Su1617 Impact of Fluoroscopy Frame Rate, Image Magnification, Collimation and Height of the Image...
1
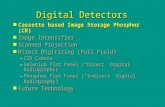
Su1617 Impact of Fluoroscopy Frame Rate, Image Magnification, Collimation and Height of the Image Intensifier on Radiation Exposure to Patients During ERCP Nirav C. Thosani* 1 , Jia Wang 2 , Soheil Damavandi 2 , Ann M. Chen 1 , Shai Friedland 1 , Subhas Banerjee 1 1 Gastroenterology and Hepatology, Stanford University, Stanford, CA; 2 Environmental Health & Safety, Stanford University, Stanford, CA Background: The use of fluoroscopy during ERCP exposes patients and endoscopy staff to the risks of ionizing radiation. Fluoroscopy during ERCP is predominantly controlled by endoscopists, who may lack detailed technical knowledge regarding the fluoroscopy machine in use. Few data exist on radiation doses received by pa- tients during ERCP and no data are available on the impact of current generation fluoroscopy machines, which allow modification of factors such as the fluoroscopy frame rate (FFR), degree of magnification (Magnification), height of image intensi- fier (Height) and Collimation, all of which can modulate the radiation dose received, for the same duration of Fluoroscopy Time. Aim: To determine the impact of FFR, Magnification, Height and Collimation on radiation exposure, using a phantom model. Methods: To simulate average patient attenuation, an acrylic abdominal phantom with dimensions of 18 cm (length) x 18 cm (breadth) x 20 cm (height) was placed on the fluoroscopy table. A 10 x 5-6 general purpose ‘in-beam’ ion chamber (Radcal, Monrovia, CA) was placed underneath the phantom to measure the Entrance Skin Dose in mRads during fluoroscopy. The Entrance Skin Dose, Effec- tive Dose Rate (mGy/min) and Dose Area product were measured by varying the exposure parameters: FFR (4 and 15/sec), Magnification [16 (lowest) 12, 9, & 6 in- ches (highest)], Height (minimum: image intensifier as close to phantom as possible, maximum: as far as possible), and at varying degrees of Collimation. Results: The lowest Effective Dose Rate was 2.6 mGy/min at the lowest modifiable settings of FFR 4, Magnification 16, and minimum Height. Compared to that, at the maximum settings of FFR 15, Magnification 6, and maximum Heaight, the Effective Dose Rate was 56.11 mGy/min (2058% increase). The Effective Dose Rate increased incrementally with higher levels of Magnification, FFR and Height (Figure 1). A similar trend of increased Entrance Skin Dose was seen with incremental higher levels of FFR, Magnigications and Height (Figure 2). A single spot film conferred an Entrance Skin Dose of 15 mRad at the lowest settings of FR, Magni- fication and Height and of 156 mRad (940% increase) at the highest settings of these parameters. A significant linear correlation was seen between use of Collimation and a decrease in the Dose Area Product. Collimation with a decrease in the field of exposure by 50%, resulted in a 50% decrease in the Dose Area Product. Conclusion: Our study establishes the effects of modulating FFR, Magnification, Height and Collimation in reducing radiation exposure during ERCP. These modifiable fluo- roscopy parameters are available in current generation fluoroscopy machines. Knowledge gained from these results should help endoscopists decrease patient radiation exposure during ERCP. Impact of FFR, Magnification and Height on Effective Dose Rate Impact of Magnification and Height on Entrance Skin Dose per spot film Table 2. Predictors of Increased Patient Radiation (50th Percentile of Dose Area Product) in Univariate and Multivariate Analysis Variable Odds Ratio 95% Confidence Interval p Value Univariate Analysis Age O 60 1.9 1.23-2.95 0.004 Sex (Male) 1.56 1.02-2.42 0.042 Sedation (GA) 1.89 1.21-2.96 0.005 Procedure Time 1.04 1.03-1.05 0.001 Indication (Choledocholithiasis) 2.46 1.50-4.01 0.001 Difficult Cannulation 10.16 3.01-34.29 0.001 Guidewires (Two or more) 2.66 1.01-7.05 0.048 Previous Stent in place 0.5 0.33-0.79 0.002 Sphincterotomy 2.52 1.61-3.93 0.001 ERCP Difficulty Grade 3 & 4 1.62 1.03-2.54 0.036 Low volume endoscopist 2.48 1.45-4.21 0.001 Balloon Sweep 1.57 1.01-2.42 0.042 Spy Glass cholangioscopy 3.47 1.34-8.92 0.010 Bile Duct Biopsy 5.85 1.27-26.84 0.023 Stanford Fluoroscopy Complexity Score (O 10) 2.59 1.06-6.30 0.036 Multivariate Analysis Age O 60 1.91 1.08-3.37 0.025 Sex (Male) 2.5 1.42-4.39 0.001 BMI (O30) 2.36 1.12-4.96 0.023 Sedation (GA) 2.14 1.14-4.01 0.018 Procedure Time 1.03 1.01-10.5 0.001 Indication (Choledocholithiasis) 2.2 1.11-4.37 0.024 Difficult Cannulation 9.6 2.08-44.30 0.004 Low volume endoscopist ( ! 200 ERCP/Year) 3.41 1.61-7.20 0.001 Stanford Fluoroscopy Complexity Score (5-10) 2.29 1.03-5.08 0.042 Stanford Fluoroscopy Complexity Score (O 10) 5.13 1.40-18.76 0.013 AB234 GASTROINTESTINAL ENDOSCOPY Volume 79, No. 5S : 2014 www.giejournal.org Abstracts
Transcript of Su1617 Impact of Fluoroscopy Frame Rate, Image Magnification, Collimation and Height of the Image...

Table 2. Predictors of Increased Patient Radiation (50th Percentile ofDose Area Product) in Univariate and Multivariate Analysis
VariableOddsRatio
95% ConfidenceInterval p Value
Univariate AnalysisAge O 60 1.9 1.23-2.95 0.004Sex (Male) 1.56 1.02-2.42 0.042Sedation (GA) 1.89 1.21-2.96 0.005Procedure Time 1.04 1.03-1.05 0.001Indication (Choledocholithiasis) 2.46 1.50-4.01 0.001Difficult Cannulation 10.16 3.01-34.29 0.001Guidewires (Two or more) 2.66 1.01-7.05 0.048Previous Stent in place 0.5 0.33-0.79 0.002Sphincterotomy 2.52 1.61-3.93 0.001ERCP Difficulty Grade 3 & 4 1.62 1.03-2.54 0.036Low volume endoscopist 2.48 1.45-4.21 0.001Balloon Sweep 1.57 1.01-2.42 0.042Spy Glass cholangioscopy 3.47 1.34-8.92 0.010Bile Duct Biopsy 5.85 1.27-26.84 0.023Stanford Fluoroscopy Complexity
Score (O 10)2.59 1.06-6.30 0.036
Multivariate AnalysisAge O 60 1.91 1.08-3.37 0.025Sex (Male) 2.5 1.42-4.39 0.001BMI (O30) 2.36 1.12-4.96 0.023Sedation (GA) 2.14 1.14-4.01 0.018Procedure Time 1.03 1.01-10.5 0.001Indication (Choledocholithiasis) 2.2 1.11-4.37 0.024Difficult Cannulation 9.6 2.08-44.30 0.004Low volume endoscopist (! 200 ERCP/Year) 3.41 1.61-7.20 0.001Stanford Fluoroscopy Complexity
Score (5-10)2.29 1.03-5.08 0.042
Stanford Fluoroscopy ComplexityScore (O 10)
5.13 1.40-18.76 0.013
Abstracts
Su1617Impact of Fluoroscopy Frame Rate, Image Magnification,Collimation and Height of the Image Intensifier on RadiationExposure to Patients During ERCPNirav C. Thosani*1, Jia Wang2, Soheil Damavandi2, Ann M. Chen1,Shai Friedland1, Subhas Banerjee11Gastroenterology and Hepatology, Stanford University, Stanford, CA;2Environmental Health & Safety, Stanford University, Stanford, CABackground: The use of fluoroscopy during ERCP exposes patients and endoscopystaff to the risks of ionizing radiation. Fluoroscopy during ERCP is predominantlycontrolled by endoscopists, who may lack detailed technical knowledge regardingthe fluoroscopy machine in use. Few data exist on radiation doses received by pa-tients during ERCP and no data are available on the impact of current generationfluoroscopy machines, which allow modification of factors such as the fluoroscopyframe rate (FFR), degree of magnification (Magnification), height of image intensi-fier (Height) and Collimation, all of which can modulate the radiation dose received,for the same duration of Fluoroscopy Time. Aim: To determine the impact of FFR,Magnification, Height and Collimation on radiation exposure, using a phantommodel. Methods: To simulate average patient attenuation, an acrylic abdominalphantom with dimensions of 18 cm (length) x 18 cm (breadth) x 20 cm (height) wasplaced on the fluoroscopy table. A 10 x 5-6 general purpose ‘in-beam’ ion chamber(Radcal, Monrovia, CA) was placed underneath the phantom to measure theEntrance Skin Dose in mRads during fluoroscopy. The Entrance Skin Dose, Effec-tive Dose Rate (mGy/min) and Dose Area product were measured by varying theexposure parameters: FFR (4 and 15/sec), Magnification [16 (lowest) 12, 9, & 6 in-ches (highest)], Height (minimum: image intensifier as close to phantom aspossible, maximum: as far as possible), and at varying degrees of Collimation.Results: The lowest Effective Dose Rate was 2.6 mGy/min at the lowest modifiablesettings of FFR 4, Magnification 16, and minimum Height. Compared to that, atthe maximum settings of FFR 15, Magnification 6, and maximum Heaight, theEffective Dose Rate was 56.11 mGy/min (2058% increase). The Effective Dose Rateincreased incrementally with higher levels of Magnification, FFR and Height (Figure1). A similar trend of increased Entrance Skin Dose was seen with incrementalhigher levels of FFR, Magnigications and Height (Figure 2). A single spot filmconferred an Entrance Skin Dose of 15 mRad at the lowest settings of FR, Magni-fication and Height and of 156 mRad (940% increase) at the highest settings of theseparameters. A significant linear correlation was seen between use of Collimation anda decrease in the Dose Area Product. Collimation with a decrease in the field ofexposure by 50%, resulted in a 50% decrease in the Dose Area Product. Conclusion:Our study establishes the effects of modulating FFR, Magnification, Height andCollimation in reducing radiation exposure during ERCP. These modifiable fluo-roscopy parameters are available in current generation fluoroscopy machines.Knowledge gained from these results should help endoscopists decrease patientradiation exposure during ERCP.
AB234 GASTROINTESTINAL ENDOSCOPY Volume 79, No. 5S : 2014
Impact of FFR, Magnification and Height on Effective Dose Rate
Impact of Magnification and Height on Entrance Skin Dose per spot film
www.giejournal.org