Statement of seizures and Epilepsy: The Epilepsy Board ... e e d 2 Hospital physician Board Review...
43
EPILEPSY BOARD REVIEW MANUAL STATEMENT OF EDITORIAL PURPOSE The Epilepsy Board Review Manual is a study guide for trainees and practicing physicians preparing for board examinations in epilepsy. Each manual reviews a topic essential to the current management of patients with epilepsy. PUBLISHING STAFF PRESIDENT, GROUP PUBLISHER Bruce M. White SENIOR EDITOR Robert Litchkofski EXECUTIVE VICE PRESIDENT Barbara T. White EXECUTIVE DIRECTOR OF OPERATIONS Jean M. Gaul NOTE FROM THE PUBLISHER: This publication has been developed with- out involvement of or review by the Amer- ican Board of Psychiatry and Neurology. Seizures and Epilepsy: Electrophysiological Diagnosis Contributor and Editor: Thomas R. Henry, MD Professor of Neurology, Director, Comprehensive Epilepsy Center, University of Minnesota Medical School, Minneapolis, MN Contributor: Zhiyi Y. Sha, MD, PhD Assistant Professor of Neurology, Department of Neurology, University of Minnesota Medical School, Minneapolis, MN Introduction ............................. 1 Generation of the Human EEG .............. 1 Technology and Applications of the EEG ...... 6 Interictal Epileptiform Activities ............ 17 Ictal Epileptiform Activities and Video-EEG Monitoring ............................. 25 Benign EEG Variants and Artifacts That Can Simulate Interictal and Ictal Epileptiform Activities ............................... 31 Special Applications of EEG in Epilepsy ...... 32 Developing Applications of EEG in Epilepsy . . . 39 Board Review Questions ................... 40 References ............................. 40 Table of Contents
-
Upload
truongmien -
Category
Documents
-
view
213 -
download
0
Transcript of Statement of seizures and Epilepsy: The Epilepsy Board ... e e d 2 Hospital physician Board Review...
EpilEpsy Board rEviEw Manual
Statement of editorial PurPoSe
The Epilepsy Board Review Manual is a study guide for trainees and practicing physicians preparing for board examinations in epilepsy. Each manual reviews a topic essential to the current management of patients with epilepsy.
PuBliSHinG Staff
PRESIDENT, GRouP PuBLISHERBruce M. White
SENIoR EDIToRRobert Litchkofski
ExEcuTIvE vIcE PRESIDENTBarbara T. White
ExEcuTIvE DIREcToR of oPERaTIoNS
Jean M. Gaul
NoTE fRoM THE PuBLISHER:This publication has been developed without involvement of or review by the American Board of Psychiatry and Neurology.
seizures and Epilepsy: Electrophysiological Diagnosis
Contributor and Editor:Thomas R. Henry, MD Professor of Neurology, Director, Comprehensive Epilepsy Center, University of Minnesota Medical School, Minneapolis, MN
Contributor:Zhiyi y. sha, MD, phDAssistant Professor of Neurology, Department of Neurology, University of Minnesota Medical School, Minneapolis, MN
introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Generation of the Human EEG . . . . . . . . . . . . . .1
Technology and Applications of the EEG . . . . . .6
interictal Epileptiform Activities . . . . . . . . . . . .17 ictal Epileptiform Activities and Video-EEG
Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . .25 Benign EEG Variants and Artifacts That Can simulate interictal and ictal Epileptiform
Activities . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31
special Applications of EEG in Epilepsy . . . . . .32
Developing Applications of EEG in Epilepsy . . .39
Board Review Questions . . . . . . . . . . . . . . . . . . .40
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40
Table of Contents

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 1
EpilEpsy BoARD REViEw MAnuAl
seizures and Epilepsy: Electrophysiological DiagnosisZhiyi Y. Sha, MD, PhD, and Thomas R. Henry, MD
introduction
Electroencephalography (EEG) and video-EEG are powerful tools in the diagnosis of seizures and epilepsy. While EEG and derived techniques have considerable utility in nervous system conditions other than epilepsy, the most frequent and essen-tial indications for EEG are in seizures and epilep-sy. The fully educated adult or pediatric epileptolo-gist usually is also a fully trained EEG expert. This review presumes considerable background in both epileptology and clinical neurophysiology.
In the clinic or hospital, the cognitively flexible EEG-epilepsy expert will be able to move from a differential diagnosis of paroxysmal clinical events reported for a patient he or she has seen, to se-lection of an appropriate EEG procedure, then to interpretation of the interictal and ictal EEG, and on to application of the findings to diagnosis of that patient. In the clinical neurophysiology laboratory, the cognitively flexible EEG-epilepsy expert will be able to interpret an interictal or ictal EEG of a pa-tient she or he has never seen and generate a dif-ferential diagnosis of possible clinical correlates of
the spikes or other recorded abnormalities. Part 1 of this series reviewed the epilepsy syndromes, with summaries of typical EEG findings in particu-lar syndromes (“syndromes-to-electrophysiology” associations).1 The core of this article reviews par-ticular interictal and ictal EEG findings, with illustra-tion of typical examples, discussion of diagnostic difficulties, and review of clinical associations (“electrophysiology-to-syndromes” associations). Generation of the human EEG is discussed with emphasis on the clinical utility and limitations of extracranial and intracranial EEG recordings. We note limitations posed by artifacts and complexities posed by nonpathological sharply contoured or rhythmic EEG potentials. We also discuss special-ized EEG techniques used in presurgical epilepsy evaluations. This summary can be supplemented with review of the cited original papers and stan-dard textbooks2,3 and EEG atlases.4–6
Generation of tHe Human eeG
The scalp EEG is a severely limited sampling of brain electrical activities. Nonetheless, scalp
copyright 2012, Turner White communications, Inc., Strafford avenue, Suite 220, Wayne, Pa 19087-3391, www.turner-white.com. all rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, mechanical, electronic, photocopying, recording, or otherwise, without the prior written permission of Turner White communications. The preparation and distribution of this publication are supported by sponsorship subject to written agreements that stipu-late and ensure the editorial independence of Turner White communications. Turner White communications retains full control over the design and production of all published materials, including selection of topics and preparation of editorial content. The authors are solely responsible for substantive content. Statements expressed reflect the views of the authors and not necessarily the opinions or policies of Turner White communications. Turner White communications accepts no responsibility for statements made by authors and will not be liable for any errors of omission or inaccuracies. Information contained within this publication should not be used as a substitute for clinical judgment.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
2 Hospital physician Board Review Manual www.turner-white.com
EEG recordings are highly informative with re-gard to state of arousal and often to interictal and ictal abnormalities of diagnostic significance in the epilepsies. In general, brain electrical activities are generated by ionic currents in neurons and glia, which are regulated by neurotransmission and other biochemical processes. Cortical neurons generate electrical currents due to action potentials, excit-atory and inhibitory postsynaptic potentials (EPSPs and IPSPs), and “intrinsic” membrane currents arising from voltage-dependent ion channels. Only the EPSPs and IPSPs in radially oriented apical dendrites of neocortical pyramidal neurons con-
tribute significantly to generation of the scalp EEG, however.7 The location and orientation of synchro-nized dipolar cortical postsynaptic potentials (PSPs) are critical to detection by scalp EEG electrodes (Figure 1, Figure 2, and Figure 3). Figures 1, 2, and 3 illustrate some of the geometric effects of cortical anatomy that permit or prevent scalp EEG recording of potentials synchronized over surfaces larger than 6 cm2. A highly focal field synchronized atop one gyral crest may be “blurred” into a larger scalp EEG distribution, in part because the scalp electrodes located away from the center of the gyral crest can detect its charge and also because intervening soft and boney tissues may conduct currents laterally. The limited spatial sampling of scalp electrodes and the low- and high-frequency filtering of the EEG machine also account, in part, for the exclusion of glial electrical potentials and neuronal action poten-
Figure 1. Two-dimensional schema of surface-negative event at gyral crest. Gloor’s schema shows that scalp potential P1 directly overlies a gyral crest that has overall major negativity, such that the solid angle (Ω1–) supports recording of a strongly negative electrical potential at this site. A scalp electrode site lateral to this area also records a strongly negative electrical potential (Ω2–), but its solid angles of sampling also “see” posi-tive ends of dipoles at the undersurface of the cortical ribbon (Ω2+). Overall, P1 is much more negative than P2, which will be quite well recorded at a channel comparing electrodes 1 and 2. (Adapted with permission from Gloor P. Contributions of elec-troencephalography and electrocorticography to the neurosur-gical treatment of the epilepsies. Adv Neurol 1975;8:59–105.)
Figure 2. Two-dimensional schema of surface-negative event over a sulcus. Gloor’s schema shows that scalp potential P1 is negative but of lower voltage due to narrowing of the solid angle of negativity (compared with P1 in Figure 1), while P2 is almost isoelectric due to equivalence of topside cortical ribbon nega-tivity and underside cortical ribbon positivity. A channel compar-ing electrodes 1 and 2 will record a small negative deflection. (Adapted with permission from Gloor P. Contributions of elec-troencephalography and electrocorticography to the neurosur-gical treatment of the epilepsies. Adv Neurol 1975;8:59–105.)
Ω2eff = Ω–2 – Ω+2
P1Ω–1 Ω+2
P2
Ω–2
Ω2eff = Ω–2 – Ω+2 ~ 0
P1 Ω–1Ω+2
P2
Ω–2
=

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 3
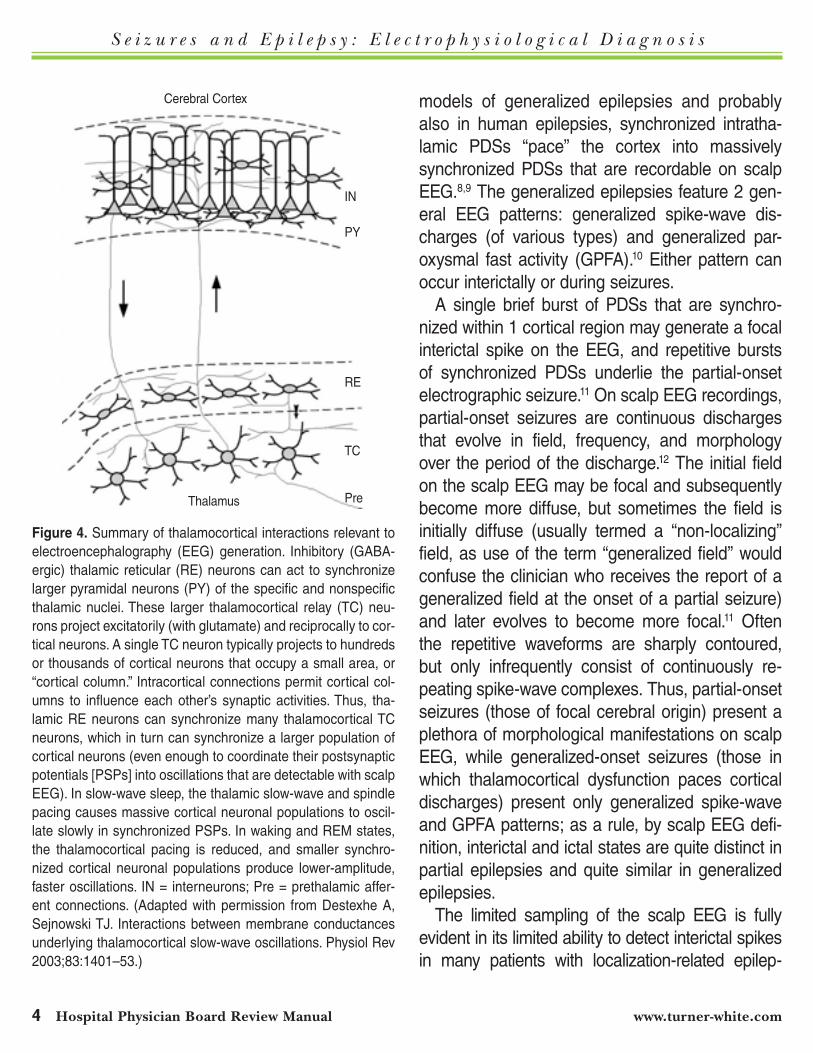
tials from the scalp EEG. The “volume conduction” effects in scalp EEG result in expansion of appar-ent electrical fields at the scalp, compared with the sites of the actual underlying electrical generators (Table 1). These electrical activities are influenced by neuronal activities originating in other neocortical areas, in limbic system structures, and especially in the thalamus (Figure 4). Thus, the scalp EEG is a limited sampling of synchronized electrical activities generated predominantly by neocortical pyramidal neurons of gyral crests, and these electrical activi-ties reflect local synaptic activities but also certain types of distant synaptic activities.
Normal EEG patterns represent synchronized oscillations of large groups of neurons; synchrony of these oscillations is more dependent on in-tracortical interactions during waking and more dependent on thalamocortical interactions during sleep.8 In general, pathologic EEG findings may reflect dysfunction originating in the neocortical neurons that generate the signal, or dysfunction originating in distant neurons and “projected” to the neocortical generators, or both.7 Small lesions that ablate cortex near the dorsolateral skull usu-ally cause reduced amplitude in overlying scalp EEG electrodes or produce no change in scalp EEG recordings. Many of the most prominent non-epileptiform EEG abnormalities, including focal or generalized persistent polymorphic delta activity, require lesions or dysfunctions that originate in subcortical white matter or subcortical gray mat-ter structures in order to produce alteration of the scalp EEG.
Epileptiform EEG abnormalities represent syn-chronized paroxysmal depolarization shifts (PDSs) in cortical neurons, a cellular phenomenon that was reviewed in part 1 of this series.1 Any PDSs that occur in the thalamus are not directly accessible to scalp EEG recording, of course. Considerable experimental evidence indicates that, in animal
Figure 3. Three-dimensional schema of electrical event over a gyral crest. Gloor’s schema shows that an electrically synchro-nized surface of a cortical gyrus presents its charge much more effectively to the overlying electrode 1 than to the laterally dis-placed electrode 2, both because the solid angle of electrode 1 (Ω1) is much larger than that of electrode 2 (Ω2) with respect to this surface, and also because electrode 1 is closer to that sur-face. In general, it appears that 6 cm2 of cortical surface must be synchronized in order to be recorded with extracranial elec-trodes. (Adapted with permission from Gloor P. Contributions of electroencephalography and electrocorticography to the neuro-surgical treatment of the epilepsies. Adv Neurol 1975;8:59–105.)
Table 1. Determinants of Amplitude, Duration, Morphology, and Topography of Extracranial EEG Oscillations
Duration of synchronous postsynaptic potentials Number of pyramidal cell apical dendrites with synchronous post-
synaptic potentials Anatomical location-orientation of cortical pyramidal cell layer Distances of electrodes from electrical generators*Conducting medium between generators and electrodes*Filtering and other properties of recording system
* “Volume conduction” effects
P1
Ω1
Ω2P2
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
4 Hospital physician Board Review Manual www.turner-white.com
models of generalized epilepsies and probably also in human epilepsies, synchronized intratha-lamic PDSs “pace” the cortex into massively synchronized PDSs that are recordable on scalp EEG.8,9 The generalized epilepsies feature 2 gen-eral EEG patterns: generalized spike-wave dis-charges (of various types) and generalized par-oxysmal fast activity (GPFA).10 Either pattern can occur interictally or during seizures.
A single brief burst of PDSs that are synchro-nized within 1 cortical region may generate a focal interictal spike on the EEG, and repetitive bursts of synchronized PDSs underlie the partial-onset electrographic seizure.11 On scalp EEG recordings, partial-onset seizures are continuous discharges that evolve in field, frequency, and morphology over the period of the discharge.12 The initial field on the scalp EEG may be focal and subsequently become more diffuse, but sometimes the field is initially diffuse (usually termed a “non-localizing” field, as use of the term “generalized field” would confuse the clinician who receives the report of a generalized field at the onset of a partial seizure) and later evolves to become more focal.11 Often the repetitive waveforms are sharply contoured, but only infrequently consist of continuously re-peating spike-wave complexes. Thus, partial-onset seizures (those of focal cerebral origin) present a plethora of morphological manifestations on scalp EEG, while generalized-onset seizures (those in which thalamocortical dysfunction paces cortical discharges) present only generalized spike-wave and GPFA patterns; as a rule, by scalp EEG defi-nition, interictal and ictal states are quite distinct in partial epilepsies and quite similar in generalized epilepsies.
The limited sampling of the scalp EEG is fully evident in its limited ability to detect interictal spikes in many patients with localization-related epilep-
Figure 4. Summary of thalamocortical interactions relevant to electroencephalography (EEG) generation. Inhibitory (GABA- ergic) thalamic reticular (RE) neurons can act to synchronize larger pyramidal neurons (PY) of the specific and nonspecific thalamic nuclei. These larger thalamocortical relay (TC) neu-rons project excitatorily (with glutamate) and reciprocally to cor-tical neurons. A single TC neuron typically projects to hundreds or thousands of cortical neurons that occupy a small area, or “cortical column.” Intracortical connections permit cortical col-umns to influence each other’s synaptic activities. Thus, tha-lamic RE neurons can synchronize many thalamocortical TC neurons, which in turn can synchronize a larger population of cortical neurons (even enough to coordinate their postsynaptic potentials [PSPs] into oscillations that are detectable with scalp EEG). In slow-wave sleep, the thalamic slow-wave and spindle pacing causes massive cortical neuronal populations to oscil-late slowly in synchronized PSPs. In waking and REM states, the thalamocortical pacing is reduced, and smaller synchro-nized cortical neuronal populations produce lower-amplitude, faster oscillations. IN = interneurons; Pre = prethalamic affer-ent connections. (Adapted with permission from Destexhe A, Sejnowski TJ. Interactions between membrane conductances underlying thalamocortical slow-wave oscillations. Physiol Rev 2003;83:1401–53.)
Cerebral Cortex
IN
PY
RE
TC
PreThalamus

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 5
sies. Intracranial electrodes routinely detect spike foci that were never evidenced on the extracranial EEG.13 In patients with hippocampal-onset complex partial seizures as determined with intracerebral and subdural electrode monitoring, hippocampal spikes (recorded with depth electrodes) typically are not synchronous with ipsilateral temporal lobe spikes that are recorded with sphenoidal and scalp electrodes. Spikes whose extracranial amplitude is maximal at a sphenoidal electrode probably are generated only in basal temporal neocortex. Spikes whose extracranial amplitude is maximal at temporal scalp electrodes probably are generated only in lateral temporal neocortex. These correlates of extracranial EEG spikes were determined with simultaneous subdural and extracranial electrode recordings and with simultaneous magnetoenceph-alographic and extracranial EEG recordings.14,15
Extracranial EEG recordings of a seizure be-ginning in a small cerebral region will show ictal discharges only after the ictal discharges have spread to a larger volume of cortex that includes superficial sites. In fact, temporal lobe seizures often show generalized or widespread bilateral distributions of the earliest scalp-EEG–detected changes; in these cases, simultaneous intracranial recordings detect ictal discharges that initially are much more focal and begin earlier than the scalp EEG ictal changes.12 It is well recognized that deep or highly focal electrographic seizures often are not recorded with extracranial electrodes, unless there is propagation of ictal discharges to sites and volumes of cortex that permit scalp EEG detec-tion.16–19 Highly focal seizures that are not detected with scalp electrodes often represent simple partial seizures.16,19 During pure amnestic seizures, bilat-eral hippocampal ictal discharges do not propa-gate out of the mesial temporal regions and no ictal discharges are detectable with scalp electrodes;
pure amnestic seizures are not accompanied by unresponsiveness or other behavioral changes.18 In patients with no evidence of static encephalopa-thy or severe unilateral hemispheric dysfunction, it is reasonable to presume that electrographic seizure activity would necessarily involve relatively large bilateral hemispheric volumes of cortex in order to produce complete unresponsiveness and global amnesia during a complex partial seizure, and that such widespread discharges would be detectable with adequately recorded scalp EEG. This tenet is the basis of diagnosis of epileptic and nonepileptic seizures by video-EEG monitoring.
False localization of the earliest ictal discharges on extracranial EEG is a further consequence of the inability of extracranial EEG to record ictal dis-charges in deep structures and highly focal ictal discharges. When the earliest ictal discharges occur over a focal temporal region on scalp or scalp-sphenoidal EEG, the most common correlate on intracerebral EEG would be initial ictal discharg-es in 1 hippocampus, followed by propagation to the ipsilateral temporal neocortex (at which time scalp-sphenoidal EEG shows its earliest ictal re-cording). A less common situation is that of falsely lateralized temporal lobe initial ictal discharges on extracranial EEG; in this situation, intracerebral EEG would record initial ictal discharges in 1 hip-pocampus, followed by atypical intracranial propa-gation patterns such that the contralateral temporal neocortex becomes involved in electrographic seizure activity before the temporal neocortex that is ipsilateral to that hippocampus, with the result that the scalp EEG records earliest ictal changes over the contralateral temporal lobe.20 In some complex cases, scalp-sphenoidal EEG recordings show bilateral independent ictal onsets over both temporal lobes, but intracerebral recordings show that in fact all of the seizures arise in one hippo-

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
6 Hospital physician Board Review Manual www.turner-white.com
campus, with typical propagation patterns during some seizures and atypical propagation patterns during other seizures.21 When the cortex interictally generates a pathological spike-wave complex with a surface-negative spike maximum at the F7-T3 electrodes (which are the “F7-T7” electrodes in the newer nomenclature), the electroencepha-lographer cannot be certain as to whether the 6 cm2 (or larger) spike generator surface was lo-cated on the left inferior frontal gyrus, on the left superior temporal gyrus, or on some other nearby surface, but can be reasonably certain that the generator was not located in the left hippocampus, in the left thalamus, or in the right hemisphere. Similarly, when an individual has interictal spikes recorded independently with maxima at the left anterolateral temporal electrodes and at the right anterolateral temporal electrodes, the electroen-cephalographer cannot determine from these data alone whether the patient has refractory seizures and whether the patient has seizures that arise only in 1 temporal lobe or arise independently in both temporal lobes (or elsewhere).
The true percentage of patients with epilepsy who never have interictal spikes on scalp EEG is not known, due to uncertainties in the true incidence and prevalence of epilepsy by type; variability in EEG techniques (in particular, durations of EEG record-ings used by various qualified electroencephalo- graphers); and limitations of scalp EEG in recording spikes from small and deep-seated sites in focal spikes, such that low-amplitude spikes on scalp EEG likely do not constitute definite scalp EEG spikes. Clearly, some syndromes are more likely to present with interictal spikes than are others. For example, mesial frontal lobe epilepsy is among the syndromes least likely to demonstrate interictal spikes despite very prolonged EEG recording.156
Conversely, some types of pathological spikes are
less likely to be associated with clinical epilepsy than are others. For example, frontal spikes are less likely to be associated with clinical epilepsy than are temporal spikes.22
The “inverse problem” requires a single correct solution to the question of precisely what area of the brain generated electrical dipoles that gen-erated the surface-negative spike or other phe-nomenon of interest in the scalp EEG recording. Extracranial EEG data cannot be used alone to fully solve the “inverse problem”; the expert elec-troencephalographer, however, is able to exclude a large range of impossible or unlikely solutions to the inverse problem, and to analyze a delimited set of reasonable possible solutions to the inverse problem; these possible solutions can be com-pared with nonelectrophysiologic data.
tecHnoloGy and aPPlicationS of eeG
principlEs oF huMan ElEcTrophysiological rEcording
Extracranially recorded EEg Standard extracranial electrodes for clinical EEG
and video-EEG are scalp electrodes placed in the 10-20 system or the 10-10 system (Figure 5), with additional electrodes for reference or comparison, including cutaneous electrocardiographic elec-trodes. “Special” extracranial electrodes include scalp electrodes that are placed at particular sites outside of the 10-20 and 10-10 systems with the intention of better recording from a target structure, such as the “true” anterior temporal electrode,23 as well as specially designed electrodes placed off the scalp. Nasopharyngeal electrodes were once thought to record well from mesiobasal temporal generators, but they are rather uncomfortable, unstable in positioning, and associated with higher levels of artifactual recordings than are scalp
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 7
electrodes.14 Sphenoidal electrodes are mildly inva-sive as they are placed into the masseter muscle under the temporal bone, but are well tolerated chronically (following recovery from acute insertional discomforts) and relatively stable in positioning14; recent studies cast doubt on the posited incre-mental access to mesiobasal temporal generators, however.24 Foramen ovale electrodes now are rarely used, as the burden of insertional pain and hemorrhagic-infectious risks of foraminal entry ap-pear equal to those of intracranial electrode place-ment, while selectivity of cerebral sampling with intracranial electrodes far exceeds the sampling offered by foramen ovale electrodes.25
intracranially recorded EEg (Macro- and Micro-electrodes)
Intracranial electrodes are placed in epidural, subdural, and intra-axial locations with a wide range of electrode morphology (Figure 6). Least invasive are epidural peg or screw electrodes, which are placed through small twist drill holes or burr holes in the skull.26 Recordings with epi-dural and all other types of intracranial electrodes markedly reduce myogenic, kinesigenic, and other artifacts compared with extracranial recordings,27 markedly increase access to electrocerebral oscil-lations above 50 Hz, and reduce voltage decline related to distance from electrocerebral genera-tors. Penetration of the dura increases rates of hemorrhage and probably of infection but in-creases access to specific targets. Insertion of subdural electrode strips though burr holes is in theory safer than stereotaxic insertion of intrace-rebral (“depth”) electrodes, as only the latter are expected to penetrate brain substance. Empirical investigations suggest that the course of manual insertion of subdural strips is not always well con-trolled, however, and unexpected tearing of small
bridging veins can cause subdural hemorrhage, while chronic meningeal cicatrix formation and anatomical complexities have caused subdural strips to actually enter the brain substance.28 Depth electrodes have a more readily controlled course of stereotaxic insertion, and modern imaging per-mits avoidance of all but the smallest of intra-axial vessels. Direct comparison of depth electrode and subdural strip electrode recordings showed that only depth electrodes record from hippocampal electrical generators and that subdural recording from the parahippocampal region rarely may miss critical ictal onset data.29 Large subdural elec-trode grid arrays require craniotomy, which is only
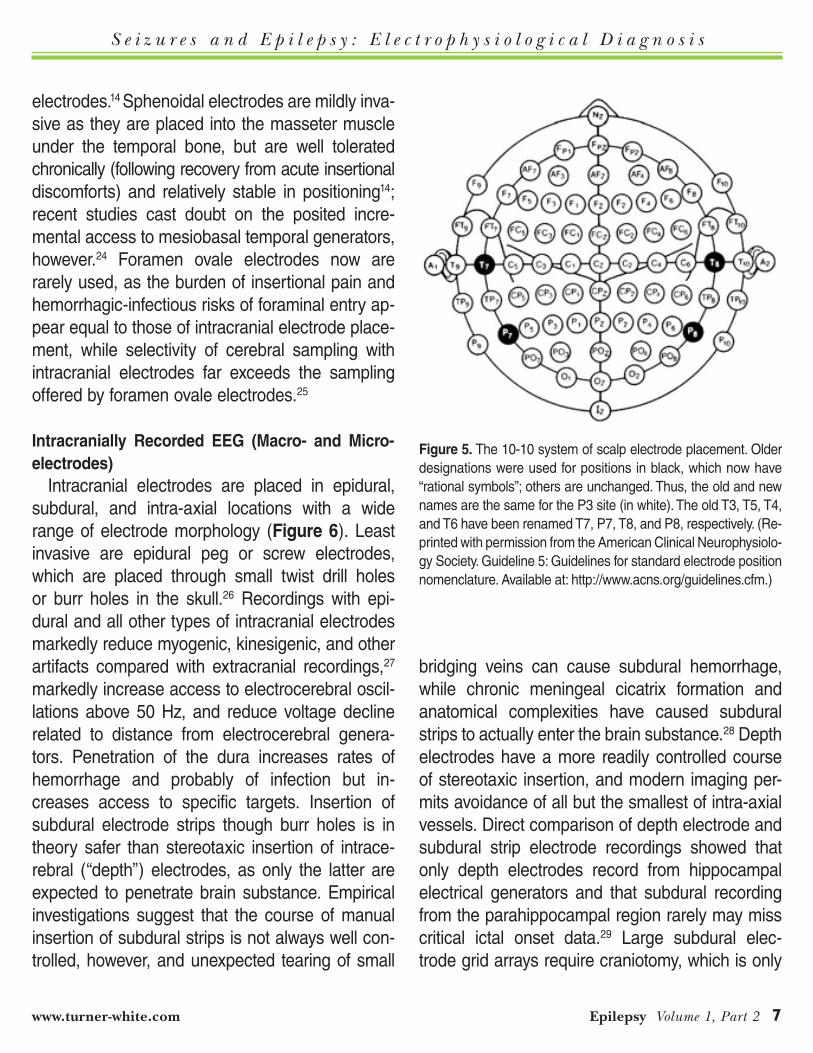
Figure 5. The 10-10 system of scalp electrode placement. Older designations were used for positions in black, which now have “rational symbols”; others are unchanged. Thus, the old and new names are the same for the P3 site (in white). The old T3, T5, T4, and T6 have been renamed T7, P7, T8, and P8, respectively. (Re-printed with permission from the American Clinical Neurophysiolo-gy Society. Guideline 5: Guidelines for standard electrode position nomenclature. Available at: http://www.acns.org/guidelines.cfm.)

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
8 Hospital physician Board Review Manual www.turner-white.com
practical to perform unilaterally but which offers superior sampling from cortical surfaces and the opportunity to map cerebral function with direct
cortical electrical stimulation (DCES) techniques. It must be borne in mind that subdural grids sample from gyral crests and not from sulcal depressions;
Figure 6. Subdural and depth electrodes. (a, B) Brain magnetic resonance (MR) images showing subdural and depth electrodes in place, with often quite prominent signal voids that cause the electrode contacts to appear much larger than they actually are. (c) Multicontact depth electrode inserted posteroanteriorly through occipital gray matter and subjacent white matter into the hippocam-pal formation, as in the brain MR image (A). (d) 4-by-8 contact subdural grid array sited over the left perisylvian area, correspond-ing to the grid seen on the coronal MR image (B). (E) Three subdural strips of 4 or 6 contacts underlying the left temporal lobe. (Adapted with permission from Schulze-Bonhage A, Dennig D, Wagner K, et al. Seizure control resulting from intrahippocampal depth electrode insertion. J Neurol Neurosurg Psychiatry 2010;81:352–3.)
A. B.
C. D. E.
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 9
this may be a minor limitation with regard to map-ping ictal onset zones, given that local propagation of seizure activity occurs rather consistently, such that gyral crest will be involved early in subjacent ictal onsets, but may be a major limitation in elec-trostimulation mapping of cerebral function as the current applied to gyral crests is unlikely to map functions at subjacent sulcal fundi.
All types of intracranial electrodes are much more limited in spatial sampling than are scalp electrodes, which benefits the anatomical speci-ficity of ictal recordings and functional maps but which reduces the opportunity to sample a wide cerebral area. If intracranial electrodes are not situ-ated at the actual site of earliest ictal discharges, then the electrodes that are nearest the actual ictal onset zone will appear to be the sites of ictal onset. Effects of inadequate cerebral sampling on localization of the ictal onset zone for resective therapy can be profound and may lead to ineffica-cious resection with iatrogenic injury to essential cerebral structures. For example, when intracra-nial electrodes have only been placed in bilateral temporal lobe structures, seizures that originate in frontal lobe limbic system structures such as the in-sula and orbitofrontal cortex are likely to propagate rapidly into mesial temporal structures (and pos-sibly to propagate so rapidly as to prevent informa-tive parallel analysis of ictal symptoms and signs), in which case the electroencephalographer may naively assume that a temporal lobe contained the ictal onset zone (which should be resected). It would be unsafe to routinely place subdural and depth electrodes into several hundred cerebral sites bilaterally. It therefore is necessary to care-fully construct hypotheses concerning the most likely ictal onset zones in the individual patient, in order to select a reasonable number of high-probability intracranial sites for seizure recording,
in some cases supplemented by a few “sentinel” electrodes at lower-probability sites (to allow for unexpected but important rejection of the principal hypotheses based on actual seizure recordings). The use of structural and functional imaging data together with extracranial EEG and other data will be discussed in detail in Part 5 of this series.
High-frequency oscillations (HFOs), termed “rip-ples” (100-250 Hz) and “fast ripples” (250–500+ Hz), are recorded with intracranial electrodes.30–33 The burgeoning area of HFO research is being pursued with animal models and human investi-gations using macroelectrodes (“clinically-sized” contacts with recording surfaces of 1–100 mm2) and smaller microelectrodes. Microelectrode re-cordings of single neurons and small neuronal assemblies are performed as research studies in human volunteers and are not widely accepted for any clinical indications.
MagnetoencephalographyMagnetoencephalography (MEG) has been used
in numerous human epilepsy research studies, and in particular to map interictal spike topography and to map functional activated cortical areas. Electrocerebral activities generate magnetic fluxes that are readily detectable with MEG instruments. Unlike EEG signals, at extracranial locations these MEG signals have not been significantly attenu-ated by distance effects and by effects of interven-ing tissues.34,35 Several epilepsy surgery programs use MEG to detect and localize interictal spikes that are undetectable with scalp EEG, in part to assist in selection of sites for intracranial electrode recording of seizures.36
The principal disadvantages of MEG as a po-tential clinical technique appear to be the consid-erable expense of MEG instruments (compared with EEG equipment), the demanding expertise
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
10 Hospital physician Board Review Manual www.turner-white.com
requirements and numerous assumptions neces-sary to delimit the anatomical range of possible flux sources into a single most likely magnetic gen-erator, and the inability to routinely record spon-taneously occurring seizures when seizures are occurring many hours apart. Possibly due to the latter limitation, MEG has not been widely adopted and many MEG experts use MEG primarily for their clinical research and as an adjunctive technique in their clinical practices.
signal averaging Evoked potentials (EPs) and other EEG-aver-
aging techniques have considerably extended the clinical applications of EEG in intraoperative moni-toring and other applications. Most of these ap-plications are not routine components of epilepsy care. An exception is the use of somatosensory EPs for electrocorticographic mapping of essential motor and sensory cortex in order to avoid iatro-genic injury during resection of frontal lobe and parietal lobe sites of ictal onset. Epileptologists who have not completed comprehensive clinical neurophysiology training should be aware of the considerable complexity of acquiring EPs with ex-tracranial or intracranial electrodes, including the numerous sources of artifacts that afflict EP analy-sis both in and out of the operating room.37,38 The physiology and technology of EPs are complex topics that exceed the purview of this epilepsy-oriented review of clinical neurophysiology.
automated spike and seizure detection and other automated analyses
The clinical utility of automated spike and sei-zure detection is widely recognized. Early research with computerized event detection algorithms was pursued in multiple laboratories. Currently, the tech-niques of Jean Gotman and his collaborators un-
derlie essentially all of the detection algorithms that are available with software packages of EEG and video-EEG equipment, often with modifications by in-house engineers of the particular equipment vendor.39,40 Most epilepsy-EEG experts use such FDA-regulated spike and seizure detection software to locate epochs of interest among the thousands of minutes of EEG data that are recorded for a single patient during video-EEG monitoring, followed by qualitative analysis to exclude detection of artifacts and to determine the field, frequency, and morphol-ogy of spikes and seizures. Mechanical and espe-cially biological sources of artifacts continue to pose major problems for automated analyses of extracra-nial EEG data in clinical applications.
Other forms of automated EEG signal process-ing have produced useful insights into seizures, epilepsy, and the EEG signal itself. For example, the initially laborious and complex recording of EEG signals during functional magnetic resonance imaging (fMRI) revealed that focal interictal spikes both activate and deactivate local cortical process-ing as indirectly measured by fMRI.41,42 Available devices and software have rendered fMRI-EEG practical for smaller research teams with less dedi-cated “magnet time” and fewer research hours, but this technique is not yet an established clinical technique. The research applications of automated EEG signal processing are extensive and beyond the scope of this clinically oriented review.
principlEs oF vidEo-EEg MoniToring
The impact of routinely available video-EEG has profoundly extended the care of individual seizure patients, not only for those who have epilepsy but especially for those who do not have epilepsy (or have a mixture of both epileptic and nonepileptic seizures). Improved video-EEG tech-niques also have directly improved planning of

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 11
epilepsy surgery, with more efficient, more com-fortable, and more widely available recording of multiple seizures in the individual patient. Other indications for video-EEG monitoring (Table 2) include therapeutic monitoring of medication re-sponse in nonconvulsive status epilepticus and acute repetitive seizures.
Seizure induction for the purpose of ictal video-EEG recording is primarily achieved with reduction of chronic antiseizure medications and with voli-tional sleep deprivation. In the past, the rate of sei-zure recording during presurgical evaluation was increased by inducing seizures with administration of proconvulsant agents such as pentylenetetrazol and with electrical stimulation of intracranial elec-trodes. These practices were rapidly abandoned after Wieser et al’s landmark study comparing the localizations of “spontaneous” seizures with those of chemically and electrically induced seizures in the same patients showed that many seizures induced chemically and electrically had ictal onset zones that never occurred with the patient’s sponta-neous seizures.43 In some instances psychogenic events have been induced with intense suggestion by hypnosis or similar techniques, but it generally is not clear whether these seizures would have oc-curred as the individual’s habitual seizure type or whether a highly suggestible individual (who may or may not have epilepsy) has had an atypical event induced with hypnosis. Most epilepsy-EEG experts rely on seizure diagnosis with events re-corded with, or without, reduction of antiseizure medications and sleep deprivation.
Paroxysmal behavioral events that involve tran-sitory unconsciousness or globally impaired con-sciousness can be caused by epileptic seizures, by certain types of nonepileptic organic events such as parasomnias and syncope, and by psy-chogenic nonepileptic events.44,45 Many individu-
als who are transiently unconscious due to a complex partial seizure are unable to recognize and report that they were unconscious, however.46 In the absence of any means to directly determine whether an individual is conscious, neurologists and others instead assess behavioral correlates of consciousness. In an individual who usually is responsive to voice and touch and who usu-ally is able to later recall verbal and nonverbal stimuli that were presented during a waking state, the paroxysmal and brief occurrence of complete unresponsiveness to voice and touch coupled with later (on regaining normally responsive alert behavior) inability to recall verbal and nonverbal stimuli that were presented during the period of unresponsiveness is a reasonable behavioral defi-nition of unconsciousness.44
Considerable harm can result from incorrect-ly diagnosing psychogenic nonepileptic seizures (“pseudoseizures”), and from diagnosing only psy-chogenic nonepileptic seizures in an individual who has both epileptic and nonepileptic seizures habitually. For many reasons, most epilepsy-EEG experts definitively diagnose nonepileptic seizures only when the reportedly habitual event has been recorded with technically adequate video-EEG, which permits the expert to examine both the re-corded behavior as well as the associated EEG activities during the event. Normal interictal EEGs
Table 2. Indications for Video-EEG Monitoring
Presurgical evaluation in refractory epilepsy Diagnosis of paroxysmal events Therapeutic monitoring in nonconvulsive status epilepticus and
other conditions Detection of unrecognized or under-reported seizures Other indications

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 15
are quite common in many forms of epilepsy; a nor-mal interictal EEG in a psychologically distressed patient is not diagnostic of psychogenic seizures. Unchanged scalp EEG activities are common dur-ing simple partial seizures; the absence of scalp EEG-recorded ictal discharges is expected during patient-reported seizures in which responsiveness is maintained, although a minority of simple partial seizures do produce scalp-EEG–recorded ictal discharges or nonspecific changes from the base-line EEG. Psychogenic events do not have any pathognomonic age or gender range, semiological history, interictal EEG findings, or imaging find-ings.45,47 Risk factors for psychogenic events can be found on mental health history and on neuro-psychological testing, but none of these risk factors excludes the possibility of epilepsy or organic non-epileptic events. Similarly, recording the habitual behavioral events with video-EEG monitoring (or polysomnography with additional EEG electrodes) is necessary to distinguish parasomnias and REM sleep behavior disorder from nocturnal epileptic seizures, as well as from nocturnal psychogenic events. Although it appears to be true that paroxys-mal psychogenic events do not arise directly from sleep states, it is relatively common to encounter individuals who report sleep-onset events that are shown on video-EEG to be psychogenic events arising during a period of nighttime waking state. Patients and their observers often report that a “sei-zure” occurred during ambulatory EEG recording, but the electroencephalographer will not be able to determine what behaviors actually occurred in the absence of video recording. Recording habitual behavioral events with video-EEG monitoring is generally required for confident diagnosis of psy-chogenic nonepileptic seizures, and usually is quite helpful in diagnosing epileptic seizures and “or-ganic” nonepileptic seizures such as parasomnias.
The central tenet of diagnostic video-EEG might be stated as: Electrographic seizure activity must involve bilateral cortex of volumes sufficient to be detected with adequately recorded scalp EEG in order to produce complete unresponsiveness and global amnesia in patients with no evidence of stat-ic encephalopathy or severe unilateral hemispheric dysfunction. In such patients, ictal discharges in cortical volumes too small to be detected with ad-equate EEG also cannot globally alter awareness, responsiveness, and memory formation. Thus, in a patient who has normal or nearly normal respon-siveness and memory in the absence of seizures, if the patient has behavioral testing during an event with complete unresponsiveness to voice and touch, for which the patient subsequently has no memory, and has technically adequate EEG recording at this time with waking or lightly drowsy EEG activities that are unchanged from baseline, the patient apparently has had a psycho-genic event. Epileptic seizures that cause global unresponsiveness and global amnesia, such as complex partial seizures and absence seizures, consistently have ictal discharges on adequately recorded scalp EEG. Organic nonepileptic events that cause global unresponsiveness and global amnesia, such as syncope and parasomnias, have EEG findings other than baseline waking or lightly drowsy activities. Under current understanding of cerebral function, only psychogenic processes would be likely to account for such events. This tenet is logical, concordant with current knowledge of cerebral function, and fits with extensive clinical experience, but cannot be considered to be “prov-en” in all possible situations of unconsciousness. When video-EEG recording of a habitual event is the principal basis for diagnosis of a psychogenic nonepileptic seizure, adherence to requirements of technical adequacy of EEG recording and of

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
16 Hospital physician Board Review Manual www.turner-white.com
behavioral testing are likely to be quite important. In many cases, the EEG diagnosis can be supple-mented with behavioral analysis of particular motor behaviors during habitual events and other data in order to strengthen the diagnosis.
principlEs oF Mapping oF EloquEnT corTEx wiTh dirEcT corTical ElEcTrical sTiMulaTion
DCES is usually performed over cortical surfaces for the purpose of mapping motor, sensory, or cog-nitive functions, but has also been performed with intracerebral electrodes for stimulation of the hippo-campus or other deep structures or for the purpose of inducing seizures. In all applications of DCES, patient safety is of paramount importance. Currently available (FDA-approved) stimulators have hard-wired stimulus isolation circuits, and providing that the isolation circuit is checked for integrity by quali-fied personnel, such a stimulator can be safely used in the electrical environment of any operating room without arranging additional electrical isolation. Ad-ditionally, modern stimulators provide current pulses of alternating polarity so that no net DC current is applied to the brain, and also provide stimulation of constant current so that it is not necessary to mea-sure the impedance between particular electrodes at each cortical site in order to calculate the voltage to be passed to achieve the desired current.
Electrocorticography is performed concurrently with DCES in order to recognize afterdischarges and electrographic seizures that will affect the interpretation of any behavioral changes induced by stimulation, as well as for purposes of patient safety. Safety is also assured by limiting the total charge delivered and the charge density over the stimulated volume of tissue. It has been demon-strated in humans that charge densities of less than about 55 microcoulombs/cm2/phase do not
induce histologically detectable lesions of sub-sequently resected tissue.48 Standard electrode strips and grids have an uninsulated surface area of about 12 to 13 mm2 per contact with the cor-tex; with bipolar wand stimulators, the size of the electrode surface area varies but is often about 4 mm2. The larger electrodes have a smaller charge density per phase for the current intensity that is produced by the stimulator. The stimula-tor should produce trains of current in alternating polarity, so that there is no net charge applied over the duration of each stimulation. Stimulation is typically applied in trains lasting 2 to 5 seconds at a rate of 50 phases/second with each phase lasting 0.3 ms. Stimulation typically begins at low intensities of current; when these stimulation pa-rameters are used with standard subdural strip and grid arrays, this would be 0.5 milliamperes of current. During cortical function mapping, if no afterdischarges or seizures occur and no behav-ioral effects are noted, current intensity is typi-cally increased sequentially to a maximum of 15 milliamperes, if using standard subdural arrays. The current setting on the stimulator should be adjusted to achieve comparable charge densities for the particular electrode surface area exposed by the particular bipolar wand stimulator.49
Afterdischarges are interictal epileptiform activi-ties that may consist of single or rhythmically or ir-regularly repetitive spike-wave, sharp wave-slow wave, or polyspike-wave discharges; less often, they consist of paroxysmal fast activity that ap-pears relatively monorhythmic.50 At an individual site of stimulation, the afterdischarges may strong-ly resemble the spontaneous interictal epileptiform activities noted to occur during the baseline pre-stimulation period of electrocorticography, so that at times it may be difficult to distinguish an afterdis-charge from a frequently occurring spontaneous

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 17
epileptiform discharge that by chance occurred at the end of cortical stimulation. Continuing stimula-tion at a site at which afterdischarges have been induced can subsequently induce an electrograph-ic seizure, particularly if current is progressively in-creased despite the occurrence of afterdischarges; this is undesirable if a secondarily generalized sei-zure is induced. If the purpose of stimulation is cor-tical function mapping, postictal regional cerebral depression may confound further behavioral test-ing. On the other hand, repeated stimulation at the same current (or transiently at a lower current) at a site at which afterdischarges have been obtained can sometimes elevate the threshold for afterdis-charge production.51 It may be desirable to elevate afterdischarge thresholds when the purpose of stimulation is language mapping, since relatively higher current densities are required for adequate local language mapping than for motor or sensory mapping over the primary sensorimotor cortices. A prolonged afterdischarge may be difficult to dis-tinguish from an electrographic seizure. When af-terdischarges or electrographic seizures occur at a particular site, it cannot be concluded that that site is ordinarily responsible for the induced behavioral responses, since there may have been propaga-tion of the electrical events to distant sites at which recording electrodes have not been placed, and activation or deactivation of the ordinary neuronal activities at these distant sites may be responsible for the observed behavioral change.
interictal ePilePtiform activitieS
inTEricTal EpilEpTiForM acTiviTiEs on scalp EEg
Focal spikes and sharp waves Temporal and frontotemporal spikes. Tem-
poral spikes and sharp waves are the most com-
monly encountered of focal epileptiform activities. They are usually seen in disorders of temporal lobe epilepsy, such as mesial temporal sclerosis (MTS). These discharges usually have a maxi-mum over the anterior temporal region and have a surface-negative polarity (in contrast to the Ro-landic spike).52 They are more frequent and more prominent during sleep and drowsiness (Figure 7). They may appear as spike followed by slow-wave activities and are often accompanied by back-ground activities such as ipsilateral temporal theta or delta slowing. Temporal lobe spike should be distinguished from small sharp spikes, which is a normal variant during light sleep. Small sharp spikes usually have short duration, low amplitude, a brief aftergoing slow wave, a wide field, and an undisturbed background activity. They are often seen bilaterally. Small sharp spikes are also called benign epileptiform transients of sleep (BETS).53,54
It is widely considered that over 90% of patients whose interictal EEG shows pathological temporal lobe spikes will actually have temporal lobe sei-zures, although the definitive population study to
Figure 7. Right temporal spike. A single spike can be seen at the right temporal region in an 83-year-old man with a history of intractable seizures.
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
18 Hospital physician Board Review Manual www.turner-white.com
establish this clinical experience is yet to be pub-lished. Clearly, the occurrence of pathological tem-poral lobe spikes on an interictal EEG would not be expected to prevent psychogenic nonepileptic sei-zures in an individual who probably has temporal lobe epilepsy; ictal EEG is necessary for definitive diagnosis of events that have been controlled with appropriate medications.55,56
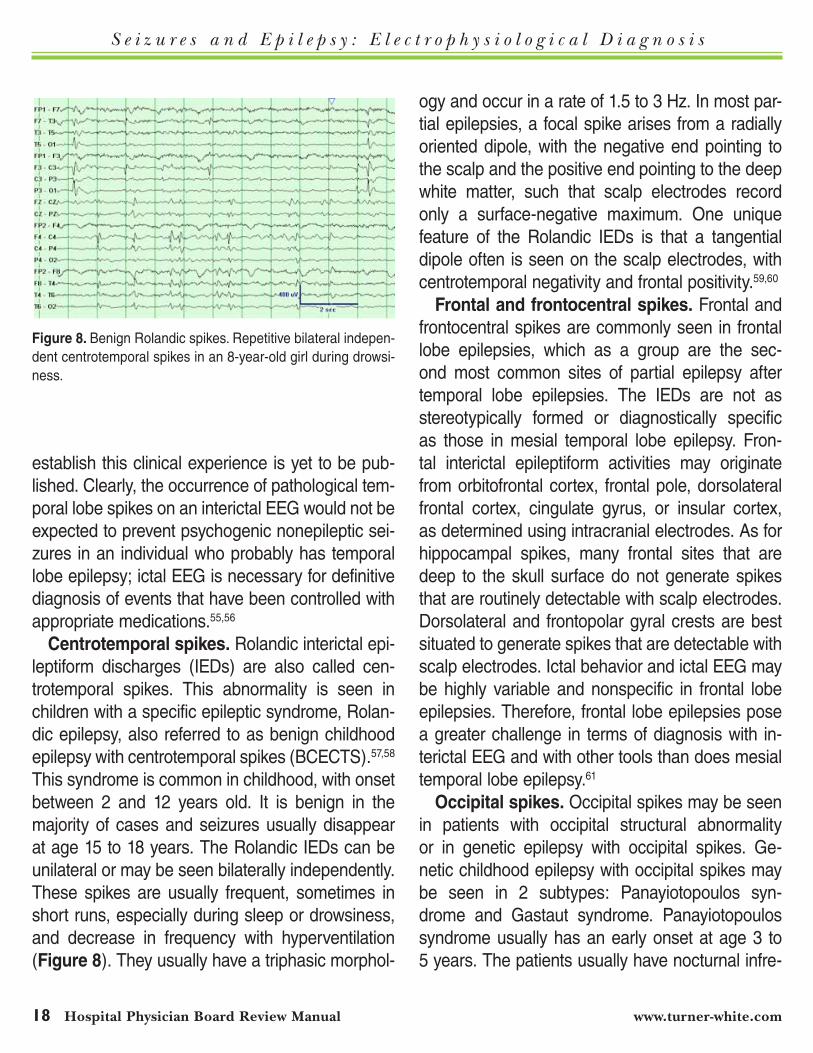
centrotemporal spikes. Rolandic interictal epi-leptiform discharges (IEDs) are also called cen-trotemporal spikes. This abnormality is seen in children with a specific epileptic syndrome, Rolan-dic epilepsy, also referred to as benign childhood epilepsy with centrotemporal spikes (BCECTS).57,58 This syndrome is common in childhood, with onset between 2 and 12 years old. It is benign in the majority of cases and seizures usually disappear at age 15 to 18 years. The Rolandic IEDs can be unilateral or may be seen bilaterally independently. These spikes are usually frequent, sometimes in short runs, especially during sleep or drowsiness, and decrease in frequency with hyperventilation (Figure 8). They usually have a triphasic morphol-
ogy and occur in a rate of 1.5 to 3 Hz. In most par-tial epilepsies, a focal spike arises from a radially oriented dipole, with the negative end pointing to the scalp and the positive end pointing to the deep white matter, such that scalp electrodes record only a surface-negative maximum. One unique feature of the Rolandic IEDs is that a tangential dipole often is seen on the scalp electrodes, with centrotemporal negativity and frontal positivity.59,60
Frontal and frontocentral spikes. Frontal and frontocentral spikes are commonly seen in frontal lobe epilepsies, which as a group are the sec-ond most common sites of partial epilepsy after temporal lobe epilepsies. The IEDs are not as stereotypically formed or diagnostically specific as those in mesial temporal lobe epilepsy. Fron-tal interictal epileptiform activities may originate from orbitofrontal cortex, frontal pole, dorsolateral frontal cortex, cingulate gyrus, or insular cortex, as determined using intracranial electrodes. As for hippocampal spikes, many frontal sites that are deep to the skull surface do not generate spikes that are routinely detectable with scalp electrodes. Dorsolateral and frontopolar gyral crests are best situated to generate spikes that are detectable with scalp electrodes. Ictal behavior and ictal EEG may be highly variable and nonspecific in frontal lobe epilepsies. Therefore, frontal lobe epilepsies pose a greater challenge in terms of diagnosis with in-terictal EEG and with other tools than does mesial temporal lobe epilepsy.61
occipital spikes. Occipital spikes may be seen in patients with occipital structural abnormality or in genetic epilepsy with occipital spikes. Ge-netic childhood epilepsy with occipital spikes may be seen in 2 subtypes: Panayiotopoulos syn-drome and Gastaut syndrome. Panayiotopoulos syndrome usually has an early onset at age 3 to 5 years. The patients usually have nocturnal infre-
Figure 8. Benign Rolandic spikes. Repetitive bilateral indepen-dent centrotemporal spikes in an 8-year-old girl during drowsi-ness.
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 19
quent seizures, with lateralized gaze and ictal vom-iting. Prognosis is usually excellent in this subtype. Gastaut syndrome is usually late onset at age 7 to 9 years. Seizures usually involve visual symptoms and postictal vomiting. These patients tend to re-spond to medications. Gastaut syndrome usually has a less favorable prognosis than the Panayio-topoulos syndrome. The EEG features of these 2 variants are essentially indistinguishable. They have occipital dysphasic spikes or sharp waves with high-voltage negative peak followed by posi-tive peak with a normal background activity.62,63
generalized spikes and sharp waves classic generalized 3-hz spike-wave dis-
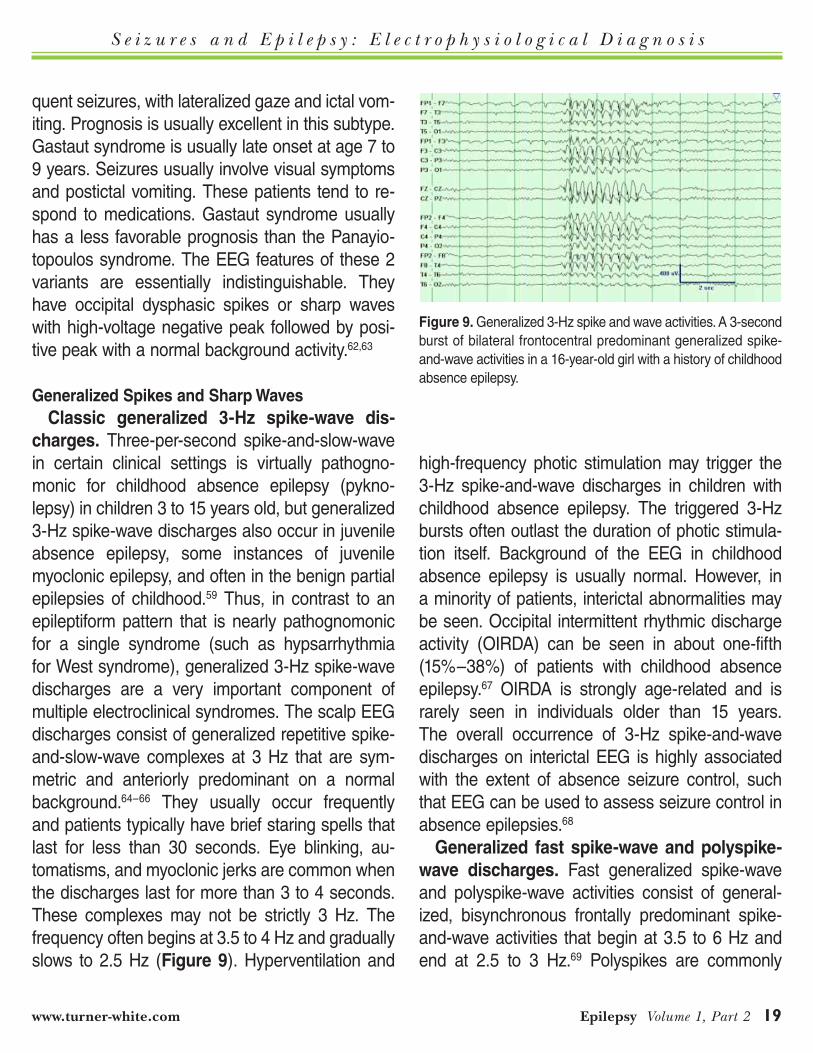
charges. Three-per-second spike-and-slow-wave in certain clinical settings is virtually pathogno-monic for childhood absence epilepsy (pykno-lepsy) in children 3 to 15 years old, but generalized 3-Hz spike-wave discharges also occur in juvenile absence epilepsy, some instances of juvenile myoclonic epilepsy, and often in the benign partial epilepsies of childhood.59 Thus, in contrast to an epileptiform pattern that is nearly pathognomonic for a single syndrome (such as hypsarrhythmia for West syndrome), generalized 3-Hz spike-wave discharges are a very important component of multiple electroclinical syndromes. The scalp EEG discharges consist of generalized repetitive spike-and-slow-wave complexes at 3 Hz that are sym-metric and anteriorly predominant on a normal background.64–66 They usually occur frequently and patients typically have brief staring spells that last for less than 30 seconds. Eye blinking, au-tomatisms, and myoclonic jerks are common when the discharges last for more than 3 to 4 seconds. These complexes may not be strictly 3 Hz. The frequency often begins at 3.5 to 4 Hz and gradually slows to 2.5 Hz (Figure 9). Hyperventilation and
high-frequency photic stimulation may trigger the 3-Hz spike-and-wave discharges in children with childhood absence epilepsy. The triggered 3-Hz bursts often outlast the duration of photic stimula-tion itself. Background of the EEG in childhood absence epilepsy is usually normal. However, in a minority of patients, interictal abnormalities may be seen. Occipital intermittent rhythmic discharge activity (OIRDA) can be seen in about one-fifth (15%–38%) of patients with childhood absence epilepsy.67 OIRDA is strongly age-related and is rarely seen in individuals older than 15 years. The overall occurrence of 3-Hz spike-and-wave discharges on interictal EEG is highly associated with the extent of absence seizure control, such that EEG can be used to assess seizure control in absence epilepsies.68
generalized fast spike-wave and polyspike-wave discharges. Fast generalized spike-wave and polyspike-wave activities consist of general-ized, bisynchronous frontally predominant spike-and-wave activities that begin at 3.5 to 6 Hz and end at 2.5 to 3 Hz.69 Polyspikes are commonly
Figure 9. Generalized 3-Hz spike and wave activities. A 3-second burst of bilateral frontocentral predominant generalized spike-and-wave activities in a 16-year-old girl with a history of childhood absence epilepsy.
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
20 Hospital physician Board Review Manual www.turner-white.com
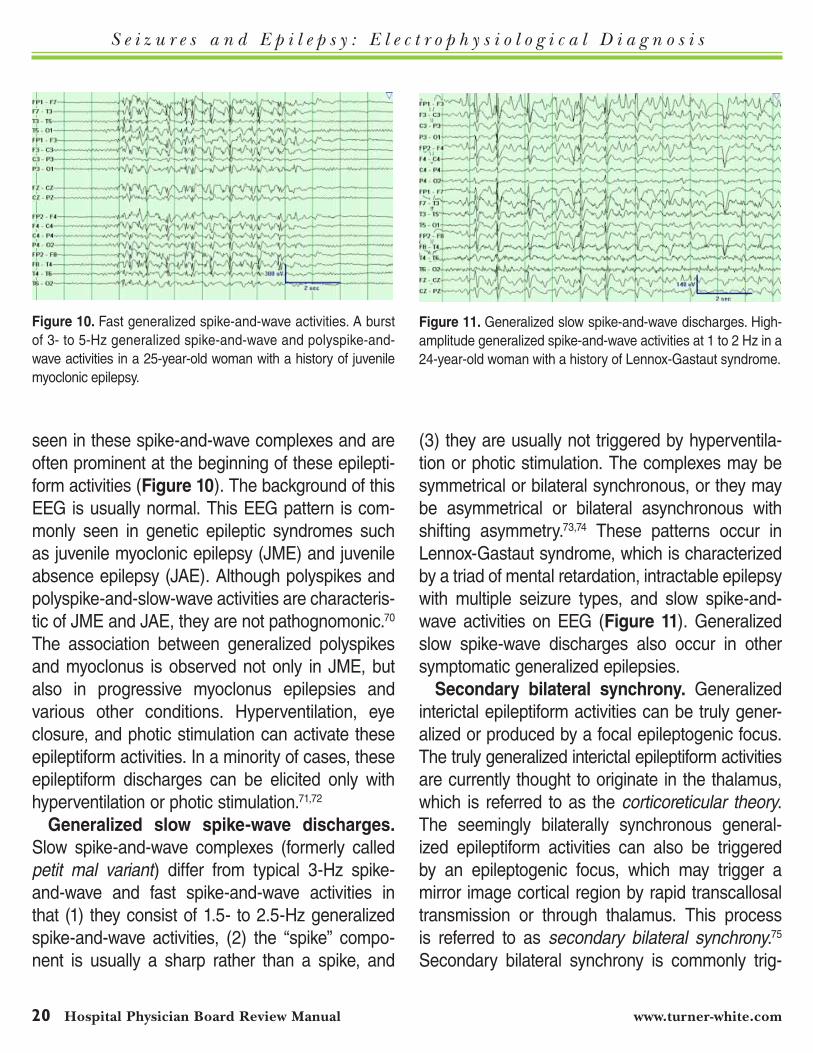
seen in these spike-and-wave complexes and are often prominent at the beginning of these epilepti-form activities (Figure 10). The background of this EEG is usually normal. This EEG pattern is com-monly seen in genetic epileptic syndromes such as juvenile myoclonic epilepsy (JME) and juvenile absence epilepsy (JAE). Although polyspikes and polyspike-and-slow-wave activities are characteris-tic of JME and JAE, they are not pathognomonic.70 The association between generalized polyspikes and myoclonus is observed not only in JME, but also in progressive myoclonus epilepsies and various other conditions. Hyperventilation, eye closure, and photic stimulation can activate these epileptiform activities. In a minority of cases, these epileptiform discharges can be elicited only with hyperventilation or photic stimulation.71,72
generalized slow spike-wave discharges. Slow spike-and-wave complexes (formerly called petit mal variant) differ from typical 3-Hz spike-and-wave and fast spike-and-wave activities in that (1) they consist of 1.5- to 2.5-Hz generalized spike-and-wave activities, (2) the “spike” compo-nent is usually a sharp rather than a spike, and
(3) they are usually not triggered by hyperventila-tion or photic stimulation. The complexes may be symmetrical or bilateral synchronous, or they may be asymmetrical or bilateral asynchronous with shifting asymmetry.73,74 These patterns occur in Lennox-Gastaut syndrome, which is characterized by a triad of mental retardation, intractable epilepsy with multiple seizure types, and slow spike-and-wave activities on EEG (Figure 11). Generalized slow spike-wave discharges also occur in other symptomatic generalized epilepsies.
secondary bilateral synchrony. Generalized interictal epileptiform activities can be truly gener-alized or produced by a focal epileptogenic focus. The truly generalized interictal epileptiform activities are currently thought to originate in the thalamus, which is referred to as the corticoreticular theory. The seemingly bilaterally synchronous general-ized epileptiform activities can also be triggered by an epileptogenic focus, which may trigger a mirror image cortical region by rapid transcallosal transmission or through thalamus. This process is referred to as secondary bilateral synchrony.75 Secondary bilateral synchrony is commonly trig-
Figure 11. Generalized slow spike-and-wave discharges. High-amplitude generalized spike-and-wave activities at 1 to 2 Hz in a 24-year-old woman with a history of Lennox-Gastaut syndrome.
Figure 10. Fast generalized spike-and-wave activities. A burst of 3- to 5-Hz generalized spike-and-wave and polyspike-and-wave activities in a 25-year-old woman with a history of juvenile myoclonic epilepsy.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 21
gered by a mesial frontal focus, which is best de-tected by transverse bipolar montages (Figure 12). Primary and secondary bilateral synchrony have completely different clinical implications and should be carefully distinguished in clinical practice.
atypical generalized spike-wave discharges. Each stereotypical form of generalized spike-wave discharges has a range of variability, with shift-ing maxima that usually are on average at the fronto- central midline, and with some variabil-ity in the rate and rhythmicity of the spike-wave complexes (whether slow, 3 Hz, or fast). When focal amplitude maxima are highly lateralized, rate and rhythms are excessively variable, and other features exceed the usual degree of stereotypy for one of the major types of generalized spike-wave discharges, the generalized discharges are usually termed atypical generalized spike-wave discharges. Some of these atypical generalized spike-wave discharges may represent second-ary bilateral synchrony, but many do not. Such atypical generalized spike-wave discharges most often occur in progressive myoclonic epilepsies and other syndromes with major interictal cerebral dysfunction, but they also can occur in idiopathic generalized epilepsies.76,77 A predominance of generalized theta slowing (rather than delta slow-ing) with atypical generalized spike-wave and polyspike-wave discharges in early childhood sug-gests Dravet syndrome, although clinical history is necessary to make this electroclinical syndromic diagnosis.78 When the frequency reaches 6 Hz, they must be distinguished from 6-Hz phantom spike-and-wave activities, which are benign vari-ants with more focal, lower-amplitude discharges.
continuous spike-and-wave during sleep. When children have generalized spike-wave dis-charge during more than 85% of the non-REM sleep recording, continuous spike-and-wave dur-
ing sleep is diagnosed. Further clinical information will be necessary to distinguish the associated electroclinical syndromes of Landau-Kleffner syn-drome versus epileptic encephalopathy with con-tinuous spike-and-wave during sleep.79,80
Multifocal independent spikes. Multifocal in-dependent spike discharges (MISD) are defined as having epileptiform waves or spikes in both hemi-spheres with 3 or more independent foci. The focal maxima of 3 or more spike foci must be at least 2 interelectrode distances apart in the 10-20 system. Patients with MISD often have frequent seizures that are intractable to multiple antiepileptic drugs and multiple seizure types including generalized tonic-clinic seizures. They often have severe cere-bral dysfunction and developmental delay. MISD is closely related to hypsarrhythmia and slow spike-and-wave activities.81 Many patients with hypsar-rhythmia have evolution of interictal EEG findings
Figure 12. Secondary bilateral synchrony. Atypical generalized spike-wave discharges of secondary bilateral synchrony are in some instances preceded by a “triggering spike,” as seen in this interictal scalp EEG in a 35-year-old man who had a focal cortical dysplasia of the right frontal lobe on MRI. Below the asterisk in this figure is a right frontal spike that precedes a high-amplitude generalized spike-wave burst. (Adapted with permission from Chang EF, Nagarajan SS, Mantle M,et al. Magnetic source imaging for the surgicalevaluation of electroencephalography-confirmed secondarybilateral syn-chrony in intractable epilepsy. J Neurosurg 2009;111:1248–56.)
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
22 Hospital physician Board Review Manual www.turner-white.com
from hypsarrhythmia into MISD, then eventually into a predominance of generalized slow spike-and-wave complexes.
other interictal Epileptiform activities on scalp EEg Temporal intermittent rhythmic delta activi-
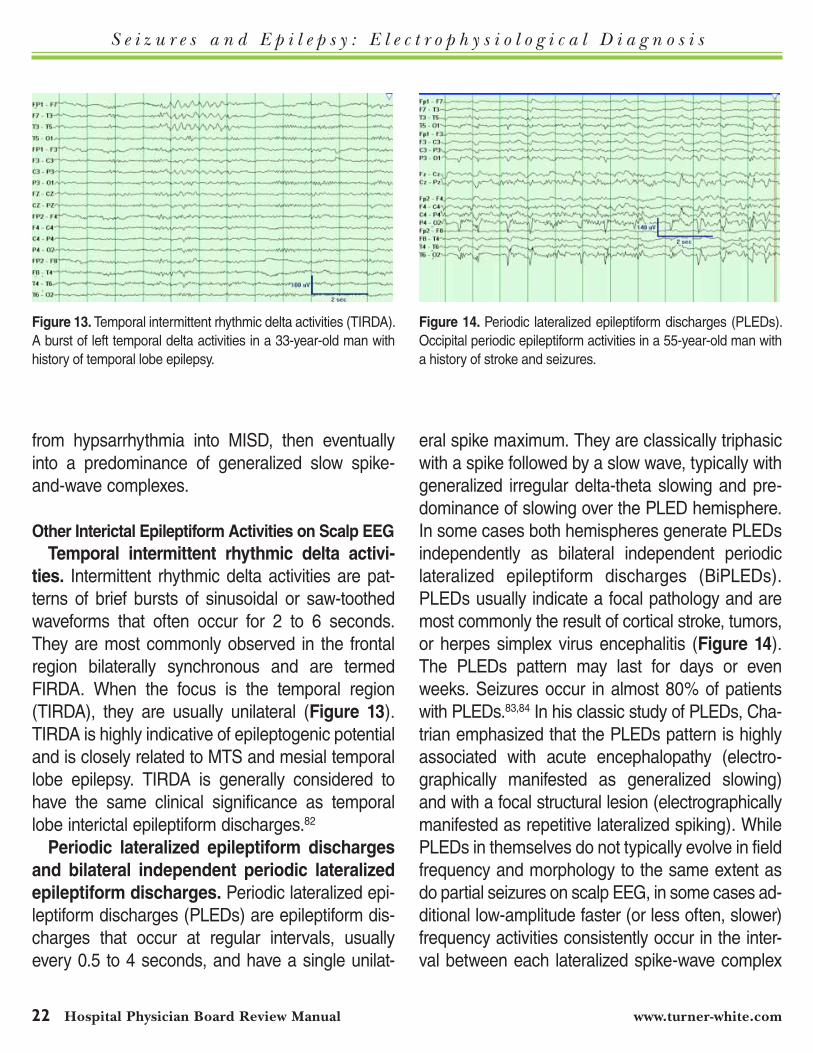
ties. Intermittent rhythmic delta activities are pat-terns of brief bursts of sinusoidal or saw-toothed waveforms that often occur for 2 to 6 seconds. They are most commonly observed in the frontal region bilaterally synchronous and are termed FIRDA. When the focus is the temporal region (TIRDA), they are usually unilateral (Figure 13). TIRDA is highly indicative of epileptogenic potential and is closely related to MTS and mesial temporal lobe epilepsy. TIRDA is generally considered to have the same clinical significance as temporal lobe interictal epileptiform discharges.82
periodic lateralized epileptiform discharges and bilateral independent periodic lateralized epileptiform discharges. Periodic lateralized epi-leptiform discharges (PLEDs) are epileptiform dis-charges that occur at regular intervals, usually every 0.5 to 4 seconds, and have a single unilat-
eral spike maximum. They are classically triphasic with a spike followed by a slow wave, typically with generalized irregular delta-theta slowing and pre-dominance of slowing over the PLED hemisphere. In some cases both hemispheres generate PLEDs independently as bilateral independent periodic lateralized epileptiform discharges (BiPLEDs). PLEDs usually indicate a focal pathology and are most commonly the result of cortical stroke, tumors, or herpes simplex virus encephalitis (Figure 14). The PLEDs pattern may last for days or even weeks. Seizures occur in almost 80% of patients with PLEDs.83,84 In his classic study of PLEDs, Cha-trian emphasized that the PLEDs pattern is highly associated with acute encephalopathy (electro-graphically manifested as generalized slowing) and with a focal structural lesion (electrographically manifested as repetitive lateralized spiking). While PLEDs in themselves do not typically evolve in field frequency and morphology to the same extent as do partial seizures on scalp EEG, in some cases ad-ditional low-amplitude faster (or less often, slower) frequency activities consistently occur in the inter-val between each lateralized spike-wave complex
Figure 14. Periodic lateralized epileptiform discharges (PLEDs). Occipital periodic epileptiform activities in a 55-year-old man with a history of stroke and seizures.
Figure 13. Temporal intermittent rhythmic delta activities (TIRDA). A burst of left temporal delta activities in a 33-year-old man with history of temporal lobe epilepsy.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 23
of the PLEDs; this phenomenon has been termed “PLEDs-plus.”85 The currently prevailing opinion is that PLEDs sometimes represent the scalp EEG manifestation of deep-seated seizures, but usually are an interictal phenomenon. The PLEDs-plus and BiPLEDs patterns appear more likely to be as-sociated with ongoing seizures than are unilateral “simple” PLEDs. Although occurrence of PLEDS usually is monophasic and nonrecurrent, in some cases PLEDs can later recur in patients whose le-sion is static (such as a chronic cerebral infarction) but who have a major acute encephalopathic insult (such as ethanol withdrawal) well after the acute phase of the focal lesion.86
generalized periodic epileptiform discharges. Generalized periodic epileptiform discharges (GPEDs) are also called bilateral periodic epi-leptiform discharges (BiPEDs). They consist of generalized epileptiform discharges that are sym-metric and synchronous. They tend to be anterior predominant. The amplitudes of the spikes are usually 100 to 1000 µV (Figure 15). GPEDs are the result of a variety of pathological conditions that are likely to produce structural abnormali-ties, such as anoxic injury, subacute sclerosing panencephalitis, and Creutzfeldt-Jakob disease. GPEDs can occur as an interictal pattern, as gen-eralized spike-wave complexes recurring every 0.5 to 4 seconds monorhythmically or irregularly, superimposed on a generalized delta-theta back-ground, in various severe encephalopathies, or with additional features of evaluation or cycling in nonconvulsive status epilepticus (see further below). BiPEDs (GPEDs) must be distinguished from BiPLEDs, as the former are bilaterally syn-chronous and the latter are bilateral independent, asynchronous, periodic epileptiform discharges.87
generalized paroxysmal fast activity. GPFA is a burst of beta activities that is commonly in the
range of 10 to 25 Hz, with a generalized and usu-ally symmetrically frontocentral predominance. (Focal or hemispheric paroxysmal fast activity occurs infrequently and does not have the same clinical associations as GPFA.) GPFA typically has sudden onset and resolution, and the am-plitude is occasionally decreased compared to the background slow-wave activities (Figure 16). When GPFA amplitude is severely decreased, the beta activities may not be immediately evi-dent and the GPFA may appear to represent a generalized attenuation such as might occur due to arousal; the pathological generalized beta activities will be evident when the display gain is increased, however. In addition to occurring in brief bursts interictally and usually in sleep, longer runs of GPFA typically occur in tonic seizures and mental retardation.88
hypsarrhythmia. Hypsarrhythmia is a rather unique EEG pattern with chaotic, disorganized, asynchronous, very high-voltage (often >300 mV) diffuse slow waves intermixed with multifocal spikes and slow waves (Figure 17).89–91 This pat-tern occurs in West syndrome in young children,
Figure 15. Generalized periodic epileptiform discharges (GPEDs). Generalized periodic epileptiform activities in a 51-year-old wom-an with a history of cardiac arrest.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
24 Hospital physician Board Review Manual www.turner-white.com
which consists of a triad of infantile spasm, psy-chomotor development delay, and EEG pattern with hypsarrhythmia. The onset of West syn-drome is mostly in the first year of life. The pattern of hypsarrhythmia is usually only seen in the early stage of the infantile spasm, and the EEG may evolve into less chaotic, lower-amplitude, slow spike-and-wave activities. The atypical forms of modified hypsarrhythmia include asymmetric hypsarrhythmia, hypsarrhythmia with a consistent focus of abnormal discharge, hypsarrhythmia with episodic attenuation, hypsarrhythmia with primarily high-voltage slow activity and paucity of sharp-wave or spike activity, and hypsarrhythmia with increased interhemispheric synchronization. Among these modified hypsarrhythmias, asym-metric hypsarrhythmia is most commonly encoun-tered.92
Burst-suppression. Interictal EEGs in the neonatal period show burst-suppression patterns in the Ohtahara syndrome and early-myoclonic encephalopathy.93,94 Burst-suppression is not spe-cific to other epileptic syndromes, although it may be encountered during aggressive medication
therapy of status epilepticus or status-associated anoxia.
photoconvulsive responses. Photoconvulsive responses, also called photoparoxysmal respons-es or photoepileptiform responses, are generalized spike-wave discharges activated by repetitive pho-tic stimulation. Red light is most effective in eliciting photoconvulsive responses.95 These responses are most often induced at photic frequencies of 10 to 20 Hz. The EEG pattern may be anterior or occipital predominant, generalized, bisynchronous, or strongly lateralized. Photoconvulsive responses are associated with different types of generalized seizures such as generalized tonic-clonic seizures, myoclonic seizures, or absence seizures. Most of the observed photoconvulsive responses are poor-ly formed spike-and-wave or polyspike-and-wave complexes.96,97 Photoconvulsive responses must be distinguished from photomyogenic responses that are noncerebral, nonepileptiform in nature. Photomyogenic responses are caused by subtle eye movement and frontotemporalis myogenic ar-tifacts (Figure 18). They are time-locked with the photic stimulations and disappear when the light
Figure 17. Hypsarrhythmia. High-amplitude, chaotic pattern with multifocal spikes and slow waves in a 6-month-old boy with an inborn error of metabolism.
Figure 16. Generalized paroxysmal fast activity (GPFA). A burst of 12- to 15-Hz generalized fast activities in a 36-year-old man with intractable seizures and mental retardation.
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 25
flashes discontinue, whereas the photoconvulsive responses will usually outlast the photic stimulation for a few seconds.98
inTEricTal EpilEpTiForM acTiviTiEs on inTracranially rEcordEd EEg
Intracranial EEG recording may obtain critical information when scalp EEG recording and other evaluations do not definitively localize the ictal onset zone. Intracranial EEG is mainly used for epilepsy surgery presurgical evaluation and cortical function-al brain mapping. Two types of intracranial monitor-ing techniques are commonly used: depth electrode and subdural electrode recording.99 The intracranial EEG recording is reviewed with the same principles as the scalp EEG with a few differences. Intracra-nial signals usually have few artifacts because the electrodes are in a relatively fixed position relative to the cortex and have no muscle contact. Although potentials recorded with intracranial electrodes can be displayed in bipolar or referential montages, they are usually grouped by lobar location, such as ante-rior or posterior temporal lobe. The fast frequencies are not filtered by the scalp and skull, which makes
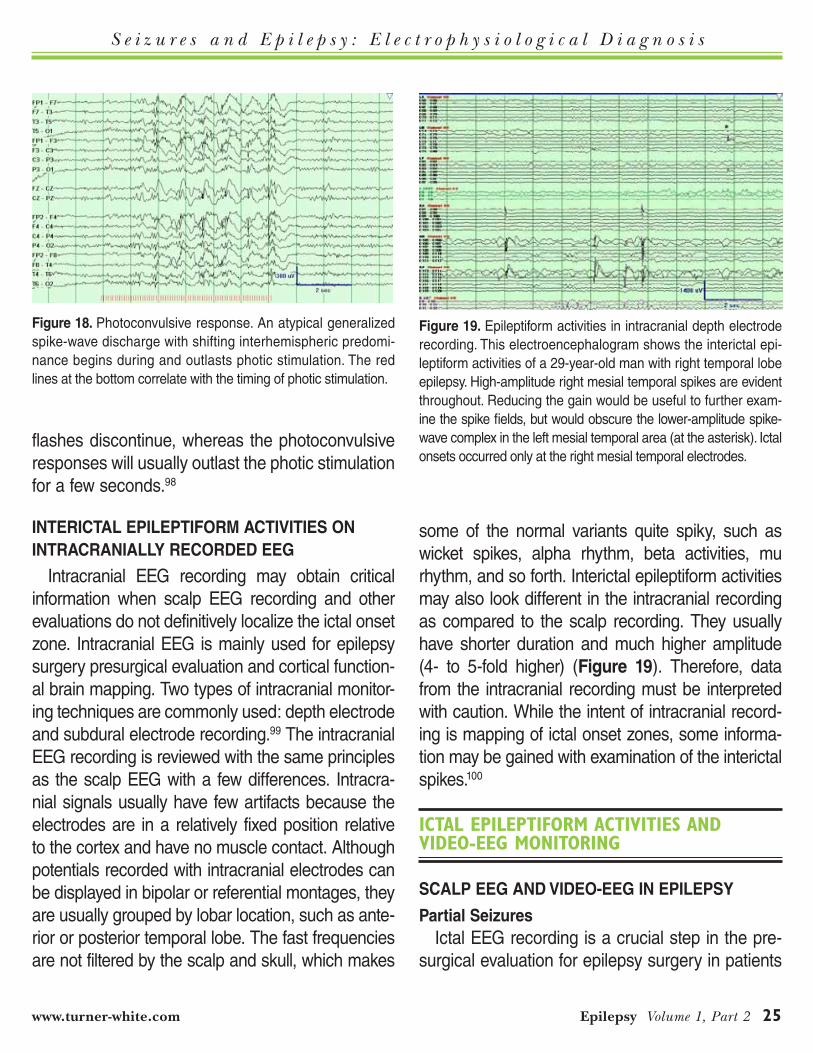
some of the normal variants quite spiky, such as wicket spikes, alpha rhythm, beta activities, mu rhythm, and so forth. Interictal epileptiform activities may also look different in the intracranial recording as compared to the scalp recording. They usually have shorter duration and much higher amplitude (4- to 5-fold higher) (Figure 19). Therefore, data from the intracranial recording must be interpreted with caution. While the intent of intracranial record-ing is mapping of ictal onset zones, some informa-tion may be gained with examination of the interictal spikes.100
ictal ePilePtiform activitieS and video-eeG monitorinG
scalp EEg and vidEo-EEg in EpilEpsy
partial seizures Ictal EEG recording is a crucial step in the pre-
surgical evaluation for epilepsy surgery in patients
Figure 19. Epileptiform activities in intracranial depth electrode recording. This electroencephalogram shows the interictal epi-leptiform activities of a 29-year-old man with right temporal lobe epilepsy. High-amplitude right mesial temporal spikes are evident throughout. Reducing the gain would be useful to further exam-ine the spike fields, but would obscure the lower-amplitude spike-wave complex in the left mesial temporal area (at the asterisk). Ictal onsets occurred only at the right mesial temporal electrodes.
Figure 18. Photoconvulsive response. An atypical generalized spike-wave discharge with shifting interhemispheric predomi-nance begins during and outlasts photic stimulation. The red lines at the bottom correlate with the timing of photic stimulation.
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
26 Hospital physician Board Review Manual www.turner-white.com
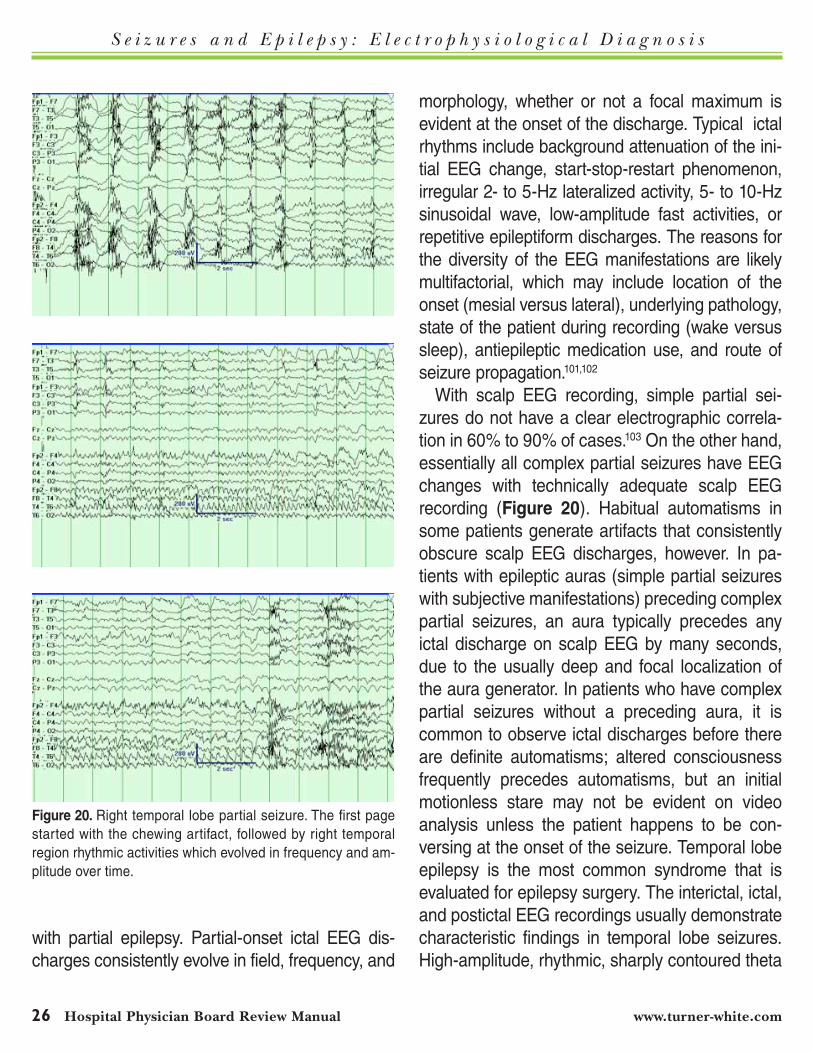
with partial epilepsy. Partial-onset ictal EEG dis-charges consistently evolve in field, frequency, and
morphology, whether or not a focal maximum is evident at the onset of the discharge. Typical ictal rhythms include background attenuation of the ini-tial EEG change, start-stop-restart phenomenon, irregular 2- to 5-Hz lateralized activity, 5- to 10-Hz sinusoidal wave, low-amplitude fast activities, or repetitive epileptiform discharges. The reasons for the diversity of the EEG manifestations are likely multifactorial, which may include location of the onset (mesial versus lateral), underlying pathology, state of the patient during recording (wake versus sleep), antiepileptic medication use, and route of seizure propagation.101,102
With scalp EEG recording, simple partial sei-zures do not have a clear electrographic correla-tion in 60% to 90% of cases.103 On the other hand, essentially all complex partial seizures have EEG changes with technically adequate scalp EEG recording (Figure 20). Habitual automatisms in some patients generate artifacts that consistently obscure scalp EEG discharges, however. In pa-tients with epileptic auras (simple partial seizures with subjective manifestations) preceding complex partial seizures, an aura typically precedes any ictal discharge on scalp EEG by many seconds, due to the usually deep and focal localization of the aura generator. In patients who have complex partial seizures without a preceding aura, it is common to observe ictal discharges before there are definite automatisms; altered consciousness frequently precedes automatisms, but an initial motionless stare may not be evident on video analysis unless the patient happens to be con-versing at the onset of the seizure. Temporal lobe epilepsy is the most common syndrome that is evaluated for epilepsy surgery. The interictal, ictal, and postictal EEG recordings usually demonstrate characteristic findings in temporal lobe seizures. High-amplitude, rhythmic, sharply contoured theta
Figure 20. Right temporal lobe partial seizure. The first page started with the chewing artifact, followed by right temporal region rhythmic activities which evolved in frequency and am-plitude over time.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 27
activities of 5 Hz or faster are a hallmark of com-plex partial seizures in mesial temporal lobe epilepsy. This pattern usually occurs only dur-ing a portion of the electrographic seizure, and it may be preceded by focal temporal-maximum discharges of other frequencies and morpholo-gies that evolve into the focal theta discharges, or by nonlocalized rhythmic discharges that later evolve into the focal theta discharges.12 Up to 80% of patients who have complex partial seizures of mesial temporal onset will have this focal theta pattern during some or most of their complex partial seizures. Importantly, this focal temporal-maximum theta pattern on scalp EEG also can occur with seizures which begin in the limbic system outside of the mesial temporal structures (such as the insula) or in ipsilateral temporal lobe neocortex as shown by concurrent intracranial recording, when the ictal discharges propagate into mesial temporal structures during the com-plex partial phase of the seizure.21 Figure 20 shows the onset and evolution of a right temporal lobe onset seizure, which has mild attenuation of the background activities at the onset and evolves to 6- to 7-Hz sinusoidal activities. Frontal lobe sei-zures are also commonly encountered in epilepsy surgical evaluation. However, frontal lobe seizures often do not have a clear EEG correlate due to artifacts in complex partial seizures, making this a significant challenge for clinicians in presurgical evaluation.104 Occipital- and parietal-onset seizures are less common than temporal lobe seizures, and may be simple partial seizures, complex par-tial, or secondarily generalized seizures, usually with clear localization on scalp EEG for diagnosis, although intracranial recordings are necessary for surgical planning.105 They may begin with visual phenomenon and progress into a generalized ton-ic-clonic seizure. Headaches may occur during or
after the seizures.106 Overall there is a greater ten-dency for seizures of mesial frontal and mesial oc-cipital origin to be falsely lateralized on scalp EEG, as compared with intracranial recordings in the same individuals whose seizures were previously or simultaneously recorded with scalp EEG.107
generalized seizuresGeneralized seizures involve both cerebral hemi-
spheres, with ictal discharges of various forms of generalized spike-wave or GPFA patterns from onset when the EEG is not obscured by artifacts. Generalized seizures can be divided into general-ized tonic-clonic, tonic, atonic, clonic, myoclonic, and absence seizures. Generalized seizures usu-ally are associated with EEG changes with scalp EEG recording. In particular, generalized tonic-clonic seizures are almost always associated with EEG changes; although the ictal onset and ictal discharges can be entirely obscured by myogenic-kinesigenic artifacts, the postictal depression is nearly always evident as postictal generalized attenuation followed by increasing amplitudes of generalized slowing with gradual return to the inter-ictal baseline. Significant myogenic artifact usually makes them difficult to interpret. In a secondarily generalized seizure, a focal onset often is seen at the beginning of the seizure, if the background is not obscured by artifacts. However, the focal onset may not be obvious if there is rapid spread (rapid secondary bilateral synchrony).82,108 Simple staring spells can be seen with absence seizures, but also with complex partial seizures and psychogenic events, so video analysis requires simultaneous EEG analysis. On the other hand, the ictal be-haviors of a generalized tonic-clonic seizure are generally so distinct from those of a psychogenic convulsion that the video analysis in itself provides considerable diagnostic significance.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
28 Hospital physician Board Review Manual www.turner-white.com
nonconvulsive status Epilepticus and other status Epilepticus
Nonconvulsive status epilepticus (NCSE) is an important entity for clinicians to recognize. Record-ing EEG is necessary to confirm a diagnosis of suspected NCSE, and in some cases a “bland,” nonfluctuating encephalopathy is surprisingly found to be caused by NCSE.109 Altered behaviors dur-ing NCSE can be confused with other conditions such as episodic behaviors of dementia. The ictal discharges in NCSE may be lateralized, as often is observed in complex partial status epilepticus, or may consist of periods of GPEDs that persist or alternate with generalized slowing or less clearly epileptiform alternating patterns.109 “Spike-wave stupor” is an electroclinical observation in a con-tinuously encephalopathic patient that can arise from uncontrolled complex partial status epilepti-cus (in partial epilepsies), from absence or atypical absence status epilepticus (in generalized epilep-sies), and probably also “de novo” (in a patient who was not previously known to have epilepsy). It is often difficult to distinguish between GPEDs that occur during or after status epilepticus from those due to other causes such as severe encephalopa-thy or diffuse cerebral injury.110 Continuous video-EEG monitoring usually is quite useful in evaluat-ing therapeutic response in NCSE, and also in patients with acute repetitive seizures who are not in full-blown NCSE.
Recording of EEG is not necessary to support the clinical diagnosis of generalized convulsive status (GCSE), and waiting for EEG can com-promise patient care. The diagnosis of GCSE is almost always made by observation of the patient. Rarely, the patient arrives comatose late in the course of untreated GCSE, when muscle activa-tion during cerebral discharges has markedly diminished. The epileptologist should be aware of
the typical evaluation of EEG findings in uncon-trolled GCSE. Detailed observations of non-human GCSE111 demonstrated a progressive sequence of EEG alterations in untreated GCSE: (1) discrete seizures; (2) merging seizures with waxing and waning amplitude and frequency of EEG rhythms; (3) continuous ictal activity; (4) continuous ictal activity punctuated by low-voltage “flat periods”; and (5) periodic epileptiform discharges on a “flat” background. For a patient who arrives at the emergency department comatose, an EEG recod-ing that shows the fourth or fifth of these patterns might be suspected for late GCSE, given that the motor convulsions may be rather subtle late in GCSE. Continuous EEG monitoring can be useful in evaluating therapeutic response in such condi-tions.
scalp EEg and vidEo-EEg in nonEpilEpTic condiTions
syncope Syncope may be seen in patients of all ages.
The cause of syncope is diverse, including vaso-vagal, reflex, and orthostatic hypotension. Recur-rent syncope may mimic seizures in that patients may have a brief period of tonic-clonic movement of their limbs and body or they may have incon-tinence during the episode.112 The electrocardio-gram tilt-table test is an effective tool for diagnosis in most of these cases,113–115 but when recurring events feature unusual behaviors, combined tilt- table testing and video-EEG monitoring may better elucidate the nature of the events. During a purely hypotensive syncopal event, the EEG will demon-strate increasing generalized slowing which may progress to a brief isoelectric period if hypotension is not rapidly reversed, followed by rapid resump-tion of baseline EEG activities on cerebral reperfu-sion (Figure 21).
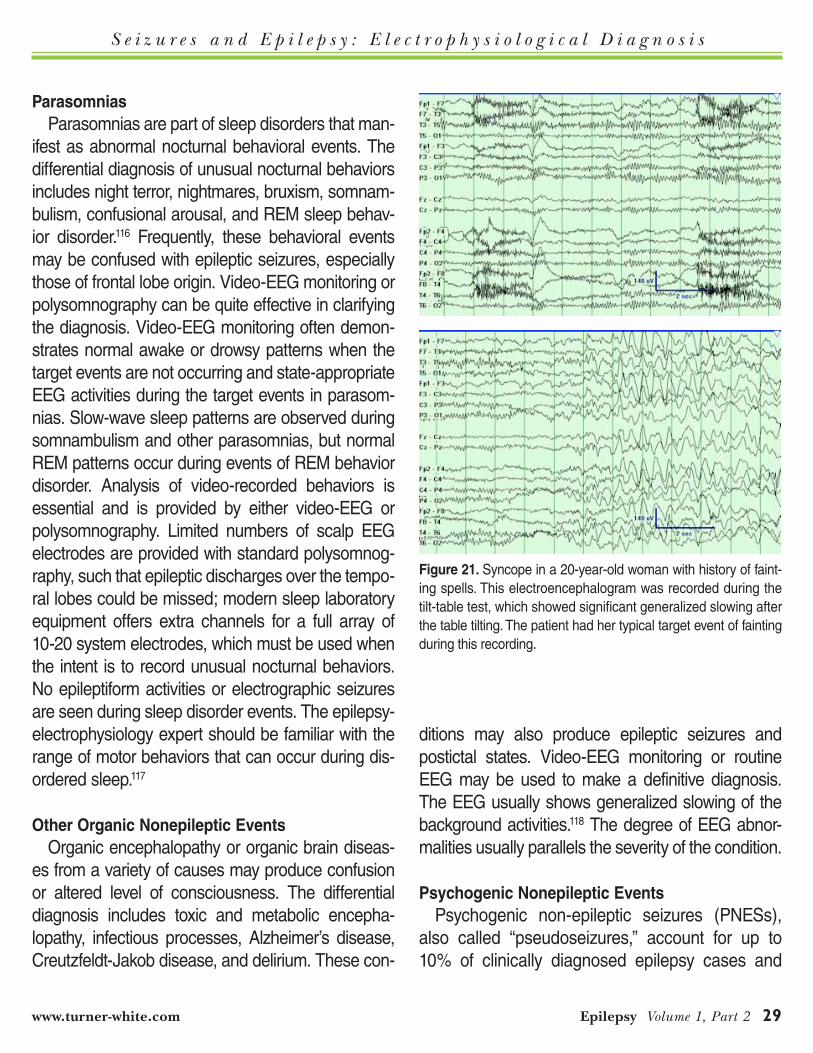
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 29
parasomnias Parasomnias are part of sleep disorders that man-
ifest as abnormal nocturnal behavioral events. The differential diagnosis of unusual nocturnal behaviors includes night terror, nightmares, bruxism, somnam-bulism, confusional arousal, and REM sleep behav-ior disorder.116 Frequently, these behavioral events may be confused with epileptic seizures, especially those of frontal lobe origin. Video-EEG monitoring or polysomnography can be quite effective in clarifying the diagnosis. Video-EEG monitoring often demon-strates normal awake or drowsy patterns when the target events are not occurring and state-appropriate EEG activities during the target events in parasom-nias. Slow-wave sleep patterns are observed during somnambulism and other parasomnias, but normal REM patterns occur during events of REM behavior disorder. Analysis of video-recorded behaviors is essential and is provided by either video-EEG or polysomnography. Limited numbers of scalp EEG electrodes are provided with standard polysomnog-raphy, such that epileptic discharges over the tempo-ral lobes could be missed; modern sleep laboratory equipment offers extra channels for a full array of 10-20 system electrodes, which must be used when the intent is to record unusual nocturnal behaviors. No epileptiform activities or electrographic seizures are seen during sleep disorder events. The epilepsy-electrophysiology expert should be familiar with the range of motor behaviors that can occur during dis-ordered sleep.117
other organic nonepileptic Events Organic encephalopathy or organic brain diseas-
es from a variety of causes may produce confusion or altered level of consciousness. The differential diagnosis includes toxic and metabolic encepha-lopathy, infectious processes, Alzheimer’s disease, Creutzfeldt-Jakob disease, and delirium. These con-
ditions may also produce epileptic seizures and postictal states. Video-EEG monitoring or routine EEG may be used to make a definitive diagnosis. The EEG usually shows generalized slowing of the background activities.118 The degree of EEG abnor-malities usually parallels the severity of the condition.
psychogenic nonepileptic Events Psychogenic non-epileptic seizures (PNESs),
also called “pseudoseizures,” account for up to 10% of clinically diagnosed epilepsy cases and
Figure 21. Syncope in a 20-year-old woman with history of faint-ing spells. This electroencephalogram was recorded during the tilt-table test, which showed significant generalized slowing after the table tilting. The patient had her typical target event of fainting during this recording.
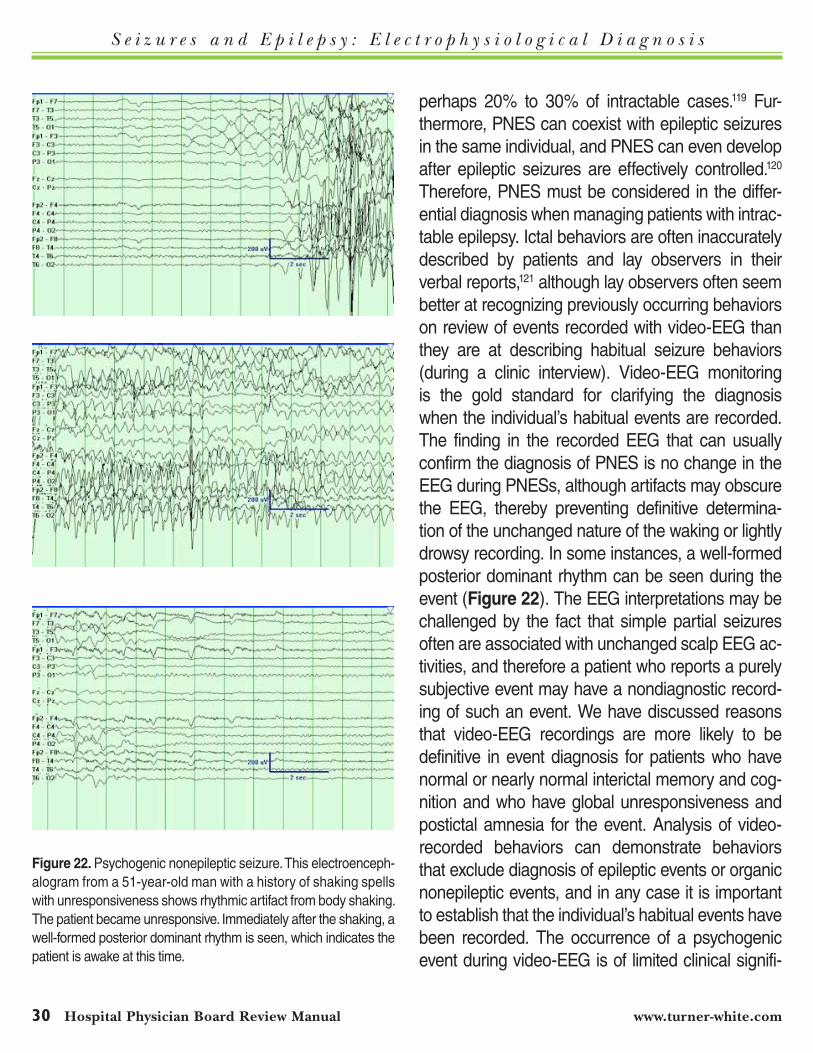
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
30 Hospital physician Board Review Manual www.turner-white.com
perhaps 20% to 30% of intractable cases.119 Fur-thermore, PNES can coexist with epileptic seizures in the same individual, and PNES can even develop after epileptic seizures are effectively controlled.120 Therefore, PNES must be considered in the differ-ential diagnosis when managing patients with intrac-table epilepsy. Ictal behaviors are often inaccurately described by patients and lay observers in their verbal reports,121 although lay observers often seem better at recognizing previously occurring behaviors on review of events recorded with video-EEG than they are at describing habitual seizure behaviors (during a clinic interview). Video-EEG monitoring is the gold standard for clarifying the diagnosis when the individual’s habitual events are recorded. The finding in the recorded EEG that can usually confirm the diagnosis of PNES is no change in the EEG during PNESs, although artifacts may obscure the EEG, thereby preventing definitive determina-tion of the unchanged nature of the waking or lightly drowsy recording. In some instances, a well-formed posterior dominant rhythm can be seen during the event (Figure 22). The EEG interpretations may be challenged by the fact that simple partial seizures often are associated with unchanged scalp EEG ac-tivities, and therefore a patient who reports a purely subjective event may have a nondiagnostic record-ing of such an event. We have discussed reasons that video-EEG recordings are more likely to be definitive in event diagnosis for patients who have normal or nearly normal interictal memory and cog-nition and who have global unresponsiveness and postictal amnesia for the event. Analysis of video- recorded behaviors can demonstrate behaviors that exclude diagnosis of epileptic events or organic nonepileptic events, and in any case it is important to establish that the individual’s habitual events have been recorded. The occurrence of a psychogenic event during video-EEG is of limited clinical signifi-
Figure 22. Psychogenic nonepileptic seizure. This electroenceph-alogram from a 51-year-old man with a history of shaking spells with unresponsiveness shows rhythmic artifact from body shaking. The patient became unresponsive. Immediately after the shaking, a well-formed posterior dominant rhythm is seen, which indicates the patient is awake at this time.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 31
cance if the individual has never had such an event previously.
pseudo-pseudoseizures As mentioned above, video-EEG is very useful
in diagnosing psychogenic events, with waking or lightly drowsy EEG activities that usually are nor-mal (or unchanged from baseline) during a period of global unresponsiveness for which the patient subsequently is amnesic. Clinicians should be aware that there are a number of conditions that can be misdiagnosed with pseudoseizures. These conditions include parasomnias, syncope, parox-ysmal dyskinesia, and epileptic seizures, in partic-ular, those of frontal lobe origin. Many frontal lobe seizures have lower-amplitude ictal discharges than do complex partial seizures of temporal lobe origin, and frontal lobe seizures often are associ-ated with vigorous and sometimes quite bizarre automatisms. When myogenic and kinesigenic artifacts significantly obscure EEG activities, no as-sumptions should be made about the nature of the obscured EEG; an ictal discharge may have been obscured. Other conditions, such as N-methyl-D-aspartate receptor autoimmune encephalitis, can present with a number of neuropsychiatric symptoms, such as episodic posturing and rhyth-mic movements.122 The absence of epileptiform activities on scalp EEG is a diagnostically useful observation when it occurs during a paroxysmal event with global impairment of consciousness (or of responsiveness-memory) and when the EEG is technically adequate (including relative absence of artifactual obscuration).
icTal rEcordings wiTh inTracranial EEg in EpilEpsy
Information obtained from EEG recorded with scalp electrodes may be insufficient in settings such
as presurgical evaluation for epilepsy. Intracranial recording may provide critical information for the accurate localization of the epileptogenic zone.21,99 Depth electrodes and subdural electrodes are the most common intracranial electrodes used in clini-cal practice. Different types of electrodes are select-ed based on the questions being posed in an intra-cranial recording. All of the EEG rhythms observed in the scalp EEG recording can be seen in the intracranial recording if the electrodes are placed in the appropriate location. The volume of cortex that produces interictal spikes has been termed the “irritative zone,” and in many individuals this is a considerably larger volume than the “ictal onset zone” where earliest ictal discharges are recorded with intracranial electrodes. Intracranial recording of seizures differs significantly from scalp EEG. In scalp EEG recording, seizures can be observed in EEG only after they have spread to adjacent areas, and a 6 cm2 area of cortex must be involved in the scalp EEG recording before changes can be observed. In intracranial recording, seizure onset can be observed in a very small region before the seizures spread (Figure 23). Hippocampal seizures can start with a different pattern such as repetitive spikes, theta to alpha activities, or high-frequency beta activities. Neocortical seizures usually start with high-frequency, low-amplitude beta activities.123,124
BeniGn eeG variantS and artifactS tHat can Simulate interictal and ictal ePilePtiform activitieS
arTiFacTs
One of the common pitfalls in EEG interpretation is to mistakenly identify artifacts as epileptiform ac-tivities or other abnormalities. Artifacts are signals that are mechanical or biological, but are noncere-bral in origin. Artifacts can be classified as physi-
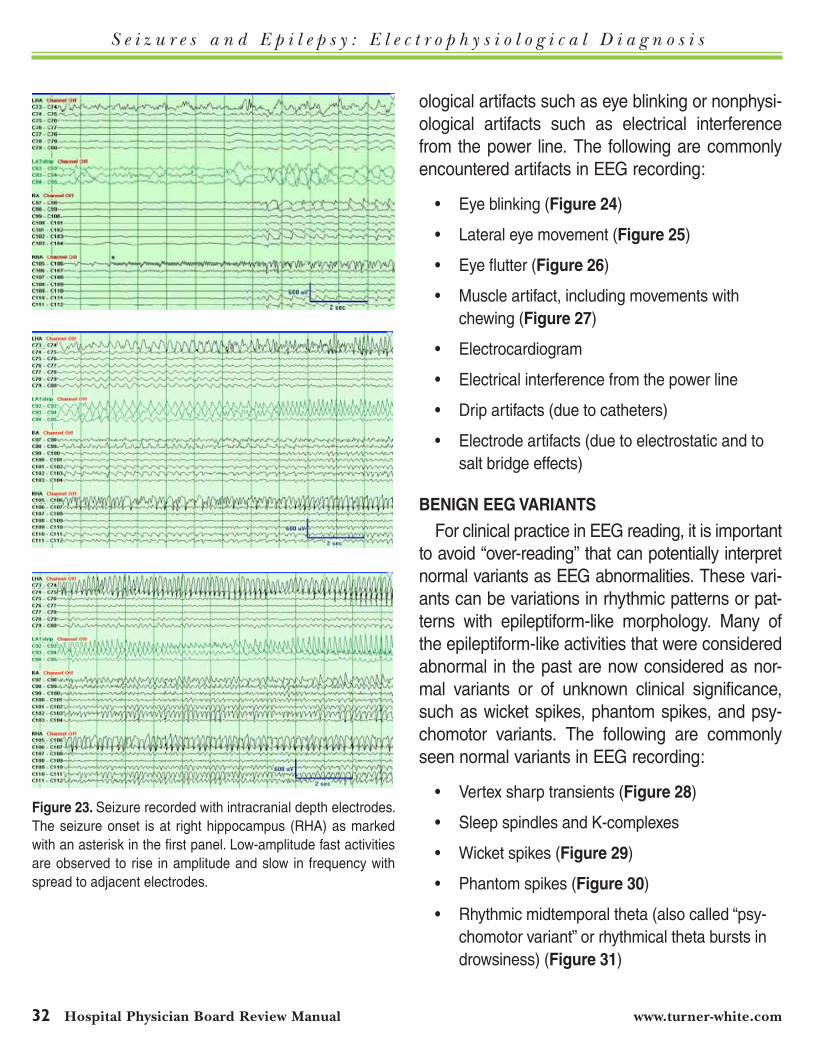
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
32 Hospital physician Board Review Manual www.turner-white.com
ological artifacts such as eye blinking or nonphysi-ological artifacts such as electrical interference from the power line. The following are commonly encountered artifacts in EEG recording:
• Eyeblinking(Figure 24)
• Lateraleyemovement(Figure 25)
• Eyeflutter(Figure 26)
• Muscleartifact,includingmovementswithchewing (Figure 27)
• Electrocardiogram
• Electricalinterferencefromthepowerline
• Dripartifacts(duetocatheters)
• Electrodeartifacts(duetoelectrostaticandtosalt bridge effects)
BEnign EEg varianTs
For clinical practice in EEG reading, it is important to avoid “over-reading” that can potentially interpret normal variants as EEG abnormalities. These vari-ants can be variations in rhythmic patterns or pat-terns with epileptiform-like morphology. Many of the epileptiform-like activities that were considered abnormal in the past are now considered as nor-mal variants or of unknown clinical significance, such as wicket spikes, phantom spikes, and psy-chomotor variants. The following are commonly seen normal variants in EEG recording:
• Vertexsharptransients(Figure 28)
• SleepspindlesandK-complexes
• Wicketspikes(Figure 29)
• Phantomspikes(Figure 30)
• Rhythmicmidtemporaltheta(alsocalled“psy-chomotor variant” or rhythmical theta bursts in drowsiness) (Figure 31)
Figure 23. Seizure recorded with intracranial depth electrodes. The seizure onset is at right hippocampus (RHA) as marked with an asterisk in the first panel. Low-amplitude fast activities are observed to rise in amplitude and slow in frequency with spread to adjacent electrodes.
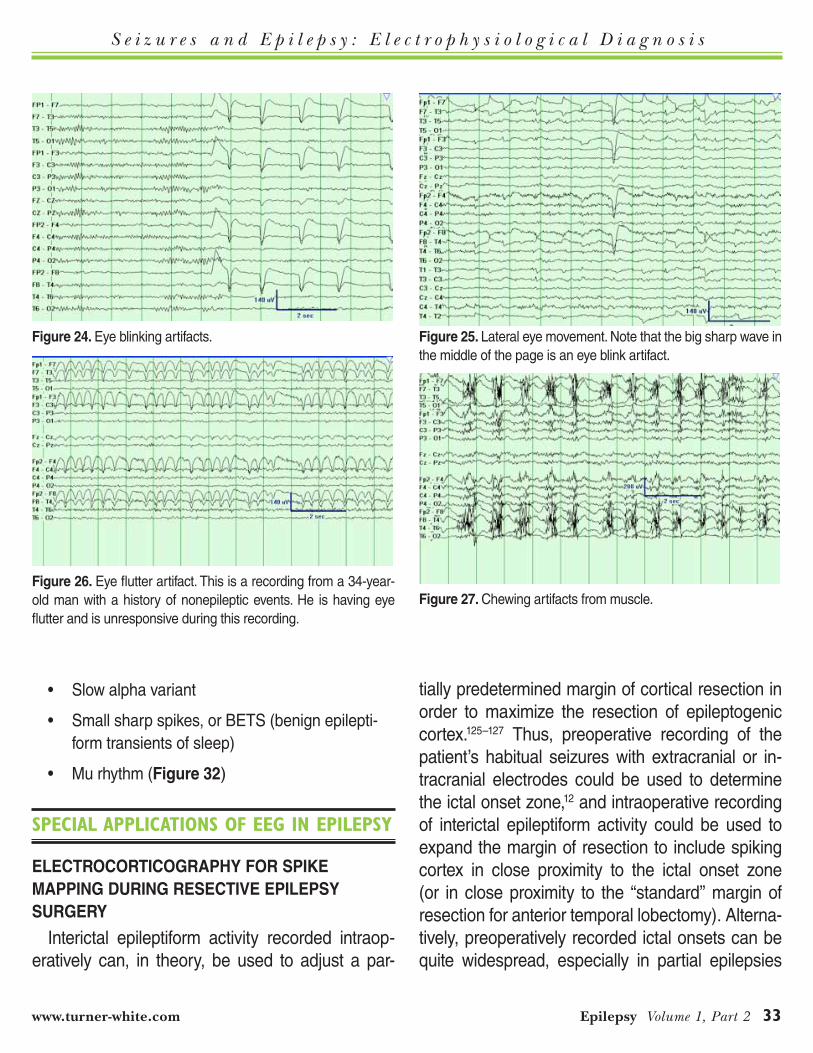
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 33
• Slowalphavariant
• Smallsharpspikes,orBETS(benignepilepti-form transients of sleep)
• Murhythm(Figure 32)
SPecial aPPlicationS of eeG in ePilePSy
ElEcTrocorTicography For spikE Mapping during rEsEcTivE EpilEpsy surgEry
Interictal epileptiform activity recorded intraop-eratively can, in theory, be used to adjust a par-
tially predetermined margin of cortical resection in order to maximize the resection of epileptogenic cortex.125–127 Thus, preoperative recording of the patient’s habitual seizures with extracranial or in-tracranial electrodes could be used to determine the ictal onset zone,12 and intraoperative recording of interictal epileptiform activity could be used to expand the margin of resection to include spiking cortex in close proximity to the ictal onset zone (or in close proximity to the “standard” margin of resection for anterior temporal lobectomy). Alterna-tively, preoperatively recorded ictal onsets can be quite widespread, especially in partial epilepsies
Figure 26. Eye flutter artifact. This is a recording from a 34-year-old man with a history of nonepileptic events. He is having eye flutter and is unresponsive during this recording.
Figure 27. Chewing artifacts from muscle.
Figure 24. Eye blinking artifacts. Figure 25. Lateral eye movement. Note that the big sharp wave in the middle of the page is an eye blink artifact.
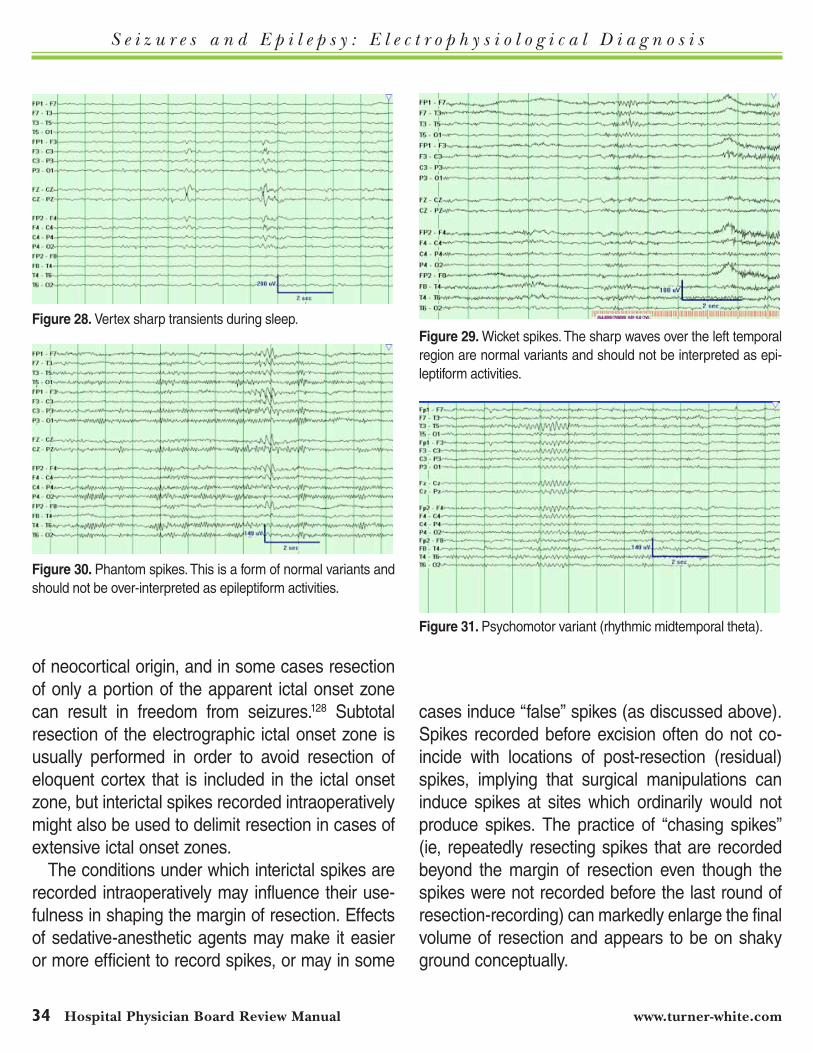
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
34 Hospital physician Board Review Manual www.turner-white.com
of neocortical origin, and in some cases resection of only a portion of the apparent ictal onset zone can result in freedom from seizures.128 Subtotal resection of the electrographic ictal onset zone is usually performed in order to avoid resection of eloquent cortex that is included in the ictal onset zone, but interictal spikes recorded intraoperatively might also be used to delimit resection in cases of extensive ictal onset zones.
The conditions under which interictal spikes are recorded intraoperatively may influence their use-fulness in shaping the margin of resection. Effects of sedative-anesthetic agents may make it easier or more efficient to record spikes, or may in some
cases induce “false” spikes (as discussed above). Spikes recorded before excision often do not co-incide with locations of post-resection (residual) spikes, implying that surgical manipulations can induce spikes at sites which ordinarily would not produce spikes. The practice of “chasing spikes” (ie, repeatedly resecting spikes that are recorded beyond the margin of resection even though the spikes were not recorded before the last round of resection-recording) can markedly enlarge the final volume of resection and appears to be on shaky ground conceptually.
Figure 30. Phantom spikes. This is a form of normal variants and should not be over-interpreted as epileptiform activities.
Figure 31. Psychomotor variant (rhythmic midtemporal theta).
Figure 28. Vertex sharp transients during sleep.Figure 29. Wicket spikes. The sharp waves over the left temporal region are normal variants and should not be interpreted as epi-leptiform activities.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 35
Surprisingly little is known about the efficacy of resecting spiking cortex that is found near the pre-planned margin of resection, perhaps because each surgeon-neurophysiologist team tends to act in a consistent fashion with regard to resecting or not resecting perimarginal spiking cortex. Some earlier investigators reported poorer seizure control in pa-tients with postresection spiking on electrocorticog-raphy129,130 or no correlation between residual spikes and seizure outcome.131,132 More recently, a group in which temporal lobectomies were tailored (adjusted in resection margins) reported that postexcisional perimarginal spiking is significantly associated with more frequent postoperative seizures, but that 47% of patients without postoperative seizures had re-sidual spikes and that 28% of patients with post-operative seizures did not have residual spikes.133
Another recent report from a center that uses stan-dard (nonadjusted) temporal lobectomy margins indicated that persistence of spiking after resection did not predict recurrent seizures in individuals, but this finding was prognostically negative across the entire group.134 Interestingly, these investigators, who recorded intraoperatively with both epicortical and intracerebral electrodes, found that absence of preresection spiking carried a worse prognosis. In planning for any form of electrocorticography, whether for spike mapping or for functional mapping with DCES, preoperative consultation with the an-esthesiologist is important to assure use of agents such as propofol that are unlikely to induce spikes or to lower the seizure threshold.135
ElEcTrocorTicography wiTh dcEs For corTical FuncTion Mapping during rEsEcTivE EpilEpsy surgEry
The primary motor cortex is located on the gyrus just anterior to the central sulcus (the precentral gyrus), but the central sulcus is frequently difficult
or impossible to reliably localize based on pre-operative MRI or intraoperative visual inspection. In some instances, there is no functional primary motor cortex on the precentral gyrus due to early or late preoperative cerebral insult or less often due to apparent localization of primary motor cor-tex outside of an identifiable precentral gyrus. For these reasons, DCES is one of several techniques that are essential to localize this functional area. Application of 2 to 4 milliamperes of current to pri-mary motor cortex typically induces clonic or tonic activity of the contralateral face or limb subserved by the particular portion of primary motor cortex. While some motor cortex areas also have sensory func-tion, sequential lowering of stimulation amplitude can usually distinguish primary motor from primary somatosensory cortex (based on the function that persists at the lowest symptomatic level of stimula-tion). Negative motor responses are brief losses of postural tone or brief interferences with volitional motor activity that occur during and are limited to the period of DCES.136 Negative motor responses are characteristic of widespread areas of frontal and extrafrontal cortex that are not in the primary motor
Figure 32. Mu rhythm. This could be abolished by moving the con-tralateral fingers, or even by thinking about the movement.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
36 Hospital physician Board Review Manual www.turner-white.com
cortex. Negative motor responses are often elicited at higher thresholds of stimulation intensity than are the tonic or clonic responses to stimulation over the motor strip.
Electrocorticographic recording of somatosen-sory evoked potentials (SSEPs) has also been used to localize the primary motor cortex. Multiple recording electrodes placed transversely across the suspected central sulcus typically will record cortical near-field potentials during upper or lower extremity sensory stimulation of the usual varieties used for SSEPs.37 The components N1 and P2 are highly restricted in distribution on electrocorticography (unlike their widespread scalp EEG distribution). The N1 and P2 components show phase reversal across the central sulcus when recorded with an-teroposteriorly aligned recording electrodes. Thus, the gyrus immediately anterior to the phase reversal is the precentral gyrus, which should contain pri-mary motor cortex.137 Movement-related potentials, including Bereitschaftspotentials and other premo-tor potentials, can also be recorded electrocorti-cographically in waking patients,138,139 but this ob-servation has yet to be exploited clinically. A major advantage of both DCES and SSEPs for mapping of motor cortex is that either can be performed while the patient is under general anesthesia.
Efforts to characterize typical responses of the supplementary motor area to DCES have yielded somewhat variable results.130,140,141 In particular, classic observations of bilateral tonic posturing induced by unilateral supplementary motor area stimulation may in fact occur less commonly than do exclusively contralateral movements.140 Re-cording of movement-related potentials while the patient is awake may help to further define the supplementary motor area.138
The major purpose of motor mapping is to define the hand area of the primary motor cortex, be-
cause resection of this cortex in a patient who has normal motor function preoperatively will result in irreversible loss of fine finger control.142 Other areas of the primary motor cortex have been resected without irreversible motor control deficits in some cases.127 Similarly, supplementary motor cortex and less specific motor-related cortex (areas at which negative motor responses are obtained) are routinely resected. In some cases it may be useful to localize these areas for purposes of obtaining agreement with ictal semiology in order to respect the apparent epileptogenic zone, as for example, in the typical supplementary motor area seizures.
Primary somatosensory cortex is normally lo-cated over the postcentral gyrus, with a general to-pography that often is similar to but rarely identical with that of the classic sensory “homunculus” (see Figure 33); the same is also true of the primary motor cortex and its “homunculus.”142 Mapping is quite similar to that performed for localization of primary motor cortex, with relatively low thresh-olds of 2 to 4 milliamperes for obtaining sensory responses. The patient typically reports some sort of simple sensation over the face or extremity contralateral to the area of localized stimulation. Because of potential suggestibility, some neuro-physiologists prefer to apply placebo stimulations to demonstrate absence of any suspect reports in the particular individual. Electrocorticographic SSEPs can also be used to localize the primary sensory cortex on the same basis described above for motor mapping.143
Penfield and Roberts144 first developed DCES for identification of language cortex based on the consistent observation that patients who were performing continuous naming tasks could have arrest of speech or other interference with nam-ing during passage of current at a limited number of cortical sites. Interference with naming can

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 37
occur at sites other than the classic Broca’s and Wernicke’s areas, and it is possible that naming is the best screening task for any localized areas of language-committed cortex. A variety of other tasks have been used for induction of errors by DCES as the basis of language mapping, includ-ing reading aloud, repetition, and comprehen-sion of verbal or written material.49 When testing language function by DCES, it is important to repeat stimulations for consistency, since greater attention is required for most language processing than for mapping with sensory or motor tasks, and patients are frequently in mild or moderate dis-comfort during waking mapping. It is also impor-tant to exclude simple motor or sensory effects of
stimulation, particularly during frontal lobe stimula-tion, by having the subject perform such tasks as repetitive alternating tongue movements that may be interfered with during stimulation (by positive or negative motor responses) even when no lan-guage processing is occurring. The thresholds at which language and other cognitive phenomena can be elicited by DCES may be as low as those associated with phenomena at primary motor and primary sensory cortex, but thresholds are usually much higher. It is important to attempt to stimulate up to 15 milliamperes before concluding that no detectable language function is represented in the area tested; at times adequate testing may be pre-vented by low afterdischarge thresholds that are
Figure 33. The motor and sensory homunculi. These “grand summary” pre- and postcentral gyrus (coronal) brain schemata of direct cortical electrical stimulation mapping were produced from hundreds of operative procedures performed over many years by Wilder Penfield and his colleagues. These summaries are concordant with preceding stimulation and ablative experiments in animal studies. Individual patients may have motosensory (precentral) and sensorimotor (postcentral) maps that deviate considerably in location from these grand summaries. For this reason, mapping of eloquent motor and sensory cortex remains a clinically useful technique. (Reprinted from Penfield W, Rasmussen T. The cerebral cortex of man: a clinical study of localization of function. New York: Macmillan; 1950.)
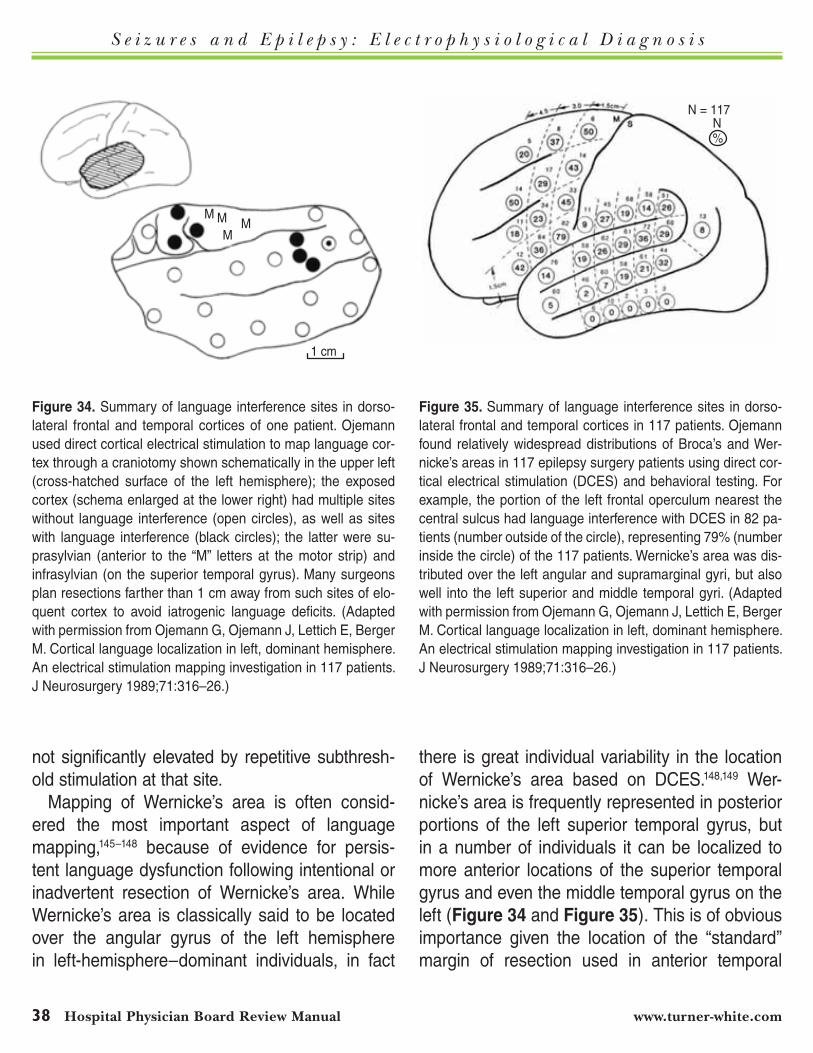
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
38 Hospital physician Board Review Manual www.turner-white.com
not significantly elevated by repetitive subthresh-old stimulation at that site.
Mapping of Wernicke’s area is often consid-ered the most important aspect of language mapping,145–148 because of evidence for persis-tent language dysfunction following intentional or inadvertent resection of Wernicke’s area. While Wernicke’s area is classically said to be located over the angular gyrus of the left hemisphere in left-hemisphere–dominant individuals, in fact
there is great individual variability in the location of Wernicke’s area based on DCES.148,149 Wer-nicke’s area is frequently represented in posterior portions of the left superior temporal gyrus, but in a number of individuals it can be localized to more anterior locations of the superior temporal gyrus and even the middle temporal gyrus on the left (Figure 34 and Figure 35). This is of obvious importance given the location of the “standard” margin of resection used in anterior temporal
Figure 34. Summary of language interference sites in dorso-lateral frontal and temporal cortices of one patient. Ojemann used direct cortical electrical stimulation to map language cor-tex through a craniotomy shown schematically in the upper left (cross-hatched surface of the left hemisphere); the exposed cortex (schema enlarged at the lower right) had multiple sites without language interference (open circles), as well as sites with language interference (black circles); the latter were su-prasylvian (anterior to the “M” letters at the motor strip) and infrasylvian (on the superior temporal gyrus). Many surgeons plan resections farther than 1 cm away from such sites of elo-quent cortex to avoid iatrogenic language deficits. (Adapted with permission from Ojemann G, Ojemann J, Lettich E, Berger M. Cortical language localization in left, dominant hemisphere. An electrical stimulation mapping investigation in 117 patients. J Neurosurgery 1989;71:316–26.)
Figure 35. Summary of language interference sites in dorso-lateral frontal and temporal cortices in 117 patients. Ojemann found relatively widespread distributions of Broca’s and Wer-nicke’s areas in 117 epilepsy surgery patients using direct cor-tical electrical stimulation (DCES) and behavioral testing. For example, the portion of the left frontal operculum nearest the central sulcus had language interference with DCES in 82 pa-tients (number outside of the circle), representing 79% (number inside the circle) of the 117 patients. Wernicke’s area was dis-tributed over the left angular and supramarginal gyri, but also well into the left superior and middle temporal gyri. (Adapted with permission from Ojemann G, Ojemann J, Lettich E, Berger M. Cortical language localization in left, dominant hemisphere. An electrical stimulation mapping investigation in 117 patients. J Neurosurgery 1989;71:316–26.)
1 cm
M MM
M
N = 117N%

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 39
lobectomies,150 which varies among surgeons but can be further adjusted based on preoperative or intraoperative findings of language mapping. Ojemann and Dodrill151 found that if the margin of resection for left anterior temporal lobectomy fell within 2 cm of a site associated with replicable naming or speech arrest errors during continuous naming performance, a standard aphasia bat-tery demonstrated increased errors 1 month postoperatively, while resections more than 2 cm distant were not associated with any postopera-tive changes on the aphasia battery. No effect of resection volume, preoperative language per-formance, or postoperative seizure control was apparent in this finding. Intraoperative language mapping in Ojemann’s series also demonstrated significant sex differences in typical localizations of Wernicke’s area, but little difference between sexes was noted in the strong tendency to have relatively small areas of language effect (2 cm2 or less).147 Others have reported more variable suc-cess in protecting language function with intraop-erative mapping of parietotemporal cortex.152,153
It is surprisingly difficult to demonstrate a Broca’s area as functionally distinct from primary motor cortex of the frontal opercular area, per-haps in part because a linguistically nonspecific finding of a negative motor response involving glossopharyngeal-laryngeal musculature will pro-duce a speech arrest indistinguishable from that associated with an anterior aphasia.154 While frontal language areas are usually not resected, it has been reported that resections including left superior frontal language areas do not induce permanent language deficits.126
The left basal temporal language area was first demonstrated by DCES155,156 and subsequently was confirmed by cerebral blood flow activation studies with PET and later with fMRI. Although
this area typically is resected and its resection is not associated with permanent language deficits according to available information, there must be some residual concern regarding the safety of re-secting this area. Patients with left temporal lobe epilepsy and left hemisphere language domi-nance frequently demonstrate naming deficits preoperatively,157 but with or without preoperative hyponomia they can demonstrate transitory, par-tially resolving, or significant permanent naming dysfunction beyond the degree of preoperative dysfunction following left temporal lobectomy.158 Since it is currently the standard of practice to resect any left fusiform gyrus and adjacent infe-rior temporal cortex which may harbor a basal temporal area, presumably it would be ethical to perform a double-blind controlled study of postop-erative language function with and without resec-tion of this area in individual’s demonstrating such an area by DCES. No report of such a study is currently available, however.
develoPinG aPPlicationS of eeG in ePilePSy
Clinical epilepsy-EEG experts must remain aware of relevant research trends in prepara-tion for new therapies and diagnostic tools. The current interest in high-frequency oscillations re-corded intracranially has been noted. Automated detection of “pre-ictal” EEG signals (Figure 36) also is an active area of epilepsy-EEG research. The potential benefits of devices and software identifying impending seizure discharges are ap-parent.159 Currently, such devices and software are not established for clinical use, but if and when they are, it is almost certain that clinical epilepsy-EEG experts will need to learn how to operate these new tools.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
40 Hospital physician Board Review Manual www.turner-white.com
referenceS
1. Henry TR. Seizures and epilepsy: pathophysiology and principles of diagnosis. Hospital Physician Epilepsy Board Review Manual. Volume 1, Part 1. July 2012.
2. Ebersole JS, Pedley TA. Current practice of clinical elec-troencephalography. 3rd ed. Philadelphia (PA): Lippincott Williams & Wilkins; 2003.
3. Schomer DL, Lopes da Silva F. Niedermeyer’s electroen-cephalography: basic principles, clinical applications, and related fields. 6th ed. Philadelphia (PA): Lippincott Williams
& Wilkins; 2011. 4. Stern JM, Engel J Jr. An atlas of EEG patterns. Philadelphia
(PA): Lippincott Williams & Wilkins; 2004. 5. Krauss GL, Fisher RS, Kaplan PW. The Johns Hopkins
atlas of digital EEG: an interactive training guide. Baltimore (MD): Johns Hopkins University Press; 2011.
6. Sperling MR, Clancy RR, eds. Atlas of electroencephalog-raphy. Amsterdam: Elsevier; 1993.
7. Gloor P. Neuronal generators and the problem of local-ization in electroencephalography: application of volume conductor theory to electroencephalography. J Clin Neuro-physiol 1985;2:327–54.
8. Steriade M, McCormick DA, Sejnowski TJ. Thalamocorti-cal oscillations in the sleeping and aroused brain. Science 1993;262:679–85.
9. Huguenard JR, McCormick DA. Thalamic synchrony and dynamic regulation of global forebrain oscillations. Trends Neurosci 2007;30:350–6.
10. Drury I, Henry TR. Ictal patterns in generalized epilepsy. J Clin Neurophysiol 1993;10:268–80.
11. Timofeev I, Steriade M. Neocortical seizures: initiation, development and cessation. Neuroscience 2004;123:299–336.
12. Risinger MW, Engel J Jr, Van Ness PC, et al. Ictal localiza-tion of temporal lobe seizures with scalp/sphenoidal record-ings. Neurology 1989;39:1288–93.
13. So N, Gloor P, Quesney LF, et al. Depth electrode investiga-tions in patients with bitemporal epileptiform abnormalities. Ann Neurol 1989;25:423–31.
14. Sperling MR, Engel J Jr. Sphenoidal electrodes. J Clin Neu-rophysiol 1986;3:67–73.
15. Sutherling WW, Barth DS. Neocortical propagation in tem-poral lobe spike foci on magnetoencephalography and elec-troencephalography. Ann Neurol 1989;25:373–81.
16. Devinsky O, Sato S, Kufta CV, et al. Electroencephalo-graphic studies of simple partial seizures with subdural electrode recordings. Neurology 1989;39:527–33.
17. Kapur J, Pillai A, Henry TR. Psychogenic elaboration of simple partial seizures. Epilepsia 1995;36:1126–30.
18. Palmini AL, Gloor P, Jones-Gotman M. Pure amnestic seizures in temporal lobe epilepsy. Definition, clinical symp-tomatology and functional anatomical considerations. Brain 1992;115:749–69.
19. Sperling MR, O’Connor MJ. Auras and subclinical seizures: characteristics and prognostic significance. Ann Neurol 1990;28:320–8.
20. Sammaritano M, Lotbiniere A, Andermann F, et al. False lat-eralization by surface EEG of seizure onset in patients with temporal lobe epilepsy and gross focal cerebral lesions. Ann Neurol 1987;21:361–9.
21. Henry TR, Ross DA, Schuh LA, Drury I. Indications and
Board rEviEw quEsTionsTest your knowledge of this topic.
Go to www.turner-white.com and select Epilepsy from the drop-down menu of specialties.
Figure 36. Automated signal processing for seizure prediction. As shown in this schematic figure, qualitatively evident interictal EEG activities (during Observation) may change before onset of an electroclinical seizure (during Prediction), possibly permitting an acute abortive intervention such as deep brain stimulation before the seizure itself. Before ictal onset is qualitatively evident on intra-cranial electroencephalography data, a pre-ictal period of signal alteration may differ from other interictal observation periods, al-lowing for automated detection of a high probability of subsequent seizure onset. This pre-ictal signal alteration may or may not be qualitatively evident, but must differ quantitatively from preced-ing interictal observation periods to support automated detection. (Adapted with permission from Litt B, Echauz J. Prediction of epi-leptic seizures. Lancet Neurology 2002;1:22–30.)
Observation Prediction Seizure
AB
C D
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 41
outcome of ictal recording with intracerebral and subdural electrodes in refractory complex partial seizures. J Clin Neurophysiol 1999;16:426–38.
22. Pillai J, Sperling MR. Interictal EEG and the diagnosis of epilepsy. Epilepsia 2006;47(suppl 1):14–22.
23. Silverman D. The anterior temporal electrode and the ten-twenty system. Electroencephalogr Clin Neurophysiol 1960;12:735–7.
24. Mintzer S, Nicholl JS, Stern JM, Engel J. Relative utility of sphenoidal and temporal surface electrodes for localization of ictal onset in temporal lobe epilepsy. Clin Neurophysiol 2002;113:911–6.
25. Pastor J, Sola RG, Hernando-Requejo V, et al. Morbidity as-sociated with the use of foramen ovale electrodes. Epilepsia 2008;49:464–9.
26. Ross DA, Henry TR, Dickinson LD. A percutaneous epidural screw electrode for intracranial electroencephalographic recording. Neurosurgery 1993;33:332–4.
27. Drury I, Schuh L, Ross D, et al. Ictal patterns in temporal lobe epilepsy recorded by epidural screw electrodes. Elec-troencephalogr Clin Neurophysiol 1997;102:167–74.
28. Ross DA, Drury I, Brunberg JA, Henry TR. Intracerebral depth electrode monitoring in partial epilepsy: the mor-bidity and efficacy of placement using magnetic reso-nance imaging-guided stereotaxic surgery. Neurosurgery 1996;39:327–34.
29. Sperling MR, O’Connor MJ. Comparison of depth and subdural electrodes in recording temporal lobe seizures. Neurology 1989;39:1497–504.
30. Bragin A, Engel J Jr, Wilson CL, et al. Hippocampal and entorhinal cortex high-frequency oscillations (100--500 Hz) in human epileptic brain and in kainic acid--treated rats with chronic seizures. Epilepsia 1999;402:127–37.
31. Engel J Jr, Bragin A, Staba R, Mody I. High-frequency oscillations: what is normal and what is not? Epilepsia 2009;50:598–604.
32. Worrell GA, Gardner AB, Stead SM, et al. High-frequen-cy oscillations in human temporal lobe: simultaneous microwire and clinical macroelectrode recordings. Brain 2008;131(Pt 4):928–37.
33. Zijlmans M, Jiruska P, Zelmann R, et al. High-frequency oscillations as a new biomarker in epilepsy. Ann Neurol 2012;71:169–78.
34. Sato S, Balish M, Muratore R. Principles of magnetoen-cephalography. J Clin Neurophysiol 1991;8:144–56.
35. Ebersole JS, Ebersole SM. Combining MEG and EEG source modeling in epilepsy evaluations. J Clin Neuro-physiol 2010;27:360–71.
36. Knowlton RC, Elgavish RA, Limdi N, et al. Functional im-aging: I. Relative predictive value of intracranial electroen-cephalography. Ann Neurol 2008;64:25–34.
37. Nuwer MR. Evoked potential monitoring in the operating room. New York: Raven Press; 1987.
38. Galloway GM, Nuwer MR, Lopez JR, Zamel KM. Intraop-erative neurophysiolgic monitoring. London: Cambrdge University Press; 2010.
39. Gotman J. Automatic seizure detection: improvements and evaluation. Electroencephalograph Clin Neurophysiol 1990;76:317–24.
40. Anderson NR, Doolittle LM. Automated analysis of EEG: op-portunities and pitfalls. J Clin Neurophysiol 2010;27:453–7.
41. Stern JM. Simultaneous electroencephalography and func-tional magnetic resonance imaging applied to epilepsy. Epilepsy Behav 2006;8:683–92.
42. Gotman J. Epileptic networks studied with EEG-fMRI. Epi-lepsia 2008;49 Suppl 3:42–51.
43. Wieser HG, Bancaud J, Talairach J, et al. Comparative value of spontaneous and chemically and electrically in-duced seizures in establishing the lateralization of temporal lobe seizures. Epilepsia 1979;20:47–59.
44. Henry TR, Ezzeddine MA. Approach to the patient with transient alteration of consciousness. Neurology: Clin Pract 2. In press, 2012.
45. Devinsky O, Gazzola D, LaFrance WC. Differentiating between nonepileptic and epileptic seizures. Nature Rev Neurosci 2011;7:210–20.
46. Blum DE, Eskola J, Bortz JJ, Fisher RS. Patient awareness of seizures. Neurology 1996;47:260–4.
47. Drury I, Selwa LM, Schuh LA, et al. Value of inpatient di-agnostic CCTV-EEG monitoring in the elderly. Epilepsia 1999;40:1100–2.
48. Gordon B, Lesser RP, Rance NE, et al. Parameters for di-rect cortical electrical stimulation in the human: histopatho-logic confirmation. Electroencephalogr Clin Neurophysiol 1990;75:371–7.
49. Ojemann GA, Sutherling WW, Lesser RP, et al. Cortical stimulation. In: Engel J Jr, ed. Surgical treatment of the epilepsies. 2nd ed. New York: Raven Press; 1993:399–414.
50. Cherlow DG, Dymond AM, Crandall PH, et al. Evoked re-sponse and afterdischarge thresholds to electrical stimula-tion in temporal lobe epileptics. Arch Neurol 1977;34:527–31.
51. Lesser RP, Luders H, Klem G, et al. Cortical afterdischarge and functional response thresholds: results of extraopera-tive testing. Epilepsia 1984;25:615–21.
52. Sharbrough FW. Commentary: extracranial EEG monitor-ing. In: Engel J Jr, ed. Surgical treatment of the epilepsies. New York: Raven Press; 1987:167–171.
53. Reiher J, Klass DW. "Small sharp spikes" (SSS): electro-encephalographic characteristics and clinical significance. Electroencephalogr Clin Neurophysiol 1970;28:94.
54. White JC, Langston JW, Pedley TA. Benign epileptiform
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
42 Hospital physician Board Review Manual www.turner-white.com
transients of sleep: clarification of the small sharp spike controversy. Neurology 1977;27:1061–8.
55. Henry TR, Drury I. Ictal behaviors during nonepileptic sei-zures differ in patients with temporal lobe interictal epilepti-form EEG activity and patients without interictal epileptiform EEG abnormalities. Epilepsia 1998;39:175–82.
56. Henry TR, Drury I. Non-epileptic seizures in temporal lobec-tomy candidates with medically refractory seizures. Neurol-ogy 1997;48:1374–82.
57. Lombroso CT. Sylvian seizures and midtemporal spike foci in children. Arch Neurol 1967;17:52–59.
58. Beaussart M. Benign epilepsy of children with rolandic (centrotemporal) paroxysmal foci. A clinical entity. Study of 221 cases. Epilepsia 1972;13:795–811.
59. Beydoun A, Garofalo EA, Drury I. Generalized spike-waves, multiple loci, and clinical course in children with EEG fea-tures of benign epilepsy of childhood with centrotemporal spikes. Epilepsia 1992;33:1091–6.
60. Graf M, Lischka A. Topographical EEG analysis of rolandic spikes. Clin Electroenphalogr 1998;29:132–7.
61. Williamson PD, et al. Clinical characteristics of partial sei-zures. In: Engel J Jr, ed. Surgical treatment of epilepsies. New York: Raven Press; 1987:101–120.
62. Panayiotopoulos CP, Michael M, Sanders S, et al. Benign childhood focal epilepsies: assessment of established and newly recognized syndromes. Brain 2008;131(Pt 9):2264–86.
63. Panayiotopoulos CP. Panayiotopoulos syndrome: a com-mon and benign childhood epileptic syndrome. London: John Libbey & Company; 2002.
64. Dalby MA. Epilepsy and 3 per second spike and wave rhythms. Acta Neurol Scand 1969;45(suppl 40):1–180.
65. Blume WT, David RB, Gomez AR. Generalized sharp and slow wave complexes. Associated clinical features and long-term follow up. Brain 1973;96:289–306.
66. Blume WT, Kaibara M, Young GB. Atlas of adult electro-encepholography. 2nd ed. New York: Lippincott Williams & Wilkins; 2002:234.
67. Holmes GL, McKeever M, Adamson M. Absence seizures in children: clinical and electroencephalographic features. Ann Neurol 1987;21:268–73.
68. Browne TR, Dreifuss FE, Penry JK, et al. Clinical and EEG estimates of absence seizure frequency. Arch Neurol 1983;40:469–72.
69. Pedley TA. Interictal epileptiform discharges: discriminating characteristic and clinical correlations. Am J EEG Technol 1980;20:101–19
70. Janz D, Christian W. Impulsiv-Petit mal. Dtsch Z Nerven-heilkd 1957;176:348–86.
71. Asconape J, Penry JK. Some clinical and EEG aspects of be-nign juvenile myoclonic epilepsy. Epilepsia 1984;25:108–14.
72. Aliberti V, Grunewald RA, Panayiotopoulos CP, Chroni E.
Focal electroencephalographic abnormalities in juvenile myoclonic epilepsy. Epilepsia 1994;35:297–301.
73. Gastaut H, Roger J, Soulayrol R, et al. Childhood epileptic encephalopathy with diffuse slow spike-waves (otherwise known as "petit mal variant") or Lennox syndrome. Epilep-sia 1966;7:139-79.
74. Markand ON. Slow spike-wave activity in EEG and asso-ciated clinical features: often called “Lennox” or “Lennox-Gastaut” syndrome. Neurology 1977;27:746–57.
75. Blume WT, Pillay N. Electrographic and clinical correlates of secondary bilateral synchrony. Epilepsia 1985;26:636–641.
76. Berkovic SF, Andermann F, Carpenter S, Wolfe LS. Pro-gressive myoclonus epilepsies: specific causes and diag-nosis. N Engl J Med 1986;315:296–305.
77. Koskiniemi M, Toivakka E, Donner M. Progressive myoc-lonus epilepsy. Electroencephalographical findings. Acta Neurol Scand 1974;50:333–59.
78. Dravet C, Bureau M, Oguni H, et al Severe myoclonic epi-lepsy in infancy (Dravet syndrome). In: Roger J, Bureau M, Dravet C, et al, eds. Epileptic syndromes in infancy, child-hood and adolescence. 4th ed. London: John Libbey; 2005.
79. Hirsch E, Marescaux C, Maquet P, et al. Landau-Kleffner syndrome: a clinical and EEG study of five cases. Epilepsia 1995;31:756–67.
80. Praline J, Hommet C, Barthez MA, et al. Outcome at adult-hood of the continuous spike-waves during slow sleep and Landau-Kleffner syndromes. Epilepsia 2003;44:1434–40.
81. Kotagal P. Multifocal independent spike syndrome: relation-ship to hypsarrhythmia and the slow spike-wave (Lennox-Gastaut) syndrome. Clin Electroencephalogr 1995;26:23–9.
82. Normand MM, Wszolek ZK, Klass DW. Temporal intermit-tent rhythmic delta activity in electroencephalograms. J Clin Neurophysiol 1995;12:280–4.
83. Garcia-Morales I, Martíez-Salio A, García-Morales I, et al. Periodic lateralized epileptiform discharges: etiology, clinical aspects, seizures, and evolution in 130 patients [Spanish]. J Clin Neurophysiol 2002;19:172–7.
84. Gross DW, Wiebe S, Blume WT. The periodicity of lateralized epileptiform discharges. Clin Neurophysiol 1999;110:1516–20.
85. Reiher J, Rivest J, Grand’Maison F, Leduc CP. Periodic lat-eralized epileptiform discharges with transitional rhythmic discharges: association with seizures. Electroencephalogr Clin Neurophysiol 1991;78:12–17.
86. Chatrian GE, Shaw CM, Leffman H. The significance of periodic lateralized epileptiform discharges in EEG: an electrographic, clinical and pathological study. Electroen-cephalogr Clin Neurophysiol 1964;17:177–93.
87. Yemisci M, Gurer G, Saygi S, Ciger A. Generalised periodic epileptiform discharges: clinical features, neuroradiological evaluation and prognosis in 37 adult patients. Seizure 2003; 12:465–72.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 43
88. Brenner RP, Atkinson R. Generalized paroxysmal fast ac-tivity: electroencephalographic and clinical features. Ann Neurol 1982;11:386–90.
89. Gibbs EL, Anderson EM, Gibbs FA. Diagnosis and prog-nosis of hypsarrhythmia and infantile spasms. Pediatrics 1954;13:66–73.
90. Lombroso CT. A prospective study of infantile spasms: clini-cal and therapeutic correlations. Epilepsia 1983;24:135–58.
91. Dulac O, Plouin P, Jambaque I. Predicting favorable outcome in idiopathic West syndrome. Epilepsia 1993;34:747–56.
92. Drury I, Beydoun A, Garofalo EA, Henry TR. Asymmetric hypsarrhythmia: clinical, electroencephalographic and ra-diological findings. Epilepsia 1995;36:41–7.
93. Ohtahara S, Yamatogi Y. Epileptic encephalopathies in early infancy with suppression-burst. J Clin Neurophysiol 2003;20:398–407.
94. Lombroso CT. Early myoclonic encephalopathy, early in-fantile epileptic encephalopathy, and benign and severe infantile myoclonic epilepsies: a critical review and personal contributions. J Clin Neurophysiol 1990;7:380–408.
95. Takahashi Y, Fujiwara T, Yagi K, Seino M. Wavelength speci-ficity of photoparoxysmal responses in idiopathic general-ized epilepsy. Epilepsia 1995;36:1084–8.
96. Newmark ME, Penry KJ. Photosensitivity and epilepsy. a review. New York: Raven Press; 1979.
97. Jayakar P, Alvarez LA, Duchowny MS, Resnick TJ. A safe and effective paradigm to functionally map the cortex in childhood. J Clin Neurophysiol 1992;9:288–93.
98. Meier-Ewert K, Broughton RJ. Photomyoclonic response of epileptic and nonepileptic subjects during wakefulness, sleep, and arousal. Electroencephalogr Clin Neurophysiol 1976;23:301–4.
99. Sperling M. Intracranial electroencephalography. In: Eb-ersole JS, Pedley TA. 2nd ed. Current practice of clinical electroencephalography. New York: Lippincott Williams & Wilkins; 2003:639–80.
100. Schuh LA, Henry TR, Ross DA, et al. Ictal spiking pat-terns recorded from temporal depth electrodes predict good outcome after anterior temporal lobectomy. Epilepsia 2000;41:316–9.
101. Klass DW. Electroencephalographic manifestations of com-plex partial seizures. Adv Neurol 1975;11:113–40.
102. Jan MM, Sadler M, Rahey SR. Electroencephalographic features of temporal lobe epilepsy. Can J Neurol Sci 2010;37:439–48.
103. Sirven JI, Sperling MR, French JA, O‘Connor MJ. Signifi-cance of simple partial seizures in temporal lobe epilepsy. Epilepsia 1996;37:450–4.
104. Salanova V, Morris HH, Van Ness PC, et al. Comparison of scalp electroencephalogram with subdural electrocorti-cogram recordings and functional mapping in frontal lobe
epilepsy. Arch Neurol 1993;50:294–9.105. Salanova V, Andermann F, Olivier A, et al. Occipital lobe
epilepsy: electroclinical manifestations, electrocorticography, cortical stimulation and outcome in 42 patients treated be-tween 1930 and 1991. Brain 1992;115:1655–80.
106. Gastaut H. A new type of epilepsy: benign partial epilepsy of childhood with occipital spike-waves. Clin Electroencepha-logr 1982;13:13–22.
107. Foldvary N, Klem G, Hammel J, et al. The localizing value of ictal EEG in focal epilepsy. Neurology 2001;57:2022–8.
108. Verma A, Radtke R. EEG of partial seizures. J Clin Neuro-physiol 2006;23:333–9.
109. Litt B, Wityk R, Hertz S, et al. Nonconvulsive status epilepti-cus in the critically ill elderly. Epilepsia 1998;39:1194–1202.
110. Husain AM, Mebust KA, Radtke RA. Generalized periodic epileptiform discharges: etiologies, relationship to status epi-lepticus, and prognosis. J Clin Neurophysiol 1999;16:51–8.
111. Treiman DM, Walton NY, Kendrick C. A progressive sequence of electroencephalographic changes during generalized con-vulsive status epilepticus. Epilepsy Res 1990;5:49–60.
112. Pratt JL, Fleisher GR. Syncope in children and adolescents. Pediatr Emerg Care 1989;5:80–2.
113. Thilenius OG, Quinones JA, Husayni TS, Novak J. Tilt test for diagnosis of unexplained syncope in pediatric patients. Pediatrics 1991;87:334–8.
114. Benditt DG, Nguyen JT. Syncope: therapeutic approaches. J Am Coll Cardiol 2009;53:1741–51.
115. Parry SW, Tan MP. An approach to the evaluation and man-agement of syncope in adults. BMJ 2010;340:c880.
116. Kales A, Soldatos CR, Kales JD. Sleep disorders: insomnia, sleep-walking, night terrors, nightmares, and enuresis. Ann Intern Med 1987;106:582–92.
117. Derry CP, Duncan JS, Berkovic SF. Paroxysmal motor disor-ders of sleep: The clinical spectrum and differentiation from epilepsy. Epilepsia 2006;47:1775–91.
118. Lüders, HO, Noachtar S. Atlas and classification of electroen-cephalography. Philadelphia: WB Saunders; 1999.
119. Devinsky O. Patients with refractory seizures. N Engl J Med 1999;340:1565–70.
120. Kuyk J, Leijten F, Meinardi H, et al. The diagnosis of psycho-genic non-epileptic seizures: a review. Seizure 1997;6:243–53
121. Syed TU, LaFrance EC, Kahriman ES, et al. Can semiology predict psychogenic nonepileptic seizures? a prospective study. Ann Neurol 2011;69:997–1004.
122. Caplan JP, et al. Pseudopseudoseizures: conditions that may mimic psychogenic non-epileptic seizures. Psychosomatics 2011;52:501–6.
123. Jung WY, Pacia SV, Devinsky R. Neocortical temporal lobe epilepsy: intracranial EEG features and surgical outcome. J Clin Neurophysiol 1999;16:419–25.
S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
44 Hospital physician Board Review Manual www.turner-white.com
124. Lange HH, Lieb JP, Engel J Jr, Crandall PH. Temporo-spatial patterns of preictal spike activity in human temporal lobe epilepsy. Electroencephalogr Clin Neurophysiol 1983; 56:543–55.
125. Awad I, Rosenfeld J, Ahl J, Hahn J, Lüders H. Intractable epi-lepsy and structural lesions of the brain: mapping, resection strategies and seizure outcome. Epilepsia 1991;32:179-186.
126. Ojemann G. Different approaches to resective epilepsy sur-gery: "standard" and "tailored." Epilepsy Res 1992;13:221–32.
127. Ojemann GA. Intraoperative tailoring of temporal lobe resec-tions. In: Engel J Jr, ed. Surgical treatment of the epilepsies. 2nd ed. New York: Raven Press; 1993:481–8.
128. Sutherling WW, Risinger MW, Crandall PH, et al. Focal func-tional anatomy of dorsolateral frontocentral seizures. Neurol-ogy 1990;40:87–98.
129. Bengzon ARA, Rasmussen T, Gloor P, et al. Prognostic factors in the surgical treatment of temporal lobe epileptics. Neurology 1968;18:717–31.
130. Penfield W, Jasper H. Epilepsy and the functional anatomy of the human brain. Boston: Little, Brown; 1954.
131. Fenyes I, Zoltan I, Fenyes G. Temporal epilepsies with deep-seated epileptogenic foci. Arch Neurol 1961;4:559–71.
132. Ajmone-Marsan C, Baldwin M. ECoG in temporal lobe epi-lepsy. In: Baldwin M, Bailey P, eds. Temporal lobe epilepsy. Springfield (IL): Chas. C. Thomas; 1958:368–95.
133. Fiol ME, Gates JR, Torres F, Maxwell RE. The prognostic value of residual spikes in the postexcision electrocortico-gram after temporal lobectomy. Neurology 1991;41:512–6.
134. McBride M, Binnie C, Janota I, Polkey C. Predictive value of intraoperative electrocorticograms in resective epilepsy surgery. Ann Neurol 1991;30:526–32.
135. Samra S, Sneyd JR, Ross DA, Henry TR. Effects of propofol sedation on seizures and intracranially recorded epilepti-form activity in patients with partial epilepsy. Anesthesiology 1995;82:843–51.
136. Lüders H, Lesser RP, Morris HH, et al. Negative motor re-sponses elicited by stimulation of the human cortex. In: Wolf P, Dam M, Janz D, Dreifuss FE, eds. Advances in epileptol-ogy. Vol. 16. New York: Raven Press; 1987:229–32.
137. Lüders H, Lesser RP, Hahn J. Basal temporal language area demonstrated by electrical stimulation. Neurology 1986;36:505–10.
138. Ikeda A, Lüders HO, Burgess RC, et al. Movement-related potentials recorded from supplementary motor area and primary motor area: role of supplementary motor area in voluntary movements. Brain 1992;115:1017–43.
139. Ikeda A, Shibasaki H. Invasive recording of movement-related cortical potentials in humans. J Clin Neurophysiol 1992;9:509–20.
140. Fried I, Katz A, McCarthy G, et al. Functional organization of human supplementary motor cortex studied by electrical
stimulation. J Neurosci 1991;11:3656–66. 141. Morris HH, Dinner DS, Lüders H, et al. Supplementary motor
seizures: clinical and electroencephalographic findings. Neu-rology 1988;38:1075–82.
142. Penfield WJ, Brodley E. Somatic motor and sensory repre-sentation in the cerebral cortex of man as studied by electri-cal stimulation. Brain 1937;60:389–443.
143. Wood CC, Spencer DD, Allison T, et al. Localization of human sensorimotor cortex during surgery by cortical surface re-cordings of somatosensory evoked potentials. J Neurosurg 1988;68:99–111.
144. Penfield W, Roberts L. Speech and brain mechanisms. Princ-eton (NJ): Princeton University Press; 1959.
145. Lesser RP, Luders H, Morris HH. Electrical stimulation of Wernicke‘s area interferes with comprehension. Neurology 1986;36:658–63.
146. Ojemann G. Cortical organization of language. J Neurosci 1991;11:2281–7.
147. Ojemann GA, Mateer C. Human language cortex: localiza-tion of memory, syntax and sequential motor phoneme iden-tification systems. Science 1979;205:1401–3.
148. Ojemann GA, Ojemann J, Lettich E, Berger M. Cortical lan-guage localization in left, dominant hemisphere: an electrical stimulation mapping investigation in 117 patients. J Neuro-surg 1989;71:316–26.
149. Ojemann G. Organization of short-term verbal memory in language areas of human cortex: evidence from electrical stimulation. Brain Lang 1978;5:331–48.
150. Crandall PH. Cortical resections. In: Engel J Jr, ed. Surgi-cal treatment of the epilepsies. New York: Raven Press; 1987:377–416.
151. Ojemann GA, Dodrill CB. Verbal memory deficits after left temporal lobectomy for epilepsy: mechanism and intraopera-tive prediction. J Neurosurg 1985;62:101–7.
152. Hermann B, Wyler A, Somes G. Language function following anterior temporal lobectomy. J Neurosurg 1991;74:560–6.
153. Hermann B, Wyler A. Comparative results of dominant tem-poral lobectomy under general or local anesthesia: language outcome. J Epilepsy 1988;1:127–34.
154. Lesser RP, Luders H, Dinner DS, et al. The location of speech and writing functions in the frontal language area. Brain 1984;107:275–91.
155. Lüders H, Lesser RP, Hahn J. Basal temporal language area demonstrated by electrical stimulation. Neurology 1986;36:505–10.
156. Burnstine TH, Lesser RP, Hart J, et al. Characterization of the basal temporal language area in patients with left temporal lobe epilepsy. Neurology 1990;40:966-70.
157. Mayeaux R, Brandt J, Rosen J, Benson DF. Interictal memory and language impairment in temporal lobe epilepsy. Neurology 1980;30:120–5.

S e i z u r e s a n d E p i l e p s y : E l e c t r o p h y s i o l o g i c a l D i a g n o s i s
www.turner-white.com Epilepsy Volume 1, Part 2 45
158. Stafiniak P, Saykin AJ, Sperling MR. Acute naming deficits following dominant temporal lobectomy: prediction by age at 1st risk for seizures. Neurology 1990;40:1509–12.
159. Litt B, Esteller R, Echauz J, et al. Epileptic seizures may begin hours in advance of clinical onset: a report of five pa-tients. Neuron 2001;30:51–64.
Copyright 2012 by Turner White Communications Inc., Wayne, PA. All rights reserved.