Substance misuse and violence: a comparison of special hospital inpatients diagnosed with either...
11
Substance misuse and violence: a comparison of special hospital inpatients diagnosed with either schizophrenia or personality disorder MARK CORBETT Research Worker, Rampton Hospital Authority, Retford, Nottinghamshire, DN22 0PD, UK CONOR DUGGAN Professor, Division of Forensic Mental Health, University of Leicester, Leicester LE5 OLE, UK EMMET LARKIN Forensic Psychiatrist and Clinical Director, Arnold Lodge RSU, Cordelia Close, Leicester LE5 0LE, UK ABSTRACT: There is increasing interest in the relationship between schizophrenia, substance misuse and serious violence. We compared the pattern of substance misuse in inpatients with schizophrenia convicted of serious offences with that of a matched group with personality disorder. We also compared those with and without a history of substance misuse in their use of drugs or alcohol at the time of their violent index offence. We matched 75 substance misusing patients with schizophrenia with a group of patients with personality disorder and compared the types of substances misused in both groups. We compared these two groups with a larger sample of inpatients without a history of substance misuse to determine the presence of substance misuse at the time of the index offence. No differences were found between the matched groups in their choice of drugs. Drug abusing male inpatients with a personality disorder were significantly more likely to have consumed alcohol at the time of the violent offence compared with the other groups. Although the reporting of substance misuse was unexpectedly low, our data (a) showed no evidence that patients with schizophrenia preferentially choose to misuse specific types of drugs compared with personality disor- dered patients and (b) that intoxication with alcohol at the time of the violent offence may be important in male patients with a personality disorder and a history of sub- stance misuse. Introduction The established link between schizophrenia, substance misuse and violence suggests that this will be an increasingly important area for mental health workers. Although schizophrenia has only a modest association with violence overall (Wessley et al., 1994), it is over-associated with serious violence espe- cially in the presence of substance misuse (Swanson et al., 1990; Swanson, 1994; Dyer, 1996). Apart from its clinical importance in increasing the risk of Criminal Behaviour and Mental Health, 8, 311–321 1998 © Whurr Publishers Ltd 311
-
Upload
mark-corbett -
Category
Documents
-
view
212 -
download
0
Transcript of Substance misuse and violence: a comparison of special hospital inpatients diagnosed with either...

Substance misuse and violence: acomparison of special hospitalinpatients diagnosed with eitherschizophrenia or personality disorder
MARK CORBETT Research Worker, Rampton Hospital Authority, Retford,Nottinghamshire, DN22 0PD, UK
CONOR DUGGAN Professor, Division of Forensic Mental Health,University of Leicester, Leicester LE5 OLE, UK
EMMET LARKIN Forensic Psychiatrist and Clinical Director, Arnold LodgeRSU, Cordelia Close, Leicester LE5 0LE, UK
ABSTRACT: There is increasing interest in the relationship between schizophrenia,substance misuse and serious violence. We compared the pattern of substance misusein inpatients with schizophrenia convicted of serious offences with that of a matchedgroup with personality disorder. We also compared those with and without a history ofsubstance misuse in their use of drugs or alcohol at the time of their violent indexoffence. We matched 75 substance misusing patients with schizophrenia with a groupof patients with personality disorder and compared the types of substances misused inboth groups. We compared these two groups with a larger sample of inpatients withouta history of substance misuse to determine the presence of substance misuse at thetime of the index offence. No differences were found between the matched groups intheir choice of drugs. Drug abusing male inpatients with a personality disorder weresignificantly more likely to have consumed alcohol at the time of the violent offencecompared with the other groups. Although the reporting of substance misuse wasunexpectedly low, our data (a) showed no evidence that patients with schizophreniapreferentially choose to misuse specific types of drugs compared with personality disor-dered patients and (b) that intoxication with alcohol at the time of the violent offencemay be important in male patients with a personality disorder and a history of sub-stance misuse.
Introduction
The established link between schizophrenia, substance misuse and violencesuggests that this will be an increasingly important area for mental healthworkers. Although schizophrenia has only a modest association with violenceoverall (Wessley et al., 1994), it is over-associated with serious violence espe-cially in the presence of substance misuse (Swanson et al., 1990; Swanson,1994; Dyer, 1996). Apart from its clinical importance in increasing the risk of
Criminal Behaviour and Mental Health, 8, 311–321 1998 © Whurr Publishers Ltd 311
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 311

violence, there is the additional question about whether these patients chooseto misuse certain substances over others. This selective matching of specificsubstances (and their subjective effects) with specific symptoms might suggestthat substance misuse in schizophrenia is an attempt at self-medication(Dixon et al., 1991) and might also illuminate the neurochemical basis ofschizophrenia (McLellan and Druley, 1977).
The previous studies on whether there is a relationship between schizo-phrenia and a specific pattern of substance misuse have shown inconsistentfindings. Schneier and Siris (1987) in a review, concluded that a strikinglynon-random distribution of substance misuse existed with schizophrenicgroups using more amphetamines, cocaine, cannabis, hallucinogens,inhalants, tobacco and caffeine, and less alcohol, opiates and sedative hypnotics than control populations (of varying composition). Although thissupports a selective matching by diagnosis, few of the studies in this reviewcontrolled for social and demographic factors which might, independent ofdiagnosis, correlate with the choice of substances misused. It is no surprisetherefore that several other studies (for instance, Mueser et al., 1990, 1992;El-Guebaly and Hodgins, 1992; Cuffel et al., 1993; Baigent et al., 1995) con-clude that price, availability, and demographic characteristics (such as sex, ageand socioeconomic status) are strong predictors of type of substance abuse andthat diagnoses have little, if any, influence. However, these studies again didnot involve pairing patients with schizophrenia with controls of a differentpsychiatric diagnosis. Since the pattern of substance misuse has changed radi-cally over the past 20 years (Pope et al., 1990), such matching between thepatients with schizophrenia and the control population is essential to ensurethat like is compared with like.
Another important question is whether a history of substance misusemakes it more likely that such substances are used at the time of a violentoffence and therefore that this might increase the risk of such offending.Common sense would suggest that this be the case but we need to establishthis association.
Our study had two aims: (a) to investigate whether patients detained inhigh security with schizophrenia selectively misuse certain substances com-pared with a matched sample of patients with personality disorder and (b) todetermine the importance of substance misuse at the time of the violent indexoffence in those with and without a history of long-term drug misuse.
Method
The sample
The study sample was selected from psychiatric patients admitted tothree English high security (special) hospitals (Ashworth, Broadmoor orRampton) between 1972 and 1995. All the patients within special hospitals
312 Corbett et al.
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 312

are compulsorily detained and the majority have been convicted of violentoffences. Data were obtained from the Special Hospitals’ Case Register whichis a database of information obtained from standardized structured interviewswith patients on admission in addition to data gathered from the patient’smedical history file, medical records, criminal records and police reports. Togain entry into the study, the patient had to have a sole diagnosis by theresponsible medical officer (RMO) of either schizophrenia or of personalitydisorder and to have admitted to substance misuse (see below). We includedonly Caucasians, thereby avoiding the controversy surrounding diagnosis ofschizophrenia in Afro-Caribbeans (Littlewood and Lipsedge, 1981), whilealso excluding the need to match patients for ethnicity. In addition to thisprimary comparison, we also selected two comparison groups, again allCaucasian, one with a diagnosis of schizophrenia and the other with a diag-nosis of personality disorder, who had also been convicted of violent indexoffences but who did not admit to a history of substance misuse.
Drug misuse
As part of the initial case register interview, details of illicit drug use duringthe year before admission were requested and are coded as follows:
(i) those who have taken the drug on one occasion or on very few occasionsonly;
(ii) those who have taken the drug intermittently (e.g. at weekends over atleast three months);
(iii) those who have taken the drug regularly (daily or several times a weekover several months or longer);
(iv) those who consider themselves as addicted or who have a history of atten-dance at a drug treatment unit.
Amphetamines, barbiturates, cannabis, LSD and opiates are all coded in thisway. Only patients coded as level (ii), (iii) or (iv), for at least one of thesesubstances, were eligible for inclusion in this study. The study is thereforeconcerned with whether or not a patient admitted to the regular use of a par-ticular substance and not necessarily whether or not they were classed as sub-stance abusers. We also classed as positive those patients who admitted todrinking four units of alcohol, or more, per day. Information on drug or alco-hol use at the time of the index offence was also recorded separately on theSpecial Hospitals’ Case Register.
Matching
To control for different patterns of drug use over time, between age groups,and between social classes, patients were matched for decade of birth, age on
Substance misuse and violence 313
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 313

314 Corbett et al.
admission (five-year intervals, i.e. 15–20, 20–25, etc.) and social class (classi-fied according to the Office of Population Censuses and Surveys’ Classificationof Occupations publication). Patients were also to be paired for sex but, of the111 patients with schizophrenia who satisfied the inclusion criteria, only three(3%) were female compared with 45 out of 160 (28%) for the personality dis-order group. The pairing was therefore confined to males only, with the femalepersonality disorder group being described separately. After endeavouring tomatch the 111 patients suffering from schizophrenia with the 160 personalitydisordered patients on the three criteria, 75 pairs resulted.
Statistical analysis
McNemar’s test (with a continuity correction) was used to calculate the chi2
values for the matched samples. For those samples that were not matched, astandard chi2 (for two independent proportions) was used.
Results
Of the 1111 patients with a sole diagnosis of schizophrenia admitted to any ofthe three special hospitals between 1972 and 1995, 167 (15%) admitted toillegal substance misuse at Case Register level (ii) or above (only threepatients were classed as level (iv)). Only 3.3% of the 1111 were classified asdrug dependent and 2.3% as alcohol dependent by their RMO. There were885 patients with personality disorder of whom 158 (18%) admitted to drugmisuse. Of these 885, 4.5% and 6.4% were classified as drug or as alcoholdependent respectively by their consultant. The ages of the study cohorts wereas follows: men with schizophrenia (mean 27.6, SD 5.8, range 19.6–45.0), menwith personality disorder (mean 27.3, sd, 6.3, range, 18.6–47.0), women withpersonality disorder (mean 23.6, SD 4.4, range 17.7–40.3). Table 1 shows thepercentage of those who admitted to misusing each type of drug in the
Table 1: Details of substance misuse prevalence in the three cohorts of special hospital patientswho admitted to substance misuse during the year before admission (% in parentheses)
Personality disorder Schizophrenia Personality disorderMales (n = 75) Males (n = 75) Females (n = 45)
Amphetamines 26* (35) 21(28) 23 (51)Barbiturates 15 (20) 8 (11) 11 (24)Cannabis 67* (91) 73 (97) 35 (78)LSD 18* (24) 15 (20) 17 (38)Opiates 8 (11) 10* (14) 14 (31)Alcohol 63 (84) 62 (83) 35** (80)
Note:* n = 74; **n = 44
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 314

matched pair of male patients and for the female patients with a personalitydisorder.
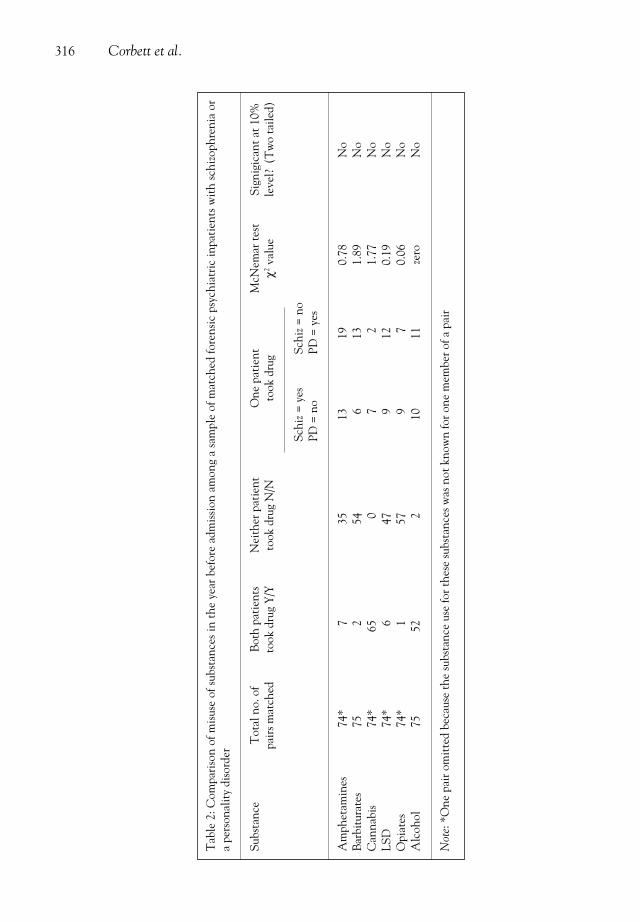
For the paired male sample the mean number of illegal substances used (aminimum of one and a maximum of five per patient) was 1.8 for the patientswith a personality disorder and 1.7 for the patients with schizophrenia (notsignificantly different when analysed using the paired t-test, assuming normaldistributions). Six patients with schizophrenia and seven patients with a per-sonality disorder were also coded as having abused another type of substancenot included in the table (e.g. ecstasy or cocaine). The mean number of illegalsubstances abused for the personality disordered females was 2.5. Table 2shows the results of the analyses examining any differences between the twomatched groups regarding choice of drug used; none of the comparisons wassignificantly different.
Criminal offences
Table 3 shows the index offences committed by the three patient groups. Wegrouped together the homicidal and violent offences and compared their fre-quency with the remainder of the offending in the two male groups usingMcNemar’s test. The schizophrenia group were significantly more likely tohave been convicted of a violent or homicidal offence compared with thepersonality disordered group (chi2=13.8, p <0.001). Conversely, those withpersonality disorder were more likely to have been convicted of a sexualoffence or arson.
Table 4 compares those in our sample with a history of substance misusewho had committed a violent or homicidal index offence with a sample of sim-ilarly diagnosed patients who had also committed a violent or homicidal indexoffence, but who had not admitted to substance misuse in the year prior toadmission to hospital. The table compares the numbers in each diagnostic cat-egory for drug or alcohol intoxication at the time of the index offence. Of the60 patients with schizophrenia and a history of substance misuse, 26 (43%) hadtaken drugs or alcohol at the time of the offence (five taking both). Of the 36patients with personality disorder, a history of substance misuse and a homici-dal or violent offence, 23 (64%) had taken drugs or alcohol at the time of theoffence (with again five taking both). For the two groups with a history of sub-stance misuse, the patients with a personality disorder were significantly morelikely to have consumed alcohol at the time of the offence compared with thepatients with schizophrenia (chi2=9.1, p <0.003). When the rates of substancemisuse in these two groups are compared with similarly diagnosed patients witha violent offence but without a reported history of substance misuse, both theformer groups as expected were more likely to have taken illegal drugs at thetime of the offence (27% versus 5% for those with schizophrenia and 22% ver-sus 3% for the personality disordered). For alcohol, however, the pattern wasdifferent: patients with personality disorder and a history of substance misuse
Substance misuse and violence 315
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 315
316 Corbett et al.
Tab
le 2
: Com
pari
son
of m
isus
e of
sub
stan
ces
in t
he y
ear
befo
re a
dmis
sion
am
ong
a sa
mpl
e of
mat
ched
fore
nsic
psy
chia
tric
inpa
tien
ts w
ith
schi
zoph
reni
a or
a pe
rson
alit
y di
sord
er
Subs
tanc
eT
otal
no.
of
Bot
h pa
tien
ts
Nei
ther
pat
ient
One
pat
ient
M
cNem
ar te
st
Sign
igic
ant a
t 10%
pair
s mat
ched
took
dru
g Y
/Yto
ok d
rug
N/N
took
dru
gχ2
valu
ele
vel?
(T
wo
taile
d)
Schi
z = y
esSc
hiz =
no
PD =
no
PD =
yes
Am
phet
amin
es74
*7
3513
190.
78N
oB
arbi
tura
tes
752
546
131.
89N
oC
anna
bis
74*
650
72
1.77
No
LSD
74*
647
912
0.19
No
Opi
ates
74*
157
97
0.06
No
Alc
ohol
7552
210
11ze
roN
o
Not
e: *
One
pai
r om
itte
d be
caus
e th
e su
bsta
nce
use
for t
hese
subs
tanc
es w
as n
ot k
now
n fo
r one
mem
ber o
f a p
air
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 316

were twice as likely as the two comparison groups to have taken alcohol at thetime of the index offence. Conversely, patients with schizophrenia and a histo-ry of substance misuse were no more likely than the two comparison groups tohave taken alcohol at the time of the violent offence.
Discussion
There were three main findings from this study. First, we failed to establishthat patients with schizophrenia detained in a special hospital had a differentpattern in their choice of illicit drugs compared with similarly detained
Table 4: Comparison of sample groups of special hospital patients for whether drugs oralcohol were taken shortly before the index offence (violent and homicide offences only)(% in parentheses)
Personality Schizophrenic, Personality Schizophrenic,disordered, history of illegal disordered, no history
history substance misuse no history of illegal of illegal of illegal substance misuse
substance misuse substance misuse
n 36* 60 273 for alcohol 356 for alcohol**244 for drugs **360 for drugs
Took alcohol 20 (56) 15 (25) 74 (27) 70 (20)Took illegalsubstances 8 (22) 16 (27) 7 (3) 17 (5)
Notes:*Details of drugs/alcohol relating to the offence were not known for four of the 40violent/homicide patients with a personality disorder ** The sample sizes for drugs and alcohol at the time of offence are different because forsome patients only partial information was available, e.g. it was known that a patient wasdefinitely under the influence of alcohol but the presence of drugs was coded ‘not known’.
Table 3: Index offences committed by special hospital patients with substance misuse histo-ries in the year before admission (% in parentheses)
Type of offence Personality disorder Schizophrenia Personality(m) (m) disorder (f)
Homicide 21 (28) 40 (53) 3 (7)Violence 19 (25) 20 (27) 10 (22)Threat of murder 2 (3) 1 (1) 0 (0)Sexual 14 (19) 1 (1) 1 (2)Arson 10 (13) 3 (4) 19 (42)Robbery 1 (1) 8 (11) 2 (4)Other 7 (9) 1 (1) 6 (13)No Offence 1 (1) 1 (1) 4 (9)Total 75 75 45
Substance misuse and violence 317
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 317

patients with personality disorder. That is, we did not find a selective associa-tion of certain illicit drugs with diagnosis. Second, we found that patientswith a history of substance misuse were significantly more likely to take illegaldrugs at the time of their violent index offence compared with violent offend-ers with the same diagnosis but without a history of drug abuse. Third, wefound that the personality-disordered men who also admitted to a history ofsubstance misuse were twice as likely as the comparison groups to take alcoholat the time of the violent offence.
We found no significant differences between matched groups of drug abus-ing patients with schizophrenia or a personality disorder on examining thepattern of substance misuse. These findings support the belief of Mueser et al.(1992) that it is the availability of illicit drugs which is the important deter-minant of who abuses which substance, irrespective of its psychoactive effects,and that the prevalence of substance abuse in an individual’s social environ-ment, including their ethnic and peer group, influences the availability of dif-ferent drugs, and hence the likelihood that they will be abused. Hence thefailure to control for such variables as age, socioeconomic factors, sex and eth-nicity may explain the differences found between the drug habits of patientswith schizophrenia and the comparison groups found in previous studies.
Our data show that patients with schizophrenia do not use a specific groupof drugs as compared with a matched group of personality disordered patients.Cuffel et al. (1993), in another study which again did not support a specificpattern of drug misuse, observed that while certain demographic variables(ethnicity, socioeconomic status and marital status) were not associated withgreater risk for substance abuse in those with schizophrenia, other demograph-ic factors (such as being young and a male) were, as well as the co-occurrenceof depression. They conjectured that drug misuse in schizophrenia wasinvolved with the general effect of relieving boredom, depression and anxiety,and also to facilitate social contact.
Our second finding that those with a history of substance abuse are alsomore likely to take drugs at the time of the violent index offence is notsurprising but nevertheless is clinically important. These data have greatervalidity in that there was independent evidence from the depositions of themental state of the offender at the time of the index offence and hence thesource was not merely the individual’s own self-report which is prone tounder-reporting and comprised much of the data for the Case Register. In thecomparison between those with and without a history of substance misuse, wefound that the former were five times (for those with schizophrenia) andseven times (for those with personality disorder) more likely to have takendrugs at the time of the violent index offence.
Alcoholism has a significant association with violent offending (Hodge,1993). For example, Thomas and McMurran (1993) studied a sample of patientsat Rampton Hospital and found that, among those who had committed homi-cide, there was a disproportionate number of patients with a history of high
318 Corbett et al.
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 318

alcohol consumption. Our third finding also supports this association with atleast a fifth of the patients taking alcohol at the time of the violent offence.However, this use of alcohol was especially prominent (56%) in the personality-disordered male patients who also admitted to a history of substance misuse. Incontrast, patients with schizophrenia and a history of substance misuse had thesame level of alcohol intoxication as the two control non-substance-misusingcomparison groups. Again, we believe that this may be important clinically inthat future violent behaviour in personality-disordered individuals (as comparedwith those with schizophrenia) is very difficult to predict. This finding requiresreplication but suggests that the combination of illicit drugs, alcoholic intoxica-tion and personality disorder in males may be an important predictor of futureviolent behaviour. Hence, these results may be important for both risk manage-ment and the targeting of therapeutic intervention.
This study had limitations. First, the study considered special hospitalpatients only and this severely limits the generalizability of the results.Second, the retrospective nature of the study severely restricted the nature ofthe inquiry. For instance, data on the use of cocaine were not collected andtherefore we did not include this commonly misused drug in the analysis.Third, it was not possible to examine many female patients with a history ofsubstance misuse and schizophrenia which may be a reflection of the lesssevere course in female patients with schizophrenia (Goldstein, 1988). Fourth,patients with a dual diagnosis of schizophrenia and substance misuse may bemisdiagnosed as having schizophrenia when the features of psychosis may bedrug induced. However, we believe that this is unlikely in this setting as thepatients had usually been ill for some time and further substance misuse with-in a special hospital is most unlikely, therefore we would argue that this is atrue co-morbidity of schizophrenia and substance misuse.
A more significant limitation, given the reported frequent co-occurrence ofmental disorder with substance misuse, was that such a co-occurrence in thissample was relatively uncommon. This low rate of substance misuse in thementally disordered in special hospitals has also been reported recently in amore systematic record survey of all patients resident in special hospitals over asix-month period (Taylor et al., 1998). They found rates of substance misuse of7.5% in those with schizophrenia alone and 14% in those with personality dis-order alone. The comparable figures in our study were 15% and 18% respec-tively. There are a number of non-mutually exclusive explanations for theselow rates. First, the presence of substance misuse may not be adequatelyinquired about or documented. Second, patients are known to under-reporttheir level of substance misuse (Test et al., 1989) and may be especially likelyto do so when being compulsorily detained. Third, the presence of co-morbidsubstance misuse may be a barrier to being admitted to a special hospital.Fourth, as Taylor et al. (1998) point out, patients admitted to a special hospitalgenerally have long durations of admission, hence data on current inpatientsmay reflect a pattern of behaviour which was prevalent several years previously
Substance misuse and violence 319
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 319

when substance misuse was much less common. Without more data, it is notpossible to judge which of these is the correct explanation; however, for thisstudy under-reporting is not such a problem provided that there was not a sys-tematic bias in the under-reporting of either group and we have no reason tobelieve that this was the case. Set against these limitations, our study had theadvantage over many previous investigations in that it contained a relativelylarge sample which we matched by factors which might affect substance misuse(e.g. decade of birth etc.).
In conclusion, we have established that while patients with schizophreniado not have a specific pattern of drug misuse, patients with either schizophre-nia or personality disorder who have a history of substance misuse are signifi-cantly more likely to use illicit drugs at the time of a violent offence comparedwith similarly diagnosed patients without such a history. We have also shownthat alcohol was a frequent accompaniment in violent offending in all thegroups studied but that it was especially common in male patients with a his-tory of substance misuse and personality disorder. From these data, we canonly conjecture about the role of substance misuse in the offending behaviourbut it is clear that this is common in those who commit violent offences. Asthere is now an imperative to estimate the risk of future violence among thementally disordered, these data provide additional empirical support for theimportance of eliciting a history of substance misuse for both satisfactory riskmanagement and the better targeting of our therapeutic effort (Johns, 1997).
Acknowledgement
The authors would like to thank Mrs Rita Dacey for her assistance in provid-ing data from the Special Hospitals’ Case Register. The authors would alsolike to thank Professor Pamela Taylor and Doctor Andrew Johns for theirhelpful comments on an earlier draft of this manuscript.
References
Baigent M, Holme G, Hafner RJ (1995) Self reports of the interaction between substance abuseand schizophrenia. Australian and New Zealand Journal of Psychiatry29: 69–74.
Cuffel BJ, Heithoff KA, Lawson W (1993) Correlates of patterns of substance abuse amongpatients with schizophrenia. Hospital and Community Psychiatry 44(3): 247–51.
Dixon L, Haas G, Weiden PJ et al. (1991) Drug abuse in schizophrenic patients: clinical corre-lates and reasons for use. American Journal of Psychiatry 148 (2): 224–30.
Dyer C (1996) Violence may be predicted among psychiatric patients. British Medical Journal313–18.
El-Guebaly N, Hodgins DC (1992) Schizophrenia and substance abuse: prevalence issues.Canadian Journal of Psychiatry 37: 704–10.
Goldstein JM (1988) Gender differences in the course of schizophrenia. American Journal ofPsychiatry 145: 684–9.
Hodge JE (1993) Alcohol and violence. In Taylor PJ, ed. Violence in Society) London: RoyalCollege of Physicians, pp 127–37.
320 Corbett et al.
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 320

Johns A (1997) Substance misuse: a primary risk and a major problem of comorbidity.International Review of Psychiatry 9: 233–41.
Littlewood R, Lipsedge M (1981) Some social and phenomenological characteristics of psy-chotic immigrants. Psychological Medicine 11: 289–302.
McLellan AT, Druley KA (1977) Non random relation between drugs of abuse and psychiatricdiagnosis. Journal of Psychiatric Research 13: 179–84.
Mueser KT, Yarnold PR, Levinson DF et al. (1990) Prevalence of substance abuse in schizo-phrenia: demographic and clinical correlates. Schizophrenia Bulletin 16 (1): 31–56.
Mueser KT, Yarnold PR, Bellack AS (1992) Diagnostic and demographic correlates of sub-stance abuse in schizophrenia and major affective disorder. Acta Psychiatrica Scandinavica85: 48–55.
Office of Population Censuses and Surveys (1980) Classification of Occupations. London:HMSO.
Pope HG, Ionescu-Pioggia M, Aizley HG et al. (1990) Drug use and life style among collegeundergraduates in 1989: a comparison with 1969 and 1978. American Journal of Psychiatry147: 998–1001.
Schneier FR, Siris SG (1987) A review of psychoactive substance use and abuse in schizophre-nia: patterns of drug choice. Journal of Nervous and Mental Disease 175 (11): 641–52.
Swanson JW (1994) Mental disorder substance abuse and community violence: an epidemio-logical approach. In Monahan J, Steadman H, eds. Violence and Mental DisorderDevelopments in Risk Assessment. Chicago: University of Chicago Press, pp 101–36.
Swanson JW, Holzer CE, Ganju VK et al. (1990) Violence and psychiatric disorder in the com-munity: evidence from the Epidemiologic Catchment Area Surveys. Hospital andCommunity Psychiatry 41 (7): 761–70.
Taylor PJ, Leese M, Williams D, Butwell M, Daly R, Larkin E (1998) Mental disorder and vio-lence: a special (high security) hospital study. British Journal of Psychiatry 172: 218–26.
Test MA, Wallisch LS, Allness DJ et al. (1989) Substance abuse in young adults with schizo-phrenic disorders. Schizophrenia Bulletin 15: 465–76.
Thomas G, McMurran M (1993) Alcohol related offending in male special hospital patients.Medicine Science and the Law 33: 29–32.
Wessley S, Castle D, Douglas AJ, Taylor PJ (1994) The criminal careers of incident cases ofschizophrenia. Psychological Medicine 24 483–502.
Address correspondence to: Professor Conor Duggan PhD, MD, MRCPsych, Division ofForensic Mental Health, University of Leicester, East Midlands Centre for Forensic MentalHealth, Arnold Lodge, Cordelia Close, Leicester, LE5 OLE, UK.
Substance misuse and violence 321
CBMH 8(4)2nd/JH copy 15/12/05 9:42 am Page 321


















