Stroke Blood Supply Obj - First Aid
3
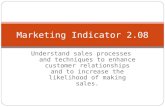
NEUROLOGY NEUROLOGY—ANATOMY AND PHYSIOLOGY SECTION III 459 Cerebral arteries—cortical distribution Anterior cerebral artery (supplies anteromedial surface) Middle cerebral artery (supplies lateral surface) Posterior cerebral artery (supplies posterior and inferior surfaces) Watershed zones Between anterior cerebral/middle cerebral, posterior cerebral/middle cerebral arteries. Damage in severe hypotension upper leg/upper arm weakness, defects in higher-order visual processing. Regulation of cerebral perfusion Brain perfusion relies on tight autoregulation. Cerebral perfusion is primarily driven by PCO 2 (PO 2 also modulates perfusion in severe hypoxia). Therapeutic hyperventilation ( PCO 2 ) helps intracranial pressure in cases of acute cerebral edema (stroke, trauma) via cerebral perfusion by vasoconstriction. Cerebral blood flow Hypoxemia increases cerebral perfusion pressure only when PO 2 < 50 mmHg Cerebral perfusion pressure ∝ PCO 2 until PCO 2 > 90 mmHg Arterial gas pressure (mmHg) 50 100 150 Arterial gas pressure (mmHg) 40 80 120 Normal Cerebral blood flow Normal normal PO 2 normal PCO 2 O 2 CO 2
description
Stroke and blood supply
Transcript of Stroke Blood Supply Obj - First Aid
-
N E U ROLOGY ` N E U ROLOGYANATOMY AN D P HYS IOLOGY SECTION III 459
Cerebral arteriescortical distribution
Anterior cerebral artery (supplies anteromedial surface)Middle cerebral artery (supplies lateral surface)Posterior cerebral artery (supplies posterior and inferior surfaces)
Watershed zones Between anterior cerebral/middle cerebral, posterior cerebral/middle cerebral arteries. Damage in
severe hypotension p upper leg/upper arm weakness, defects in higher-order visual processing.
Regulation of cerebral
perfusion
Brain perfusion relies on tight autoregulation.
Cerebral perfusion is primarily driven by
PCO2 (PO2 also modulates perfusion in severe
hypoxia).
Therapeutic hyperventilation (r PCO2) helps r intracranial pressure in cases of acute cerebral edema (stroke, trauma) via r cerebral perfusion by vasoconstriction.
Cerebral blood flow
Hypoxemia increases cerebral perfusion pressureonly when PO2 < 50 mmHg
Cerebral perfusion pressure PCO2 untilPCO2 > 90 mmHg
Arterial gaspressure (mmHg)50 100 150
Arterial gaspressure (mmHg)40 80 120
Normal
Cerebral blood flow
Normal
normal PO2
normal PCO2
O2
CO2
TashaHighlight
-
N E U ROLOGY ` N E U ROLOGYANATOMY AN D P HYS IOLOGYSECTION III460
Effects of strokes
ARTERY AREA OF LESION SYMPTOMS NOTES
Anterior circulation
MCA Motor cortexupper limb and face.
Sensory cortexupper limb and face.
Temporal lobe (Wernicke area); frontal lobe (Broca area).
Contralateral paralysisupper limb and face.
Contralateral loss of sensationupper and lower limbs, and face.
Aphasia if in dominant (usually left) hemisphere. Hemineglect if lesion affects nondominant (usually right) side.
ACA Motor cortexlower limb.
Sensory cortexlower limb.
Contralateral paralysislower limb.
Contralateral loss of sensationlower limb.
Lenticulo-
striate
artery
Striatum, internal capsule. Contralateral hemiparesis/hemiplegia.
Common location of lacunar infarcts, 2 to unmanaged hypertension.
Posterior circulation
ASA Lateral corticospinal tract.
Medial lemniscus. Caudal medullahypoglossal nerve.
Contralateral hemiparesisupper and lower limbs.
r contralateral proprioception. Ipsilateral hypoglossal dysfunction
(tongue deviates ipsilaterally).
Stroke commonly bilateral.Medial medullary syndrome
caused by infarct of paramedian branches of ASA and vertebral arteries.
PICA Lateral medullavestibular nuclei, lateral spinothalamic tract, spinal trigeminal nucleus, nucleus ambiguus, sympathetic fibers, inferior cerebellar peduncle.
Vomiting, vertigo, nystagmus; r pain and temperature sensation from ipsilateral face and contralateral body; dysphagia, hoarseness, r gag reflex; ipsilateral Horner syndrome; ataxia, dysmetria.
Lateral medullary (Wallenberg)
syndrome. Nucleus ambiguus effects are
specific to PICA lesions. Dont pick a (PICA) horse
(hoarseness) that cant eat (dysphagia).
AICA Lateral ponscranial nerve nuclei; vestibular nuclei, facial nucleus, spinal trigeminal nucleus, cochlear nuclei, sympathetic fibers.
Middle and inferior cerebellar peduncles.
Vomiting, vertigo, nystagmus. Paralysis of face, r lacrimation, salivation, r taste from anterior 23 of tongue, r corneal reflex. Facer pain and temperature sensation. Ipsilateral r hearing. Ipsilateral Horner syndrome.
Ataxia, dysmetria.
Lateral pontine syndrome. Facial nucleus effects are specific to AICA lesions.
Facial droop means AICAs pooped.
PCA Occipital cortex, visual cortex. Contralateral hemianopia with macular sparing.
Basilar artery Pons, medulla, lower midbrain,
corticospinal and corticobulbar
tracts, ocular cranial nerve nuclei,
paramedian pontine reticular
formation.
Preserved consciousness and
blinking, quadriplegia, loss of
voluntary facial, mouth, and
tongue movements.
Locked-in syndrome.
TashaHighlight
TashaHighlight
TashaHighlight
TashaHighlight
-
N E U ROLOGY ` N E U ROLOGYANATOMY AN D P HYS IOLOGY SECTION III 461
Effects of strokes (continued)
ARTERY AREA OF LESION SYMPTOMS NOTES
Communicating arteries
ACom Most common lesion is aneurysm. Can lead to stroke. Saccular (berry) aneurysm can impinge cranial nerves.
Visual field defects. Lesions are typically aneurysms, not strokes.
PCom Common site of saccular aneurysm. CN III palsyeye is down and out with ptosis and pupil dilation.
Lesions are typically aneurysms, not strokes.
Aneurysms In general, an abnormal dilation of artery due to weakening of vessel wall.
Berry aneurysm Occurs at the bifurcations in the circle of
Willis A . Most common site is junction
of the anterior communicating artery and
anterior cerebral artery. Rupture (most
common complication) leads to subarachnoid
hemorrhage (worst headache of life) or
hemorrhagic stroke. Can also cause bitemporal
hemianopia via compression of optic chiasm.
Associated with ADPKD, Ehlers-Danlos
syndrome, and Marfan syndrome. Other risk
factors: advanced age, hypertension, smoking,
race (q risk in blacks). A Berry aneurysm. Coronal (left) and sagittal (right) contrast CT shows berry aneurysm (arrows). Charcot-Bouchard
microaneurysm
Associated with chronic hypertension; affects
small vessels (e.g., in basal ganglia, thalamus).
Central post-stroke
pain syndrome
Neuropathic pain due to thalamic lesions. Initial sensation of numbness and tingling followed in
weeks to months by allodynia (ordinarily painless stimuli cause pain) and dysaesthesia. Occurs in
10% of stroke patients.
TashaHighlight
TashaHighlight
TashaHighlight