Staying Balanced Spring 2008 1. “Universal solvent” 60% of body’s weight Cells “haf to...
80
Staying Balanced Spring 2008 1
-
Upload
cassandra-hopkins -
Category
Documents
-
view
215 -
download
1
Transcript of Staying Balanced Spring 2008 1. “Universal solvent” 60% of body’s weight Cells “haf to...
Staying Balanced
Spring 2008
1

“Universal solvent”60% of body’s weightCells “haf to have it.”
▪ –Arnold Schwarzenegger
2
154# person x .60 (60%) = 92# Water is approx 8# per gallon 11 ½ gallons water (Obese people/ less) (Thin people/ more) Infants Elders
3

The fundamental unitRequires:
Cell membrane Enzymes Internal membranes Genetic material
4
EpithelialConnectiveMuscleNervous
5
All metabolic reactions occurThe precise regulation of volume and
composition of body fluid is essential to health.
6
Intracellular Fluid - ICFExtracellular Fluid – ECF
Intravascular Fluid- Plasma Interstitial Fluid
7

Fluid in all body cells75% of the water (60%)
31.50 L (70 kg adult)40% of total body weight
8
20% of water (60%)10.50 L (70 kg adult))
Includes intravascular and interstitial compartments
9

Intravascular
4% of (60%)
▪ 7.5 L
10
Interstitial 16% of (60%)
▪ 17.5 LFluid between cells and outside
the vascular bed Connective tissue, cartilage, bone,
CSF, intraocular fluid
11
Water – Universal Solvent
Intake & Output (I&O)
12
HomeostasisThe body’s need for balance
13

Newborns – TBW ~ 80%
Children – TBW ~ 60-65%
Elders – TBW < ~ 60%
14
Food - 1200 mlDrink - 1000 mlMetabolic
sources - 300 ml
= 2,500 ml
Lungs - 400 mlKidneys - 1500 mlSkin - 400 ml Intestine (Feces) -
200 ml
= 2,500 ml
15

Osmoreceptors - anterior hypothalamus
Baroreceptors - carotid sinus, aortic arch, kidneys High and low blood pressure
16

Anti-diuretic hormone (ADH) If tide goes out Pituitary Gland Excretes
Tide comes in!!!▪ Re-absorb from kidneys▪ Decrease urine
Thirst also regulates
17
Abnormal decrease in TBW
Thus the weigh-in at fires
Rarely involves only water loss
Electrolyte loss
18
Signs and symptoms?
Treatment?
19

GI losses N/V/D
Insensible losses Normal losses + with fever Hyperventilation High Environmental Temps
Increased sweating
20
Internal losses “Third” spacing
▪ Peritonitis
▪ Pancreatitis
▪ Malnourished▪No protein to retain water
21
Plasma Losses
Burns
Surgical Drains
Open Wounds
22

Signs of shockSkin changes (turgor)Orthostatic hypotensionThirst Increased pulse rateFurrowed tongue
23

Decreased BP Dry mucosa Infants: Anterior fontanelle sunken
▪ Dry diapers
▪ Absent tears
▪ Cap refill > 2 seconds
▪ Dry mucosa
24
O2
ABCsFluids
Flavor?Consider PASGECG
25
EdemaPeripheral vs. central (more later…)
Aggressive treatment if Pulmonary Edema
26
ABCsO2
Consider ETTMeds:
NTG. Lasix M.S.
27
Medical causes Diabetes Heat
Emergencies Blood Loss
Traumatic causes Blood loss
28

In H2O dissociate into ionsCations = positiveAnions = negative
29
Sodium (Na+) Prevalent in ECF
▪ “Water follows it” Nerve impulses Hyper/ Hyponatremia
Potassium (K+) Prevalent in ICF Nerve impulses Hypo/ Hyperkalemia
30
Calcium (Ca++) Prevalent in ICF Muscle contraction Nerve impulse Hypo/hypercalcemia
31

Magnesium (Mg++) Present in ICF
Necessary for many processes Found in some:
Antacids Laxatives
Most associated with phosphate Renal Functions
32
Chloride (Cl-) Present in ECF Balances cations Fluid balance Renal function Usually found hanging around sodium
33

Bicarbonate (HCO3-)
Found in ECF
The Buffer Neutralizes Acidic (H+)
Tx for acidosis
34

Phosphate (HPO4--)
Found in ICF - buffer
Energy stores
Mg++ in renal function
35

Electrolytes - mEq/LNon-Electrolytes -
Glucose
Urea
Proteins
36

OsmosisDiffusionActive TransportFacilitated Diffusion
37
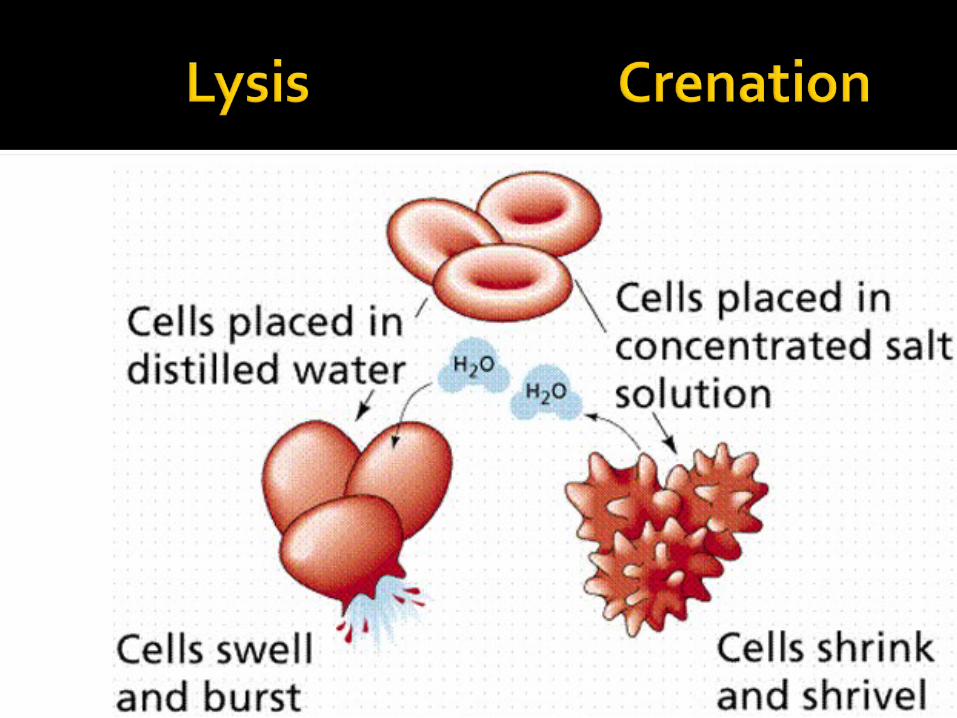
IsotonicHypertonicHypotonicOsomotic gradient - difference in
concentration
38

Movement of
water
(solvent)
Semi-
permeable
membrane
Towards
higher solute
concentration39
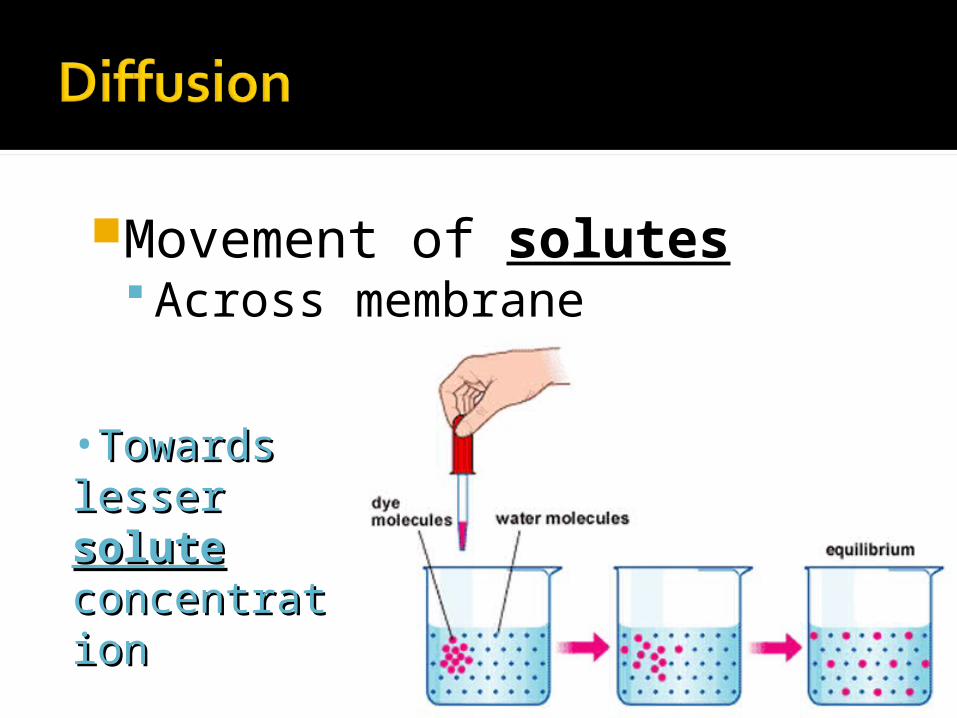
Movement of solutes Across membrane
40
•Towards Towards lesser lesser solutesolute concentrationconcentration
Movement of solutesAcross membrane
Against osmotic gradientRequires energy (ATP)
Sodium-potassium pump
41

42

Helper proteins Insulin
Open gateGlucose
43

44
Governs movement of water and solutes across cell membrane
Pressure exerted by concentration of solutes
Pulls from other side of membrane
45
46
Colloid osmotic pressure Plasma
Hydrostatic pressure Blood pressure
▪ Filtration
47
Localized Site of injury Organ systems - brain, lungs, heart,
abdomen
Generalized Dependent edema
▪ Pitting edema48

Body water in interstitial
spaces not available for
metabolism
Relative dehydration
49
Decrease in production of plasma
proteins Liver disorder
Burns
Open wounds
50

Increase in hydrostatic pressure Venous obstruction Salt and water retention Thrombophlebitis Liver obstruction Tight clothing Prolonged standing
51
Increased capillary permeability - plasma proteins escape Inflammation and immune response Allergic reactions Burns Trauma Cancer
52
Lymphatic channel obstruction Infection
Surgery
53

54
Blood transfusions
Plasma Formed Elements
Leukocytes (WBCs)Erythrocytes (RBCs) >99%Thrombocytes
55

Mostly Water (92%)
56
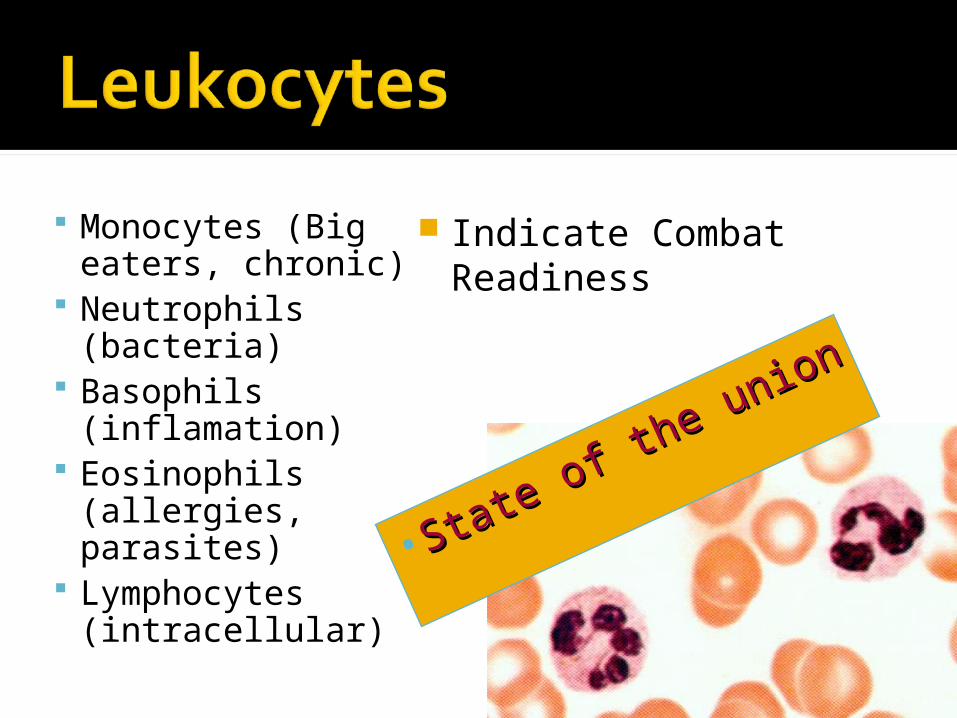
Monocytes (Big eaters, chronic)
Neutrophils (bacteria)
Basophils (inflamation)
Eosinophils (allergies, parasites)
Lymphocytes (intracellular)
Indicate Combat Readiness
57
•State of the union
State of the union
Transports oxygen40-45% Hematocrit
After specimen is
spunHemoglobin -
Iron-based compound;
binds with oxygen
58
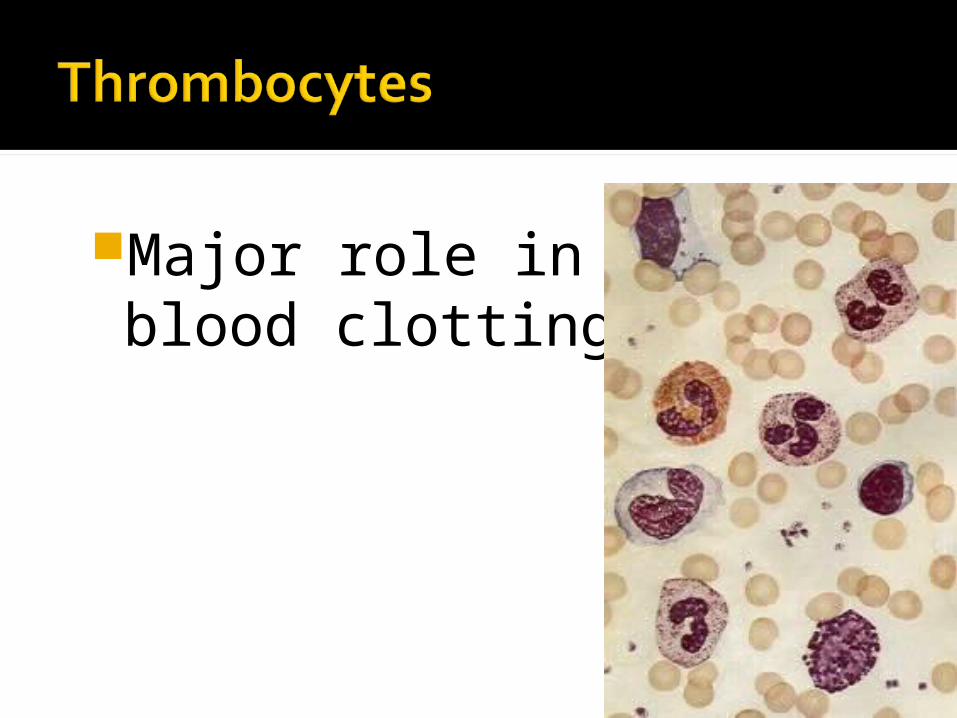
Major role in blood clotting
59
Determined by ratio of plasma to formed elements
60
AntigensBlood type proteins
AntibodiesResistance (in serum)
61
A A Antigen B Antibody
B B Antigen A Antibody
AB A & B Antigen No Antibodies “Universal Recipient”
62

ONo AntigensA & B Antibodies (serum)
“Universal Donor”
63

Measured in + or –+ = Anti-Rh antibodies present
- = Ok.- = No Anti-Rh antibodies pres.
- = Ok + = Sensitization ++ = Severe reaction / death
64

Blood type Volume infused Time
Packed Cells:
Preferred method
250-350 ml 2 – 3 hours
Whole blood: 550 ml 2 – 3 hours
Leukopoor RBCs:
Prevents febrile non-hemolytic reactions
250 – 500 ml 2 – 3 hours
65

Blood type Volume infused Time
Irradiated RBCs
Used in immunodeficient clients
250 – 350 ml 2 – 3 hours
Fresh frozen plasma:
Has most coagulation factors
Used in DIC, liver disease
200 – 250 ml 1 hour
66

Physician’s order Check type and cross-match; verify with
partner Check blood bag for bubbles, cloudiness,
dark color, sediment Check patients vital signs
Temperature BP Pulse Respirations
67
Rotate blood bag gently Pull back tabs on blood unit bag,
expose port. Spike blood bag port carefully and hang
unit. (Be sure clamp is closed). Open clamp and fill drip chamber. Make
sure filter is submerged in blood. Open clamp on tubing, carefully run
blood through tubing, and place needle on end of tubing.
68
Check primary IV solution – Never use dextrose solutions!
Attach blood tubing into IV port and tape into place.
Shut off primary IV and begin transfusion.
Administer blood slowly for first 15 minutes, ~ 20 gtts/min. ALLOWS TIME TO OBSERVE FOR
ADVERSE REACTION
69

When blood bag is empty, clamp off tubing to bag, open clamp to normal saline bag, and flush line.
Close all clamps and remove blood tubing from injection port.
Monitor patient for s/s of transfusion reaction.
70

S/SSudden increase in temperature (may be 105o)
Hypotension
Dry, flushed skin
Abdominal pain
Headache
Lumbar pain
Sudden chill
Urticaria
Respiratory wheezing, laryngeal edema
71

Stop transfusion immediately Change tubing Observe for shock Monitor vitals every 15 minutes until
stable Keep blood tubing and bag for ED staff. Control hyperthermia Consider antihistamine if allergic
reaction
72
A 40 y/o male driver involved in a head-on collision at ~ 40 mph. Pt is seat belted with a lap belt only. Pt is CAO PPTE on arrival, c/o acute abd. Pain and SOB. P – rapid, thready BP – unable to auscultate RR – rapid
73

DDX?
Why?
TX?
Why?
74

This patient is 82 y/o, and calls you at 0030, c/o feeling ill.
Pt is CAO PPTE, but slow to respond B/P 120/76 P 94, irreg. RR 24 Skin cool, dry, pale Mucous membranes dry with
furrowed tongue and sunken eyes75

DDX?
Why?
Tx?
Why?
76
You are called to a 60 year old male c/o SOB, chest pain. His sx started ~ 2 hrs ago while painting the garage. He says the chest pain went away almost immediately, but he’s increasingly short of breath.
PMH: Pulmonary edema, Angina, HTN, recent URI
77

Pt is CAO PPTE, anxious, in tripod position. BBS decreased with coarse crackles in the
bases BP 130/60 HR 126, sl irreg. RR 36, shallow Skin pale, cool, dry with poor turger, dry
mucous membranes, furrowed tongue78

DDX?
Why?
Tx?
Why?
79

80