Subdural empyema: Areview casesfalx and the left falcine subdural space irrigated with penicillin...
13
J. Neurol. Neurosurg. Psychiat., 1964, 27, 422 Subdural empyema: A review of 29 cases EDWARD HITCHCOCK1 AND ALEXANDER ANDREADIS2 From the Department of Neurological Surgery, Radcliffe Infirmary, Oxford In 1948, Schiller, Cairns, and Russell presented 33 cases of subdural empyema arising over 20 years most of which were treated in this department. Their paper dealt with the results of penicillin instillations into the subdural space and marked a major thera- peutic advance in the treatment of this condition. We felt it would be of interest to review 29 subsequent cases and to note the present-day problems in their management. The history of the recognition of this condition has been outlined in detail by Kubik and Adams (1943) and by Courville (1944), and there is little to add to their accounts. Schiller et al. (1948) used the term 'purulent pachy meningitis interna' because of a supposed resem- blance to peritonitis. 'Subdural abscess' is often used, but should only be applied when there is loculation and a membrane is formed. Subdural empyema is a better term, indicating pus in a pre-formed space. AETIOLOGY Stern and Boldrey (1952) listed 10 aetiological condi- tions for the production of this condition, but the commonest cause of subdural empyema is otorrhino- logical disease. In our series of 29 cases 26 arose as complications of ear or nose infections whilst Schiller et al. (1948) reported 29 such cases out of a total of 33. Much less commonly it follows the rupture of an intracerebral abscess, and rarely it is secondary to penetrating wounds of the skull and cranial osteo- myelitis from other causes. Other less common causes are leptomeningitis and bacteraemia, or infection of subdural haematoma (Stern and Boldrey, 1952). Of the three 'miscellaneous' cases in our series one fol- lowed ventriculography, one was presumably an infected subdural haematoma in a child, and the remaining patient developed a pre-pontine subdural empyema secondary to osteomyelitis of the skull base. Early reports of subdural infection usually referred to otitic disease as the cause but from the late 1930s 'Present address: The Royal Infirmary, Manchester. 2Present address: Polyclinic of Athens, 3 Piraeus Street, Athens, Greece. sinus infection became increasingly responsible, and today sinus infection far exceeds otitic as the cause of subdural empyema. Thus in our series 20 cases were 'paranasal' and six 'otitic' whereas Schiller et al. (1948) had 23 cases following sinus disease and six cases from mastoid infection. The reason is not im- mediately apparent. Probably many patients suffered in the past from undiagnosed sinus infection. Stern and Boldrey (1952) and others have noted a relative increase in the incidence of subdural empyema as compared to brain abscess. Schiller et al. (1948) reported 33 cases of subdural empyema in 20 years. Since then in this department we have had 31 cases (two are excluded from this series be- cause of insufficient information) in the 14 years from 1949 to 1962 and the number of cases of brain abscess admitted during this time was 115. Un- fortunately we are unable to quote comparable numbers of abscesses for the 20 years covered in the paper of Schiller et al. (1948) as some of their cases of subdural empyema were treated elsewhere. How- ever, by dividing the last 14 years into two equal periods some conclusions can be drawn. There were 69 cases of brain abscess and 14 of subdural empyema during the years 1949 to 1955 and 46 of brain abscess and 17 of subdural empyema during the second seven- year period. Although the numbers are small they appear to support the observation of Stern and Boldrey (1952). Table I outlines the cases of this series grouped under age, sex, and primary focus of infection. There is a preponderance of males over females, 23 to six, and this has been noted by many authors, although no explanation can be given. It cannot be related to the larger size of the paranasal sinuses in men, since the condition is common in children when the sinuses are hardly formed, and neither does it appear to bear any relation to occupation. The age ranged from 8 months to 67 years, but the overall peak age lay between 10 and 20 years. In otitic disease, however the peak lay in the age group 40 to 60 years. The incidence of acute or chronic disease was different for paranasal or otitic infections (see Table I). In the 'paranasal' group 17 patients had acute in- fections without a history of chronic sinusitis and only three patients had chronic infections. Con- 422 Protected by copyright. on February 4, 2021 by guest. http://jnnp.bmj.com/ J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. Downloaded from
Transcript of Subdural empyema: Areview casesfalx and the left falcine subdural space irrigated with penicillin...

J. Neurol. Neurosurg. Psychiat., 1964, 27, 422
Subdural empyema: A review of 29 cases
EDWARD HITCHCOCK1 AND ALEXANDER ANDREADIS2
From the Department of Neurological Surgery, Radcliffe Infirmary, Oxford
In 1948, Schiller, Cairns, and Russell presented 33cases of subdural empyema arising over 20 yearsmost of which were treated in this department. Theirpaper dealt with the results of penicillin instillationsinto the subdural space and marked a major thera-peutic advance in the treatment of this condition. Wefelt it would be of interest to review 29 subsequentcases and to note the present-day problems in theirmanagement.The history of the recognition of this condition
has been outlined in detail by Kubik and Adams(1943) and by Courville (1944), and there is little toadd to their accounts.
Schiller et al. (1948) used the term 'purulent pachymeningitis interna' because of a supposed resem-blance to peritonitis. 'Subdural abscess' is often used,but should only be applied when there is loculationand a membrane is formed. Subdural empyema is abetter term, indicating pus in a pre-formed space.
AETIOLOGY
Stern and Boldrey (1952) listed 10 aetiological condi-tions for the production of this condition, but thecommonest cause of subdural empyema is otorrhino-logical disease. In our series of 29 cases 26 arose ascomplications ofear or nose infections whilst Schilleret al. (1948) reported 29 such cases out of a total of33.Much less commonly it follows the rupture of an
intracerebral abscess, and rarely it is secondary topenetrating wounds of the skull and cranial osteo-myelitis from other causes. Other less common causesare leptomeningitis and bacteraemia, or infection ofsubdural haematoma (Stern and Boldrey, 1952). Ofthe three 'miscellaneous' cases in our series one fol-lowed ventriculography, one was presumably aninfected subdural haematoma in a child, and theremaining patient developed a pre-pontine subduralempyema secondary to osteomyelitis of the skullbase.Early reports of subdural infection usually referred
to otitic disease as the cause but from the late 1930s
'Present address: The Royal Infirmary, Manchester.2Present address: Polyclinic of Athens, 3 Piraeus Street, Athens,Greece.
sinus infection became increasingly responsible, andtoday sinus infection far exceeds otitic as the cause ofsubdural empyema. Thus in our series 20 cases were'paranasal' and six 'otitic' whereas Schiller et al.(1948) had 23 cases following sinus disease and sixcases from mastoid infection. The reason is not im-mediately apparent. Probably many patients sufferedin the past from undiagnosed sinus infection.
Stern and Boldrey (1952) and others have noted arelative increase in the incidence of subduralempyema as compared to brain abscess. Schilleret al. (1948) reported 33 cases of subdural empyemain 20 years. Since then in this department we havehad 31 cases (two are excluded from this series be-cause of insufficient information) in the 14 years from1949 to 1962 and the number of cases of brainabscess admitted during this time was 115. Un-fortunately we are unable to quote comparablenumbers of abscesses for the 20 years covered in thepaper of Schiller et al. (1948) as some of their casesof subdural empyema were treated elsewhere. How-ever, by dividing the last 14 years into two equalperiods some conclusions can be drawn. There were69 cases ofbrain abscess and 14 ofsubdural empyemaduring the years 1949 to 1955 and 46 of brain abscessand 17 ofsubdural empyema during the second seven-year period. Although the numbers are small theyappear to support the observation of Stern andBoldrey (1952).
Table I outlines the cases of this series groupedunder age, sex, and primary focus of infection. Thereis a preponderance of males over females, 23 to six,and this has been noted by many authors, althoughno explanation can be given. It cannot be related tothe larger size of the paranasal sinuses in men, sincethe condition is common in children when the sinusesare hardly formed, and neither does it appear tobear any relation to occupation. The age ranged from8 months to 67 years, but the overall peak age laybetween 10 and 20 years. In otitic disease, howeverthe peak lay in the age group 40 to 60 years.The incidence of acute or chronic disease was
different for paranasal or otitic infections (seeTable I).In the 'paranasal' group 17 patients had acute in-fections without a history of chronic sinusitis andonly three patients had chronic infections. Con-
422
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Subdural empyema: A review of 29 cases
TABLE I 2 Indirect extension is more common in paranasalAGE, SEX, AND ORIGIN OF THE 29 CASES sinus disease. According to Courville (1944) the
Age (years) mode of spread is by progressive thrombophlebitis of0-10 10-20 20-40 40-60 60+ Total the mucosal veins and subsequent spread to dural
Male 3 8 6 4 2 23 veins, venous sinuses, and cerebral veins. OrbitalFemale 0 3 0 2 1 6 oedema indicates extension of thrombophlebitisTotal 3 11 6 6 3 29 along the veins of the orbit and it is frequently found.Died 1 4 0 3 2 10 Indeed, Stevens and Welch (1956) reported retinalParanasal thrombophlebitis in one case. The infection may limitChronic acute 0 0 3 0 0 3 .maAcute 2 10 3 2 0 17 itself to the subdural space, or to the brain, producingTotal 2 10 6 2 0 20 either a subdural empyema or an intracerebralDied 0 3 0 1 0 4 abscess following cortical thrombophlebitis. Not in-Chronic acute 0 1 0 2 2 5 frequently subdural empyema and intracerebralAcute 0 0 0 1 0 1 abscess may thus arise simultaneously.Total 0 1 0 1 2 6 Entering the subdural space the infection elicits a
Others prompt inflammatory reaction with exudate. Pus isTotal 1 0 0 1 1 3 rapidly formed and membrane formation, althoughDied 1 0 0 1 1 3 it does occur, is not marked in the early stages.
Wood (1952) stated that antibiotics may allow timeversely with the 'otitic' group only one patient had for membrane and granulation tissue to form but inacute otitis, the remaining five presenting with our series it was encountered only twice at the firstacute exacerbations of chronic ear infections. The operation.numbers in the otitic group were small, but these The extension of pus depends on the primary sitefindings may be related to the different modes of of infection and the anatomical peculiarities of thespread of infection. subdural space. Collections beneath the hemispheres
Seven patients had had operations on the ears or are uncommon and thin, and dorso-lateral and inter-nose before admission to this department. In five of hemispherical (Figs. 1 and 2) collections commonthem signs of subdural involvement were already (Courville, 1944). Because these desperately illpresent. It seems very unlikely, therefore, that such patients lie recumbent gravity aids spread posteriorly.procedures cause subdural infection. From the study of our cases, both at operation and
necropsy, the extension of pus from the variousprimary sites appeared to follow fairly well-defined
PATHOLOGY paths.
Since the brain and membranes fill the cranium com-pletely the subdural space is a potential space. Thedorso-lateral part, however, together with the inter-hemispherical fissure, is relatively free, imposing noobstruction to the formation and flow of fluid(Schiller et al., 1948). The 'basal' subdural space ispractically non-existent, and fluid accumulations atthis site are therefore uncommon and small (Cour-ville, 1944).
Infection may enter the subdural space by tworoutes:1 Direct extension by erosion of osteitic areas of thebony wall and of the dura separating the purulentfocus from the subdural space: according to Cour-ville (1944) this is uncommon in paranasal sinus in-fections. In otitic infections, however, this routeseems more common; in our six cases four had duralinvolvement observed either at necropsy (two cases)or at operation (two cases). In the remaining twocases the information was inadequate. This observa-tion may account for the preponderance of chronicinfections in the otitic group.
PARANASAL SUPPURATION Since the portal of entryis usually through communicating veins, subduralcollections usually form at the frontal poles in rela-tion to the affected sinus. In the fronto-polar routethe pus extends posteriorly over the convexity of thefrontal lobe. This occurred in 19 of our 20 'para-nasal' cases. The spread was diffuse with a tendencyto form the major collection over the dorso-lateralaspect of the hemisphere (Fig. 3). Its posterior limitwas variable. In five patients the collection waslimited to the frontal lobe, in 10 patients it hadreached the mid-parietal region, and in the remain-ing four it extended to the parieto-occipital area.None appeared to have reached the convexity of theoccipital pole. Pus extended along the Sylvian fissurein eight patients. In four patients pus was foundalongside the falx, presumably having seeped be-tween the superior cerebral veins and pacchioniangranulations.The parafalcine route may allow the spread of the
pus either posteriorly or beneath the free edge of thefalx to the opposite hemisphere. The latter occurred
423
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Edward Hitchcock and Alexander Andreadis
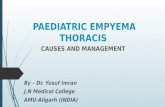
FIG. 1. Coronal section ofthe brain from a case ofsubdural empyema show-ing pUis over the dorso-lateral aspect of the hemisphere.
FIG. 3. The brain from a case of subdural empyeshowing the extent of the collection of pus overdorso-lateral aspect of the hemisphere.
V 0SA i ,+ffi i L.... :
FIG. 2. Coronal section of the brain from a case of subdural empyema showingcollection ofpus on the medial surface of the brain alongside the falx.
424
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Subdural empyema: A review of29 cases
in three of the four patients with secondary falcinecollections and these three patients are the only'paranasal' cases with bilateral subdural empyema.Primary falcine collection occurred once only.
Subfrontal collections were found in three patients,in one at operation and in the remaining two atnecropsy.
OTITIC SUPPURATION Intracerebral abscess is muchcommoner than subdural empyema in this condition.When a subdural collection does form, however, ittends to pass posteriorly and medially over thetentorium towards the falx, and extend along theroutes already outlined. In its course pus may seepover the edge of the tent into the posterior fossa andthen a cerebellar subdural empyema results. Morecommonly, however, the pus remains above thetentorium. Its progress along the falx is impeded bygravity and it rarely extends far anteriorly. Directextension over the lateral aspect of the temporallobe is less common. Three of our six otitic cases hadclear evidence of pus along the falx and/or theoccipital poles, and in these no pus was found overthe temporal lobe. In another two cases pus wasdistributed over the major part of the convexity, butin one case the presence of a falcine collection couldnot be excluded. In the remaining case the pus wasconfined to the posterior fossa obviously throughdirect spread of the infection from the petrous bone.To sum up, there are three common sites for pus to
collect in subdural empyema, namely, the frontalpoles extending on to the fronto-parietal regions,the para-falcine spaces, and the occipital poles. Thisinformation is essential to the correct placing ofburr holes, and collections at these sites deserve con-sideration as causes of relapse.The following summary illustrates the spread of
pus along the falx and in this case into the posteriorfossa. It also emphasizes that intracerebral abscess orintracerebellar abscess should be considered inpatients failing to improve or relapsing.
CASE 1 B.P. (R.I. 104616). a 13-year-old boy, sufferedfrom bilateral chronic otitis media and had had a rightradical mastoidectomy five years earlier. He was admittedwith a one-month history of vertigo and increasinglysevere headache following an upper respiratory tractinfection. The discharge from the left ear became profuseand finally he was admitted to another hospital on 18April, 1949 with signs of meningitis. His cerebrospinalfluid contained 1,800 cells per c.mm., mostly polymorphs,and he was treated with intramuscular penicillin, one doseof intrathecal penicillin, and oral sulphadiazine. Withintwo days the cerebrospinal fluid had improved, but hisgeneral condition had deteriorated and he became coma-tose with a right hemiparesis. A left radical mastoidect-omy was performed immediately and revealed a large
extradural abscess and granulations over the middlefossa dura. The following day, 21 April, he had a com-plete right hemiplegia with right-sided convulsions andremained comatose. The left temporal lobe was exploredthrough the mastoidectomy wound but no abscess found.He gradually improved, however, over the next two weeksbut on 5 May was drowsy with a pyrexia of 103°F. andwas transferred to this department. Here he was foundto be very drowsy with mild bilateral papilloedema and aright hemiparesis. A diagnosis of left temporal lobeabscess was made and a left temporal burr hole was madeimmediately. Needling of the temporal lobe revealed noabscess but a left frontal burr hole allowed the evacuationof about 20 ml. of thick subdural pus from the medial sideof the hemisphere. A catheter was inserted 5 cm. along thefalx directed posteriorly for penicillin instillations. Duringthe operation there was a dramatic improvement andwithin 24 hours he was eating and sitting up in bed.Regular instillations of penicillin down the tube had beencontinued as well as intramuscular penicillin and oralsulphadiazine. Two days after the first operation, however,(7 May) the level of consciousness deteriorated and afurther operation was performed to exclude a posteriorloculation. A left occipital burr hole, later enlarged,demonstrated about 20 ml. of thick pus along the medialside of the hemisphere. A catheter was inserted along thefalx and the left falcine subdural space irrigated withpenicillin between the frontal and occipital catheters.Again there was a dramatic improvement. On 10 May,the initial subdural pus was reported as growing proteusorganisms and streptomycin was now administered, bothsubdurally and systemically. About this time he wasnoted to have attacks of titubation and left-sideoi tremor,a.nd the following day (11 May) respiration suddenlyceased and he died.
Necropsy revealed a left frontal lobe convexity subduralempyema and a large abscess in the left para-falcinesubdural space extending from the frontal to the occipitalpole. There was an extensive subdural empyema over thesuperior surface of the cerebellum and a large left cere-bellar abscess associated with a dural slough overlyingan osteitis of the left petrous bone.
BACTERIOLOGY
The commonest organism isolated was streptococcus,in half of the cases in its anaerobic form. Otherorganisms (Staphylococcus and Gram-negative bacillisuch as Clostridium and especially Proteus) also oc-curred. Table II shows the numbers actually grown.In two patients no bacteriology was done and inanother four no growth was obtained, although intwo of these four patients Gram-positive cocci wereseen on films.
Schiller et al. (1948) had positive cultures in 27patients and in 24 of these streptococci, presumablysensitive to penicillin, were grown. Even supposingthat in the remaining three cases the organisms werepenicillin-resistant, comparison with our figuresshows that penicillin-resistant organisms are in-
425
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Edward Hitchcock and Alexander Andreadis
TABLE IIORGANISMS IN SUBDURAL EMPYEMA
Organisms on Culture Number of Penicillin- Penicillin-Patients sensitive resistant
Streptococcus 9Streptococcus andStaph. aureus 1Streptococcus andCl. welchii 1Streptococcus, B. coli,and proteus 1Staphylococcus aureus 3Staph. aureus and proteus 1Staph. aureus and B. coli 1Proteus 2B. anitratum 1Micrococci anddiphtheroids 3Totals 23
9
3
2
pus, and certainly if it were not, we could not expectany of the complete recoveries from subdural
Sensitivity empyema that now commonly occur. The barrier isUnkown penetrated at many points, especially at the vertex,
by cerebral veins as they enter the dural sinuses. In-fection may enter the cortex by an extending throm-bophlebitis and result in localized cortical or sub-cortical inflammation. Five cases had intracerebralabscess. Characteristically, many of these were mul-tiple and small, but tended to coalesce and form onelarge single cavity often of considerable extent.
CLINICAL FEATURES
2411
creasingly grown in these infections. This is particu-larly evident in the 'otitic' group where four of oursix patients had proteus.
ASSOCIATED LESIONS
Their relative frequency appears to vary fromauthor to author. Swelling of the scalp was grosslyevident in four of our cases, and was then associatedwith osteomyelitis or extradural abscess as in Potts'puffy tumour'. In two cases there was frank cellulitiswith brawny induration and fluctuation due to sub-galeal pus. In one case where a scalp flap was raisedthe galea and pericranium were necrotic with pusoozing through in many places. Neither of these caseshad peri-orbital oedema, and this supported Cour-ville's view that the lesions are concomitant ratherthan consecutive.
Whilst some authors have found osteomyelitis orextradural abscess in all their cases, others have not.Courville (1944) regarded them as uncommon ac-companiments of subdural empyema, and converselystated that in cases of osteomyelitis of the skull sub-dural suppuration is uncommon. In our series,frank osteomyelitis occurred in 10 (50%) of the para-nasal cases and in three (50 %) of the otitic. The bonein these cases of acute infection was still firm, al-though pus would often well into the burr holes fromthe diploe.
Lepto-meningeal reactions, as judged by pleo-cytosis in the cerebrospinal fluid, were relativelycommon in our experience. Eight of the nine casescoming to necropsy had fibrinous exudate in thesubarachnoid space under the subdural empyema orsmall subarachnoidal purulent collections.
It is perhaps remarkable that the cortex escapesdirect invasion for so long, separated as it is fromlarge collections of subdural pus by the thin layer ofcells forming the arachnoid. This tenuous membraneis known to be relatively impermeable to toxins and
The clinical presentation of this condition is variable,but certain general features are common. The tem-perature rises and there is severe generalized head-ache. Vomiting is common. The patient gradually orrapidly becomes irritable and drowsy, but thesechanges are often insidious and to the inexperiencedappear only as a vague generalized deteriorationfrequently attributed to the primary infection, as atthis stage there may be little in the way of focalneurological abnormalities. Meningism is commonand indeed the cerebrospinal fluid may contain a highconcentration of protein and moderate pleocytosis.In the early stages the cerebrospinal fluid is some-times normal, however, and such a finding may en-courage the view that the central nervous system isunaffected. This period of invasion usually extendsfrom 24 to 36 hours. Less commonly the disease isfulminating in character and symptoms of invasionof the subdural space quickly follow symptoms of theprimary infection. These cases are clearly those ofoverwhelming infections and the history may be asshort as six or seven hours.
Finally, focal disturbances appear. In dominanthemisphere collections, dysphasia is a frequent earlysymptom, often appearing as a reluctance to talk andregarded by the inexperienced as an expected ac-companiment to the headache and systemic infec-tion. Minimal weakness of one or more limbs pro-gresses insidiously or rapidly to complete paralysis.In some cases this is, preceded by focal or generalepileptic seizures. Papilloedema may be noted. It isusually not until this stage is reached that the diag-nosis is considered and rarely is there any delay intransferring patients to a neurosurgical unit for assess-ment although almost invariably with a diagnosis ofintracerebral abscess. By now, the patient is stupor-ous or frankly comatose and if transfer is delayed thecondition progresses to a moribund state with de-cerebrate rigidity. The time taken by the infectionto manifest itself eloquently by the occurrence offocal fits, hemiplegia, aphasia, stupor, and so forthis variable. It may be as short as a few hours or as
426
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Subdural empyema: A review of29 cases
long as 11 days from the stage of invasion, as in oneof our patients.Table III presents the relative frequency of symp-
toms and signs in our cases. It should be noted thatheadache, present in 100% in the early stages, is re-duced to 75% in the established stage and this ap-parent improvement is really a reflection of thedeterioration of consciousness. It should also benoted that the relative frequency of symptoms in theparanasal group closely parallels that in the otiticcases. Patients with pus on the convexity of the brainusually present with contralateral hemiplegia, oftenwith focal seizures of face, arm, and leg. Sensory dis-turbances are less common, whilst in collections overthe dominant hemisphere aphasia is usual. Thesingle primary falcine collection in our series pre-sented with a lower limb monoplegia which rapidlyprogressed up the trunk to involve the arm, butcharacteristically spared the face. It differs in no wayfrom secondary falcine collections.
TABLE IIIINCIDENCE OF DIFFERENT SYMPTOMS AND SIGNS
Paranasal (20 cases) Otitic (6 cases)Symptoms and Signs At Onset Established At Onset Established
Evidence of systemicinfection 19Paralysis (usually hemi-plegia) 13Stiff neck and Kernigism 12Disturbed consciousness 13Headache 20High intracranial pressure 8Mental changes 10Vomiting 10Epilepsy 7Visual field defects ISensory changes 5Aphasia (in left hemi-sphere involvement)
20 (100%) 5 6 (100%)
20 (100%)18 (90%)16 (80%)15 (75%)15 (75%)12 (60%)10 (50%)9 (45%)9 (45%)8 (40%)
100%
4 6 (100%)5 6 (100%)5 6 (100%)4 4 (66%)2 3 (50%)3 4 (66%)4 4 (66%)2 3 (50%)2 3 (50%)1 4 (66%)
It has been stated (Schiller et al., 1948) that ade-quate treatment with penicillin may modify theclinical picture. Unfortunately information about theantibiotics given for the primary infection before ad-mission to this department was not adquate enoughto permit analysis. In the few cases where informationwas available the antibiotics did not appear to in-fluence either the time of onset of the subduralempyema or its subsequent course. In only two caseswas there transient relief of early symptoms with sub-sequent relapse. Furthermore the clinical picture asdescribed by Schiller et al. (1948) differs in no wayfrom that in our series.
SPECIAL INVESTIGATIONS
Although the diagnosis may often be made onclinical grounds, special investigations are often
needed to establish it definitely. Because of this acritical examination has been made of the variousspecial investigations used in the diagnosis of thecondition.
Table IV represents the findings for cerebrospinalfluid in cases where this investigation was performed(the three untreated cases have been excluded).High protein concentrations and pleocytosis arecommon but eight cases (35 %) presented with nearlynormal cerebrospinal fluid and with only slightpleocytosis or raised protein level. One case at theonset presented with a relatively low protein and alymphocytic pleocytosis. As a result of surgicaltreatment there was in most cases a rapid fall in thecell count and usually in the protein content althoughthe latter sometimes rose despite clinical improve-ment. In one case only were organisms found in thecerebrospinal fluid, illustrating the rarity of frankmeningitis.
TABLE IVCEREBROSPINAL FLUID
At onset (5 cases) Abnormal cerebrospinal fluid 5Cells 420-3,760 (90% polymorphs)l 4Protein 110-200 }Cells (100 lymphocytes) 1Protein 70 f
Established (23 cases) Abnormal cerebrospinal fluid 15(1 case with organisms: sterile culture)Cells 35-4,880 15Polymorphs 90%, protein 30-560 10Lymphocytes 90%, protein 35-114 3Unknown 2Normal cerebrospinal fluid 6Slightly abnormal cerebrospinal fluid 2
Post-operative (21 cases) Rapid fall in cell count within five days 19Increased cell count 2Protein variable (often increased)
Ce1lls are given in number per c.mm. and protein in mg. per 100 ml.
A plain skull radiograph may yield valuable in-formation. In the 'paranasal' group 19 out of 20cases had plain skull radiographs taken, and 18 ofthese showed opacity of the frontal and ethmoidalsinuses, often as part of a pansinusitis, which was,however, always predominantly unilateral and on thesame side as the intracranial collection. Three casesshowed evidence of early osteomyelitis of the sinuswall. Two 5-year-olds had well-marked suturediastasis, and in one other case there was a pinealshift. Only one case out of the 19 had a completelynormal skull radiograph. All six otitic cases had skullradiographs taken and all showed evidence ofmastoid disease on the appropriate side, manifest byloss of cellularity, sclerosis, or erosion. One casedemonstrated a well-marked pineal shift. Only twoofthe three miscellaneous cases had skull radiographstaken; in an 8-month-old child with pus on the con-vexity there was progressive increase in skull size-with suture diastasis, and in the remaining case
427
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Edward Hitchcock and Alexander Andreadis
retrospective examination of the radiographs re-vealed osteomyelitis of the dorsum sellae. While itmust be acknowledged that many of these changes arenot-specific, it is noteworthy that evidence of sinus ormastoid disease was present in the vast majority ofcases and always this was most marked on the sameside as the intracranial collection.
Eighteen cases had electroencephalographic re-cordings pre-operatively, post-operatively, or both.Ten cases had pre-operative E.E.G.s, and here theusual findings were lateralized, frequently focal, slowwaves and sometimes suppression of activity over theaffected area. The focal slow waves often encouragedthe diagnosis of intracerebral abscess. In eight out ofthe 10 cases the localization was fairly accurate andabnormalities were found on the involved side but inone a contralateral collection was missed. In theother two the localization was grossly inaccurate.Eleven cases had post-operative electroencephalo-grams. Suppression of activity and slow waves, oftenwith large delta foci, were again frequent findings.In four cases the E.E.G. showed abnormalities in theregion where pus was extending and these wererecordings during a relapse. Once again, intra-cerebral abscess was usually diagnosed, but thelocalization was fairly accurate. Seven cases showedan improving post-operative record with return tonormal rhythm and areas previously silent showingrecovery of activity. Pre-operatively, therefore, elec-troencephalography was not of great value indiagnosis; it did, however, reveal abnormality andserved to give some rough localization. Post-operat-ively it was rather more useful, serving to indicateprogression of the lesion or improvement.
Carotid angiography was performed on 17patients, in some cases more than once. Thirteenpatients had the investigation pre-operatively and innine it showed evidence ofan extracerebral collection.In two cases angiography failed to demonstrate anexisting subdural empyema; the presence of a frontalintracerebral abscess in one of these may have ob-scured the issue. In the remaining two cases thesubdural collection was situated in the posteriorfossa and in one of these the angiogram showedhydrocephalic stretching of the pericaleosal artery.Nine post-operative angiograms were performed andseven out of these suggested the presence of a newcollection. In two cases this was confirmed by sub-sequent operation and evacuation. The remainingfive cases had no exploration despite which clinicalimprovement occurred. In most of these the site ofthe presumed collection was alongside the falx. Inanother case an air encephalogram gave evidence ofasimilar space-occupying lesion but this was not con-firmed by angiography nor by subsequent operation.The value of angiography is best illustrated by the
following case which also demonstrates the problemsof management.
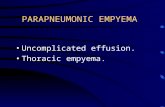
CASE 2 F.M. (R.I. 308845), a 39-year-old clerk with ahistory of chronic sinus infection, developed increasingheadache, vomiting, delirium, and dysphasia some threeweeks after recovery from a bad cold and 48 hours beforeadmission. An emergency operation to drain pus fromthe frontal sinus was performed elsewhere, but the follow-ings day, because of the dysphasia and a mild right hemi-paresis, he was transferred to this Unit as a case of sus-pected frontal abscess. The cerebrospinal fluid contained132 cells per c.mm., mainly lymphocytes, and 56 mg. ofprotein per 100 ml. On admission on 1 June 1961 he wasalert but aphasic with a total right flaccid hemiplegia. Aleft carotid angiogram confirmed the diagnosis of a left-sided subdural collection (Fig. 4a). A retrospectiveexamination of the angiograms suggested absent orpoor filling of the frontal veins. At operation the sameday, a right frontal burr hole revealed no pus, but overthe whole left fronto-temporal and anterior parietalregions abundant thick creamy-yellow pus was found.Catheters were inserted for penicillin instillation. Post-operatively, he developed frequent right focal fits, butwith general and local administration of penicillin heimproved over the next few weeks to almost completerecovery. Then over three or four days he relapsed in-sidiously with general malaise, drowsiness, and finallywith a paraparesis most marked in the left leg. Bilateralcarotid angiograms (19 June) revealed evidence of aparasagittal collection (Fig. 4b), and bilateral burr holesrevealed subdural pus again on the left, but only a fewflecks on the right. More catheters were inserted andsystemic and local antibiotic treatment continued. Hefailed to regain consciousness after this operation, whichwas under general anaesthesia, and required a trache-ostomy. For several days he remiined comatose, withchest infection and continuous left focal fits. On 23 June,because of his failure to improve, new burr holes weremade revealing a small right-sided subdural haematomaand further left frontal pus. His condition still remaineddesperate, however, and one week later (1 July) newbilateral carotid angiograms demonstrated a further rightsubdural collection and more right-sided burr holes weremade. An extensive subdural abscess was found at thesite of the former haematoma, which was becoming en-capsulated. Further catheters were inserted and intensivepenicillin administration was continued, and within a fewhours of operation he showed a striking improvement.He then made a slow recovery from the coma and doublehemiplegia. He spoke for the first time since the initialrelapse on 17 July, by which time the fits had stopped.Finally, two months after admission, all antibiotic treat-ment was stopped. He continued to improve over the nexttwo months and was transferred to the NeurologicalDepartment at Stoke Mandeville Hospital for rehabilita-tion. After a few weeks he was mobilized and was dis-charged home. His improvement continued and at thetime of his last attendance in September 1962 he was ableto look after himself and to perform his previous occupa-tion of a clerk. He still had focal fits which were becomingless frequent.
428
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Subdural empyema: A review of 29 cases
FIG. 4a
FIG. 4. Case 2. (a) Left carotid angiogramshowing displacement of the middle cerebralvessels away from the inner table of the skullin the antero-posterior view. The lateral view ofthe phlebogram of the same examination showspoor filling of the frontal veins.(b) Left carotid angiogram showing displace-ment of the posterior branches of both peri-callosal arteries away from the midline.
FIG. 4b
In our series air encephalograms were rarelyperformed before operation and only when thediagnosis of subdural empyema was unsuspected.Three cases had pre-operative air studies; one re-vealed hydrocephalus and two demonstrated dis-placement of the fourth ventricle (in pre-pontineand posterior fossa purulent collections). Seven caseshad air studies performed because of relapse, and allrevealed ventricular distortion. Five showed evidenceof a parafalcine space-occupying lesion but only twowere explored and in these pus was found. In onepatient air encephalography suggested the presenceof a frontal mass which was subsequently shown to bean intracerebral abscess. In a further case air ence-phalography merely demonstrated hydrocephalus.
Twelve patients had air studies performed beforetheir discharge in order to exclude any further lesion.Seven of these revealed slight abnormalities such asventricular dilatation, slight ventricular shift and onthe involved side a loss of subarachnoid air (Fig.5b), presumably because of closure of the subarach-noid space by exudate. This block in the cerebro-spinal fluid pathway may account for the commonfinding of developing papilloedema in cases other-wise improving. In one patient evidence of frontalabscess, previously demonstrated during a period ofrelapse, was again found but this time markedly in-creased in size and subsequently this abscess wasremoved. Two patients were perfectly normal.
Angiography, in our opinion, is the most useful
429
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

4EdwardHitchcock and Alexander Andreadis
special investigation. Its chief value lies in confirmingthe diagnosis and revealing sites of pus clinically un-suspected and in this it had a high rate of success. Italso helps to exclude or demonstrate the presence ofan associated intracerebral abscess. In the caseswhere it failed special views, such as anteriorobliques, might well have revealed the collections.However, a negative angiogram does not exclude thepresence of a subdural empyema.
If all these special studies are negative the diseaseonce suspected must be excluded by burr holeexploration.Some patients are dangerously ill on admission
and operation is performed immediately as no delayis permissible. In these cases the finding of pus onthe convexity ofthe brain may satisfy the surgeon, butfurther collections or associated lesions, such as intra-cerebral abscess, must be excluded and as soon as thepatient's condition permits an angiogram should beperformed.
TREATMENT
In this series treatment consisted in making burr holessited over the suspected area of involvement, butattempts to get to the limits of the collection wererarely made. The pus was removed by depressing thebrain, and occasionally the space was irrigated withpenicillin. The subdural collection was rarely verylarge; it was impossible to make accurate measure-ments but the amount rarely exceeded 20 ml. Rubbercatheters were then inserted, sometimes two or threeinto each hole at the sites of pus. It was not alwayseasy to insert the catheters into the space because ofthe swollen brain and on one occasion intravenousurea had to be used. Two or three millilitres ofintrathecal penicillin (2,000 units per ml.) was in-stilled down each tube, which was then closed offwith spiggots. Subsequently penicillin was introducedat varying intervals, usually eight-hourly or four-hourly. Little or no drainage of pus occurred, and thepurpose of the tubes was to administer the anti-biotic; the initial evacuation was usually sufficient.This procedure went on for approximately five toseven days and then the tubes were removed seriatim.There was no trouble with wound sepsis and the burrholes healed quickly. Throughout this period sys-temic penicillin and sulphonamides were also beinggiven and fits, when present, were controlled by anti-convulsants. General nutrition was maintained bytube feeding if necessary. At operation a swab wastaken for bacteriology and when the sensitivity of theorganisms was known the antibiotic was continuedor changed to a more appropriate one. In the earlydays we were cautious in instilling new antibioticsinto the subdural space, so a few patients were given
systemic wide-spectrum antibiotics, whilst penicillinonly was continued down the catheters.
POST-OPERATIVE PROGRESS
The patients' post-operative improvement was oftendramatic and sometimes immediate. Systemicevidence of infection and disturbances of con-sciousness usually quickly improved and the focalsigns of hemiparesis, fits, and hemianopia usuallyshowed a marked improvement by the fifth toseventh day. In a few patients the signs of subduralinfection re-appeared in the first 24 to 48 hours. Fromabout the seventh day progress was rapid and iftreatment had been successful the patients quicklybecame mobile. At the time of their discharge theywere relatively asymptomatic. This in eight out of 18cases was at approximately four weeks but variedbetween nine days and 18 weeks from admission.Air encephalography was usually performed beforedischarging the patient because of the frequency ofintracerebral abscess (17 %). A failure to improve bythe fifth or sixth day, or any increase in signs ordevelopment of new signs, encouraged specialstudies (angiography or ventriculography) and usu-ally new burr holes were made. A relapse after aninitial improvement was not uncommon and usuallywas due to a re-accumulation of pus on the con-vexity of the brain and even more frequently to theformation of a falcine collection.The 'falx syndrome' (List, 1955) was present
clinically in 11 of the 29 cases (nine paranasal andtwo otitic), and presented either early in the courseof the disease or more commonly as a cause ofrelapse. These patients had sensory or motor dis-turbances in one or other lower limb, more markeddistally, and involving the proximal muscle groupsprogressively. Finally, the trunk, the arm, andultimately the face, were involved. The sparing ofthe face is such a characteristic feature that it shouldimmediately lead to a suspicion of a falcine collec-tion. Focal fits localized to one leg or spreading toinvolve the trunk and arm occurred, and sometimesbilateral falcine collections resulted in a profoundparaparesis and a rather vague sensory loss. Such acollection is often indicated a few days before therelapse by a failure of the leg to improve at the samerate as the arm on the hemiplegic side. The spread ofthe pus over the convexity, however, is accompaniedby signs so dramatic that a falcine collection may beoverlooked. Usually there is increased pyrexia,general malaise, and a deterioration in the level ofconsciousness, but it was remarkable that falcinecollections appeared not to exert such a profoundeffect as convexity collections in these respects.There were a few patients with the 'falx syndrome'
in whom evacuation of the falcine pus undoubtedly
430
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Subditral empyema: A review of 29 cases
contributed to recovery from the relapse, and onone occasion saved a life. In such cases, therefore,fresh burr holes are indicated. If no collection can bedemonstrated it may be reasonably assumed that thedisorder is due to thrombophlebitis and that thepatient will recover. This happened, without anyfurther operation, in a few cases with clinical evidenceof the syndrome. Recovery also occurred in somecases in which falcine collections were demonstratedby angiography but no operation was performed forone reason or another. This is a matter of consider-able interest and, to our minds may, represent theinfluence of antibiotics pervading the subdural space,thus limiting the infection to small parafalcineabscesses. Furthermore it indicates that the origin ofsymptoms must be attributed to a concomitantthrombophlebitis rather than to pus accumulatingin the space. Another explanation is that the angio-
graphic appearances of a collection may be due tolocalized swelling as a result of thrombophlebitis.The following case illustrates these points.
CASE 3 E.H. (R.I. 138022), a 31-year-old man with asix-week history of frontal sinusitis, suddenly developedweakness of the right leg, progressing to a profound righthemiparesis two days before admission to this unit. Hehad been admitted elsewhere and within a few hours be-came dysphasic, with a pyrexia of 101°F. The cerebro-spinal fluid was cloudy, containing 420 cells per c.mm.,largely polymorphs, and 158 mg. of protein per 100 ml.His condition continued to deteriorate and he was trans-ferred on 28 February 1951. He was found to have acomplete right hemiplegia and right homonymous hemi-anopia, with very slight nominal dysphasia. A left carotidangiogram suggested a falcine collection. Pus was foundin the left frontoparietal subdural space ard also a smallextradural abscess was seen behind the frontal sinus.With systemic and subdural penicillin the power in theright arm improved, but the hemianopia, weakness of theright leg, and cortical sensory loss remained. On 9 Marchthe left carotid angiogram was repeated (Fig. 5a) and thefalcine collection appeared to have increased. The follow-ing day the leg began to recover and shortly afterwardsthe hemianopia decreased. On 21 March an air encephalo-gram (Fig. 5b) demonstrated depression of the left lateralventricle, regarded as due to a small left parasagittalspace-occupying lesion. A falcine exploration was ar-ranged, but before this could be done the right legweakness greatly improved and the visual fields expanded.The patient was discharged but returned for left carotidangiograms on 16 May by which time the appearanceswere normal. There had been further improvement in thesensation and power of the right foot. One year later hehad given up the toe-raising spring prescribed, and 10years later (11 April 1962) he had only a trace of weaknessin the left foot.
RESULTS OF TREATMENT
In assessing the results of the treatment, we examinedthe cases in the light of the rapidity of onset, delay
TABLE VSENSITIVITY OF ORGANISMS AND PROGRESS IN SUBDURAL
INFECTIONS
Subdural and Penicillin and No Subdural TotalSystemic Wide-spectrum PenicillinPenicillin Antibiotics
Subdurally
FIG. 5. Case 3. Left carotid angiogram showing displace-ment of the posterior branches of the pericallosal arteryaway from the midline.Air encephalogram showing depression of the left lateralventricle. It also shows absence of siibai achnoid air on theleft side.
TotalDeadSensitivity unknownDeadPenicillin-sensitiveDeadPenicillin-resistantDeadPenicillin-resistantbut sensitive towide-spectrum anti-bioticsDead
24 2 36 1 310 0 12 0 19 0 12 0 15 0 12 0 1
00
2
291011310363
0 20 1
431
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Edward Hitchcock and Alexander Andreadis
in treatment, bacterial sensitivity, and extent of thecollection of pus. The numbers were too small toallow any statistical analysis in these respects andwe are only able to give our impressions.There appeared to be no particular relationship
between mortality and the time taken to develop theestablished condition. On the other hand, there ap-peared to be some relationship between delay intreating established cases and mortality rate; al-though two patients who had the infection for 20 and31 days respectively, survived, in general those whodid best were treated early.A relationship appeared to exist between bacterial
sensitivity and morality (Table V). Cases withpenicillin-resistant organisms appeared to have abiigher mortality rate. In fact bacterial resistance wasof greater importance than the extent of the collec-tion of pus. After a trial of penicillin had failed,subsequent treatment with wide-spectrum antibio-tics produced no improvement, possibly because theiradministration was delayed.
ANALYSIS OF DEATHS The overall mortality was 10out of 29 cases, but three of these were undiagnosedand therefore untreated, so that the mortality ratefor treated cases is seven out of 26 cases. Of these,two were admitted moribund and had little hope ofrecovery. Excluding cases untreated or with delayeddiagnosis, the mortality rate was five out of 24. Intwo further patients diagnosis after admission to theneurosurgical unit was delayed. One patient died ofpulmonary embolus and electrolyte imbalance, butin addition had an undiagnosed falx collection, towhichthe death may be partially attributed. Twopatients died of undiagnosed cerebral abscess.The association with cerebral abscess formation is
interesting. Five of the 29 patients had intracerebralabscess, either concomitantly or subsequently; threeof these were from paranasal infection and two fromotitic. Of these five patients, three died. The danger ofdiagnosing subdural empyema, evacuating the col-lection, and failing to treat an intracerebral abscessis important. Similarly the treatment of intracerebralabscess only, in the presence of a subdural collectionof pus may also be fatal.
SUBSEQUENT PROGRESS
There was a rapid improvement in many of the dis-abilities until the time of the patient's discharge:hemiplegia, hemianopia, and aphasia may clear upalmost completely.
If there was a slight residual disability, e.g., slightweakness of one leg, improvement was observed tooccur over a period of three years. A few patientscontinued to improve after that period, but at the
end of three years most patients had little or nodisability.Two patients did badly, however. One subse-
quently died in a mental hospital with severe mentalchanges and aphasia, and the other, a child, has hadto have special schooling, largely because of un-controllable epilepsy.
Epilepsy is a frequent presenting symptom of thiscondition and it may persist during the acute stage.Of the 19 survivors, 17 (89%) had fits while inhospital. The incidence of epilepsy thereafter de-clines so that at the end of three years the numberof patients still having fits had fallen to five (26%).However, although epilepsy occurring in the acutestage of the illness may cease when the infection ismastered it may recur in the future, and of the 12patients who have been followed up for more thanthree years, foui (33 %) had fits. Two of the survivorswith fits also had intracerebral abscesses treated.These figures are comparable to those of North-
croft and Wyke (1957) but the number with fits willprobably increase, as one patient had her firstseizure five years after the infection; she was one ofthe two who had no fits during the acute stage. Thereare no patients in this series who have not suffered aseizure either at the onset of the illness or some yearslater.
This high incidence of epilepsy leads us to advisethe administration of anticonvulsants in all cases foran indefinite period. This is the practice of the de-partment. In fact all 19 patients had anticonvulsantswhile in hospital. However, at the end of the firstthree years only 13 of the 19 survivors were stilltaking them and thereafter only three.
SUGGESTED MANAGEMENT
Amongst the methods advised in the treatment ofthis condition, the most usual is multiple burr holesto allow the frequent instillation of antibiotics andto a lesser extent to provide drainage.- Glass (1947)and Le Beau (1949), however, advised an osteo-plastic flap, and Keith (1949) a limited craniectomyin all cases. In our experience such procedures arerarely necessary and then only if an extensive explor-ation seems indicated or if there is gross osteomyelitis.Occasionally an osteoplastic flap is necessary toexpose and remove thick exudate.
In all cases, it is important to exclude the presenceof bilateral collections of pus, and it is obviouslydesirable to explore the presumed normal side firstthrough a clean field. In cases of paranasal infectionthe burr hole is sited about 2X5 cm. from the midline inthepre-coronal frontal region, and ifnopus is revealedthe wound is closed. A similar frontal burr hole shouldthen be made on the affected side, and if pus is found
432
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

Subdural empyema: A review of 29 cases
a mid-parietal burr hole, again 2 5 cm. from themidline, should be made. If no pus is revealed at thissite, it is unnecessary to make an occipital burr hole,but a temporal one should be made in all cases.These burr holes are usually adequate to define thelimits of the collection. Other burr holes may beappropriately sited in the regions where the pus ap-pears to extend. When the limits of the collectionhave been demonstrated pus is evacuated by de-pressing the brain with a suitable instrument andallowing the pus to well up into the wound. At thisstage, a swab should be taken for culture andsensitivity. It is particularly important to make asmear immediately to determine whether theorganisms are Gram-positive or Gram-negative, sothat an appropriate antibiotic can be administered.The brain is often swollen and easily damaged, andgreat care is necessary in depressing the cortex,especially at the margins of the collections. Someauthors have advocated lumbar puncture in orderto collapse the cerebral hemisphere and so facilitatethe introduction of drainage tubes and irrigation ofthe subdural space. In one case we produced the sameeffect by administering intravenous urea, but suchprocedures are usually unnecessary and inadvisable,in that they possibly facilitate further spread. Whenit appears that all the pus has been evacuated, number8 or 10 French soft rubber catheters should be in-serted through each burr hole. Usually two or threecatheters inserted radially in different directionsallow the subdural space to be well irrigated with theantibiotic solution.
In the otitic cases, the first burr hole should bemade mid-parietal on the healthy side, again 2 5 cm.from the midline, since extension to the oppositehemisphere usually occurs via the falx. On theaffected side an occipital parasagittal burr hole isthen made and if pus is found a mid-parietal hole aswell. Again further burr holes may be made to de-fine the limits of the collection. In all cases, however,a temporal burr hole should be made.We have used subdural instillations of penicillin
solutions as used for intrathecal injections at astrength of approximately 2,000 units per ml., andupon occasion we have also used 50 mg. of strepto-mycin per millilitre. The actual dose of penicillinvaried; we have been able to insert a total up to20 ml. of antibiotic solution through the subduralcatheters. In patients with epilepsy there may appearto be an increase in seizures during the instillation ofpenicillin but this need not cause anxiety. Ourbacteriological studies have shown that the organ-isms are frequently penicillin-resistant (see Table I).However, in practice, although laboratory sensitivi-ties are useful, they do not always accord with clinicalexperience and accordingly we suggest that penicillin
and streptomycin should be administered both locallyand systematically in all cases at least until the sensi-tivities become available. Biehl (1955) also suggestedthis combination because of the predominance ofnon-haemolytic streptococci in such infections. Inthe case of otitic infections where proteus organismsare commonly present streptomycin should always beused. We have given erythromycin, 50 mg. per ml.,into the subdural space without any abnormal re-actions, and also tetracycline. These wide-spectrumantibiotics would be effective substitutes for penicillinand streptomycin in cases with resistant organisms.The antibiotic used in the tubes is also given systemic-ally and sulphadiazine and potassium citrate aregiven by mouth. Subarachnoid therapy is rarelynecessary but a lumbar puncture should be performedevery three or four days during the acute illness toexclude the development of meningitis. Penicillinmay then be injected intrathecally.The subdural catheters should be spigotted and the
burr holes sutured, the tubes being tied to one of thestitches. It is convenient to gather the tubes togetherwith a rubber band, bringing them through thedressing on the head so that subsequent instillationsmay be given without disturbing the wounds. Theantibiotic should be instilled at four-hourly intervalsfor the first 24 hours and then eight-hourly, and thecatheters left in situ for four or five days. Some maybecome blocked, and if they cannot be unblockedeasily by irrigation or shortening of the tube, theyshould be removed. After two or three days it is acommon experience that the volume of fluid it ispossible to instil becomes less. As the tubes are notused for drainage they should be spigotted aftereach instillation. There may be a little release of pus,however, and this should be cultured for organismsand sensitivity. Even after the removal of the tubessystemic antibiotics should be continued for a furtherseven or eight days in spite of the patient's improve-ment.
Signs of relapse or failure to improve imply eitherthat the organisms are insensitive to the antibiotic ad-ministered, or that a fresh collection has formed in-accessible to the irrigating fluids. Angiography is themost useful investigation and may then reveal afresh collection which will require more burr holesand tubes. Apart from new collections, however, thesubdural empyema may re-accumulate on the sameside, and it may then be necessary either to re-openthe burr holes or make new ones. If investigationsor inspections suggest loculation and formation of athick capsule, it may be necessary to turn an osteo-plastic flap to remove it, but it has not been con-sidered necessary in our series.The general condition of the patient should re-
ceive attention throughout, and especially with
433
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from

434Edward Hitchcock and Alexander Andreadis
regard to adequate fluid intake and physiotherapy forparalysed limbs. The relapses are usually insidiousbut may be acute and these patients require thekeenest observation throughout their stay in hospital.
SUMMARY
The clinical, laboratory, radiological, and patho-logical features of 29 cases of subdural empyemaadmitted to the Radcliffe Infirmary from 1949 to1962 inclusive are reviewed.Paranasal sinus or ear infection was the usual
cause.Pathways for the extension of pus in the subdural
space are described.The problems of diagnosis are discussed and the
value of angiography emphasized.The occurrence of penicillin-resistant organisms,
especially in cases following otitic infections, isstressed, and an operative method of treatment,using multiple burr holes and subdural instillations ofpenicillin and streptomycin, and on occasion wide-spectrum antibiotics, is advocated.
We have pleasure in acknowledging the advice and assist-ance of Mr. Joe Pennybacker in the preparation of this
report of patients passing through the Department ofNeurological Surgeiy Mr. John Potter kindly read themanuscript and made helpful suggestions. Dr. PhilipSheldon advised us on the radiology. This work wasundertaken while E.H. was in receipt of a grant from theSir Hugh Cairns Memorial Fund.
REFERENCES
Biehl, J. P. (1955). Subdural empyema secondary to acute frontalsinusitis. J. Amer. med. Ass., 158, 721-724.
Courville, C. B. (1944). Subdural empyema secondary to purulentfrontal sinusitis. Arch. Otolaryng., 39, 211-230.
Glass, R. L. (1947). Osteoplastic flap method in the treatment ofsubdural abscess. J. Neurosurg., 4, 391-393.
Keith, W. S. (1949). Subdural empyema. Ibid., 6, 127-139.Kubik, C. S., and Adams, R. D. (1943). Subdural empyema. Brain, 66,
18-42.Le Beau, J. (1949). Traitement chirurgical de l'empy6me sous-dural
et sous-arachnoldien. Rev. neurol., 81, 828-851.List, C. F. (1955). Diagnosis and treatment of acute subdural em-
pyema. Neurology (Minneap.), 5, 663-670.Northcroft, G. B., and Wyke, B. D. (1957). Seizures following surgical
treatment of intracranial abscesses, J. Neurosurg., 14, 249-263.Schiller, F., Cairns, H., and Russell, D. S. (1948). The treatment of
purulent pachymeningitis and subdural suppuration withspecial reference to penicillin. J. Neurol. Neurosurg. Psychiat.,11, 143-182.
Stern, W. E., and Boldrey, E. (1952). Subdural purulent collections.Surg. Gynec. Obstet. 95, 623-630.
Stephens, J., and Welch, K. (1956). Subdural abscess with retinalthrombophlebitis, Neurology, 6, 889-890.
Wood, P. H. (1952), Diffuse subdural suppuration. J. Laryng., 66,496-515.
434
Protected by copyright.
on February 4, 2021 by guest.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.27.5.422 on 1 October 1964. D
ownloaded from