paediatric acute severe asthma paediatric life threatening asthma
Upload
chulalongkorn-allergy-and-clinical-immunology-research-groupCategory
view
103download
6
Studies of Biologic agents in severe asthma
Lalita Teaprasert; M.D. 17 Feb 2017

Outline
• Introduction • Studies of Biologic agents - Omalizumab - Lebrikizumab - Mepolizumab - Tralokinumab - Reslizumab - Benralizumab
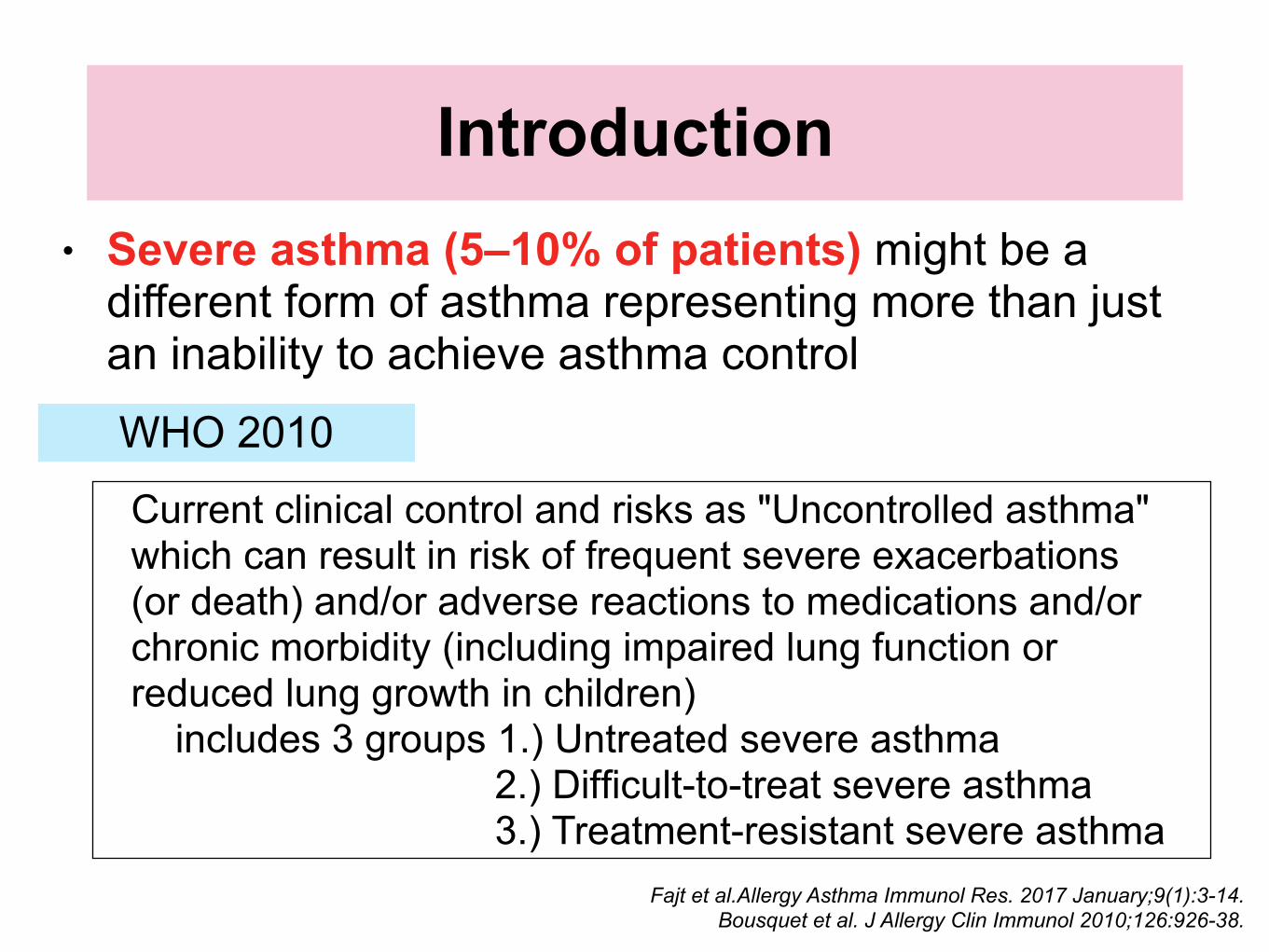
Introduction• Severe asthma (5–10% of patients) might be a
different form of asthma representing more than just an inability to achieve asthma control
Fajt et al.Allergy Asthma Immunol Res. 2017 January;9(1):3-14. Bousquet et al. J Allergy Clin Immunol 2010;126:926-38.
Current clinical control and risks as "Uncontrolled asthma" which can result in risk of frequent severe exacerbations (or death) and/or adverse reactions to medications and/or chronic morbidity (including impaired lung function or reduced lung growth in children) includes 3 groups 1.) Untreated severe asthma 2.) Difficult-to-treat severe asthma 3.) Treatment-resistant severe asthma
WHO 2010
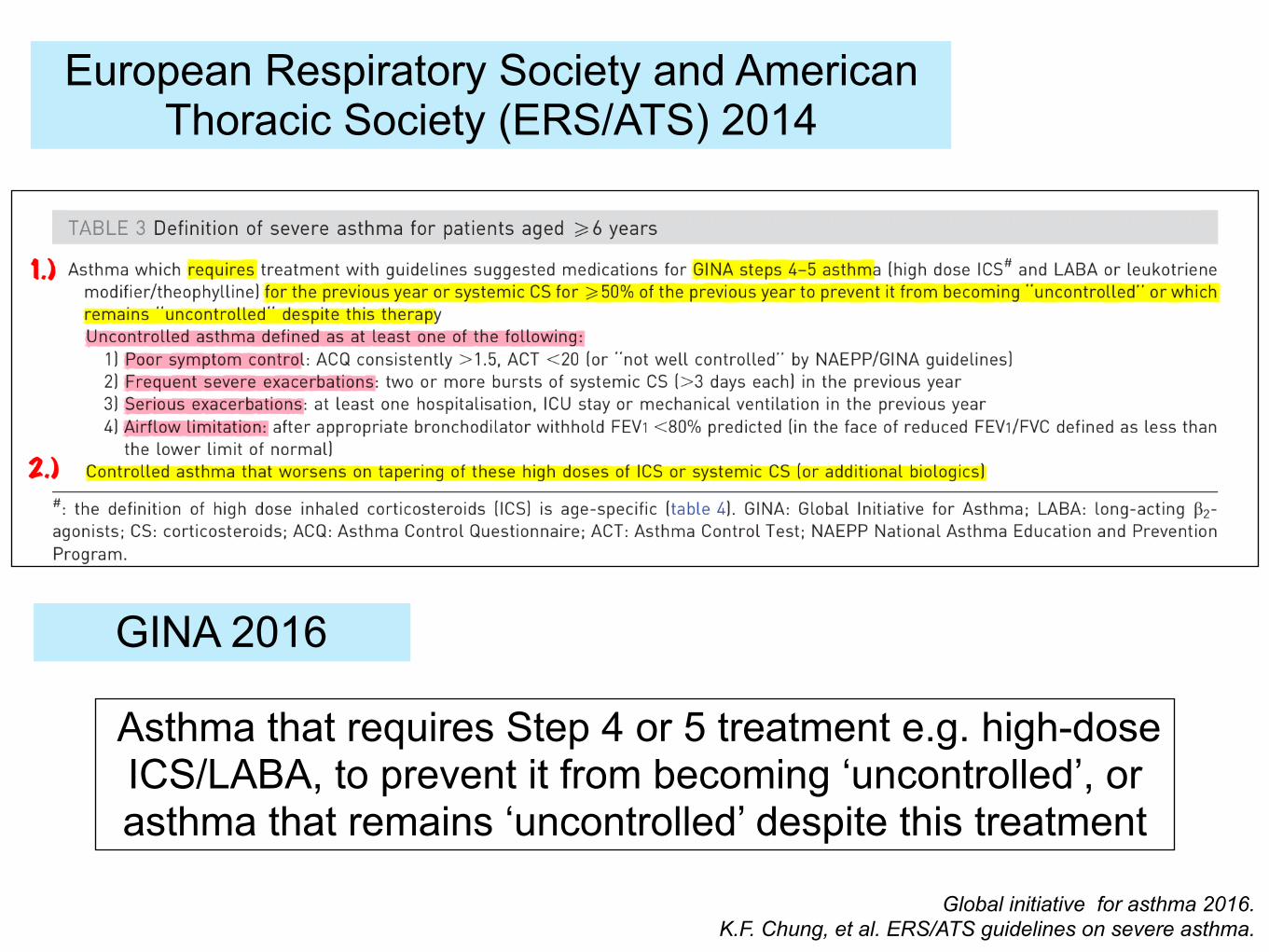
European Respiratory Society and American Thoracic Society (ERS/ATS) 2014
Asthma that requires Step 4 or 5 treatment e.g. high-dose ICS/LABA, to prevent it from becoming ‘uncontrolled’, or asthma that remains ‘uncontrolled’ despite this treatment
GINA 2016
Global initiative for asthma 2016. K.F. Chung, et al. ERS/ATS guidelines on severe asthma.

Charriot J, et al. Eur Respir Rev 2016; 25: 77–92.
Phenotype & Endotype

GINA 2016
Global Strategy for Asthma Management and Prevention 2016.

Expert Panel Report 3,National Heart, Lung, and Blood Institute. August 28, 2007.
EPR-3

mo xi zu mu
Monoclonal Ab
k or ki precedes the mab for interleukin agents l or li in immunomodulatory agents
J.B. Bice et al. / Ann Allergy Asthma Immunol 112 (2014) 108e115.

Fajt et al.Allergy Asthma Immunol Res. 2017 January;9(1):3-14.
Selected therapeutic targets of asthmaMost biologics to date in adults have focused on these Th 2 cytokines
including anti–IL-4–, anti–IL-5–, and anti–IL-13–based therapies

Major immunologic pathways and biologic therapies
J.B. Bice et al. / Ann Allergy Asthma Immunol 112 (2014) 108e115.

1.) Omalizumab : 2003 2.) Mepolizumab : 2015 3.) Reslizumab : 2016
Muraro et al.PRACTALL consensus report. J Allergy Clin Immunol 2016;137:1347-58.

Asthma biomarkers used in biologic trials
J.B. Bice et al. / Ann Allergy Asthma Immunol 112 (2014) 108e115.

Omalizumab
L. Francés. Actas Dermosifiliogr 2014;105:45-52 - Vol. 105.
• Recombinant DNA-derived, humanized antibody • First FDA-approved biologic : 2003 • Age ≥ 12 yr --> In July 2016, FDA approved Age ≥ 6 yr • Moderate-to- severe persistent asthma whose disease is
not adequately controlled with ICSs alone
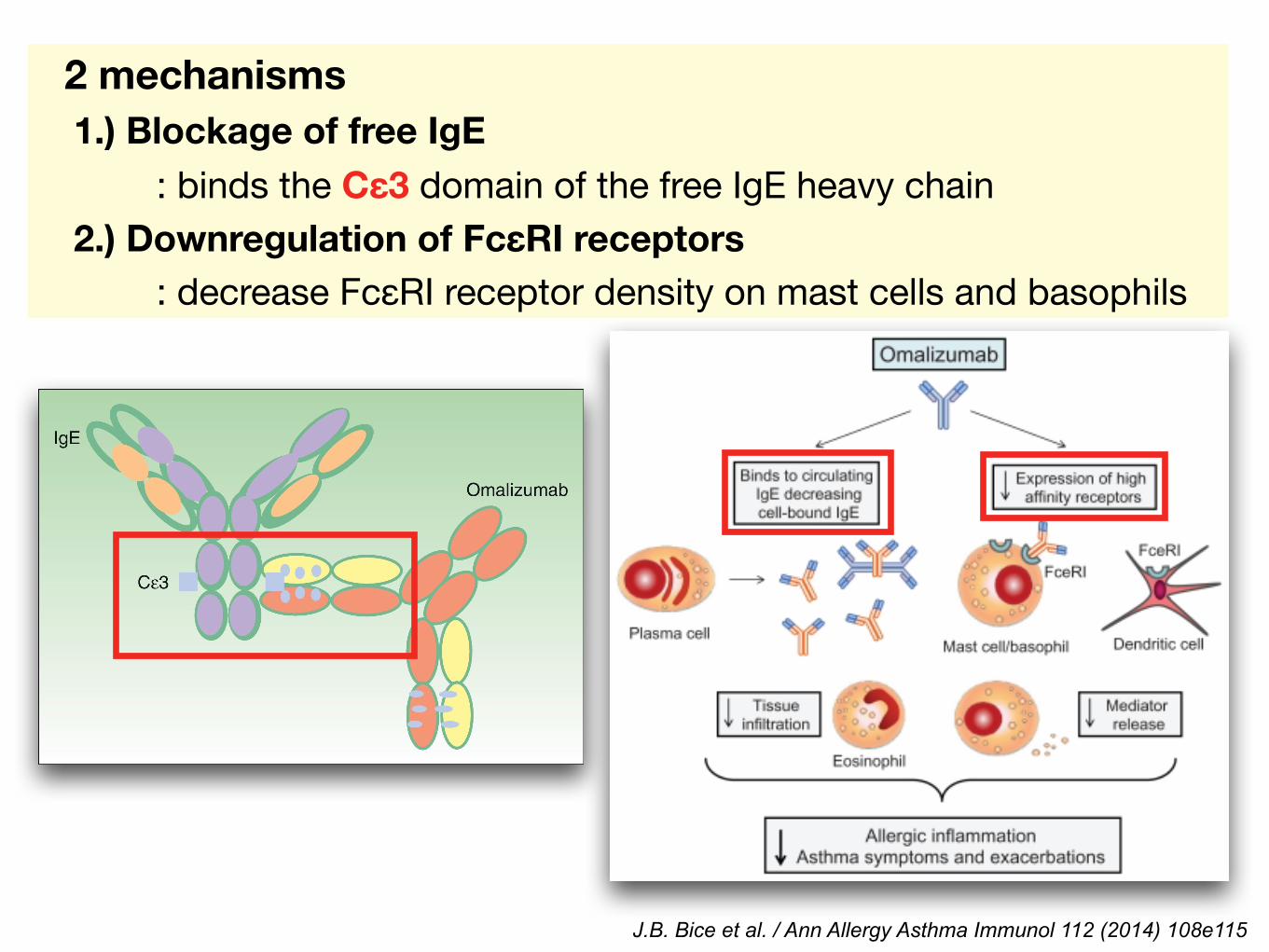
2 mechanisms 1.) Blockage of free IgE : binds the Cε3 domain of the free IgE heavy chain 2.) Downregulation of FcεRI receptors : decrease FcεRI receptor density on mast cells and basophils
J.B. Bice et al. / Ann Allergy Asthma Immunol 112 (2014) 108e115

https://www.xolair.com/pdf/dosingtables.pdf

Busse WW and Morgan WJ, et al. N Engl J Med 2011; 364:1005-1015.
• P : 419 inner-city participants, 6-20 years old - predominantly moderate-to-severe persistent or uncontrolled asthma • I, C : Randomization 1.) 208 to omalizumab 2.) 211 to placebo Rx 60 weeks • O : - Primary outcome was symptoms of asthma
ICATA
Randomized, double-blind, placebo-controlled, parallel-group, multicenter trial

Busse WW and Morgan WJ, et al. N Engl J Med 2011; 364:1005-1015.
• Omalizumab resulted in absolute reductions in exacerbations,
symptom days, and hospitalizations compared with placebo

Busse WW and Morgan WJ, et al. N Engl J Med 2011; 364:1005-1015.
• Omalizumab was found to nearly eliminate the seasonal
variability of exacerbations in the fall and spring
Reduced 109 mcg/ day
• P : 850 patients aged 12 to 75 years who had inadequately controlled asthma despite treatment with high-dose ICS plus LABAs, with or without other controllers • I, C : Omalizumab (n=427) or placebo (n= 423) was added to existing medication regimens for 48 weeks • O : Primary end point was the rate of protocol defined exacerbations over the study period
Prospective, multicenter, randomized, parallel-group, double-blind, placebo-controlled trial
Hanania NA, et al. Ann Intern Med. 2011;154:573-582.
EXTRA

Asthma exacerbation rate during the 48-week treatment period was significantly lower in the omalizumab group than in the placebo group
Hanania NA, et al. Ann Intern Med. 2011;154:573-582.

Omalizumab increased the time to first asthma exacerbation (hazard ratio, 0.74 [CI, 0.60 to 0.93]; P=0.008)
Hanania NA, et al. Ann Intern Med. 2011;154:573-582.

• Omalizumab compared with placebo during the 48-week study period - Improved mean AQLQ(S) scores (0.29 point [CI, 0.15 to 0.43]) - Reduced mean daily albuterol puffs (0.27 puff/d [CI, 0.49 to 0.04 puff/d]) - Decreased mean asthma symptom score (0.26 [CI, 0.42 to 0.10])
• The incidence of adverse events (80.4% vs. 79.5%) and serious adverse events (9.3% vs. 10.5%) were similar in the omalizumab and placebo groups
Omalizumab provided additional clinical benefit for patients with severe allergic asthma that is inadequately
controlled with high-dose ICS and LABA therapy.

Milgrom H, et al. PEDIATRICS Vol. 108 No. 2 August 2001
• P : 334 patients, 6 to 12 years - moderate to severe allergic asthma requiring treatment with inhaled corticosteroids (ICSs equivalent to 168-420 mg/d BDP and bronchodilator therapy as needed for ≥ 3 months before randomization) • I, C : Randomized into the double-blind study - 225 patents to omalizumab (76 dosed every 2 weeks, 149 dosed every 4 weeks) -109 to placebo (35 dosed every 2 weeks, 74 dosed every 4 weeks)

Study Protocol
• After a 1-week enrollment and screening period • 3 phases 1.) run-in phase (4–6 weeks) 2.) stable-steroid phase (16 weeks) 3.) steroid dose-reduction phase (12 weeks) • Over the first 8 weeks of steroid dose-reduction phase, BDP was reduced step-wise, approximately 25% of the baseline dose every 2 weeks, until total elimination or worsening of asthma, to establish the minimum effective dose of BDP • Participants were maintained on this minimum effective
dose of BDP during the last 4 weeks of the steroid dose-reduction phase.

Milgrom H, et al. PEDIATRICS Vol. 108 No. 2 August 2001
• O : Omalizumab group decreased BDP dose, and reduction was greater than that of the placebo group (median reduction 100% vs 66.7%)

Treatment with omalizumab is safe in children with asthma. It reduces the requirement for inhaled corticosteroids while
protecting against disease exacerbation
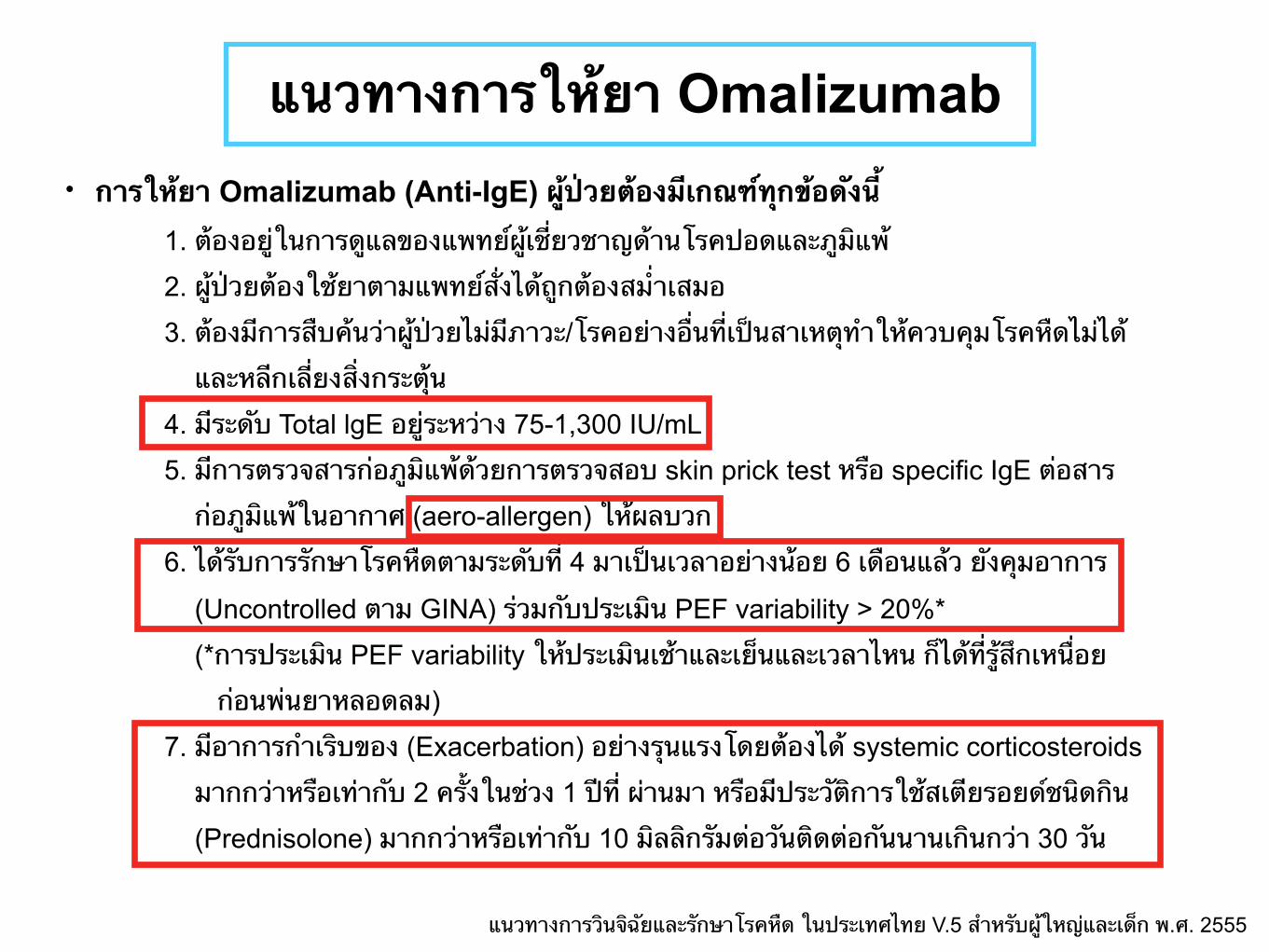
แนวทางการให้ยา Omalizumab• การให้ยา Omalizumab (Anti-IgE) ผู้ป่วยต้องมีเกณฑ์ทุกข้อดังนี้ 1. ต้องอยู่ในการดูแลของแพทย์ผู้เชี่ยวชาญด้านโรคปอดและภูมิแพ้
2. ผู้ป่วยต้องใช้ยาตามแพทย์สั่งได้ถูกต้องสม่ำเสมอ
3. ต้องมีการสืบค้นว่าผู้ป่วยไม่มีภาวะ/โรคอย่างอื่นที่เป็นสาเหตุทำให้ควบคุมโรคหืดไม่ได้
และหลีกเลี่ยงสิ่งกระตุ้น
4. มีระดับ Total lgE อยู่ระหว่าง 75-1,300 IU/mL
5. มีการตรวจสารก่อภูมิแพ้ด้วยการตรวจสอบ skin prick test หรือ specific IgE ต่อสาร
ก่อภูมิแพ้ในอากาศ (aero-allergen) ให้ผลบวก
6. ได้รับการรักษาโรคหืดตามระดับที่ 4 มาเป็นเวลาอย่างน้อย 6 เดือนแล้ว ยังคุมอาการ
(Uncontrolled ตาม GINA) ร่วมกับประเมิน PEF variability > 20%*
(*การประเมิน PEF variability ให้ประเมินเช้าและเย็นและเวลาไหน ก็ได้ที่รู้สึกเหนื่อย
ก่อนพ่นยาหลอดลม)
7. มีอาการกำเริบของ (Exacerbation) อย่างรุนแรงโดยต้องได้ systemic corticosteroids
มากกว่าหรือเท่ากับ 2 ครั้งในช่วง 1 ปีท่ี ผ่านมา หรือมีประวัติการใช้สเตียรอยด์ชนิดกิน
(Prednisolone) มากกว่าหรือเท่ากับ 10 มิลลิกรัมต่อวันติดต่อกันนานเกินกว่า 30 วัน
แนวทางการวินจิฉัยและรักษาโรคหืด ในประเทศไทย V.5 สำหรับผู้ใหญ่และเด็ก พ.ศ. 2555

J.B. Bice et al. / Ann Allergy Asthma Immunol 112 (2014) 108e115.

• Mepolizumab (Nucala, GSK) : humanized IgG1 mAb against IL-5
• Reslizumab (Cinqair,Teva) : humanized IgG4 mAb against IL-5
• Benralizumab (Astra) : humanized Ab targeting the alpha-chain of IL-5 receptor
Anti IL-5

Patterson MF, et al. Journal of Asthma and Allergy 2015:8 125–134.
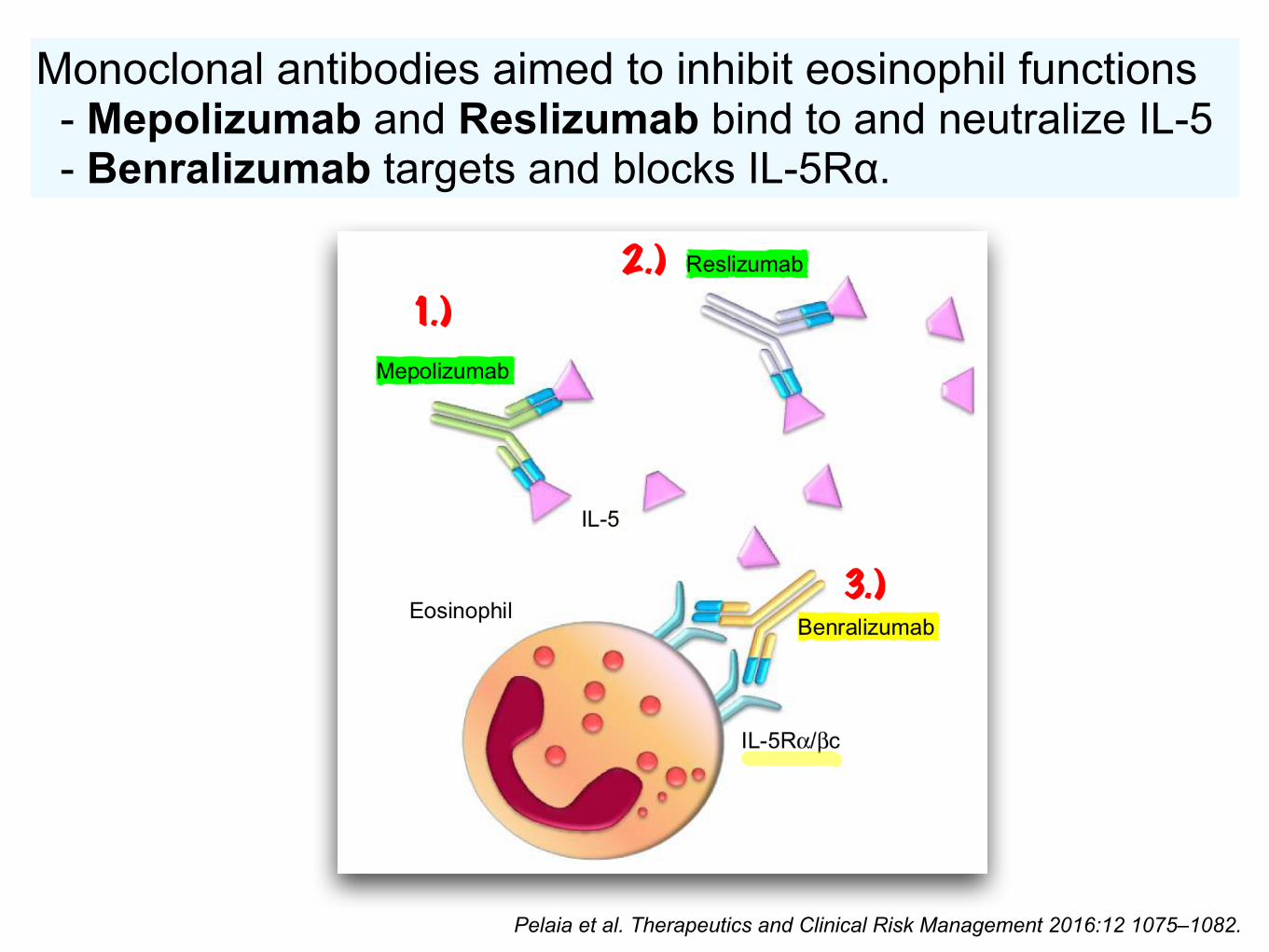
Pelaia et al. Therapeutics and Clinical Risk Management 2016:12 1075–1082.
Monoclonal antibodies aimed to inhibit eosinophil functions - Mepolizumab and Reslizumab bind to and neutralize IL-5 - Benralizumab targets and blocks IL-5Rα.

Mepolizumab
http://en.pharmacodia.com/web/drug/1_2056.html
NUCALA (mepolizumab) • Humanized IgG1 mAb against IL-5 • FDA Approved : Nov 2015 • Age ≥ 12 yr • Severe eosinophilic asthma - Blood eosinophils ≥ 150 cells/µl at initiation of Rx OR ≥ 300 cells/µl in the past 12 months • 100 mg SC q 4 wk
Haldar P, et al. N Engl J Med 2009;360:973-84.
• P : 61 subjects, age > 18 yr. - refractory eosinophilic asthma and a history of recurrent severe exacerbations
• I,C : 1.) Mepolizumab 750 mg IV : 29 subjects 2.) Placebo : 32 subjects (duration 1 year)
• O : Primary outcome --> number of severe exacerbations per subject during the 50-week treatment Secondary outcomes --> a change in asthma symptoms, scores on the Asthma Quality of Life Questionnaire (AQLQ)
Randomized, double-blind, placebo-controlled, parallel-group study

• Mepolizumab therapy reduces exacerbations and improves
• AQLQ scores in patients with refractory eosinophilic asthma
P=0.02
P=0.02
Haldar P, et al. N Engl J Med 2009;360:973-84.

Ian D Pavord, et al. Lancet 2012; 380: 651–59.
• P : 621 patients, 12–74 years - Hx of recurrent severe asthma exacerbations, and had signs of eosinophilic inflammation • I, C : Random in 4 group (1:1:1:1 ratio), 52 weeks treatment - Mepolizumab 75 mg : 154 patients - Mepolizumab 250 mg : 152 patients - Mepolizumab 750 mg : 156 patients - Placebo (100 mL 0.9% NaCl) : 159 patients • O : Primary outcome was the rate of clinically significant asthma exacerbations (acute asthma requiring treatment with oral corticosteroids, admission, or a visit to an emergency department)
Multicenter, double-blind, placebo-controlled trial DREAM

• Compared with placebo reduced the number of clinically significant exacerbations per patient per year
• 75 mg mepolizumab : 48% (95% CI 31–61%; p<0.0001) 250 mg mepolizumab : 39% (95% CI19–54%; p=0.0005)
750 mg mepolizumab : 52% (95% CI 36–64%; p<0.0001)
Ian D Pavord, et al. Lancet 2012; 380: 651–59.
Mepolizumab is an effective and well tolerated treatment that reduces the risk of asthma exacerbations in patients
with severe eosinophilic asthma.

• P : 576 patients, 12-82 yr. - Recurrent asthma exacerbations and evidence of eosinophilic inflammation • I, C : 1.) 75-mg intravenous 2.) 100-mg subcutaneous 3.) placebo subcutaneous every 4 weeks for 32 weeks • O : Primary outcome was the rate of exacerbations
Ortega HG, et al. NEJM 371;13, September 25, 2014.
MENSARandomized, double-blind, double-dummy study
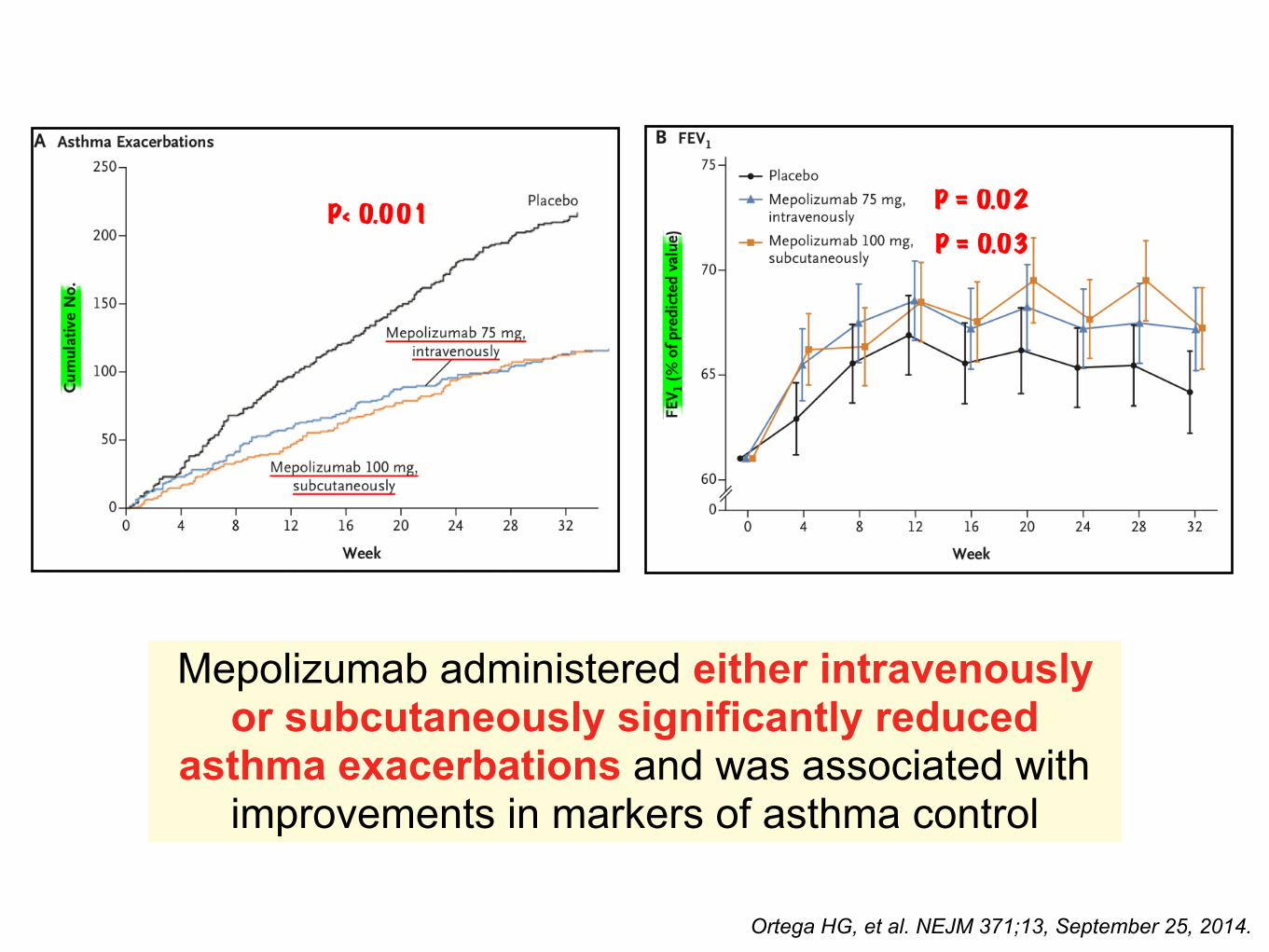
Ortega HG, et al. NEJM 371;13, September 25, 2014.
Mepolizumab administered either intravenously or subcutaneously significantly reduced
asthma exacerbations and was associated with improvements in markers of asthma control

• P : 135 patients, severe eosinophilic asthma • I, C : 135 participants, Mean age 50 yr.
SIRIUSMulticenter, randomized, placebo-controlled, double-blind, parallel-group study
Bel EH, et al. NEJM 371;13, September 25, 2014.
N = 69
N = 66

Bel EH, et al. NEJM 371;13, September 25, 2014.
• O :- A reduction in the glucocorticoid-dose stratum was 2.39 times greater in the mepolizumab group than in the placebo group (95% confidence interval, 1.25 to 4.56; P = 0.008) - Median percentage reduction from baseline in the glucocorticoid dose was 50% in the mepolizumab group, as compared with no reduction in the placebo group (P = 0.007)

Bel EH, et al. NEJM 371;13, September 25, 2014.
P = 0.007P = 0.04
P = 0.004Daily oral glucocorticoid therapy to maintain asthma control, mepolizumab had a significant glucocorticoid-
sparing effect, reduced exacerbations, and improved control of asthma symptoms

Reslizumab
Pelaia et al. Therapeutics and Clinical Risk Management 2016:12 1075–1082.
CINQUIR (Reslizumab) • Humanized IgG4 kappa mAb against IL-5 • FDA approved : March 2016 • Age > 18 yr • Severe eosinophilic asthma Blood eosinophils > 400 cells/µl at initiation of Rx • 3 mg/kg q 4 wk IV infusion over 20-50 min

• P : - 12- to 75-year-old patients, poorly controlled asthma maintained on medium-to-high doses ICSs, peripheral eosinophil count of 400/mL and have one or more exacerbations in the previous year • I, C : Randomly assigned (1:1) 1.) intravenous reslizumab (3 mg/kg) 2.) placebo every 4 weeks for 1 year
Castro M et al., Lancet Respir Med 2015;3:355-66.
• Two duplicate, multicentre, Double-blind, parallel-group, randomised, placebo-controlled phase 3 trials
• Multicenter : Asia, Australia, North America, South America, South Africa, and Europe
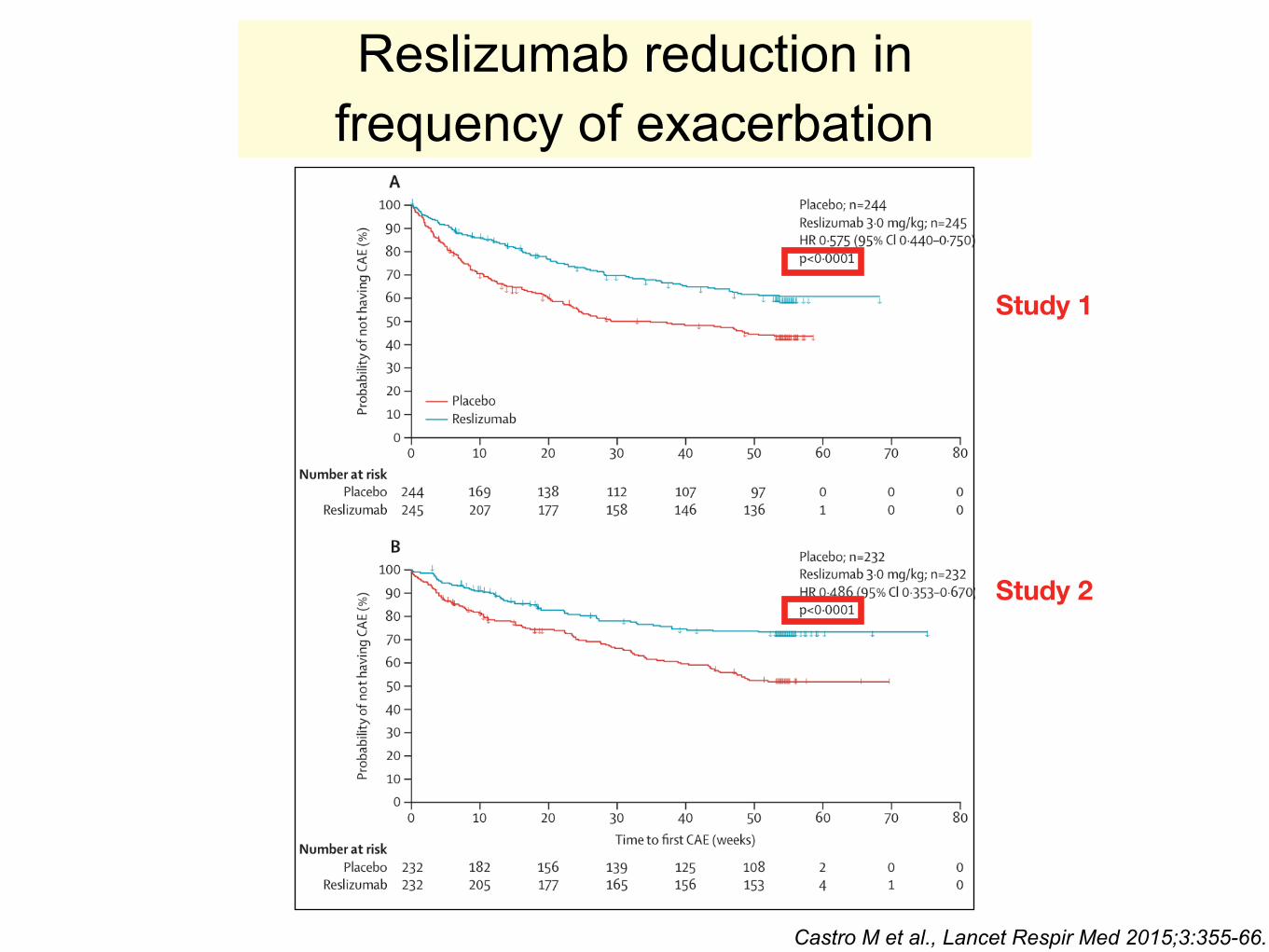
Reslizumab reduction in frequency of exacerbation
Castro M et al., Lancet Respir Med 2015;3:355-66.
Study 1
Study 2

Castro M et al., Lancet Respir Med 2015;3:355-66.
Improvement in FEV1 was evident for reslizumab by at wk 4, which was sustained through to wk 16 & 52

Reslizumab also improved AQLQ total score, ACQ-7 score, ASUI score
Castro M et al., Lancet Respir Med 2015;3:355-66.

Support the use of reslizumab in patients with asthma & elevated blood
eosinophil who are inadequately controlled on ICS
Castro M et al., Lancet Respir Med 2015;3:355-66.

Benralizumab
Randomised, double-blind, parallel-group, placebo-controlled phase 3 study at 374 sites in 17 countries
• P : 1,205 severe uncontrolled asthmatics (age 12-75 yr) - diagnosis of asthma for at least 1 year and at least two exacerbations while on high-dosage inhaled corticosteroids and long-acting β 2 -agonists (ICS plus LABA) in the previous year
Bleecker ER, et al.Lancet 2016; 388: 2115–27
SIROCCO

• I, C : Randomly assigned (1:1:1) 1) Benralizumab 30 mg SC q 4 wk 2) Benralizumab 30 mg SC q 4 wk for 3 doses then q 8 wk 3) Placebo for 48 wk
• O : Primary endpoint --> annual exacerbation rate ratio versus placebo Secondary endpoints --> prebronchodilator FEV 1 and total asthma symptom score at week 48, for patients with blood eosinophil counts of at least 300 cells per µL
Bleecker ER, et al.Lancet 2016; 388: 2115–27

Both dosing regimens of benralizumab significantly decreased the annual asthma exacerbation rate compared with placebo at week 48 Rate ratio versus placebo - Q4W was 0.55 (95% CI 0.42–0.71; p<0.0001) - Q8W was 0.49 (0.37–0.64; p<0.0001)

• During the 48-week period, the curves for the cumulative number of exacerbations in the benralizumab treated and placebo cohorts diverged as early as 4 weeks
• Additionally, the time to first asthma exacerbation was longer for both

• Among those with baseline blood eos > 300 - q 4 or 8 wk regimen --> reduced exacerbation rate & improved prebronchodilator FEV1 - q 8 wk regimen --> improved symptoms
Bleecker ER, et al.Lancet 2016; 388: 2115–27
Confirm the efficacy and safety of benralizumab for patients with severe asthma and elevated eosinophils, which are uncontrolled by
high-dosage ICS plus LABA, and provide support for benralizumab to be an additional option to treat this disease in this patient population

J.B. Bice et al. / Ann Allergy Asthma Immunol 112 (2014) 108e115.
• Lebrikizumab : fully humanized IgG4 mAb that binds to IL-13
• Tralokinumab : human monoclonal IgG4, which potently and specifically neutralizes IL-13
Anti IL-13

Lebrikizumab
Downstream production of periostin by bronchial epithelial cells acting on fibroblasts, ultimately resulting in mucus production,
goblet cell hyperplasia, myeloblast differentiation, smooth muscle cells contraction, airway remodeling, and airway
hyperresponsiveness

LAVOLTA I, II
• P : 1081 patients in LAVOLTA I 1067 patients in LAVOLTA II - Age 18–75 years with uncontrolled asthma, pre-bronchodilator FEV 1 40–80% predicted, bronchodilator response of at least 12%, and on stable background therapy with inhaled corticosteroids (500–2000 µg per day fluticasone propionate or equivalent) for at least 6 months and at least one additional controller medication
Randomised, multicentre, multinational, double-blind, placebo-controlled trials
Hanania NA, et al.Lancet Respir Med 2016; 4: 781–96
• I, C : Randomly assigned (1:1:1) 1.) Lebrikizumab 37.5 mg 2.) Lebrikizumab 125 mg 3.) Placebo subcutaneously once every 4 weeks x 52 weeks • O : Primary efficacy endpoint --> rate of asthma exacerbations during
the 52-week placebo-controlled period in biomarker-high patients (periostin ≥50 ng/mL or blood eosinophils ≥300 cells per µL, and including patients high in both)
Secondary efficacy endpoints --> absolute change in pre- bronchodilator FEV 1 from baseline at week 52; time to first asthma exacerbation; rate of urgent asthma- related health-care use; AQLQ(S); ACQ-5

Rate of asthma exacerbations over 52 weeks by biomarker group
Lebrikizumab did not consistently show significant reduction in asthma exacerbations in biomarker-high patients

Tralokinumab
• P : 452 severe uncontrolled asthma (age 18-75 yr), with 2-6 exacerbations in past year
Randomised, double-blind, placebo-controlled, parallel-group, multicentre, phase 2b study at 98 sites in North America,
South America, Europe, and Asia
Brightling CE. Lancet Respir Med 2015; 3: 692–701

• I, C : Randomly assigned (1:1:1) 1.) tralokinumab SC q 2 wk (over 1 yr) , n=150 2.) tralokinumab SC q 2 wk for 12 wk, then q 4 wk , n=151 3.) placebo , n=151
• O : Primary endpoint --> annual exacerbation rate ratio versus placebo at 52 week in the intention-to-treat population Secondary endpoints --> prebronchodilator FEV 1 and Asthma Control Questionnaire-6 (ACQ-6), and Asthma Quality of Life Questionnaire– Standardised Version (AQLQ[S])
Brightling CE. Lancet Respir Med 2015; 3: 692–701

Prebronchodilator FEV1 was increased for tralokinumab q 2 wk, but not q 4 wk
Brightling CE. Lancet Respir Med 2015; 3: 692–701
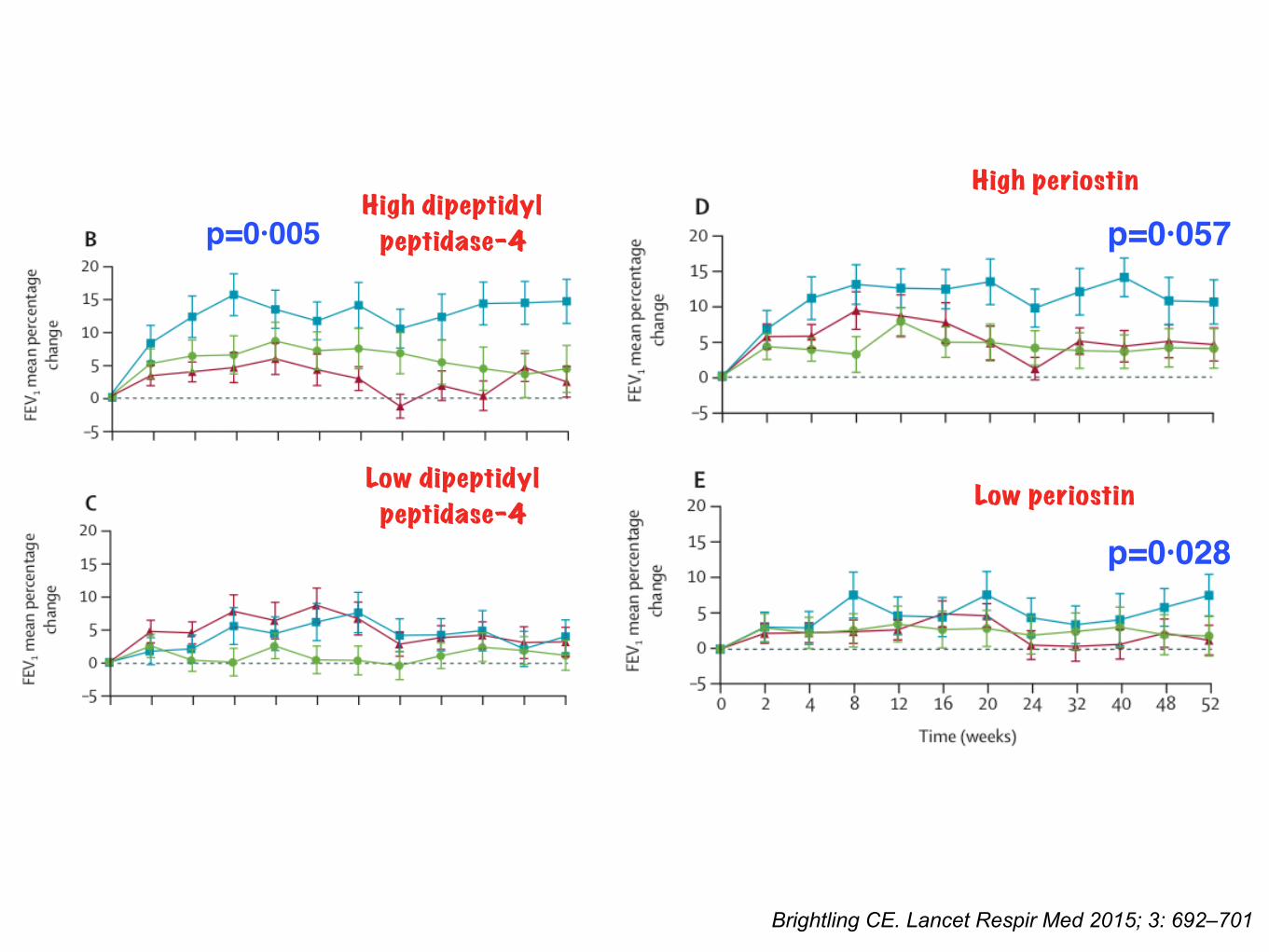
High dipeptidyl peptidase-4
Low dipeptidyl peptidase-4
High periostin
Low periostin
Brightling CE. Lancet Respir Med 2015; 3: 692–701
p=0·005 p=0·057
p=0·028

Tralokinumab did not reduce exacerbation rate in patients with severe uncontrolled asthma - Improvement in FEV1 in defined subgroups - Potential utility of DPP-4 & periostin as biomarkers of IL-13 pathway activation

J.B. Bice et al. / Ann Allergy Asthma Immunol 112 (2014) 108e115.

• Dupilumab : fully human monoclonal antibody to the alpha subunit of the IL-4 receptor
Anti IL-4 receptor alpha

Randomized, double-blind, placebo-controlled, parallel-group phase 2A study was conducted at
28 sites in the United States
Wenzel S, et al. N Engl J Med 2013;368:2455-66.
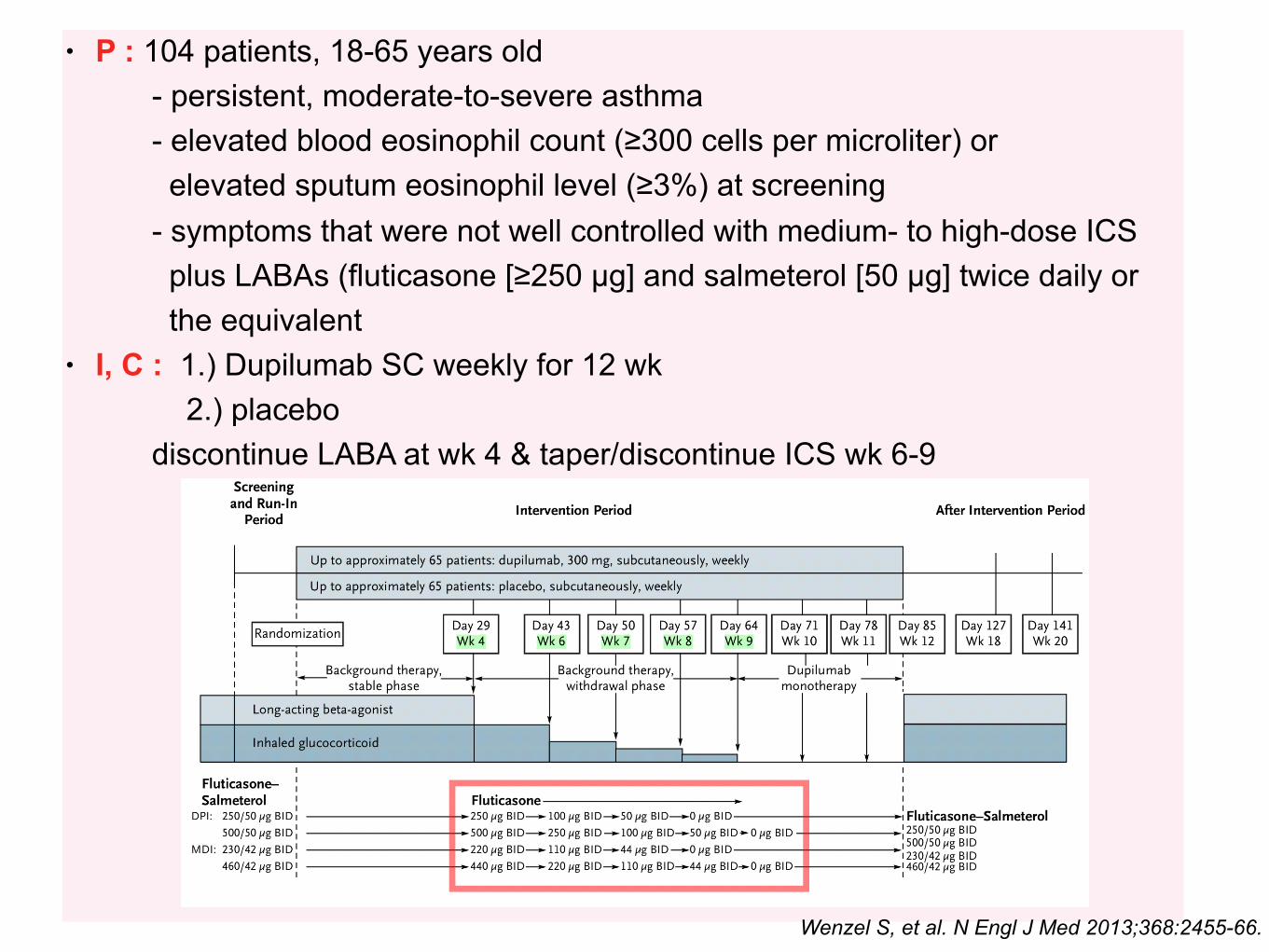
• P : 104 patients, 18-65 years old - persistent, moderate-to-severe asthma - elevated blood eosinophil count (≥300 cells per microliter) or elevated sputum eosinophil level (≥3%) at screening - symptoms that were not well controlled with medium- to high-dose ICS plus LABAs (fluticasone [≥250 µg] and salmeterol [50 µg] twice daily or the equivalent • I, C : 1.) Dupilumab SC weekly for 12 wk 2.) placebo discontinue LABA at wk 4 & taper/discontinue ICS wk 6-9
Wenzel S, et al. N Engl J Med 2013;368:2455-66.

• O : - Exacerbation --> 87% reduction with dupilumab - Improvements for most measures of lung function & asthma control
Wenzel S, et al. N Engl J Med 2013;368:2455-66.

In patients with moderate-to-severe asthma & elevated eosinophil who used ICS + LABA, dupilumab was
associated with fewer exacerbations when LABA & ICS were withdrawn, with improved lung function & reduced
levels of Th2- associated inflammatory markers
Wenzel S, et al. N Engl J Med 2013;368:2455-66.

Muraro et al.PRACTALL consensus report. J Allergy Clin Immunol 2016;137:1347-58.
Conclusions

Thank you
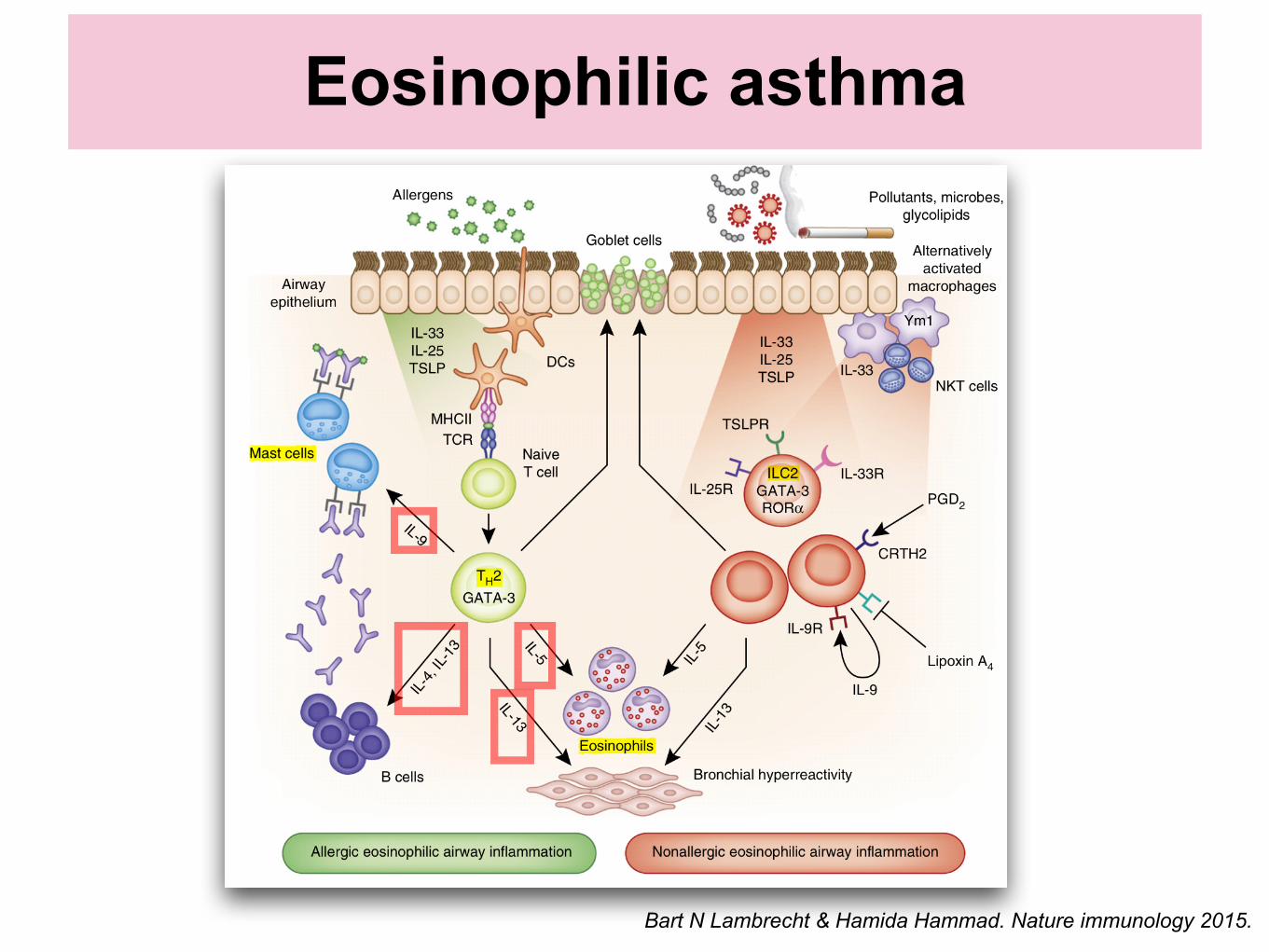
Eosinophilic asthma
Bart N Lambrecht & Hamida Hammad. Nature immunology 2015.

Monoclonal Ab

Tan et al.Journal of Asthma and Allergy 2016:9 Pelaia et al. Therapeutics and Clinical Risk Management 2016:12 1075–1082.

Molecular mechanisms and signaling pathways activated by IL-5 in eosinophils
Pelaia et al. Therapeutics and Clinical Risk Management 2016:12 1075–1082.