Prescription Drug Abuse And The Toxicology Of Medication Monitoring
description

Substance Substance Abuse/Toxicology Abuse/Toxicology
CMECME
December 5, 2007December 5, 2007
Samuel KimSamuel Kim
Lawren WellischLawren Wellisch

ObjectivesObjectives Review signs & symptoms of substance Review signs & symptoms of substance
abuse/overdoseabuse/overdose– Opioids, Sedative-Hypnotics, Anti-cholinergics, Opioids, Sedative-Hypnotics, Anti-cholinergics,
Sympathomimetics/Stimulants, Hallucinogens, Sympathomimetics/Stimulants, Hallucinogens, NSAIDsNSAIDs
Review RI protocols for Review RI protocols for poisoning/intoxication calls (general poisoning/intoxication calls (general standards of care)standards of care)
Discuss special concerns for common callsDiscuss special concerns for common calls– Alcohol intoxicationAlcohol intoxication– Drug useDrug use– Intentional overdose/suicide attemptIntentional overdose/suicide attempt

SIGNS & SYMPTOMSSIGNS & SYMPTOMS
OFOF
SUBSTANCE ABUSE / SUBSTANCE ABUSE / OVERDOSEOVERDOSE

OpioidsOpioids
Examples:Examples:– Rx painkillers Rx painkillers
(Demerol, Percocet, (Demerol, Percocet, Vicodin, Vicodin, Oxycodone, Oxycodone, Morphine, Codeine Morphine, Codeine etc.)etc.)
– HeroinHeroin– OpiumOpium
S/Sx:S/Sx:– HypoventilationHypoventilation– Pinpoint pupils Pinpoint pupils
(miosis)(miosis)– Sedation/ComaSedation/Coma– HypotensionHypotension

Sedative-HypnoticsSedative-Hypnotics
Examples:Examples:– Benzodiapenes Benzodiapenes
(Xanax, Valium, (Xanax, Valium, Rohypnol, Ativan Rohypnol, Ativan etc.)etc.)
– Barbituates Barbituates (phenobarbitol, (phenobarbitol, amobarbitol etc.)amobarbitol etc.)
– Alcohol*Alcohol*
S/Sx:S/Sx:– Slurred speechSlurred speech– Sedation/ComaSedation/Coma– HypoventilationHypoventilation– HypotensionHypotension
*-emesis*-emesis
-hematemesis-hematemesis

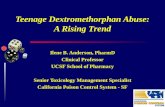
Extra information on AlcoholExtra information on AlcoholBeverage intake in 1 hr BAC (mg/dL) in 150lb man Behavioral Effects1 oz 100-proof spirits1 glass wine1 can beer2 oz 100-proof spirits2 glass wine2 can beer4 oz 100-proof spirits4 glass wine4 can beer6 oz 100-proof spirits6 glass wine6 can beer8 oz 100-proof spirits8 glass wine8 can beer10 oz 100-proof spirits10 glass wine10 can beer12 oz 100-proof spirits12 glass wine12 can beer14 oz 100-proof spirits14 glass wine14 can beer16 oz 100-proof spirits16 glass wine16 can beer24 oz 100-proof spirits24 glass wine24 can beer
Slow reaction time, impaired motor function, and less cautious; should not drive; may activate vomiting reflex
No noticeable effect
Lower alertness, impaired judgment, good feeling, less inhibition
Large increase in reaction times
Marked depression of sensory and motor abilities
Severe depression of sensory and motor abilities
Stuporous and unconscious of surroundings
Unconscious
Lethal dose in 50% of population
Lethal dose in 95% of population12
1/2
1
2
3
4
5
6
0.200
0.250
0.300
0.350
0.025
0.050
0.100
0.150
0.400
0.600
7
8
From Mosby’s Paramedic Textbook, Revised Third Edition, Table 36-5

Anti-cholinergicsAnti-cholinergics
Examples:Examples:– Diphenhydramine Diphenhydramine
(Benadryl)(Benadryl)
– Some Tricyclic Anti-Some Tricyclic Anti-depressants (Elavil, depressants (Elavil, Tofranil etc.)Tofranil etc.)
S/Sx:S/Sx:– TachycardiaTachycardia– HyperthermiaHyperthermia– HypertensionHypertension– Dilated pupils Dilated pupils
(mydriasis)(mydriasis)– Dry skin/ mucous Dry skin/ mucous
membranesmembranes– Sedation/Agitation/ Sedation/Agitation/
Seizures/Coma/DeliriumSeizures/Coma/Delirium– Decreased bowel Decreased bowel
soundssounds

Sympathomimetics / Sympathomimetics / StimulantsStimulants
Examples:Examples:– Amphetamines/ Amphetamines/
Methamphetamines Methamphetamines (“Meth”, Ecstacy, (“Meth”, Ecstacy, Speed, “uppers”)Speed, “uppers”)
– Cocaine/CrackCocaine/Crack
S/Sx:S/Sx:– HypertensionHypertension– TachycardiaTachycardia– Dilated pupils Dilated pupils
(mydriasis)(mydriasis)– Agitation/seizuresAgitation/seizures– HyperthermiaHyperthermia

HallucinogensHallucinogens Examples:Examples:
– LSD (“acid”)LSD (“acid”)– PCPPCP– Psilocybin (Mushrooms, Psilocybin (Mushrooms,
“shrooms”)“shrooms”)
– Marijuana*Marijuana*
S/Sx:S/Sx:– Similar to Similar to
sympathomimeticssympathomimetics Accompanied by Accompanied by
hallucinations, hallucinations, delusions, paranoiadelusions, paranoia
– *Usually produces *Usually produces euphoria, relaxation, euphoria, relaxation, drowsiness, short-term drowsiness, short-term memory impairment. memory impairment.
– Can progress to Can progress to depression/confusiondepression/confusion
– Anxiety and panic can Anxiety and panic can occur, especially in occur, especially in FIRST TIME USERS.FIRST TIME USERS.

NSAIDSNSAIDS Examples:Examples:
– Ibuprofen (Advil)Ibuprofen (Advil)– Acetaminophen (Tylenol)Acetaminophen (Tylenol)– Aspirin/ ASA*Aspirin/ ASA*
S/Sx:S/Sx:– Ibuprofen and Ibuprofen and
Acetaminophen are Acetaminophen are sometimes used for suicide sometimes used for suicide attempts, but extremely attempts, but extremely high doses are needed to high doses are needed to produce adverse affects.produce adverse affects.
Ibuprofen: >300mg/kg “to Ibuprofen: >300mg/kg “to produce mild effects”produce mild effects”
– 90 200mg pills in 60kg pt90 200mg pills in 60kg pt Acetaminophen: <140mg/kg Acetaminophen: <140mg/kg
“without serious effect.”“without serious effect.”– 25 325mg pills in 60kg pt25 325mg pills in 60kg pt– 17 500mg pills in 60kg pt17 500mg pills in 60kg pt
– *Aspirin overdose (acute or *Aspirin overdose (acute or chronic) can be lethalchronic) can be lethal
Nausea/vomitingNausea/vomiting HyperventilationHyperventilation ““ringing in the ears”ringing in the ears” Risk of seizuresRisk of seizures

ProtocolsProtocolsandand
General Standards of General Standards of CareCare

RI Protocol:RI Protocol:Poisoning and OverdosePoisoning and Overdose
If pt is unconscious or has impaired If pt is unconscious or has impaired consciousness, follow Impaired Consciousness consciousness, follow Impaired Consciousness protocolprotocol
Contact Poison Control (1-800-682-9211) or Contact Poison Control (1-800-682-9211) or Med ControlMed Control– Activated Charcoal (1gm/kg PO)Activated Charcoal (1gm/kg PO)– Syrup of Ipecac (adult: 30mL PO + 8oz Syrup of Ipecac (adult: 30mL PO + 8oz
water)water) (ped: 15mL PO + 8oz water) (ped: 15mL PO + 8oz water)
ALS: monitor, IVALS: monitor, IV TransportTransport Bring “clues”: medications, vials, needlesBring “clues”: medications, vials, needles DocumentDocument

RI Protocol:RI Protocol:Impaired ConsciousnessImpaired Consciousness
Rule out trauma (C-spine immobilization, Spineboard)Rule out trauma (C-spine immobilization, Spineboard) Initial assessment, ABCs; Left lateral position as indicatedInitial assessment, ABCs; Left lateral position as indicated Manage airway, respirations, (O2 as needed)Manage airway, respirations, (O2 as needed) Obtain history from family/bystanders (including medications)Obtain history from family/bystanders (including medications) Physical Exam (AVPU/GCS, vital signs, pupils, med-alert tags)Physical Exam (AVPU/GCS, vital signs, pupils, med-alert tags) Treat shock as indicatedTreat shock as indicated
ALS – monitor, IVALS – monitor, IV– bG<60mg/dLbG<60mg/dL
Thiamine (100mg IV)Thiamine (100mg IV) D50 (25gm IV) or Glucagon (1mg D50 (25gm IV) or Glucagon (1mg
IM/SQ)IM/SQ)– Narcan (2.0mg IV/IM/SQ)Narcan (2.0mg IV/IM/SQ)
BLSBLS–bG<60mg/dLbG<60mg/dLadminister administer Glucagon (1mg) Glucagon (1mg) IM/SQ)IM/SQ)
Transport, DocumentTransport, Document

Activated CharcoalActivated Charcoal
IndicationsIndications– Poisoning or Poisoning or
overdoseoverdose
DosageDosage– 1 gm/kg (0.5 gm/lb) 1 gm/kg (0.5 gm/lb)
POPO
ContraindicationsContraindications– Ingestion of:Ingestion of:
HydrocarbonHydrocarbon Petroleum distillatePetroleum distillate A caustic substanceA caustic substance
– Altered mental Altered mental statusstatus
– Inability to swallowInability to swallow

Naloxone (Narcan)Naloxone (Narcan)
IndicationsIndications– Suspected narcotic Suspected narcotic
overdoseoverdose
DosageDosage– 2.0 mg IV / IM / SQ, 2.0 mg IV / IM / SQ,
3 min intervals3 min intervalsoror
– 0.4 mg IV / IM / SQ, 0.4 mg IV / IM / SQ, 1 min intervals1 min intervals
– Total dose of 10 mgTotal dose of 10 mg
ContraindicationsContraindications– Do not use in Do not use in
meperidine (MPPP)-meperidine (MPPP)-induced seizuresinduced seizures
– Ped: 0.1 mg/kg IV / Ped: 0.1 mg/kg IV / IM / SQ,IM / SQ,3 min intervals3 min intervalsTotal dose of 10 mgTotal dose of 10 mg

Syrup of IpecacSyrup of Ipecac
IndicationsIndications
DosageDosage– >8 y.o., 30mL PO>8 y.o., 30mL PO
followed by 8oz followed by 8oz waterwater
– <8 y.o., 15 mL PO<8 y.o., 15 mL POfollowed by 4oz followed by 4oz waterwater
ContraindicationsContraindications– Has no gag reflexHas no gag reflex– Is actively seizing or Is actively seizing or
vomittingvomitting– Has ingested:Has ingested:
Sharp objectSharp object HydrocarbonHydrocarbon Petroleum distillatePetroleum distillate Caustic substance Caustic substance
(acid/alkali)(acid/alkali)

Sodium bicarbonate Sodium bicarbonate (NaHCO(NaHCO33))
IndicationsIndications– TCA overdoseTCA overdose– Contact Med Contact Med
Control!Control!
DosageDosage– 1 mEq/kg IV1 mEq/kg IV
ContraindicationsContraindications– HypocalcemiaHypocalcemia– HypokalemiaHypokalemia– HypernatremiaHypernatremia– Abd pain of Abd pain of
unknown originsunknown origins

GENERAL STANDARDS OF GENERAL STANDARDS OF CARECARE

ALWAYS! ALWAYS! HISTORYHISTORY
Baseline vitalsBaseline vitals RespirationsRespirations PulsePulse Skin (color, temperature, moisture)Skin (color, temperature, moisture) Capillary RefillCapillary Refill SpOSpO22
Blood pressureBlood pressure LOCLOC PupilsPupils Blood GlucoseBlood Glucose
– Deterioration can be rapid, make sure to keep Deterioration can be rapid, make sure to keep track of patients LOC and note times on run track of patients LOC and note times on run reportreport

ALWAYS!ALWAYS!HISTORYHISTORY
Five critical questions for substance Five critical questions for substance abuse/intoxication calls:abuse/intoxication calls:– What substance(s)What substance(s) did you take? did you take?– WhenWhen did you take it (become exposed did you take it (become exposed
to it)?to it)?– How muchHow much did you take? did you take?– What What actionsactions have been taken? have been taken?– How much do you How much do you weighweigh??
SAMPLESAMPLE

ALWAYS!ALWAYS!TREATMENTTREATMENT
Provide oxygenProvide oxygen– Try to use nasal cannula if patient is at Try to use nasal cannula if patient is at
risk for vomiting.risk for vomiting. Frequently ReassessFrequently Reassess
– Continual reassessment is especially Continual reassessment is especially critical for substance abuse/overdose critical for substance abuse/overdose calls. Be prepared to assist ventilations calls. Be prepared to assist ventilations etc.etc.

ALWAYS!ALWAYS! EMT HEALTH AND SAFETYEMT HEALTH AND SAFETY
Protect yourself!Protect yourself!– Patients can be dangerous if they are Patients can be dangerous if they are
becoming belligerent, do not want becoming belligerent, do not want treatment, or are suffering from treatment, or are suffering from delusions/paranoia. delusions/paranoia.
– If you feel threatened, protect yourself If you feel threatened, protect yourself first.first.Remember, Scene Safety.Remember, Scene Safety.
– Request DPS assistance if necessary.Request DPS assistance if necessary.

Avoid Tunnel VisionAvoid Tunnel Vision Keep in mind that there may be factors unrelated Keep in mind that there may be factors unrelated
to substance abuse contributing to the patient’s to substance abuse contributing to the patient’s S/Sx S/Sx – Examples:Examples:
TraumaTrauma underlying psychological conditionsunderlying psychological conditions diabetic/medical emergenciesdiabetic/medical emergencies
Never make assumptions, you may not know the Never make assumptions, you may not know the whole story (could your patient have been whole story (could your patient have been “slipped” something?)“slipped” something?)
Don’t neglect treating all aspects of the patient’s Don’t neglect treating all aspects of the patient’s conditioncondition
Consider the vulnerability of your patient if LOC Consider the vulnerability of your patient if LOC or A&O status is compromised.or A&O status is compromised.

Contacting poison controlContacting poison control
Telephone NumberTelephone Number– Med control can also contact Med control can also contact
poison control for you.poison control for you. When to callWhen to call
– Anytime you’re unfamiliar with Anytime you’re unfamiliar with the effects of the substance the effects of the substance ingested.ingested.

SPECIAL CONSIDERATIONSSPECIAL CONSIDERATIONSforfor
COMMON CALLSCOMMON CALLS

Alcohol/EtOH IntoxicationAlcohol/EtOH IntoxicationGUIDELINES FOR TRANSPORT TO UHSGUIDELINES FOR TRANSPORT TO UHS
Transport to UHS is not permitted if:Transport to UHS is not permitted if:– Patient has used any substance besides Patient has used any substance besides
alcoholalcohol– Patient is combative or unresponsivePatient is combative or unresponsive– Beds are unavailable in infirmaryBeds are unavailable in infirmary– Patient is not a Brown student Patient is not a Brown student
(MUST present a BROWN ID!!)(MUST present a BROWN ID!!) Transport decision is up to the Transport decision is up to the
supervisorsupervisor

Alcohol/EtOH IntoxicationAlcohol/EtOH IntoxicationGUIDELINES FOR REFUSALSGUIDELINES FOR REFUSALS
Must be A&Ox4/4Must be A&Ox4/4
If patient chooses the refusal route, If patient chooses the refusal route, Ensure there is someone to watch over the Ensure there is someone to watch over the
patientpatient Advise them to call EMS if condition Advise them to call EMS if condition
changes/worsenschanges/worsens

Illegal SubstancesIllegal SubstancesSHOULD YOU TELL??SHOULD YOU TELL??
Patient confidentiality – EMTs are not Patient confidentiality – EMTs are not permitted to reveal information from permitted to reveal information from their assessments to anyone other their assessments to anyone other than health care providers to whom than health care providers to whom that information is relevantthat information is relevant– Even if a law enforcement officer asks Even if a law enforcement officer asks
you if the patient admitted to using you if the patient admitted to using illegal substances!illegal substances!

Suicide AttemptsSuicide AttemptsASSESSMENTASSESSMENT
This is now a psych call as well as a This is now a psych call as well as a medical emergency. Treat it as such!medical emergency. Treat it as such!
Medical treatment will be the same as for Medical treatment will be the same as for other substance abuse/intoxication calls, other substance abuse/intoxication calls, but your assessment and bedside manner but your assessment and bedside manner may need to be altered for the sensitive may need to be altered for the sensitive nature of this type of call.nature of this type of call.– Consider: Consider:
Documenting patient appearance/behavior (Well-Documenting patient appearance/behavior (Well-groomed? Well-dressed? Cooperative? Combative?) groomed? Well-dressed? Cooperative? Combative?) Be clear on report and with other healthcare Be clear on report and with other healthcare providers why you are suspicious of a suicide providers why you are suspicious of a suicide attempt.attempt.
Contacting Psychological ServicesContacting Psychological Services

Suicide AttemptsSuicide AttemptsREFUSALSREFUSALS
Best to persuade patient to accept Best to persuade patient to accept treatment and transporttreatment and transport– Whether or not they specifically state suicidal Whether or not they specifically state suicidal
intentionsintentions Otherwise, police can employ Protective Otherwise, police can employ Protective
Custody (PC)Custody (PC)– ““Last resort” – Is disempowering to the patient Last resort” – Is disempowering to the patient
and can exacerbate the situationand can exacerbate the situation– May be the only option if substances are May be the only option if substances are
involved and reasoning is ineffectiveinvolved and reasoning is ineffective