health care
• Identification of those outcomes is critical for identification, evaluation and prediction of successful interventions
• Assumptions underpinning this include:• Effectiveness of interventions varies among providers• Knowledge development of the effectiveness of interventions is
the responsibility of health care providers• When effectiveness is compromised, health care consumers may
be better off without providers• (Lunney, 2009)
Quality of Care
• 2008 research on quality of care in 73 hospital systems (1,510 hospitals) demonstrated significant variation in care and outcomes for patients with myocardial infarction, congestive heart failure, pneumonia and surgical infection prevention (Hines & Joshi, 2008)
• These are well defined conditions with research-based signs & symptoms
• How is this possible?
• 80% of all health care worldwide is delivered by nurses (NPR,
2009)
• Nurses are professionally accountable for interventions based on diagnoses (nursing and medical)
Quality of Care
• Evidence-based practice• Decrease variation in care• Improve reliance on research in daily practice• Improve patient outcomes
• This approach relies on:• Definitive knowledge base for nursing science and
practice• Distinct, research-based conceptual analysis of
phenomena of concern to nursing science and practice• Use of this knowledge in clinical judgment• Use of standardized terminology to represent these
concepts

Evidence-based Practice & Standardized Nursing Languages
• NANDA, NOC, NIC developed through research• NANDA-I is continually revised based on latest
research
• Evidence-based languages require, at a minimum, the following things which must be based on research & clinical literature:
• Clear, concise, conceptual label• Standardized definitions of terms• Standardized defining characteristics
Lack of Standardization & Evidence-Based Practice
• Confusion in clinical practice• Misdiagnosis• Inappropriate outcome determination• Ineffective interventions

What’s in a definition?
Axis 1 Axis 2 Axis 3 Axis 4 Axis 5 Axis 6 Axis 7
Diagnostic concept
Subject of diagnosis
Judgment Location Age Time Status of diagnosis
Anxiety Individual Compro-mised
Auditory Infant Acute Actual
Fear Family Dysfunc-tional
Cerebral Toddler Chronic Health promotion
Coping Group Excessive Kinesthe-tic
Preschool Child
Intermit-tent
Risk
Hopeless-ness
Commun-ity
Imbalanced Tactile School-aged child
Continu-ous
Memory Ineffective Visual Adole-scent
Moral distress
Low Adult
Thought process
Perceived Older adult
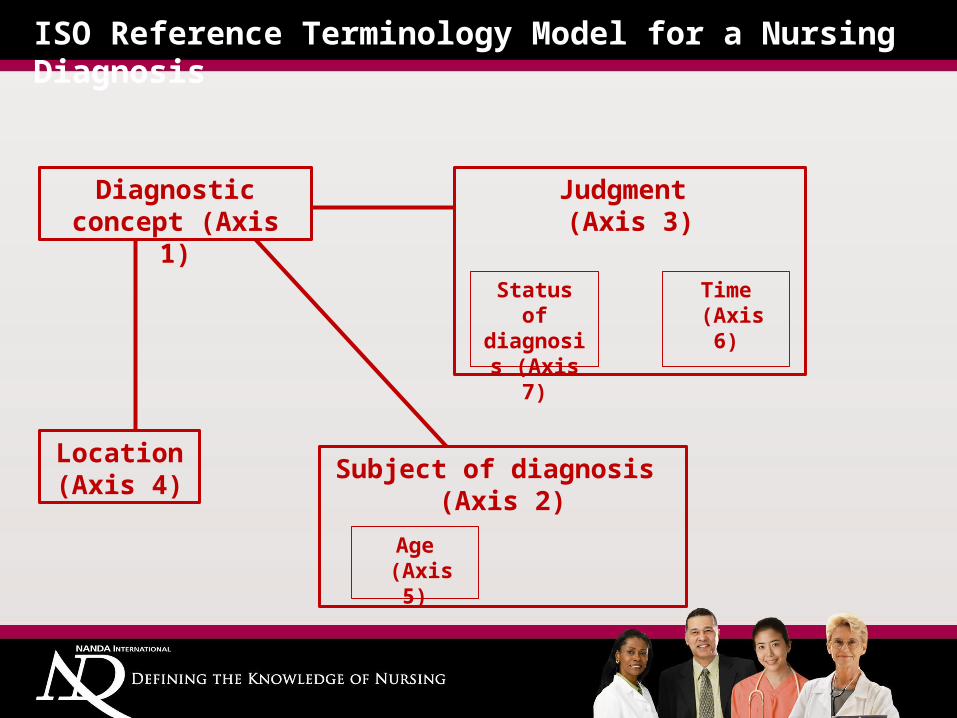
ISO Reference Terminology Model for a Nursing Diagnosis
Judgment (Axis 3)
Diagnostic concept (Axis 1)
Location (Axis 4)
Subject of diagnosis (Axis 2)
Status of diagnosis (Axis 7)
Time (Axis 6)
Age (Axis 5)

• Case study• 78 year old man whose wife has just died• Easily distracted• Paranoid• Unable to keep track of time / forgetful• Loses glasses, keys, medicine frequently• Not sleeping well – wakens frequently• Poor concentration• Jittery• Irritable• Worried
Perils of Clinical Creation of a Nursing Diagnosis

Perils of Clinical Creation of a Nursing Diagnosis
Imbalanced (Axis 3)
Thought process(Axis 1)
N/A (Axis 4)
(Individual)(Axis 2)
Actual(Axis 7)
Actual (Axis 6)
Older adult (Axis 5)
Acute imbalanced thought process

Chronic imbalanced thought process
• ACUTE• Lasting less than six months
• IMPAIRED• Damaged, weakened
• THOUGHT PROCESS• Cognitive operations and activities
• Defining characteristics• NONE
• Related factors• NONE

Chronic Pain: What is the definition?
Which is the correct definition – and why should we care???1. Unpleasant sensory & emotional experience arising from actual or
potential tissue damage or described in terms of such damage; sudden or slow onset of any intensity from mild to severe, constant or recurring without an anticipated or predictable end and a duration of greater than 6 months
OR
2. Unpleasant sensory & emotional experience arising from actual or potential tissue damage or described in terms of such damage; slow onset of any intensity from mild to severe, constant in nature, without an anticipated or predictable end and a duration of greater than 3 months

Diagnostic Reasoning in Nursing
• Complexity of the phenomena of concern for nursing are “unrivaled” (Webster, 1994) – due to the holistic nature of nursing’s focus: human responses
• The mere complexity of the phenomena necessitate that nurses clearly understand and can identify them when they occur in practice
• Requires conceptual analysis of these phenomena, including identification of the “signs & symptoms”, or defining characteristics?
• How else can we measure diagnostic accuracy?

Requisites for successful clinical experiences
• Identification and use of a holistic nursing assessment framework that lends itself to the identification of defining characteristics
• Nurses must have expertise in:• Assessment and reevaluation of those assessments• Standardized nursing languages and their component
parts• Hypothesis generation• Planning of care in conjunction with patients, families
and other health care providers• Evaluating and refining of that plan of care

Assessment
• Many texts teach the nursing process as a subset of medical diagnosis
• Ignores importance of nursing assessment• Lacks focus on patient/family individuality• Ignores patient/family priorities• Assumes that all human responses to an actual health
problem are the same
• Linking the planning of patient care to the nursing and interdisciplinary assessment is more meaningful
Successful clinical experiences
• Involve staff using evidence-based care• Identify high priority patient segments• Identify high priority human responses (nursing
diagnoses)• Identify high frequency human responses (nursing
diagnoses)• Determine realistic outcomes for each area of care• Identify critical interventions

Successful clinical experiences: Post-operative care
Recovery Room
Surgical Unit Home Health Outpatient Clinic
Acute Pain Moderate pain Mild to moderate pain
Mild pain Minimal pain
•Encourage use of research to guide potential diagnoses•Require link to assessment data to ensure patient-centeredcare•Discuss & acknowledge difficulties with languages
•Syntax•Translation•Lack of “natural” speech
•Contrast Standardized Language – and ability to computerize it – with handwritten, “home grown” terms or terms that are “put together” from a list of standardized terms – but with no accessible standardized definitions or defining characteristics
Successful clinical experiences: Electronic health record
• Begin with nursing assessment, ensuring that defining characteristics, risk and related factors are present in the assessment screens
• Use defining characteristics to suggest a list of potential diagnoses (hypothesis generation)
• Use assessment – or reassessment – to refine this list to most appropriate nursing diagnoses
• Identify achievable outcomes• Identify interventions most likely to have positive
impact at lowest cost

Strategies
• Top level nurse administrators • Must understand need for standardized languages• Lead drive to incorporate into organization• Appoint committed leaders to implement• Identify how data from languages will be used to:
• Improve patient outcomes• Improve effectiveness of nursing care• Identify nurses’ impact on patient outcomes• Validate need for more nurses• Drive cost of care down

Strategies
• Engage key stakeholders • Formal and informal leaders• Instructors / clinical educators• Informaticists• Quality improvement specialists• Strongest clinical nurses
• Set mission and vision for the project• Keep nursing discipline at the center but highlight
impact on the patient
Strategies
• Use consultants or experts to initiate project• Build excitement• Improve buy-in• Shows commitment of organization
• Support teams by providing time• Team building• Planning for implementation• “Train the trainer” curriculum design• Roll out slowly – start in areas with key champions to
gain small successes• Celebrate success
Strategies
• Provide ongoing educational updates• Encourage membership in NANDA-I to enable
international dialogue and partnership• Consistently review progress
• Impact on patient outcome critical• Identify changes in communication among nurses and
between disciplines• Engage patients and families to improve satisfaction

• Identify lack of appropriate standardized terms• Encourage and support staff to develop new
terms or adapt current terms• Submit to NANDA International, NOC and/or NIC
to improve the taxonomies• Review training with each new edition of
NANDA/NOC/NIC• Emphasize changes, but also provide general
overview of use of the languages
Successful clinical experiences