Stroke in the Rural Setting: How You Can Make A Difference · Stroke in the Rural Setting: How You...
41
Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSN Program Manager Providence Stroke Center Portland, OR
-
Upload
nguyenthuan -
Category
Documents
-
view
214 -
download
1
Transcript of Stroke in the Rural Setting: How You Can Make A Difference · Stroke in the Rural Setting: How You...

Stroke in the Rural Setting: How You Can Make A Difference. Susie Fisher, RN, BSNProgram ManagerProvidence Stroke CenterPortland, OR
Presenter
Presentation Notes
It’s hard for me to understand who wouldn’t want to live here, I’m a native Oregonian and I love how unique every corner of our state is. So how can we love living in every corner of our state and provide the best stroke care we possibly can?

State StatisticsThe Oregon ProblemTime & TreatmentsSteps to Making a DifferenceThe FutureResources
Outline
Presenter
Presentation Notes
Today, I’ll be covering…
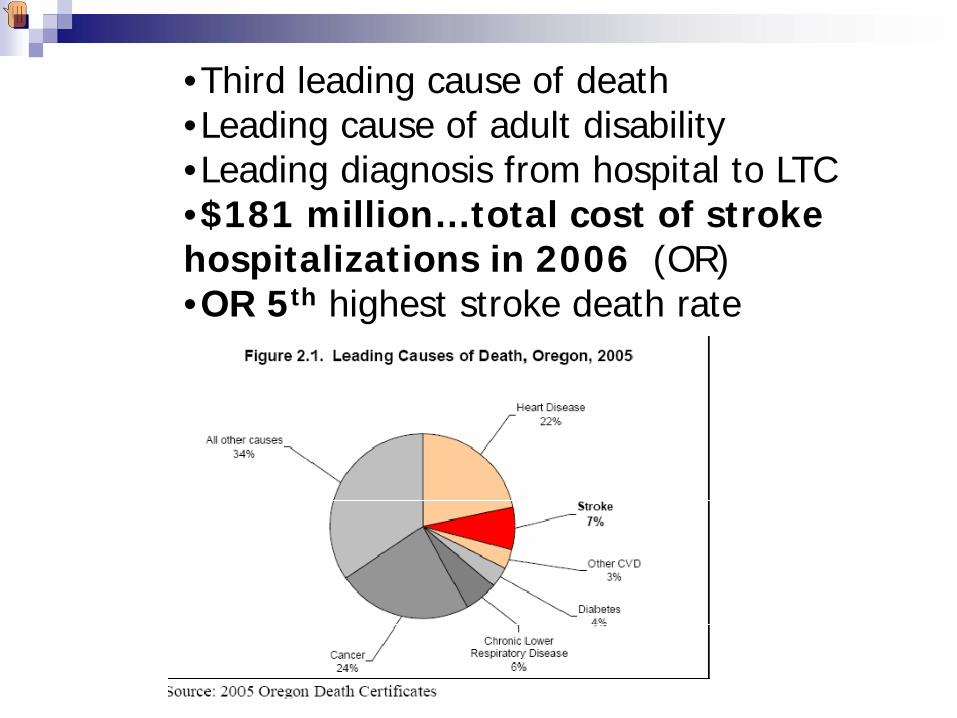
•Third leading cause of death•Leading cause of adult disability•Leading diagnosis from hospital to LTC•$181 million…total cost of stroke hospitalizations in 2006 (OR)•OR 5th highest stroke death rate
Presenter
Presentation Notes
First, let’s go through some of the national and state stroke statistics… most of us may know: In addition, OR is ranked 5th in the nation for stroke mortality, no clear reason why at this time. Research is underway. In
Presenter
Presentation Notes
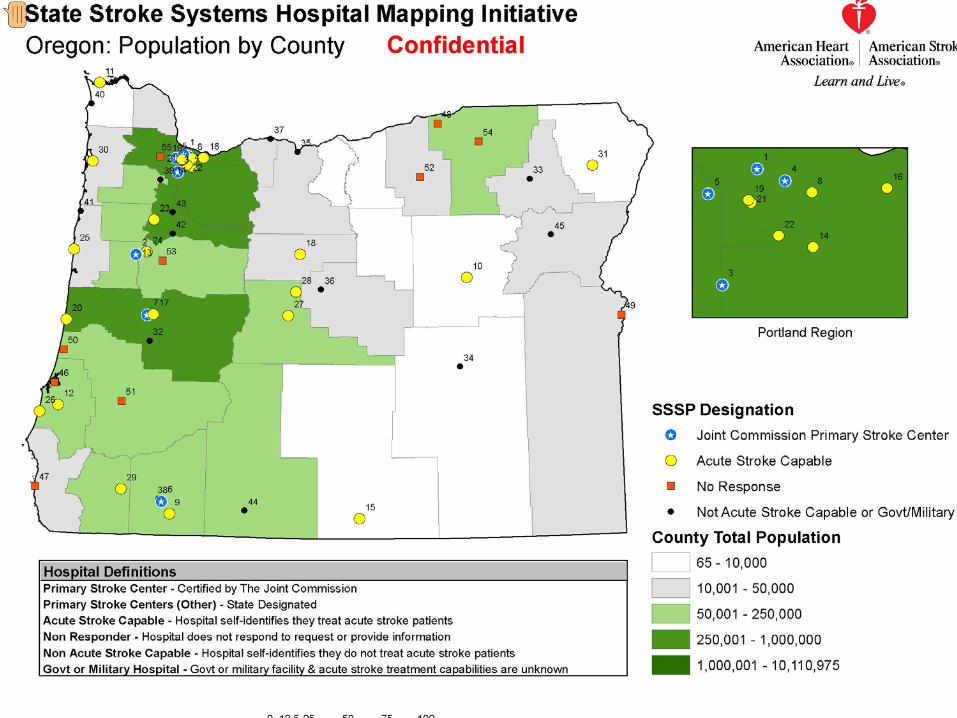
This is a great mapping project done in 07 by the AHA/ASA. You can see the population density along with self reported hospital designations. Joint Commission Primary Stroke Centers in OR include: PSV, PPMC, Legacy Good Samaritan, Legacy Meridian Park, Sacred Heart Eugene, Rogue Valley Medford. Those in yellow report they are acute stroke capable (have protocols). So if you look at this map all PSC’s are on the I-5 corridor which adds to some of the barriers for rural stroke care.
Presenter
Presentation Notes
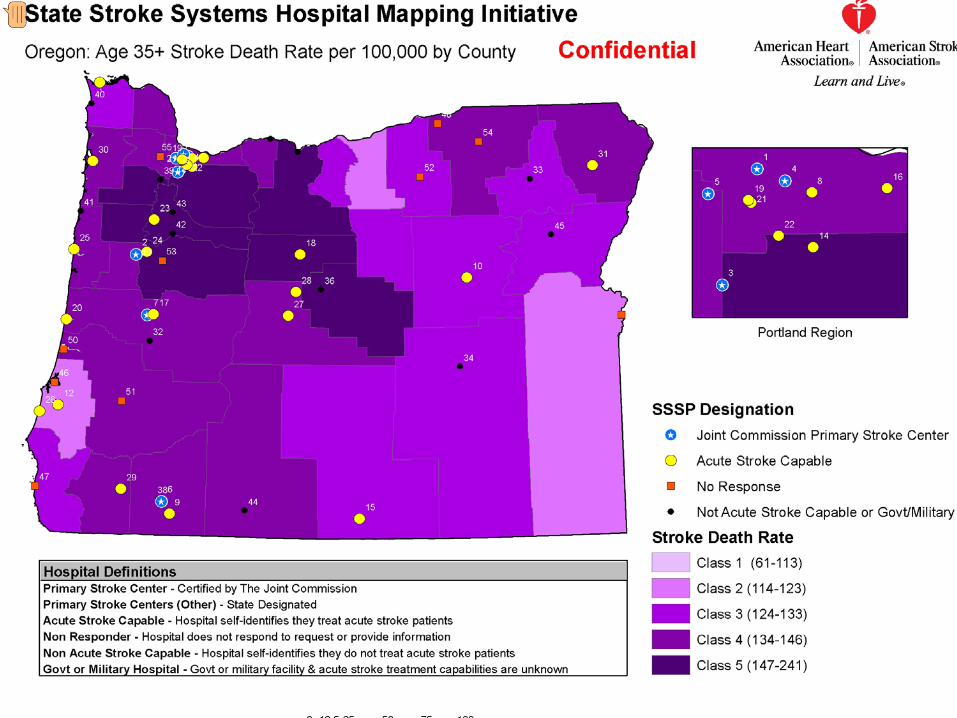
From this slide we can see that the Highest stroke death rates are clustered in North Central Oregon and along lower Columbia River

Presenter
Presentation Notes
A project done in 2008 by the NW Regional Stroke Network does a nice job of visualizing the service areas within a 90 min R/T air radius and PSC’s in OR.. Again showing a vast area of OR with more challenges for expert stroke care

Presenter
Presentation Notes
So, herein lies one of the biggest problems for stroke care in OR… the vast beauty and land, a quality so many of us love, and the challenge that places on stroke care.

Problem……
Small rural hospital Oregon (Oct. 2008) :Want to give most up to date stroke careLimited resources:
Not a Primary Stroke CenterNo Neurology coverage Limited N. Surgery, pharmacy, radiology, Hospitalist coverageLimited knowledge of tPA / specialty care
“How can we better serve our patients?”
Presenter
Presentation Notes
This was a call to me last year, and seems to reflect the concerns of so many rural providers I talk to… wanting to do the right thing but not knowing a) what exactly is the right thing? b) how to go about it?

Stroke Treatment in Rural Oregon
Local treatment is necessary due to Time dependent therapy and long distances between people and tertiary facilities capable and experienced with treatmentMinimum requirements for administering thrombolytic therapy are:
CT scanner 24/7
EMS Protocol for expediting transport & pre-notification
Acute care/t-PA protocol
Presenter
Presentation Notes
We need to start with our local site, our own resources and move out from there… to ensure we are doing the Right thing, at the right place at the right time. As we move through this, rest assured I will leave you with links to resources that there is not time to put into this presentation, including protocols for hospitals with and without CT scanners.

In the US only 4% stroke patients receive the only FDA approved treatment for acute stroke
Patients don’t often recognize their symptoms as stroke and don’t understand the need to seek emergent care via 911Primary providers have very little training or experience in treating stroke patients let alone use of t-PANeurologists are in short supply and clustered in urban areasUntil recently there was no economic incentive to treat acute stroke
Presenter
Presentation Notes
There is so much that can be done to treat or lessen the effects of a stroke if patients can recognize the symptoms, get in early to the right place where protocols will provide the most optimal outcome.

Stroke Treatment..(Ischemic)
t-PA approved in 1996… ONLY APPROVED MEDICATIONMust be given w/in 3 hrs of onset (last normal)
Requires neurological expertise, urgent CT scanningPROTOCOL necessaryPrimary Stroke Centers
Protocols, experts, guidelines, registries, data, quality improvement, outcomes
Presenter
Presentation Notes
So, much of what we’re talking about today is treatment for ISCHEMIC stroke… the “clot” kinds of stroke vs. the hemorrhage kinds of strokes to put it simply. tPA is Tissue Plasminogen Activator. Neuro expertise b/c must be given correctly to the right patient, high risk for bleeding. PSC’s are your resources,,approved by TJC they have….

Oregon, 2009TJC certified Primary Stroke Centers
Providence St. Vincent’s, 2004Legacy Good Samaritan, 2004Legacy Meridian Park, 2004Providence Portland, 2005Rogue Valley (Medford), 2006OHSU, 2007Sacred Heart (Eugene), 2008
*24/7 Comprehensive Capability
Treatment Options / ComprehensiveStroke Centers
IV t-PAIntra-arterial t-PAIntra-arterial devices
(up to 8 hr window)Clinical Trials
Drugs and devicesHypothermia
Rural Oregon… the beauty and the challenge.
Presenter
Presentation Notes
All of those wonderful treatments are great… but look where we are! Thus, the challenge.
Making a difference in your hospital & community…YOU CAN:
Find a clinical championRecruit administrative supportAssess resources (Pharmacy, Radiology, Lab, etc)
Develop protocols (ED & in-patient)Work closely with first respondersRelationship with experts for advice / transferEDUCATE staffEducate communityQuality review processes
Presenter
Presentation Notes
The challenge is not without hope and options a lot of what will lead to the best outcome for your patient is solid, guideline driven in-patient protocols.

Pre-Hospital Stroke Care
Scoop and go! Pre-notify Hospital
Presenter
Presentation Notes
We really encourage pre-hospital EMS to have stroke protocols that are quick and easy, to scoop and go, the process needs to be aligned as much as possible with acute MI processes.

Presenter
Presentation Notes
The Montana Stroke Network is a great resource for all rural hospitals, their website is included in the resources as the end. This is an example of a quick stroke scale EMS can use utilizing the Cin. Stroke Scale

Neurological Assessment Patient With Stroke-Like Symptoms
Exam elements:Level of consciousnessPupils and gazeArm and leg motor exam
strength and overall coordinationFacial symmetry and smile effortSpeech and understanding
Slurred speechClear but nonsensical speechProblems understanding simple commands
Must be quick and simple
Presenter
Presentation Notes
This slide contains animations that can be advanced by clicking your mouse.

The Emergency Room


Presenter
Presentation Notes
Along with a standardized order set, a nursing care plan is helpful to maintain the timelines and processes

Presenter
Presentation Notes
The NIH SS is the neuro specific exam for stroke patients that is a proven indicatin of stroke severity. It often drives decision making by stroke experts. Scored from lower to higher (worse) this version is the modified NIHSS. We are conducting research on a NIHSS in PE to simplify the neuro specific wording to increase accuracy for those who don’t use the tool frequently. Stay tuned

Beware!Common errors to avoid….
Blood PressureDo not treat elevated blood pressure unless > 220 systolic or, diastolic > 115Treating with t-PA must be below 185/110 The brain needs the perfusion, can worsen stroke if lower blood pressure too low
IV FluidsAvoid glucose containing solutionsCorrect hypotension and volume deficits from dehydration otherwise run fluids TKO

STAT Non-Contrast Head CT
Two pts both present w/ L sided weakness:A. Ischemic stroke R. hemisphere – not yet visibleB. R. hemispheric intracerebral hemorrrhage

tPA Administration Considerations
Must be started before 3 hours from onset (last normal)No blood on head CTReview patient’s history for other risk factorsAccurate inclusion / exclusionRecord weightBP less than 185/110 to treat
http://www2.massgeneral.org/stopstroke/protocolThromIVAdmin.aspx
Presenter
Presentation Notes
BP treatment labatolol 10-20 mg IV over 1-2 min., may repeat x1 or nirtropaste 1-2 in. Patient should not receive tPA if treatment fails

Hemorrhage SuspectedSTOP TPA INFUSION, call MD immediatelyStat head CT without contrastDraw blood for PT, PTT, plt ct, fibrinogen, and type and holdPrepare for administration of cryo and or platelets

Drip and Ship?

Remote Expert Options:
503-494-9000 Future?
< OR >
Phone Consultation
Bring the expert to you viaTelestroke


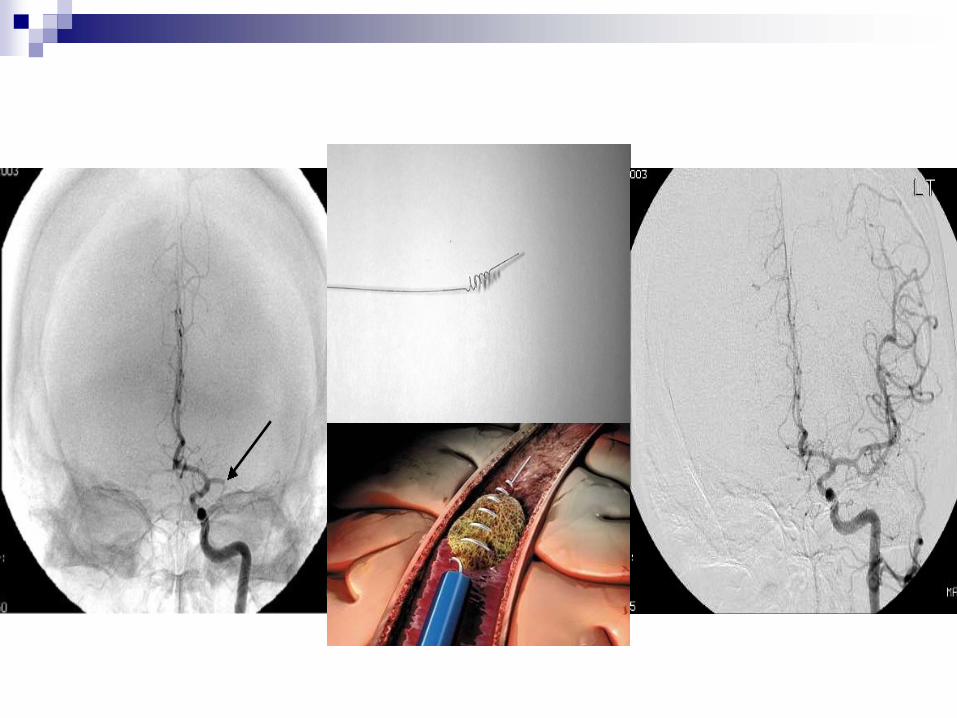
Other Treatment Options for Ischemic Strokes
If symptom onset is greater than 3 hrs ~consider up to 8 hrs:
Interventions (IA, Merci, stenting) Clinical Trials
Treatment Cont…If not a tPA candidate, ASA in ED. Rectal ASA if fails swallow eval. or if swallow eval. not complete. Keep NPO, until a formal swallow eval. is done.Admit as Inpatient and perform diagnostic testing: Carotid US, Echo, TEE, ECG monitoring for a-fib, MRI, fasting Lipid, Clotting disorder blood work (Antiphospholipid, Factor V, Antithrombin III)Rehabilitation

Presenter
Presentation Notes
Hopefully pts npo up until this point… you can’t tell by NIHSS or looking if someone has compromised swallow. One of the best ways to prevent complicatons, asp. Pneumonia, is to do a BSS. Not time consuming and can save a life
In-patient ConsiderationsNursing Issues
Started on stroke prevention medications (antithrombotic within 48 hr)?Clinical pathway followed?Blood pressure within appropriate parameters (Mean 100) Know signs of suspected Intracranial Hemorrhage and actions to take (change in LOC?)DVT prophylaxis addressed by day 2? Compression Devices/Lovenox/heparin SQ per ordersTherapies seeing patient? Review PT/OT/ST recommendations
Presenter
Presentation Notes
BP unless heart is at risk, no acute treatment is needed. If BP is normal can increase blockage and worsen stroke, maximize blood flow and minimize damage. Turn q 2, elevate paralytic extrem, avoid IV in paralytic arm

Inpatient Cont…
IV fluids (Normal Saline or LR)?Nutrition? Dietary evaluation. Assistive devices for feeding. SWALLOW SCREEN DONE? Fever? Treat if greater than 99 F with TylenolBlood glucose within appropriate parameters? Obtain sliding scale if necessary.Positioning? Pillows under affected limbs. Turn Q2hours. Accommodate limitationsRehab consults as soon as possible, if needed

Hemorrhagic Stroke Treatment
Do not give antithrombotics or anticoagulantsMonitor and treat blood pressure greater than 150/105 (Table 6, 2005 Guidelines update)NPO, until swallow eval is completedAnticipate Neurosurgical consultPossible administration of blood products
Presenter
Presentation Notes
BP treatment - nipride

Stroke‐ready Dispatch and EMS personnel Clear routing to stroke‐ready hospitalsStroke‐ready ED’s/hospitals/transfer systemsResponsive ED/stroke care teamInterdisciplinary, regional or state‐wide team to develop all of the above
The ideal stroke system interface

Small rural hospital SE Oregon..Scenario #2… future
Providers will be educated on diagnosis and stroke optionsWill call experts for advise ASAPMay treat with tPA at rural hospitalPatient will be rapidly transferred to appropriate Primary / Comprehensive Stroke Center for treatment and/or further care.Inpatient protocols to guide best care

Building the Oregon Stroke System of Care: Connecting Rural and Urban Populations to Improve Outcomes
Third Annual Meeting of the Oregon Stroke Network In Collaboration with Oregon EMS & Trauma Systems ProgramOctober 23, 2009Riverhouse Resort, Bend, OR
Information will be posted on the Office ofRural Health website

Resources
Providence Stroke Center, www.providence.org/[email protected] 503-216-1011
Montana Stroke Network, www.montanastroke.org (rural protocols/templates)
2008 Hospital Survey conducted by Heart Disease and Stroke Prevention Program with the Hospital association: http://www.oregon.gov/DHS/ph/hdsp/docs/hospcapacityrpt0929.pdf2008
Northwest Regional Stroke Network Burden Report http://www.doh.wa.gov/cfh/NWR-Stroke-Network/publications/NWRSN-Burden-Doc.pdf
2007 EMS survey conducted by the Heart Disease and Stroke Prevention Program and the AHA/ASA
http://www.oregon.gov/DHS/ph/hdsp/docs/emssurvey07.pdf
Heart Disease and Stroke Prevention Program data and data related reports are at: http://www.oregon.gov/DHS/ph/hdsp/pubs.shtml

Oregon State Stroke System of Care(Recommendations for the American Stroke Association’s Establishment of Stroke Systems of Care can be found at http://stroke.ahajournals.org/cgi/content/full/36/3/690)opportunities for your hospitals to get involved with1. Oregon Stroke Network:
• Steering Committee, • Symposium Planning Committee• Delivery of Care- EMS Subcommittee• Data/Quality Improvement/ Surveillance Subcommittee: TBD
2. NWRSN:http://www.doh.wa.gov/cfh/NWR-Stroke-Network/default.htm3. Annual OR Stroke Symposium in October, Bend 20094. Get With The Guidelines: Stroke5. Stroke Camp for Families living with Aphasia6. Telemedicine/ Telehealth: Oregon Health Network (in development)