Stroke: Lysis and Beyond September 15, 2008 Andy Jagoda, MD, FACEP Professor and Vice Chair of...
50
Stroke: Lysis and Beyond Stroke: Lysis and Beyond September 15, 2008 September 15, 2008 Andy Jagoda, MD, FACEP Professor and Vice Chair of Emergency Medicine Mount Sinai School of Medicine New York, New York
Transcript of Stroke: Lysis and Beyond September 15, 2008 Andy Jagoda, MD, FACEP Professor and Vice Chair of...

Stroke: Lysis and BeyondStroke: Lysis and Beyond
September 15, 2008September 15, 2008
Andy Jagoda, MD, FACEPProfessor and Vice Chair of Emergency Medicine
Mount Sinai School of MedicineNew York, New York

DisclosuresDisclosures
• Advisory Board: The Medicines CompanyAdvisory Board: The Medicines Company• Speakers Bureau: GenentechSpeakers Bureau: Genentech
• Past Chair, ACEP Clinical Policies Past Chair, ACEP Clinical Policies CommitteeCommittee
• Executive Board, Brain Attack Coalition, Executive Board, Brain Attack Coalition, NINDSNINDS
• Executive Board, Foundation for Education Executive Board, Foundation for Education and Research in Neurologic Emergencies and Research in Neurologic Emergencies www.ferne.orgwww.ferne.org

Key PointsKey Points
• A (documented) systematic neurologic A (documented) systematic neurologic evaluation is critical to minimizing risk . . . evaluation is critical to minimizing risk . . . And providing good patient careAnd providing good patient care
• EMS plays a pivotal role in acute stroke care EMS plays a pivotal role in acute stroke care and thus is assuming increasing liability and thus is assuming increasing liability associated with their decision makingassociated with their decision making
• Alteplase is a FDA approved treatment for Alteplase is a FDA approved treatment for acute ischemic stroke and therefore a acute ischemic stroke and therefore a decision to not use it for qualified patients decision to not use it for qualified patients must be supported in the medical recordmust be supported in the medical record

IntroductionIntroduction
• Stroke is the 3ird most common cause of Stroke is the 3ird most common cause of death in the United Statesdeath in the United States Second most common cause for Second most common cause for
patients to be in a nursing homepatients to be in a nursing home• 500,000 - 800,000 strokes / year500,000 - 800,000 strokes / year
80 - 90% Ischemic80 - 90% Ischemic 10 - 20% Hemorrhagic or SAH10 - 20% Hemorrhagic or SAH 10 - 20% Mortality within 3 months10 - 20% Mortality within 3 months
• Leading cause of disabilityLeading cause of disability

The Facts: Ischemic StrokeThe Facts: Ischemic Stroke
• TIAsTIAs 20% – 50% of strokes preceded by a TIA20% – 50% of strokes preceded by a TIA 75% resolve in <15 minutes; 97% <3 hours75% resolve in <15 minutes; 97% <3 hours New definition: event lasting less than 1 hour and New definition: event lasting less than 1 hour and
not associated with changes on neuroimagingnot associated with changes on neuroimaging• Acute Ischemic strokeAcute Ischemic stroke
Hemorrhagic conversion within 36 hours: 1% Hemorrhagic conversion within 36 hours: 1% symptomatic, 4% asymptomaticsymptomatic, 4% asymptomatic
30% have little or no disability at 3 months30% have little or no disability at 3 months 30% have mild to moderate disability at 3 months30% have mild to moderate disability at 3 months 30% have severe disability30% have severe disability 10% dead at 3 months 10% dead at 3 months

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ICH IschemicP
rop
ort
ion
of
pa
tie
nts
(%
)
Dead Dependent Independent
ICH ICH High Mortality / Limited RecoveryHigh Mortality / Limited Recovery
Manno EM, et al. Manno EM, et al. Mayo Clin ProcMayo Clin Proc. 2005;80:420-433; Mayer SA, Rincon F. . 2005;80:420-433; Mayer SA, Rincon F. Lancet NeurolLancet Neurol. 2005;4:662-672; Qureshi . 2005;4:662-672; Qureshi AI, et al. AI, et al. N Engl J Med.N Engl J Med. 2001;344:1450-1460; Taylor TN, et al. 2001;344:1450-1460; Taylor TN, et al. StrokeStroke. 1996;27:1459-1466; Reed SD, et al. . 1996;27:1459-1466; Reed SD, et al. NeurologyNeurology. 2001;57:305-314.. 2001;57:305-314.
• MortalityMortality 6-month, 30%-50%6-month, 30%-50% 1-year, 50%1-year, 50%
• Only 20% of ICH patients are independent at 6 months vs 60% of ischemic stroke patients
• Medical costs• US$125,000 lifetime cost per person (1990)• Direct and indirect costs (lost productivity + caregiver burden)

NINDS t-PA Acute Ischemic Stroke. NEJM NINDS t-PA Acute Ischemic Stroke. NEJM 19951995
• A two part, double blind study: 624 patientsA two part, double blind study: 624 patients Randomized to t-PA or placeboRandomized to t-PA or placebo
• ““Favorable outcome” defined as normal or near Favorable outcome” defined as normal or near normal at 90 daysnormal at 90 days 4 outcome measures: Barthel Index, Modified 4 outcome measures: Barthel Index, Modified
Rankin Scale, Glasgow Outcome Scale, NIHSSRankin Scale, Glasgow Outcome Scale, NIHSS• Adjusted t-PA to placebo global OR for favorable Adjusted t-PA to placebo global OR for favorable
outcome was outcome was 1.71.7 (95%CI,1.2-2.6) (95%CI,1.2-2.6) No increase in mortality and a decrease in No increase in mortality and a decrease in
hospital stayhospital stay

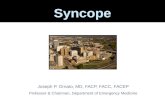
NIH-Recommended Emergency Department NIH-Recommended Emergency Department Response TimesResponse Times
The “golden hour” for evaluating and treating acute stroke
Door-to-needle time ≤60 minutes
0
Suspected stroke patient arrives at ED
CT scan initiated
CT & labs interpreted
tPA given if patient is
eligible
Minutes: 10 15 25 45 60
Initial MD evaluation
Stroke team notified
NINDS Proceedings of a National Symposium on Rapid Identification and Treatment of Acute Stroke, December 12-13, 1996. http://www.ninds.nih.gov/news_and_events/proceedings/stroke_proceedings/recs-emerg.htm. Accessed November 8, 2007.

NINDS Proceedings: 1997 / 2002NINDS Proceedings: 1997 / 2002• Public educationPublic education
• Prehospital emergency responsePrehospital emergency response
• Designated stroke centersDesignated stroke centers
• Emergency departments Emergency departments
• Hospital stroke unitsHospital stroke units
• RehabilitationRehabilitation

The Public MessageThe Public Message
• WEAKNESS OR NUMBNESS ON ONE SIDE WEAKNESS OR NUMBNESS ON ONE SIDE
OF THE BODYOF THE BODY
• DIFFICULTY WITH VISION DIFFICULTY WITH VISION
• DIFFICULTY WITH SPEECH OR DIFFICULTY WITH SPEECH OR
UNDERSTANDINGUNDERSTANDING
• UNUSUALLY SEVERE HEADACHEUNUSUALLY SEVERE HEADACHE
• DIZZINESS OR UNSTEADINESSDIZZINESS OR UNSTEADINESS

• External validityExternal validity• Imbalance of baseline NIHSS between Imbalance of baseline NIHSS between
the t-PA and placebo groupsthe t-PA and placebo groups• Treatment effect favored those patients Treatment effect favored those patients
treated within 90 minutestreated within 90 minutes• Unclear which patients were at risk for Unclear which patients were at risk for
intracerebral hemorrhageintracerebral hemorrhage
NINDS Trial CriticismNINDS Trial Criticism

NINDS Date Re-analysis CommitteeNINDS Date Re-analysis Committee• Kjell Asplund MDKjell Asplund MD
Umeå University, Umeå University, Umeå, SwedenUmeå, Sweden
• Lewis R. Goldfrank Lewis R. Goldfrank MDMDNew York University, New York University, New York, USANew York, USA
• Timothy Ingall MDTimothy Ingall MDMayo Clinic Mayo Clinic Scottsdale, Arizona, Scottsdale, Arizona, USAUSA
• Vicki Hertzberg PhDVicki Hertzberg PhDEmory University, Georgia, Emory University, Georgia, USAUSA
• Thomas Louis PhDThomas Louis PhDJohns Hopkins Bloomberg Johns Hopkins Bloomberg School of Public Health, School of Public Health, Maryland, USAMaryland, USA
• Michael O’Fallon PhDMichael O’Fallon PhDMayo Clinic Rochester, Mayo Clinic Rochester, Minnesota, USAMinnesota, USA

Committee MethodsCommittee Methods
• Concerns assessed included:Concerns assessed included: Baseline NIHSS imbalanceBaseline NIHSS imbalance Time from symptom onset to treatmentTime from symptom onset to treatment Risk factors for intracerebral hemorrhageRisk factors for intracerebral hemorrhage Predictors of favorable outcomePredictors of favorable outcome
• The analysis was adjusted for treating hospital, The analysis was adjusted for treating hospital, time to treatment, age, baseline NIHSS, time to treatment, age, baseline NIHSS, diabetes, diabetes,

ICH AnalysisICH Analysis
# of Risk # of Risk FactorsFactors
# of patients # of patients treated with t-treated with t-
PAPA
(n=310)(n=310)
# of Symptomatic ICH’s# of Symptomatic ICH’s
(# of placebo patients (# of placebo patients with ICH)with ICH)
Percentage Percentage (%)(%)
00 114114 2 (1)2 (1) 1.81.8
11 144144 7 (1)7 (1) 4.94.9
> 1> 1 5252 1111 21.221.2
Risk Factors for ICH:Risk Factors for ICH: Baseline NIHSS > 20Baseline NIHSS > 20 Age > 70 yearsAge > 70 years Ischemic changes present on initial CTIschemic changes present on initial CT Glucose > 300 mg/dl (16.7 mmol/L)Glucose > 300 mg/dl (16.7 mmol/L)

NINDS Re-analysisNINDS Re-analysis
• Initial NIHSS <20, no diabetes, age <70, normal Initial NIHSS <20, no diabetes, age <70, normal CT predict best outcome from t-PA and low risk CT predict best outcome from t-PA and low risk for ICHfor ICH
• The committee concluded, despite an increased The committee concluded, despite an increased incidence of symptomatic intracerebral incidence of symptomatic intracerebral hemorrhage in t‑PA treated patients and hemorrhage in t‑PA treated patients and subgroup imbalances in baseline stroke severity, subgroup imbalances in baseline stroke severity, there was a statistically significant benefit of t-PA there was a statistically significant benefit of t-PA treatment measured by an adjusted t-PA to treatment measured by an adjusted t-PA to placebo global odds ratio of 2.1 (95% CI: 1.5-placebo global odds ratio of 2.1 (95% CI: 1.5-2.9) for a favorable clinical outcome at 3 months2.9) for a favorable clinical outcome at 3 months

Thrombolysis with alteplase for acute ischaemic stroke Thrombolysis with alteplase for acute ischaemic stroke in the Safe Implementation of Thrombolysis in Stroke in the Safe Implementation of Thrombolysis in Stroke Monitoring Study (SITS-MOST). Lancet 2007; 369:275-Monitoring Study (SITS-MOST). Lancet 2007; 369:275-282.282.
• Prospective, open, multicentre, multinational, Prospective, open, multicentre, multinational, observational monitoring study established observational monitoring study established as a condition by the European Union for as a condition by the European Union for licensinglicensing
• 6483 patients6483 patients• 4.6% symptomatic hemorrhage at 24 hours4.6% symptomatic hemorrhage at 24 hours• 39% with no or mild disability at 3 months (vs 39% with no or mild disability at 3 months (vs
29% in pooled placebo)29% in pooled placebo)

The Case: Roseville, Illinois, 2003 The Case: Roseville, Illinois, 2003
63 year old male called EMS at 21:00 with a chief 63 year old male called EMS at 21:00 with a chief complaint of feeling dizzy and weak. Vomited complaint of feeling dizzy and weak. Vomited once. No headache, no vision change. once. No headache, no vision change.
Symptoms began after dinner; 2 cocktails and Symptoms began after dinner; 2 cocktails and 2 glasses of wine2 glasses of wine
Dizziness described as room spinningDizziness described as room spinning

Case Case
• PMHx: PMHx: HypertensionHypertension
• MedicationsMedications Enalapril, 10 mgEnalapril, 10 mg Aspirin, 81 mgAspirin, 81 mg
• Social HxSocial Hx Smoking - 1 pack per daySmoking - 1 pack per day

EMS calledEMS called
• Upon arrival at 21:30 - symptoms Upon arrival at 21:30 - symptoms resolvedresolved
• BP 190 / 110, P 80, RR 14BP 190 / 110, P 80, RR 14• Alert, O x 3Alert, O x 3
No facial droopNo facial droop No UE driftNo UE drift Speech fluentSpeech fluent

Question 1Question 1
Can vertigo be the sole presenting complaint of Can vertigo be the sole presenting complaint of posterior circulation ischemia?posterior circulation ischemia?
a)a) YesYes
b)b) NoNo

Posterior Circulation Stroke: AnatomyPosterior Circulation Stroke: Anatomy

Emergency Department PresentationEmergency Department Presentation
• Clinical Findings: Depends on the Clinical Findings: Depends on the syndromesyndrome Range: asymptomatic to comatoseRange: asymptomatic to comatose
• The 5 DsThe 5 Ds: Dizziness, Diplopia, : Dizziness, Diplopia, Dysarthria, Dysphagia, DystaxiaDysarthria, Dysphagia, Dystaxia
• Hallmarks: Hallmarks: Crossed findingsCrossed findings Cranial nerve deficits - IpsilateralCranial nerve deficits - Ipsilateral Motor / Sens deficits - Motor / Sens deficits -
ContralateralContralateral

Lee et al. Cerebellar infarction presenting Lee et al. Cerebellar infarction presenting isolated vertigo. Neurology 2006; 67:1178-1183isolated vertigo. Neurology 2006; 67:1178-1183
• 240 consecutive patients with confirmed 240 consecutive patients with confirmed cerebellar infarction by MRIcerebellar infarction by MRI
• 25 patients presented with isolated 25 patients presented with isolated spontaneous prolonged vertigo spontaneous prolonged vertigo with with imbalanceimbalance
• ““Cerebellar infarction simulating vestibular Cerebellar infarction simulating vestibular neuritis is more common than previously neuritis is more common than previously thought”thought”

Pitfalls in the diagnosis of cerebellar infarction. Pitfalls in the diagnosis of cerebellar infarction. Acad Emerg Med 2007:14:63-68Acad Emerg Med 2007:14:63-68
• Retrospective chart review: 15 cases of Retrospective chart review: 15 cases of misdiagnosismisdiagnosis
• 12 patients presented with “dizziness”12 patients presented with “dizziness”• 7 patients were younger than 50 and 7 patients were younger than 50 and
presented with headache and dizzinesspresented with headache and dizziness• Majority did not have gait / coordination Majority did not have gait / coordination
testedtested

Pitfalls in the diagnosis of cerebellar infarction. Pitfalls in the diagnosis of cerebellar infarction. Acad Emerg Med 2007:14:63-68Acad Emerg Med 2007:14:63-68
• All of the patients had initial CT read as normalAll of the patients had initial CT read as normal• ED diagnosisED diagnosis
migraine, gastroenteritis, presyncopemigraine, gastroenteritis, presyncope• Final diagnoses: Final diagnoses:
4 vertebral artery dissections4 vertebral artery dissections 3 vertebral artery occlusions3 vertebral artery occlusions 1 atrial thrombus1 atrial thrombus 1 patent foramen ovale1 patent foramen ovale

Can vertigo be the sole presenting complaint of Can vertigo be the sole presenting complaint of posterior circulation ischemia?posterior circulation ischemia?
• Kerber et al. Stroke among patients with dizziness, Kerber et al. Stroke among patients with dizziness, vertigo, imbalance in the ED: a population based vertigo, imbalance in the ED: a population based study. Stroke 2006:37:2484study. Stroke 2006:37:2484 1666 patients presenting with dizziness, vertigo or 1666 patients presenting with dizziness, vertigo or
imbalanceimbalance 9 (0.7%) had a stroke or TIA9 (0.7%) had a stroke or TIA
• If the neurologic exam is normal, including careful If the neurologic exam is normal, including careful assessment of gait and cerebellar function, it is assessment of gait and cerebellar function, it is unlikely that isolated dizziness or vertigo is the result unlikely that isolated dizziness or vertigo is the result of CNS ischemiaof CNS ischemia

Question 2Question 2
Which of the following would you recommend Which of the following would you recommend to EMS:to EMS:
a)a) Do not transportDo not transport
b)b) Transport to the closest hospitalTransport to the closest hospital
c)c) Transport to a designated stroke centerTransport to a designated stroke center

Stroke Centers: The ThesisStroke Centers: The Thesis
• Thrombolytic and other interventions Thrombolytic and other interventions are effective treatments in improving are effective treatments in improving outcomes from acute strokeoutcomes from acute stroke
• Protocols facilitate efficient resource Protocols facilitate efficient resource utilization and lead to improved utilization and lead to improved outcomesoutcomes
• Failure to adhere to protocols Failure to adhere to protocols increase morbidity and mortalityincrease morbidity and mortality

11 elements of a Primary Stroke Center11 elements of a Primary Stroke CenterJAMA 2000; 283:3102-3109 JAMA 2000; 283:3102-3109
• EMS integrated into the acute stroke responseEMS integrated into the acute stroke response• Acute stroke team available 24 / 7 Acute stroke team available 24 / 7 • Written care protocols Written care protocols • ED integrated into the acute stroke teamED integrated into the acute stroke team• Stroke unitStroke unit• Neurosurgical services available within 2 hoursNeurosurgical services available within 2 hours• Commitment from the institution Commitment from the institution • Neuroimaging done / interpreted within 45 min of arrivalNeuroimaging done / interpreted within 45 min of arrival• Laboratory services with rapid turn around of testsLaboratory services with rapid turn around of tests• Quality improvement program including a database or Quality improvement program including a database or
registryregistry• Continuing education programContinuing education program

JCAHO Disease Specific Care CertificationJCAHO Disease Specific Care Certification
• Joint initiative between ASA and JCAHOJoint initiative between ASA and JCAHO• Voluntary participationVoluntary participation
Approximately 1000 centers Approximately 1000 centers certified(25%)certified(25%)
• Premise is that accreditation process will Premise is that accreditation process will drive quality measures and improve drive quality measures and improve outcomesoutcomes
• No emergency medicine society has No emergency medicine society has endorsed this initiativeendorsed this initiative t-PA controversyt-PA controversy OvercrowdingOvercrowding Medical legal implicationsMedical legal implications


Is there a standard of care?
• Canadian Association of Canadian Association of
Emergency PhysiciansEmergency Physicians
• American Academy of American Academy of
Emergency MedicineEmergency Medicine
• Society for Academic Society for Academic
Emergency MedicineEmergency Medicine
• American College of American College of
Emergency PhysiciansEmergency Physicians

American College of Emergency American College of Emergency PhysiciansPhysicians
• IV t-PA may be an efficacious therapy for IV t-PA may be an efficacious therapy for the management of acute ischemic stroke if the management of acute ischemic stroke if properly used incorporating the guidelines properly used incorporating the guidelines established by the NINDSestablished by the NINDS
• The decision for an ED to use IV t-PA for The decision for an ED to use IV t-PA for acute stroke should begin at the institutional acute stroke should begin at the institutional level with commitments from hospital level with commitments from hospital administration, the ED, neurology, administration, the ED, neurology, neurosurgery, radiology, and laboratory neurosurgery, radiology, and laboratory services to ensure that the systems services to ensure that the systems necessary for the safe use of fibrinolytic necessary for the safe use of fibrinolytic agents are in place.agents are in place.

Case Case
• Patient is transported to the closest Patient is transported to the closest hospitalhospital BP- 190 / 110, P-80, RR-14, 98%, BS BP- 190 / 110, P-80, RR-14, 98%, BS
110110 Alert, Ox3; NAD Alert, Ox3; NAD Heart and lungs: “normal”Heart and lungs: “normal” CN: “intact”CN: “intact” Sensation: “intact”Sensation: “intact” ECG: normal sinus rhythmECG: normal sinus rhythm

Question 3Question 3
Which of the following would you recommend?Which of the following would you recommend?
a)a) Discharge with PMD follow upDischarge with PMD follow up
b)b) Discharge on increased aspirinDischarge on increased aspirin
c)c) Discharge on clopidogrelDischarge on clopidogrel
d)d) Discharge on ASA / dipyridamoleDischarge on ASA / dipyridamole
e)e) Admit to the hospitalAdmit to the hospital

TIA and StrokeTIA and Stroke
• Johnston, et al. JAMA 2000; 284:2901Johnston, et al. JAMA 2000; 284:2901 Follow-up of 1707 ED patients diagnosed Follow-up of 1707 ED patients diagnosed
with TIAwith TIA Stroke rate at 90 days was 10.5%Stroke rate at 90 days was 10.5%
• Half of these occurred in the first 48 hours Half of these occurred in the first 48 hours after ED presentationafter ED presentation
• Gladstone, et al. CMAJ 2004; 170:1099-1104Gladstone, et al. CMAJ 2004; 170:1099-1104 371 consecutive patients with TIA 371 consecutive patients with TIA 8% ischemic stroke in 30 days; ½ within 48 8% ischemic stroke in 30 days; ½ within 48
hourshours• 12% in motor deficit group12% in motor deficit group

Patients at highest risk for stroke after TIAPatients at highest risk for stroke after TIA
• Age > 60Age > 60• Blood pressure elevationBlood pressure elevation• Clinical feature:Clinical feature:
Focal weaknessFocal weakness Speech ImpairmentSpeech Impairment
• DiabetesDiabetes• Duration > 60 minutesDuration > 60 minutes

ED DispositionED DispositionED DispositionED Disposition
• Consider ED discharge if:Consider ED discharge if: Further testing will not change Further testing will not change
treatmenttreatment Prior work-upPrior work-up Not a candidate for CEA or Not a candidate for CEA or
anticoagulationanticoagulation• ECGECG• Cardiac echoCardiac echo• Carotid ultrasoundCarotid ultrasound

Case Case
• Discharge diagnosis: “Dizziness – resolved”Discharge diagnosis: “Dizziness – resolved” Limit alcohol useLimit alcohol use Return to ED if symptoms reoccurReturn to ED if symptoms reoccur Call your doctor in the amCall your doctor in the am

Case ContinuedCase Continued
• 5 days later while visiting son, patient 5 days later while visiting son, patient acutely developed vertigo, left sided facial acutely developed vertigo, left sided facial droop, right sided weakness, slurred speechdroop, right sided weakness, slurred speech
• Lethargic with decreased gag Lethargic with decreased gag • BP 210 / 120, P 110, RR 14, POx 92% RABP 210 / 120, P 110, RR 14, POx 92% RA• BS 110BS 110• Transported to the same ED and arrived Transported to the same ED and arrived
within 45 minutes of symptom onsetwithin 45 minutes of symptom onset

Case Case
• CT obtained and showed no blood, no edemaCT obtained and showed no blood, no edema• ““Clot buster” treatment discussed with the Clot buster” treatment discussed with the
family who give consent for treatmentfamily who give consent for treatment• t-PA box is opened and only contains Retaplaset-PA box is opened and only contains Retaplase
There is no alteplase in the hospitalThere is no alteplase in the hospital• Regional stroke center contacted and Regional stroke center contacted and
arrangements made for aero-medical transportarrangements made for aero-medical transport• Patient is intubatedPatient is intubated

Question 4Question 4
How would you manage the blood How would you manage the blood pressure?pressure?
a)a) No BP interventionNo BP intervention
b)b) Labetolol IVLabetolol IV
c)c) Nicardipine IVNicardipine IV
d)d) Nitroprusside IVNitroprusside IV
e)e) Nitroglycerin pasteNitroglycerin paste

Case Case
• The patient arrived at the stroke center 2 The patient arrived at the stroke center 2 hours and 15 minutes from the onset of hours and 15 minutes from the onset of symptoms)symptoms)
• BP 160 / 90BP 160 / 90• CT was CT was not not sent with the patientsent with the patient
decision made to repeat the studydecision made to repeat the study

Question 5Question 5
CT showed no infarct, edema, or hemorrhage 3 CT showed no infarct, edema, or hemorrhage 3 hours and 30 minutes post symptom onset. hours and 30 minutes post symptom onset. Which of the following would you Which of the following would you recommend?recommend?
a)a) NothingNothing
b)b) Intravenous t-PAIntravenous t-PA
c)c) Intra-arterial t-PA / clot retrivalIntra-arterial t-PA / clot retrival

Indication and UsageIndication and Usage• tPA is indicated for the management of acute ischemic stroke in adults to improve
neurological recovery and reduce the incidence of disability• Treatment should only be initiated within 3 hours after the onset of stroke
symptoms, and after exclusion of intracranial hemorrhage by a CT scan or other diagnostic imaging method sensitive for the presence of hemorrhage (see CONTRAINDICATIONS in the full Prescribing Information)
Appropriate Treatment With tPA: Appropriate Treatment With tPA: Bleeding RiskBleeding Risk
Bleeding RiskBleeding Risk• The most common complication encountered during tPA treatment is bleeding • The rate of symptomatic intracranial hemorrhage* was 6.4% in the NINDS trials • The type of bleeding associated with thrombolytic therapy can be divided into 2 broad
categories: Internal bleeding, involving intracranial and retroperitoneal sites, or the
gastrointestinal, genitourinary, or respiratory tract Superficial or surface bleeding, observed mainly at invaded or disturbed
sites (eg, venous cutdowns, arterial punctures, sites of recent surgical intervention)
• Should serious bleeding (not controlled by local pressure) occur, the infusion of tPA should be terminated immediately

Appropriate Treatment With tPA: Appropriate Treatment With tPA: Contraindications & Selected Eligibility ConsiderationsContraindications & Selected Eligibility Considerations
Contraindications• Evidence of intracranial hemorrhage on
pretreatment evaluation • Suspicion of subarachnoid hemorrhage on
pretreatment evaluation • Intracranial or intraspinal surgery, serious
head trauma, or stroke in the previous 3 months
• History of intracranial hemorrhage • Active internal bleeding • Intracranial neoplasm, arteriovenous
malformation, or aneurysm • Known bleeding diathesis • Seizure at the onset of stroke • Uncontrolled hypertension at time of
treatment (ie, >185 mm Hg systolic or >110 mm Hg diastolic)
Selected eligibility considerations Included in the AHA/ASA 2007 Guidelines
• Diagnosis of ischemic stroke causing measurable neurological deficit
• No gastrointestinal or urinary tract hemorrhage in previous 21 days
• No major surgery in the previous 14 days• No arterial puncture at a noncompressible
site in the previous 7 days• Not taking an oral anticoagulant or, if
anticoagulant being taken, INR ≤1.7• If receiving heparin in previous 48 hours,
aPTT must be in normal range.• Platelet count ≥100,000/mm3
• Blood glucose concentration ≥50 mg/dL • No seizure with postictal residual
neurological impairments• CT does not show a multilobar infarction
(hypodensity >1/3 cerebral hemisphere).

tPA Should Be Used With Caution tPA Should Be Used With Caution in Certain Patientsin Certain Patients
• Patients with severe neurologic deficit (eg, NIHSS >22) Patients with severe neurologic deficit (eg, NIHSS >22) at presentationat presentation
• Patients with major and early infarct signs on a cranial Patients with major and early infarct signs on a cranial CT scan (eg, substantial edema, mass effect, or CT scan (eg, substantial edema, mass effect, or midline shift) midline shift)
• Patients of advanced age (eg, >75 years)Patients of advanced age (eg, >75 years)• Due to the increased risk of misdiagnosis of acute Due to the increased risk of misdiagnosis of acute
ischemic stroke, special diligence is required in making ischemic stroke, special diligence is required in making this diagnosis in patients whose blood glucose values this diagnosis in patients whose blood glucose values are <50 mg/dL or >400 mg/dLare <50 mg/dL or >400 mg/dL
• Patients with minor strokes or rapidly resolving Patients with minor strokes or rapidly resolving symptoms symptoms
Alteplase full Prescribing Information 2005.

Case Study: OutcomeCase Study: Outcome
• Patient did not receive t-PA Patient did not receive t-PA • 6 month modified Rankin scale score: 36 month modified Rankin scale score: 3
Ambulate with walkerAmbulate with walker• Patient does well enough to sue:Patient does well enough to sue:
EMS for not taking him to a stroke centerEMS for not taking him to a stroke center The first emergency physician for failure to The first emergency physician for failure to
diagnosediagnose The second EP for not treating with t-PAThe second EP for not treating with t-PA
• EP sues hospital for not having alteplaseEP sues hospital for not having alteplase Stroke Center physicians for delay in care Stroke Center physicians for delay in care
(repeated CT) and failure to treat(repeated CT) and failure to treat

Do you want to take the case for:Do you want to take the case for:
a)a) The plaintiffThe plaintiff
b)b) The defenseThe defense

ConclusionsConclusions
• A (documented) systematic neurologic A (documented) systematic neurologic evaluation is critical to minimizing risk . . . evaluation is critical to minimizing risk . . . And providing good patient careAnd providing good patient care
• EMS plays a pivotal role in acute stroke care EMS plays a pivotal role in acute stroke care and is assuming increasing liability and is assuming increasing liability associated with their decision makingassociated with their decision making
• Alteplase is a FDA approved treatment for Alteplase is a FDA approved treatment for acute ischemic stroke and therefore a acute ischemic stroke and therefore a decision to not use it for qualified patients decision to not use it for qualified patients must be supported in the medical recordmust be supported in the medical record