
StatementofIntendedUse/Disclaimers · StatementofIntendedUse/Disclaimers ......
90
Transcript of StatementofIntendedUse/Disclaimers · StatementofIntendedUse/Disclaimers ......



Statement of Intended Use/Disclaimers All informa,on, data, and material contained, presented, or provided in this program / presenta,on (“Informa,on”) is for general informa,on purposes only and solely the opinion of the authors and presenters. The Informa,on should not be construed or intended as providing personalized medical or legal advice. The Informa,on is not necessarily considered mainstream health care. It is leP to the discre,on and judgment and is the sole responsibility of the recipient of the Informa,on to determine if products, procedures, treatments, tests, and therapies described are appropriate for the client. Neither the speakers nor the sponsors of Func,onal Neurology Seminars can be held responsible for the Informa,on, opinions, or any inadvertent errors or omissions in the prepara,on or presenta,on of the Informa,on. The Informa,on should not be construed as a claim regarding any procedure, treatment, therapy, test, or product. It is the sole responsibility of the recipient of this Informa,on to comply with local, state, and federal laws regarding the use of such Informa,on, as it relates to the scope and type of user’s prac,ce. It is the concern of the Department of Health and Human Services that no homeopathic and/or nutri,onal supplement be used to replace established, conven,onal medical approaches, especially in cases of emergencies or serious or life-‐threatening diseases, or condi,ons. Func,onal Neurology Seminars shares in this concern, as replacing conven,onal treatment with homeopathic and/or nutri,onal supplements, especially in serious cases, may deprive the client of necessary treatment thereby causing harm and could also pose a major legal liability for the healthcare professional involved. The Informa,on has not been evaluated by the Food and Drug Administra,on. Any nutri,onal product or procedure reported in this presenta,on is not intended to diagnose, treat, cure, or prevent disease. Various forms of care described in the FNS seminar series should not be used to replace conven,onal neurological care or replace other forms of medically necessary care. Dr. Da,s Kharrazian has the following financial interests. He is a member of Apex Energe,cs, Inc.'s Scien,fic Advisory Board, is a paid consultant to Apex Energe,cs, and receives royal,es on the sale of DVDs and CDs. Dr. Kharrazian is also a member of the editorial board of the Journal of Func,onal Neurology, Rehabilita,on, and Ergonomics. He receives no financial compensa,on for his par,cipa,on on this board. Dr. Kharrazian serves on the Curriculum Advisory Commi\ee of the Ins,tute for Func,onal Medicine. He receives no financial compensa,on for his par,cipa,on on this commi\ee. Dr. Brock has the following financial interests. Dr. Brock is a paid employee of Cerebrum Health Centers and owner and operator or Drbrocklectures.com and does consul,ng work for various clinics. Dr. Brock is a paid instructor for the Academy of Osteopathic Science, unpaid vice president of the Interna,onal Associa,on of Func,onal Neurology and Rehabilita,on, unpaid member of the human council of human func,on and an unpaid board member of the American Associa,on of Integra,ve Medicine. Dr. Brock is a paid lecturer for Apex Energe,cs. Dr. Brock has been engaged as an industry expert by Moleculara Laboratories to assist in the development of educa,onal lectures and to educate healthcare prac,,oners in its technology and the applica,on of its tes,ng. As such, he receives commissions from Moleculara as permi\ed by and in compliance with federal and state laws, codes and regula,ons, including Stark and other an,-‐kickback provisions. He is not an employee of Moleculara and does not own any stock. Dr. Kharrazian has been engaged as an industry expert by Cyrex Laboratories, LLC to assist in the development of clinical assays and to educate healthcare prac,,oners in its technology and the applica,on of its arrays. As such, he receives commissions from Cyrex as permi\ed by and in compliance with federal and state laws, codes and regula,ons, including Stark and other an,-‐kickback provisions. He is not an employee of Cyrex and does not own any stock. All marks and their use are thereby duly governed by the respec,ve owners and any and all rights in connec,on with those marks are en,rely reserved. The presenter receives a speaker’s fee and is reimbursed for his/her travel and related accommoda,ons by the sponsor, Apex Energe,cs, Inc. Dr. Kharrazian nor Dr. Brock have any financial interests in Laboratory Corpora,on of America, Quest Diagnos,cs, Incorporated, Diagnos-‐Techs, Inc., Principal Lab, Inc, Metametrix, Inc., Metabolic Solu,ons Development Company, LLC, Immunosciences Lab, Inc., RealTime Laboratories, Inc., Direct Laboratory Services, Inc., or Genova Diagnos,cs or other labs men,oned in this series other than those listed in this disclaimer.
3

Dr. Joel Brandon Brock MSN, BSN, RN, DC, NP-‐-‐C, DCM, DCN, DAAIM, BCIM, DCBCN, DACNB, FACNB, FICC
Dr. Brandon Brock is a Cer,fied Family Nurse Prac,,oner, Chiropractor and a func,onal neurology diplomate with mul,ple clinical interests, including Func,onal Integra,ve Neurology. In Dallas Texas he serves as a staff clinician at Cerebrum Health Centers and does work at Innova,ve Health and Wellness Group and Founda,on Physicians Group. Along with being a clinician, Dr. Brock has a passion for lecturing and providing learners with didac,c and academic skills in a way that is easy to digest, comprehend and u,lize in a clinical seeng. He has developed thousands of mul,disciplinary hours of curriculum that he or others have presented pertaining to neurology, nutri,on, physical diagnosis, pharmacology, immunology, endocrinology, and this has impacted students of mul,ple educa,onal and clinical backgrounds, including medical doctors, nurse prac,,oners and chiropractors. Offering educa,onal support for Physical and Occupa,onal Therapists, Die,,ans, Naturopaths, Acupuncturists, Oriental Medical Prac,,oners, Health Coaches and lay people that want to learn how to live a healthier life is also part of Dr. Brock's mission. He enjoys teaching for Apex Energe,cs as well as providing educa,on and support to facilitate learning for mul,ple groups and agencies. This includes state associa,on mee,ngs to governmental panels. Dr. Brock is also enjoying the process of developing in part his own func,onal neurology program (Func,onal Neurology Seminars), and short educa,onal lectures that many healthcare and medical providers can learn from over a variety of topics. Dr. Brock is currently a clinical lecturer of Pharmacology at the Ins,tute of Healthcare Professions, clinical neurology lecturer at the Academy of Osteopathic Science and vice president of the Interna,onal Associa,on of Func,onal Neurology and Rehabilita,on (IAFNR) and a board member of the American Academy of Integra,ve Medicine (AAIM). He was recently chosen as a member for the Council of Human Func,on and has been an expert on TAP Integra,ve. Dr. Brock received the most outstanding func,onal neurology teacher of the year from the ACA council of Neurology four years straight and two ,mes from IAFNR (Interna,onal Associa,on of Func,onal Neurology and Rehabilita,on). This year Dr. Brock received the humanitarian award as a result of his research on injured Military Veterans and PTSD and trauma,c brain injury from IAFNR. Dr. Brock is also the honorable recipient of the pres,gious Living Legacy Award from Samford Universi,es Ida Moffe\ School Nursing in 2015 and he was recently named the spotlight student of his doctoral program at Duke University. He holds diplomate status in Neurology, Conven,onal Medicine, Nutri,on, Integra,ve Medicine and a fellowship from the Interna,onal College of Chiropractors as well as the American Chiroprac,c Neurology Board. Currently Dr. Brock is working on a Doctorate of Nursing Prac,ce from Duke University and he is planning on immediately upon comple,on of the program at Duke, star,ng a conjoined PhD program with a major in nursing and a minor in behavioral neuroscience. Dr. Brock’s unique blend of clinical and teaching experience along with a background in medicine, chiroprac,c, neurology and nutri,on has created a very unique clinical background that has helped him treat difficult cases and offers comprehensive and mul,-‐-‐-‐perspec,ve angles on educa,on and clinical presenta,ons. Ul,mately you can typically find him spending ,me with his new wife Tara or his children, Addy, Zoey, Kennedy and Conner. They all love to travel, read, learn and live life. Dr. Brock's wife is a fantas,c English teacher at Sunnyvale High School and Dr. Brock points out that his wife Tara is the best and most grounded thing in his life, along with his kids, co-‐workers and friends.
4

Dr. Da%s Kharrazian DC, DHSc, DACNB, DABCN, FACN, CNS
Dr. Da,s Kharrazian is an Associate Clinical Professor at Loma Linda University School of Medicine. He has contributed significantly to the field of func,onal neurology as an educator, author, and researcher. He is credited with integra,ng the func,onal medicine model with rehabilita,ve neurology to evolve the specialty into a more comprehensive treatment model of brain dysfunc,on. He developed several post-‐graduate programs, protocols, examina,on forms, and ques,onnaire forms in the field of func,onal neurology that are being been used by thousands of health care professionals. His peers at the first Interna,onal Associa,on of Func,onal Neurology and Rehabilita,on (IAFNR) annual mee,ng recognized him with the “Clinical Trailblazer” Award for his contribu,on to evolving the field of func,onal neurology. He has also received numerous accolades for his development of func,onal medicine programs. He is the author of the best-‐selling book, Why Isn’t my Brain Working? This book has received hundreds of posi,ve tes,monials and five star reviews from readers throughout the world and is being translated into several other languages. Many reviewers have called his book the most complete and innova,ve compila,on of work for func,onal neurology nutri,onal concepts. Dr. Kharrazian teaches neuroscience and human brain dissec,on at Bastyr University California and is an Adjunct Professor at Na,onal University of Health Sciences, where he is developing post-‐graduate programs in func,onal neurology. He has developed a 30-‐part Neuroendocrine-‐Immune Series and a Mastering Brain Chemistry course that has been taught to thousands of health care professionals throughout the country and approved by the University of Bridgeport Postgraduate Department. Dr. Kharrazian is also a faculty member of the Ins,tute for Func,onal Medicine (IFM) and supports program development in func,onal medicine, func,onal neurology, neurological physical examina,on, and neurology diagnos,c applica,ons to brain-‐based disorders. The IFM provides medical physicians with con,nuing medical educa,on credits required for physician re-‐licensure and is accredited by the Accredita,on Council for Con,nuing Medical Educa,on. Dr. Kharrazian is a Fellow of the American College of Nutri,on, a Diplomate of the Board of Nutri,on Specialists, A Diplomate of the American Chiroprac,c Neurology Board, and a Diplomate of the American Clinical Board of Nutri,on. He earned a Master of Science degree in Human Nutri,on from the University of Bridgeport, a Doctor of Health Science from Nova Southeastern University, and a Doctor of Chiroprac,c degree from Southern California University of Health Sciences. He is currently comple,ng his Ph.D. degree at Nova Southeastern University with doctoral research in autoimmunity and immunology. Dr. Kharrazian completed a one-‐year post-‐doctorate clinical scholar research program at Harvard Medical School and is an associate alumni member of Harvard University and Harvard Medical School. He has published several scien,fic papers in the fields of nutri,on, autoimmunity, toxicology, and is conduc,ng research in autoimmune molecular mimicry and environmentally induced immune reac,vity. He is on the scien,fic editorial board for the Journal of Func,onal Neurology, Rehabilita,on and Ergonomics and Alterna,ve Medicine Therapies in Health and Medicine. He is also is a requested scien,fic reviewer for several scien,fic journals, including the Bri,sh Journal of Medicine and Medical Research. In addi,on to his contribu,on to func,onal neurology, Dr. Kharrazian has wri\en numerous papers, manuals, and clinical educa,onal material for blood chemistry analysis, hormone and endocrine analysis, complex immunology tes,ng, gastrointes,nal analysis, and func,onal medicine. He has trained more than 20 doctors to teach his model of func,onal medicine throughout the country. Dr. Kharrazian’s approach and clinical model are taught at more than 200 loca,ons each year. Dr. Kharrazian is also the author of the best-‐selling book, Why Do I S,ll Have Thyroid Symptoms When My Lab Tests are Normal? This book led readers to develop of the largest Hashimoto’s community (Hashimoto’s 411) on Facebook, and the development of a non-‐profit pa,ent advocacy group (Hashimoto’s Awareness) to support thyroid pa,ents from around the world. Dr. Kharrazian serves on the Nutri,on Leaders Council. This is an en,ty that directly contributes to the Accredita,on Council for Nutri,on Professional Educa,on, ACNPE (university nutri,on program accredita,on), Board for Nutri,on Specialists, BCNS, (creden,aling Body and Advocacy), and the American Nutri,on Associa,on, ANA (educa,onal and advocacy organiza,on). Dr. Kharrazian is a consultant to the nutri,on industry and has formulated more than 100 products, which are used by health care professionals. He also serves as a consultant to Cyrex Laboratory, where he provides expert clinical opinion on the development of complex immunology profiles. Dr. Kharrazian has a private prac,ce for pa,ents from around the world seeking non-‐pharmaceu,cal alterna,ves to manage chronic condi,ons. He uses diet, nutri,on, neurological rehabilita,ve exercises, and lifestyle applica,ons in his protocols. His prac,ce has a two-‐year wai,ng list and is limited to pa,ents suffering from chronic condi,ons. Most of Dr. Kharrazian’s pa,ents are referred from other health care professionals both na,onally and interna,onally. As an educator, researcher, and clinician, Dr. Kharrazian has blended his scien,fic research with clinical experience to develop effec,ve concepts and applica,ons for complex health disorders, which have been used by thousands of health care professionals and pa,ents around the world.
5

Func,onal Neurology Seminars LP © 2016
















World Parkinson Congress
WATCH VIDEO PRESENTATION IN LIVESTREAM OR REPLAYS

Parkinsonian Gait Examples
WATCH VIDEO PRESENTATION IN LIVESTREAM OR REPLAYS


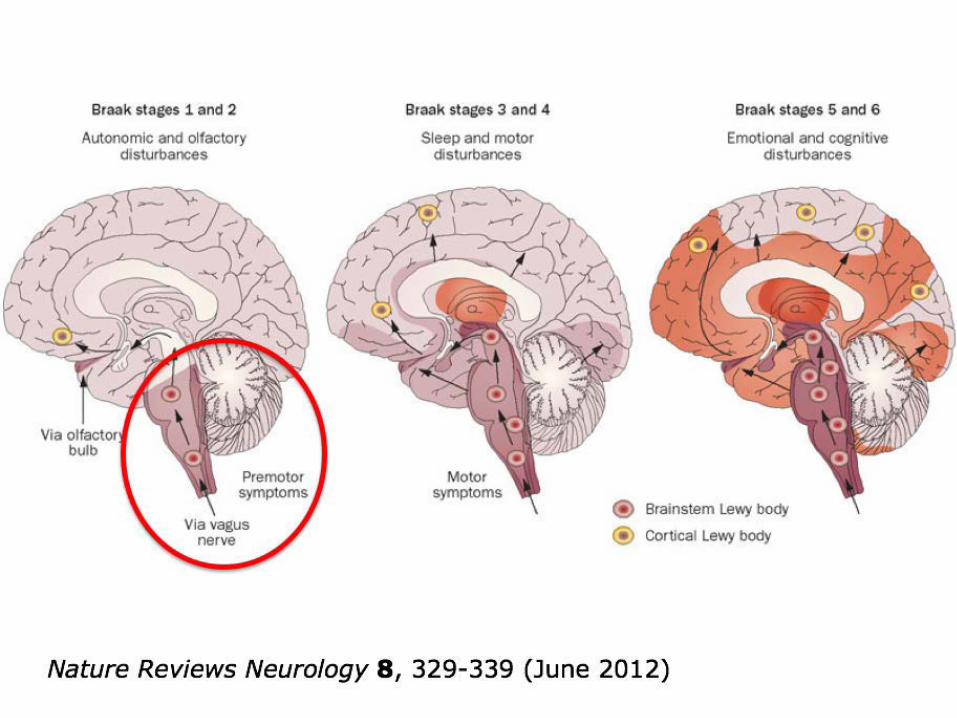
Nature Reviews Neurology 8, 329-339 (June 2012)





BRAINA JOURNAL OF NEUROLOGY
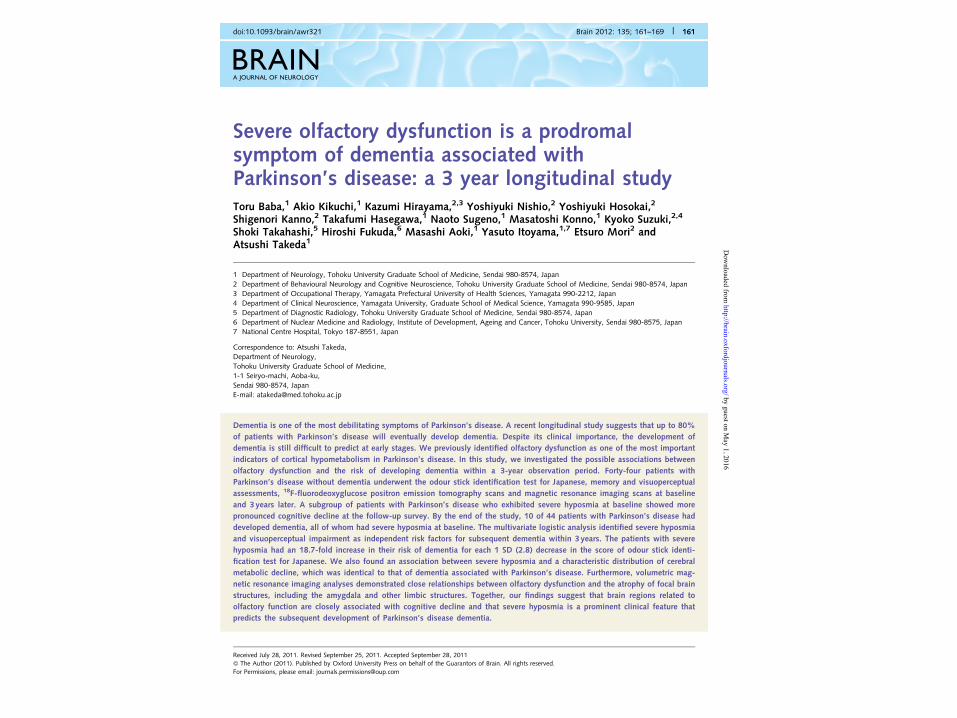
Severe olfactory dysfunction is a prodromalsymptom of dementia associated withParkinson’s disease: a 3 year longitudinal studyToru Baba,1 Akio Kikuchi,1 Kazumi Hirayama,2,3 Yoshiyuki Nishio,2 Yoshiyuki Hosokai,2
Shigenori Kanno,2 Takafumi Hasegawa,1 Naoto Sugeno,1 Masatoshi Konno,1 Kyoko Suzuki,2,4
Shoki Takahashi,5 Hiroshi Fukuda,6 Masashi Aoki,1 Yasuto Itoyama,1,7 Etsuro Mori2 andAtsushi Takeda1
1 Department of Neurology, Tohoku University Graduate School of Medicine, Sendai 980-8574, Japan2 Department of Behavioural Neurology and Cognitive Neuroscience, Tohoku University Graduate School of Medicine, Sendai 980-8574, Japan3 Department of Occupational Therapy, Yamagata Prefectural University of Health Sciences, Yamagata 990-2212, Japan4 Department of Clinical Neuroscience, Yamagata University, Graduate School of Medical Science, Yamagata 990-9585, Japan5 Department of Diagnostic Radiology, Tohoku University Graduate School of Medicine, Sendai 980-8574, Japan6 Department of Nuclear Medicine and Radiology, Institute of Development, Ageing and Cancer, Tohoku University, Sendai 980-8575, Japan7 National Centre Hospital, Tokyo 187-8551, Japan
Correspondence to: Atsushi Takeda,Department of Neurology,Tohoku University Graduate School of Medicine,1-1 Seiryo-machi, Aoba-ku,Sendai 980-8574, JapanE-mail: [email protected]
Dementia is one of the most debilitating symptoms of Parkinson’s disease. A recent longitudinal study suggests that up to 80%
of patients with Parkinson’s disease will eventually develop dementia. Despite its clinical importance, the development of
dementia is still difficult to predict at early stages. We previously identified olfactory dysfunction as one of the most important
indicators of cortical hypometabolism in Parkinson’s disease. In this study, we investigated the possible associations between
olfactory dysfunction and the risk of developing dementia within a 3-year observation period. Forty-four patients with
Parkinson’s disease without dementia underwent the odour stick identification test for Japanese, memory and visuoperceptual
assessments, 18F-fluorodeoxyglucose positron emission tomography scans and magnetic resonance imaging scans at baseline
and 3 years later. A subgroup of patients with Parkinson’s disease who exhibited severe hyposmia at baseline showed more
pronounced cognitive decline at the follow-up survey. By the end of the study, 10 of 44 patients with Parkinson’s disease had
developed dementia, all of whom had severe hyposmia at baseline. The multivariate logistic analysis identified severe hyposmia
and visuoperceptual impairment as independent risk factors for subsequent dementia within 3 years. The patients with severe
hyposmia had an 18.7-fold increase in their risk of dementia for each 1 SD (2.8) decrease in the score of odour stick identi-
fication test for Japanese. We also found an association between severe hyposmia and a characteristic distribution of cerebral
metabolic decline, which was identical to that of dementia associated with Parkinson’s disease. Furthermore, volumetric mag-
netic resonance imaging analyses demonstrated close relationships between olfactory dysfunction and the atrophy of focal brain
structures, including the amygdala and other limbic structures. Together, our findings suggest that brain regions related to
olfactory function are closely associated with cognitive decline and that severe hyposmia is a prominent clinical feature that
predicts the subsequent development of Parkinson’s disease dementia.
doi:10.1093/brain/awr321 Brain 2012: 135; 161–169 | 161
Received July 28, 2011. Revised September 25, 2011. Accepted September 28, 2011! The Author (2011). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved.For Permissions, please email: [email protected]
by guest on May 1, 2016
http://brain.oxfordjournals.org/D
ownloaded from




BRAINA JOURNAL OF NEUROLOGY
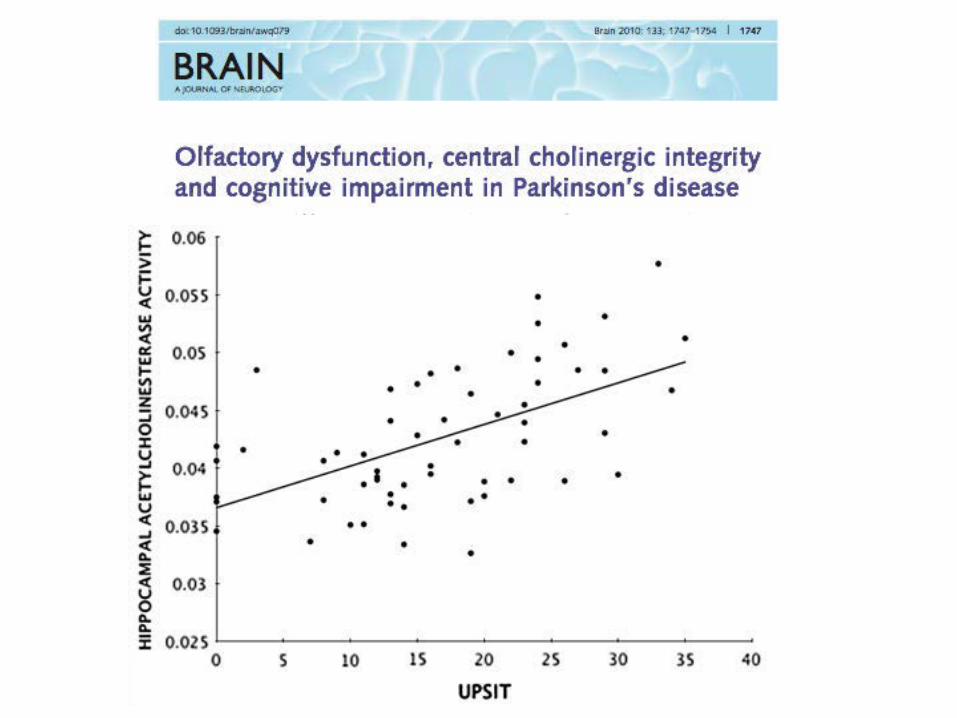
Olfactory dysfunction, central cholinergic integrityand cognitive impairment in Parkinson’s diseaseNicolaas I. Bohnen,1,2,3 Martijn L. T. M. Muller,1 Vikas Kotagal,2 Robert A. Koeppe,1
Michael A. Kilbourn,1 Roger L. Albin2,3 and Kirk A. Frey1,2
1 Department of Radiology, Division of Nuclear Medicine, University of Michigan, Ann Arbor, MI 48109, USA2 Department of Neurology, University of Michigan, Ann Arbor, MI 48109, USA3 Neurology Service and GRECC, VAAAHS, Ann Arbor, MI 48105, USA
Correspondence to: Nicolaas I. Bohnen,Functional Neuroimaging, Cognitive and Mobility Laboratory,Departments of Radiology and Neurology,University of Michigan, 24 Frank Lloyd Wright Drive,Box 362, Ann Arbor, MI, USAE-mail: [email protected]
Olfactory dysfunction is common in subjects with Parkinson’s disease. The pathophysiology of such dysfunction, however,
remains poorly understood. Neurodegeneration within central regions involved in odour perception may contribute to olfactory
dysfunction in Parkinson’s disease. Central cholinergic deficits occur in Parkinson’s disease and cholinergic neurons innervate
regions, such as the limbic archicortex, involved in odour perception. We investigated the relationship between performance on
an odour identification task and forebrain cholinergic denervation in Parkinson’s disease subjects without dementia. Fifty-eight
patients with Parkinson’s disease (mean Hoehn and Yahr stage 2.5! 0.5) without dementia (mean Mini-Mental State
Examination, 29.0! 1.4) underwent a clinical assessment, [11C]methyl-4-piperidinyl propionate acetylcholinesterase brain posi-
tron emission tomography and olfactory testing with the University of Pennsylvania Smell Identification Test. The diagnosis of
Parkinson’s disease was confirmed by [11C]dihydrotetrabenazine vesicular monoamine transporter type 2 positron emission
tomography. We found that odour identification test scores correlated positively with acetylcholinesterase activity in the
hippocampal formation (r = 0.56, P50.0001), amygdala (r = 0.50, P50.0001) and neocortex (r = 0.46, P = 0.0003). Striatal mono-
aminergic activity correlated positively with odour identification scores (r = 0.30, P50.05). Multiple regression analysis includ-
ing limbic (hippocampal and amygdala) and neocortical acetylcholinesterase activity as well as striatal monoaminergic activity,
using odour identification scores as the dependent variable, demonstrated a significant regressor effect for limbic acetylcholin-
esterase activity (F = 10.1, P50.0001), borderline for striatal monoaminergic activity (F = 1.6, P = 0.13), but not significant for
cortical acetylcholinesterase activity (F = 0.3, P = 0.75). Odour identification scores correlated positively with scores on cognitive
measures of episodic verbal learning (r = 0.30, P50.05). These findings indicate that cholinergic denervation of the limbic
archicortex is a more robust determinant of hyposmia than nigrostriatal dopaminergic denervation in subjects with moderately
severe Parkinson’s disease. Greater deficits in odour identification may identify patients with Parkinson’s disease at risk for
clinically significant cognitive impairment.
Keywords: acetylcholinesterase; cognitive impairment; Parkinson’s disease; positron emission tomography; smell
Abbreviations: AChE = acetylcholinesterase; UPSIT = University of Pennsylvania Smell Identification Test; VMAT2 = vesicularmonoamine transporter type 2
doi:10.1093/brain/awq079 Brain 2010: 133; 1747–1754 | 1747
Received December 8, 2009. Revised March 3, 2010. Accepted March 5, 2010. Advance Access publication April 22, 2010! The Author(s) 2010. Published by Oxford University Press on behalf of Brain.This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/2.5),which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

The University of Pennsylvania Smell Identification Test (UPSIT)











Peanut Butter Test for Alzheimer’s
WATCH VIDEO PRESENTATION IN LIVESTREAM OR REPLAYS

Quick smell test to help Identify Alzheimer’s disease
• Star,ng with a li\le peanut bu\er at the bo\om of a ruler, measure the distance from the nostril where pa,ents were first able to detect the odor.
• Pa,ents who detected the odor at least 6 cm worse with the leP nostril than with the right were also diagnosed with Alzheimer’s.
• Pa,ents diagnosed with other types of demen,a and healthy older people did not show this leP-‐worse-‐than-‐right nostril difference.
• This reliable, noninvasive test may help detect Alzheimer’s early because evidence suggests the smell area of the brain, par,cularly on the leP side, is the first area affected








J Neurol Neurosurg Psychiatry. 2002 May;72(5):560-‐563. Gluten sensi%vity as a neurological illness.
MRI of a patient with gluten ataxia showing rapid onset of cerebellar atrophy over a period of 15 months before the diagnosis of gluten ataxia

Gluten ataxia
• “Gluten ataxia…should be considered in the differen,al diagnosis of all pa%ents with idiopathic sporadic ataxia.”
• “Early diagnosis and treatment with a gluten-‐free diet can improve ataxia and prevent its progression.”
Cerebellum. 2008;7(3):494-‐498.


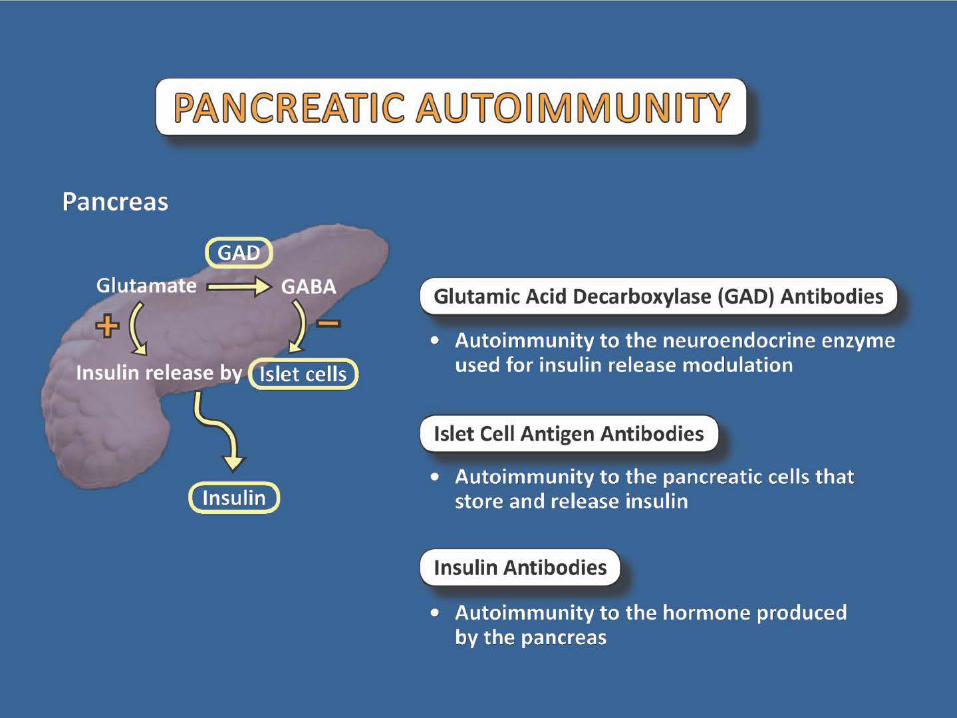
Autoantibodies to glutamic acid decarboxylase in three patients with cerebellarataxia,
late-onset insulin-dependent diabetes mellitus, and polyendocrine autoimmunity.
• “GAD-‐Abs should be sought in pa,ents with cerebellar ataxia who have late-‐onset IDDM and other organ-‐specific autoimmune manifesta,ons.”
Neurology. 1997 Oct;49(4):1026-‐30.

Anti-thyroperoxidase antibodies from patients with Hashimoto's encephalopathy bind to cerebellar astrocytes.
• “Normal human astrocytes from primary cultures also reacted with an,-‐TPO mAb.”
• “Specific astrocyte binding of an,-‐TPO aAb suggests a role of these aAb in the Hashimoto’s encephalopathy pathogenesis”
J Neuroimmunol. 2007 Dec;192(1-‐2):13-‐20.

Funct Neurol Rehabil Ergon 2014;4(2-3) ISSN: 2156-941X © 2014 Nova Science Publishers, Inc.
Neuroendocrine-Immunology Mechanisms of Subtle Cerebellum Impairment
Datis Kharrazian∗ Basytr University California, San Diego, CA
Abstract Cerebellum degeneration and impairment may occur from both clinically obvious and subtle mechanisms.
Obvious mechanisms of cerebellum disease include acute onset found with trauma and vascular lesions, compressive signs found with tumor, infectious mechanisms associated with fever and abnormal immune serology, and genetic patterns that have distinct identifying clinical features. Subtle neuroendocrine-immune mechanisms that can impair and degenerate the cerebellum include gluten specific cross-reactivity, Hashimoto’s encephalopathy, hypothyroidism, dysglycemia, subtle cerebellum autoimmunity, paraneoplastic cerebellum syndrome, or toxicological insults to cerebellum granulocytes and Purkinje cells. This paper reviews subtle neuroendocrine-immune mechanisms that insult the cerebellum.
Keywords: cerebellum, gluten specific cerebellar ataxia, and Hashimoto's encephalopathy,
Introduction Neurology professionals find various stages of cerebellum impairment in their practices. Early
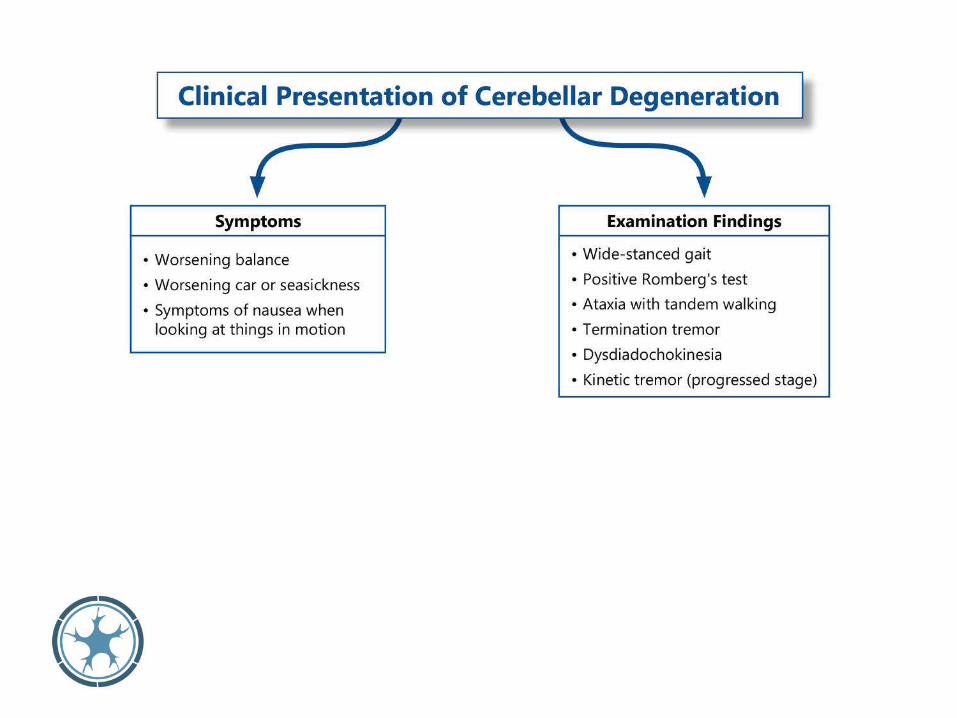
degenerative disease findings are identical to progressed findings and are differentiated by a graded scale of mild, moderate, and severe. Clinical findings of cerebellum disease include wide-stance and scissor gait, hypotonia, pendulum reflexes, ataxia, truncal titubation, poor posture, vertigo, dysdiadochokinesia, ocular and limb dysmetria, nystagmus, saccadic intrusion into smooth pursuit, hypometric and hypermetric saccades, abnormal optikinetic reflexes, inability to cancel the vestibule-ocular reflexes, square-wave jerks, scanning dysarthria and tremor of voice, kinetic and termination tremors, autonomic dystonia, and cognitive affective syndromes. [1]
Various neuroendocrine-immune mechanisms may promote degenerative changes in the cerebellum. They include metabolic, vascular, toxic, infectious, traumatic, carcinogenic, developmental, inflammatory, and genetic mechanisms. In addition to evaluating subjective and objective findings when looking at cerebellum impairment, it’s also important to identify various mechanisms of cerebellum disease. This paper focuses on identifying early mechanisms of cerebellum disease, excluding obvious mechanisms such as traumatic brain injury, tumors, stroke, infections, and genetic disorders. These more obvious mechanisms have clear clinical presentation either from their
∗ Correspondence: Dr. Datis Kharrazian, 1001 Canvasback Court, Carlsbad CA, 92011 Email: [email protected]





Clinical Pearl
• Remember, pa\erns of neurodevelopmental delays that may have been improved into adulthood are usually the first regions to show pa\erns of neurodegenera,on into late adulthood.


























![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://static.fdocuments.in/doc/165x107/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)


