
Statistical Issues in Incorporating and Testing Biomarkers in Phase III Clinical Trials FDA/Industry...
23
Statistical Issues in Incorporating and Testing Biomarkers in Phase III Clinical Trials FDA/Industry Workshop; September 29, 2006 Daniel Sargent, PhD Sumithra Mandrekar, PhD Division of Biostatistics, Mayo Clinic
-
Upload
brady-blea -
Category
Documents
-
view
213 -
download
0
Transcript of Statistical Issues in Incorporating and Testing Biomarkers in Phase III Clinical Trials FDA/Industry...
Statistical Issues in Incorporating and Testing
Biomarkers in Phase III Clinical Trials
Statistical Issues in Incorporating and Testing
Biomarkers in Phase III Clinical Trials
FDA/Industry Workshop; September 29, 2006
Daniel Sargent, PhD
Sumithra Mandrekar, PhD
Division of Biostatistics, Mayo Clinic
L Collette, EORTC
FDA/Industry Workshop; September 29, 2006
Daniel Sargent, PhD
Sumithra Mandrekar, PhD
Division of Biostatistics, Mayo Clinic
L Collette, EORTC
2
What are we testingWhat are we testing
• A (novel) therapeutic whose efficacy is predicted by a marker?
• A marker proposed to predict the efficacy of an (existing) therapeutic?
• A (novel) therapeutic whose efficacy is predicted by a marker?
• A marker proposed to predict the efficacy of an (existing) therapeutic?

3
Preliminary informationPreliminary information
Methods & feasibility ofmeasurement of the marker
in the target population
Specificity to the cancer of interestCut point for classification
Prevalence of marker expression in the target population
Properties as a prognostic marker(in absence of treatment or
With non targeted std agent)Expected marker predictive effect
Endpoint of interest

4
Phase II/III TrialsPhase II/III Trials
Patient Selection for targeted therapies
• Test the recommended dose on patients who are most likely to respond based on their molecular expression levels
• May result in a large savings of patients (Simon & Maitournam, CCR 2004)
Patient Selection for targeted therapies
• Test the recommended dose on patients who are most likely to respond based on their molecular expression levels
• May result in a large savings of patients (Simon & Maitournam, CCR 2004)

5
Trials in targeted populationsTrials in targeted populations
• Gains in efficiency depend on marker prevalence and relative efficacy in marker + and marker - patients
• Gains in efficiency depend on marker prevalence and relative efficacy in marker + and marker - patients
Prevalence Relative Efficacy
Efficiency Gain
25% 0% 16x
25% 50% 2.5x
50% 0% 4x
50% 50% 1.8x
75% 0% 1.8x
75% 50% 1.3x(Simon & Maitournam, CCR 2004)

6
Phase II/III TrialsPhase II/III Trials
Designs for Targeted Trials
May use standard approaches.
Possible Issues
• Could lead to negative trials when the agent could have possible “clinical benefit”, since precise mechanism of action is unknown
• Could miss efficacy in other patients
• Inability to test association of the biologic endpoints with clinical outcomes in a Phase II setting
Designs for Targeted Trials
May use standard approaches.
Possible Issues
• Could lead to negative trials when the agent could have possible “clinical benefit”, since precise mechanism of action is unknown
• Could miss efficacy in other patients
• Inability to test association of the biologic endpoints with clinical outcomes in a Phase II setting

7
Targeted TrialsTargeted Trials
Additional considerations
• Not always obvious as to who is likely to respond - often identified only after testing on all patients
• Slower accrual, and need to screen all patients anyway
• Need real time method for assessing patients who are / are not likely to respond
Additional considerations
• Not always obvious as to who is likely to respond - often identified only after testing on all patients
• Slower accrual, and need to screen all patients anyway
• Need real time method for assessing patients who are / are not likely to respond

8
Example: C-225 in colon cancerExample: C-225 in colon cancer
• Early trials mandated EGRF expression • (Saltz, JCO 2004, Cunningham, NEJM 2004)
• Response rate did not correlate with expression level (Cunningham, NEJM 2004)
• Faint: RR 21%• Weak or Moderate: RR 25%• Strong: RR 23%
• Case series demonstrates no correlation between expression and response
• (Chung, JCO 2005)
• Currently indicated only in patients with EGFR expressing tumors, but most current studies do not require EGFR expression
• Early trials mandated EGRF expression • (Saltz, JCO 2004, Cunningham, NEJM 2004)
• Response rate did not correlate with expression level (Cunningham, NEJM 2004)
• Faint: RR 21%• Weak or Moderate: RR 25%• Strong: RR 23%
• Case series demonstrates no correlation between expression and response
• (Chung, JCO 2005)
• Currently indicated only in patients with EGFR expressing tumors, but most current studies do not require EGFR expression

9
Design of Tumor Marker StudiesDesign of Tumor Marker Studies
• Current staging and risk-stratification methods incompletely predict prognosis or treatment efficacy
• New therapeutic options emerging
• Optimizing and individualizing therapy is becoming increasingly desirable
• Very few potential biological markers are developed to the point of allowing reliable use in clinical practice
• Current staging and risk-stratification methods incompletely predict prognosis or treatment efficacy
• New therapeutic options emerging
• Optimizing and individualizing therapy is becoming increasingly desirable
• Very few potential biological markers are developed to the point of allowing reliable use in clinical practice

10
Prognostic MarkerPrognostic Marker
Single trait or signature of traits that separates different populations with respect to the risk of an outcome of interest in absence of treatment or despite non targeted “standard” treatment
Single trait or signature of traits that separates different populations with respect to the risk of an outcome of interest in absence of treatment or despite non targeted “standard” treatment
PrognosticNo treatment or
Standard, non targeted treatment
Marker +
Marker –

11
Predictive MarkerPredictive Marker
Single trait or signature of traits that separates different populations with respect to the outcome of interest in response to a particular (targeted) treatment
Single trait or signature of traits that separates different populations with respect to the outcome of interest in response to a particular (targeted) treatment
PredictiveNo treatment
or Standard
Marker +
Marker –
Targeted
Treatment

12
Prognostic markerSeries of patients
with standard treatment
Predictive MarkersRandomized Clinical Trials
Validation
Designs?

13
Randomized TrialsRandomized Trials
• Trials to assess clinical usefulness of predictive markers – i.e., does use of the marker result in a clinical benefit of a therapy
• Upfront stratification for the marker status before randomization
• Randomize and use a marker-based strategy to compare outcome between marker-based arm with non-marker based arm
Sargent et al, JCO 2005
• Trials to assess clinical usefulness of predictive markers – i.e., does use of the marker result in a clinical benefit of a therapy
• Upfront stratification for the marker status before randomization
• Randomize and use a marker-based strategy to compare outcome between marker-based arm with non-marker based arm
Sargent et al, JCO 2005

14
Register Test Marker
Marker Level (-)
Randomize
Treatment A
Marker Level (+)
Treatment B
Sargent et al., JCO 2005
Design I: upfront StratificationDesign I: upfront Stratification
Randomize
Treatment A
Treatment B
Power trial separately withinmarker groups
15
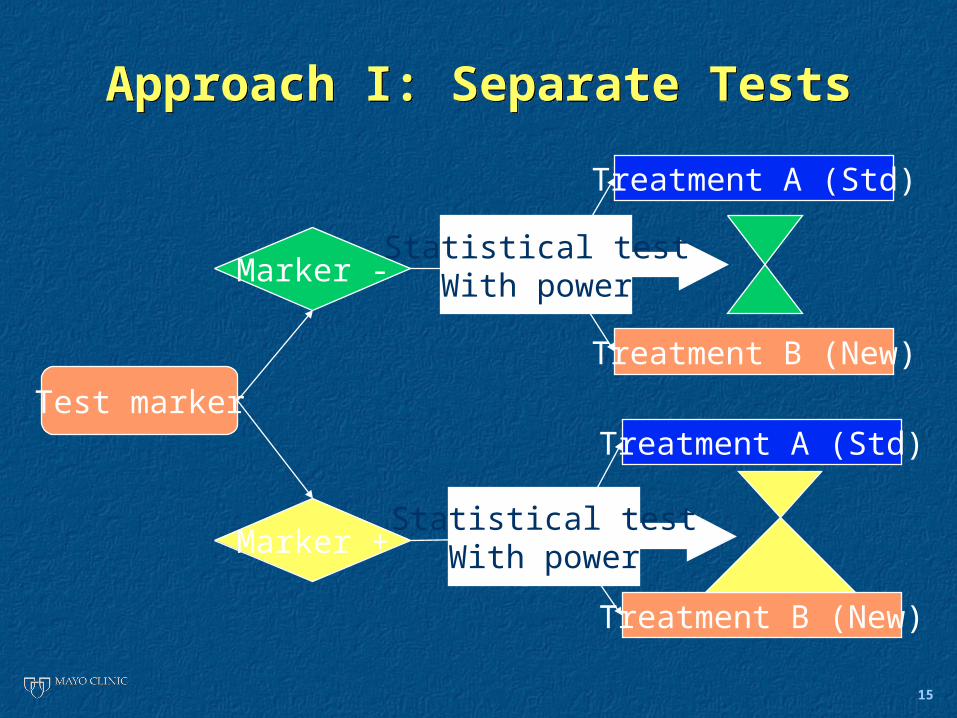
Approach I: Separate TestsApproach I: Separate Tests
Marker -
Marker +
R
R
Test marker
Treatment A (Std)
Treatment B (New)
Treatment A (Std)
Treatment B (New)
Statistical testWith power
Statistical testWith power
16
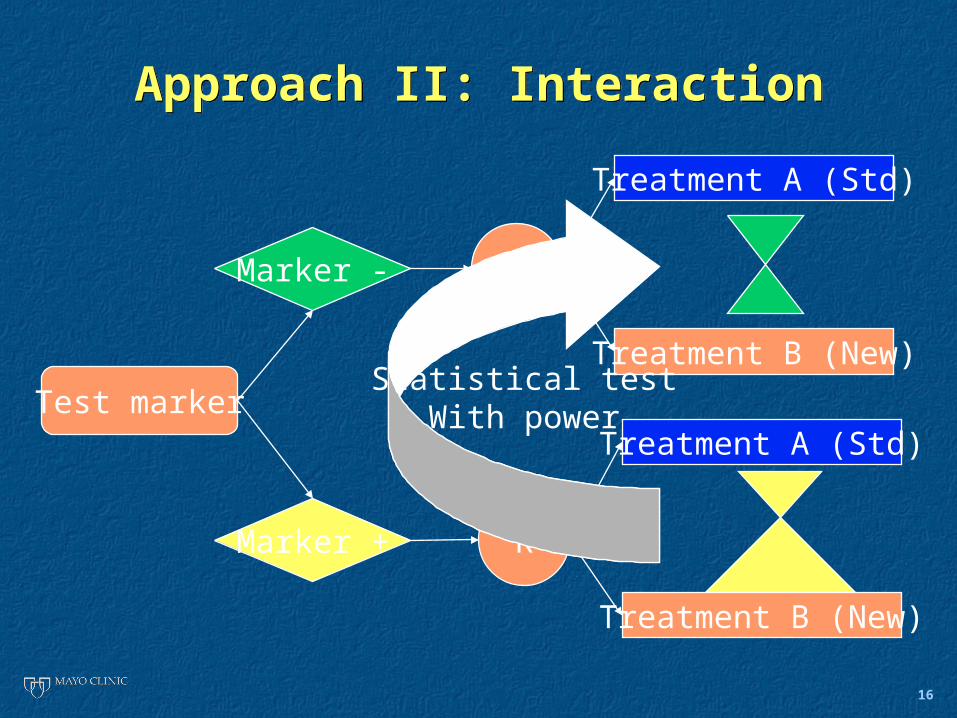
Approach II: InteractionApproach II: Interaction
Marker -
Marker +
R
R
Test marker
Treatment A (Std)
Treatment B (New)
Treatment A (Std)
Treatment B (New)
Statistical testWith power

17
Marker-based strategy designMarker-based strategy design
M -
M +
RTest
marker
Treatment A
Treatment B
Marker-Based
Strategy
Non MarkerBased
Strategy
Treatment A
StatisticalTest with
Power

18
Register
Marker Based Strategy
Non Marker Based Strategy
Randomize
Treatment A
Treatment B
Marker Level (-)
Treatment A
Marker Level (+) Treatment B
Test Marker
Sargent et al., JCO 2005
Design II: Marker Based StrategyDesign II: Marker Based Strategy
Randomize

19
Median OS Irinotecan/
Oxaliplatin (IO)
Irinotecan/5-FU/L
TS low
(50%) 16 months
20 months
TS high
(50%) 14 months 12 months
HR: 1.25
Sample Size Interaction DesignSample Size Interaction Design
HR: 0.86
844 †
1705 †
2223†2756†
HR: 0.691220 †
20
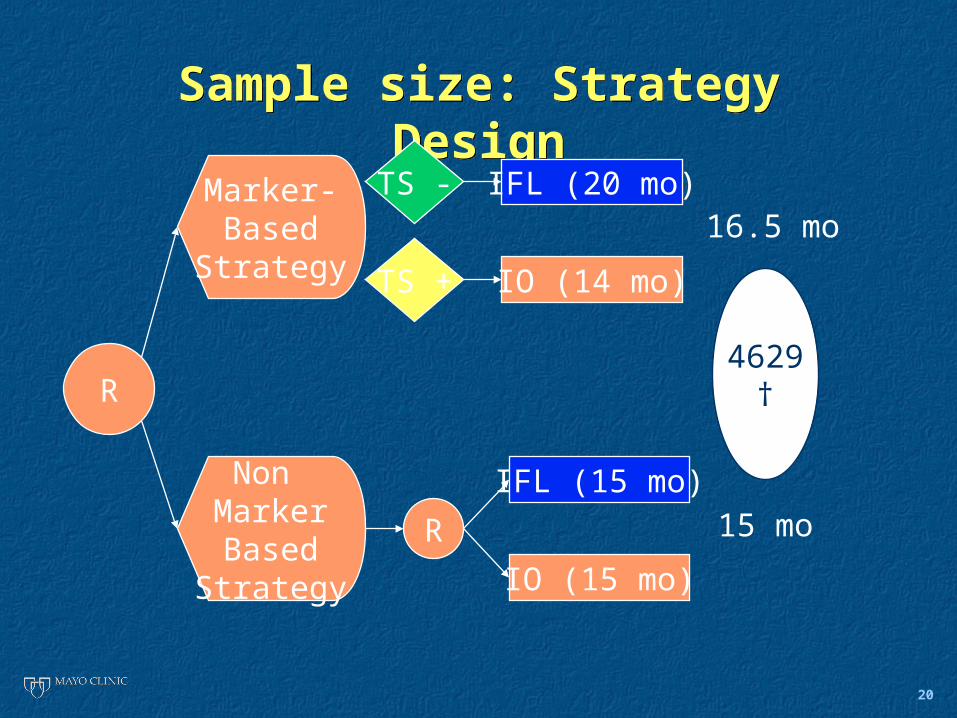
Sample size: Strategy DesignSample size: Strategy Design
TS -
TS +
IFL (20 mo)
IO (14 mo)
Marker-Based
Strategy
Non MarkerBased
Strategy
IFL (15 mo)
IO (15 mo)
R 15 mo
16.5 mo
HR0.91R4629
†
21
DiscussionDiscussion
• Sample Size • Typically large, especially if the
marker effect size is modest• Depends on many factors such as
• The marker prevalence in the target population
• The baseline risk in the unselected population receiving standard treatment
• The expected treatment difference in all marker groups
• Sample Size • Typically large, especially if the
marker effect size is modest• Depends on many factors such as
• The marker prevalence in the target population
• The baseline risk in the unselected population receiving standard treatment
• The expected treatment difference in all marker groups

22
ConclusionsConclusions
• The Marker Based Strategy design is preferable whenever more than one treatment are involved or when the treatment choice is based on a panel of markers
• That design generally requires more patients than the Interaction design
• The marker is also prognostic • Dilution (marker + patients receive the targeted
therapy in the randomized non marker based group)
• The Marker Based Strategy design is preferable whenever more than one treatment are involved or when the treatment choice is based on a panel of markers
• That design generally requires more patients than the Interaction design
• The marker is also prognostic • Dilution (marker + patients receive the targeted
therapy in the randomized non marker based group)

23
ConclusionsConclusions
• In the case of a single marker and two treatments, Interaction Design preferable
• Separate Tests versus Interaction ?• Depends on strength of evidence needed for the
marker effect and sample size
• Whenever the interaction HR is larger than any of the treatment HRs (generally qualitative interaction) the interaction approach demands less patients
• A partial Separate Tests approach may be useful whenever no treatment difference is expected in one of the marker groups
• In the case of a single marker and two treatments, Interaction Design preferable
• Separate Tests versus Interaction ?• Depends on strength of evidence needed for the
marker effect and sample size
• Whenever the interaction HR is larger than any of the treatment HRs (generally qualitative interaction) the interaction approach demands less patients
• A partial Separate Tests approach may be useful whenever no treatment difference is expected in one of the marker groups


















