Stuart Weatherby Consultant Neurologist Derriford Hospital. Plymouth.
42
Stuart Weatherby Consultant Neurologist Derriford Hospital. Plymouth
-
Upload
imogene-price -
Category
Documents
-
view
225 -
download
3
Transcript of Stuart Weatherby Consultant Neurologist Derriford Hospital. Plymouth.

Stuart WeatherbyConsultant Neurologist
Derriford Hospital. Plymouth

David Hartley, Treaty of Paris
William Wilberforce
John Venn
Amy Johnson

Factors that may affect use, or apparent efficacy of migraine prophylaxis
Factors predicting chronic painThe patient. The doctor
Principles of prophylaxis How to choose First line, Second line, third line Magnitude of effects Herbal Psychological Injection- Acupuncture and
Botox
When should I give prophylaxis?
What prophylaxis should I give?
What benefit should my patient expect?


Fear -central role in the duration of pain Through medial prefrontal region, ventral lateral
frontal region, and cingulate regions
Anxiety and depression may also be markers for CNS chemical changes that play a significant role in the duration of pain.
Between 30-50% of people with chronic daily headache can become depressed
Catastrophizing more than 7 times more powerful a predictor than any other predictor or clinical variable among acute back pain patients in determining the risk of subsequent chronic pain

‘Its all part of a ‘chronic pain syndrome’’ ‘They have pain because they are
depressed’ ‘They don’t respond to anything’ ‘Analgesic overuse’ ‘Cold feet’ or is it secondary headache

Prophylaxis is used to reduce the number of attacks in circumstances when acute therapy, used appropriately, gives inadequate symptom control.

Frequent headaches (more than 2 per week) Attack duration > 48 hours Severity is extreme Migraine attacks with prolonged aura Unacceptable adverse effects occur with acute
treatment Substantially interferes with the patient’s daily
routine, despite acute treatment Special circumstances such as hemiplegic
migraine or attacks with a risk of permanent neurologic injury
Patient preference

Most prophylactics are used within a dose range, and in general must be up-titrated slowly to an effective dose (or to the maximum dose) in order to avoid side-effects that will precipitate premature discontinuation.
This can lead to a delay in efficacy which itself, unfortunately, sometimes triggers discontinuation
Tell patient it takes ages to get to a therapeutic dose

Migraine is cyclical: treatment is required for periods of exacerbation.
Uninterrupted prophylaxis over very long periods is rarely appropriate.
If effective continue for 4-6 months, then gradual withdrawal to establish continued need.
In absence in the absence of unacceptable side-effects, 6-8 weeks is a reasonable trial

The criteria for preferring one prophylactic drug to another
are based upon: • evidence of efficacy; • comorbidity • contraindications,
including risks in pregnancy;
Also good evidence that poor compliance is a major factor and that once-daily dosing is preferable.

The formal evidence-base for efficacy is good for:-
Betablockers, Topiramate Valproate
Adequate for amitriptyline
Poor for other prophylactics


Cardioselectivity and hydrophilicity both improve the side-effect profile
On this basis, atenolol 25-100mg bd might be preferred over metoprolol 50-100mg bd and over propranolol LA 80mg od-160mg bd.

First-line when migraine coexists with: • Tension-type headache • Another chronic pain condition; • Disturbed sleep; • Depression
Desipramine*, nortriptyline* and protriptyline* are less sedative alternatives

Valproate 300-1000mg bd
Does not affect hormonal contraception.
Adverse events
Weight gain and alopecia. Blood cell count, platelet count,
bleeding time and coagulation tests are recommended
prior to starting treatment and in case of spontaneous
bruising or bleeding. Liver dysfunction is reported rarely.
Topiramate 25mg od-50mg bd (can go 100mg bd)Enzyme-inducer and can reduce the efficacy of COCP
50% ‘pins and needles’,Usually resolve with continued use.25% relative anorexia and loss of 10% of body weight, 15% cognitive dysfunction. Kidney stonesDepressionSecondary angle-closure glaucoma has been reportedDiscontinuation 22% topiramate vs 11% placeboPretend they have epilepsy

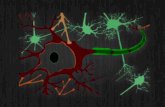
Migraine- Subclinical structural brain changes and persistent alteration of pain perception
In some cases correlated with the duration of the diseaseFrequency of attacks might play a role in the transformation of episodic migraine to chronic
Anticonvulsants- Increase activation threshold resulting in neuronal
stabilisation and cortical neurons hyperexcitability, electrophysiological feature underlying the pathogenesis of epilepsy and migraine.

Gabapentin* 300mg od-800mg tds
Betablockers and Amitryptiline together
Flunarizine
Methysergide 1-2mg tds Beware retroperitoneal fibrosis, 5HT
agonist activity/rebound headache/drug holidays

(Verapamil)
Flunarizine 808 pts Flunarizine vs Propranolol Responders (50% reduction), 5mg:46%. 10mg:53%.
Propranolol:48% Drop out due to adverse effects
5mg:16.7%. 10mg: 19.3%. Propranolol:16.7% HC Deiner et al Cephalalgia 2002;22:209-221
Flunarizine blocks voltage-gated Na(+) and Ca(2+) currents in cultured rat cortical neurons: A possible locus of action in the prevention of migraine.
Neurosci Lett. 2011 Jan 10;487(3):394-9.

Pizotifen- little Clonidine- little Pregabalin Verapamil* MR 120-240mg bd has limited
clinical-trials. Headache is sometimes a side-effect. Lisinopril montelukast Candesartan riboflavin and co-enzyme Q10 some
evidence Lamotrigine Zonisamide Levetiracetam Placebo controlled trial 96 pts, Resistant pts. Median duration
20 yrs. Poss trend to effect. Small subpopulation who benefit? Worse mental health on keppra.
Beran Cephalalgia November 8, 2010-


50% resp No. Studies
Participants
OR CI
First cross-over
4 205 1.72 1.23, 2.40
Pooled cross-over
9 668 1.94 1.61, 2.35
Cochrane Database of Systematic Reviews 2004, Issue 2
Compared with placebo or other drugs in 58 trials. 5072 participants
26 placebo controlled trials
Unclear whether effects persist after stopping propranolol.
Drug comparisons did not yield any clear-cut differences. Sample size was, however, insufficient in most trials to establish equivalence.

48 50
0
10
20
30
40
50
60
70
Flunarizine (p<0.01) Propranolol (p<0.0005)
No. of attacks reduced by more than 50%
% o
f Pat
ient
s
Headache 1989; 29: 218-223

Drug No. studies No pt OR CI
Valpr 4 454 3.34 1.46, 7.67
Gabapentin 1 87 4.67 1.54, 14.14
Topiramate 6 898 3.34 2.36, 4.73
Chronicle E, Mulleners Cochrane Database Syst Rev. 2004;(3)
Anticonvulsants, (cf placebo) as a class:- Data from 2024 patients
-Reduce migraine frequency- 8 trials (n = 841), 1.4 attacks per 28 days (CI -0.93 to -0.26).
No. of pts reduced migraine freq by 50% or more (cf placebo)- 10 trials (n = 1341)
OR 3.90; 95% CI 2.61 to 5.82; NNT 3.8; 95% CI 3.2 to 4.6
NNHs for various clinically important adverse events:-Valproate from 6.6 to 16.3.Topiramate from 2.4 to 32.9.

Topiramate significantly reduced the mean number of monthly migraine days (±SD) by 3.5 ± 6.3, compared with placebo (−0.2 ± 4.7, P < 0.05)
78% analgesic overuse at baseline Bussone... Goadsby TOP CHROME study 2007 Cephalagia , 27 (7) , 814 – 823
Diener, Dodick, Goadsby et al Cephalalgia October 2009 vol. 29 no. 10 1021-1027

Feverfew 5 trials, 343 pts. Can contain carcinogens. Not
conclusive Pittler MH, Ernst E. Feverfew for preventing migraine. Cochrane database of systematic reviews 2004: CD002286.5
170 pts placebo control. Logistic regression of responder rates OR 3.4, P = 0.0049, in favour of feverfew extract Diener et al Cephalalgia 2005 vol. 25 no. 11 1031-1041
Butterbur 245 pts Proportion with ≥50% reduction 68% for
75-mg and 49% for the placebo arm (p < 0.05). Burping and ?carcinogens in european preparations?
Lipton RB, et al Neurology 2004; 63:2240–2244.

Melatonin. Open label 3mg at night helps Neurology 2004;
63:757.
Placebo control 46 pts negative. Neurology 2010 vol. 75 no. 17 1527-1532
Co Q 10
Riboflavin, Magesium- some class B evidence

Grade A evidence: Relaxation training Biofeedback combined with relaxation training Electromyographic biofeedback Cognitive-behavioral therapy. Silberstein SD for the US Headache Consortium. (2000)
www.neurology.org/cgi/reprint/55/6/754.pdf.
Psychological therapies for the management of chronic pain (excluding headache) in adults
40 studies (4781 pts). ‘Weak effects in improving pain. Minimal effects on disability associated with chronic
pain. Effective in altering mood outcomes, and evidence these
changes maintained at six months Cochrane Database of Systematic Reviews 2009, Issue 2.

Psychological therapies for the management of chronic and recurrent pain in children and adolescents
29 studies 1432 pts. 20 were for headache. (OR) of 5.51 (CI 3.28 to 9.24, P < 0.05) NNT = 2.57 (CI 2.2 to 3.13) At follow-up, the OR was 9.91 (95% CI 3.73 to 26.33),
P < 0.05) NNT = 1.99 (CI 1.63 to 2.72. ‘Psychological treatments are effective in pain control
for children with headache and benefits appear to be maintained’
Cochrane Database of Systematic Reviews 2009, Issue 2. Art. No.: CD003968




22 trials, 4419 pts Benefit to treatment
of acute migraine attacks only or to routine care.
No evidence for an effect of 'true' acupuncture over sham interventions.
Cochrane Database Syst Rev. 2009 Jan 21;(1):CD001218.

GONI/operations- covered later
Medication overuse- covered later Menstrual migraine- covered later


Men or women aged 18 to 65 years1
Headache occurring 15 days/4 weeks,3 with each day consisting of 4 hours of continuous headache and 50% of baseline headache days being migraine days1*
≥4 distinct headache episodes/4 weeks, with each episode consisting of 4 hours of continuous headache1 Patients overusing acute medications were not
excludedOnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial Cephalalgia July 1, 2010 30: 793-803 OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial Cephalalgia July 1, 2010 30: 804-814
*Migraine days or probable migraine days. Migraine defined by ICHD-II 1.1, 1.2, and 1.6.

p<0.001
Nearly 70% of patients treated with BOTOX® throughout the entire study experienced ≥50% reduction in migraine days from baseline at Week 56 (67.8% vs. 59.6% for placebo; p=0.018)3
Mean ± standard error.The double-blind phase included 688 subjects in the BOTOX® group and 696 in the placebo group. Migraine days at baseline: 19.1 BOTOX® group vs 18.9 placebo group, p=0.328.
1. Dodick DW et al. Headache 2010;50:921–936.2. Aurora SK et al. Presented at IHC 2009.3. Allergan Data on File – 50% responder rate at Week 56.
Mea
n c
han
ge
in f
req
uen
cy m
igra
ine
day
s fr
om
bas
elin
e (d
ays/
28-d
ay p
erio
d)
52484440363228241612840
Study week
020 56
-2
-4
-6
-8
-10
-12
-14
BOTOX® (n=688)
Placebo (n=696)
p=0.018
p=0.01
p=0.024
p=0.013p=0.003
p=0.006p=0.003
p<0.001
p<0.001p<0.001
p<0.001
p<0.001
Double-blind phase:BOTOX® vs. placebo
Open-label phase:All patients on BOTOX®
Mea
n c
han
ge
in f
req
uen
cy o
f m
igra
ine
day
s fr
om
bas
elin
e (d
ays/
28-d
ay p
erio
d)
p<0.001

1. Coeytaux RR et al. J Clin Epidemiol 2006;59:374–380.2. Dodick DW et al. Headache 2010;50:921–936.3. Allergan Data on File – HIT-6 Scores (56 weeks).
*Between-group difference exceeded the minimally important difference (MID) for HIT-6 (2.3 units) indicating a clinically significant effect of BOTOX® treatment.1 The double-blind phase included 688 subjects in the BOTOX® group and 696 in the placebo group. Total HIT-6 scores at baseline: 65.5 BOTOX® group vs 65.4 placebo group; p=0.638.
*Between-group difference exceeded the minimally important difference (MID) for HIT-6 (2.3 units) indicating a clinically significant effect of BOTOX® treatment.1 The double-blind phase included 688 subjects in the BOTOX® group and 696 in the placebo group. Total HIT-6 scores at baseline: 65.5 BOTOX® group vs 65.4 placebo group; p=0.638.
p<0.001
p<0.001
483628242012840
Weeks
016 56
-2
-3
-5
-6
-8
-9
BOTOX®
Placebo
p<0.001
p<0.001p<0.001
p<0.001
Double-blind phase:BOTOX® vs. placebo
Open-label phase:All patients on BOTOX®
-7
-4
-1
Ch
ang
e fr
om
bas
elin
e in
tota
l H
IT-6
sco
re
p=0.069p=0.022p=0.002
p=0.002
2.4*

Factors that may affect use, or apparent efficacy of migraine prophylaxis
Factors predicting chronic painThe patient. The doctor
Principles of prophylaxis How to choose First line, Second line, third line Magnitude of effects Herbal Psychological Injection- Acupuncture and
Botox
When should I give prophylaxis?
What prophylaxis should I give?
What benefit should my patient expect?


High rates of FMS in chronic migraine Peres (Neurology 2001)
FMS in 36% of patients with primary headacheThose with comorbid FMS had highest level of
migraine severity DeTommaso et al (Cephalagia 2008)
Patients with FMS show increased sensitivity to various stimuli, with abnormal central pain mechanism and augmented pain experience.
Suggestion episodic migraine, chronic daily headache and FMS are continuum of the same disorder
Peres (Current Neurol Neuroscience Rep 2003) and Centonze (Neurol Sci 2004)

Reduction in attack frequency Reduction in attack intensity / severity Decrease in migraine-induced disability % of patients with >50% reduction in
attack frequency