stops night terrors.s3.amazonaws.com/gscprogram/Expert+Call...NIGHT TERRORS ARE COMMON • Affects...
22
stops night terrors.
Transcript of stops night terrors.s3.amazonaws.com/gscprogram/Expert+Call...NIGHT TERRORS ARE COMMON • Affects...

stops night terrors.

Confidential – Do Not Distribute
THE CHILDREN’S SLEEP COMPANY
LULLY

Andy Rink, MDCMO/Co-Founder
Indiana University School of Medicine - MDNorthwestern University – General Surgery Residency
Specialty Fellow, Stanford Biodesign
Mark Mahowald, MDSleep Medicine
University of Minnesota
Shannon Sullivan, MDPediatric Sleep Medicine
Stanford University
Donna McMillan, MDPediatricsPalo Alto
Medical Foundation

NIGHT TERRORS ARE COMMON
• Affects 2-12 year olds
• INCIDENCE: 3.8% = 1.5 M kids per year• PREVALENCE: 8.3% = 3.6 M kids
[1] Nguyen BH, Pérusse D, Paquet J, et al. Sleep terrors in children: a prospective study of twins. Pediatrics. 2008;122(6):e1164-7. [2] Petit D, Touchette E, Tremblay RE, Boivin M, Montplaisir J. Dyssomnias and parasomnias in early childhood. Pediatrics. 2007;119(5):e1016-25. [3] Laberge L, Tremblay RE, Vitaro F, Montplaisir J. Development of parasomnias from childhood to early adolescence. Pediatrics. 2000;106(1 Pt 1):67-74. [4] Simonds JF, Parraga H. Prevalence of sleep disorders and sleep behaviors in children and adolescents. J Am Acad Child Psychiatry. 1982 Jul;21(4):383-8. [5] Fisher HL, Lereya ST, Thompson A, Lewis G, Zammit S, Wolke D. Childhood parasomnias and psychotic experiences at age 12 years in a United kingdom birth cohort. Sleep. 2014;37(3):475-82. [6] Ohayon MM, Guilleminault C, Priest RG. Night terrors, sleepwalking, and confusional arousals in the general population: their frequency and relationship to other sleep and mental disorders. J Clin Psychiatry. 1999;60(4):268-76. [7] Bjorvatn B, Grønli J, Pallesen S. Prevalence of parasomnias in the general population. Sleep Med. 2010;11(10):1031-4.

NIGHT TERRORS
• Signs– Suddenly act in fear, pain with crying, scream– Child unresponsive to external stimuli– Amnesia for episode– Occur within 4 hours of sleep onset
[1] American Academy of Sleep Medicine. The international classification of sleep disorders, revised. 2001: 142-161.

NIGHT TERRORS
• Diagnosis– Parent history– No referral needed unless concerns for other
sleep disorder
[1] American Academy of Sleep Medicine. The international classification of sleep disorders, revised. 2001: 142-161.


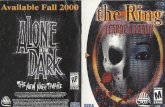
CAUSE OF NIGHT TERRORS
Awake
REM
Deep
Light
one
mechanism: underlying slow wave sleep (deep sleep) abnormality
occurs each night, independent of whether a night terror will occur
[1] Zadra A, et. al. Somnambulism: clinical aspects and pathophysiological hypotheses. Lancet neurology 2013;12:285-94. [2] Guilleminault CG, et. al. NREM sleep instability in children with sleep terrors: The role of slow wave activity interruptions. Clinical Neurophysiology 2008;119:985-992.

DISCUSSION
• How often do you see a child with night terrors?
• How do you manage night terrors?
Confidential – Do Not Distribute

TREATMENT
• Education, reassurance• Scheduled awakenings
one
Confidential – Do Not Distribute

THE PROBLEM
• Scheduled awakenings– Full awakenings– Hard to know what time to do SA– Hard to remember to do it each night– Low compliance
Confidential – Do Not Distribute

THE SOLUTION:
Guide parents through SA’s
Partial awakeningPrecise timingHigh engagement
Works with behavior changes, sleep hygiene improvement
Confidential – Do Not Distribute

HOW PARENTS USE IT1. Placed under the mattress2. Answer 3 questions in Lully app
Confidential – Do Not Distribute

CLINICAL STUDY OVERVIEW
Design: Prospective study, n=12 children with severe, chronic night terrors. Nightly device use for 4 weeks
Confidential – Do Not Distribute
2 weeks 4 weeks 4 weeksBaseline Therapeutic phase (device use period) Follow up
Screening: phone screen, full history, PSQ-SDB (screen for OSA)
nightly device use, nightly sleep lognightly sleep log nightly sleep log
Outcome: Night terror reduction after 4 weeks of device use and 4 week follow up

INDIVIDUAL DATA
Confidential – Do Not Distribute

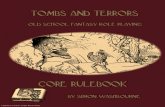
NIGHT TERROR REDUCTION
Confidential – Do Not Distribute
2 week baseline Weeks 3, 4
Mean # nt’s 14.63 3.63
SD 11.96 4.93
p 0.0051
reduction in night terror episodes (primary endpoint)
75%

CLINICAL – RESULTS
• Night terror reduction was high– After 4 weeks of device use: 75% (p=0.005)– After 4 week follow up: 88% (p=0.127)
• No serious adverse events (SAEs) reported– 1 family reported transient early rising in the
morning (qualitative)• 1 family reported nocturnal enuresis
improved with device use
Confidential – Do Not Distribute

"Un-f***ing-believable!”
“Night-terror free!!”
“I haven't known a normal night in over 2 years so thank you so much!“
“You were on our list of things to be thankful for this holiday season! You have brought so much peace to our
family. Thank you for giving us hope and peace!“
Confidential – Do Not Distribute
Edy G., Atlanta
Cathy F., Seattle
Roger P., New York
Emily H., Minneapolis

PRODUCT REVIEWS
Confidential – Do Not Distribute

WORKING WITH PARENTS
Confidential – Do Not Distribute
Provide parents with night terrors pdf and recommend product

AFFILIATE PROGRAM
• Custom affiliate link for Gentle Sleep Coaches– http://www.shareasale.com/r.cfm?B=813623&U=106
4310&M=63129&urllink=www%2Eshareasale%2Ecom%2Fshareasale%2Ecfm%3FmerchantID%3D63129
• 20% flat commission– Approx $25 for Lully Sleep Guardian original– Approx $40 for Lully Sleep Guardian Plus