Stroke Nursing

of 64
Transcript of Stroke Nursing
-
8/7/2019 Stroke Nursing
1/64
-
8/7/2019 Stroke Nursing
2/64
2009, American Heart Association. All rights reserved.
A Comprehensive Overview of Nursing andA Comprehensive Overview of Nursing and
Interdisciplinary Care of the Acute IschemicInterdisciplinary Care of the Acute Ischemic
Stroke Patient, A Scientific Statement FromStroke Patient, A Scientific Statement Fromthe American Heart Associationthe American Heart Association
Debbie Summers, MSN, RN, FAHA, Chair; Anne Leonard, MPH, RN,
FAHA, Co-Chair; Deidre Wentworth, MSN, RN; Jeffrey L. Saver, MD,
FAHA; Jo Simpson, BSN, RN; Judy Spilker, BSN, RN; Nanette Hock,MSN, RN, FAHA; Elaine Miller, DNS, RN, FAHA;
Pamela H. Mitchell, PhD, RN, FAHA.
On behalf of the American Heart Association Council on
Cardiovascular Nursing and the Stroke Council.
-
8/7/2019 Stroke Nursing
3/64
2009, American Heart Association. All rights reserved.
This slide set was developed andThis slide set was developed andedited by Anne Leonard RN,edited by Anne Leonard RN,
MPH, and Debbie Summers, RN,MPH, and Debbie Summers, RN,MSN, APRN on behalf of theMSN, APRN on behalf of thewriting group.writing group.
-
8/7/2019 Stroke Nursing
4/64
2009, American Heart Association. All rights reserved.
Applying the Evidence
This writing panel applied the Rules ofThis writing panel applied the Rules of
Evidence and formulation of strength ofEvidence and formulation of strength ofevidence (recommendations) used by otherevidence (recommendations) used by otherAmerican Heart Association (AHA) writingAmerican Heart Association (AHA) writinggroups (Table 1). We also crossgroups (Table 1). We also cross--reference otherreference otherAHA guidelines as appropriate.AHA guidelines as appropriate.
-
8/7/2019 Stroke Nursing
5/64
2009, American Heart Association. All rights reserved.
-
8/7/2019 Stroke Nursing
6/64
2009, American Heart Association. All rights reserved.
Overview of StrokeOverview of Stroke A majorA majorPublic Health ProblemPublic Health Problem
About 85% of strokes are ischemic, andAbout 85% of strokes are ischemic, and
about 15% are hemorrhagic.about 15% are hemorrhagic.
Approximately 795,000 strokes occur eachApproximately 795,000 strokes occur each
year.year.
Stroke is the 3Stroke is the 3rdrd leading cause of death in theleading cause of death in the
US, and the first cause of death worldwide.US, and the first cause of death worldwide. Stroke is a leading cause of adult disability.Stroke is a leading cause of adult disability.
The cost of stroke in the US is over 68 billionThe cost of stroke in the US is over 68 billion
dollars annually.dollars annually.
-
8/7/2019 Stroke Nursing
7/64
2009, American Heart Association. All rights reserved.
Demographics of StrokeDemographics of Stroke
Women have about 60,000 more strokesWomen have about 60,000 more strokesthan men.than men.
Native Americans have the highestNative Americans have the highestprevalence.prevalence.
African Americans have almost twice theAfrican Americans have almost twice therate compared to Caucasians.rate compared to Caucasians.
Hispanics have slightly higher ratesHispanics have slightly higher ratescompared to noncompared to non--Hispanic whites.Hispanic whites.
Modifiable risk factors must beModifiable risk factors must beaddressed in our aging population withaddressed in our aging population withthe propensity to stroke.the propensity to stroke.
-
8/7/2019 Stroke Nursing
8/64
2009, American Heart Association. All rights reserved.
Nursing and StrokeNursing and Stroke
Nurses play a pivotal role in theNurses play a pivotal role in the
care of stroke patients.care of stroke patients. This paper includes nursing careThis paper includes nursing caredirected in two phases of the acutedirected in two phases of the acutestroke experience:stroke experience:
The emergent or hyperacute phaseThe emergent or hyperacute phase The acute phaseThe acute phase
-
8/7/2019 Stroke Nursing
9/64
2009, American Heart Association. All rights reserved.
Nursing Care of the Stroke PatientNursing Care of the Stroke Patient
Stroke is a complex disease requiringStroke is a complex disease requiring
the efforts and skills of thethe efforts and skills of themultidisciplinary team.multidisciplinary team.
Nurses are often responsible for theNurses are often responsible for thecoordination of that care.coordination of that care.
Coordinated care can result in:Coordinated care can result in:improved outcomes, decreased LOS,improved outcomes, decreased LOS,translating to decrease costs.translating to decrease costs.
-
8/7/2019 Stroke Nursing
10/64
2009, American Heart Association. All rights reserved.
Definition of StrokeDefinition of Stroke
Ischemic strokeIschemic stroke
Caused by a blocked blood vessel inCaused by a blocked blood vessel inthe brain.the brain.
Hemorrhagic StrokeHemorrhagic Stroke
Caused by a ruptured blood vessel inCaused by a ruptured blood vessel in
the brain.the brain.
-
8/7/2019 Stroke Nursing
11/64
2009, American Heart Association. All rights reserved.
Etiology of Ischemic StrokesEtiology of Ischemic Strokes
20% caused by large vessel atherothrombotic20% caused by large vessel atherothrombotic
causes (intracranial or carotid artery).causes (intracranial or carotid artery). 25% caused by small vessel disease25% caused by small vessel disease
(penetrating artery disease).(penetrating artery disease).
20% caused by cardiac sources20% caused by cardiac sources
(cardioembolism)(cardioembolism) 30% from unknown causes.30% from unknown causes.
-
8/7/2019 Stroke Nursing
12/64
2009, American Heart Association. All rights reserved.
Risk factors for Ischemic StrokeRisk factors for Ischemic Stroke
HypertensionHypertension
DiabetesDiabetes
Heart DiseaseHeart Disease
SmokingSmoking
High CholesterolHigh Cholesterol
Male genderMale gender AgeAge
Ethnicity/RaceEthnicity/Race
-
8/7/2019 Stroke Nursing
13/64
2009, American Heart Association. All rights reserved.
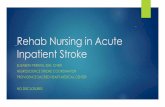
CT Scan Right Occipital/ParietalInfarction
-
8/7/2019 Stroke Nursing
14/64
2009, American Heart Association. All rights reserved.
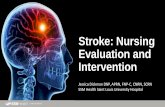
Etiology of Hemorrhagic StrokeEtiology of Hemorrhagic Stroke
Caused by a primaryCaused by a primary
either intracerebraleither intracerebralhemorrhage orhemorrhage orsubarachnoidsubarachnoidhemorrhage.hemorrhage.
SAH 3%
ICH 10%
-
8/7/2019 Stroke Nursing
15/64
2009, American Heart Association. All rights reserved.
CT Scan Right SubcorticalIntracerebral Hemorrhage
-
8/7/2019 Stroke Nursing
16/64
2009, American Heart Association. All rights reserved.
Risk Factors for HemorrhagicRisk Factors for HemorrhagicStrokeStroke
HypertensionHypertension
Bleeding disordersBleeding disorders
African American raceAfrican American race
Vascular malformationVascular malformation
Excessive alcohol useExcessive alcohol use
Liver dysfunctionLiver dysfunction
-
8/7/2019 Stroke Nursing
17/64
2009, American Heart Association. All rights reserved.
Phase I of Stroke Care
Emergent care from the first 3 to 24Emergent care from the first 3 to 24
hours after the onset of strokehours after the onset of strokesymptoms.symptoms.
Prehospital call to EMSPrehospital call to EMS
Emergency RoomEmergency Room
-
8/7/2019 Stroke Nursing
18/64
2009, American Heart Association. All rights reserved.
Nursing RoleEMS Instruction In many community and academic institutions, education of
EMS providers has become a function of the nurse educator.
Before beginning an EMS stroke education program, the nurseeducator should verify local policies and regulations governing
acceptable practice for paramedics and EMT
s in that region orstate.
Prehospital CollaborationPrehospital Collaboration Once a potential stroke is suspected, EMS personnel and
nurses must determine the time at which the patient was lastknown to be well (last known well time). This time is the singlemost important determinant of treatment options during the
hyperacute phase.
Assessment includes:Assessment includes: ABCs, identifying the onset of symptoms (last known wellABCs, identifying the onset of symptoms (last known well
time), oxygenation, blood glucose, load and go, andtime), oxygenation, blood glucose, load and go, anddelivering the patient to a center that can deliver acutedelivering the patient to a center that can deliver acutestroke care according to evidence based protocols.stroke care according to evidence based protocols.
-
8/7/2019 Stroke Nursing
19/64
2009, American Heart Association. All rights reserved.
Education of PreHospital PersonnelEducation of PreHospital Personnel
Cincinnati PreCincinnati Pre--Hospital ScaleHospital Scale
FASTFAST
LAPSSLAPSS
Emphasize Load and Go conceptEmphasize Load and Go concept
rtrt--PA only FDA approved drug forPA only FDA approved drug forAISAIS
-
8/7/2019 Stroke Nursing
20/64
2009, American Heart Association. All rights reserved.
Class I RecommendationsClass I RecommendationsPreHospital AssessmentPreHospital Assessment
To increase the number of stroke patients whoTo increase the number of stroke patients who
receive timely treatment, educational programsreceive timely treatment, educational programsfor physicians, hospital personnel, and EMSfor physicians, hospital personnel, and EMSpersonnel are recommendedpersonnel are recommended(Class I, Level of Evidence B).(Class I, Level of Evidence B).
Stroke education of EMS personnel should beStroke education of EMS personnel should be
provided on a regular basis, perhaps as oftenprovided on a regular basis, perhaps as oftenas twice a year, to ensure proper recognition,as twice a year, to ensure proper recognition,field treatment, and delivery of patients tofield treatment, and delivery of patients toappropriate facilitiesappropriate facilities(Class I, Level of Evidence C).(Class I, Level of Evidence C).
-
8/7/2019 Stroke Nursing
21/64
2009, American Heart Association. All rights reserved.
Class I Recommendations
From the Field to the ED: Stroke PatientTriage and Care
EDs should establish standard operating procedures andprotocols to triage stroke patients expeditiously (Class I,Level of Evidence B).
Standard procedures and protocols should be established forbenchmarking time to expeditiously evaluate and treat eligiblestroke patients with rtPA (Class I, Level of Evidence B).
Target treatment with rtPA should be within 1 hour of the
patients arrival in the ED (Class I, Level of Evidence A).
Eligible patients can be treated between the 3-4.5 hourwindow when carefully evaluated carefully for exclusions totreatment. (Class I, Level of Evidence B)
-
8/7/2019 Stroke Nursing
22/64
2009, American Heart Association. All rights reserved.
Class 1 Recommendations
Education Priorities for Assessment andTreatment in the Fieldd
EMS personnel should be trained to administer avalidated prehospital stroke assessment, such as the
Cincinnati Prehospital Stroke Scale or the Los AngelesPrehospital Stroke Screen (Class I, Level of Evidence B).
EMS personnel should be trained to determine the lastknown well time using standardized definitions to collectthe most accurate information.(Class I, Level of Evidence B).
EMS personnel should use the neurological/strokeassessment approach to gather basic physiologicalinformation about the patient and communicate thepatients condition to the receiving hospital(Class I, Level of Evidence B).
-
8/7/2019 Stroke Nursing
23/64
2009, American Heart Association. All rights reserved.
EMERGENCY NURSING INTERVENTIONS IN THEEMERGENCY/HYPERACUTE PHASE OF STROKE:The First 24 Hours
Stroke symptoms can evolve overStroke symptoms can evolve over
minutes to hours.minutes to hours. Nurses should be aware of unusualNurses should be aware of unusual
stroke presentations.stroke presentations.
ED assessments include: NeurologicalED assessments include: Neurological
assessment, vital signs + temperature,assessment, vital signs + temperature,and should be done not less than everyand should be done not less than every30 minutes.30 minutes.
-
8/7/2019 Stroke Nursing
24/64
2009, American Heart Association. All rights reserved.
The 5 Key Stroke Syndromes: ClassicSigns Referable to Different Cerebral Areas
Left (DominantLeft (Dominant
Hemisphere)Hemisphere) Left gaze preferenceLeft gaze preference
Right visual fieldRight visual fielddeficitdeficit
Right hemiparesisRight hemiparesis
Right hemisensoryRight hemisensorylossloss
Right (NondominantRight (Nondominant
Hemisphere)Hemisphere) Right gaze preferenceRight gaze preference
Left visual field deficitLeft visual field deficit
Left hemiparesisLeft hemiparesis
Left hemisensory lossLeft hemisensory loss
neglect (left hemineglect (left hemi--inattention)inattention)
-
8/7/2019 Stroke Nursing
25/64
2009, American Heart Association. All rights reserved.
The 5 Key Stroke Syndromes:The 5 Key Stroke Syndromes:Classic Signs Referable to DifferentClassic Signs Referable to DifferentCerebral AreasCerebral Areas
BrainstemBrainstem
Nausea and/or vomitingNausea and/or vomiting Diplopia, dysconjugateDiplopia, dysconjugategaze, gaze palsygaze, gaze palsy
Dysarthria, dysphagiaDysarthria, dysphagia
Vertigo, tinnitusVertigo, tinnitus
Hemiparesis orHemiparesis orquadriplegiaquadriplegia
Sensory loss inSensory loss inhemibody or all 4 limbshemibody or all 4 limbs
DecreasedDecreasedconsciousnessconsciousness
Hiccups, abnormalHiccups, abnormalrespirationsrespirations
CerebellumCerebellum
T
runcal/gait ataxiaT
runcal/gait ataxia Limb ataxia neckLimb ataxia neckstiffnessstiffness
-
8/7/2019 Stroke Nursing
26/64
2009, American Heart Association. All rights reserved.
Hemorrhage Symptoms
HemorrhageHemorrhage
Focal neurological deficits as in AISFocal neurological deficits as in AIS Headache (especially in subarachnoidHeadache (especially in subarachnoidhemorrhage)hemorrhage)
Neck painNeck pain
Light intoleranceLight intolerance Nausea, vomitingNausea, vomiting
Decreased level of consciousnessDecreased level of consciousness
-
8/7/2019 Stroke Nursing
27/64
2009, American Heart Association. All rights reserved.
Administration ofThrombolytic Treatment
RtRt--PA is packaged as a crystalline powder andPA is packaged as a crystalline powder andis reconstituted with sterile water.is reconstituted with sterile water.
Dosing: calculate rtDosing: calculate rt--PA at 0.9mg/kgPA at 0.9mg/kg Give a 10% bolus over 1 minuteGive a 10% bolus over 1 minute Give the rest (90%) over 1 hourGive the rest (90%) over 1 hour Max dose for any patient is 90mgMax dose for any patient is 90mg
To prevent accidental overdose, it is important to wasteTo prevent accidental overdose, it is important to waste
amount with another nurse before administering toamount with another nurse before administering topatient.patient.
Prior to administering rtPrior to administering rt--PA make sure all invasive linesPA make sure all invasive linesare in place (e.g., endotracheal and indwelling urinaryare in place (e.g., endotracheal and indwelling urinarycatheter).catheter).
-
8/7/2019 Stroke Nursing
28/64
2009, American Heart Association. All rights reserved.
Nursing Assessment:Nursing Assessment:
Schedule of Neurological Assessment and VitalSchedule of Neurological Assessment and VitalSigns and Other Acute Care Assessments inSigns and Other Acute Care Assessments inThrombolysisThrombolysis--Treated and NonthrombolysisTreated and NonthrombolysisTreated PatientsTreated Patients
Patients treated with ThrombolyticsPatients treated with Thrombolytics Patients not treated with thrombolyticsPatients not treated with thrombolytics
Neurological assessment and vital signs
(except temp) q 15 min during rtPAinfusion, then every 30 min for 6 h, thenq 60 min for 16 hrs (total of 24 hrs)
Note: Frequency of blood pressureassessments may need to be increasedif systolic BP stays u180 mm Hg or
diastolic BP stays u105 mm Hg.
Temp q 4 hrs or prn
Treat temps >99.6F with acetaminophenas ordered
In ICU, every hour with neurological
checks or more frequently if necessary
In non-ICU setting, depending onpatients condition and neurologicalassessments, at a minimum checkneurological and vital signs q 4 hrs
-
8/7/2019 Stroke Nursing
29/64
2009, American Heart Association. All rights reserved.
Schedule of Neurological Assessment and VitalSchedule of Neurological Assessment and Vital
Signs and Other Acute Care Assessments inSigns and Other Acute Care Assessments inThrombolysisThrombolysis--Treated and NonthrombolysisTreated and NonthrombolysisTreated PatientsTreated Patients
Patients treated with ThrombolyticsPatients treated with Thrombolytics Patients not treated with thrombolyticsPatients not treated with thrombolytics
Call physician if:
Systolic BP >185 or 105 or 24/minTemp >99.6F
Worsening of stroke symptoms or other
decline in neurological status
Call physician for further treatment based
on clinician/institution guidelines:
Systolic BP >220 or 120 or 24/minTemp >99.6F
Worsening of stroke symptoms or otherdecline in neurological status
-
8/7/2019 Stroke Nursing
30/64
2009, American Heart Association. All rights reserved.
Schedule of Neurological Assessment and VitalSchedule of Neurological Assessment and Vital
Signs and Other Acute Care Assessments inSigns and Other Acute Care Assessments inThrombolysisThrombolysis--Treated and NonthrombolysisTreated and NonthrombolysisTreated PatientsTreated Patients
Patients treated with thrombolyticsPatients treated with thrombolytics Patients not treated with thrombolyticsPatients not treated with thrombolytics
IV fluids NS at 75-100 mL/hr IV fluids NS at 75-100 mL/hr
No heparin, warfarin, aspirin, clopidogrel ordipyridamole for 24 hrs, then start the
antithrombotic as ordered
Antithrombotics should be ordered withinfirst 24 hrs of hospital admission
Brain CT or MRI after rtPA therapy (at 24hrs) Repeat brain CT scan or MRI may beordered 24-48 hrs after stroke or prn
-
8/7/2019 Stroke Nursing
31/64
2009, American Heart Association. All rights reserved.
Schedule of Neurological Assessment and VitalSchedule of Neurological Assessment and VitalSigns and Other Acute Care Assessments inSigns and Other Acute Care Assessments inThrombolysisThrombolysis--Treated and NonthrombolysisTreated and NonthrombolysisTreated PatientsTreated Patients
Patients treated with ThrombolyticsPatients treated with Thrombolytics Patients not treated with thrombolyticsPatients not treated with thrombolytics
For O2 sat
-
8/7/2019 Stroke Nursing
32/64
2009, American Heart Association. All rights reserved.
Emergent Stroke Workup
All patientsAll patients NonNon--contrast brain CT or brain MRIcontrast brain CT or brain MRI BloodBlood
glucoseglucose Serum electrolytes/renal function testsSerum electrolytes/renal function tests
ECGECG
Markers of cardiac ischemiaMarkers of cardiac ischemia
Complete blood count, including plateletComplete blood count, including platelet
countcount Prothrombin time/INRProthrombin time/INR
aPTTaPTT
Oxygen saturationOxygen saturation
-
8/7/2019 Stroke Nursing
33/64
2009, American Heart Association. All rights reserved.
Emergent Stroke Workup
Selected patientsSelected patients Hepatic function testsHepatic function tests Toxicology screenToxicology screen Blood alcohol levelBlood alcohol level Pregnancy testPregnancy test Arterial blood gas tests (if hypoxia isArterial blood gas tests (if hypoxia is
suspected)suspected) Chest radiography (if lung disease isChest radiography (if lung disease is
suspected)suspected) Lumbar puncture (if SAH is suspected andLumbar puncture (if SAH is suspected and
CT scan is negative for blood)CT scan is negative for blood) EEG (if seizures are suspected)EEG (if seizures are suspected)
-
8/7/2019 Stroke Nursing
34/64
2009, American Heart Association. All rights reserved.
Stroke/Medical History Questions Time patient last known well (will be used as presumedTime patient last known well (will be used as presumed
time of onset)time of onset) Time symptoms were first observed (if different fromTime symptoms were first observed (if different from
time last known well)time last known well)
Was anyone with patient when symptoms began? If so,Was anyone with patient when symptoms began? If so,who?who? History of diabetes?History of diabetes? History of hypertension?History of hypertension? History of seizures?History of seizures?
History of trauma related to current event?History of trauma related to current event?
History of myocardial infarction or angina?History of myocardial infarction or angina? History of cardiac arrhythmias? Atrial fibrillation?History of cardiac arrhythmias? Atrial fibrillation? History of prior stroke orTIA?History of prior stroke orTIA?
What medications is patient currently taking? Is patientWhat medications is patient currently taking? Is patientreceiving anticoagulation therapy with warfarin?receiving anticoagulation therapy with warfarin?
-
8/7/2019 Stroke Nursing
35/64
2009, American Heart Association. All rights reserved.
Recommendations forTreatment of ElevatedRecommendations forTreatment of ElevatedBlood Pressure in Acute Ischemic Stroke:Blood Pressure in Acute Ischemic Stroke:Nursing KnowledgeNursing Knowledge
Blood Pressure Level NotBlood Pressure Level Noteligible for thrombolytic therapyeligible for thrombolytic therapy
TreatmentTreatment
Systolic
-
8/7/2019 Stroke Nursing
36/64
2009, American Heart Association. All rights reserved.
Recommendations forTreatment of ElevatedRecommendations forTreatment of ElevatedBlood Pressure in Acute Ischemic Stroke:Blood Pressure in Acute Ischemic Stroke:Nursing KnowledgeNursing Knowledge
Blood Pressure Level Not eligible forBlood Pressure Level Not eligible forthrombolytic therapythrombolytic therapy
TreatmentTreatment
Systolic >220 mm HgSystolic >220 mm Hg
oror
Diastolic 140 mm Hg Nitroprusside 0.5 g/kg per min IVNitroprusside 0.5 g/kg per min IVinfusion as initial dose with continuousinfusion as initial dose with continuousblood pressure monitoring. Aim for ablood pressure monitoring. Aim for a
10% to 15% reduction of blood pressure10% to 15% reduction of blood pressure
-
8/7/2019 Stroke Nursing
37/64
2009, American Heart Association. All rights reserved.
Recommendations forTreatment of ElevatedRecommendations forTreatment of ElevatedBlood Pressure in Acute Ischemic Stroke:Blood Pressure in Acute Ischemic Stroke:Nursing KnowledgeNursing Knowledge
Blood Pressure Level Eligible forBlood Pressure Level Eligible forthrombolytic therapythrombolytic therapy
TreatmentTreatment
PrePre--treatmenttreatmentSystolic >185 mm HgSystolic >185 mm Hg ororDiastolic >110 mmDiastolic >110 mmHgHg
Check blood pressure every 15 min for 2 h,Check blood pressure every 15 min for 2 h,then every 30 min for 6 hrs, and then everythen every 30 min for 6 hrs, and then everyhour for 16 hrshour for 16 hrs
Sodium nitroprusside 0.5 g/kg per min IVSodium nitroprusside 0.5 g/kg per min IVinfusion as initial dose and titrate toinfusion as initial dose and titrate todesired blood pressure leveldesired blood pressure level
Labetalol 10Labetalol 1020 mg IV over 120 mg IV over 12 min.2 min.
May repeatMay repeat vv 11 orornitropaste 1nitropaste 12 in2 in ororNicardipine drip, 5 mg/h, titrate up by 0.25Nicardipine drip, 5 mg/h, titrate up by 0.25mg/h at 5mg/h at 5-- to 15to 15--minute intervals;minute intervals;maximum dose: 15 mg/hr, if bloodmaximum dose: 15 mg/hr, if bloodpressure is not reduced and maintained atpressure is not reduced and maintained atdesired levels (systolic 185 mm Hg anddesired levels (systolic 185 mm Hg anddiastolic 110 mm Hg), do not administerdiastolic 110 mm Hg), do not administerrtPArtPA
-
8/7/2019 Stroke Nursing
38/64
2009, American Heart Association. All rights reserved.
Recommendations forTreatment of ElevatedRecommendations forTreatment of ElevatedBlood Pressure in Acute Ischemic Stroke:Blood Pressure in Acute Ischemic Stroke:Nursing KnowledgeNursing Knowledge
Blood Pressure Level Eligible forBlood Pressure Level Eligible forthrombolytic therapythrombolytic therapy
TreatmentTreatment
During and after treatmentDuring and after treatment
1.1. Monitor blood pressureMonitor blood pressure
2.2. 2. Diastolic >140 mm Hg2. Diastolic >140 mm Hg
3.3. 3. Systolic >230 mm Hg3. Systolic >230 mm Hg oror
Labetalol 10 mg IV over 1Labetalol 10 mg IV over 12 min, may2 min, mayrepeat every 10repeat every 10--20 min, maximum dose:20 min, maximum dose:30 mg30 mg
oror
Labetalol 10 mg IV followed by infusion atLabetalol 10 mg IV followed by infusion at22--8 mg/min8 mg/min
ororNicardipine drip, 5 mg/h, titrate up toNicardipine drip, 5 mg/h, titrate up todesired effect by increasing 2.5 mg/hdesired effect by increasing 2.5 mg/hevery 5 min to maximum dose of 15 mg/hrevery 5 min to maximum dose of 15 mg/hr
-
8/7/2019 Stroke Nursing
39/64
2009, American Heart Association. All rights reserved.
Recommendations forTreatment of ElevatedRecommendations forTreatment of ElevatedBlood Pressure in Acute Ischemic Stroke:Blood Pressure in Acute Ischemic Stroke:Nursing KnowledgeNursing KnowledgeBlood Pressure Level Eligible forBlood Pressure Level Eligible forthrombolytic therapythrombolytic therapy
TreatmentTreatment
Diastolic121Diastolic121140 mm Hg140 mm Hg May repeat or double labetalol every 10May repeat or double labetalol every 10
min to a maximum dose of 300 mg or givemin to a maximum dose of 300 mg or giveinitial labetalol bolus and then startinitial labetalol bolus and then startlabetalol drip at 2 to 8 mg/minlabetalol drip at 2 to 8 mg/min
OrOr
Nicardipine 5 mg/h IV drip as initial dose,Nicardipine 5 mg/h IV drip as initial dose,titrate up to desired effect by increasingtitrate up to desired effect by increasing2.5 mg/h every 5 min to maximum dose of2.5 mg/h every 5 min to maximum dose of
15 mg/hr15 mg/hrTitrate to desired effect by increasing 2.5Titrate to desired effect by increasing 2.5mg/hr every 5 min to maximum dose of 15mg/hr every 5 min to maximum dose of 15mg/hr. If blood pressure is not controlledmg/hr. If blood pressure is not controlledby labetalol, consider sodiumby labetalol, consider sodiumnitroprusside but avoid if possible.nitroprusside but avoid if possible.
-
8/7/2019 Stroke Nursing
40/64
2009, American Heart Association. All rights reserved.
Recommendations forTreatment of ElevatedRecommendations forTreatment of ElevatedBlood Pressure in Acute Ischemic Stroke:Blood Pressure in Acute Ischemic Stroke:Nursing KnowledgeNursing Knowledge
Blood Pressure Level Eligible forBlood Pressure Level Eligible for
thrombolytic therapythrombolytic therapy
TreatmentTreatment
4. Systolic 1804. Systolic 180230 mm Hg230 mm Hg orDiastolicorDiastolic105105120 mm Hg120 mm Hg
Labetalol 10 mg IV over 1Labetalol 10 mg IV over 12 min, may2 min, mayrepeat every 10repeat every 10--20 minutes, maximum20 minutes, maximumdose of 30 mgdose of 30 mg
May repeat or double labetalol every 10May repeat or double labetalol every 10--20 min to a maximum dose of 30 mg20 min to a maximum dose of 30 mg oror
Give initial labetalol 10 mg IV followed byGive initial labetalol 10 mg IV followed by
infusion at 2infusion at 2--8 mg/min bolus and then8 mg/min bolus and thenstart a labetalol drip at 2start a labetalol drip at 2--8 mg/min8 mg/min
-
8/7/2019 Stroke Nursing
41/64
2009, American Heart Association. All rights reserved.
Intensive Monitoring
30% of patients will deteriorate in the first 2430% of patients will deteriorate in the first 24hours.hours.
Intensive monitoring by nurses trained inIntensive monitoring by nurses trained instroke is very importantstroke is very important
Trained in neurological assessment (NIHSS)Trained in neurological assessment (NIHSS)
Trained in monitoring of bleedingTrained in monitoring of bleedingcomplications (major and minor)complications (major and minor)
Ongoing management of blood pressure,Ongoing management of blood pressure,temperature, oxygenation, and bloodtemperature, oxygenation, and bloodglucoseglucose
-
8/7/2019 Stroke Nursing
42/64
2009, American Heart Association. All rights reserved.
Acute Care
Nursing focus on stabilization of the strokeNursing focus on stabilization of the strokepatient through frequent evaluation ofpatient through frequent evaluation ofneurological status, BP management andneurological status, BP management andprevention of complicationsprevention of complications
Clinical pathways and stroke orders thatClinical pathways and stroke orders thataddress these issues and include consultationsaddress these issues and include consultations
of multidisciplinary team should be developedof multidisciplinary team should be developed
-
8/7/2019 Stroke Nursing
43/64
2009, American Heart Association. All rights reserved.
General Supportive Care ofStroke Focus on prevention ofcomplications
Dysphagia Screening to prevent risk ofDysphagia Screening to prevent risk of
aspiration pneumonia and determine feedingaspiration pneumonia and determine feedingmobilitymobility
Early mobility to prevent DVT, pulmonaryEarly mobility to prevent DVT, pulmonaryemboliemboli
Bowel and bladder careBowel and bladder care best to avoid urinarybest to avoid urinarycatheter insertion but if necessary remove ascatheter insertion but if necessary remove assoon as possiblesoon as possible
Other interventions include:Other interventions include:
Falls preventionFalls prevention
Skin CareSkin Care
-
8/7/2019 Stroke Nursing
44/64
2009, American Heart Association. All rights reserved.
NINDS rtNINDS rt--PA Stroke Study GroupPA Stroke Study GroupHemorrhage AlgorithmHemorrhage Algorithm Nursing AlertNursing Alert
Care ElementCare Element Suspect ICH orSuspect ICH orSystemic BleedSystemic Bleed
22--24 h After ICH24 h After ICH 22--24 h After ICH24 h After ICH
ConsultationsConsultations Neurosurgery if Neurosurgery ifICH suspectedICH suspected
Hematology if ICHHematology if ICHsuspectedsuspected
General surgery ifGeneral surgery ifsystemic bleedsystemic bleedsuspectedsuspected
SameSame Same 2Same 2--24 h After ICH24 h After ICH
Same 2Same 2--24 h After24 h AfterICHICH
Vital signs q 15Vital signs q 15minmin
Neuro exam,Neuro exam,signs of ICP q 15signs of ICP q 15minmin
Continuous ECGContinuous ECGmonitoringmonitoring
Look for otherLook for otherbleeding sitesbleeding sites
Vital signs q 1 hVital signs q 1 hand prnand prn
Signs of ICP,Signs of ICP,neuro examneuro exam
GCS/pupil checkGCS/pupil checkq 1 hr and prnq 1 hr and prn
Monitor ECGMonitor ECG
Monitor SVO2,Monitor SVO2,ICPICP
Advance vital signs prnAdvance vital signs prn
Advance neuro examAdvance neuro exam
Consider discontinuingConsider discontinuingECGECG
-
8/7/2019 Stroke Nursing
45/64
2009, American Heart Association. All rights reserved.
NINDS rtNINDS rt--PA Stroke Study GroupPA Stroke Study GroupHemorrhage AlgorithmHemorrhage Algorithm -- Nursing AlertNursing Alert
Care ElementCare Element Suspect ICH orSuspect ICH orSystemic BleedSystemic Bleed
22--24 h After ICH24 h After ICH 22--24 h After ICH24 h After ICH
STAT diagnostics CT head,noncontrast or MRIwith GRE sequence
Labs: PT/aPTT/INR,fibrinogen, CBC withplatelets, type andcross-match
Pulse oximetry,consider SVO2,brain oximeter
Consider ICP
monitorConsiderhemodynamicmonitoring
Check stool foroccult blood
Labs:Labs:
Na2+,Na2+,
osmolality (if onosmolality (if onmannitol)mannitol)
Glucose q 6 h andGlucose q 6 h andprn (in patients withprn (in patients withhistory of DM)history of DM)
ABGs CO2 30ABGs CO2 30--3535(hyperventilation if(hyperventilation ifordered)ordered)
Consider ICPConsider ICPmonitormonitor
Consider discontinuing O2Consider discontinuing O2monitoringmonitoring
-
8/7/2019 Stroke Nursing
46/64
2009, American Heart Association. All rights reserved.
NINDS rtNINDS rt--PA Stroke Study GroupPA Stroke Study GroupHemorrhage AlgorithmHemorrhage Algorithm Nursing AlertNursing Alert
Care ElementCare Element Suspect ICH orSuspect ICH orSystemic BleedSystemic Bleed
22--24 h After ICH24 h After ICH 22--24 h After ICH24 h After ICH
Treatments If receivingthrombolytics,
STOP INFUSION
Considerhyperventilation
Consider mannitol
Consider blood products(cryoprecipitate, FFP,PLTs, PRBCs, other medssuch as factor VIIa)
Consider surgery. Applypressure to compressiblesites for major or minorsystemic bleeds
Keep PO2 >90 mmKeep PO2 >90 mmHgHg
ConsiderConsider
hyperventilationhyperventilation
Consider mannitolConsider mannitol25 g q 425 g q 4--6 h6 h
Consider surgery;Consider surgery;treat DKA/HOC withtreat DKA/HOC withinsulin drip prn.insulin drip prn.
Keep PO2 >90 mm HgKeep PO2 >90 mm Hg
Wean hyperventilationWean hyperventilation
Wean mannitolWean mannitolWean blood pressure drips,Wean blood pressure drips,add oral agent as toleratedadd oral agent as tolerated
-
8/7/2019 Stroke Nursing
47/64
2009, American Heart Association. All rights reserved.
NINDS rtNINDS rt--PA Stroke Study GroupPA Stroke Study GroupHemorrhage AlgorithmHemorrhage Algorithm Nursing AlertNursing Alert
CareCareElementElement
Suspect ICH orSuspect ICH orSystemic BleedSystemic Bleed
22--24 h After ICH24 h After ICH 22--24 h After ICH24 h After ICH
ActivityActivity Bed rest
Change position q 1-2 has tolerated
SameSame Advance as toleratedAdvance as tolerated
NutritionNutrition Feed as soon as possible
NPO. Consider enteralfeedings with NGT or
DHT
SameSame Consider feeding asConsider feeding asswallowing screen defines,swallowing screen defines,considerTPN or otherconsiderTPN or otherenteral feedingenteral feeding
-
8/7/2019 Stroke Nursing
48/64
2009, American Heart Association. All rights reserved.
Nursing AlertNursing Alert Assessing ICPAssessing ICP
Signs and symptoms of increasing ICPSigns and symptoms of increasing ICP a medical emergencya medical emergency
Early signs: decreased level of consciousness, deterioration in motorEarly signs: decreased level of consciousness, deterioration in motorfunction, headache, visual disturbances, changes in blood pressure orfunction, headache, visual disturbances, changes in blood pressure orheart rate, changes in respiratory patternheart rate, changes in respiratory pattern
Late signs: pupillary abnormalities, more persistent changes in vital signs,Late signs: pupillary abnormalities, more persistent changes in vital signs,
changes in respiratory pattern with changes in arterial blood gaseschanges in respiratory pattern with changes in arterial blood gasesIntervention: thorough neurological assessment, notify physicianIntervention: thorough neurological assessment, notify physicianimmediately, emergency brain imaging, maintain ABCsimmediately, emergency brain imaging, maintain ABCs
General measures to prevent elevation of ICPGeneral measures to prevent elevation of ICP
HOB up 30HOB up 30 or as physician specifies, reverse Trendelenburg position mayor as physician specifies, reverse Trendelenburg position maybe used if blood pressure is stable. Head position may be one of the singlebe used if blood pressure is stable. Head position may be one of the singlemost important nursing modalities for controlling increased ICP.most important nursing modalities for controlling increased ICP.
Good head and body alignment: prevents increased intrathoracic pressureGood head and body alignment: prevents increased intrathoracic pressureand allows venous drainage.and allows venous drainage.
Pain management: provide good pain control on a consistent basisPain management: provide good pain control on a consistent basis
Keep patient normothermic.Keep patient normothermic.
-
8/7/2019 Stroke Nursing
49/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
Antihypertensive drugs are recommended for prevention of recurrent strokeAntihypertensive drugs are recommended for prevention of recurrent strokeand other vascular events in persons who have had an ischemic stroke andand other vascular events in persons who have had an ischemic stroke andbeyond the hyperacute period.beyond the hyperacute period.
This benefit extends to persons with and w/o a history of hypertension andThis benefit extends to persons with and w/o a history of hypertension andshould be considered for all ischemic stroke and TIA patients.should be considered for all ischemic stroke and TIA patients.
An absolute target BP level and reduction are uncertain and should beAn absolute target BP level and reduction are uncertain and should beindividualized; benefit has been associated with an average reduction of lessindividualized; benefit has been associated with an average reduction of lessthan 10/5 mm Hg, and normal BP levels have been defined as < 120/80 mm Hgthan 10/5 mm Hg, and normal BP levels have been defined as < 120/80 mm Hgby JNCby JNC--77
Several lifestyle modifications have been associated with BP reductions andSeveral lifestyle modifications have been associated with BP reductions andshould be included as part of a comprehensive approach.should be included as part of a comprehensive approach.
Optimal drug regimen remains uncertain; however, available data support theOptimal drug regimen remains uncertain; however, available data support theuse of diuretics and the combination of diuretics and an ACEI. Choice ofuse of diuretics and the combination of diuretics and an ACEI. Choice ofspecific drugs and targets should be individualized on the basis of reviewedspecific drugs and targets should be individualized on the basis of revieweddata and consideration, as well as specific patient characteristics (e.g.,data and consideration, as well as specific patient characteristics (e.g.,
extracranial cerebrovascular occlusive disease, renal impairment, cardiacextracranial cerebrovascular occlusive disease, renal impairment, cardiacdisease, and DM).disease, and DM).
Hypertension
-
8/7/2019 Stroke Nursing
50/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
More rigorous control of blood pressure and lipids should beMore rigorous control of blood pressure and lipids should beconsidered in patients with diabetes.considered in patients with diabetes.
Although all major classes of antihypertensives are suitable forAlthough all major classes of antihypertensives are suitable forthe control of BP, most patients will require greater than 1the control of BP, most patients will require greater than 1agent. ACEIs and ARBs are more effective in reducing theagent. ACEIs and ARBs are more effective in reducing theprogression of renal disease and are recommended as firstprogression of renal disease and are recommended as first--choice medications for patients with DM.choice medications for patients with DM.
Glucose control is recommended to nearGlucose control is recommended to near--normoglycemic levelsnormoglycemic levels
among diabetics with ischemic stroke orTIA to reduceamong diabetics with ischemic stroke orTIA to reducemicrovascular complications.microvascular complications.
The goal for Hb A1c should be less than or equal to 7%.The goal for Hb A1c should be less than or equal to 7%.
Diabetes
-
8/7/2019 Stroke Nursing
51/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
Ischemic stroke orTIA patients with elevated cholesterol, comorbid CAD,Ischemic stroke orTIA patients with elevated cholesterol, comorbid CAD,or evidence of an atherosclerotic origin should be managed according toor evidence of an atherosclerotic origin should be managed according toNCEP III guidelines, which include lifestyle modification, dietaryNCEP III guidelines, which include lifestyle modification, dietaryguidelines, and medication recommendations.guidelines, and medication recommendations.
Statin agents are recommended, and the target goal for cholesterolStatin agents are recommended, and the target goal for cholesterollowering for those with CHD or symptomatic atherosclerotic disease is anlowering for those with CHD or symptomatic atherosclerotic disease is anLDLLDL--C of less than 100 mg/dL and LDLC of less than 100 mg/dL and LDL--C less than 70 mg/dL for veryC less than 70 mg/dL for very--highhigh--risk persons with multiple risk factors.risk persons with multiple risk factors.
Patients with ischemic stroke orTIA presumed to be due to anPatients with ischemic stroke orTIA presumed to be due to anatherosclerotic origin but with no preexisting indications for statinsatherosclerotic origin but with no preexisting indications for statins
(normal cholesterol levels, no comorbid CAD, or no evidence of(normal cholesterol levels, no comorbid CAD, or no evidence ofatherosclerosis) are reasonable to consider for treatment with a statinatherosclerosis) are reasonable to consider for treatment with a statinagent to reduce the risk of vascular events.agent to reduce the risk of vascular events.
Ischemic stroke orTIA patients with low HDLIschemic stroke orTIA patients with low HDL--C may be considered forC may be considered fortreatment with niacin or gemfibrozil.treatment with niacin or gemfibrozil.
Cholesterol Control
-
8/7/2019 Stroke Nursing
52/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
All ischemic stroke orTIA patients who have smoked in theAll ischemic stroke orTIA patients who have smoked in the
past year should be strongly encouraged not to smoke.past year should be strongly encouraged not to smoke.
Avoid environmental smoke.Avoid environmental smoke.
Counseling, nicotine products, and oral smoking cessationCounseling, nicotine products, and oral smoking cessationmedications have been found to be effective for smokers.medications have been found to be effective for smokers.
Smoking Cessation
-
8/7/2019 Stroke Nursing
53/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
Patients with prior ischemic stroke orTIA who are heavyPatients with prior ischemic stroke orTIA who are heavydrinkers should eliminate or reduce their consumption ofdrinkers should eliminate or reduce their consumption of
alcohol.alcohol. Light to moderate levels of less than or equal 2 drinks per dayLight to moderate levels of less than or equal 2 drinks per day
for men and 1 drink per day for nonpregnant women may befor men and 1 drink per day for nonpregnant women may beconsidered.considered.
Alcohol Use
Obesity
Weight reduction may be considered for all overweightischemic stroke orTIA patients to maintain the goal of a BMI of
18.5 to 24.9 kg/m2 and a waist circumference of less than 35 in
for women and less than 40 in for men. Clinicians should
encourage weight management through an appropriate balance
of caloric intake, physical activity, and behavioral counseling.
-
8/7/2019 Stroke Nursing
54/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
Physical activityPhysical activity
For those with ischemic stroke orTIA who are capable ofFor those with ischemic stroke orTIA who are capable ofengaging in physical activity, at least 30 minutes ofengaging in physical activity, at least 30 minutes of
moderatemoderate--intensity physical exercise most days of theintensity physical exercise most days of theweek may reduce risk factors and comorbid conditionsweek may reduce risk factors and comorbid conditionsthat increase the likelihood of recurrence of stroke.that increase the likelihood of recurrence of stroke.
For those with disability after ischemic stroke, asupervised therapeutic exercise regimen isrecommended.
-
8/7/2019 Stroke Nursing
55/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
For recent TIA or ischemic stroke within the last 6 mo and ipsilateral severeFor recent TIA or ischemic stroke within the last 6 mo and ipsilateral severe(70% to 99%) carotid artery stenosis, CEA is recommended by a surgeon with a(70% to 99%) carotid artery stenosis, CEA is recommended by a surgeon with aperioperative morbidity and mortality < 6%.perioperative morbidity and mortality < 6%.
For recentT
IA or ischemic stroke and ipsilateral moderate (50% to 69%)For recentT
IA or ischemic stroke and ipsilateral moderate (50% to 69%)carotid stenosis, CEA is recommended, depending on patientcarotid stenosis, CEA is recommended, depending on patient--specific factorsspecific factorssuch as age, gender, comorbidities, and severity of initial symptoms.such as age, gender, comorbidities, and severity of initial symptoms.
If stenosis is less than 50%, there is no indication for CEA.If stenosis is less than 50%, there is no indication for CEA.
If CEA is indicated, surgery within 2 wks rather than delayed is suggested.If CEA is indicated, surgery within 2 wks rather than delayed is suggested. Among patients with symptomatic severe stenosis (greater than 70%) in whomAmong patients with symptomatic severe stenosis (greater than 70%) in whom
the stenosis is difficult to access surgically, medical conditions that greatlythe stenosis is difficult to access surgically, medical conditions that greatlyincrease risk for surgery, or other circumstances exist (i.e., radiationincrease risk for surgery, or other circumstances exist (i.e., radiation--inducedinducedstenosis or restenosis after CEA; CAS is not inferior to endarterectomy.stenosis or restenosis after CEA; CAS is not inferior to endarterectomy.
CAS is reasonable when performed by operators with periprocedural morbidityCAS is reasonable when performed by operators with periprocedural morbidityand mortality rates of 4% to 6%.and mortality rates of 4% to 6%.
For patients with symptomatic carotid occlusion, EC/IC bypass surgery is notFor patients with symptomatic carotid occlusion, EC/IC bypass surgery is notrecommended routinely.recommended routinely.
Extracranial Carotid Artery Disease
-
8/7/2019 Stroke Nursing
56/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
Endovascular treatment of patients with symptomaticEndovascular treatment of patients with symptomaticextracranial vertebral stenosis may be considered whenextracranial vertebral stenosis may be considered when
patients are having symptoms despite medical therapiespatients are having symptoms despite medical therapies(antithrombotics, statin(antithrombotics, statins,s, and other treatments for risk factors).and other treatments for risk factors).
Extracranial vertebrobasilar disease
Intracranial Disease
The usefulness of endovascular therapy (angioplasty and/or stent
placement) is uncertain for patients with hemodynamically
significant intracranial stenosis who have symptoms despite medicaltherapies (antithrombotics, statins, and other treatments for risk
factors) and is considered investigational.
-
8/7/2019 Stroke Nursing
57/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
Atrial FibrillationAtrial Fibrillation
For patients with ischemic stroke orTIA with persistent or paroxysmalFor patients with ischemic stroke orTIA with persistent or paroxysmal(intermittent) AF, anticoagulation with adjusted(intermittent) AF, anticoagulation with adjusted--dose warfarin (targetdose warfarin (target
INR, 2.5; range, 2.0INR, 2.5; range, 2.03.0) is recommended.3.0) is recommended.
In patients unable to take oral anticoagulants, aspirin 325 mg/d isIn patients unable to take oral anticoagulants, aspirin 325 mg/d isrecommended.recommended.
Acute MI and LV thrombus For patients with an ischemic stroke causedAcute MI and LV thrombus For patients with an ischemic stroke causedby an acute MI in whom LV mural thrombus is identified byby an acute MI in whom LV mural thrombus is identified byechocardiography or another form of cardiac imaging, oralechocardiography or another form of cardiac imaging, oralanticoagulation is reasonable, aiming for an INR of 2.0 to 3.0 for at leastanticoagulation is reasonable, aiming for an INR of 2.0 to 3.0 for at least3 mo and up to 1 year.3 mo and up to 1 year.
Aspirin should be used concurrently for the ischemic CAD patientAspirin should be used concurrently for the ischemic CAD patientduring oral anticoagulant therapy in doses up to 162 mg/d, preferably induring oral anticoagulant therapy in doses up to 162 mg/d, preferably in
the entericthe enteric--coated form.coated form.
-
8/7/2019 Stroke Nursing
58/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:
Knowing and Practicing the GuidelinesKnowing and Practicing the GuidelinesCardiomyopathyCardiomyopathy
For patients with ischemic stroke orTIA who have dilatedFor patients with ischemic stroke orTIA who have dilatedcardiomyopathy, either warfarin (INR, 2.0 to 3.0) or antiplateletcardiomyopathy, either warfarin (INR, 2.0 to 3.0) or antiplatelettherapy may be considered for prevention of recurrent events.therapy may be considered for prevention of recurrent events.
Valvular heart disease, Rheumatic mitral valve diseaseValvular heart disease, Rheumatic mitral valve disease
For patients with ischemic stroke orTIA who have rheumaticmitral valve disease, whether or not AF is present, long-termwarfarin therapy is reasonable, with a target INR of 2.5 (range,2.03.0).
Anti-platelet agents should not be routinely added to warfarinin the interest of avoiding additional bleeding risk.
For ischemic stroke orTIA patients with rheumatic mitral valvedisease, whether or not AF is present, who have a recurrentembolism while receiving warfarin, adding aspirin (81 mg/d)may be indicated.
-
8/7/2019 Stroke Nursing
59/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:Knowing and Practicing the GuidelinesKnowing and Practicing the Guidelines
Mitral valve prolapse (MVP)Mitral valve prolapse (MVP)
For patients with MVP who have ischemic stroke orTIAs, longFor patients with MVP who have ischemic stroke orTIAs, long--term antiplatelet therapy is reasonable.term antiplatelet therapy is reasonable.
Mitral Annular Calcification (MAC)Mitral Annular Calcification (MAC) For patients with ischemic stroke orTIA and MAC not
documented to be calcific, antiplatelet therapy may beconsidered.
Among patients with mitral regurgitation resulting from MACwithout AF, antiplatelet or warfarin therapy may be considered.
-
8/7/2019 Stroke Nursing
60/64
2009, American Heart Association. All rights reserved.
Nursing Care and Secondary Prevention:Nursing Care and Secondary Prevention:Knowing and Practicing the GuidelinesKnowing and Practicing the GuidelinesAortic Valve Disease For patients with ischemic stroke orTIA and aortic valve
disease who do not have AF, antiplatelet therapy may beconsidered.
Prosthetic Heart ValvesProsthetic Heart Valves For patients with ischemic stroke orTIA who have modernFor patients with ischemic stroke orTIA who have modern
mechanical prosthetic heart valves, oral anticoagulants aremechanical prosthetic heart valves, oral anticoagulants arerecommended, with an INR target of 3.0 (range, 2.5recommended, with an INR target of 3.0 (range, 2.53.5).3.5).
For patients with mechanical prosthetic heart valves who haveFor patients with mechanical prosthetic heart valves who havean ischemic stroke or systemic embolism despite adequatean ischemic stroke or systemic embolism despite adequate
therapy with oral anticoagulants, aspirin 75 to 100 mg/d, intherapy with oral anticoagulants, aspirin 75 to 100 mg/d, inaddition to oral anticoagulants, and maintenance of the INR at aaddition to oral anticoagulants, and maintenance of the INR at atarget of 3.0 (range, 2.5target of 3.0 (range, 2.53.5) is reasonable.3.5) is reasonable.
For patients with ischemic stroke orTIA who haveFor patients with ischemic stroke orTIA who havebioprosthetic heart valves with no other source ofbioprosthetic heart valves with no other source ofthromboembolism, anticoagulation with warfarin (INR, 2.0thromboembolism, anticoagulation with warfarin (INR, 2.03.0)3.0)may be considered.may be considered.
-
8/7/2019 Stroke Nursing
61/64
2009, American Heart Association. All rights reserved.
Stroke Educational ProgramsStroke Educational Programs AHA/ASAAHA/ASA
Stroke: Patient Education Tool Kit
Power to End Stroke
African American Power to End Stroke
Power to End Stroke FamilyReunion Toolkit
Stroke Connection magazine
How Stroke Affects Behavior: OurGuide to Physical and EmotionalChanges
Living with Atrial Fibrillation: OurGuide to Managing a Key Stroke RiskFactor
Living with Disability After Stroke
Sex After Stroke: Our Guide to
Intimacy After Stroke
Stroke: Are You at Risk? Our Guide toStroke Risk Factors
Understanding Stroke: Our Guide toExplaining Stroke and How to Reduce
Your Risk
Caring for Someone with Aphasia
High Blood Pressure and Stroke
Warning Signs of Stroke: Our Easy-reading Guide to Emergency Action
Being a Stroke Family Caregiver
Smoking and Your Risk of Stroke
Just Move: Our Guide to PhysicalActivity
Diabetes, Heart Disease and Stroke
-
8/7/2019 Stroke Nursing
62/64
2009, American Heart Association. All rights reserved.
Stroke Educational ProgramsStroke Educational Programs -- NINDSNINDS
What You Need to Know About Stroke
Stroke Risk Factors and Symptoms Brain Basics: Preventing Stroke
Neurological Diagnostic Tests and Procedures
Questions and Answers About Stroke
Questions and Answers About Carotid
Endarterectomy
-
8/7/2019 Stroke Nursing
63/64
2009, American Heart Association. All rights reserved.
Stroke Educational ProgramsStroke Educational Programs -- NSANSA
Stroke SmartStroke Smartmagazinemagazine Stroke Fact SheetStroke Fact Sheet
African Americans and Stroke BrochureAfrican Americans and Stroke Brochure Cholesterol BrochureCholesterol Brochure Explaining Stroke BrochureExplaining Stroke Brochure Intracranial Atherosclerosis BrochureIntracranial Atherosclerosis Brochure Recurrent Stroke Prevention BrochureRecurrent Stroke Prevention Brochure Reducing Risk and Recognizing Symptoms BrochureReducing Risk and Recognizing Symptoms Brochure
Transient Ischemic Attack BrochureTransient Ischemic Attack Brochure Stroke Rapid Response EMS/Prehospital EducationStroke Rapid Response EMS/Prehospital Education Hip Hop StrokeHip Hop Stroke Brainiac Kids Stroke EducationBrainiac Kids Stroke Education
-
8/7/2019 Stroke Nursing
64/64
2009 American Heart Association All rights reserved
Discharge Planning
Goal is to ensure a safe transitionGoal is to ensure a safe transition
between the acute care facility,between the acute care facility,rehabilitation and outpatient settings.rehabilitation and outpatient settings.
Nurses can work with dischargeNurses can work with discharge
planners to optimally meet the dischargeplanners to optimally meet the dischargeneeds of the patient and family.needs of the patient and family.