statistical modelling of the effect of meteorological parameters on occurrence of measles
42
STATISTICAL MODELLING OF THE EFFECT OF METEOROLOGICAL PARAMETERS ON OCCURRENCE OF MEASLES IN AKURE. ADEYEMI ADEDAYO OLALEKAN (2016)
-
Upload
adeyemi-adedayo -
Category
Documents
-
view
13 -
download
0
Transcript of statistical modelling of the effect of meteorological parameters on occurrence of measles

STATISTICAL MODELLING
OF THE EFFECT OF
METEOROLOGICAL
PARAMETERS ON
OCCURRENCE OF MEASLES
IN AKURE.
ADEYEMI ADEDAYO OLALEKAN
(2016)
1
CERTIFICATION
I certify that this Project “entitled Statistical modelling of the effect of meteorological
parameters on the occurrence of measles in Akure, Ondo state, Nigeria.” is as a result of the
research undertaken by Adeyemi Adedayo Olalekan with matriculation number
MET/11/4698 and was carried out under the supervision of Dr A. Akinbobola of the
department of Meteorology and Climate Science, Federal university of technology, Akure,
Ondo State
………………………………… ……………………
Dr A. Akinbobola Date / Signature
………………………………… ……………………...
Dr. E.C. Okogbue Date / Signature
(H.O.D.)

2
DEDICATION
This report is dedicated to Almighty God, my source of inspiration and guidance throughout
the period as undergraduate and also to my loving parent Mr. & Mrs. Adeyemi and siblings for their
support throughout the period.

3
ACKNOWLEDGEMENT
My sincere gratitude goes to almighty God for granting me good health, peace and success
throughout my undergraduate program.
Also my appreciation goes to my parent Mr. and Mrs. Adeyemi for their unending love,
support both financially and morally, may the good Lord bless you.
To my dear brothers and sister; Adeyemi Oluwaseun, Adeyemi Temitope, Adeyemi Titilayo
and Adeyemi Tobiloba and to my roommates and friends; Adegbite Oluwatoba and Obafemi
Timilehin for their love and support throughout the Undergraduate program
I also want to express my profound thanks to my project supervisor: Dr. Ademola
Akinbobola who has always been there as father, a lecturer, a friend and a disciplinarian in the
course of undergoing this research.
Finally, I thank the entire lecturers of the Department of Meteorology and Climate Sciences,
F.U.T.Akure, The H.O.D. Dr Okogbue, Prof. Omotosho, Dr.A.Akinbobola, Prof. Odekunle, Prof.
A.A. Balogun,, Dr. A.Adefisan, Dr. I. Balogun, Dr. V. Ajayi, Dr. Oluleye, Mr R.A. Balogun, Mr. K.
Ladipo, Mr. A.B. Okunlola, Mrs B.M. Dada and Mr Gbode for their assistance in the course of this
study.

4
LIST OF TABLES
Table 1. Seasonal index for Measles Occurrence
Table 2. Quarterly index for Measles Occurrence
Table 3. Mean Monthly Correlation between measles occurrence and meteorological
variables using Spearman’s Rank Correlation coefficient
Table 4. Multiple linear regression Model equations
Table 5. Validating Measles’s Model 1
Table 6. Validating Measles’s Model 2
Table 7. Probability of monthly occurrence of Measles
Table 8. Relative Risk of meteorological parameters with respect to measles.

5
LIST OF FIGURES
Fig 1. Map of Ondo State showing Akure.
Fig 2 Map of Nigeria showing the study area, Akure.
Fig 3. Graph of annual distribution of measles
Fig 4. Mean Monthly variation of Relative Humidity and measles
Fig 5. Mean Monthly variation of Min Temp and measles
Fig 6. Mean Monthly variation of Max Temp and measles
Fig 7. Mean Monthly variation of rainfall and measles
Fig 8. Mean Monthly variation of Solar Radiation and measles
Fig 9. Seasonal trend in reported measles cases
Fig 10. Seasonal Variation of Measles with RH
Fig 11. Seasonal Variation of Measles with Tmin
Fig 12. Seasonal Variation of Measles with Tmax
Fig 13 Seasonal Variation of Measles with Rainfall
Fig 14. Seasonal Variation of Measles with Solar Radiation
Fig 15. Observed and Predicted measles patients for Model 1
Fig 16. Observed and Predicted measles patients for Model 2

6
Abstract
This research work is aimed at evaluating the effect of meteorological parameters on the prevalence
of measles using statistical method so as to help make policies related to current control and possible
future elimination strategies. Measles occurrence is a major public health concern in this country and
it is an infectious, vaccine-preventable disease. It kills an estimated 750,000 children each year.
Over half of the deaths occur in Sub-Saharan Africa. Incidence is reducing with more children
getting vaccinated.
The weather variables used are monthly Relative humidity, rainfall, solar radiation, maximum and
minimum temperature and were obtained from meteorological department of the ministry of
agriculture, fisheries and forest reserve, Akure, Ondo state. Monthly data of reported cases of
measles between 2009 and 2014 from State hospital, Akure Ondo state. Graphical representations
were used to determine the variation of weather parameters on monthly and seasonal pattern.
Spearman’s Rank correlation coefficient to test and identify the strength of the relationship between
the monthly measles incidence and the weather parameters. The P-value was used to determine the
significant level of the weather variables on the occurrence and the variables to be used in the
predictive equation. Poisson Multiple regression models in generalized Linear models (GLMs) were
used to develop predictive models. Also, Poisson probability distribution function was used to
determine the monthly probability of the occurrence of the diseases and to know the weather
variables that lead to statistical changes in clinical-reported malaria cases.
The weather variable mean monthly variation shows that Maximum temperature, Minimum
temperature and solar radiation and measles occurrence are directly related and others are inversely
related. The correlation shows that there is a huge effect of these variables on measles especially
maximum and minimum temperature and solar radiation with 0.59, 0.62 and 0.64 all at 95%
confidence level. May and April showed highest mean monthly clinical reported cases of measles
and in terms of seasons, the transition season to early rainy season have highest reported cases of
measles occurrence which accounted for 41% of the total occurrence of reported cases of measles
occurrence. Two statistical models were developed in estimating the occurrence with the first model
developed using the whole weather parameters in the study and the second model developed using
only the weather parameters that have positive correlation at 95% confidence level with measles
prevalence. The probability of occurrence of the disease estimated by both models showed that
model 2 performed better though both models underestimated. Error analysis was done to determine
the reliability of the estimated values of both model 1 and model 2 and shown graphically. The

7
relative Risk of measles occurrence associated with relative humidity, Max temp, Min temp, rainfall,
solar radiation are 0.3312, 2.4539, 29.7181, 0.98399, 0.27831 respectively with Min temperature
having the highest risk.
This research will help in estimating measles prevalence and probability of occurrence overtime with
the model developed.
Keywords: measles, weather variables, seasons, statistical model.
8
Title Page…………………………………………………………………………………………………i
Certification……………………………………………………………………………………………..ii
Dedication………………………………………………………………………………………………iii
Acknowledgements…………………………………………………………………………………iv
List of Tables……………………………………………………………………………………………v
List of Figures…………………………………………………………………………………………..vi
Abstract………………………………………………………………………………………………….vii
TABLE OF CONTENTS
CHAPTER ONE .............................................................................................................................................. 10
INTRODUCTION ......................................................................................................................................... 10
1.1. Background to the Study ............................................................................................................... 10
1.2. Statement of the Research Problem ............................................................................................... 11
1.3. Research Questions ....................................................................................................................... 12
1.4. Aim And Objectives ...................................................................................................................... 12
1.5. Significance of the Study ............................................................................................................... 12
CHAPTER TWO ............................................................................................................................................. 14
LITERATURE REVIEW .............................................................................................................................. 14
CHAPTER THREE......................................................................................................................................... 20
RESEARCH METHODOLOGY .................................................................................................................. 20
3.1. Study Area .......................................................................................................................................... 20
3.2. Data..................................................................................................................................................... 21
CHAPTER FOUR ........................................................................................................................................... 23
RESULTS AND DISCUSSION .................................................................................................................... 23
4.1. Annual distribution of Measles occurrence ........................................................................................ 23
4.2. Monthly Variation of Meteorological variables with Measles occurrence ......................................... 23
4.3. Seasonal variation of meteorological parameters and measles Occurrence ....................................... 27
4.4. Statistical relationship between Measles and meteorological variables ............................................. 31
4.5. Weather-Disease Statistical Model ..................................................................................................... 32
4.6. Probability of occurrence of the diseases ........................................................................................... 35
4.7. Models Performance ........................................................................................................................... 36
4.8. Error Analysis ..................................................................................................................................... 36
4.9. Relative Risk of meteorological parameters with respect to measles. ................................................ 37

9
CHAPTER FIVE ............................................................................................................................................. 38
CONCLUSION AND RECOMMENDATION ............................................................................................ 38
5.1. Conclusion .......................................................................................................................................... 38
5.2. Recommendation ................................................................................................................................ 39
References ........................................................................................................................................................ 40

10
CHAPTER ONE
INTRODUCTION
1.1. Background to the Study
While our personal health may seem to relate mostly to prudent local environmental
exposures and health care access, sustained population health requires the life supporting “services
“of the biosphere. Population of all animal species depend on supplies of food and water, freedom
from excess infectious diseases and the physical safety and comfort conferred by climatic stability.
The world’s climate system is fundamental to this life support (WHO, Climate Change and Human
Health-Risk and Response, 2003).The characteristics, geographical distributions and seasonal
variations of many infectious diseases are prima facie evidence that their occurrence is linked to
weather and climate. Factors such as temperature, precipitation and humidity affects the life cycle of
many disease pathogens and vectors (both directly and indirectly through ecological changes) and
this can potentially affect the timing and intensity of disease outbreaks. Human societies have had
long experience of naturally occurring climatic vicissitudes. Many diseases are highly sensitive to
changing temperatures and precipitation. These include common diseases such as malaria, typhoid,
cough, diarrhoea, measles, asthma, meningitis and dengue fever as well as other major killer such as
malnutrition and diarrhoea (WHO, Climate Change and Human Health, 2007).
Researchers such as (Kenneth, Thomas, & Rebecca, 2008) have attempted to explore this
important aspect of human life: health and how the weather elements of a place could be a
major determinant of the state of health of the people. Some of these effects are positive while
others are negative, some are direct and some indirect. These clearly indicate the nature of
relationship that exists between weather and disease variables.
Climate variability and its impacts on human health are areas of research that have been
receiving very much attention from scientists and policy makers all around the world over the last

11
decade or so. The subject of climate change and variability is older than the subject of its impacts
(Chen, 2002) Climatic factors influence the emergence and re-emergence of infectious diseases in
addition to multiple human, biological, and ecological determinants.
Climatologists have identified upward trends in global temperatures and now estimate
an unprecedented rise of 2.0 degrees centigrade by the year 2100. Of major concern is that these
changes can affect the introduction and dissemination of many serious infectious diseases (Patz,
1996)
The temporal and spatial changes in temperature, precipitation and humidity expected to
occur under different climatic scenarios could affect the biology and ecology of vectors and
intermediate hosts and consequently the risk of disease transmission (WHO, 2005). Climatic
factors, particularly temperature and rainfall, may have a profound impact on transmission cycles of
diseases by influencing the availability of vector breeding sites, extending vector longevity, altering
host breeding of migration pattern and maintaining aggregation of vectors and host around water
bodies (Hensel, 1979)
1.2. Statement of the Research Problem
The studies of the relationship between weather and the occurrence of diseases have taken
various approaches globally; (Akinyemi Gabriel Omonijo, 2011) studied the Effect of thermal
environment on the temporal, spatial and seasonal occurrence of measles in Ondo state, Nigeria.
Their result shows that a high transmission of measles occurred in the months of January to May
during the dry season when human thermal comfort indices are very high. (Bukhari, 2009) Studied
temperature and rainfall variability and the outbreak of meningitis and measles in Zaria L.G.A. He
observed that measles showed a negative relationship with rainfall. There is no study to the best of

12
my knowledge that correlates several climatic elements with common diseases and builds a statistical
model to show the effect and help predict future occurrences especially in the study area.
1.3. Research Questions
1. What is the relationship between this disease and weather condition?
2. Does the occurrence of this disease exhibit seasonality?
1.4. Aim And Objectives
Aim
To evaluate the effect of meteorological parameters on the prevalence of measles
using statistical methods
Objectives
The objectives of this project are to;
assess the correlation between meteorological parameters and the prevalence of measles
generate a weather-disease statistical model which can be used to estimate the number of
occurrence.
1.5. Significance of the Study
Climate is an inevitable dominant element of man’s environment and powerful factors
in his well-being. Its critical elements such as temperature, rainfall and humidity can
influence diseases. Although medical science has made remarkable progress in fighting
diseases through modern technology, the health of the human population is still
influenced to a great extent by weather and climate. It is also good to know that the
13
environmental conditions that favour persistence of the vectors that transmit most of these
diseases need also to be considered.
This work investigates if any relationship exists between Max and Min temperature,
relative humidity, solar radiation and rainfall and measles occurrences and if these
parameters can be used to explain the monthly and seasonal variation in measles
occurrence. The parameters which have the most significant influence on the disease are
further studied using statistical analysis to ascertain this level of significance.
This study is quite significant because it will help in determining the role that
meteorological elements play in measles outbreak and transmission. It will also provide
information on what enhances the survival of the causative agents of the diseases. This
study therefore wishes to device a statistical model to help in prediction of future
occurrences of measles in the study area

14
CHAPTER TWO
LITERATURE REVIEW Every day man, wherever he may be on the earth’s surface has to live with the weather. In
regions of the world where weather exhibits day to day changes, it is general to open a conversation
with a few commands about the weather, with the result that we are made more and more aware of
the elements and the part they play in our lives. The geographical location is a key determinant of the
sensitivity of a species to environmental change. A change in the suitability of the weather within the
current geographical distribution of the disease will after the development, survival and reproduction
rate of vectors and pathogens and so affect the intensity of disease transmission and resultant
exposure of the population to the disease.
Scientific interest in the role of the environment, including weather and climate, in the
dynamics of infectious disease has been further stimulated by the growing problems of emergence
and re-emergency of infectious diseases despite series of intervention policies worldwide (Lipp E.K.,
2002). For example, measles has remained a public health challenge despite the enormous efforts by
the World Health Organization (WHO) and United Nations Children’s Fund (UNICEF) towards
reducing the global burden of this disease.
Measles, not just another viral exanthema is a highly communicable disease predominantly of
the pre-school and early school-age children (2-5 years). It is one of the six killer diseases of
childhood caused by a paramyxovirus commonly seen in the tropics. It is characterized by fever,
cough, coryza, and conjunctivitis. In other words, measles is also called rubella, and is a highly
contagious respiratory infection that is caused by a virus. It causes a total – body skin rash and flu-
like symptoms, including a fever, cough, and runny nose. The measles virus is from the family
parmyxovirus which normally grows, in the cell that lines the back of the throat and lungs. Measles
is a human disease and is not known to occur in animals. When the virus is breathing into the
respiratory tract of an uninfected individual, it passes through the cells of the tiny bronchioles into
15
the blood stream; the virus enters into the lymphatic system and begins to multiply or about 10-14
days (incubation period) (Duke, 2003).
Since measles is caused by a virus, there is no specific medical treatment and the virus has to
run its course. But a child who is infected should be sure to receive plenty of fluid and rest, and be
kept from spreading the infection to others (Healthscout, 2010). Severe measles is more likely among
poorly nourished young children, especially those with insufficient vitamin A, or whose immune
systems have been weakened by HIV/AIDS or other diseases. Most measles-related deaths are
caused by complications associated with the disease. Complications are more common in children
under the age of five, or adults over the age of 20. The most serious complications include blindness,
encephalitis (an infection that causes brain swelling) severe diarrhoea and related dehydration, ear
infection or severe respiratory infections such as pneumonia. As high as 10% of measles cases result
in death among populations with high levels of malnutrition and a lack of adequate health care
(Coleman, 2010). Unvaccinated young children are at highest risk of measles and its complications,
including death. Any non-immune person (who has not been vaccinated or previously recovered
from the disease) can become infected. In 2008, about 83% of the world’s children received one dose
of measles vaccine by their first birthday through routine health services-up from 72% in 2000. Two
doses of the vaccine are recommended to ensure immunity, as about 15% of vaccinated children fail
to develop immunity from the first dose.
(Akinbobola A., 2010) used Monthly temperature, relative humidity and rainfall for the
period 1990- 2003 for Akure, a city in the southwest to establish a relationship with Measles
occurrences and got threshold values of these Meteorological variables showing that high measles
attack occurred for a distinct temperature range of 32-340C if the relative humidity is not too high
(60%-80%).
(Akinbobola A., 2010) investigated if any relationship exists between temperature, relative
humidity and rainfall and measles occurrences and if these parameters can be used to explain the

16
monthly, inter-annual and seasonal variation in measles occurrence but three weather variables will
not explicitly show the relationship compared to five weather parameters.
The extensiveness of the disease at any time depends upon the number of susceptible persons
in a community. Children who are malnourished are mostly, susceptible to the disease. Young
infants between 4 and 6 months are vulnerable to measles because of reduced maternal anti bodies in
women with immunosuppressive disease (Coleman, 2010). The disease kills an average of one out of
every ten afflicted children in rural areas where treatment possibilities are very few or even non-
existent. Though as simple as the disease may look and despite that it is preventable, it is one of the
diseases with high mortality rate in children (Ray, 1970) . Most deaths are caused by complications
of the viral infection. There is increased mortality rate in infants below the age of nine (9) months
who are too young to have been vaccinated against the disease since rates of sero-conversion are
low. Measles is a handicap for the future of the community since it wipes out or disables a large
proportion of its children; therefore it calls for intervention in order to enhance or promote the future
of the community. (Ray, 1970). Despite the advent of measles vaccine, the illness remains one of the
most severe infectious diseases of the developing world. Over two Million children die of measles
each year. The greatest mortality rate is seen in the poor regions of the world where access to basic
health care services such as clinics, vaccines etc are limited (Coleman, 2010).
Genetically and anti-genetically, MeV is related closely to viruses that are pathogens of
sheep, goat and cattle ( (T, 1999); (Sheshberadaran H, 1986); weather patterns are known to play a
significant role in the transmission of such viruses ( (AG, 2007); (I.C., 2003)). Measles virus is
assumed to have evolved in an environment where the above mentioned animals and humans live in
close proximity (McNeil, 1976) after the commencement of livestock farming and domestication of
animals in the early centres of civilisation in the Middle East (Furuse Y, 2010). Today, measles
remains one of the top ten leading causes of death globally ( (Strebel P, 2003); (WHO, 2007); (GHC,

17
2009)) and remains prevalent in many developing countries, especially in parts of Africa and Asia
where more than 20 million measles cases are reported annually (WHO, 2009)
In Nigeria, measles is an important cause of childhood morbidity and mortality. In January
2007, a total of 1,346 patients were admitted to hospital due to measles, of which 62% of cases were
aged 1–4 years and 23% were between 5 and 14 years of age (WHO, 2007). Measles outbreaks have
been increasingly common in Nigeria (WHO, 2008) despite the adoption of the WHO’s four-pronged
strategy and The National Program on Immunization with the aim of reducing fatal cases of measles
to near zero. (Persinger.P., 1975) found that variability in occurrences of many diseases is related to
seasonal trends in temperatures, (although significant year-to-year differences do occur). Bronchitis,
peptic ulcers, adrenal ulcer, glaucoma, goitre and eczema are related to seasonal variations in
temperature, (W., 1963).
The studies of (Egunjobi, 1993) and (Adetunji O.O., 2007) stated that measles in Nigeria
sometimes occurs immediately after the end of the rainy season, and often reaches epidemic
proportions in the dry season during February, March and April.
There is a general agreement that weather has a profound influence on human wellbeing.
Most of the researches have been done by medical scientists and a minor amount of the work has
been performed by climatologists. For example; some of the researchers suggest that extreme
weather events appear to have the greatest influence on health. (Driscoll, 1971b) correlated daily
mortality for 10 cities with weather conditions in January, April, July and October and found that
large diurnal variations in temperature, dew-point and pressure were associated with many high
mortality days. In addition, hot humid weather with concomitant high pollutant concentrations were
also contributory mechanisms other studies do not attribute large variations in mortality to extreme
events, but rather to the normal seasonal changes in weather (Ericsson, 2010).

18
Climate has potential to alter the average exposure of human populations to vector-borne
diseases by changing the geographical distribution of condition that is suitable for the vector and
diseases pathogen. An increase in global temperature will result in an expansion of warm
temperature regiment into higher altitude and latitudes. Any associated changes in rainfall in tropical
and subtropical zones will also render habitats more or less suitable for vector. In addition, the
implications of the asymmetrical increases of temperature with global warming for the epidemiology
of victor-borne disease need to be clarified. Greater effects of low temperatures on vectors survival,
behaviour, and disease transmission in cold limited climates than from smaller and less frequent
increases in extreme maximum temperatures. These changes would make temperature environments
more receptive to many tropical vector-borne diseases while having less negative efforts on tropical
environments (Gagge, 1979).
Measles and Meningitis rarely occur, but when they occur, it is usually during the hot period
(Marcus, 2012). Socioeconomic, poor hygiene/sanitation and environmental conditions are major
driving factors responsible for the seasonal fluctuations in measles transmission in Ondo State,
Nigeria. (Akinyemi Gabriel Omonijo, 2011)
The disease kills an average of one out of every ten infected children especially in the tropics.
Most deaths are caused by complications of the viral infection such as when it is super imposed by
other bacterial infections such as streploredpneumonea or when it suppresses the immunity of the
individual. Between 1992 – 1997, the West Africa sub-region reported the highest measles morbidity
(121 measles cases per100,000 inhabitants) while significant, reduction in reported measles
incidence and mortality was observed in South Africa sub-region (Coleman, 2010). While the
African nations are still battling with the disease, the Asian and European Countries have long ago
eliminated it to almost an in-existing rate. In China, the average annual measles incidence decreased
from 9.0 to 5.7 cases per 100,000 population and mortality rate falls from less than 0.3-0.1 death per
million population as at 2000 (Coleman, 2010). Most of the studies like on association between

19
climatic variation and disease incidence could not account for the complex web of factors that
influence diseases and thus may not be reliable indicators of future change. Most of the studies only
used a single parameter of climate i e. temperature and correlate it with a single disease.
Meteorological Factors and Measles Occurrence in Akure,Ondo State, Nigeria (Akinbobola, 2010)
made use of just three weather parameters (Temperature, Rainfall, Relative humidity) to show the
relationship with measles occurrence. There is no statistical model to the best of my knowledge that
has been developed to show the effect of meteorological parameters on measles especially in the
study area. This is one of the concerns of this study. This is the gap that this study will have to fill.
The disease is most prevalent when the temperatures is in range of between 32oC to 34oC
and relative humidity of between 60% and 80%.Furthermore, at temperatures below 32oC and
relative Humidity of less than 60%, there were very few measles patients (Akinbobola, 2010).
Persinger, 1980 found that variability in occurrences of many diseases is related to seasonal trends in
temperatures, (although significant year-to-year differences do occur). Bronchitis, peptic ulcers,
adrenal ulcer, glaucoma, goitre and eczema are related to seasonal variations in temperature, (Trop,
1963).

20
CHAPTER THREE
RESEARCH METHODOLOGY
3.1. Study Area
Akure (7° 15′ 0ˈˈN, 5° 11′ 42ˈˈE) is a city in the south-western Nigeria and is the largest city
and capital of Ondo state. The city has population of 588,000 based on 2006 population census. It
has a tropical wet-and-dry climate. Ondo State has a mean annual rainfall of about 1,500 mm and
2,000 mm in the derived savannah and humid forest zones, respectively (Adefolalu, 1997)
Fig 1. Map of Ondo State showing Akure.
21
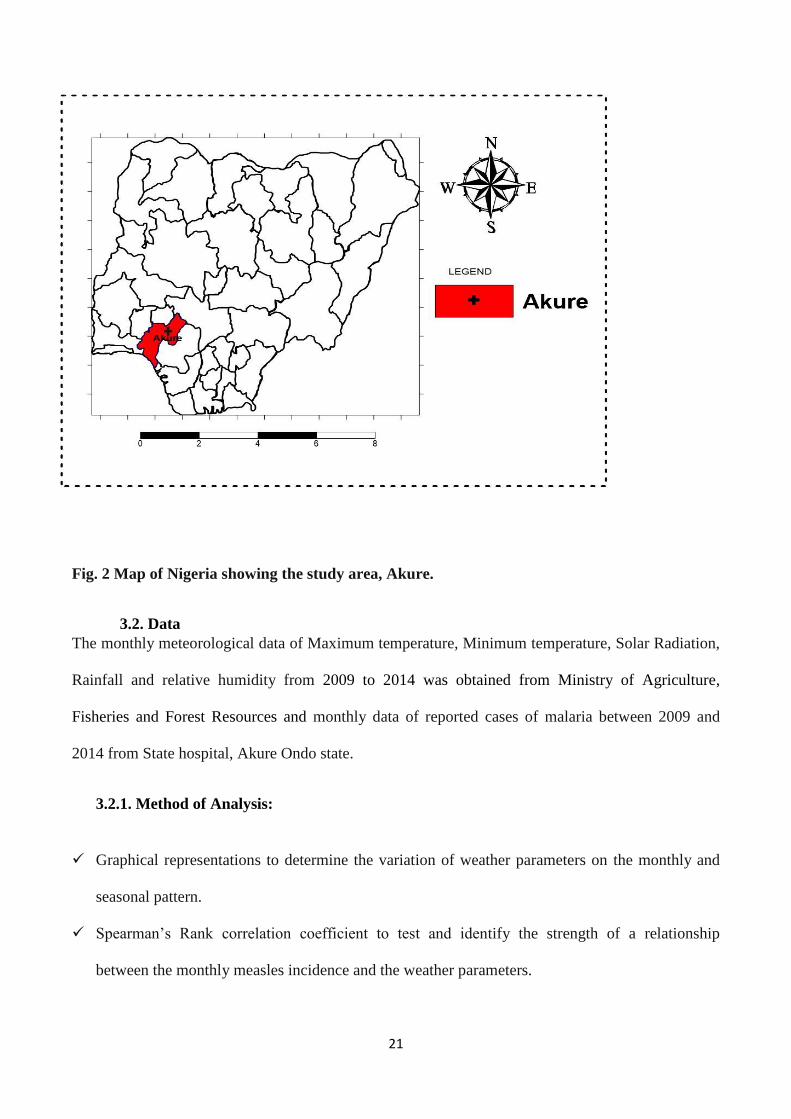
Fig. 2 Map of Nigeria showing the study area, Akure.
3.2. Data
The monthly meteorological data of Maximum temperature, Minimum temperature, Solar Radiation,
Rainfall and relative humidity from 2009 to 2014 was obtained from Ministry of Agriculture,
Fisheries and Forest Resources and monthly data of reported cases of malaria between 2009 and
2014 from State hospital, Akure Ondo state.
3.2.1. Method of Analysis:
Graphical representations to determine the variation of weather parameters on the monthly and
seasonal pattern.
Spearman’s Rank correlation coefficient to test and identify the strength of a relationship
between the monthly measles incidence and the weather parameters.

22
r = 1 - 6 ∑ 𝑑2
𝑛3−𝑛 or r = 1 –
6 ∑ 𝑑2
𝑛(𝑛2−1)
Where: d = difference btw two ranks
n = numbers of samples
The range of the spearman’s rank correlation coefficient is btw -1 to +1
The seasonal index using the formula;
Seasonal Index = Average of season
Total Average of all seasons∗ 100
Quarter Index = Average Quarter
Total average of all Quarters ∗ 100
Poisson probability distribution function will be used to build a model to determine the monthly
probability of the occurrence of the diseases and to know the weather variables that lead to
statistical changes in clinical-reported malaria cases
𝑃 (X =𝑥
𝜆) =
𝑒−𝜆λ𝑥
𝑥!
x = number of patients
λ = Monthly average
e = constant (2.87)
The Relative Risk of the effects of weather parameters on the occurrence of Measles will be
established from multiple linear equations derived. (Y = mx + c)
RR = exp(m) RR = Relative Risk
m = coefficient of the weather parameters

23
CHAPTER FOUR
RESULTS AND DISCUSSION
4.1. Annual distribution of Measles occurrence
From 2009 to 2014 the rate of reported clinical measles cases has been decreasing at the rate
of 3 patients per year (figure 3). Reported measles cases increased from 2009 to 2011, then there was
a sharp decrease from 2011 to 2012. Afterwards a sharp increase from 2012 to 2013 and finally a
decrease 2013 to 2014.
Fig 3. Graph of annual distribution of measles cases in Akure.
4.2. Monthly Variation of Meteorological variables with Measles occurrence
Variation between Relative Humidity and Measles Occurrence
Figure 4 shows the Monthly variation of Relative Humidity and Measles occurrence for the
year 2009 to 2014. It was observed that relative humidity was at its peak in August and September
while measles occurrence was in March. It can be seen that relative humidity has little effect on the
Measles = -2.5429*year + 5210.1
50
60
70
80
90
100
110
120
130
140
2008 2009 2010 2011 2012 2013 2014 2015
Mea
sles
Case
s
Years

24
occurrences of measles because no consistency was observed between relative humidity and measles
except the incidence of Measles that comes during the month of the first increase in Relative
Humidity. This is similar to the result of (Moses et al. 2012)
Fig 4. Mean Monthly variation of Relative Humidity and measles cases in Akure
Variation between Minimum Temperature and Measles Occurrence
Fig 5 shows the monthly variation between minimum temperature and Measles. The peak of
minimum temperature occurred on March followed by February, measles occurrence followed the
same pattern, and this shows that high minimum temperature has a strong effect on the occurrences
of measles, this is similar to the findings of (Akinbobola 2006).
Fig 5. Mean Monthly variation of Min Temp and measles cases in Akure
0
5
10
15
20
68.070.072.074.076.078.080.082.0
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Mea
sles
cas
es
Rel
ativ
e H
um
idit
y (
%)
MonthsRelative Humidity measles
0
5
10
15
20
17.0
18.0
19.0
20.0
21.0
22.0
23.0
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Mea
sles
cas
es
Mim
imu
m T
emp
erat
ure
(ºC
)
MonthsTmin measles

25
Variation between Maximum Temperature and Measles Occurrence
Fig 6 shows the monthly variation between Maximum temperature and Measles. The peak of
Maximum temperature occurred on March followed by February, measles occurrence followed the
same pattern, and this shows that high Maximum temperature has a strong effect on the occurrences
of measles, this is similar to the findings of (Akinbobola 2006).
Fig 6. Mean Monthly variation of Max Temp and measles cases in Akure
Variation between Maximum Temperature and Measles Occurrence
Fig 7 shows the Monthly variation between Rainfall and Measles. It was observed that
Measles incidences were high during the months of March and April which matches with the months
with little rainfall, this revealed that there is a slight relationship between rainfall and Measles
Occurrence.
0
5
10
15
20
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Mea
sles
Max
imu
m T
emp
erat
ure
(ºC
)
MonthsTmax Measles

26
Fig 7. Mean Monthly variation of rainfall and measles cases in Akure
Variation between Solar Radiation and Measles Occurrence
Fig 8 shows the Monthly Variation of Solar Radiation and Measles Occurrence. It shows
Solar Radiation being at its peak in January and February which are associated with dry season.
Measles occurrence being at its peak in March which is the peak of dry season. This shows that there
is a strong relationship between Solar radiation and Measles Occurrence for the year 2009 to 2014.
Fig 8. Mean Monthly variation of Solar Radiation and measles cases in Akure
02468101214161820
0.0
50.0
100.0
150.0
200.0
250.0
Mea
sles
case
s
Ra
infa
ll (
mm
)
Monthsrainfall measles
0
2
4
6
810
12
14
16
18
20
0.00
2.00
4.00
6.00
8.0010.00
12.00
14.00
16.00
18.00
20.00
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Mea
sles
Sola
r R
adia
tio
n
(MJ/
m^2
/day
)
Monthssolar rad measles

27
4.3. Seasonal variation of meteorological parameters and measles Occurrence
The transition season, between Dry Season and Wet season, is the season with the highest
occurrence of measles with 41% of the total annual occurrence. Measles cases are more prevalent
during transition and dry season where Relative humidity and Rainfall are moderate but maximum
and minimum temperature and Solar Radiation are high
Table 1.Seasonal index for Measles occurrence
S/N SEASONS SEASONAL INDEX (%)
1 Dry Season 39
2 Transition 41
3 Wet Season 20
Table 2.Quarterly index for Measles occurrence
S/N QUARTERS QUARTERLY INDEX (%)
1 1st Quarter 33.3
2 2nd Quarter 30.3
3 3rd Quarter 12.1
4 4th Quarter 24.2

28
In table 1, the dry season has the highest occurrence of measles with the value of 39% followed by
the transition season with value 41% and wet season with value 20% meanwhile the quarterly index
in table 2 revealed that the 1st quarter has the highest occurrence of measles with value 33.3%
followed by the 2nd quarter, 30.3% then the 4th quarter, 24.2% and finally the 3rd quarter with value
12.1%.
Fig 10 shows seasonal variation of Relative Humidity and measles. As showed in the graph,
the peak of measles occurs during the transition season to wet season which signifies that little
amount of relative humidity is favourable for the production of measles infection
Fig 10.Seasonal Variation of Measles with RH cases in Akure
Fig 11 shows the seasonal variation of minimum temperature and measles. The transition
season is the season with peak mean seasonal minimum temperature which is the season with the
highest measles cases and dry season is the season with lowest mean seasonal minimum temperature
and wet season is the season with lowest cases of measles, this showed that high minimum
temperature is highly favourable for measles and affect the measles infection.
0.0
2.0
4.0
6.0
8.0
10.0
12.0
71.0
72.0
73.0
74.0
75.0
76.0
77.0
78.0
79.0
80.0
DRY SEASON TRANSITION WET SEASONM
easl
es
Rel
ativ
e H
um
idit
y (%
)
SeasonsRH MEASLES

29
Fig 11.Seasonal Variation of Measles with Tmin cases in Akure
Fig 12 shows the seasonal variation of maximum temperature and measles. This shows dry season
having the highest maximum temperature. Measles occurrence increases with the increase in the
maximum temperature and decreases with decrease in maximum temperature, which revealed that
maximum temperature has a direct and strong effect on measles case
Fig 12.Seasonal Variation of Measles with Tmax cases in Akure
0.0
2.0
4.0
6.0
8.0
10.0
12.0
20.4
20.6
20.8
21.0
21.2
21.4
21.6
21.8
22.0
22.2
22.4
DRY SEASON TRANSITION WET SEASON
Mea
sles
Min
imu
m T
emp
erat
ure
(̊c)
SeasonsTmin MEASLES
0.0
2.0
4.0
6.0
8.0
10.0
12.0
26.0
27.0
28.0
29.0
30.0
31.0
32.0
33.0
34.0
DRY SEASON TRANSITION WET SEASON
Mea
sles
Max
imum
Tem
per
ature
(̊c)
SeasonsTmax MEASLES

30
Fig 13 shows the seasonal variation of rainfall and measles. As showed in the graph that the
peak of measles occurs during the transition season while the lowest record of measles occurrence is
during the wet season which signifies that high rainfall is not favourable for the prevalence of
measles.
Fig 13 Seasonal Variation of Measles with Rainfall cases in Akure
Fig 14 shows the seasonal variation of measles and solar radiation. Measles occurrence has
its peak at the transition period and solar radiation is very high during that period too which signifies
that solar radiation is a major factor in measles occurrence.
0.0
2.0
4.0
6.0
8.0
10.0
12.0
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0
180.0
200.0
DRY SEASON TRANSITION WET SEASON
Mea
sles
Rai
nfa
ll (
mm
)
SeasonsRAINFALL MEASLES

31
Fig 14.Seasonal Variation of Measles with Solar Radiation cases in Akure
4.4. Statistical relationship between Measles and meteorological variables
Table 3 shows the correlation Rainfall (RR), Relative Humidity (RH), Minimum temperature
(Tmin), Maximum temperature (Tmax), and Solar radiation (SR) have with measles occurrence.
Maximum temperature, Minimum temperature and Solar radiation showed a significant relationship
with measles occurrence at 95% confidence level while Rainfall and Relative humidity have a
negative correlation which means a decrease in Rainfall and Relative humidity leads to an increase in
measles occurrence.
Mean Monthly Correlation between measles occurrence and meteorological variables
using Spearman’s Rank Correlation coefficient
Table 3.
S/N Meteorological Parameters R R2 P-value
1 Rainfall (RR) -0.37063 0.137366 0.235621
2 Maximum Temperature (Tmax) 0.587413 0.345054 0.044609
0.0
2.0
4.0
6.0
8.0
10.0
12.0
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
DRY SEASON TRANSITION WET SEASON
Mea
sles
So
lar
Rad
iati
on
(m
j/m
^2/d
ay
SeasonsSR MEASLES

32
3 Minimum Temperature (Tmin) 0.615385 0.378698 0.03317
4 Relative Humidity (RH) -0.60839 0.37014 0.035806
5 Solar Radiation (SR) 0.643357 0.413908 0.024003
4.5. Weather-Disease Statistical Model
Statistical models for estimating the occurrence of measles were developed using Poisson
Multiple Linear Regression in Generalized Linear Models, (GLMs) since it has been found out that
some of the meteorological parameters have high correlation with the diseases as it can be seen in
Table 3.
Two models were developed for the disease; Model 1 was developed using all the
meteorological parameters while model 2 was developed using only the meteorological parameters
that has positive correlation with measles occurrence. Five out of six years data were used to develop
the model while the 6th was used to validate the models. The Models are as follows:
Model 1:
Measles = 13.6474 - 1.105012765RH + 0.897680391Tmax + 3.391756234Tmin -0.016135948RR
- 1.279017197SR
Model 2:
Measles = 7.5416079 + 1.1085015Tmax + 3.0288238Tmin - 1.043331SR - 1.081946RH
In Model 1, Relative humidity, Maximum temperature, minimum temperature, rainfall and
solar radiation were used while in Model 2, Maximum temperature, Minimum temperature, Solar
radiation and Relative Humidity were used since they show strong effect on measles occurrence with

33
correlation of 0.587413, 0.615385, 0.643357 and -0.60839 respectively all at 95% confidence level.
The negative figure for Relative humidity shows that Relative humidity must be low for measles
occurrence.
Multiple linear Regression Models
The table below shows the Stepwise multiple linear Regression Models of the effect of weather
parameters on measles occurrence singularly and combined.
Table 4 multiple linear regression Model equations
S/N EQUATIONS
1. M1 = 27.49825 - 0.30217RH
2. M2 = -9.60097 + 0.460336MaxT
3. M3 = -35.5541 + 1.851642MinT
4. M4 = 5.517414 - 0.00645RR
5. M5 = -2.67716 + (0.508888SR)
6. M6 = - 100.1920035 + 2.168027582Tmax + 2.3827087244Tmin - 0.675342774SR
7. M7= 7.5416079 + 1.1085015Tmax + 3.0288238Tmin - 1.043331SR - 1.081946RH
8. M8 = 13.6474 - 1.105012765RH + 0.897680391Tmax + 3.391756234Tmin - 0.016135948RR
- 1.279017197SR
Models Validation
Validating Measles’s Model 1

34
Table 5.
MONTHS OBSERVED ESTIMATED RESIDUAL % DIFFERENCE
JANUARY 6 1 5 86
FEBRUARY 7 13 -6 -85
MARCH 4 21 -17 -422
APRIL 6 16 -10 -173
MAY 10 16 -6 -58
JUNE 8 14 -6 -78
JULY 0 11 -11 0
AUGUST 0 3 -3 0
SEPTEMBER 7 9 -2 -33
OCTOBER 4 14 -10 -258
NOVEMBER 5 10 -5 -106
DECEMBER 0 11 -11 0
Validating Measles’s Model 2
Table 6.
MONTHS OBSERVED PREDICTED RESIDUAL % DIFFERENCE
JANUARY 6 13 -7 -111
FEBRUARY 7 12 -5 -69
MARCH 4 20 -16 -398
APRIL 6 12 -6 -106
MAY 10 10 0 5

35
JUNE 8 10 -2 -29
JULY 0 6 -6 0
AUGUST 0 4 -4 0
SEPTEMBER 7 5 2 24
OCTOBER 4 9 -5 -125
NOVEMBER 5 8 -3 -63
DECEMBER 0 13 -13 0
4.6. Probability of occurrence of the diseases
Table 7 shows the probability of measles occurrence estimated using both models
Table 7. Probability of monthly occurrence of Measles
POISSON PROBABILITY ANALYSIS FOR MODEL 1 AND 2
MONTHS MODEL 1 MODEL 2
Jan 0.000175 0.018115673
Feb 0.029151 0.046928911
Mar 6.7E-06 1.47683E-05
Apr 0.002037 0.021389287
May 0.036813 0.123670819
Jun 0.027612 0.105373375
Jul 1.67E-05 0.001699051
Aug 0.031007 0.027549545
Sep 0.108873 0.11646686
Oct 0.001043 0.033850924
Nov 0.03267 0.086585709

36
Dec 2.16E-05 3.59639E-06
4.7. Models Performance
It’s found out that model 2 in the measles model performed better because meteorological
parameter with P-vales less than 0.05(at 95% confident level) were used and all of them has high
correlation. The models underestimated, this can lead to only two conclusions first the
meteorological parameters used in this study might not be the only environmental factors responsible
for the prevalence of these diseases. Secondly non climatic such as land cover, water bodies,
hygiene, population and public intervention factors are kept constant.
4.8. Error Analysis
The error analysis of the data was done to determine the reliability for the estimated values and
numerical values of the Poisson probability analysis in Table 7. The graphical representations of the
analysis are shown:
Fig 15. Observed and Predicted measles patients for Model 1
0
5
10
15
20
25
30
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
No
of
Pat
ien
ts
Months
Model 1
OBSERVED PREDICTED

37
Fig 16. Observed and Predicted measles patients for Model 2
4.9. Relative Risk of meteorological parameters with respect to measles.
S/N Weather Parameters Relative Risk
1 Relative Humidity (RH) 0.331207
2 Max Temp (Tmax) 2.453904
3 Min Temp (Tmin) 29.7181
4 Rainfall (RR) 0.983994
5 Solar Radiation (SR) 0.278311
The table above shows the relative risk of the weather parameters. It can be seen that 1oC
increase in minimum temperature is having more risk related to 1oC increase in maximum
temperature and 1% increase in rainfall. Also 1mm increase in rainfall is having more risk related to
1% increase in relative humidity all on measles occurrence.
0
5
10
15
20
25
30
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Model 2
OBSERVED PREDICTED

38
CHAPTER FIVE
CONCLUSION AND RECOMMENDATION
5.1. Conclusion
After analysing both the meteorological and medical data set collected, it was found out that
meteorological parameters has significant effects on the occurrence of measles occurrence in Akure,
Southwestern, Nigeria. Measles occurrence in Akure from 2009 to 2014 has been on the decrease.
From time series analysis of the data collected measles did not occur throughout the year but the
incidence is more prevalent during the transition season and least occurrence was seen during the wet
season when relative humidity and rainfall are low.
The result shows that there is significantly direct association between maximum and
minimum temperature and solar radiation and measles occurrence. Relative humidity had an indirect
relationship with measles occurrence due to its high negative correlation showing that a decrease in
relative humidity leads to high risk of measles occurrence. Rainfall had no direct relationship with
measles occurrence.
The seasonal variation of the meteorological parameters and the disease analysed showed
more evidences that meteorological parameters has influence on the prevalence of the diseases than
the monthly variation.
The model developed underestimated due to the fact that meteorological parameters are
possibly not the only environmental factors that influence measles occurrence. Other factors that
determine the occurrence are; lack of immunisation, improper sanitation, and wind propagation,
contact with patient. Minimum temperature, maximum temperature, solar radiation and relative
humidity are predictors of measles occurrence in the study area.
Thresholds has been identified for various meteorological parameters used in the study area
such as solar radiation and temperature. Based on the result there is a clear seasonality in pattern of
reported measles cases.

39
5.2. Recommendation
Having found out the peak period of the reported cases of the disease and the meteorological
conditions (weather and climate) favourable for disease, the government at different level, private
and non – governmental can create awareness and campaign about the onset of the disease and the
period of maximum occurrence of the disease.
This research work would also serve as tool for health personnel for planning on future
management of measles and it will aid pharmacies in the production of vaccines as a way of reducing
the effect and curing the virus. In lieu of this, our hospitals should adopt efficient ways of data
archival to improve and encourage researches in this line of study.
The model has to be improved in more advance manner to increase its accuracy, this can be done
using more year data set and more meteorological parameters.
More research work has to be done to cover a larger geographical location so that the model will
be effectively utilized.

40
References
A.G., O. (Weather variables and the occurrence of specific diseases of West African Dwarf (WAD) goats in
Ondo State). 2007. Nigeria : Proceedings of the International Conference on the Impacts of Extreme
Weather and Climate on Socio-Economic Development in Africa, Nigerian Meteorological Society,
Akure, 1–15 November, pp 34–38.
Adefolalu. (1997). Hydro-ecozone mapping of Ondo/Ekiti State,Nigeria. Ondo State. project Final report, pp.
141.
Adetunji O.O., O. E. (2007). Measles among hospitalized Nigerian children. Internet J Pediatr and Neonatol
7(1):1–11.
AG, O. (2007). Weather variables and the occurrence of specific. Proceedings of the International Conference
on the Impacts of Extreme Weather and Climate on Socio-Economic Development in Africa. Nigeria:
Nigerian Meteorological Society, Akure,.
Akinbobola A., O. J. (2010). Meteorological Factors and Measles Occurrence in Akure,Ondo State, Nigeria.
J.Meteorol. Rel. Sci., 4 35–47 (2010).
Akinyemi Gabriel Omonijo, A. M. (2011). Effect of thermal environment on the temporal,spatial and seasonal
occurrence of measles. Nigeria: Int J Biometeorol (2012) 56:873–885.
Bukhari, T. (2009). Temperature and Rainfall Variability and Outbreak of Meningitis and Measles in Zaria
L.G.A of Kaduna State, Nigeria. An Unpublished B.Sc Dissertation, Department of Geography,
Ahmadu Bello University, Zaria.
Chen, A. A. (2002). Investigating the link between early season caribean rainfall and the EL Nino + 1 year.
International Journal of Climatology, 22, PP 87 – 106.
Coleman, T. (2010). Forecasting Illness: The Weather-Health Connectionth. http://www.al-hikmah.org/fore-
casting illness.htn.
Driscoll. (1971b). Relationship between Meteorological Variables and Mortality Rate. Chicago Manucipal
press plc.
Duke. (2003). Environmental Health Principles. Fatcher pub.
Egunjobi. (1993). Spatial distribution of mortality from leading notifiable diseases in Nigeria. Soc Sci Med
36(10):1267–1272.
Ericsson, C. (2010). How Does Our Cold Weather Affect Our Health. Retrieved 27th March, 2009 from
http://www.usatoday.com/weather/health/whealth.htm.
Furuse Y, S. A. (2010). Origin of measles virus:divergence from rinderpest virus between the 11th and 12th
centuries. Virol J 7:52.
Gagge, A. (1979). The Role of Humidity during Warm Discomfort in Indoor Climate: Effects on Human
Comfort, Performance and Health in Residential, Commercial and Light Industry Building. Edited by
Fanger P.O and.
GHC. (2009). Causes of child death. Washington DC: Global Health Council.

41
Healthscout. (2010). Measles-Synptoms, Treatment and Prevention.
http://www.Hea;thscout.com/ency/68/732/main.
Hensel, H. (1979). Thermoreception and Human Comfort in INDOOR CLIMATE;Effect on Human
Comfort,Performance and Health in Residential,Commercial and Light-industry Building. Edited by
Fanger,P.O and Valbjorn,O.Gometed Press,London.
I.C., O. (2003). Incidence and modulating effects of environmental factors on trypanosomosis, peste des petit
ruminants (PPR) and bronchopneumonia of West African dwarf goats in Imo state, Nigeria. Livest Res
Rural Dev 15 (9) (Available at: http://www.lrrd.org/lrrd15/9/okoli159.htm).
Kenneth, L., Thomas, R., & Rebecca, J. a. (2008). Climate and vector- borne diseases. . American Journaj of
Preventive Medicine. Vol 35 (5), pp 436-450.
Lipp E.K., H. A. (2002). Effects of Global Climate on Infections Diseases: The Cholera Model “Clinical
Microbiology". Reviews, vol. 15, No. 4, October, pp. 757-770.
http://www.mbio,ncsu.edu/SL/MB590790/Cholare/cholera.pdf. downloaded June,2011.
McNeil. (1976). Plagues and peoples.
Patz, J. A. (1996). Global Climate Change and Emerging Infections Diseases. Journal of the medical
Association,” vol . 275, No.3, PP 217 -223.
Persinger, O. (1980). Lag responses in mood reports to change in the weather matrix. Inter. J . Biomet; 19,
108 -114.
Persinger.P. (1975). Our Environment and Our Health. Lisbon publishers.
Ray, V. (1970). Economic Activities in Zaria”in Journal of Zaria and its Region,Vol4. Department of Geography
Ahmadu Bello University, Zaria.
Sheshberadaran H, N. E. (1986). The antigenic relationship between measles, canine distemper and
rinderpest viruses studied with monoclonal antibodies. J Gen Virol 67:1381–1392.
Strebel P, S. C.-B. (2003). The unfinished measles immunization agenda. J Infect Dis 15(187):1–7.
T, B. (1999). Morbillivirus infections, with special emphasis on. Vet Microbiol 69:3–13.
W., T. (1963). The Burden of Climate on Man. Queen Lister Press.
WHO. (2003). Climate Change and Human Health-Risk and Response. France.
WHO. (2005). World Malaria Report.
WHO. (2007). AFRO Measles Surveillance . Feedback Bulletin June pp 1–7.
WHO. (2007). Climate Change and Human Health. http:/www.euro.who.int/mediacentre/PRI.
WHO. (2008). Measles Surveillance and Outbreak. WHO-African Region 17 April pp 1-4.
WHO. (2009). Measles Fact Sheet. Geneva Switzerland:
http://www.who.int/mediacentre/facrsheets/fs286/en.