
Student Must See
44
Complete right-sided pneumothorax Lung is compressed against mediastinum Shift of heart and trachea to left Tension pneumothorax
-
Upload
lettasamudra -
Category
Documents
-
view
217 -
download
0
description
semoga bermanfaat
Transcript of Student Must See

Complete right-sided
pneumothorax
Lung is compressed
against mediastinum
Shift of heart and trachea to
left
Tension pneumothorax

Pneumomediastinum
Streaky, linear densities due
to air in the mediastinumStreaky, linear
densities due to air in the mediastinum

Pneumomediastinum – CT scan
Air surrounding esophagus in mediastinum
Extraluminal contrast from
perforation along left
lateral wall of distal
esophagus

Pneumoperitoneum
Air outlines under surface of left hemidiaphragm
Air outlines under surface of
right hemidiaphragm

Pneumoperitoneum
Air outlines both sides of the wall of the stomach-a sign of free air in
the peritoneal cavity

Pneumoperitoneum - CT
CT scans on 2 different people show a small and large amount of free air in the peritoneal cavity which rises to the highest point (anterior abdomen with the
person lying on their back) and is not contained within bowel
Free airFree air
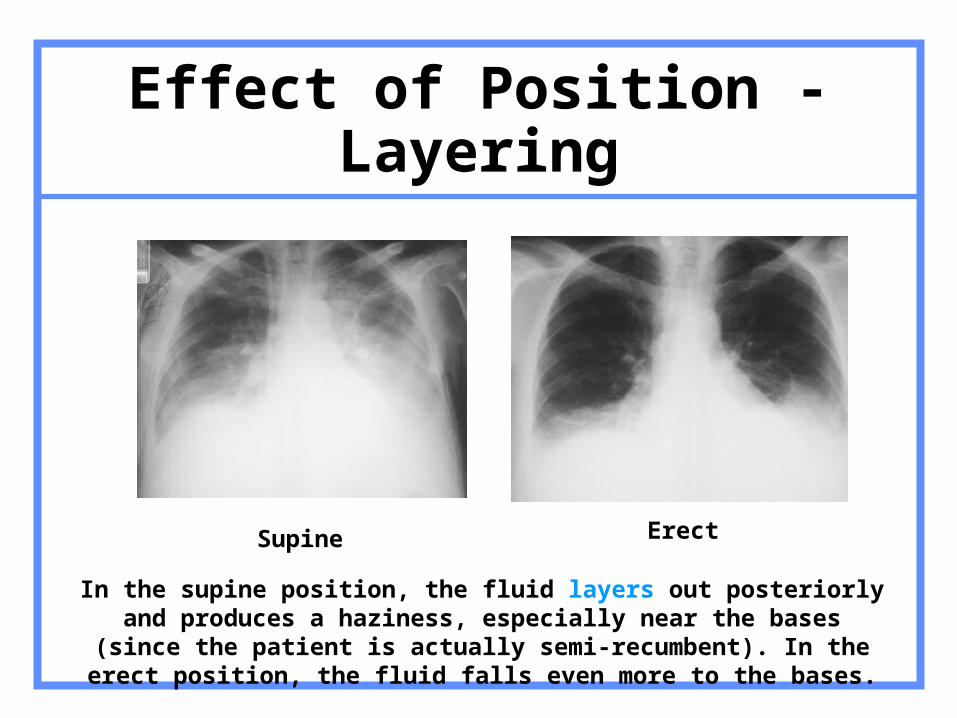
Effect of Position - Layering
Supine Erect
In the supine position, the fluid layers out posteriorly and produces a haziness, especially near the bases (since the patient is actually semi-
recumbent). In the erect position, the fluid falls even more to the bases.

Pulmonary Venous Hypertension from Mitral Stenosis
Size (not number) of vessels at the apex exceeds size of vessels at the base in this upright person. This is called “cephalization.” Normally the vessels at the base exceed the size of the vessels at the apex

Pulmonary Interstitial Edema
Pulmonary interstitial edema produced by Kerly A and C lines

Pulmonary Alveolar Edema
Bilateral, diffuse airspace disease more marked centrally than at the periphery of the lung (“bat-wing appearance”)

Aortic Dissection
Linear lucency in the contrast-filled descending aorta is the intimal flap of an aortic dissection

Aortic Dissection
• Widened mediastinum
• Left pleural effusion
• Chest pain
Should make you think of an aortic dissection

Classification of Dissecting Aneurysms
Stanford classification
• Widened mediastinum
• Left pleural effusion
• Chest pain

Aortic rupture
Red arrows point to active extravasation of contrast from the aorta into the retroperitoneum
Thrombus inside the lumen of the aorta
Red arrows point to active extravasation of contrast from the aorta into the retroperitoneum
AortaAorta

Ruptured Aortic Aneurysm
Enlargement of abdominal aorta > 3cm Usually 2 to atherosclerosis Below renals, above iliacs
About 20-25% rupture <4cm~10%; >10 cm~60% Retroperitoneal, usually on left Into GI tract: massive hemorrhage Into IVC: rapid cardiac decompensation
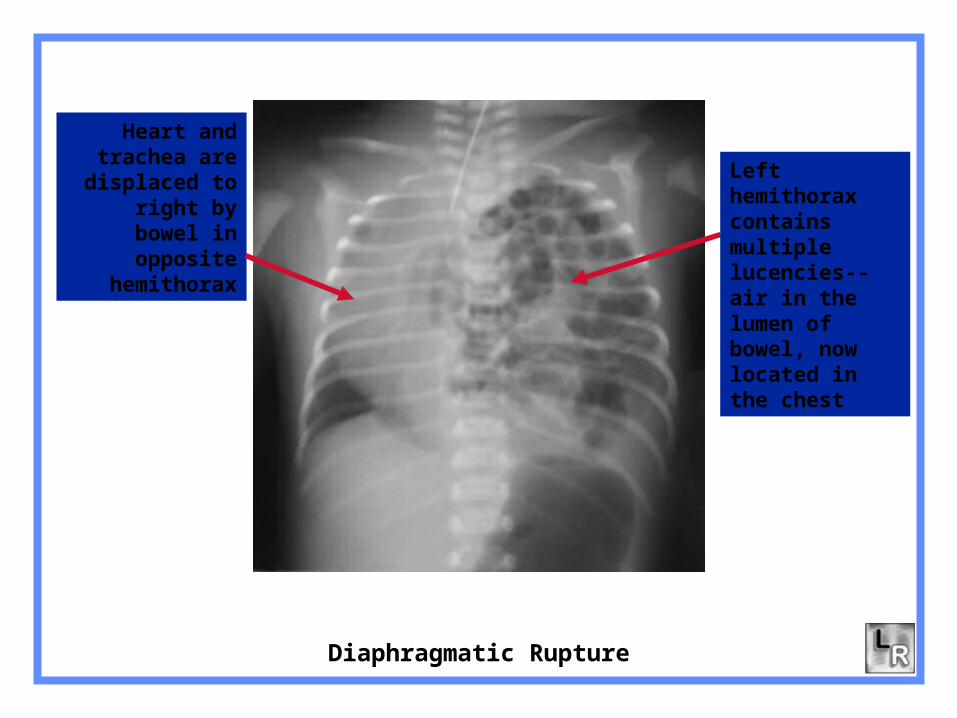
Diaphragmatic Rupture
Left hemithorax contains multiple lucencies--air in the lumen of bowel, now located in the chest
Heart and trachea are
displaced to right by bowel in
opposite hemithorax

Diaphragmatic RuptureGeneral
5% of all diaphragmatic hernias Most (90%) are left-sided
Central and posterior >10cm in length Contain stomach, colon, small bowel,
omentum, spleen
Half have no initial abnormal radiographic findings
Half are missed clinically

36 year-old with acute abdominal pain. Why?

Small Bowel Obstruction
Multiple air-containing and dilated loops of
small bowel
No gas in rectosigmoid
Multiple air-fluid levels
in small bowel

Sigmoid Volvulus
Sigmoid twists around this point
Obstructed, dilated sigmoid has a “coffee-bean” shape

Cecal Volvulus
Dilated loop in LUQ is cecum which has twisted on itself
Dilated loops of small bowel from small bowel obstruction at ileocecal valve

Sigmoid Volvulus – Barium Enema
Cecum twists at this point
producing “Bird’s-Beak”
sign

74 year-old with change of bowel habits

Large bowel obstruction – Sigmoid carcinoma
Dilated loops of large bowel with abrupt cut-off in
sigmoid
Barium enema shows annular constricting carcinoma of sigmoid producing obstruction
Rectum
Dilated large bowel

Ascites
Ascites
Ascites is lower in attenuation than adjacent, contrast-enhanced liver

R3
Massive ascites on CT
Massive ascites (red arrows) in a patient
with a pseudocyst of the pancreas (green
arrow)

R3
Tip of central venous catheter coils back on itself in right brachiocephalic vein (red arrow).

Tip of endotracheal tube is in right mainstem bronchus (red arrow) leading to atelectasis of the right upper lobe and entire
left lung

Traumatic intracranial hemorrhageEpidural Hematoma
Crescentic area of increased attenuation on non contrast-enhanced CT with convexity toward brain is characteristic of an epidural hematoma

Traumatic intracranial hemorrhage Subdural hematoma
Crescentic low attenuation lesion at periphery of brain containing a fluid-fluid level from blood

Traumatic intracranial hemorrhage Intraparenchymal hemorrhage
Intraparenchymal hemorrhage

Subarachnoid hemorrhage from ruptured aneurysm
R3 R3
Acute hemorrhage in the basilar cisterns (red arrows) and Sylvian fissures (green arrows) in two patients with ruptured aneurysms

Colloid Cyst of 3rd ventricle producing obstructive hydrocephalus
R3
Markedly enlarged
frontal horns Colloid Cyst obstructing third ventricle
Choroid plexus (normal)

Hydrocephalus from Choroid Plexus Papilloma
R3
Lateral ventricles – anterior and
posterior horns
Large mass represents a choroid plexus papilloma

Hydrocephalus from Cerebral Atrophy
Lateral ventricles – anterior and
posterior horns

58 year-old woman with breast cancer and headache
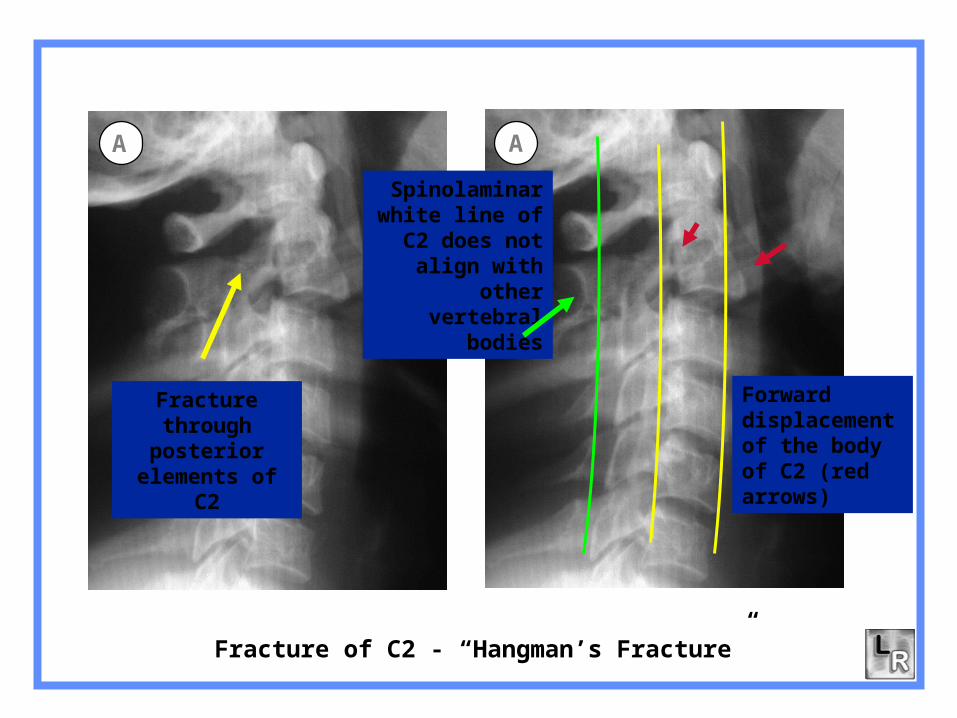
Fracture through posterior
elements of C2
Forward displacement of the body of C2 (red arrows)
Spinolaminar white line of C2
does not align with other
vertebral bodies
Fracture of C2 - “Hangman’s Fracture”
A A

Hangman’s Fracture
l Most common fracture of C2 n Most common cervical spine fracture
l Hyperextension/compression fracture
l Fractures through the pedicles of C2 with anterior slip of C2 on C3
l Not associated with neuro deficit

Locked facets
The inferior
articular facet of
C5 (red arrow) has
slipped forward
and lies anterior to
the superior
articular facet of
C6 (green arrow)
— a condition
known as a
“locked facet”
C5
C6
B

Fractures of the metaphysis (red arrow) and epiphysis (green arrow) (Salter-Harris IV) extend into joint
Fracture of radial styloid (yellow arrows) extends into wrist joint5
Fractures extending into joints

Posterior “fat-pad sign” indicates fluid in the joint
Fracture of radial head
Fracture of the radial head with traumatic joint effusion
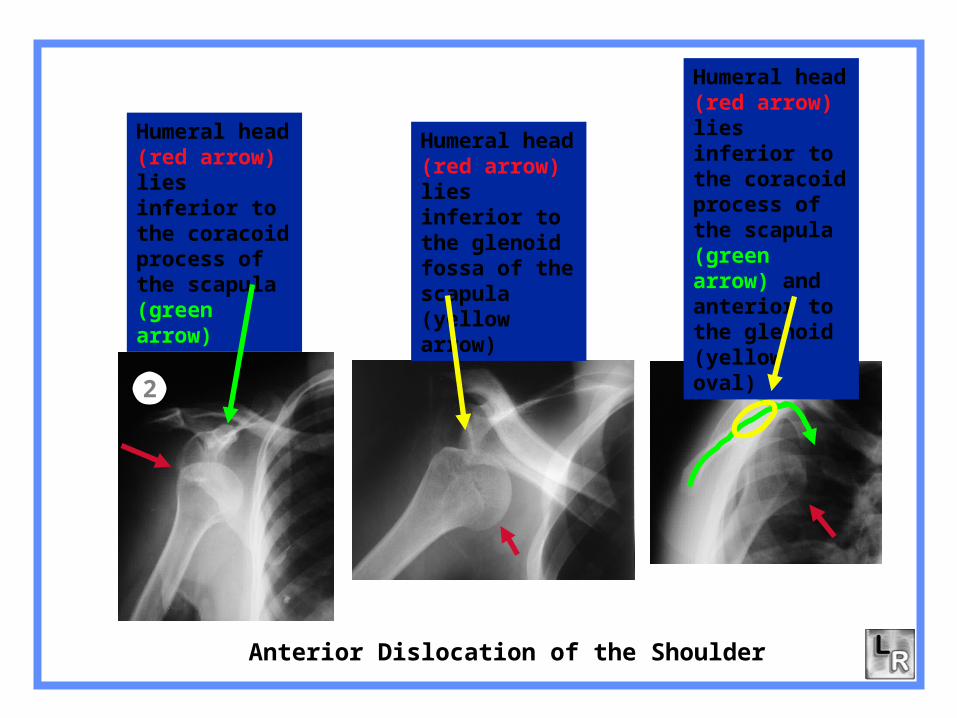
Anterior Dislocation of the Shoulder
2
Humeral head (red arrow) lies inferior to the coracoid process of the scapula (green arrow)
Humeral head (red arrow) lies inferior to the glenoid fossa of the scapula (yellow arrow)
Humeral head (red arrow) lies inferior to the coracoid process of the scapula (green arrow) and anterior to the glenoid (yellow oval)

Posterior Dislocation of the Shoulder
1
Humeral head (red arrow) lies posterior to the glenoid fossa of the humerus (yellow arrow)
Humeral head (red arrow) lies beneath the acromion process of the scapula (green arrow) and posterior to glenoid (yellow oval)
Humeral head (red arrow) assumes the shape of a “lightbulb” because it is fixed in internal rotation



















