stroke ischemic
18
Ischemic Stroke Author: Edward C Jauch, MD, MS, FAHA, FACEP; Chief Editor: Helmi L Lutsep, MD more... Updated: Jan 20, 2015 Practice Essentials Ischemic stroke (see the image below) is characterized by the sudden loss of blood circulation to an area of the brain, resulting in a corresponding loss of neurologic function. Acute ischemic stroke is caused by thrombotic or embolic occlusion of a cerebral artery and is more common than hemorrhagic stroke. Maximum intensity projection (MIP) image from a computed tomography angiogram (CTA) demonstrates a filling defect or high grade stenosis at the branching point of the right middle cerebral artery (MCA) trunk (red circle), suspicious for thrombus or embolus. CTA is highly accurate in detecting large vessel stenosis and occlusions, which account for approximately one third of ischemic strokes. See Acute Stroke, a Critical Images slideshow, for more information on incidence, presentation, intervention, and additional resources. Essential update: Study indicates intraarterial treatment improves functional recovery in acute ischemic stroke A randomized clinical trial from the Netherlands indicates that endovascular intervention benefits functional outcomes in patients with acute ischemic stroke resulting from a proximal intracranial arterial occlusion. In the study, by Berkhemer et al, 500 patients were randomized to receive intraarterial treatment (within 6 hours of symptom onset) or usual treatment alone. Although 89% of the patients were treated with tissuetype plasminogen activator (tPA) prior to randomization, only those who were found on computed tomography (CT) angiography to still have a proximal arterial occlusion were entered into the study. In most of the patients who received intraarterial treatment, the procedure was performed with latestgeneration stent retrievers. [1, 2] The investigators found that at 90 days, the rate of functional independence (modified Rankin scale score of 02) in the intraarterial treatment group was 32.6%, compared with 19.1% in the usualtreatmentonly group, while after 5 7 days, the National Institutes of Health Stroke Scale (NIHSS) score was an average of 2.9 points lower in the intra arterial treatment patients than it was in the other group. The two groups did not differ significantly with regard to the rate of morality or symptomatic intracerebral hemorrhage. Signs and symptoms Consider stroke in any patient presenting with acute neurologic deficit or any alteration in level of consciousness. Common stroke signs and symptoms include the following: Abrupt onset of hemiparesis, monoparesis, or (rarely) quadriparesis Hemisensory deficits Monocular or binocular visual loss Visual field deficits Diplopia Dysarthria Facial droop Ataxia Vertigo (rarely in isolation) Nystagmus Aphasia Sudden decrease in level of consciousness Although such symptoms can occur alone, they are more likely to occur in combination. No historical feature distinguishes ischemic from hemorrhagic stroke, although nausea, vomiting, headache, and sudden change in level of consciousness are more common in hemorrhagic strokes. In younger patients, a history of recent trauma, coagulopathies, illicit drug use (especially cocaine), migraines, or use of oral contraceptives should be elicited. With the availability of fibrinolytic therapy for acute ischemic stroke in selected patients, the physician must be able to perform a brief but accurate neurologic examination on patients with suspected stroke syndromes. The goals of the neurologic examination include the following: Confirming the presence of a stroke syndrome Distinguishing stroke from stroke mimics Establishing a neurologic baseline, should the patient's condition improve or deteriorate
description
ischemic stroke
Transcript of stroke ischemic
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 1/18
IschemicStrokeAuthor:EdwardCJauch,MD,MS,FAHA,FACEPChiefEditor:HelmiLLutsep,MDmore...
Updated:Jan20,2015
PracticeEssentialsIschemicstroke(seetheimagebelow)ischaracterizedbythesuddenlossofbloodcirculationtoanareaofthebrain,resultinginacorrespondinglossofneurologicfunction.Acuteischemicstrokeiscausedbythromboticorembolicocclusionofacerebralarteryandismorecommonthanhemorrhagicstroke.
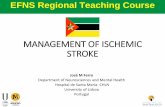
Maximumintensityprojection(MIP)imagefromacomputedtomographyangiogram(CTA)demonstratesafillingdefectorhighgradestenosisatthebranchingpointoftherightmiddlecerebralartery(MCA)trunk(redcircle),suspiciousforthrombusorembolus.CTAishighlyaccurateindetectinglargevesselstenosisandocclusions,whichaccountforapproximatelyonethirdofischemicstrokes.
SeeAcuteStroke,aCriticalImagesslideshow,formoreinformationonincidence,presentation,intervention,andadditionalresources.
Essentialupdate:Studyindicatesintraarterialtreatmentimprovesfunctionalrecoveryinacuteischemicstroke
ArandomizedclinicaltrialfromtheNetherlandsindicatesthatendovascularinterventionbenefitsfunctionaloutcomesinpatientswithacuteischemicstrokeresultingfromaproximalintracranialarterialocclusion.Inthestudy,byBerkhemeretal,500patientswererandomizedtoreceiveintraarterialtreatment(within6hoursofsymptomonset)orusualtreatmentalone.Although89%ofthepatientsweretreatedwithtissuetypeplasminogenactivator(tPA)priortorandomization,onlythosewhowerefoundoncomputedtomography(CT)angiographytostillhaveaproximalarterialocclusionwereenteredintothestudy.Inmostofthepatientswhoreceivedintraarterialtreatment,theprocedurewasperformedwithlatestgenerationstentretrievers.[1,2]
Theinvestigatorsfoundthatat90days,therateoffunctionalindependence(modifiedRankinscalescoreof02)intheintraarterialtreatmentgroupwas32.6%,comparedwith19.1%intheusualtreatmentonlygroup,whileafter57days,theNationalInstitutesofHealthStrokeScale(NIHSS)scorewasanaverageof2.9pointslowerintheintraarterialtreatmentpatientsthanitwasintheothergroup.Thetwogroupsdidnotdiffersignificantlywithregardtotherateofmoralityorsymptomaticintracerebralhemorrhage.
Signsandsymptoms
Considerstrokeinanypatientpresentingwithacuteneurologicdeficitoranyalterationinlevelofconsciousness.Commonstrokesignsandsymptomsincludethefollowing:
Abruptonsetofhemiparesis,monoparesis,or(rarely)quadriparesisHemisensorydeficitsMonocularorbinocularvisuallossVisualfielddeficitsDiplopiaDysarthriaFacialdroopAtaxiaVertigo(rarelyinisolation)NystagmusAphasiaSuddendecreaseinlevelofconsciousness
Althoughsuchsymptomscanoccuralone,theyaremorelikelytooccurincombination.Nohistoricalfeaturedistinguishesischemicfromhemorrhagicstroke,althoughnausea,vomiting,headache,andsuddenchangeinlevelofconsciousnessaremorecommoninhemorrhagicstrokes.Inyoungerpatients,ahistoryofrecenttrauma,coagulopathies,illicitdruguse(especiallycocaine),migraines,oruseoforalcontraceptivesshouldbeelicited.
Withtheavailabilityoffibrinolytictherapyforacuteischemicstrokeinselectedpatients,thephysicianmustbeabletoperformabriefbutaccurateneurologicexaminationonpatientswithsuspectedstrokesyndromes.Thegoalsoftheneurologicexaminationincludethefollowing:
ConfirmingthepresenceofastrokesyndromeDistinguishingstrokefromstrokemimicsEstablishinganeurologicbaseline,shouldthepatient'sconditionimproveordeteriorate
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 2/18
Establishingstrokeseverity,usingastructuredneurologicexamandscore(NationalInstitutesofHealthStrokeScale[NIHSS])toassistinprognosisandtherapeuticselection
Essentialcomponentsoftheneurologicexaminationincludethefollowingevaluations:
CranialnervesMotorfunctionSensoryfunctionCerebellarfunctionGaitDeeptendonreflexesLanguage(expressiveandreceptivecapabilities)Mentalstatusandlevelofconsciousness
Theskullandspinealsoshouldbeexamined,andsignsofmeningismusshouldbesought.
SeeClinicalPresentationformoredetail.
Diagnosis
Emergentbrainimagingisessentialforconfirmingthediagnosisofischemicstroke.Noncontrastcomputedtomography(CT)scanningisthemostcommonlyusedformofneuroimagingintheacuteevaluationofpatientswithapparentacutestroke.Thefollowingneuroimagingtechniquesarealsoused:
CTangiographyandCTperfusionscanningMagneticresonanceimaging(MRI)CarotidduplexscanningDigitalsubtractionangiography
Lumbarpuncture
AlumbarpunctureisrequiredtoruleoutmeningitisorsubarachnoidhemorrhagewhentheCTscanisnegativebuttheclinicalsuspicionremainshigh
Laboratorystudies
Laboratorytestsperformedinthediagnosisandevaluationofischemicstrokeincludethefollowing:
Completebloodcount(CBC):Abaselinestudythatmayrevealacauseforthestroke(eg,polycythemia,thrombocytosis,thrombocytopenia,leukemia)orprovideevidenceofconcurrentillness(eg,anemia)Basicchemistrypanel:Abaselinestudythatmayrevealastrokemimic(eg,hypoglycemia,hyponatremia)orprovideevidenceofconcurrentillness(eg,diabetes,renalinsufficiency)Coagulationstudies:MayrevealacoagulopathyandareusefulwhenfibrinolyticsoranticoagulantsaretobeusedCardiacbiomarkers:ImportantbecauseoftheassociationofcerebralvasculardiseaseandcoronaryarterydiseaseToxicologyscreening:Mayassistinidentifyingintoxicatedpatientswithsymptoms/behaviormimickingstrokesyndromesPregnancytesting:Aurinepregnancytestshouldbeobtainedforallwomenofchildbearingagewithstrokesymptomsrecombinanttissuetypeplasminogenactivator(rtPA)isapregnancyclassCagentArterialbloodgasanalysis:Inselectedpatientswithsuspectedhypoxemia,arterialbloodgasdefinestheseverityofhypoxemiaandmaybeusedtodetectacidbasedisturbances
SeeWorkupformoredetail.
Management
Thegoalfortheemergentmanagementofstrokeistocompletethefollowingwithin60minutesofpatientarrival[3]:
Assessairway,breathing,andcirculation(ABCs)andstabilizethepatientasnecessaryCompletetheinitialevaluationandassessment,includingimagingandlaboratorystudiesInitiatereperfusiontherapy,ifappropriate
Criticaltreatmentdecisionsfocusonthefollowing:
TheneedforairwaymanagementOptimalbloodpressurecontrolIdentifyingpotentialreperfusiontherapies(eg,intravenousfibrinolysiswithrtPAorintraarterialapproaches)
Involvementofaphysicianwithaspecialinterestinstrokeisideal.Strokecareunitswithspeciallytrainedpersonnelexistandimproveoutcomes.
Ischemicstroketherapiesincludethefollowing:
FibrinolytictherapyAntiplateletagents[4,5]Mechanicalthrombectomy
Treatmentofcomorbidconditionsmayincludethefollowing:
ReducefeverCorrecthypotension/significanthypertensionCorrecthypoxiaCorrecthypoglycemiaManagecardiacarrhythmiasManagemyocardialischemia
Strokeprevention
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 3/18
Primarystrokepreventionreferstothetreatmentofindividualswithnoprevioushistoryofstroke.Measuresmayincludeuseofthefollowing:
PlateletantiaggregantsStatinsExerciseLifestyleinterventions(eg,smokingcessation,alcoholmoderation)
Secondarypreventionreferstothetreatmentofindividualswhohavealreadyhadastroke.Measuresmayincludeuseofthefollowing:
PlateletantiaggregantsAntihypertensivesStatinsLifestyleinterventions
SeeTreatmentandMedicationformoredetail.
BackgroundAcuteischemicstroke(AIS)ischaracterizedbythesuddenlossofbloodcirculationtoanareaofthebrain,typicallyinavascularterritory,resultinginacorrespondinglossofneurologicfunction.Alsopreviouslycalledcerebrovascularaccident(CVA)orstrokesyndrome,strokeisanonspecificstateofbraininjurywithneuronaldysfunctionthathasseveralpathophysiologiccauses.Strokescanbedividedinto2types:hemorrhagicorischemic.Acuteischemicstrokeiscausedbythromboticorembolicocclusionofacerebralartery.(Seetheimagebelow.)
Maximumintensityprojection(MIP)imagefromacomputedtomographyangiogram(CTA)demonstratesafillingdefectorhighgradestenosisatthebranchingpointoftherightmiddlecerebralartery(MCA)trunk(redcircle),suspiciousforthrombusorembolus.CTAishighlyaccurateindetectinglargevesselstenosisandocclusions,whichaccountforapproximatelyonethirdofischemicstrokes.
Nearly800,000peoplesufferstrokeseachyearintheUnitedStates8292%ofthesestrokesareischemic.Strokeisthefourthleadingcauseofadultdeathanddisability,resultinginover$72billioninannualcost.[6]
Ischemicandhemorrhagicstrokecannotbereliablydifferentiatedonthebasisofclinicalexaminationfindingsalone.Furtherevaluation,especiallywithbrainimagingtests(ie,computedtomography[CT]scanningormagneticresonanceimaging[MRI]),isrequired.(SeeWorkup.)
Strokecategories
ThesystemofcategorizingstrokedevelopedinthemulticenterTrialofORG10172inAcuteStrokeTreatment(TOAST)dividesischemicstrokesintothefollowing3majorsubtypes[4]:
LargearterySmallvessel,orlacunarCardioembolicinfarction
Largearteryinfarctionsofteninvolvethromboticinsituocclusionsonatheroscleroticlesionsinthecarotid,vertebrobasilar,andcerebralarteries,typicallyproximaltomajorbrancheshowever,largearteryinfarctionsmayalsobecardioembolic.
Cardiogenicemboliareacommonsourceofrecurrentstroke.Theymayaccountforupto20%ofacutestrokesandhavebeenreportedtohavethehighest1monthmortality.[7](SeePathophysiology.)
Treatment
Recanalizationstrategies,includingintravenousrecombinanttissuetypeplasminogenactivator(rtPA)andintraarterialapproaches,attempttoestablishrevascularizationsothatcellsintheischemicpenumbra(ametabolicallyactiveregion,peripheraltotheischemicarea,wherebloodflowisreduced)canberescuedbeforeirreversibleinjuryoccurs.Restoringbloodflowcanmitigatetheeffectsofischemiaonlyifperformedquickly.
TheUSFoodandDrugAdministration(FDA)hasapprovedtheuseofrtPAinpatientswhomeetcriteriasetforthbytheNationalInstituteofNeurologicDisordersandStroke(NINDS).Inparticular,rtPAmustbegivenwithin3hoursofstrokeonsetandonlyafterCTscanninghasruledouthemorrhagicstroke.
OnthebasisofrecentEuropeandata,theAmericanHeartAssociationandAmericanStrokeAssociationrecommendedexpandingthewindowoftreatmentfrom3hoursto4.5hours,withmorestringentexclusioncriteriaforthelaterperiod(seeTreatment).TheFDAhasnotyetapprovedrtPAforthisexpandedindication,butthishasbecomethecommunitystandardinmanyinstitutions.
Otheraspectsoftreatmentforacuteischemicstrokeincludethefollowing:
Treatmentofneurologiccomplications
Supplementaloxygenasrequired
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 4/18
AntiplatelettherapyGlycemiccontrolOptimalbloodpressurecontrolPreventionofhyperthermia
SeealsoHemorrhagicStroke.
AnatomyThebrainisthemostmetabolicallyactiveorganinthebody.Whilerepresentingonly2%ofthebody'smass,itrequires1520%ofthetotalrestingcardiacoutputtoprovidethenecessaryglucoseandoxygenforitsmetabolism.
Knowledgeofcerebrovasculararterialanatomyandtheterritoriessuppliedbythecerebralarteriesisusefulindeterminingwhichvesselsareinvolvedinacutestroke.Atypicalpatternsofbrainischemiathatdonotconformtospecificvasculardistributionsmayindicateadiagnosisotherthanischemicstroke,suchasvenousinfarction.
Arterialdistributions
Inasimplifiedmodel,thecerebralhemispheresaresuppliedby3pairedmajorarteries,specifically,theanterior,middle,andposteriorcerebralarteries.
Theanteriorandmiddlecerebralarteriescarrytheanteriorcirculationandarisefromthesupraclinoidinternalcarotidarteries.Theanteriorcerebralartery(ACA)suppliesthemedialportionofthefrontalandparietallobesandanteriorportionsofbasalgangliaandanteriorinternalcapsule.(Seetheimagebelow.)
Lateralviewofacerebralangiogramillustratesthebranchesoftheanteriorcerebralartery(ACA)andSylviantriangle.ThepericallosalarteryhasbeendescribedtoarisedistaltotheanteriorcommunicatingarteryordistaltotheoriginofthecallosomarginalbranchoftheACA.ThesegmentalanatomyoftheACAhasbeendescribedasfollows:theA1segmentextendsfromtheinternalcarotidartery(ICA)bifurcationtotheanteriorcommunicatingarteryA2extendstothejunctionoftherostrumandgenuofthecorpuscallosumA3extendsintothebendofthegenuofthecorpuscallosumA4andA5extendposteriorlyabovethecallosalbodyandsuperiorportionofthesplenium.TheSylviantriangleoverliestheopercularbranchesofthemiddlecerebralartery(MCA),withtheapexrepresentingtheSylvianpoint.
Themiddlecerebralartery(MCA)suppliesthelateralportionsofthefrontalandparietallobes,aswellastheanteriorandlateralportionsofthetemporallobes,andgivesrisetoperforatingbranchestotheglobuspallidus,putamen,andinternalcapsule.TheMCAisthedominantsourceofvascularsupplytothehemispheres.(Seetheimagesbelow.)
Thesupratentorialvascularterritoriesofthemajorcerebralarteriesaredemonstratedsuperimposedonaxial(left)andcoronal(right)T2weightedimagesthroughthelevelofthebasalgangliaandthalami.Themiddlecerebralartery(MCAred)suppliesthelateralaspectsofthehemispheres,includingthelateralfrontal,parietal,andanteriortemporallobesinsulaandbasalganglia.Theanteriorcerebralartery(ACAblue)suppliesthemedialfrontalandparietallobes.Theposteriorcerebralartery(PCAgreen)suppliesthethalamiandoccipitalandinferiortemporallobes.Theanteriorchoroidalartery(yellow)suppliestheposteriorlimboftheinternalcapsuleandpartofthehippocampusextendingtotheanteriorandsuperiorsurfaceoftheoccipitalhornofthelateralventricle.
Frontalviewofacerebralangiogramwithselectiveinjectionoftheleftinternalcarotidartery(ICA)illustratestheanteriorcirculation.Theanteriorcerebralartery(ACA)consistsoftheA1segmentproximaltotheanteriorcommunicatingartery,withtheA2segmentdistaltoit.Themiddlecerebralartery(MCA)canbedividedinto4segments:theM1(horizontalsegment)extendstotheanteriorbasalportionoftheinsularcortex(thelimeninsulae)andgivesofflaterallenticulostriatebranches,theM2(insularsegment),M3(opercularbranches),andM4(distalcorticalbranchesonthelateralhemisphericconvexities).
Theposteriorcerebralarteriesarisefromthebasilararteryandcarrytheposteriorcirculation.Theposteriorcerebralartery(PCA)givesrisetoperforatingbranchesthatsupplythethalamiandbrainstemandthecorticalbranchestotheposteriorandmedialtemporallobesandoccipitallobes.(SeeTable1,below.)
Thecerebellarhemispheresaresuppliedasfollows:
Inferiorlybytheposteriorinferiorcerebellarartery(PICA),arisingfromthevertebralartery(seetheimagebelow)
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 5/18
Frontalprojectionfromarightvertebralarteryangiogramillustratestheposteriorcirculation.Thevertebralarteriesjointoformthebasilarartery.Theposteriorinferiorcerebellararteries(PICAs)arisefromthedistalvertebralarteries.Theanteriorinferiorcerebellararteries(AICAs)arisefromtheproximalbasilarartery.Thesuperiorcerebellararteries(SICAs)arisedistallyfromthebasilararterypriortoitsbifurcationintotheposteriorcerebralarteries(PCAs).
SuperiorlybythesuperiorcerebellararteryAnterolaterallybytheanteriorinferiorcerebellarartery(AICA),fromthebasilarartery
Table1.VascularSupplytotheBrain(OpenTableinanewwindow)
VASCULARTERRITORY StructuresSuppliedAnteriorCirculation(Carotid)AnteriorCerebralArtery Corticalbranches:medialfrontalandparietallobe
Mediallenticulostriatebranches:caudatehead,globuspallidus,anteriorlimbofinternalcapsule
MiddleCerebralArtery Corticalbranches:lateralfrontalandparietallobeslateralandanteriortemporallobe
Laterallenticulostriatebranches:globuspallidusandputamen,internalcapsule
AnteriorChoroidalArtery Optictracts,medialtemporallobe,ventrolateralthalamus,coronaradiata,posteriorlimboftheinternalcapsule
PosteriorCirculation(Vertebrobasilar)PosteriorCerebralArtery Corticalbranches:occipitallobes,medialandposteriortemporalandparietallobes
Perforatingbranches:brainstem,posteriorthalamusandmidbrain
PosteriorInferiorCerebellarArtery
Inferiorvermisposteriorandinferiorcerebellarhemispheres
AnteriorInferiorCerebellarArtery
Anterolateralcerebellum
SuperiorCerebellarArtery Superiorvermissuperiorcerebellum
PathophysiologyAcuteischemicstrokesresultfromvascularocclusionsecondarytothromboembolicdisease(seeEtiology).Ischemiacausescellhypoxiaanddepletionofcellularadenosinetriphosphate(ATP).WithoutATP,thereisnolongertheenergytomaintainionicgradientsacrossthecellmembraneandcelldepolarization.Influxofsodiumandcalciumionsandpassiveinflowofwaterintothecellleadtocytotoxicedema.[8,9,10]
Ischemiccoreandpenumbra
Anacutevascularocclusionproducesheterogeneousregionsofischemiaintheaffectedvascularterritory.Localbloodflowislimitedtoanyresidualflowinthemajorarterialsourceplusthecollateralsupply,ifany.
Affectedregionswithcerebralbloodflowoflowerthan10mL/100goftissue/minarereferredtocollectivelyasthecore.Thesecellsarepresumedtodiewithinminutesofstrokeonset.[11]
Zonesofdecreasedormarginalperfusion(cerebralbloodflow
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 6/18
systemsfail.Disruptionofcellularmetabolismalsoimpairsnormalsodiumpotassiumplasmamembranepumps,producinganintracellularincreaseinsodium,whichinturnsincreasesintracellularwatercontent.Thiscellularswellingisreferredtoascytotoxicedemaandoccursveryearlyincerebralischemia.
Cerebralischemiaimpairsthenormalsodiumcalciumexchangeproteinalsofoundoncellplasmamembranes.Theresultinginfluxofcalciumleadstothereleaseofanumberofneurotransmitters,includinglargequantitiesofglutamate,whichinturnactivatesNmethylDaspartate(NMDA)andotherexcitatoryreceptorsonotherneurons.
Theseneuronsthenbecomedepolarized,causingfurthercalciuminflux,furtherglutamaterelease,andlocalamplificationoftheinitialischemicinsult.Thismassivecalciuminfluxalsoactivatesvariousdegradativeenzymes,leadingtothedestructionofthecellmembraneandotheressentialneuronalstructures.[12]Freeradicals,arachidonicacid,andnitricoxidearegeneratedbythisprocess,whichleadstofurtherneuronaldamage.
Ischemiaalsodirectlyresultsindysfunctionofthecerebralvasculature,withbreakdownofthebloodbrainbarrieroccurringwithin46hoursafterinfarction.Followingthebarriersbreakdown,proteinsandwaterfloodintotheextracellularspace,leadingtovasogenicedema.Thisproducesgreaterlevelsofbrainswellingandmasseffectthatpeakat35daysandresolveoverthenextseveralweekswithresorptionofwaterandproteins.[13,14]
Withinhourstodaysafterastroke,specificgenesareactivated,leadingtotheformationofcytokinesandotherfactorsthat,inturn,causefurtherinflammationandmicrocirculatorycompromise.[12]Ultimately,theischemicpenumbraisconsumedbytheseprogressiveinsults,coalescingwiththeinfarctedcore,oftenwithinhoursoftheonsetofthestroke.
Infarctionresultsinthedeathofastrocytes,aswellasthesupportingoligodendroglialandmicroglialcells.Theinfarctedtissueeventuallyundergoesliquefactionnecrosisandisremovedbymacrophages,withthedevelopmentofparenchymalvolumeloss.Awellcircumscribedregionofcerebrospinalfluidlikelowdensity,resultingfromencephalomalaciaandcysticchange,iseventuallyseen.Theevolutionofthesechronicchangesmaybeseenintheweekstomonthsfollowingtheinfarction.(Seetheimagesbelow.)
Vasculardistributions:Middlecerebralartery(MCA)infarction.Noncontrastcomputedtomography(CT)scanningdemonstratesalargeacuteinfarctionintheMCAterritoryinvolvingthelateralsurfacesoftheleftfrontal,parietal,andtemporallobes,aswellastheleftinsularandsubinsularregions,withmasseffectandrightwardmidlineshift.Thereissparingofthecaudateheadandatleastpartofthelentiformnucleusandinternalcapsule,whichreceivebloodsupplyfromthelaterallenticulostriatebranchesoftheM1segmentoftheMCA.Notethelackofinvolvementofthemedialfrontallobe(anteriorcerebralartery[ACA]territory),thalami,andparamedianoccipitallobe(posteriorcerebralartery[PCA]territory).
Vasculardistributions:Anteriorcerebralartery(ACA)infarction.Diffusionweightedimageontheleftdemonstrateshighsignalintheparamedianfrontalandhighparietalregions.TheoppositediffusionweightedimageinadifferentpatientdemonstratesrestricteddiffusioninalargerACAinfarctioninvolvingtheleftparamedianfrontalandposteriorparietalregions.Thereisalsoinfarctionofthelateraltemporoparietalregionsbilaterally(bothmiddlecerebralartery[MCA]distributions),greaterontheleftindicatingmultivesselinvolvementandsuggestingemboli.
Vasculardistributions:Posteriorcerebralartery(PCA)infarction.Thenoncontrastcomputedtomography(CT)imagesdemonstratePCAdistributioninfarctioninvolvingtherightoccipitalandinferomedialtemporallobes.Theimageontherightdemonstratesadditionalinvolvementofthethalamus,alsopartofthePCAterritory.
Vasculardistributions:Anteriorchoroidalarteryinfarction.Thediffusionweightedimage(left)demonstrateshighsignalwithassociatedsignaldropoutontheapparentdiffusioncoefficient(ADC)mapinvolvingtheposteriorlimboftheinternalcapsule.Thisisthetypicaldistributionoftheanteriorchoroidalartery,thelastbranchoftheinternalcarotidartery(ICA)beforebifurcatingintotheanteriorandmiddlecerebralarteries.Theanteriorchoroidalarterymayalsoarisefromthemiddlecerebralartery(MCA).
Hemorrhagictransformationofischemicstroke
Hemorrhagictransformationrepresentstheconversionofanischemicinfarctionintoanareaofhemorrhage.Thisisestimatedtooccurin5%ofuncomplicatedischemicstrokes,intheabsenceoffibrinolytictreatment.Hemorrhagictransformationisnotalwaysassociatedwithneurologicdecline,withtheconversionrangingfromthedevelopmentofsmallpetechialhemorrhagestotheformationofhematomasthatproduceneurologicdeclineandmay
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 7/18
necessitatesurgicalevacuationordecompressivehemicraniectomy.
Proposedmechanismsforhemorrhagictransformationincludereperfusionofischemicallyinjuredtissue,eitherfromrecanalizationofanoccludedvesselorfromcollateralbloodsupplytotheischemicterritoryordisruptionofthebloodbrainbarrier.Withdisruptionofthebloodbrainbarrier,redbloodcellsextravasatefromtheweakenedcapillarybed,producingpetechialhemorrhageormorefrankintraparenchymalhematoma.[8,15,16]
Hemorrhagictransformationofanischemicinfarctoccurswithin214dayspostictus,usuallywithinthefirstweek.Itismorecommonlyseenfollowingcardioembolicstrokesandismorelikelytooccurwithlargerinfarctvolumes.[5,8,17]HemorrhagictransformationisalsomorelikelyfollowingadministrationofrtPAinpatientswhosenoncontrastCT(NCCT)scansdemonstrateareasofhypodensity.[18,19,20]
Poststrokecerebraledemaandseizures
Althoughclinicallysignificantcerebraledemacanoccurafteranteriorcirculationischemicstroke,itisthoughttobesomewhatrare(1020%).[3]Edemaandherniationarethemostcommoncausesofearlydeathinpatientswithhemisphericstroke.
Seizuresoccurin223%ofpatientswithinthefirstdaysafterischemicstroke.[3]Afractionofpatientswhohaveexperiencedstrokedevelopchronicseizuredisorders.
EtiologyIschemicstrokesresultfromeventsthatlimitorstopbloodflow,suchasextracranialorintracranialthromboticembolism,thrombosisinsitu,orrelativehypoperfusion.Asbloodflowdecreases,neuronsceasefunctioning.Althougharangeofthresholdshasbeendescribed,irreversibleneuronalischemiaandinjuryisgenerallythoughttobeginatbloodflowratesoflessthan18mL/100goftissue/min,withcelldeathoccurringrapidlyatratesbelow10mL/100goftissue/min
Riskfactors
Riskfactorsforischemicstrokeincludemodifiableandnonmodifiableconditions.Identificationofriskfactorsineachpatientcanuncovercluestothecauseofthestrokeandthemostappropriatetreatmentandsecondarypreventionplan.
Nonmodifiableriskfactorsincludethefollowing(althoughtherearelikelymanyothers):
AgeRaceSexEthnicityHistoryofmigraineheadaches[21]FibromusculardysplasiaHeredity:Familyhistoryofstrokeortransientischemicattacks(TIAs)
Inaprospectivestudyof27,860womenaged45yearsorolderwhowereparticipatingintheWomen'sHealthStudy,Kurthetalfoundthatmigrainewithaurawasastrongriskfactorforanytypeofstroke.Theadjustedincidenceofthisriskfactorper1000womenperyearwassimilartothoseofotherknownriskfactors,includingsystolicbloodpressure180mmHgorhigher,bodymassindex35kg/m2orgreater,historyofdiabetes,familyhistoryofmyocardialinfarction,andsmoking.[22]
Formigrainewithaura,thetotalincidenceofstrokeinthestudywas4.3per1000womenperyear,theincidenceofischemicstrokewas3.4per1000peryear,andtheincidenceofhemorrhagicstrokewas0.8per1000peryear.
Modifiableriskfactorsincludethefollowing[23]:
Hypertension(themostimportant)DiabetesmellitusCardiacdisease:Atrialfibrillation,valvulardisease,heartfailure,mitralstenosis,structuralanomaliesallowingrighttoleftshunting(eg,patentforamenovale),andatrialandventricularenlargementHypercholesterolemiaTIAsCarotidstenosisHyperhomocystinemiaLifestyleissues:Excessivealcoholintake,tobaccouse,illicitdruguse,physicalinactivity[24]ObesityOralcontraceptiveuse/postmenopausalhormoneuseSicklecelldisease
In2014,theAmericanHeartAssociationandtheAmericanStrokeAssociationissuedguidelinesforthereductionofstrokeriskspecificallyinwomen.Thesegenderspecificrecommendationsincludethefollowing[25,26]:
AstrokeriskscoreshouldbedevelopedspecificallyforwomenWomenwithahistoryofhighbloodpressurebeforepregnancyshouldbeconsideredforlowdoseaspirinand/orcalciumsupplementtreatmenttoreducetheriskofpreeclampsiaBloodpressuremedicationmaybeconsideredforpregnantwomenwithmoderatelyhighbloodpressure(150159mmHg/100109mmHg),andpregnantwomenwithseverehighbloodpressure(160/110mmHgorabove)shouldbetreatedWomenshouldbescreenedforhighbloodpressurebeforetheystartusingbirthcontrolpillsbecauseofanincreasedriskofstrokeWomenwithmigraineheadacheswithaurashouldbeencouragedtoquitsmokingtoreducetheriskofstrokeWomenoverage75shouldbescreenedforatrialfibrillation
Geneticandinflammatorymechanisms
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 8/18
Evidencecontinuestoaccumulatethatinflammationandgeneticfactorshaveimportantrolesinthedevelopmentofatherosclerosisand,specifically,instroke.Accordingtothecurrentparadigm,atherosclerosisisnotablandcholesterolstoragedisease,aspreviouslythought,butadynamic,chronic,inflammatoryconditioncausedbyaresponsetoendothelialinjury.
Traditionalriskfactors,suchasoxidizedlowdensitylipoprotein(LDL)cholesterolandsmoking,contributetothisinjury.Ithasbeensuggested,however,thatinfectionsmayalsocontributetoendothelialinjuryandatherosclerosis.
Hostgeneticfactors,moreover,maymodifytheresponsetotheseenvironmentalchallenges,althoughinheritedriskforstrokeislikelymultigenic.Evenso,specificsinglegenedisorderswithstrokeasacomponentofthephenotypedemonstratethepotencyofgeneticsindeterminingstrokerisk.
Anumberofgenesareknowntoincreasesusceptibilitytoischemicstroke.MutationstotheF2andF5genesarerelativelycommoninthegeneralpopulationandincreasetheriskofthrombosis.Mutationsinthefollowinggenesalsoareknowntoincreasetheriskofstroke:
NOS3:Anitricoxidesynthetasegeneinvolvedinvascularrelaxation[27]ALOX5AP:Involvedinthemetabolismofarachidonicacid[28]PRKCH:Involvedinmajorsignaltransductionsystems[29]
Hyperhomocysteinemiaandhomocystinuria
Hyperhomocysteinemiaisimplicatedinthepathogenesisofischemicstroke.Themostcommonconcernismutationsinthe5,10methylenetetrahydrofolatereductase(MTHFR)gene.Inmanypopulations,themutantallelefrequencyreachespolymorphicproportions,andtheriskfactorforcerebrovasculardiseaseisrelatedtotheserumlevelofhomocysteine.Furthermore,inpersonswhoarecompoundheterozygotesforMTHFRmutation,ifelevatedhomocysteineisfounditcanbeloweredwithoralfolicacidtherapy.
Inaddition,hyperhomocysteinemiacanbeseenincystathionebetasynthetase(CBS)deficiency,whichisgenerallyreferredtoashomocystinuria.Thisdisorderisinheritedinanautosomalrecessivemanner.Symptomsusuallymanifestearlyinlife.Patientshaveamarfanoidhabitus,ectopialentis,andmyopiaandgenerallyhaveintellectualdisability.[30]
Thromboemboliceventsarethemostcommoncauseofdeathforpatientswithhomocystinuriaandmaybeofanytype,includingmyocardialinfarction.Theriskofhavingavasculareventinhomocystinuriais50%byage30.[31]ItwaspreviouslysuggestedthatpersonswhoareheterozygousformutationsintheCBSgenemayhaveanincreasedriskofcerebrovasculardiseaseaswell,butseveralmorerecentstudiesonthissubjectfailedtoreplicatethisfinding.
Amyloidangiopathies
Amyloidangiopathiesarealsoknowntoincreaseriskforstrokeanddementia.MutationsintheCST3genearecausativeandareinheritedinanautosomaldominantmanner.Suffererswillhavediffusedepositionofamyloid,includinginthebrain.Theonsetofsymptomsistypicallyinthethirdorfourthdecadeoflife,withdeathoccurringbeforeage60years.TheseangiopathiesappeartobemostcommonintheIcelandicpopulation.[32]
CADASIL
Cerebralarteriopathy,autosomaldominant,withsubcorticalinfarctsandleukoencephalopathy(CADASIL),iscausedbymutationsintheNOTCH3gene.Itaffectsthesmallarteriesofthebrain.Strokelikeepisodestypicallyoccuratameanageof46years,withanagerangeof1967years.Whitematterchangesinthebrainaretypicallyevidentbyyoungadulthoodandprogressovertime.[33]
Migraineheadachesoccurin3040%ofpeoplewithCADASIL.Approximately60%ofsymptomaticindividualshavecognitivedeficits,whichcanstartasearlyasage35years,andmanydevelopmultiinfarctdementia.[34]
Othermutations
Genomewideassociationstudieshaverevealedadditionallocithatarecommonlyassociatedwithischemicstroke.Earlyonsetischemicstrokehasbeenfoundtobeassociatedwith2singlenucleotidepolymorphismson2q23.3.[35]
LargevesselstrokehasbeenassociatedwithvariationsinHDAC9,PITX2,andZFHX3.[36]HDAC9islocatedon7p21.1,whilePITX2andZFHX3arelocatedon9p21.Itisofnotethatthe9p21locushasalsobeenassociatedwithcardiovasculardisease.
Apolymorphismat2q36.3wasfoundinwhichadenosinesubstitutionconferredalowerriskofischemicstrokeinanadditivefashion.[37]Anadditionalstudysuggestedanassociationbetweenischemicstrokeandalocuson12p13.[38]
Formoreinformation,seeGeneticandInflammatoryMechanismsinStroke.Inaddition,completeinformationonthefollowingmetabolicdiseasesandstrokecanbefoundinthefollowingmainarticles:
MethylmalonicAcidemiaHomocystinuria/HomocysteinemiaFabryDiseaseMELASSyndromeHyperglycemiaandHypoglycemiainStroke
Largearteryocclusion
Largearteryocclusiontypicallyresultsfromembolizationofatheroscleroticdebrisoriginatingfromthecommonorinternalcarotidarteriesorfromacardiacsource.Asmallernumberoflargearteryocclusionsmayarisefromplaqueulcerationandinsituthrombosis.LargevesselischemicstrokesmorecommonlyaffecttheMCAterritory,withtheACAterritoryaffectedtoalesserdegree.(Seetheimagesbelow.)
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 9/18
Noncontrastcomputedtomography(CT)scanina52yearoldmanwithahistoryofworseningrightsidedweaknessandaphasiademonstratesdiffusehypodensityandsulcaleffacementwithmasseffectinvolvingtheleftanteriorandmiddlecerebralarteryterritoriesconsistentwithacuteinfarction.Therearescatteredcurvilinearareasofhyperdensitynotedsuggestiveofdevelopingpetechialhemorrhageinthislargeareaofinfarction.
Magneticresonanceangiogram(MRA)ina52yearoldmandemonstratesocclusionoftheleftprecavernoussupraclinoidinternalcarotidartery(ICA,redcircle),occlusionorhighgradestenosisofthedistalmiddlecerebralartery(MCA)trunkandattenuationofmultipleM2branches.Thediffusionweightedimage(right)demonstrateshighsignalconfirmedtobetruerestricteddiffusionontheapparentdiffusioncoefficient(ADC)mapconsistentwithacuteinfarction.
Maximumintensityprojection(MIP)imagefromacomputedtomographyangiogram(CTA)demonstratesafillingdefectorhighgradestenosisatthebranchingpointoftherightmiddlecerebralartery(MCA)trunk(redcircle),suspiciousforthrombusorembolus.CTAishighlyaccurateindetectinglargevesselstenosisandocclusions,whichaccountforapproximatelyonethirdofischemicstrokes.
Lacunarstrokes
Lacunarstrokesrepresent1320%ofallischemicstrokes.TheyresultfromocclusionofthepenetratingbranchesoftheMCA,thelenticulostriatearteries,orthepenetratingbranchesofthecircleofWillis,vertebralartery,orbasilarartery.Thegreatmajorityoflacunarstrokesarerelatedtohypertension.(Seetheimagebelow.)
Axialnoncontrastcomputedtomography(CT)scandemonstratesafocalareaofhypodensityintheleftposteriorlimboftheinternalcapsuleina60yearoldmanwithacuteonsetofrightsidedweakness.Thelesiondemonstrateshighsignalonthefluidattenuatedinversionrecovery(FLAIR)sequence(middleimage)anddiffusionweightedmagneticresonanceimaging(MRI)scan(rightimage),withlowsignalontheapparentdiffusioncoefficient(ADC)mapsindicatinganacutelacunarinfarction.Lacunarinfarctsaretypicallynomorethan1.5cminsizeandcanoccurinthedeepgraymatterstructures,coronaradiata,brainstem,andcerebellum.
Causesoflacunarinfarctsincludethefollowing:
MicroatheromaLipohyalinosisFibrinoidnecrosissecondarytohypertensionorvasculitisHyalinearteriosclerosisAmyloidangiopathyMicroemboli
Embolicstrokes
Cardiogenicembolimayaccountforupto20%ofacutestrokes.Embolimayarisefromtheheart,theextracranialarteries,includingtheaorticarchor,rarely,therightsidedcirculation(paradoxicalemboli)withsubsequentpassagethroughapatentforamenovale.[39]Sourcesofcardiogenicemboliincludethefollowing:
Valvularthrombi(eg,inmitralstenosisorendocarditisorfromuseofaprostheticvalve)Muralthrombi(eg,inmyocardialinfarction,atrialfibrillation,dilatedcardiomyopathy,orseverecongestiveheartfailure)Atrialmyxoma
Acutemyocardialinfarctionisassociatedwitha23%incidenceofembolicstrokes,ofwhich85%occurinthefirstmonthaftertheinfarction.[40]Embolicstrokestendtohaveasuddenonset,andneuroimagingmaydemonstratepreviousinfarctsinseveralvascularterritoriesormayshowcalcificemboli.
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 10/18
Cardioembolicstrokesmaybeisolated,multipleandinasinglehemisphere,orscatteredandbilateralthelatter2typesindicatemultiplevasculardistributionsandaremorespecificforcardioembolism.Multipleandbilateralinfarctscanbetheresultofembolicshowersorrecurrentemboli.Otherpossibilitiesforsingleandbilateralhemisphericinfarctionsincludeembolioriginatingfromtheaorticarchanddiffusethromboticorinflammatoryprocessesthatcanleadtomultiplesmallvesselocclusions.(Seetheimagebelow.)[41,42]
Cardioembolicstroke:Axialdiffusionweightedimagesdemonstratescatteredfociofhighsignalinthesubcorticalanddeepwhitematterbilaterallyinapatientwithaknowncardiacsourceforembolization.Anareaoflowsignalintheleftgangliocapsularregionmaybesecondarytopriorhemorrhageorsubacutetochroniclacunarinfarct.Recurrentstrokesaremostcommonlysecondarytocardioembolicphenomenon.
Formoreinformation,seeCardioembolicStroke.
Thromboticstrokes
Thrombogenicfactorsmayincludeinjurytoandlossofendothelialcellsthislossexposesthesubendotheliumandresultsinplateletactivationbythesubendothelium,activationoftheclottingcascade,inhibitionoffibrinolysis,andbloodstasis.Thromboticstrokesaregenerallythoughttooriginateonrupturedatheroscleroticplaques.Arterialstenosiscancauseturbulentbloodflow,whichcanpromotethrombusformationatherosclerosis(ie,ulceratedplaques)andplateletadherence.Allcausetheformationofbloodclotsthateitherembolizeoroccludetheartery.
Intracranialatherosclerosismaybethecauseofthromboticstrokeinpatientswithwidespreadatherosclerosis.Inotherpatients,especiallyyoungerpatients,othercausesshouldbeconsidered,includingthefollowing[8,43]:
Hypercoagulablestates(eg,antiphospholipidantibodies,proteinCdeficiency,proteinSdeficiency,pregnancy)SicklecelldiseaseFibromusculardysplasiaArterialdissectionsVasoconstrictionassociatedwithsubstanceabuse(eg,cocaine,amphetamines)
Watershedinfarcts
Vascularwatershed,orborderzone,infarctionsoccuratthemostdistalareasbetweenarterialterritories.Theyarebelievedtobesecondarytoembolicphenomenonortoseverehypoperfusion,asoccurs,forexample,incarotidocclusionorprolongedhypotension.(Seetheimagebelow.)[44,45,46]
Magneticresonanceimaging(MRI)scanwasobtainedina62yearoldmanwithhypertensionanddiabetesandahistoryoftransientepisodesofrightsidedweaknessandaphasia.Thefluidattenuatedinversionrecovery(FLAIR)image(left)demonstratespatchyareasofhighsignalarrangedinalinearfashioninthedeepwhitematter,bilaterally.Thisconfigurationistypicalfordeepborderzone,orwatershed,infarction,inthiscasetheanteriorandposteriormiddlecerebralartery(MCA)watershedareas.Theleftsidedinfarctshavecorrespondinglowsignalontheapparentdiffusioncoefficient(ADC)map(right),signifyingacuity.Anoldleftposteriorparietalinfarctisnotedaswell.
Flowdisturbances
Strokesymptomscanresultfrominadequatecerebralbloodflowbecauseofdecreasedbloodpressure(andspecifically,decreasedcerebralperfusionpressure)orasaresultofhematologichyperviscosityfromsicklecelldiseaseorotherhematologicillnesses,suchasmultiplemyelomaandpolycythemiavera.Intheseinstances,cerebralinjurymayoccurinthepresenceofdamagetootherorgansystems.Formoreinformation,seeBloodDyscrasiasandStroke.
Epidemiology
StrokeistheleadingcauseofdisabilityandthefourthleadingcauseofdeathintheUnitedStates.[47,48]Eachyear,approximately795,000peopleintheUnitedStatesexperiencenew(610,000people)orrecurrent(185,000people)stroke.[6]Epidemiologicstudiesindicatethat8292%ofstrokesintheUnitedStatesareischemic.
AccordingtotheWorldHealthOrganization(WHO),15millionpeoplesufferstrokeworldwideeachyear.Ofthese,5milliondie,andanother5millionareleftpermanentlydisabled.[49]
Race,sex,andagerelateddemographics
IntheUnitedStates,blackshaveanageadjustedriskofdeathfromstrokethatis1.49timesthatofwhites.[50]Hispanicshavealoweroverallincidenceofstrokethanwhitesandblacksbutmorefrequentlacunarstrokesandstrokeatanearlierage.
Menareathigherriskforstrokethanwomenwhitemenhaveastrokeincidenceof62.8per100,000,withdeathbeingthefinaloutcomein26.3%ofcases,whilewomenhaveastrokeincidenceof59per100,000andadeathrateof39.2%.
Althoughstrokeoftenisconsideredadiseaseofelderlypersons,onethirdofstrokesoccurinpersonsyoungerthan
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 11/18
65years.[48]Riskofstrokeincreaseswithage,especiallyinpatientsolderthan64years,inwhom75%ofallstrokesoccur.
PrognosisIntheFraminghamandRochesterstrokestudies,theoverallmortalityrateat30daysafterstrokewas28%,themortalityrateat30daysafterischemicstrokewas19%,andthe1yearsurvivalrateforpatientswithischemicstrokewas77%.However,theprognosisafteracuteischemicstrokevariesgreatlyinindividualpatients,dependingonthestrokeseverityandonthepatientspremorbidcondition,age,andpoststrokecomplications.[4]
AstudyutilizingthelargenationalGetWithTheGuidelinesStrokeregistryfoundthatthebaselineNationalInstitutesofHealthStrokeScale(NIHSS)scorewasthestrongestpredictorofearlymortalityrisk,evenmoresothancurrentlyusedmortalitypredictionmodelsincorporatingmultipleclinicaldata.[51]Cardiogenicemboliareassociatedwiththehighest1monthmortalityinpatientswithacutestroke.
Thepresenceofcomputedtomography(CT)scanevidenceofinfarctionearlyinpresentationhasbeenassociatedwithpooroutcomeandwithanincreasedpropensityforhemorrhagictransformationafterfibrinolytictherapy(seePathophysiology).[5,52,53]Hemorrhagictransformationisestimatedtooccurin5%ofuncomplicatedischemicstrokesintheabsenceoffibrinolytictherapy,althoughitisnotalwaysassociatedwithneurologicdecline.Indeed,hemorrhagictransformationrangesfromthedevelopmentofsmallpetechialhemorrhagestotheformationofhematomasrequiringevacuation.
Acuteischemicstrokehasbeenassociatedwithacutecardiacdysfunctionandarrhythmia,whichthencorrelatewithworsefunctionaloutcomeandmorbidityat3months.Datasuggestthatseverehyperglycemiaisindependentlyassociatedwithpooroutcomeandreducedreperfusioninfibrinolysis,aswellasextensionoftheinfarctedterritory.[54,55,56]
InstrokesurvivorsfromtheFraminghamHeartStudy,31%neededhelpcaringforthemselves,20%neededhelpwhenwalking,and71%hadimpairedvocationalcapacityinlongtermfollowup.Formoreinformation,seetheMedscapeReferencearticleMotorRecoveryinStroke.
PatientEducationPubliceducationmustinvolveallagegroups.Incorporatingstrokeintobasiclifesupport(BLS)andcardiopulmonaryresuscitation(CPR)curriculaisjustonewaytoreachayoungeraudience.Avenuestoreachanaudiencewithahigherstrokeriskcouldincludelocalchurches,employers,andseniororganizationstopromotestrokeawareness.
TheAmericanStrokeAssociation(ASA)advisesthepublictobeawareofthesymptomsofstrokethatareeasilyrecognized,includingthesuddenonsetofanyofthefollowing,andtocall911immediately:
Numbnessorweaknessofface,arm,orleg,especiallyon1sideofthebody
ConfusionDifficultyinspeakingorunderstandingDeteriorationofvisionin1orbotheyesDifficultyinwalking,dizziness,andlossofbalanceorcoordinationSevereheadachewithnoknowncause
Inthespringof2013,theASAlaunchedastrokepubliceducationcampaignthatusestheacronymFASTtoteachthewarningsignsofstrokeandtheimportanceofcalling911,asfollows:
F:FacedroopingA:ArmweaknessS:SpeechdifficultyT:Timetocall911
Forpatienteducationinformation,seetheStrokeHealthCenterandtheBrainandNervousSystemHealthCenter,aswellasStroke,TransientIschemicAttack(TIA,Ministroke),andStrokeRelatedDementia.
ContributorInformationandDisclosuresAuthorEdwardCJauch,MD,MS,FAHA,FACEPProfessor,Director,DivisionofEmergencyMedicine,Professor,DepartmentofNeurosciences,AssociateViceChairofResearch,DepartmentofMedicine,MedicalUniversityofSouthCarolinaCollegeofMedicine
EdwardCJauch,MD,MS,FAHA,FACEPisamemberofthefollowingmedicalsocieties:AmericanCollegeofEmergencyPhysicians,AmericanHeartAssociation,AmericanMedicalAssociation,NationalStrokeAssociation,SocietyforAcademicEmergencyMedicine,andSouthCarolinaMedicalAssociation
Disclosure:GenentechGrant/researchfundsSitePI
Coauthor(s)BrianStettler,MDAssistantProfessor,ProgramDirector,EmergencyMedicineResidencyProgram,DepartmentofEmergencyMedicine,andFacultyGreaterCincinnati/NorthernKentuckyStrokeTeam,UniversityofCincinnati
Disclosure:Nothingtodisclose.
ChiefEditorHelmiLLutsep,MDProfessorandViceChair,DepartmentofNeurology,OregonHealthandScienceUniversitySchoolofMedicineAssociateDirector,OregonStrokeCenter
HelmiLLutsep,MDisamemberofthefollowingmedicalsocieties:AmericanAcademyofNeurologyandAmericanStrokeAssociation
Disclosure:StrykerNeurovascularConsultingfeeReviewpanelmembership
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 12/18
AdditionalContributorsJeffreyLArnold,MD,FACEPChairman,DepartmentofEmergencyMedicine,SantaClaraValleyMedicalCenter
JeffreyLArnold,MD,FACEPisamemberofthefollowingmedicalsocieties:AmericanAcademyofEmergencyMedicineandAmericanCollegeofPhysicians
Disclosure:Nothingtodisclose.
JosephUBecker,MDFellow,GlobalHealthandInternationalEmergencyMedicine,StanfordUniversitySchoolofMedicine
JosephUBecker,MDisamemberofthefollowingmedicalsocieties:AmericanCollegeofEmergencyPhysicians,EmergencyMedicineResidentsAssociation,PhiBetaKappa,andSocietyforAcademicEmergencyMedicine
Disclosure:Nothingtodisclose.
SalvadorCruzFlores,MD,MPH,FAHA,FCCMProfessorofNeurologyandEpidemiology,SidneyWSouersEndowedChair,DirectorofSouersStrokeInstitute,CerebrovascularandNeurointensiveCareSection,Director,VascularNeurologyFellowshipTrainingProgram,InterimChairman,DepartmentofNeurologyandPsychiatry,StLouisUniversitySchoolofMedicineDirector,NeuroscienceIntensiveCareUnit(5ICU),StLouisUniversityHospital
SalvadorCruzFlores,MD,MPH,FAHA,FCCMisamemberofthefollowingmedicalsocieties:AmericanAcademyofHospiceandPalliativeMedicine,AmericanAcademyofNeurology,AmericanCollegeofPhysicians,AmericanHeartAssociation,AmericanSocietyofNeuroimaging,AmericanStrokeAssociation,NationalStrokeAssociation,NeurocriticalCareSociety,andSocietyofCriticalCareMedicine
Disclosure:AxioincHonorariaReviewpanelmembershipRocheHonorariaReviewpanelmembershipLillyHonorariaReviewpanelmembershipBiotronikHonorariaReviewpanelmembership
JStephenHuff,MDAssociateProfessorofEmergencyMedicineandNeurology,DepartmentofEmergencyMedicine,UniversityofVirginiaSchoolofMedicine
JStephenHuff,MDisamemberofthefollowingmedicalsocieties:AmericanAcademyofEmergencyMedicine,AmericanAcademyofNeurology,AmericanCollegeofEmergencyPhysicians,andSocietyforAcademicEmergencyMedicine
Disclosure:Nothingtodisclose.
RichardSKrause,MDSeniorClinicalFaculty/ClinicalAssistantProfessor,DepartmentofEmergencyMedicine,UniversityofBuffaloStateUniversityofNewYorkSchoolofMedicineandBiomedicalSciences
RichardSKrause,MDisamemberofthefollowingmedicalsocieties:AlphaOmegaAlpha,AmericanAcademyofEmergencyMedicine,AmericanCollegeofEmergencyPhysicians,andSocietyforAcademicEmergencyMedicine
Disclosure:Nothingtodisclose.
FranciscoTalavera,PharmD,PhDAdjunctAssistantProfessor,UniversityofNebraskaMedicalCenterCollegeofPharmacyEditorinChief,MedscapeDrugReference
Disclosure:MedscapeSalaryEmployment
CharlesRWiraIII,MDAssistantProfessor,SectionofEmergencyMedicine,YaleUniversitySchoolofMedicineDEMLiaisonandAttendingPhysician,YaleAcuteStrokeService,DepartmentofNeurology,YaleNewHavenHospital
CharlesRWiraIII,MDisamemberofthefollowingmedicalsocieties:AmericanCollegeofEmergencyPhysicians,AmericanHeartAssociation,AmericanStrokeAssociation,NeurocriticalCareSociety,SocietyforAcademicEmergencyMedicine,andSocietyofCriticalCareMedicine
Disclosure:Nothingtodisclose.
References
1. HughesS.EndovascularStrokeTherapyProvenatLast:MRCLEANPublished.MedscapeMedicalNews[serialonline].Dec172014AccessedDec222014.Availableathttp://www.medscape.com/viewarticle/836744.
2. BerkhemerOA,FransenPS,BeumerD,etal.ARandomizedTrialofIntraarterialTreatmentforAcuteIschemicStroke.NEnglJMed.Dec172014[Medline].
3. [Guideline]AdamsHPJr,delZoppoG,AlbertsMJ,BhattDL,BrassL,FurlanA,etal.Guidelinesfortheearlymanagementofadultswithischemicstroke:aguidelinefromtheAmericanHeartAssociation/AmericanStrokeAssociationStrokeCouncil,ClinicalCardiologyCouncil,CardiovascularRadiologyandInterventionCouncil,andtheAtheroscleroticPeripheralVascularDiseaseandQualityofCareOutcomesinResearchInterdisciplinaryWorkingGroups:theAmericanAcademyofNeurologyaffirmsthevalueofthisguidelineasaneducationaltoolforneurologists.Stroke.May200738(5):1655711.[Medline].
4. AdamsHPJr,DavisPH,LeiraEC,ChangKC,BendixenBH,ClarkeWR,etal.BaselineNIHStrokeScalescorestronglypredictsoutcomeafterstroke:AreportoftheTrialofOrg10172inAcuteStrokeTreatment(TOAST).Neurology.Jul13199953(1):12631.[Medline].
5. Tissueplasminogenactivatorforacuteischemicstroke.TheNationalInstituteofNeurologicalDisordersandStrokertPAStrokeStudyGroup.NEnglJMed.Dec141995333(24):15817.[Medline].
6. RogerVL,GoAS,LloydJonesDM,BenjaminEJ,BerryJD,BordenWB,etal.Heartdiseaseandstroke
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 13/18
statistics2012update:areportfromtheAmericanHeartAssociation.Circulation.Jan32012125(1):e2e220.[Medline].
7. SaccoRL,ShiT,ZamanilloMC,KargmanDE.Predictorsofmortalityandrecurrenceafterhospitalizedcerebralinfarctioninanurbancommunity:theNorthernManhattanStrokeStudy.Neurology.Apr199444(4):62634.[Medline].
8. DonnanGA,FisherM,MacleodM,DavisSM.Stroke.Lancet.May102008371(9624):161223.[Medline].
9. DirnaglU,IadecolaC,MoskowitzMA.Pathobiologyofischaemicstroke:anintegratedview.TrendsNeurosci.Sep199922(9):3917.[Medline].
10. YuanJ,YanknerBA.Apoptosisinthenervoussystem.Nature.Oct122000407(6805):8029.[Medline].
11. LatchawRE,YonasH,HunterGJ,YuhWT,UedaT,SorensenAG,etal.Guidelinesandrecommendationsforperfusionimagingincerebralischemia:Ascientificstatementforhealthcareprofessionalsbythewritinggrouponperfusionimaging,fromtheCouncilonCardiovascularRadiologyoftheAmericanHeartAssociation.Stroke.Apr200334(4):1084104.[Medline].
12. KasnerSE,GrottaJC.Emergencyidentificationandtreatmentofacuteischemicstroke.AnnEmergMed.Nov199730(5):64253.[Medline].
13. GotohO,AsanoT,KoideT,TakakuraK.Ischemicbrainedemafollowingocclusionofthemiddlecerebralarteryintherat.I:Thetimecoursesofthebrainwater,sodiumandpotassiumcontentsandbloodbrainbarrierpermeabilityto125Ialbumin.Stroke.JanFeb198516(1):1019.[Medline].
14. BellBA,SymonL,BranstonNM.CBFandtimethresholdsfortheformationofischemiccerebraledema,andeffectofreperfusioninbaboons.JNeurosurg.Jan198562(1):3141.[Medline].
15. MullinsME,LevMH,SchellingerhoutD,GonzalezRG,SchaeferPW.Intracranialhemorrhagecomplicatingacutestroke:howcommonishemorrhagicstrokeoninitialheadCTscanandhowoftenisinitialclinicaldiagnosisofacutestrokeeventuallyconfirmed?.AJNRAmJNeuroradiol.Oct200526(9):220712.[Medline].
16. LydenPD,ZivinJA.Hemorrhagictransformationaftercerebralischemia:mechanismsandincidence.CerebrovascBrainMetabRev.Spring19935(1):116.[Medline].
17. NighoghossianN,HermierM,AdeleineP,BlancLasserreK,DerexL,HonnoratJ,etal.Oldmicrobleedsareapotentialriskfactorforcerebralbleedingafterischemicstroke:agradientechoT2*weightedbrainMRIstudy.Stroke.Mar200233(3):73542.[Medline].
18. GonzlezRG.Imagingguidedacuteischemicstroketherapy:From"timeisbrain"to"physiologyisbrain".AJNRAmJNeuroradiol.Apr200627(4):72835.[Medline].
19. AlbersGW,AmarencoP,EastonJD,SaccoRL,TealP.Antithromboticandthrombolytictherapyforischemicstroke:theSeventhACCPConferenceonAntithromboticandThrombolyticTherapy.Chest.Sep2004126(3Suppl):483S512S.[Medline].
20. DubeyN,BakshiR,WasayM,DmochowskiJ.Earlycomputedtomographyhypodensitypredictshemorrhageafterintravenoustissueplasminogenactivatorinacuteischemicstroke.JNeuroimaging.Apr200111(2):1848.[Medline].
21. BrooksM.MigraineLinkedtoDoubleRiskforSilentStroke.MedscapeMedicalNews.Availableathttp://www.medscape.com/viewarticle/825451.AccessedMay27,2014.
22. AndersonP.Migrainewithaura'major'contributortoallstroketypes.MedscapeMedicalNews[serialonline].June27,2013AccessedJuly9,2013.Availableathttp://www.medscape.com/viewarticle/806983.
23. [Guideline]GoldsteinLB,BushnellCD,AdamsRJ,AppelLJ,BraunLT,ChaturvediS,etal.Guidelinesfortheprimarypreventionofstroke:aguidelineforhealthcareprofessionalsfromtheAmericanHeartAssociation/AmericanStrokeAssociation.Stroke.Feb201142(2):51784.[Medline].[FullText].
24. KurlS,LaukkanenJA,RauramaaR,LakkaTA,SiveniusJ,SalonenJT.Cardiorespiratoryfitnessandtheriskforstrokeinmen.ArchInternMed.Jul282003163(14):16828.[Medline].
25. BushnellC,McCulloughLD,AwadIA,ChireauMV,FedderWN,FurieKL,etal.GuidelinesforthePreventionofStrokeinWomen:AStatementforHealthcareProfessionalsFromtheAmericanHeartAssociation/AmericanStrokeAssociation.Stroke.Feb62014[Medline].
26. HughesS.FirstAHA/ASAGuidelinestoReduceStrokeRiskinWomen.Medscape[serialonline].Availableathttp://www.medscape.com/viewarticle/820277.AccessedFebruary11,2014.
27. MarsdenPA,HengHH,SchererSW,StewartRJ,HallAV,ShiXM,etal.Structureandchromosomallocalizationofthehumanconstitutiveendothelialnitricoxidesynthasegene.JBiolChem.Aug151993268(23):1747888.[Medline].
28. MillerDK,GillardJW,VickersPJ,SadowskiS,LveillC,ManciniJA,etal.Identificationandisolationofamembraneproteinnecessaryforleukotrieneproduction.Nature.Jan181990343(6255):27881.[Medline].
29. KuboM,HataJ,NinomiyaT,MatsudaK,YonemotoK,NakanoT,etal.AnonsynonymousSNPinPRKCH(proteinkinaseCeta)increasestheriskofcerebralinfarction.NatGenet.Feb200739(2):2127.[Medline].
30. MuddSH,SkovbyF,LevyHL,PettigrewKD,WilckenB,PyeritzRE,etal.Thenaturalhistoryofhomocystinuriaduetocystathioninebetasynthasedeficiency.AmJHumGenet.Jan198537(1):131.[Medline].[FullText].
31. TestaiFD,GorelickPB.Inheritedmetabolicdisordersandstrokepart2:homocystinuria,organicacidurias,andureacycledisorders.ArchNeurol.Feb201067(2):14853.[Medline].
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 14/18
32. JenssonO,GudmundssonG,ArnasonA,BlndalH,PetursdottirI,ThorsteinssonL,etal.HereditarycystatinC(gammatrace)amyloidangiopathyoftheCNScausingcerebralhemorrhage.ActaNeurolScand.Aug198776(2):10214.[Medline].
33. ObersteinSA.DiagnosticstrategiesinCADASIL.Neurology.Jun24200360(12):2020authorreply2020.[Medline].
34. DichgansM.CognitioninCADASIL.Stroke.Mar200940(3Suppl):S457.[Medline].
35. ChengYC,O'ConnellJR,ColeJW,StineOC,DuekerN,McArdlePF,etal.Genomewideassociationanalysisofischemicstrokeinyoungadults.G3(Bethesda).Nov20111(6):50514.[Medline].[FullText].
36. TheInternationalStrokeGeneticsConsortium(ISGC)theWellcomeTrustCaseControlConsortium2(WTCCC2),BellenguezC,BevanS,GschwendtnerA,SpencerCC,etal.GenomewideassociationstudyidentifiesavariantinHDAC9associatedwithlargevesselischemicstroke.NatGenet.Feb5201244(3):32833.[Medline].[FullText].
37. ArreguiM,FisherE,KnppelS,BuijsseB,diGiuseppeR,FritscheA,etal.Significantassociationsofthers2943634(2q36.3)geneticpolymorphismwithadiponectin,highdensitylipoproteincholesterolandischemicstroke.Gene.Feb252012494(2):1905.[Medline].
38. IkramMA,SeshadriS,BisJC,FornageM,DeStefanoAL,AulchenkoYS,etal.Genomewideassociationstudiesofstroke.NEnglJMed.Apr232009360(17):171828.[Medline].[FullText].
39. ArboixA,AlioJ.Acutecardioemboliccerebralinfarction:answerstoclinicalquestions.CurrCardiolRev.Feb20128(1):5467.[Medline].[FullText].
40. WittBJ,BallmanKV,BrownRDJr,MeverdenRA,JacobsenSJ,RogerVL.Theincidenceofstrokeaftermyocardialinfarction:ametaanalysis.AmJMed.Apr2006119(4):354.e19.[Medline].
41. WesselsT,WesselsC,EllsiepenA,ReuterI,TrittmacherS,StolzE.Contributionofdiffusionweightedimagingindeterminationofstrokeetiology.AJNRAmJNeuroradiol.Jan200627(1):359.[Medline].
42. RohJK,KangDW,LeeSH,YoonBW,ChangKH.Significanceofacutemultiplebraininfarctionondiffusionweightedimaging.Stroke.Mar200031(3):68894.[Medline].
43. AdamsH,AdamsR,DelZoppoG,GoldsteinLB.Guidelinesfortheearlymanagementofpatientswithischemicstroke:2005guidelinesupdateascientificstatementfromtheStrokeCounciloftheAmericanHeartAssociation/AmericanStrokeAssociation.Stroke.Apr200536(4):91623.[Medline].
44. DerdeynCP,KhoslaA,VideenTO,FritschSM,CarpenterDL,GrubbRLJr.Severehemodynamicimpairmentandborderzoneregioninfarction.Radiology.Jul2001220(1):195201.[Medline].
45. PollanenMS,DeckJH.Directedembolizationisanalternatecauseofcerebralwatershedinfarction.ArchPatholLabMed.Oct1989113(10):113941.[Medline].
46. WaterstonJA,BrownMM,ButlerP,SwashM.Smalldeepcerebralinfarctsassociatedwithocclusiveinternalcarotidarterydisease.Ahemodynamicphenomenon?.ArchNeurol.Sep199047(9):9537.[Medline].
47. U.S.CentersforDiseaseControlandPreventionandtheHeartDiseaseandStrokeStatistics2007Update,publishedbytheAmericanHeartAssociation.Availableathttp://www.strokecenter.org/patients/stats.htm.AccessedSeptember2008.
48. TowfighiA,SaverJL.StrokedeclinesfromthirdtofourthleadingcauseofdeathintheUnitedStates:historicalperspectiveandchallengesahead.Stroke.Aug201142(8):23515.[Medline].
49. MacKayJ,MensahGA.WorldHealthOrganization.GlobalBurdenofStroke.TheAtlasofHeartDiseaseandStroke.Availableathttp://www.who.int/cardiovascular_diseases/en/cvd_atlas_15_burden_stroke.pdf.
50. SchneiderAT,KisselaB,WooD,KleindorferD,AlwellK,MillerR,etal.Ischemicstrokesubtypes:apopulationbasedstudyofincidenceratesamongblacksandwhites.Stroke.Jul200435(7):15526.[Medline].
51. FonarowGC,SaverJL,SmithEE,BroderickJP,KleindorferDO,SaccoRL,etal.Relationshipofnationalinstitutesofhealthstrokescaleto30daymortalityinmedicarebeneficiarieswithacuteischemicstroke.JAmHeartAssoc.Feb20121(1):4250.[Medline].[FullText].
52. vonKummerR,AllenKL,HolleR,BozzaoL,BastianelloS,ManelfeC,etal.Acutestroke:usefulnessofearlyCTfindingsbeforethrombolytictherapy.Radiology.Nov1997205(2):32733.[Medline].
53. HackeW,KasteM,FieschiC,ToniD,LesaffreE,vonKummerR,etal.Intravenousthrombolysiswithrecombinanttissueplasminogenactivatorforacutehemisphericstroke.TheEuropeanCooperativeAcuteStrokeStudy(ECASS).JAMA.Oct41995274(13):101725.[Medline].
54. BrunoA,LevineSR,FrankelMR,BrottTG,LinY,TilleyBC,etal.AdmissionglucoselevelandclinicaloutcomesintheNINDSrtPAStrokeTrial.Neurology.Sep10200259(5):66974.[Medline].
55. BrunoA,BillerJ,AdamsHPJr,ClarkeWR,WoolsonRF,WilliamsLS,etal.Acutebloodglucoselevelandoutcomefromischemicstroke.TrialofORG10172inAcuteStrokeTreatment(TOAST)Investigators.Neurology.Jan15199952(2):2804.[Medline].
56. BairdTA,ParsonsMW,PhanhT,ButcherKS,DesmondPM,TressBM,etal.Persistentpoststrokehyperglycemiaisindependentlyassociatedwithinfarctexpansionandworseclinicaloutcome.Stroke.Sep200334(9):220814.[Medline].
57. MandelzweigL,GoldbourtU,BoykoV,TanneD.Perceptual,social,andbehavioralfactorsassociatedwithdelaysinseekingmedicalcareinpatientswithsymptomsofacutestroke.Stroke.May200637(5):124853.[Medline].
58. NationalInstitutesofHealthStrokeScale.Availableat
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 15/18
http://www.ninds.nih.gov/doctors/NIH_Stroke_Scale.pdf.AccessedOctober2008.
59. HuffJS.Strokemimicsandchameleons.EmergMedClinNorthAm.Aug200220(3):58395.[Medline].
60. LibmanRB,WirkowskiE,AlvirJ,RaoTH.Conditionsthatmimicstrokeintheemergencydepartment.Implicationsforacutestroketrials.ArchNeurol.Nov199552(11):111922.[Medline].
61. RuncheyS,McGeeS.Doesthispatienthaveahemorrhagicstroke?:clinicalfindingsdistinguishinghemorrhagicstrokefromischemicstroke.JAMA.Jun92010303(22):22806.[Medline].
62. EastonJD,SaverJL,AlbersGW,AlbertsMJ,ChaturvediS,FeldmannE,etal.Definitionandevaluationoftransientischemicattack:ascientificstatementforhealthcareprofessionalsfromtheAmericanHeartAssociation/AmericanStrokeAssociationStrokeCouncilCouncilonCardiovascularSurgeryandAnesthesiaCouncilonCardiovascularRadiologyandInterventionCouncilonCardiovascularNursingandtheInterdisciplinaryCouncilonPeripheralVascularDisease.TheAmericanAcademyofNeurologyaffirmsthevalueofthisstatementasaneducationaltoolforneurologists.Stroke.Jun200940(6):227693.[Medline].
63. TintinalliJ,KellenG,StapczynskiJ.AmericanCollegeofEmergencyPhysicians.EmergencyMedicine:AComprehensiveStudyGuide.6th.NewYork:McGrawHill2004:13821390.
64. LeiraEC,ChangKC,DavisPH,ClarkeWR,WoolsonRF,HansenMD,etal.Canwepredictearlyrecurrenceinacutestroke?.CerebrovascDis.200418(2):13944.[Medline].
65. MolyneuxAJ,KerrRS,YuLM,ClarkeM,SneadeM,YarnoldJA,etal.Internationalsubarachnoidaneurysmtrial(ISAT)ofneurosurgicalclippingversusendovascularcoilingin2143patientswithrupturedintracranialaneurysms:arandomisedcomparisonofeffectsonsurvival,dependency,seizures,rebleeding,subgroups,andaneurysmocclusion.Lancet.Sep392005366(9488):80917.[Medline].
66. ByrneJV.Theaneurysm"cliporcoil"debate.ActaNeurochir(Wien).Feb2006148(2):11520.[Medline].
67. SorensenAG,BuonannoFS,GonzalezRG,SchwammLH,LevMH,HuangHellingerFR,etal.Hyperacutestroke:evaluationwithcombinedmultisectiondiffusionweightedandhemodynamicallyweightedechoplanarMRimaging.Radiology.May1996199(2):391401.[Medline].
68. GonzlezRG,SchaeferPW,BuonannoFS,SchwammLH,BudzikRF,RordorfG,etal.DiffusionweightedMRimaging:diagnosticaccuracyinpatientsimagedwithin6hoursofstrokesymptomonset.Radiology.Jan1999210(1):15562.[Medline].
69. MarksMP,OlivotJM,KempS,LansbergMG,BammerR,WechslerLR,etal.PatientswithacutestroketreatedwithintravenoustPA36hoursafterstrokeonset:correlationsbetweenMRangiographyfindingsandperfusionanddiffusionweightedimagingintheDEFUSEstudy.Radiology.Nov2008249(2):61423.[Medline].[FullText].
70. SchellingerPD,BryanRN,CaplanLR,DetreJA,EdelmanRR,JaigobinC,etal.Evidencebasedguideline:TheroleofdiffusionandperfusionMRIforthediagnosisofacuteischemicstroke:reportoftheTherapeuticsandTechnologyAssessmentSubcommitteeoftheAmericanAcademyofNeurology.Neurology.Jul13201075(2):17785.[Medline].
71. SorensenAG,CopenWA,OstergaardL,BuonannoFS,GonzalezRG,RordorfG,etal.Hyperacutestroke:simultaneousmeasurementofrelativecerebralbloodvolume,relativecerebralbloodflow,andmeantissuetransittime.Radiology.Feb1999210(2):51927.[Medline].
72. CamerlingoM,CastoL,CensoriB,FerraroB,GazzanigaGC,MamoliA.TranscranialDopplerinacuteischemicstrokeofthemiddlecerebralarteryterritories.ActaNeurolScand.Aug199388(2):10811.[Medline].
73. SagarG,RileyP,VohrahA.Isadmissionchestradiographyofanyclinicalvalueinacutestrokepatients?.ClinRadiol.Jul199651(7):499502.[Medline].
74. MeerwaldtR,SlartRH,vanDamGM,LuijckxGJ,TioRA,ZeebregtsCJ.PET/SPECTimaging:fromcarotidvulnerabilitytobrainviability.EurJRadiol.Apr201074(1):1049.[Medline].
75. HandschuR,PoppeR,RaussJ,NeundrferB,ErbguthF.Emergencycallsinacutestroke.Stroke.Apr200334(4):10059.[Medline].
76. WilliamsJE,RosamondWD,MorrisDL.Strokesymptomattributionandtimetoemergencydepartmentarrival:thedelayinaccessingstrokehealthcarestudy.AcadEmergMed.Jan20007(1):936.[Medline].
77. ZweiflerRM,MendizabalJE,CunninghamS,ShahAK,RothrockJF.Hospitalpresentationafterstrokeinacommunitysample:theMobileStrokeProject.SouthMedJ.Nov200295(11):12638.[Medline].
78. LacyCR,SuhDC,BuenoM,KostisJB.Delayinpresentationandevaluationforacutestroke:StrokeTimeRegistryforOutcomesKnowledgeandEpidemiology(S.T.R.O.K.E.).Stroke.Jan200132(1):639.[Medline].
79. PuolakkaT,VyrynenT,HpplO,SoinneL,KuismaM,LindsbergPJ.Sequentialanalysisofpretreatmentdelaysinstrokethrombolysis.AcadEmergMed.Sep201017(9):9659.[Medline].
80. FordAL,WilliamsJA,SpencerM,McCammonC,KhouryN,SampsonTR,etal.ReducingdoortoneedletimesusingToyota'sleanmanufacturingprinciplesandvaluestreamanalysis.Stroke.Dec201243(12):33958.[Medline].[FullText].
81. [BestEvidence]BrunoA,KentTA,CoullBM,ShankarRR,SahaC,BeckerKJ,etal.Treatmentofhyperglycemiainischemicstroke(THIS):arandomizedpilottrial.Stroke.Feb200839(2):3849.[Medline].
82. BellolioMF,GilmoreRM,SteadLG.Insulinforglycaemiccontrolinacuteischaemicstroke.CochraneDatabaseSystRev.Sep720119:CD005346.[Medline].
83. HackeW,KasteM,BluhmkiE,BrozmanM,DvalosA,GuidettiD,etal.Thrombolysiswithalteplase3to4.5hoursafteracuteischemicstroke.NEnglJMed.Sep252008359(13):131729.[Medline].
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 16/18
84. [Guideline]DelZoppoGJ,SaverJL,JauchEC,AdamsHPJr.Expansionofthetimewindowfortreatmentofacuteischemicstrokewithintravenoustissueplasminogenactivator:ascienceadvisoryfromtheAmericanHeartAssociation/AmericanStrokeAssociation.Stroke.Aug200940(8):29458.[Medline].[FullText].
85. WahlgrenN,AhmedN,DvalosA,HackeW,MillnM,MuirK,etal.Thrombolysiswithalteplase34.5hafteracuteischaemicstroke(SITSISTR):anobservationalstudy.Lancet.Oct112008372(9646):13039.[Medline].
86. [BestEvidence]JauchEC,SaverJL,AdamsHPJr,BrunoA,ConnorsJJ,DemaerschalkBM,etal.GuidelinesfortheEarlyManagementofPatientsWithAcuteIschemicStroke:AGuidelineforHealthcareProfessionalsFromtheAmericanHeartAssociation/AmericanStrokeAssociation.Stroke.Jan312013[Medline].
87. BrooksM.StrokeaRaceAgainsttheClock,ReviewConfirms.MedscapeMedicalNews.Availableathttp://www.medscape.com/viewarticle/830611.AccessedSeptember2,2014.
88. EmbersonJ,LeesKR,LydenP,BlackwellL,AlbersG,BluhmkiE,etal.Effectoftreatmentdelay,age,andstrokeseverityontheeffectsofintravenousthrombolysiswithalteplaseforacuteischaemicstroke:ametaanalysisofindividualpatientdatafromrandomisedtrials.Lancet.Aug52014[Medline].
89. StrbianD,RinglebP,MichelP,etal.Ultraearlyintravenousstrokethrombolysis:doallpatientsbenefitsimilarly?.Stroke.Aug222013[Medline].
90. BrooksM.'UltraEarly'ThrombolysisCutsDisabilityinMildStroke.MedscapeMedicalNews[serialonline].Aug282013AccessedSep32013.Availableathttp://www.medscape.com/viewarticle/810126.
91. [BestEvidence]DiedlerJ,AhmedN,SykoraM,UyttenboogaartM,OvergaardK,LuijckxGJ,etal.Safetyofintravenousthrombolysisforacuteischemicstrokeinpatientsreceivingantiplatelettherapyatstrokeonset.Stroke.Feb201041(2):28894.[Medline].
92. AlexandrovAV,MolinaCA,GrottaJC,GaramiZ,FordSR,AlvarezSabinJ,etal.Ultrasoundenhancedsystemicthrombolysisforacuteischemicstroke.NEnglJMed.Nov182004351(21):21708.[Medline].
93. TsivgoulisG,EggersJ,RiboM,PerrenF,SaqqurM,RubieraM,etal.Safetyandefficacyofultrasoundenhancedthrombolysis:acomprehensivereviewandmetaanalysisofrandomizedandnonrandomizedstudies.Stroke.Feb201041(2):2807.[Medline].
94. BroderickJP,PaleschYY,DemchukAM,YeattsSD,KhatriP,HillMD,etal.EndovasculartherapyafterintravenoustPAversustPAaloneforstroke.NEnglJMed.Mar72013368(10):893903.[Medline].[FullText].
95. SchonewilleWJ,WijmanCA,MichelP,RueckertCM,WeimarC,MattleHP,etal.TreatmentandoutcomesofacutebasilararteryocclusionintheBasilarArteryInternationalCooperationStudy(BASICS):aprospectiveregistrystudy.LancetNeurol.Aug20098(8):72430.[Medline].
96. LindsbergPJ,MattleHP.Therapyofbasilararteryocclusion:asystematicanalysiscomparingintraarterialandintravenousthrombolysis.Stroke.Mar200637(3):9228.[Medline].
97. CAST:randomisedplacebocontrolledtrialofearlyaspirinusein20,000patientswithacuteischaemicstroke.CAST(ChineseAcuteStrokeTrial)CollaborativeGroup.Lancet.Jun71997349(9066):16419.[Medline].
98. TheInternationalStrokeTrial(IST):arandomisedtrialofaspirin,subcutaneousheparin,both,orneitheramong19435patientswithacuteischaemicstroke.InternationalStrokeTrialCollaborativeGroup.Lancet.May311997349(9065):156981.[Medline].
99. Abciximabinacuteischemicstroke:arandomized,doubleblind,placebocontrolled,doseescalationstudy.TheAbciximabinIschemicStrokeInvestigators.Stroke.Mar200031(3):6019.[Medline].
100. AdamsHPJr,EffronMB,TornerJ,DvalosA,FrayneJ,TealP,etal.Emergencyadministrationofabciximabfortreatmentofpatientswithacuteischemicstroke:resultsofaninternationalphaseIIItrial:AbciximabinEmergencyTreatmentofStrokeTrial(AbESTTII).Stroke.Jan200839(1):8799.[Medline].
101. SareGM,GeeganageC,BathPM.Highbloodpressureinacuteischaemicstrokebroadeningtherapeutichorizons.CerebrovascDis.200927Suppl1:15661.[Medline].
102. PotterJF,RobinsonTG,FordGA,MistriA,JamesM,ChernovaJ,etal.Controllinghypertensionandhypotensionimmediatelypoststroke(CHHIPS):arandomised,placebocontrolled,doubleblindpilottrial.LancetNeurol.Jan20098(1):4856.[Medline].
103. SandsetEC,BathPM,BoysenG,JatuzisD,KrvJ,LdersS,etal.Theangiotensinreceptorblockercandesartanfortreatmentofacutestroke(SCAST):arandomised,placebocontrolled,doubleblindtrial.Lancet.Feb262011377(9767):74150.[Medline].
104. JeffreyS.CATIS:NoBenefitofBPReductioninAcutePhaseofStroke.MedscapeMedicalNews.Availableathttp://www.medscape.com/viewarticle/814531.AccessedNovember24,2013.
105. HeJ,ZhangY,XuT,ZhaoQ,WangD,ChenCS,etal.EffectsofImmediateBloodPressureReductiononDeathandMajorDisabilityinPatientsWithAcuteIschemicStroke:TheCATISRandomizedClinicalTrial.JAMA.Nov172013[Medline].
106. GobinYP,StarkmanS,DuckwilerGR,GrobelnyT,KidwellCS,JahanR,etal.MERCI1:aphase1studyofMechanicalEmbolusRemovalinCerebralIschemia.Stroke.Dec200435(12):284854.[Medline].
107. SmithWS,SungG,StarkmanS,SaverJL,KidwellCS,GobinYP,etal.Safetyandefficacyofmechanicalembolectomyinacuteischemicstroke:resultsoftheMERCItrial.Stroke.Jul200536(7):14328.[Medline].
108. SmithWS,SungG,SaverJ,BudzikR,DuckwilerG,LiebeskindDS,etal.Mechanicalthrombectomyforacuteischemicstroke:finalresultsoftheMultiMERCItrial.Stroke.Apr200839(4):120512.[Medline].
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 17/18
109. BoseA,HenkesH,AlfkeK,ReithW,MayerTE,BerlisA.ThePenumbraSystem:amechanicaldeviceforthetreatmentofacutestrokeduetothromboembolism.AJNRAmJNeuroradiol.Aug200829(7):140913.[Medline].
110. SaverJL,JahanR,LevyEI,JovinTG,BaxterB,NogueiraRG,etal.SolitaireflowrestorationdeviceversustheMerciRetrieverinpatientswithacuteischaemicstroke(SWIFT):arandomised,parallelgroup,noninferioritytrial.Lancet.Oct62012380(9849):12419.[Medline].
111. NogueiraRG,LutsepHL,GuptaR,JovinTG,AlbersGW,WalkerGA,etal.TrevoversusMerciretrieversforthrombectomyrevascularisationoflargevesselocclusionsinacuteischaemicstroke(TREVO2):arandomisedtrial.Lancet.Oct62012380(9849):123140.[Medline].
112. AndersonP.Medicalmanagementstillbestsintracranialstenting.MedscapeMedicalNews[serialonline].October31,2013AccessedNovember5,2013.Availableathttp://www.medscape.com/viewarticle/813604.
113. DerdeynCP,ChimowitzMI,LynnMJ,FiorellaD,TuranTN,JanisLS,etal.Aggressivemedicaltreatmentwithorwithoutstentinginhighriskpatientswithintracranialarterystenosis(SAMMPRIS):thefinalresultsofarandomisedtrial.Lancet.Oct252013[Medline].
114. RothwellPM,MarkusHS.Improvedmedicaltreatmentinsecondarypreventionofstroke.Lancet.Oct252013[Medline].
115. MarionDW.Controllednormothermiainneurologicintensivecare.CritCareMed.Feb200432(2Suppl):S435.[Medline].
116. OlsenTS,WeberUJ,KammersgaardLP.Therapeutichypothermiaforacutestroke.LancetNeurol.Jul20032(7):4106.[Medline].
117. HemmenTM,RamanR,GulumaKZ,MeyerBC,GomesJA,CruzFloresS,etal.Intravenousthrombolysisplushypothermiaforacutetreatmentofischemicstroke(ICTuSL):finalresults.Stroke.Oct201041(10):226570.[Medline].
118. [BestEvidence]denHertogHM,vanderWorpHB,vanGemertHM,AlgraA,KappelleLJ,vanGijnJ,etal.TheParacetamol(Acetaminophen)InStroke(PAIS)trial:amulticentre,randomised,placebocontrolled,phaseIIItrial.LancetNeurol.May20098(5):43440.[Medline].
119. HofmeijerJ,KappelleLJ,AlgraA,AmelinkGJ,vanGijnJ,vanderWorpHB.Surgicaldecompressionforspaceoccupyingcerebralinfarction(theHemicraniectomyAfterMiddleCerebralArteryinfarctionwithLifethreateningEdemaTrial[HAMLET]):amulticentre,open,randomisedtrial.LancetNeurol.Apr20098(4):32633.[Medline].
120. JttlerE,SchwabS,SchmiedekP,UnterbergA,HennericiM,WoitzikJ,etal.DecompressiveSurgeryfortheTreatmentofMalignantInfarctionoftheMiddleCerebralArtery(DESTINY):arandomized,controlledtrial.Stroke.Sep200738(9):251825.[Medline].
121. VahediK,HofmeijerJ,JuettlerE,VicautE,GeorgeB,AlgraA,etal.Earlydecompressivesurgeryinmalignantinfarctionofthemiddlecerebralartery:apooledanalysisofthreerandomisedcontrolledtrials.LancetNeurol.Mar20076(3):21522.[Medline].
122. VahediK,VicautE,MateoJ,KurtzA,OrabiM,GuichardJP,etal.Sequentialdesign,multicenter,randomized,controlledtrialofearlydecompressivecraniectomyinmalignantmiddlecerebralarteryinfarction(DECIMALTrial).Stroke.Sep200738(9):250617.[Medline].
123. WijdicksEF,ShethKN,CarterBS,GreerDM,KasnerSE,KimberlyWT,etal.RecommendationsfortheManagementofCerebralandCerebellarInfarctionWithSwelling:AStatementforHealthcareProfessionalsFromtheAmericanHeartAssociation/AmericanStrokeAssociation.Stroke.Jan302014[Medline].
124. HughesS.AHA/ASAGuidelineonStrokeWithBrainSwelling.Medscape[serialonline].Availableathttp://www.medscape.com/viewarticle/820481.AccessedFebruary25,2014.
125. PadmaV,FisherM,MoonisM.Roleofheparinandlowmolecularweightheparinsinthemanagementofacuteischemicstroke.ExpertRevCardiovascTher.May20064(3):40515.[Medline].
126. CLOTS(ClotsinLegsOrsTockingsafterStroke)TrialsCollaboration.DennisM,SandercockP,ReidJ,GrahamC,ForbesJ,MurrayG.Effectivenessofintermittentpneumaticcompressioninreductionofriskofdeepveinthrombosisinpatientswhohavehadastroke(CLOTS3):amulticentrerandomisedcontrolledtrial.Lancet.Aug102013382(9891):51624.[Medline].
127. CollaborativeoverviewofrandomisedtrialsofantiplatelettherapyI:Preventionofdeath,myocardialinfarction,andstrokebyprolongedantiplatelettherapyinvariouscategoriesofpatients.AntiplateletTrialists'Collaboration.BMJ.Jan81994308(6921):81106.[Medline].[FullText].
128. [BestEvidence]AmarencoP,BogousslavskyJ,CallahanA3rd,GoldsteinLB,HennericiM,RudolphAE,etal.Highdoseatorvastatinafterstrokeortransientischemicattack.NEnglJMed.Aug102006355(6):54959.[Medline].
129. ChimowitzMI,LynnMJ,HowlettSmithH,SternBJ,HertzbergVS,FrankelMR,etal.Comparisonofwarfarinandaspirinforsymptomaticintracranialarterialstenosis.NEnglJMed.Mar312005352(13):130516.[Medline].
130. BaigentC,BlackwellL,CollinsR,EmbersonJ,GodwinJ,PetoR,etal.Aspirinintheprimaryandsecondarypreventionofvasculardisease:collaborativemetaanalysisofindividualparticipantdatafromrandomisedtrials.Lancet.May302009373(9678):184960.[Medline].[FullText].
131. [BestEvidence]RidkerPM,CookNR,LeeIM,GordonD,GazianoJM,MansonJE,etal.Arandomizedtrialoflowdoseaspirinintheprimarypreventionofcardiovasculardiseaseinwomen.NEnglJMed.Mar312005352(13):1293304.[Medline].
132. HughesS.NewAHA/ASAStrokeSecondaryPreventionGuidelines.MedscapeMedicalNews[serialonline].May22014AccessedMay122014.Availableathttp://www.medscape.com/viewarticle/824525.
-
17/4/2015 IschemicStroke
http://emedicine.medscape.com/article/1916852overview#a0156 18/18
MedscapeReference2011WebMD,LLC
133. [Guideline]KernanWN,OvbiageleB,BlackHR,etal.GuidelinesforthePreventionofStrokeinPatientsWithStrokeandTransientIschemicAttack:AGuidelineforHealthcareProfessionalsFromtheAmericanHeartAssociation/AmericanStrokeAssociation.Stroke.May12014[Medline].[FullText].
134. GeeganageCM,DienerHC,AlgraA,ChenC,TopolEJ,DenglerR,etal.Dualormonoantiplatelettherapyforpatientswithacuteischemicstrokeortransientischemicattack:systematicreviewandmetaanalysisofrandomizedcontrolledtrials.Stroke.Apr201243(4):105866.[Medline].
135. [BestEvidence]HalkesPH,vanGijnJ,KappelleLJ,KoudstaalPJ,AlgraA.Aspirinplusdipyridamoleversusaspirinaloneaftercerebralischaemiaofarterialorigin(ESPRIT):randomisedcontrolledtrial.Lancet.May202006367(9523):166573.[Medline].
136. [BestEvidence]DenglerR,DienerHC,SchwartzA,GrondM,SchumacherH,MachnigT,etal.Earlytreatmentwithaspirinplusextendedreleasedipyridamolefortransientischaemicattackorischaemicstrokewithin24hofsymptomonset(EARLYtrial):arandomised,openlabel,blindedendpointtrial.LancetNeurol.Feb20109(2):15966.[Medline].
137. DienerHC,BogousslavskyJ,BrassLM,CimminielloC,CsibaL,KasteM,etal.Aspirinandclopidogrelcomparedwithclopidogrelaloneafterrecentischaemicstrokeortransientischaemicattackinhighriskpatients(MATCH):randomised,doubleblind,placebocontrolledtrial.Lancet.Jul24302004364(9431):3317.[Medline].
138. [BestEvidence]ConnollyS,PogueJ,HartR,PfefferM,HohnloserS,ChrolaviciusS,etal.ClopidogrelplusaspirinversusoralanticoagulationforatrialfibrillationintheAtrialfibrillationClopidogrelTrialwithIrbesartanforpreventionofVascularEvents(ACTIVEW):arandomisedcontrolledtrial.Lancet.Jun102006367(9526):190312.[Medline].
139. [Guideline]WannLS,CurtisAB,EllenbogenKA,EstesNA3rd,EzekowitzMD,JackmanWM,etal.2011ACCF/AHA/HRSfocusedupdateonthemanagementofpatientswithatrialfibrillation(updateonDabigatran):areportoftheAmericanCollegeofCardiologyFoundation/AmericanHeartAssociationTaskForceonpracticeguidelines.Circulation.Mar152011123(10):114450.[Medline].[FullText].
140. UchinoK,HernandezAV.Dabigatranassociationwithhigherriskofacutecoronaryevents:metaanalysisofnoninferiorityrandomizedcontrolledtrials.ArchInternMed.Mar122012172(5):397402.[Medline].
141. [Guideline]FurieKL,KasnerSE,AdamsRJ,AlbersGW,BushRL,FaganSC,etal.Guidelinesforthepreventionofstrokeinpatientswithstrokeortransientischemicattack:aguidelineforhealthcareprofessionalsfromtheamericanheartassociation/americanstrokeassociation.Stroke.Jan201142(1):22776.[Medline].[FullText].
142. AndersonP.Waitonelectivesurgeryafterstroke.MedscapeMedicalNews[serialonline].July17,2014AccessedJuly21,2014.Availableathttp://www.medscape.com/viewarticle/828447.
143. ChiongW,KimAS,HuangIA,FarahanyNA,JosephsonSA.Testingthepresumptionofconsenttoemergencytreatmentforacuteischemicstroke.JAMA.Apr23302014311(16):168991.[Medline].
144. EbingerM,WinterB,WendtM,WeberJE,WaldschmidtC,RozanskiM,etal.Effectoftheuseofambulancebasedthrombolysisontimetothrombolysisinacuteischemicstroke:arandomizedclinicaltrial.JAMA.Apr23302014311(16):162231.[Medline].
145. FonarowGC,ZhaoX,SmithEE,SaverJL,ReevesMJ,BhattDL,etal.Doortoneedletimesfortissueplasminogenactivatoradministrationandclinicaloutcomesinacuteischemicstrokebeforeandafteraqualityimprovementinitiative.JAMA.Apr23302014311(16):163240.[Medline].
146. HughesS.DESTINYII:benefitofsurgeryforstrokewithswelling.MedscapeMedicalNews[serialonline].March24,2014AccessedApril1,2014.Availableathttp://www.medscape.com/viewarticle/822472.
147. JeffreyS.TARGET:STROKECutsDoortoNeedleTime,ImprovesOutcomes.MedscapeMedicalNews.Availableathttp://www.medscape.com/viewarticle/824008.AccessedApril29,2014.
148. JrgensenME,TorpPedersenC,GislasonGH,JensenPF,BergerSM,ChristiansenCB,etal.Timeelapsedafterischemicstrokeandriskofadversecardiovasculareventsandmortalityfollowingelectivenoncardiacsurgery.JAMA.Jul162014312(3):26977.[Medline].
149. JttlerE,UnterbergA,WoitzikJ,BselJ,AmiriH,SakowitzOW,etal.Hemicraniectomyinolderpatientswithextensivemiddlecerebralarterystroke.NEnglJMed.Mar202014370(12):1091100.[Medline].
150. RopperAH.Hemicraniectomytohalveorhalvenot.NEnglJMed.Mar202014370(12):115960.[Medline].
151. ShiberJR,FontaneE,AdewaleA.Strokeregistry:hemorrhagicvsischemicstrokes.AmJEmergMed.Mar201028(3):3313.[Medline].