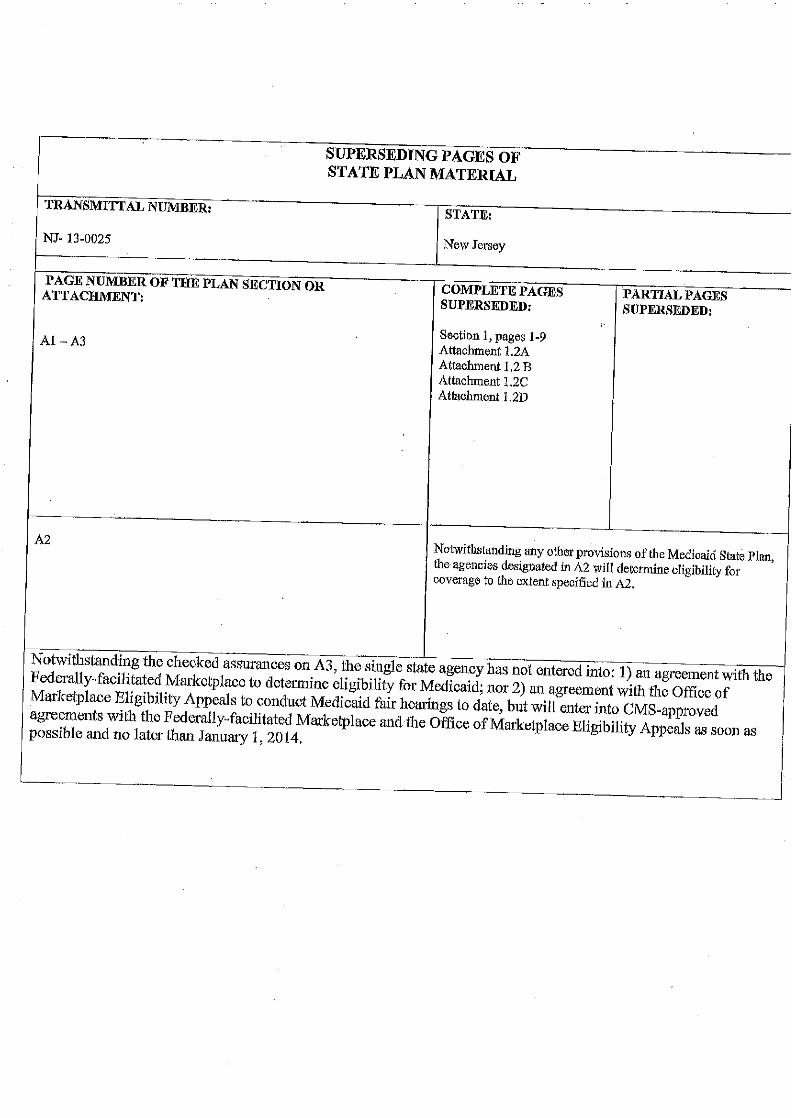
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY …€¦ · · 2014-09-10state plan under title...
190
- HCFA-AT-80-38 (BPP) .( 22, 1980 STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT ASSISTANCE PROGRAM .. -:-- ... .. ,._*,".
Transcript of STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY …€¦ · · 2014-09-10state plan under title...

-
HCFA-AT-80-38 (BPP).( 22, 1980
STATE PLAN UNDER TITLE XIX
OF THE SOCIAL SECURITY ACT
~1EDICAL ASSISTANCE PROGRAM
.. r~-;:"2~:,":---~ -:-- ...~-,:.-
.. ,._*,".

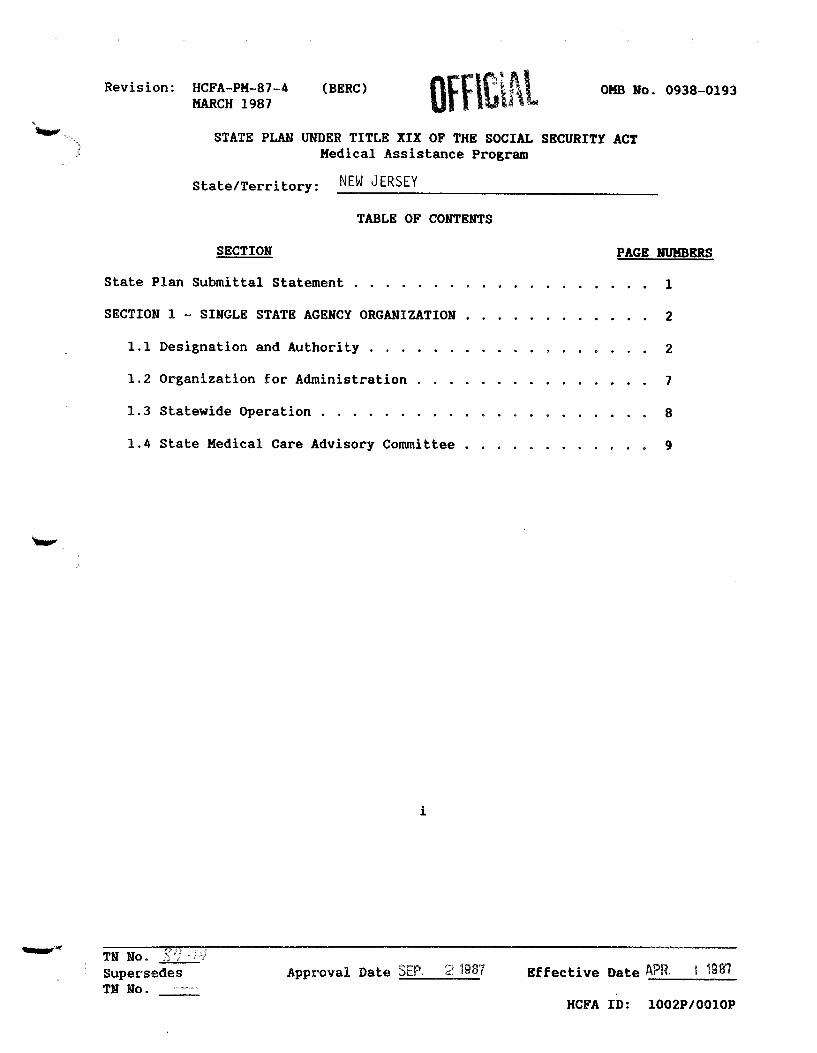
Revision: HCFA-PM-87-4MARCH 1987
(BERC) OfHC,Al OHa No. 0938-0193
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACTMedical Assistance P~og~am
State/Te~~ito~y:
SECTION
NEW JERSEY
TABLE OF CONTENTS
PAGE NUMBERS
State Plan Submittal Statement
SECTION 1 - SINGLE STATE AGENCY ORGANIZATION
1.1 Designation and Autho~ity ...
1.2 O~ganization fo~ Administ~ation
1.3 Statewide Ope~ation ....
1.4 State Medical Ca~e Adviso~y Committee.
i
1
2
2
7
8
9
TN No. gil· i"fSupe~sedes
TN No.App~ova1 Date SEP. 2 1987 Effective Date APR. 1 1981
HCFA ID: 1002P/0010P

Revision: HCFA-PM-87-4 (BERC) OMB No. 0938-0193MARCH 1987 OfflC\Al.......
SECTION PAGE IJUHBERS
SECTION 2 - COVERAGE AND ELIGIBILITY . . . . . . . . . . . . . . · · 10
2.1 Application, Determination of Eligibilityand Furnishing Medicaid . . . . . . . • .
2.2 Coverage and Conditions of Eligibility
2.3 Residence . . . .2.4 Blindness
2.5 Disability
2.6 Financial Eligibility ."
2.7 Medicaid Furnished out of State
ii
· 10
· • 12
13
· . 14
15
16
· 18
TN No. 8"11·· i'fSupersedesTN No.
Appt'oval Date SEP. 2 19B7 Effective Date APR. 1 1987
HCFA ID: 1002P/OOI0P

Revision: HCFA-PM-87-4MARCH 1987
SECTION
(BERC)
OffiCIALOKa No. 0938-0193
PAGE mJMBERS
SECTION 3 - SERVICES: GENERAL PROVISIONS
3.1 Amount, Duration, and Scope of Services.
3.2 Coordination of Medicaid with Medicare Part B
19
. 19
. . 29
3.3 Medicaid for Individuals Age 65 or Overin Institutions for Mental Diseases 30
3.4 Special Requirements Applicable tosterilization Procedures . . . . . . . . . . . 31
3.5 Medicaid for Medicare Cost Sharing forQualified Medicare Beneficiaries . . . . . . . • . 31a
3.6 Ambulatory Prenatal Care for Pregnant Womenduring Presumptive Eligibility Period . . . . • . . . . . . • 31b
Hi
TN No. .1SupersedesTN No.
Approval Date SEP. 2 1987 Effective Date APR. 1 1987
HCFA ID: 1002P/OOI0P

Revision: HCFA-PM-87-4HARCH 1987
SECTION
(BERC)
OFFICIALOHa No. 0938-0193
PAGE NUMBERS
SECTION 4 - GENERAL PROGRAM ADMINISTRATION
4.1 Methods of Administration.
4.2 Hearings for Applicants and Recipients
4.3 Safeguarding Info~ation on Applicantsand Recipients . . . . .
4.4 Medicaid Quality Control
4.S Medicaid Agency Fraud Detection andInvestigation Program
4.6 Reports . .
4.7 Maintenance of Records
4.8 Availability of Agency Program Manuals
4.9 Reporting Provider Payments to theInternal Revenue Service
4.10 Free Choice of Providers
4.11 Relations with Standard-Settingand Survey Agencies . . . . . .
4.12 Consultation to Medical Facilities
4.13 Required Provider Agreement.
4.14 Utilization Control
32
· 32
· 33
· 34
3S
· 36
· 37
. . 38
· 39
40
41
· 42
44
· 4S
· 46
4.15 Inspections of Care in Skilled Nursingand Inte~ediate Care Facilities andInstitutions for Mental Diseases . . . . . . . . . 51
4.16 Relations with State Health and vocationalRehabilitation Agencies and Title V Grantees 52
4.17 Liens and Recoveries
4.18 Cost Sharing and Similar Charges
4.19 Payment for Services
iv
· 53
· 54
· 57
TN No. ')'1 ···1;)
SupersedesTN No.
Approval Date SfF'. 2 1987 Effective Date APR. 1 1981
HCFA ID: 1002P/0010P
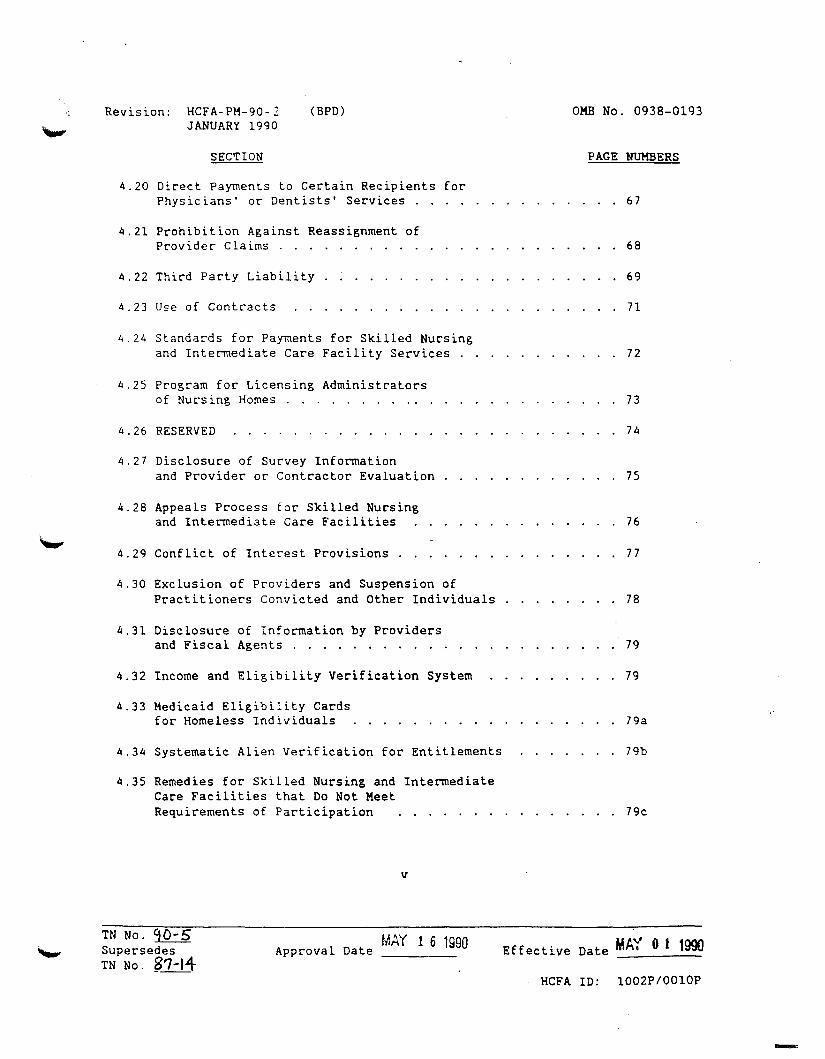
Revision: HCFA-PM-90-2JANUARY 1990
(BPD) OMB No. 0938-0193
SECTION PAGE NUMBERS
4.20 Direct Payments to Certain Recipients forPhysicians' or Dentists' Services. . 67
4.21 Prohibition Against Reassignment ofProvider Claims . . 68
4.22 Third Parly Liability 69
4.23 Use of Contracts 71
4.24 Standards for Payments for Skilled Nursingand Intermediate Care Facility Services 72
4.25 Program for Licensing Administratorsof Nursing Homes " 73
4.26 RESERVED 74
4.27 Disclosure of Survey Informationand Provider or Contractor Evaluation . . . . . . . . . . . . 75
4.28 Appeals Process for Skilled Nursingand Intermediate Care Facilities
4.29 Conflict of Interest Provisions.
76
77
4.30 Exclusion of Providers and Suspension ofPractitioners Convicted and Other Individuals . . . . . . . . 78
4.31 DiscLosure of Information by Providersand Fiscal Agents . . . . . . . . .
4.32 Income and Eligibility Verification System
4.33 Medicaid Eligibility Cardsfor Homeless Individuals
4.34 Systematic Alien Verification for Entitlements
4.35 Remedies for Skilled Nursing and IntermediateCare Facilities that Do Not MeetRequirements of Participation
v
79
79
79a
79b
. . . . . . . . 79c
TN No. 90-5SupersedesTN No. 3'7-14
MAY 1 6 1990Approval Date Effective Date MAY 0 1 1990
HCFA 10: l002P/OOIOP
-
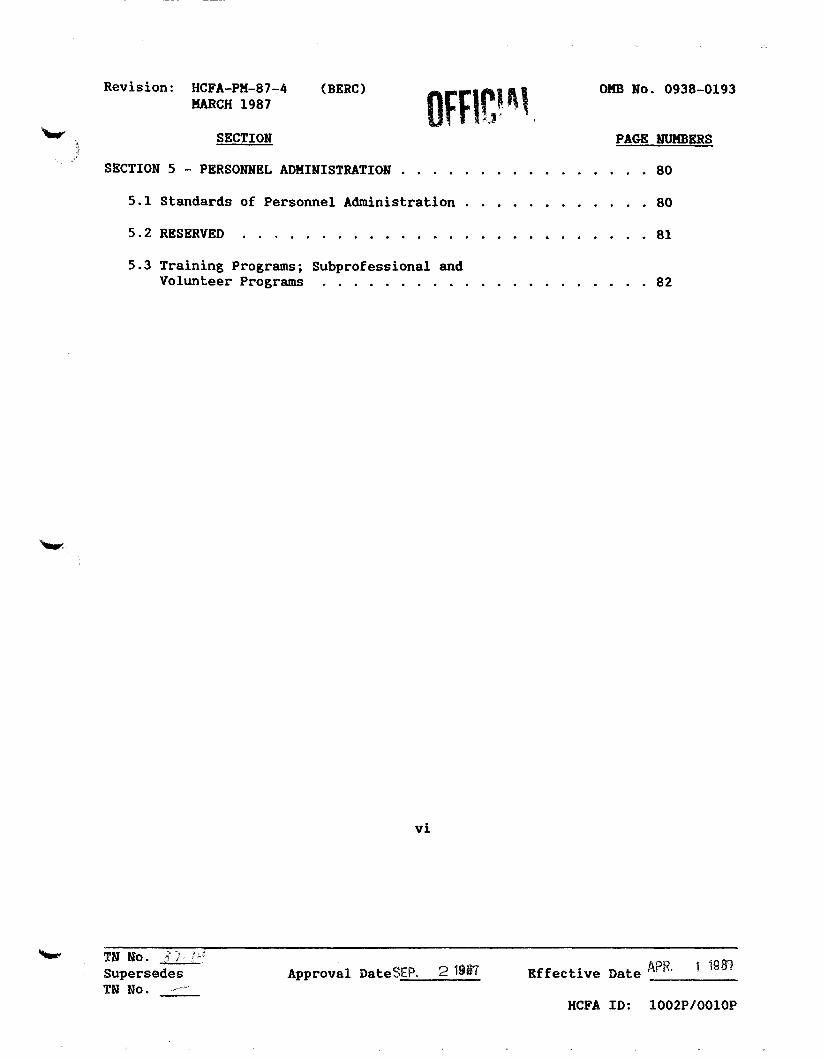
Revision: HCFA-PM-87-4KARCH 1987
SECTION
(BERC) OKB No. 0938-0193
PAGE WKBERS
SECTION 5 - PERSONNEL ADMINISTRATION
5.1 Standards of Personnel Administration
5.2 RESERVED
· 80
· 80
· 81
5.3 Training Programs; SUbprofessional andVolunteer Programs . . . . . . . . . . . . . . . . . . . . . 82
vi
TN No. :,; ... ;' "'I
SupersedesTN No.
Approval DateSEPo 2 1987 APR 1 1~81Effective Date 0 _
HCFA ID: 1002P/0010P

Revision: HCFA-PK-87-4KARCH 1987
SECTION
(BERC)
Off\t\~lOKB No. 0938-0193
PAGE HUHBERS
SECTION 6 - FINANCIAL ADMINISTRATION
6.1 Fiscal Policies and Accountability
6.2 Cost Allocation
6.3 State Financial Participation.
vii
83
83
84
• 85
21987 1 1987TN No. -, .'\ .; j
SupersedesTN No. __
Approval Date SEP,----- Effective Date APR.-----HCFA ID: 1002P/0010P

Revision: HCFA-PM-91- 4August 1991
(BPD) OFF/CIAL Olm No. 0938-
SECTION
SECTION 7 - GENERAL PROVISIONS
7.1 Plan Amendments.
7.2 Nondiscrimination
7.3 Maintenance of AFDC Effort
7.4 State Governor's Review ..
viii
PAGE NUMBERS
· 86
• 86
87
88
• 89
TN No. :::::!:E3a.. DECSupersedes '1 Approval Date 5 1991TN No. 8_",/+ -----
Effective Date OCT 11991
HCFA ID: 7982E

Revision: HCFA-PM-91-4 (BPD) OMB No.: 0938Page 1
{)ff\t\~l
LIST OF AITACHMENTS
No. Title of Attachments
*1.1-A Attorney General's Certification
*1.1-B Waivers under the Intergovernmental Cooperation Act
1.2-A Organization and Function of State Agency
1.2-B Organization and Function of Medical Assistance Unit
1.2-C Professional Medical and Supporting Staff
1.2-D Description of Staff Making Eligibility Determination
2.1-A (Reserved)
*2.2-A Groups Covered and Agencies Responsible for EligibilityDeterminations
* Supplement 1 -
* Supplement 2 -
* Supplement 3 -
Reasonable Classifications of Individuals underthe Age of21, 20, 19 and 18Definitions of Blindness and Disability ,(Territories only)Method of Determining Cost Effectiveness ofCaring for Certain Disabled Children at Home
*2.6-A Eligibility Conditions and Requirements (States only)
* Supplement 1 -
* Supplement 2 -
* Supplement 3 -
* Supplement 4 -
*Forms Provided
TN # --"-03"'----=07-'-- _Supersedes TN # 91-32
Income Eligibility Levels - CategoricallyNeedy, Medically Needy and Qualified MedicareBeneficiariesResource Levels - Categorically Needy,Including Groups with Incomes Up to aPercentage of the Federal Poverty Level,Medically Needy, and other Optional GroupsReasonable Limits on Amounts for NecessaryMedical or Remedial Care Not Covered underMedicaidSection 1902(f) Methodologies for Treatment ofIncome that Differ from those of the SSIProgram
Effective Date ~ 113'129RnlApproval Date _
03-07-MA (NJ)
• Supplement 5 -
-..i • Supplement Sa-
..• Supplement 6 J
~~ • Supplement 7
• Supplement 8 -• Supplement 8a-
• Supplement 8b-
* Supplement 9 -* Supplement 10-
* Supplement 11-
* Supplement 1 -
* Supplement 2 -
* Supplement 3 -
* Supplement 4 -
* Supplement 5 -
* Supplement 6 -
*Forrns Provided
Revision: HCFA-PM-91-8October 1991
OMS No.:Page 2
(MB)
Title of Attachment
Section 1902(f) Methodologies for Treatment otResources that Differ from those of the S8IProgramMethodologies for Treatment of Resources torIndividuals With Incomes Up to a Percentage ofthe Federal Poverty LevelStandards for Optional State SupplementaryPaymentsIncome Levels for 1902(f) States Categorically Needy Who Are Covered underRequirements More Restrictive than SSIResource Standards for 1902(f) States Categorically NeedyMore Liberal Methods of Treating Income UnderSection 1902(r)(2) of the ActMore Liberal Methods of Tre~t1ng ResourcesUnder Section 1902(r)(2) of the ActTransfer of ResourcesConsideration of Medicaid QualifyingTrusts--Undue HardshipCost-Effective Methods for COBRA Groups(States and Territories)
Eligibility Conditions and Requirements (Territories only)
Income Eligibility Levels - CategoricallyNeedy, Medically Needy, and Qualified MedicareBeneficiariesReasonable Limits on Amounts for NecessaryMedical or Remedial Care Not Covered underMedicaidResource Levels for Optional Groups withIncomes Up to a Percentage of the FederalPoverty Level and Medically NeedyConsideration of Medicaid QualifyingTrusts--Undue HardshipMore Liberal Methods of Treating Income underSection 1902(r)(2) of the ActMore Liberal Methods of Treating Resourcesunder Section 1902(r)(2) of the Act
!£.
*2.6-A
TN No. q~-d-supersedesq.. ,lopprovalTN No. I- 301-.
MAR ZS 19C?Date ~~ Effective Date
HCFA ID: 7982E
JAN1 199Z
....
Revision: HCFA-PM-91-4August 1991
(BPD) OMB No: 0938Page 3
*3.1-A
Title of Attachment
Amount, Duration, and Scope of Medical and Remedial Care andServices Provided to the Categorically Needy
*Supplement 1- Case Management ServicesSupplement 2- Alternative Health Care Plans for FamiliesCovered Under Section 1925 of the Act
OFFICIAL
*3.1-B
3.1-C
3.1-0
*3.1-E
3.1-F
4.11-A
4.14-A
4.14-B
....... 4.16-A
4.17-A
*4.18-A
*4.18-B
*4.18-C
*4.18-0
*4.18-E
4.19-A
Amount, Duration, and Scope of Services Provided Medically NeedyGroups
Standards and Methods of Assuring High Quality Care
Methods of Providing Transportation
Standards for the Coverage of Organ Transplant Procedures
State Plan Preprint for Mandatory Enrollment into Managed Care
Standards for Institutions
Single Utilization Review Methods for Intermediate Care Facilities
Multiple Utilization Review Methods for Intermediate Cate Facilities
Cooperative Arrangements with State Health and State Vocational RehabilitationAgencies and with Title V Grantees
Determining that an Institutionalized Individual Cannot BeDischarged and Returned Home
Charges Imposed on Categorically Needy
Medically Needy- Premium
Charges Imposed on Medically Needy and other Optional Groups
Premiums Imposed on Low Income Pregnant Women and Infants
Premiums Imposed on Qualified Disabled and Working Individuals
Methods and Standards for Establishing Payment Rates- InpatientHospital Care
*Forms Provided
TN # ~03,,----O,,-,7 _......Supersedes TN # 91-32
Effective Date AUG 13 2003Approval Date MAR 1 7 2004
03-07-MA (NJ)

Methods and Standards for Establishing Payment Rates - Other Typesof Care
,~~•
Revision: HCFA-PM-91-aOctober 1991
No.
4.19-S
OFFICiAL(MB)
Title of Attachment
OMS Ro.:Page ..
* Supplement 1 - Methods and Standards for Establishing PaymentRates for Title XVIII Deductible/Coinsurance
1Jt
4.19-C Payments for Reserved Seds
4.19-0 Methods and Standards for Establishing Payment Rates - SkilledNursing and Intermediate Care Facility Services
4.19-E Timely-Claims Payment - Definition of Claim
4.20-A Conditions for Direct Payment for Physicians' and Dentists' Services
4.22-A Requirements for Third Party Liability--Identifying Liable Resources
*4.22-S Requirements for Third Party Liability--Payment of Claims
*4.22-C Cost-Effective Methods for Employer-Sased Group Health Plans
*4.32-A Income and Eligibility Verification System Procedures: Requests toOther State Agencies
*4.33-A Method for Issuance of Medicaid Eligibility Cards to HomelessIndividuals
7.2-A Methods of Administration - Civil Rights (Title VI)
*Forms Provided
HCFA ID: 7982E
1992JANlEffective Date -------
MAR 2 3 1~82Date
TN No. q~-~supersedesq/ ~ ApprovalTN No. - :..;J..
Revision: HCFA-PM-91- 4AUGUST 1991
(BPD) OFFICIAL OMS No. 0938-
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACTMEDICAL ASSISTANCE PROGRAM
State/Terri tory:__Ne_w_J_e_r_s...;ey=-- _
Citation
42 CFR430.10
As a condition for receipt of Federal funds undertitle XIX of the Social Security Act, the
Department of Human Services(Single State Agency)
submits the following State plan for the medicalassistance program, and hereby agrees to administerthe program in accordance with the provisions of thisState plan, the requirements of titles XI and XIX ofthe Act, and all applicable Federal regulations andother official issuances of the Department.
TN No. =::91-3&supersedes'1 M Approval DateTN No. _.1-.3
DEC 5 1991 Effective Date
HCFA 10: 7982E
{JCT 1 .::~ l
len: Hc:7\-AT-80-38 (BPP)~ ~~y 22, 1980
2
~- -.
NEt·! JERSEYState-------------------------SINci..E STA'IE AGEN::Y ORGAi."UZATICN
Citation42 CPR 431.10AT-79-29
'1 # 77-3,-,"supersedes
'IN # 7"-~t
1.1 Desianation and Authoritv
(a) The DEPARTMENT OF HU~lAN SERVI CES
is the sir~le State agency designatedto administer or supervise theadministration of the Medicaidprogram under title XIX of the SocialSec~rity Act, (All ~ef~rences inthis plan to "the Medicaid agency"mean the agency named in thisparagraph. )
ATTAC~IT l.l-~ is a certificationsigned by the State Attorney Generalidentifying the single State agencyand citing the legal authority underwhich it administers or supervisesadministration of the program.
Approval Date K - /8 - 7] Effective Date 1-1-77
:: ,.,.....:- ~: -
1"',.\: ","_~,~" .. ,.- -.

3
Revision: 6C?A-.~-80-38(BPP)
May 22, 1980
NEW JERSEYState-------------------------CitationSec. 1902 (a)of the Act
1.1 (b) The State agency that administered orsupervised the administration of theplan atproved under title X of theAct as of January I, 1965, has beenseparately designated to administeror supervise the administration ofthat part of this plan which relatesto blind individuals.
U Yes. The State agency socesignated is
This agencJ has a separate plancover ing t."1at fOrtion of t.~e
State plan under title XIX forwhich it is responsible.
!.l:J Not applicable. The entire planunder title XIX is administeredor supervised 'rJj t.!':le StateagencJ named in paragraph 1.1(a).
~;.>,.::;.:}-:-"',7:-:: ~.:. ....... .'J•• • '_
'IN # 77 - 3upersedes
......:J.,: # 7~ 0# ;:./
Approval Date f-/8-77 Effective Date /-1-77

Revision:
4
ECFA-.~-80-38(BPP)
rA.ay 22, 1980
I •. ",..,0- •..
~';!.>. ~-~.: -
NEH JERSEYState--------------------------CitaticnIntersovernrnentalCooporation Actof 1968
'IN it 77 - 3'"'.ppersedes
'.~ # 7fb-ZI'--'
1.1(c) Naivers of the single State agencyrequirement which are cJrrentlyoperative have been granted underau~~rity of the IntergovernmentalCooperation Act of 1968.
U Yes. ATI'A01MEN1' 1.1-B descr ibesthese waivers and the afProvedalternative organizationalarrangements.
U :kJt applicable. Haivers are r.olonger in effect.
1.1.1 Not applicable. No waivers haveever beo-n granted.
Afproval Date ~ -/8-77 Effective Date /-1-77
--,"---r::.:.:~:.,:::"'.. '._............-......
NHI JERSEY
5
t 100: OCFA-AT-80-38 (BPP)~ May 22, 1980
State-------------------------
~'" .
Citaticn42 ern 431.10AT-79-29
n:l # 77 - 3.......Jupersedes
1N # 7tD-2-1
1.1 (d) U The agenC'j named in paragraph1.1(a) has responsibility forall determinaticns ofelig~bi1ity for Medicaid underthis plan.
LJI Determinaticns of eligibilityfor Medicaid under this plan aremade by the agency (ies)specified in ATrFCHMENr 2.2-A.There is a written agrea~ent
betwe""J1 the agenC'j named inparagraph 1.1 (a) and otheragency (ies) making suchdeterminaticns for specificgroups oovered under this plan.The agreement defines therelationships and respectiveresponsibilities of ~~e agencies.
Approval Date 1- /8- 77 Effective Date ,- 1-77
:'";'.-'" ;"; .:.'
\:.,','.

--......_,;-.ND~ JERSEYState------------------------
6
~vision: HCFA-AT-BO-38 (BFP)~ May 22, 1980
Citaticn42 ern 431.10AT-79-29
1.1(e) All other provisions of ~,is plan areadministered by the Medicaid agencjexcept for those functions for whichfiJ1a]. authority has l:e2n granted to aProfessional Standards ReviewOrganization under title XI of the ~~t.
(f) All other requirements of 42 CFR 431.10are met.
:~..•.• ,,"i" ."':",,'
IN # 77-3"-'" Sup€rsedes
'IN # 74. -ZIAfproval Date f - Ie ... 77 Effective Date 1- J. 77

NHJ JERSEY
7
~''''ision: EC.t:'A-AT-80-38 (BPP)May 22, 1980
State-------------------------
..... ,.
-
Citation42 CPR 431.11AT-79-29
'IN # 74 -7;1persedes
'-"ill # 74 - ..,.
1.2 Orqanization for Administraticn
(a) ATTACHMENT 1.2-A contains a descriptionof the organization and functions of theMedicaid agency and an organizationchart of "the agency.
(b) Within the State agency, the Division
of Medical Assistance and Health Serviceshas been designated as the medicalassistance unit. A~.c~'!EL'IT 1.2-3contains a description Ot theorganization and functions of themedical assistance unit and anorganization chart of the unit.
(c) ~~~~ 1.2-C contains a descriptionof the kinds and numbers of professionalmedical personnel and supporting staffused in the administration of the planand their responsibilities.
(d) Eligibility determinations ar~ made byState or local staff of an agenC'j otherthan the agency named in paragraph1.1 (a). ATI'A01MENl' 1. 2-D contains adescription of the staff designated toITl.ake such determinations a.'1d thefunctions they will perform.
IlJ Not applicable. Only staff of theagency named in paragraph 1.1(a)make such determinations.
Approval Date 4-2.J-7S- Effective Date 7-/-74
.(. ' .~.'..:

8
~evisicn: ECFA-AT-80- 38 (BPP)May 22, 1980
;;~....:<:: .~/ ~~·::~'~I- .t·,
~. :$....:._
State ---.;.~.;.;;;IE.;.;.~I.....:J;,..;;:E:.:.:R.:::;.;SE::.,:Y:-..- _
Citaticn42 em431. 50 (b)AT-79-29
'IN ~ 74 - 7Sup.eEseces'IN # 74 - +
1.3 Statewide Operation
The plan is in operation on a Statewidebasis in accordance with all requirementsof 42 CPR 431.50.
LxI The plan is State administered.
U The plan is administered by t.~e
p:JlitiC2.l su.tdivisions of the Stateand is mandatory on them.
Approval Date 4-21-75 Effective.Date 7-1-74
9
Revision: HCFA-AT-80-38 (BPP)May 22,1980
State: New Jersey
OFFICIAL
Citation42CFR43 1. 12(b)AT-78-90
42CFR438.104
1.4 State Medical Care Advisory Committee
There is an advisory committee to the Medicaidagency director on health and medical careServices established in accordance with andMeeting all the requirements of 42 CFR 431.12.
-X- The State enrolls recipients in MCa, PIHP, PAHP, and/orPCCM programs. The State assures that it complies with therequirements of 42 CFR 438.104(c) to consult with the Medical CareAdvisory Committee in the review of marketing materials.
03-07-MA (NJ)
TN # ---"'03==---"-07-'-- ~
Supersedes TN #_7'-4'----=07-'-- _...... AUG 1 3 inn":!Effectlve Date .. J
Approval DateMAR 1 7 2004

9a
Revision: HCFA-PM-94-3 (MS)APRIL 1994State/Territory: New Jersey
------~------Citation
OFFICiAL
1928 of the Act
1.5 Ped~atric Immunization Program
1. The State has implemented a program for thedistribution of pediatric vaccine. to programregistered providers for the immunization offederally vaccine-eligible children in accordancewith section 1928 as indicated below.
a. The state program will provide eachvaccine-eligible child with medicallyappropriate vaccine. according to theschedule developed by the Advisory Committeeon Immunization Practices and without chargefor the vaccines.
b. The State will outreach and encourage avariety of providers to participate in theprogram and to administer vaccines inmultiple setting., e.g., private health careproviders, providers that receive funds underTitle V of the Indian aealth care ImprovementAct, health programs or facilities operatedby Indian tribes, and maintain a list ofprogram-registered providers.
c. With respect to any population of vaccineeligible children a substantial portion ofwhose parents have limited ability to speakthe English language, the State will identifyprogram-registered providers who are able tocommunicate with this vaccine-eligiblepopulation in the language and culturalcontext which is most appropriate.
d. The State will instruct program-registeredproviders to determine eligibility inaccordance with section 1928(b) and (h) ofthe Social Security Act.
e .. The State will assure that no programregistered provider will charge more for theadministration of the vaccine than theregional maximum established by theSecretary. The State will inform programregistered providers of the maximum fee forthe administration of vaccines.
f. The State will asaure that no vaccin_eligible child is denied vaccines because ofan inability to pay an administration fee.
g. Except as authorized under section 1915(b) ofthe Social Security Act or as ~tted bythe secretary to prevent fraud or abuse, theState will not impose any additionalqualifications or conditions, in addition tothose indicated above, in order for aprovider to qualify as a program-registeredprovider.
TN No. GfS-LSUpRrsedesTN No. 91f-j&3
Approval Date IM\'.! 1995 Effective Date .JUl 1- .. -
Revision: HCPA-PM-94-3 (HB)APRIL 1994State/Territory:
Citation
9b
New Jersey
llff\&\~l
1928 of the Act 2. The State haa not modified or repealed anyImmunization Law in effect as of Hay 1, 1993 toreduce the amount of health insurance coverage ofpediatric vaccines.
3. The State Medicaid Agency has coordinated withthe State Public Health Agency in the completionof this preprint page.
4. The State agency with overall respon8ibility forthe implementation and enforcement of theprovisions of section 1928 is:
State Medicaid Agency
X State Public Health Agency
TN No. 1£- i lAY 0 1 t8&BSupersedes Approval Date __TNNO.~
Effective Date JUL 1- 1995
-
10
SECTION 2 - COVERAGE AND ELIGIBILITY
HCFA-PM-91- 4 (BPD)AUGUST 1991
Revision:
State: New Jersey
OMB No.: 0938-
Citation42 CFR435.10 andSubpart J
2.1 Application, Determination of Eligibility andFurnishing Medicaid
(a) The Medicaid agency meets all requirements of42 CFR Part 435, Subpart J for processingapplications, determining eligibility, and furnishingMedicaid.
TN No. q7- 90 Date JAN 15 1992Supersedesn ApprovalTN No. )5-8"
Effective Date
HCFA ID: 7982E
OCT 0 1 1991
NEW JERSEY MEDICAID STATE PLAN
11
"-" .Revision: HCFA-PM- (MB)
Staterrerritory: --'N~e:.;w"'_"_Je=_'r~se::.y'__ _
OFFICIAL
Citation42CFR435.9141902(a)(34)of the Act
1902(e)(8) and1905(a) of theAct
1902(a)(47) and,-,,1920 of the Act
2.1(b) (1)
(2)
(3)
Except as provided in items 2. 1(b)(2) and (3)below, individuals are entitled to Medicaidservices under the plan during the three monthspreceding the month of application, if they were, oron application fvould have been, eligible. Theeffective date of prospective and retroactive eligibilityis specified in Attachment 2.6-A.
For individuals who are eligible for Medicarecost-sharing expenses as qualified Medicarebeneficiaries under section 1902(a)(1O)(E)(i) of theAct, coverage is available for services furnished afterthe end of the month in which the individual is firstdetermined to be a qualified Medicare beneficiary.Attachment 2.6-A specifies the requirem~nts fordetermination of eligibility for this group.
Pregnant women are entitled to ambulatory prenatalcare under the plan during a presumptive eligibilityperiod in accordance with section 1920 of the Act.Attachment 2.6-A specifies the requirements fordetermination of eligibility for this group.
03-07-MA (NJ)
TN # --",-0=:-3--",-0-,--7 _~Supersedes TN #----'9"-=3"--~19-"- _
Effective Date AUG 13 2003Approval Date MM< Y i roOt}
11a
Revision: HCFA-PM-91-S (MB)Octoberl991
"-Jl
•State/Territory: New Jersey
OMS No.
Citation
1902{a)(55)of the Act
2.1(d) The Medicaid agency has procedures to takeapplications, assist applicants, and performinitial processing of applications from those lowincome pregnant women, infants, and children underage 19, described in S1902(a)(10)(A)(i)(IV),(a)(lO)(A)(i)(VI), (a)(lO)(A)(i)(VII), and(a)(10)(A)(ii)(IX) at locations other than thoseused by the title IV-A program including FQHCs anddisproportionate share hospitals. Sucrapplication forms do not include the ADFC formexcept as permitted by HCFA instructions.
TN No. '1 a..-J-.supersede~1 ~APprovalTN No. - I
DateMAR ZI 1992
Effective Date
HCFA ID: 7985E
JAN]
state:
citation
Page' 11a. a
New Jersey
434.2048 FR 54013
The state Agency undertakes tooperate a program which meets allrequirements of 1903(m) as well asapplicable regulations in 42 CFRPart 434 and is defined inAttachment 2.1-A(a).
If :JM 11981TM No. '~\ ~- il Approval DatJf V 2 8 1989. Effective Date
SUPERSEDES 11~~_~v~~l


wnwiPage 11 e
STATE PLAN UNDER TITLE XIX OF THL SOCIAL SECURITY ACTState: New Jersey
SECTION 2 COVERAGE AND ELIGIBILITY
Citation(s)
1902(e)(13)ofthe Act
2.1 Application. Determination of Elmibility and Furnishing Medicaid(Continued)
|X| (e) Express Lane Option. The Medicaid State agency elects theoption to rely on a finding from an Express Lane agency whendetermining whether a child satisfies one or more components ofMedicaid eligibility. The Medicaid State agency agrees to meetall of the Federal statutory and regulatory requirements for thisoption. This authority may not apply to eligibilitydeterminations made before April 11, 2011 or after September30,2013.
( 1 ) The Express Lane option is applied to:
[XJInitial determinations I i Redeterminations I Both
(2) A child is defined as younger than age:
M19 ' 2 0 @21
(3) The following public agencies arc approved by theMedicaid State agency as Express Lane agencies:
New Jersey Department of Agriculture as administered by and through the New JerseyDepartment of Education
11-06-MATN No.: 11-06New
Approval Date FEB Q 8 2012. Effective Date .APR 0 3 ?Q11
Page 11
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACTState: New Jersey
SECTION 2 COVERAGE AND ELIGIBILITY
Citation(s)
2.1 Application. Determination of Eligibility and Furnishing Mcdieaid(Continued)
(4) The following component/components of Medicaid eligibility aredetermined under the Express Lane option. Also, specify anydifferences in budget unit , deeming, income exclusions, incomedisregards, or other methodology between Medicaid eligibilitydeterminations for such children and the determination under theExpress Lane option.
The components of Medicaid eligibility under this Express Lane option are income andresidency.
Under this Express Lane option, income is determined by individual eligibility for Free lunchwithin the School Lunch Program (SEP), which has an income threshold of 130% FPL. The SLPdetermines income using adjusted gross income. This is different because without the ExpressLane option, earned income disregards, the child support disregard and child care deductionswould have been used when calculating financial eligibility for Medicaid.
Residency is accepted based on the child's status as a student in the school district, as determinedby the Express Lane Agency. This is different because without the Express Lane option,families must provide proof of residency by submitting documentation such as school records orutility bills.
Full eligibility is then determined by:-verifying citizenship and identity using available electronic data bases-determining family size using our subsequent application.
(5) Check off which option is used to satisfy the Screen and Enrollrequirement before a child may be enrolled under title XXI.
[] (a)Screening threshold established by the Medicaid agency as:
(i) percentage of the Federal poverty level(exceeds the highest Medicaid income threshold applicableto a child by a minimum of 30 percentage points); or
11-06-MATNNo.: 11-06 Approval I)atepr£g_Q_g_2Q^ffective Date Af>D_Q_ 1 2011
NewPage 11 g
STATE PLAN UNDER TITLE XIX OF TI IE SOCIAL SECURITY ACTState: New Jersey
SECTION 2 -COVERAGI-; AND ELIGIBILITY
Citation(s)
L ( i i ) percentage of the Federal poverty level (that reflectsthe value of any differences between income methodologies ofMedicaid and the Express Lane);
\_\) Temporary enrollment pending screen and enroll.
|x| (e) State's regular screen and enroll process for CHIP.
2.1 Applicalion. Determination of Eligibility and Furnishing Medicaid(Continued)
0(6) Check off if the State elects the option for automatic enrollmentwithout a Medicaid application, based on data obtained from othersources and with the child's or family's affirmative consent to thechild's Medicaid enrollment.
Q (7)Check off if the State elects the option to rely on a finding froman Express Lane agency that includes gross income or adjustedgross income shown by State income tax records or returns.
11-06-MATNNo.: 11-06 Approval Date p£g 0 ft 2012l Effective Date APR-Q-L20H'New

Revision: HCFA-PM-91- 4AUGUST 1991
State:
(BPO)
New Jersey
12
OMS No.: 0938-
Citation42 CFR435.10
2.2 Coveraae and Conditions of Eligibility
Medicaid is available to the groups specified inATTACHMENT 2.2-A.
1-/ Mandatory categorically needy and other requiredspecial groups only.
1-/ Mandatory categorically needy, other required specialgroups, and the medically needy, but no otheroptional groups.
1-/ Mandatory categorically needy, other required specialgroups, and specified optional groups.
1-j! Mandatory categorically needy, other required specialgroups, specified optional groups, and the medicallyneedy.
The conditions of eligibility that must be met arespecified in ATTACHMENT 2.6-A.
All applicable requirements of 42 CFR Part 435and sections 1902(a)(10)(A)(i)(IV), (V), and (VI),1902(a)(10)(A)(ii)(XI), 1902(a)(10)(E), 1902(1) and (m),1905(p), (q) and (s), 1920, and 1925 of the Act are met.
TN No. CZ! 90 JAN 1 5 1802Supersedes ~pproval DateTN No. 87-'t..-
OCT 0 1 1991Effective Date
HCFA ID: 7982E

Revision: HCFA-PM-87-4KARCH 1987
state:
13
(SERC)
NEW JERSEY
OHB 110.: 0938-0193
Citation435.10 and435.403, and1902(b) of theAct, P.L. 99-272(Section 9529)and P.L. 99-509(Section 9405)
2.3 Residence
Medicaid is furnished to e1icible individuals whoare residents of the State under 42 CFR 435.403,regardless of whether or not the individualsmaintain the residence pe~anently or maintain itat a fixed address.
TIl &0. 3!l:..1!1SupersedesTil &0. ilL-
Approval Date SEP. 2 1981 APR I 19B7IEffective Date . _
HCFA ID: 1006P/00IOP
Revision: HCFA-PH-87-4HARCH 1987
state:
14
(BERC)
NEW JERSEY
0938-0193
Citation42 CFR 435.530(b)42 CFR 435.531AT-78-90AT-79-29
2•4 Blindness
All of the requirements of 42 CFR 435.530 and42 CFR 435.531 are met. The more restrictivedefinition of blindness in terms of ophthalmicmeasurement used in this plan is specified inATTACHHEJIT 2. 2-A.
TN No. JI:L.L"fSupersedesTN No. ..2.J:L:J
Approval DateS~E~P_. 2_1_9_87 Effective Date _A_P_R_o__1_1_9_87
HCFA 10: 1006P/0010P

Revision: HCFA-PM-91- 4 (BPD)AUGUST 1991
15
OMB No. 0938-
Citation42 CFR435.121,435.540(b)435.541
State:
2.5
New Jersey
Disability
All of the requirements of 42 CFR 435.540 and 435.541are met. The state uses the same definition ofdisability used under the SSI program unless a morerestrictive definition of disability is specified inItem A.14.b. of ATTACHMENT 2.2-A of this plan.
TN No. 9/~ 'toSupersedes !APproval DateTN No. 8'7- 1 r..
JAN 15 1992Effective Date
HCFA ID: 7982E
OCT 0 1 1991
16-17Revision: HCFA-PM-92-1 (MB)
FEBRUARY 1992
State:
Citation(s)
New Jersey
2.6 Financial Eligibility
42 CFR435.10 andsubparts G & H1902(a) (10) (A) (i)( II I), ( IV), (V),( VI ), and (VII),1902(a) (10) (A) (ii)(IX), 1902(a)(lO)(A)(ii)(X), 1902(a) (10) (C),1902(f),1902(1)and (m),1905(p) and (5),1902(r) (2),and 1920
(a) The financial eligibility conditions forMedicaid-only eligibility groups and forpersons deemed to be cash assistancerecipients are described in ATTACHMENT 2.6-A.
TN No. AI s ~lJ.-~~ :JUL 2 1 1992Supersedes .pproval DateTN No. :l1-4IJ
Effective Date APR 1 1992
Revision: HCFA-PM-86-20SEPTEHBER 1986
(BERC) OKB-No. 0938-0193
State/Territory: NEW JERSEY
Citation
431.52 and1902(b) of theAct. P.L. 99-272(Section 9529)
2.7 Medicaid Furnished Out of State
Medicaid is furnished under the conditionsspecified in 42 CFR 431.52 to an eligibleindividual who is a resident of the Statewhile the individual is in another State. to thesame extent that Medicaid is furnished to residentsin the State.
TN NO. &'k"J1SupersedesTN NO. &,2' -I f'
Approval Date MAY 2 9 1981 OCT 1 1986Effective Date · __
HCFA ID:0053C/0061E

Revision: HCFA-PM-94-5APRIL 1994
State/Territory:
19
(MB)
NevI Jersey
OffiCIAL
Citation
SECTION 3 - SERVICES: GENERAL PROVISIONS
3.1 Amount, Duration, and Scope of Services
42 CFRPart 440,Subpart B1902(a), 1902(e),1905(a), 1905(p),1915, 1920, and1925 of the Act
(a) Medicaid is provided in accordance with therequirements of 42 CFR Part 440, Subpart Bandsections 1902(a), 1902(e), 1905(a), 1905(p),1915, 1920, and 1925 of the Act.
(1) Categorically needy.
Services for the categorically needy are describedbelow and in ATTACHMENT 3.1-A. These servicesinclude:
1902(a) (10)(A) and1905(a) of the Act
(i) Each item or service listed in section1905(a)(1) through (5) and (21) of the Act,is provided as defined in 42 CFR Part 440,Subpart A, or, for EPSDT services, section1905(r) and 42 CFR Part 441, Subpart B.
(ii) Nurse-midwife services listed in section1905(a)(17) of the Act, are provided to theextent that nurse-midwives are authorized topractice under State law or regulation andwithout regard to whether the services arefurnished in the area of management of thecare of mothers and babies throughout thematernity cycle. Nurse-midwives arepermitted to enter into independent provideragreements with the Medicaid agency withoutregard to whether the nurse-midwife is underthe supervision of, or associated with, aphysician or other health care provider.
Not applicable. Nurse-midwives are notauthorized to practice in this State.
TN No. q go-olS fTtHSupersedes Approval Date ..:JNl %S 1995TNNO.~
Effective Date OCT 1- 1994
OffICIAl19a
Revision: HCFA-PM-911991
(BPD) OMS No.: 0938-
State/Territory: N_E_W__J_E_R_S_E_y ___
1902(e)(5) ofthe Act
1902(a)(lO),clause (VII)of the matterfollow ing (E)of the Act
3.1Ia)(1) Amount, Duration, and Scope of Services:Categorically Needy (Continued)
(iii) Pregnancy-related, including familyplanning services, and postpartumservices for a 60-day period(beginning on the day pregnancy ends)and any remaining days in the month inwhich the 60th day falls are provided towomen who, while pregnant, were eligiblefor, applied for, and received medicalassistance on the day the pregnancy ends.
~ (iv) Services for medical conditions that maycomplicate the pregnancy (other thanpregnancy-related or postpartum services) areprovided to pregnant women.
(v) Services related to pregnancy (includingprenatal, delivery, postpartum, and familyplanning services) and to other conditionsthat may complicate pregnancy are the sameservices provided to poverty level pregnantwomen eligible under the provision ofsections 1902(a)(lO)(A)(i)(IV) and1902(a)(lO)(A)(ii)(IX) of the Act.
Effective DateTN No. q 7-3.1supersede~ /6 ApprovalTN No. ~-,
Date FEB to 1mHCFA ID: 7982E
OCT 1 199 1
Rev~s~o~: HCFA-PM-92-7'c:c,)ber 2.992
(ME)
19b OFFIC'AlState/Territory: New Jersey
Clt.ation 3.1 (a) (1) Amount, Duration, and Scope of Services:Categorically Needy (Continued)
(vi) Home health services are provided toindividuals entitled to nursing facilityservices as indicated in item 3.1(b) ofthu plan.
1902(e)(7) ofthe Act
(vii) Inpatient services that are being furnishedto infants and children described insection 1902(1)(1)(8) through (D), orSection 1905(n)(2) of the Act on the datethe infant or child attains the maximum ag~
for coverage under the approved State planWill continue until the end of the stay forwhich the inpatient services are furnished.
1902(e)(9) of theAct.
(viii) Respiratory care services are providedto ventilator dependent individuals asindicated 1n item 3.1,h) of this plan.
1902(a)(52)ar.d 1925 of theAct
(ix) Services are provided to familieseligible under section 1925 of the Actas indicated in item 3.5 of this plan.
1905(a) (23)and 1929
(x) Home and Community Care for FunctionallyDisabled Elderly IndiViduals, as defined,described and limited in Supplement 2 toAttachment 3.1-A and Appendices A-G toSupplement 2 to Attachment 3.1-A.
ATTACHMENT 3.1-A identifies the medical and remedi~l
services prOVided to the categorically needy, specifies alllimitations on the amount, duration and scope of tho.eservices, and lists the additional coverage (that i. inexcess of established service limits) for pregnancy-relatedservices and services for conditions that may complicatethe pregnancy.
Effective Date APR 1 - 1994-------AUG 1 5 199'
Approval DateTN No. ::=3 if-/3SupersedesTN No. ~1-3S
State of New JerseyPACE State Plan Amendment Pre-Print
19-C l( ....
.. ~ ~~egk \
Citation 3.1 (a)( I) Amount, Duration, and Scope of Services: Categorically Needy(Continued)
1905(a)(26) and 1934_-,x~ Program of All-Inclusive Care for the Elderly (PACE) services, as
described and limited in Supplement 3 to Attachment 3.I-A.
ATTACHMENT 3.l-A identifies the medical and remedial services provided tothe categorically needy. (Note: Other programs to be offered to CategoricallyNeedy beneficiaries would specify all limitations on the amount, duration andscope of those services. As PACE provides services to the frail elderly populationwithout such limitation, this is not applicable for this program. In addition, otherprograms to be offered to Categorically eedy beneficiaries would also list theadditional coverage -that is in excess of established service limits- forpregnancy-related services for conditions that may complicate the pregnancy. AsPACE is for the frail elderly population, this also is not applicable for thisprogram.)
07-02-MA (NJ)
TN __"'-07<.::-"'02=-- _
Supersedes TN _-"9~8~-IL:l4t-.
Approval Date ft!.J'.i 1 3 '." ,~r:p <) "'12M .,
Effective Date __"'_"-__'._f~U~t.l,-!I.:..1

State of New Jersey
Page 19d
OffltlAlCitation
19150)
3.1 (a)( I) Amount, Duration, and Scope of Services: Categorically Needy(Continued)
19150) Self-Directed Personal Assistance ServicesState Plan Amendment Pre-Print
_-"X,- Self-Directed Personal Assistance Services, as described and limited inSupplement 4 to Anachment3.I-A.
AITACHMENT 3.I-A identifies the medical and remedial services provided tothe categorically needy.
j\lL 2. 3 10118IN ~r~D~ MA Approv.l Oate:__-
~~persedeS TN ~Effective Oate~'~
____----------------=-_miW'rlt-""(N..;,:,J<....)__New

Revision: HCFA-PM-94-5APRIL 1994
State/Territory:
20
New Jersey
OFFICIALOMS No.: 0938-
Citation 3.1 Amount, Duration and Scope of Services (cont.)
42 CFR Part 440,
1902(e)(5) of
(a)(2) Medically Needy.
I=K=I This State plan covers the medically needy. Theservices described below and in ATTACHMENT 3.1-8are provided.
Services for the medically needy include:
(i) If services in an institution for mentaldiseases or an intermediate care facility forthe mentally retarded (or both) are prOVided toany medically needy group, then each medicallyneedy group is provided either the serviceslisted in section 1905(a)(1) through (5) and(17) of the Act, or seven of the services listedin Section 1905(a)(1) through (20). Theservices are prOVided as defined in 42 CFR Part440, Subpart A and in sections 1902, 1905, and1915 of the Act.
(ii) Nurse-midwife services listed in section1905(a)(17) of the Act, are provided to theextent that nurse-midwives are authorized topractice under State law or regulation andwithout regard to whether the services arefurnished in the area of management of the careof mothers and babies throughout the maternitycyc1 e. Nurse-mi dwi ves are permitted to enterinto independent provider agreements with theMedicaid agency without regard to whether thenurse-midwife is under the supervision of, orassociated with, a physician or other healthcare provider.
Not applicable. Nurse-midwives are notauthorized to practice in this State.
(iii) Prenatal care and delivery services for pregnantwomen.

Revision: HCFA-PM-91- 4AUGUST 1991
State/Territory:
(BPD)
New Jersey
OMB No.: 0938-
3.1(a)(2)Citation
42 CFR 440.140,440.150,Subpart B,442.441,Subpart C1902(a)(20)and (21) of the Act
Amount, Duration, and Scope of Services:Medically Needy (Continued)
(iii) Pregnancy-related, including familyplanning services, and postpartum services fora 60-day period (beginning on the day thepregnancy ends) and any remaining days in themonth in which the 60th day falls are providedto women who, while pregnant, were eligiblefor, applied for, and received medicalassistance on the day the pregnancy ends.
~(iv) Services for any other medical condition thatmay complicate the pregnancy (other thanpregnancy-related and postpartum services) areprovided to pregnant women.
(v) Ambulatory services, as defined in ATTACHMENT3.1-B, for recipients under age 18 andrecipients entitled to institutional services.
~/ Not applicable with respect to recipientsentitled to institutional services; theplan does not cover those services forthe medically needy.
(vi) Home health services to recipients entitled tonursing facility services as indicated in item3.1(b) of this plan.
f-/(vii)Services in an institution for mentaldiseases for individuals over age 65 ..
f-/(viii)Services in an intermediate carefacility for the mentally retarded.
TN No. 91- ':j.rl F£8 :3 lQ92supersedesTApproval Date _
TN No. '87- ItJEffective Date OCT 0 J 1S91
HCFA ID: 7982E
Revision: HCFA-PM-92- 7October 1992
State/Territory:
(MB)
2Gb
New Jersey
OFFICIAL
Citation 3.1(a)(2) Amount, Duration, and Scope of Services:Medically Needy (continued)
1902(e)(9) ofthe Act
1905(a) (23)and 1929
(ix)
(x)
Respiratory care services are providedto ventilator dependent individuals asindicated in item 3.1(h) of this plan.
Home and Community Care for Functionally DisabledElderly Individuals, as defined, described andlimited in Supplement 2 to Attachment 3.1-A andAppendices A-G to Supplement 2 to Attachment 3.1-A.
ATTACHMENT 3.1-8 identifies the services provided to each coveredgroup of the medically needy; specifies all limitations on theamount, duration, and scope of those items; and specifies theambulatory services provided under this plan and any limitationson them. It also lists the additional coverage (that is inexcess of established service limits) for pregnancy-relatedservices and services for conditions that may complicate thepregnancy.
TN No. 9If - '.3SupersedesTN No. --.:J 3 - :3,S
Approval Date AUG 1 5 1994 Effective Date APR 1 - 199(

20-C
State of ew JersevPACE State Plan Amendment Pre-Print
Citation 3.1 (a)(2) Amount, Duration, and Scope of Services: Medically Needy (Continued)1905(a)(26) and 1934
Program of All-Inclusive Care for the Elderly (PACE) services, as described andlimited in Supplement 3 to Attachment 3.t-A.
AITACHMENT 3.I-B identifies services provided to each covered group of themedically needy. ( ote: Other programs to be offered to Medically Needybeneficiaries would specify all limitations on the amount, duration and scope ofthose services. As PACE provides services to the frail elderly population withoutsuch limitation, this is not applicable for this program. In addition, otherprograms to be offered to Medically Needy beneficiaries would also list theadditional coverage -that is in excess of established service limits- forpregnancy-related services for conditions that may complicate the pregnancy. AsPACE is for the frail elderly population, this also is not applicable for thisprogram.)
07-02-MA (NJ)
T 07-02~~\r: ~ 2> ·I~~
Approval Date '__"_'_
Supersedes TN _~9'..Q8'.:.-1!.:4!- Effective Date SfP__2_"_7--=..:200:..::.:1
Revision: HCFA-PM-97-3December 1997
(CMSO)
21
State:
Citation
New Jersey
3.1 Amount, Duration, and Scope of Services (continued)
(iii)Other Reauired Special Groups: QualifvingIndividuals - 1
(a) (4) (i) O~er Required Special Groups: QualifiedDisabled and Working Individuals
DMAHS1902 (a) (10) (E) (i)and clause (VIII)of the matterfollowing (F),and 1905 (p) (3)of the ActDMAHS1902 (a) (10)(E) (ii) and1905(s) of theAct
D~.AHS
1902 (a) (10)(E) (iii) and1905 (p) (3) (7-1.) (ii)
..... of the Act
DMAHS1902 (a) (10)
(E) (iv) (I) 1905 (p) (3)(A) (ii) I and 1933 ofthe Act
OFfiCiAl
(a) (3) O~~er Required Special Groups: QualifiedMedicare Beneficiaries
Medicare cost sharing for qualifiedMedicare beneficiaries described insection 1905(p) of the Act is providedonly as indicated in item 3.2 of thisplan.
Medicare Part A premiums. for qualifieddisabled and working individualsdescribed in section 1902 (a) (10) (E) (ii)
of the Act are provided as indicated initem 3.2 of this plan.
(ii) O~~er Required Special Groups: SpecifiedLow-Income Medicare Beneficiaries
Medicare Part B premiums for specifiedlow-income Medicare beneficiariesdescribed in section 1902 (a) (10) (E) (iii)of the Act are provided as indicated initem 3.2 of this plan.
Medicare Part B premiums for qualifyingindividuals described in1902 (a) (10) (E) (iv) (I) and subject to 1933of the Act are provided as indicated initem 3.2 of this plan.
98-9-MA- (NJ)
TN No. '\ \ - '\
Supersedes Approval DateTN No. <A '\ - , "-\
JU~ 2Effective Date
.. 21 ContinuedRevision: HCFA-PM-97-3 (CMSO)
December 1997State: New Jersey
DMAHS1902 (a) (10)(E) (iv) (II), 1905 (p) (3)(A) (iv) (II), 1905 (p) (3)the Act
DMAHS1925 of theAct
(a) (5)
(iv) Other Required Special Groups: QualifyingIndividuals - 2
The portion of the amount of increase tothe Medicare Part B premium attributableto the Home Health provisions forqualifying individuals described in1902 (A) (10) (El (iv) (II) and subject to1933 of the Act are provided as indicatedin item 3.2 of this plan.
Other Required Special Groups: FamiliesReceiving Extended Medicaid Benefits
Extended Medicaid benefi ts for familiesdescribed in section 1925 of the Act areprovided as indicated in item 3.5 of thisplan.
Off\t~l
98-9-MA- (NJ)
TN No.
superse1is. Approval DateTN No. -n-ew-
Effective DateJAM 1 1998
Revision: HCFA-PM-91, 1991
State/Territory:
21a
(BPD)
,el'; 'Jel'sey
OFFICIALOMS No.: 0938-
3. 1 Amoun~_,Duration, and Scope of Services (Continued)
Sec. 245A(h)of theImmigration andNationality Act
(a)(6) Limited Coverage for Certain Aliens
(i) Aliens granted lawful temporary residentstatus under section 245A of the Immigrationand Nationality Act who meet the financial andcategorical eligibility requirements under theapproved State Medicaid plan are provided theservices covered under the plan if they--
(A) Are aged, blind, or disabled individuals asdefined in section l614(a)(I) of the Act;
(B) Are children under 18 years of age; or
(C) Are Cuban or Haitian entrants as defined insection SOl(e)(I) and (2)(A) of P.L. 96-422in effect on April 1, 1983.
(ii) Except for emergency services andpregnancy-related services, as defined in 42CFR 447.53(b) aliens granted lawful temporaryresident status under section 245A of theImmigration and Nationality Act who are notidentified in items 3.l(a)(6)(i)(A) through (C)above, and who meet the financial andcategorical eligibility requirements under theapproved State plan are provided services underthe plan no earlier than five years from thedate the alien is granted lawful temporaryresident status.
TN No. qZ-j5Supersedes a ApprovalTN No. '67- D
Date FEB ! 11 1092 Effective Date
HCFA ID: 7982E
OCT 1 1931

Revision: HCFA-PM-9l-,\'(:;'ST 1991
(BPD)
2lbOffiCIAL
OMB No.: 0938-
State/Territory: '_ie_\_~_0_'e__r_s_e~y __
Citation 3.1 (a) (6) Amount, Duration, and Scope of Services: LimitedCoverage for CeJtain Aliens (continued)
1902(a) and 1903(v)of the Act
1905(a)(9) ofthe Act
1902(a)(47)and 1920 ofthe Act
42 CFR 441.5550 FR 436541902(a) (43),1905(a) (4) (B),and 1905(r) ofthe Act
(iii) Aliens who are no~ lawfully admitted forpermanpnt residence or otherwise permanentlyresiding in the United States under color oflaw who meet the eligibility conditions underthis plan, except for the requirement forreceipt of AFDC, 551, or a State supplementarypayment, are provided Medicaid only for careand services necessary for the treatment of anemergency medical condition (includingemergency labor and delivery) as defined insection 1903(v)(3) of the Act.
(a)(7) Homeless Individuals.
Clinic services furnished to eligibleindividuals who do not reside in a permanentdwelling or do not have a fixed home or mailingaddress are provided without restrictionsregarding the site at which the services arefurnished.
(a)(8) Ambulatory prenatal care for pregnantwomen is provided during a presumptiveeligibility period if the care is furnished by aprovider that is eligible for payment under theState plan.
(a)(9) EPSDT Services.
The Medicaid agency meets the requirements ofsections 1902(a)(43), 1905(a)(4)(B), and1905(r) of the Act with respect to early andperiodic screening, diagnostic, and treatment(EPSDT) services.
TN No. 17-35Supersedes Approval DateTN No. -Ne.. f1Ip\;n
FEe" 1\ ~mEffective Date
He FA I D: 7982 E
OCT 1 lS91

Revision: HCFA-PM-911991-.
(BPD)
22
OMB No.: 0938- OFFfC!~t
State: "-'N~e..:.!w....J~e~rs~eJ_.y _
Citation
42 CFR 441.60
3. 1(a)(9)
-IXJ
Amount, Duration, and Scope of Services: EPSDTSennces(continued)
The Medicaid agency has in effect agreements with continuing careproviders. Described below are the methods employed to assure theproviders' compliance with their agreements.......
42 CFR 440.240and 440.250
(a)(10) Comparability of Sennces
1902(a) and 1902(a)( 10), 1902(a)(52),1903(v),1915(g),1925(b)(4), and 1932of the Act
. *J!>escribed here:
-/ /
Except for those items or services for which sections1902(a), 1902(a)(10), 1903(v), 1915, 1925, and 1932 of theAct, 42 CFR 440.250, and section 245A of theImmigration and Nationality Act, permit exceptions:
(i) Services made available to the categorically needy are equal inamount, duration, and scope for each categorically needy person.
(ii) The amount, duration, and scope of sennces made available to thecategorically needy are equal to or greater than those madeavailable to the medically needy.
(iii) Services made available to th~ "medically needy are equal inamount, duration, and scope for each person in amedically needy coverage group.
(iv) Additional coverage for pregnancy-related service andservices for conditions that may complicate the pregnancy are equalfor categorically and medically needy.
The Agency and/or its Fiscal Agents, will monitor a sample of claims,conduct peer review, make recommendations to physician casemanagers, review physician profiles, and conduct a survey of fee-forservice Medicaid patients.
03-07-MA eNJ)
TN # -"'-0""-3--"'-0-'---7 _.........;upersedes TN #_9~1~-.:=...3",-5 _
. AUG 1 3 2003Effective Date MAR 1 1 2004Approval Date _
23
Revision: F.C:A-AT-80-38 (BPP)May 22, 1980
I::.. "" -.(." .'~...l' .' :.:.
_..---.~-
NEloJ JERSEYState-------------------------Citation
. 42 CFR Part440, Sul:part B42 ~ 441.15Kr-i8-90Kr-BO-34
3.1 (b) Hone health services are provided inac::ordance with the requirements of 42 CFR441.15.
(1) Hone health services are provided toall categorically needy individuals21 years of a;:;e or (Ner.
(2) Hane health services are provided toall categorically needy L'1dividualsunder 21 years of age.
a 1 Yes
U Not applicable. The State ?landoes not provide for skillednursing facility services forsuch individuals.
(3) Hane health services are provided tothe medically needy:
I .
~.~
".' '. -- '.;_:'-~=.: L~" _
......
!Y'
U
ou:-,L.
Yes, to all
Yes, to individuals age 21 orover; SNFservices are provided
Yes, to individuals under age21; SNF services are provided
No; SNF services are rot provided
Not applicable; the medicallyneedy are rot included \IDderthis plan
I.·· .••
~:-....~~ .L~"
.. ;
'IN ~(p.::J!LSUPersedesW- #1J'1-lg
Approval Date JUL. 2 3 1986 Effective DatE'..lJL. 1 1986
I
Revi si on: "HCFA- PM-·93-24
(BPO)
OFFICIAL
Citation
State/Territory H~ew~~Je~rus~e~y __
3.1 Amount. Duration and Scope of Services (continued)
42 CFR 431.53
42 CFR 483.10
(c)(l) Assurance of Transportation
Provision is made for assuring necessarytransportation of recipients to and fromproviders. Methods used to assure suchtransportation are described in ATTACHMENT 3.1-0.
(c)(2) Payment for Nursing Facility Services
The State includes in nursing facility services atleast the items and services specified in 42 CFR483.10(c}(8}(i}.
TN No .__C/~3,,--....::3~7_-:--_Supersedes Approva1 Date JAN 12 1994TN No. Q(-3S
93-37 -MA (HJ). OCT 1 - 1993Effective Oate _
25
Revision: B:?A-;;T-80-38 (BPP)May 22, 1980
NE\oi JERSEYState-------------------------Citaticn42 CPR 440.260Nr-78-90
3.1(d) Methods ard Standards to AssureQuality of Services
The standards established and themethods used to assure high qualitycare are descr ibed in ATrAOlMENI' 3.1-<:.
~. •. ',,:<, •
': ",,;.,"
f:.>.-.;-:::'.:.".r..·~·";.!"";·· .. •
.'
'IN # 71. -11r.Supersedes
.... IN # 74-11Afproval Date ~- 9 - 77 Effective Date /tJ-I-7t..
• • 1 ., ••
NE\·J JERSEY
26
Revision: HC2A-.~-80-38{BPP)
~y 22, 1980
State-------------------------
."~.~;: '.':'~'~.~;.
."
.','
Citaticn42 ern 441. 20AT-78-90
3.1{e) Familv Planning Services
The requirements of 42 CPR 441.20 are metregarding freeecm from coercion or pressureof rniOO and OJnscience, and freedom ofchoice of·method to be used for familyplanning.
. ..... :..
.; ..... .: ' ..
-',
'IN ~ 7, -/~supersedes
~ j.N # 74-11Approval Date 8- 9- 77 Effective Date 10-1-7"
Revision: HCFA-PM-87- 5APRIL 1987
27
(BERC) OKE No.: 0938-0193
state/Territory: NEW JERSEY
Citation42 CFR 441. 30AT-78-90
1903(i)(1)of the Act,P.L. 99-272(Section 9507)
3.1 (f) (1) optometric Services
optometric services (other than those providedunder 55435.531 and 436.531) are not now butwere previously provided under the plan.Services of the type an optometrist is legallyauthorized to perform are specifically includedin the term "physicians' services" under thisplan and are reimbursed whether furnished by aphysician or an optometrist.
1..1/ Yes.
/ / No. The conditions described in the firstsentence apply but the term "physicians'services" does not specifically includeservices of the type an optometrist islegally authorized to perform.
/ / Not applicable. The conditions in thefirst sentence do not apply.
(2) Organ Transplant Procedures
Organ transplant procedures are provided.
L/ No.
/X/ Yes. Similarly situated individuals aretreated alike and any restriction on thefacilities that may, or practitioners whomay, provide those procedures is consistentwith the accessibility of high quality careto individuals eligible for the proceduresunder this plan. Standards for thecoverage of organ transplant procedures aredescribed at ATTACHMENT 3.1-E.
TN No. 81, IiSupersedesTN No. '7b' Ito
Approval Date SEP. 2 1981 Effective Date A",-P"",R__i.j..-l.1<IJ9Bu..7l-
HCFA ID: 1008P/0011P
tr u.s. GOVERNMENT PRINTING OFFICE' 987- 1 8 1 - 2 7 0 I 6 0 1 7 4
Revision: HCFA-PH-87-4KARCH 1987
(BERC) OMB No.: 0938-0193
state/Territory: NEW JERSEY
Citation42 CFR 431.110(b)AT-78-90
1902(e)(9) ofthe Act,P.L. 99-509(Section 9408)
3.1 (g) Participation by Indian Health Service Facilities
Indian Health Service facilities are accepted asproviders, in accordance with 42 CFR 431.110(b), onthe same basis as other qualified providers.
(h) Respiratory Care Services for Ventilator-DependentIndividuals
Respiratory care services, as defined insection 1902(e)(9)(C) of the Act, are providedunder the plan to individuals who--
(1) Are medically dependent on a ventilator forlife support at least six hours per day;
(2) Have been so dependent as inpatients during asingle stay or a continuous stay in one or morehospitals, SNFs or ICFs for the lesser of--
L-/ 30 consecutive days;
L-/ days (the maximum number of inpatientdays allowed under the State plan);
(3) Except for home respiratory care, would requirerespiratory care on an inpatient basis in ahospital, SNF, or ICF for which Medicaidpayments would be made;
(4) Have adequate social support services to becared for at home; and
(5) Wish to be cared for at home.
I I Yes. The requirements of section 1902(e)(9) of theAct are met.
LY Hot applicable. These services are not included inthe plan.
TN No. 8t[ '·1'1SupersedesTN No. .-1L:~r{
Approval Date SEP. 2 1981 Effective Date APR. 1 19B7
HCFA 10: 1008P/0011P
29
(MB)~CFA-PM-9J-5
~IAY 199)New Jersey
State:
Revi.sion:
Citation 3.2 Coordination of Medicaid Nith Medicare and OtherInsurance
(a) Premiums
(1) Medicare Part A and Part B
1902(a)(10)(E)(i) and1905(p)(1) of the Act
(i) Qualified Medicare Beneficiary(QMB)
The Medicaid agency pays MedicarePart A premiums (if applicable) andPart B premiums for individuals inthe QMB group defined in Item A.25 ofATTACHMENT 2.2-A, through the grouppremium payment arrangement, unlessthe agency has a Buy-in agreement forsuch payment, as indicated below.
Buy-In agreement for:
Part A X Part B
The Medicaid agency payspremiums, for which thebeneficiary would be liable, forenrollment in an HMOparticipating in Medicare.
TN No. 93-aS FEB 2supersedesa~_ILL Approval Date - 1994TNNO.~
Effective Date OCT 1 - 1993

Revision: HCFA-PM-97-3December 1997
(CMSO)
29a
State: New Jersey
CitationDMAHS1902 (a) (10) (E) (ii)
and 1905(s) of the Act
DMAHS1902 (a) (10) (E) (iii)and 1905 (p) (3) (A) (ii)of the Act
DMAHS1902 (a) (10) (E) (iv) (I) ,
-.. 1905 (p) (3) (A) (ii), and1933 of the Act
(ii) Qualified Disabled and WorkingIndividual (QDWI)
The Medicaid agency pays MedicarePart A premiums under a grouppremium payment arrangement, subjectto any contribution required asdescribed in ATTACHMENT 4.18-E, forindividuals in the QDWI groupdefined in item A.26 of ATTACHMENT2.2-A of this plan.
(iii) Soecified Low-Income MedicareBeneficiary (SLMB)
The Medicaid agency pays MedicarePart B premiums under the State buyin process for individuals in theSLMB group defined in item' A.27 ofATTACHMENT 2.2-A of this plan.
(iv) Qualifying Individual-1(QI-1)
The Medicaid agency pays MedicarePart B premiums under the State buyin process for individuals describedin 1902 (a) (10) (E) (iv) (I) and subjectto 1933 of the Act.
DMAHS1902 (a) (10) (E) (iv) (II) ,
1905(p) (3) (A) (ii), and1933 of the Act
(v) Qualifying Individual-2(QI-2)
The Medicaid agency pays the portionof the amount of increase to theMedicare Part B premium attributableto the Home Health Provision to theindividuals described in 1902 (a) (10)(E) (iv) (II) and subject to 1933 of theAct.
___nn\t.~\. 98-9-MA- (NJ)
TN No. ~ ~ - '\SupersedesTN No. C\ '1-\-;-
Approval Date,tS,
Effective Date~Il 1991
Revision: HCFA-PM-97-3December 1997
(CMSO)
29b
State:
CitationDMAHS1843(b) and 1905(a)of the Act and42 CFR 431. 625
...... DMAHS1902 (a) (30) and1905(a) of the Act
New Jersey
(2)
(vi) Other Medicaid Recipients
The Medicaid agency pays MedicarePart B premiums to make MedicarePart B coverage available to thefollowing individuals:
x All individuals who are: (a)receiving benefits under titlesI, IV-A, X, XIV, or XVI (AABDor SSI); b) receiving Statesupplements under title XVI; orc) within a group listed at 42ern 431.625 (d) (2) .
x Individuals receiving title IIor Railroad Retirementbenefits.
Medically needy individuals(FFP is not available for thisgroup) .
Other Health Insurance
x The Medicaid agency pays insurancepremiums for medical or any other type ofremedial care to maintain a third partyresource for Medicaid covered servicesprovided to eligible individuals (exceptindividuals 65 years of age or older anddisabled individuals, entitled to MedicarePart A but not enrolled in Medicare PartB) .
OFFICIAl98-9-MA- (NJ)
TN No. d\~ - '\... Supersedes Approval Date
TN No. f\~-\'-\
JUN Z 1998Effective Date JAM 1 1988

OFFlC\Al2C?c
(M3)
State:
Revision: HC?A-?~-q3-~
MA Rc. H 1'\13
NEW JERSEY
1902(a)(30),1902(n),1905(a),and 1916 0: the Ac~
SU~C~2~ent : ~~ AT7ACE~E~T 4. :9-3desc~~~es ~~e ~ethods ane standa~cs :c~
escablishi~g ~aymen~ cates for se~~~ces
ccve~ed under ~edLcare, ane/o~ ~~e
met~odclo~J fcr payment of Med~care
deduct~ble and coinsurance amounts, ~o ~~e
extent ava~laDle for each of the follow~n~
groups.
Sections 1902(a) ( 10) (E) ( i) and1905(p)(3) of the Act
(i) Qualified Medicare Beneficiaries(QM3S)
The Medicaid agency pays MedicarePart A and Part B deductible andcoinsurance amounts for QMBs(subject to any nominal Medicaidcopayment) for all servicesavailable under Medicare.
1902(a) (10), 1902(a) (30),and 1905(a) of the Act
(ii) Other Medicaid Recipients
The Medicaid agency pays forMedicaid services also covered underMedicare and furnished to recipientsentitled to Medicare (subject to anynominal Medicaid copayment). Forservices furnished to individualswho are. described in section3.2(a)(1)(iv), payment is made asfollows:
42 CFR 431. 625 For the entire range ofservices available underMedicare Part B.
X Only for the amount, duration,and scope of services otherwiseavailable under this plan.
1902(a)(10), 1902(a)(30),1905(a), and 1905(p)of the Act
(iii) Dual Eligible--QMB plus
The Hedicaid agency pays MedicarePart A and Part B deductible andcoinsurance amounts for all servicesavailable under Medicare and paysfor all Medicaid services furnishedto individuals eligible both as QHBsand categorically or medically needy(subject to any nominal Medicaidcopayment).
TN No.~ 6 nM--. Supersedes (J L":2 L Approval Date MAY 2 1'3~TNNO.~
Effective Date JAN 1- 1993
Revision: HCFA-PM-91-8October 1991
State/Territory:
(MB)
New Jersey
OMB No.:
Citation Condition or Requirement
1906 of theAct
1902(a) (10) (F)of the Act
(c) Premiums, Deductibles, Coinsuranceand Other Cost Sharing Obligations
The Medicaid agency pays allpremiums, deductibles, coinsuranGe andother cost sharing obligations for itemsand services covered under the Stateplan (subject to any nominal MedicaidcopaYffient) for eligible individuals inemployer-based cost-effective grouphealth plans.
When coverage for eligible familymembers is not possible unlessineligible family members enroll, theMedicaid agency pays premiums forenrollment of other family members whencost-effective. In addition, theeligible individual is entitled toservices covered by the State plan whichare not included in the group healthplan. Guidelines for determining costeffectiveness are described in section4.22(h).
(d) /---/ The Medicaid agency pays premiumsfor individuals described in item19 of Attachment 2.2-A.
TN No.Superce es Approval Dat9CT 15 1992TN No. i&~ew
Effective Date JUL 1~' 1981HCFA ID: 7983E

NE\~ JERSEY
30
qevision: HCFA-.~-80-3S(BFP)
May 22, 1980
State-------------------------Cit::ltirn42 CPR 441.101,42 CFR 431.620(c)and (d)AT-79-29
3.3 Med.iC::lid for Individuals Aqe 65 or Over inInstitutions for ~~~tal Diseases
MediC::lid is provided for individuals 65 yearsof age or older who are patients ininstitutions for mental diseases.
LxI Yes. The requirements of 42 CPR Part 441,Sutpart C, and 42 CPR 431.620 (c) and (d)are met.
U Not: acolicable. c1ed.icaid is not providedto aged individuals in suc~ institutionsunder this plan.
":.'•..- ........ -,- ....
,~•. '1":, • ...
'IN # 7d:J - ItoSupersedes
.'-'" 'IN * 74 - 9Awroval Date i- 9- '7 Effective Date/o -1-7~
31
Revision: ECFA-AT-80-38 (BPP)May 22, 1980
'.r~..t~.,;, J, ~
~. '.". ~."'
NEVI JERSEYState------------------------Cit=.tion42 ern 441. 252NJ:-78-99
3.4 Soecial Reauirements .1\cplicable toSterilization Procedures
All requirements of 42 CPR Part 441, Subpart Fare met.
.... ',...
'IN # 79-~Supersedes
~ 'IN *7' -It.Afproval Date 3-;U.- 79 Effective Date3-K-79
Revision: HCFA-PM-91'< 1991
(BPO)
31a OFFICIALOMS No.: 0938-
Citation1902(a)(52)and 1925 ofthe Act (a) Services provided to families during the first
6-rnonth period of extended Medicaid benefits underSection 1925 of the Act are equal in amount,duration, and scope to services provided tocategorically needy AFDC recipients as described inATTACHMENT 3.1-A (or may be greater if providedthrough a caretaker relative employer's healthinsurance plan).
(b) Services provided to families during the second6-month period of extended Medicaid benefits undersection 1925 of the Act are--
LXI Equal in amount, duration, and scope toservices provided to categorically needy AFDCrecipients as described in ATTACHMENT 3.1-A (ormay be greater if provided through a caretakerrelative employer's health insurance plan).
Equal in amount, duration, and scope toservices provided to categorically needy AFDCrecipients, (or may be greater if providedthrough a caretaker relative employer's healthinsurance plan) minus anyone or more of thefollowing acute services:
LI Nursing facility services (other thanservices in an institution for mentaldiseases) for individuals 21 years of age orolder.
LI Medical or remedial care provided bylicensed practitioners.
LI Home health services.
TN No. 97 "3.;2supersedes7~ Approval DateTN No. _J.-!l:
FEB! 6 1WlEffective Date ~O~C~I__~1~1~9.91~ _
HCFA ID: 7982E
Revision: HCFA-PM-91- i.
AU~CST 1991
State:
31b
(BPD)
:ie'.., Jersey
OfFICIALOMB No.: 093::'-
3.5 Families Receiving Extended Medicaid Benefits(Continued)
1-/ Private duty nursing services.
1-/ Physical therapy and related services.
1-/ Other diagnostic, screening, preventive, andrehabilitation services.
1-/ Inpatient hospital services and nursingfacility services for individuals 65 yearsof age or over in an institution for mentaldiseases.
1-/' Intermediate care facility services for thementally retarded.
1-/ Inpatient psychiatric services forindividuals under age 21-
1-/ Hospice services.
1-/ Respiratory care services.
1-/ Any other medical care and any other type ofremedial care recognized under State law andspecified by the Secretary.
Effective Date ~O~C~T~_1~1~99~1-----
TN No. 27-Jo:-Supersedes Approval DateTN No. qO·2,
HCFA 10: 7982E

Revision: HCFA-PM-9l--.AL'CTST 1991
State:
3lc
(BPO)
flew Jersey
OFFICIALOMB No.: 0938-
Citation 3.5 Families Receiving Extended Meaicaid Benefits(Continued)
(c)L/ The agency pays the family's premiums, enrollmentfees, deductibles, coinsurance, and similar costsfor health plans offered by the caretaker'semployer as payments for medical assistance--
L/ 1st 6 months L/ 2nd 6 months
L/ The agency requires caretakers to enroll inemployers' health plans as a condition ofeligibility.
L/ 1st 6 mos. L/ 2nd 6 mos.
(d)LI (1) The Medicaid agency provides assistance tofamilies during the second 6-month period ofextended Medicaid benefits through thefolloWing alternative methods:
LI Enrollment in the family option of anemployer's health plan.
L/ Enrollment in the family option of a Stateemployee health plan.
LI Enrollment in the State health plan for theuninsured.
LI Enrollment in an eligible health maintenanceorganization (HMO) with a prepaid enrollmentof less than 50 percent Medicaid recipients(except recipients of extended Medicaid).
TN No. 9 1-..71;;-supersedesU {)_ L Approval DateTN No. :L Ir;d
FEB 2 1\ 1m OCT 1991Effective Date __~~~1~~ _
HCFA ID: 7982E
Revision: HCFA-PM-91-4 (BPD)August 1991
31d
OMB No.: 0938-
State: New Jersey
Citation 3.5 Families Receiving Extended Medicaid Benefits(Continued)
Supplement 2 to Attachment 3.1-A specifies and describesthe alternative health care plan(s) offered, includingrequirements for assuring that recipients have access toservices of adequate quality.
(2) The agency--
(i) Pays all premiums and enrollments fees imposed on thefamily for such plan(s).
D
3.6
D
(ii) Pays all deductibles and coinsurance imposed on thefamily for such plan(s).
Unemployed Parent
For purposes of determining whether a child is deprived onthe basis of the unemployment of a parent, the agency--
uses the standard for measuring unemployment which wasin the AFDC State plan in effect on July 16, 1996.
uses the following more liberal standard to measureunemployment:
The total of earned and unearned income does not exceedthe AFDC income standards.
(\fHt\~l
99-10-MA
<q '\-\~) 'I
_~" ....-~41;_:, '"" \ ',-,. I _.JUN I 5 f99S
Supersedes ·(N

31e
1_/ Enrollment ~~ ~~ eligi~le
health maifi~e~~nce
organization (HMO) that has anenrollment of less than 50percent of Med~caid recipientswho are not recipients ofextended Medicaid.
Supplement 2 to ATTACHME~~ 3.1-Aspecifies and describes thealternative health care plan(s)offered, including requirements forassuring that recipients haveaccess to services of adequatequality.
(2) The agency--
(i) Pays all premiums andenrollment fees imposed on thefamily for such plants).
/ / (ii) Pays all deductibles andcoinsurance imposed on thefamily for such plants).
JUL 2D 1990
APR 0 1 1990
Approval Date--------------
Effective Date
;upersedes TN----'--------

Revision: HCFA-PK-87-4MARCH 1987
(BERC)
32
OKB No.: 0938-0193
State/Territory: NEW JERSEY
Citation42 CFR 431.15AT-79-29
SECTION 4 - GEHERAL PROGRAM ADMINISTRATION
4.1 Methods of Administration
The Medicaid agency employs methods of administrationfound by the Secretary of Health and Human Services tobe necessary for the proper and efficient operation ofthe plan.
I'N No. 91-/'lSupersedesTN No. lIft· i;a
Approval Date SEP. 2 1981
..
Effective Date APR. 1 1981
HCFA ID: 1010P/0012P
"' ..
... ' , ....~
NE\~ JERSEYState------...;..;.;:~=:.=.:=-'---------------
33
Revisicn: HC.?A-AT-80- 38 (BPP)May 22, 1980
Citaticn42 ern 431. 202AT-79-29AT-80-34
4.2 Hearinc;s for Aoolic::mts and Re::ioients
The MediC3.id agency has a system of hearingsthat meets all the require.'1Ients of 42 em Part431, Subpart E.
-:....- .. ---- .....--
'IN # 74 -~Super3edes'ill # 74 - I
Approval Date 4 - 1~-7S'" Effective Date" -3 -7~

Page 33.
stat•. N_ew~J;..;e"""r ....se.;;.Yr--. _
,,1tationJ
~L 101-508
Section 4724
TN NO. q@-IJ[~~~lHl'
SUPERSEDES TN NO. ~ ~~ 'tYw i
Service. Durinq Appeal
The State shall continue to providemedical assistance until a finaldetermination of disability orblindness is made by SSA in tho••cases where a state determination ofdisability or blindness I IlIAd. inaccor~ance with section 1614(a) ~fthe Social Security act, was reversedby a SUbsequent SSA decision.
YES
CJ NO
OCT 8 1992APPROVAL DATE---------EFFECTIVE· DATE~UL '1- 19~

state/Territory:
'-'"r. _. . .- ..
Revision: HCFA-AT-87-9AUGUST 1987
(BERC)
NEW JERSEY
OKB No.: 0938-0193
"-,'.0'
.,-" to,'\, .. '
~, .
-,, '
0-
, .....:' ~ ..
citation42 CFR 431.301AT-79-29
52 FR 5967
4.3 ~,afeguarding Information on Applicants and Recipients
Under state statute which imposes legal sanctions,safeguards are provided that restrict the use ordisclosure of information concerning applicants andrecipients to purposes directly connected with theadministration of the plan.
All other requirements of 42 CFR- Part 431, Subpart Fare met.
TY Yo. 8.1- a"bSupersedesTY No. 1.!i::..1I
Approval Date J__AN 2_9 '_990 Effective Date
HCFA ID:
lb;. 1'8~I I
1010Pl0012P

Revision: HCFA-PM-87-4KARCH 1987
(BERC) OMB No.: 0938-0193
state/Territory: NEW JERSEY
Citation42 CFR 431.800(c)50 FR 218391903(u) (1) (D) ofthe Act.P.L. 99-509(Section 9407)
4.4 Medicaid Quality Control
(a) A system of quality control is implemented inaccordance with 42 CFR Part 431. Subpart P.
(b) The state operates a claims processing assessmentsystem that meets the requirements of 431.800(e).(g). (h~(k).
(r) *'L/ Yes.
/ ij Not applicable. The State has an approvedMedicaid Management Information System (MMIS).
1 1981TN No. 87"1'/SupersedesTN No.
Approval Date _SE_P_,__2_._U3_81 Effective Date APR.-----HCFA ID: 1010P/0012P
36
Revision: HCrA-PK-88-10 (BERC)SEPTEKB!R 1988
OFFICIALOM! Ho.: 0938-0193
State/Territory: New Jersey
\------ .
II
I,
I'I.<1
10iT'
II;;!'I
I
J
Citation42 en 455.12AT-78-9048 FR 374252 Fa 48817
TIl Ho. 'a~-31
Super••d••nT 110. ~Lf
4.5 Medicaid Aleney Fraud Detection and InvestisationProsram
The Medicaid asency has established and will maintainmethods, criteria, and procedures that meet allrequirements of 42 crR 455.13 throush 455.21 and 455.23for prevention and control of prosram fraud and abuse.
Approval Date JAN 19 19891ffective Date OCT 1 1988
HcrA 10: 1010P/0012P

Section 4.5 Page 1
STATE PLAN UNDER TITLE XiX OF THE SOCIAL SECURITY ACT STATE OF NEW JERSEY
4.5 Medicaid Recovery Audit Contractor Program
Citation
Section 1902(a)(42)(B)(i)
of the Social Security Act
x
NA
The State has established a program under which it will contract
with one or more recovery audit contractors (RACs) for the
purpose of identifying underpayments and overpayments of
Medi-::aid claims under the State plan and under any waiver of the
State plan.
The State is seeking an exception to establishing such program
for the following reasons:
Section 1902(a)(42)(B)(i i)( I)
of the Act
x The State/Medicaid agency has contracts of the type(s) listed in
section 1902(a)(42)(B)(ii)(l) of the Act. All contracts meet the requirements of the statute. RACs are consistent with the
statute.
Place a check mark to provide assurance of the following:
X The State will make payments to the RAC(s) only from amounts
recovered.
X The State will make payments to the RAC(s) on a contingent
Basis for collecting overpayments.
Section 1902 (a )(42)( B)(ii)( II Haa)
of the Act
The following payment methodology shall be used to determine State
payments to Medicaid RACs for identification and recovery of
overpayments (e.g., the percentage of the contingency fee):
(rate has not yet been determined)
x The 5tate attests that the contingency fee rate paid to the
Medi:aid RAC will not exceed the highest rate paid to Medicare
RACs, as published in the Federal Register.
NA The State attests that the contingency fee rate paid to the Medicaid RAC will exceed the highest rate paid to Medicare
RACs, as published in the Federal RegisteL The State will only
submit for FFP up to the amount equivalent to that published
rate.
NA The contingency fee rate paid to the Medicaid RAC that will
exceed the highest rate paid to Medicare RACs, as published in
the Federal Register. The State will submit a justification for that
TN No. -=10=---=1=-3 _ .Frs .2 3 "UN superse~des ApprovaIDate: __~ __ Effective Date: 12/30/10 TN No. NE
~;

Section 4.5 Page 2
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
STATE OF NEW JERSEY o..m~f'IlL '"'''I ~.JrF.l c~~ .\JC...
4.5 Medicaid Recovery Audit Contractor Program
rate and will submit for FFP for the full amount of the contingency fee.
Section 1902 (a)(42)(B)(iiJ(lI)(bb) of the Act
X The following payment methodology shall be used to determine State payments to Medicaid RACs for the identification of underpayments (e.g., amount of flat fee, the percentage of the contingency fee): CO'1tingency based on underpayments identified.
Section 1902 (a)(42)(B)(ii)(lIl)
of the Act X The State has an adequate appeal process in place for entities
to appeal any adverse determination made by the Medicaid I Section 1902 (a)(42)( B)(ii)(lV){aa) RAC(s). I of the Act
X The State assures that the amounts expended by the State to carry out the program will be amounts expended as necessary for the proper and efficient administration of the State plan or a waiver of the plan.
ISection 1902(a)(42J(B}(ii)(IV(bb)
of the Act
X The State assures that the recovered amounts will be subject to a State's quarterly expenditure estimates and funding of the State's share.
Section 1902 (a)( 42)( B)(iiJ( IV}(cc) Of the Act
X Efforts of the Medicaid RAC(sl will be coordinated with other contractors or entities performing audits of entities receiving payments under the State plan or waiver in the State, and/or State and Federal law enforcement entities and the eMS Medicaid Integrity Program.
--
Approval Date: _ Effective Date: 12/30/10
36a
Revision: HCFA-PM-99-3 (CMSO)JUNE 1999
State: New Jersey
CitationSection 1902(a)(64) ofthe Social Security ActP.L. 105-33
4.5a Medicaid Agency Fraud Detection and InvestigationProgram
The Medicaid agency has established a mechanismto receive reports from beneficiaries and othersand compile data concerning alleged instances ofwaste, fraud, and abuse relating to the operation ofthis title.
99- 19 MA-(NJ)
C\..~ -\'\
Approval Da~CT_~~9'ffective Date _ rJUt - 1 1999TN No.
Supersedet\.Z _ ....TNNo.~
37
Revision: HCFA-~-80-38(BP~)
~1ay 22, 1980
The M....odicaid agency will submit allreports in the form and with the contentrequired by G~e Secretary, and will complywith any provisions that the Secretaryfinds necessary to verify and assure thecorrectl'1eSS of the reports. Allrequirements of 42 CPR 431.16 are met.
4.6 Reoorts
State. NE_\,_J_J_ER_S_E_Y _~
Cit3.tion42 ern 431.16AT-79-29
.. ..'1
'TI'l # 77 - /4Supersedes .'IN # 7' ... Ii
Approval Date 1-1/- 7f_ Effective Date 1~-J-77

38
Re'Jision: HCFA-AT-80- 38 (BPP)May 22, 1980
4,'f-:: 1.((..... ;~..'. . - ~' '--,,:............ -~;... ',- ..
NHJ JERSEYState-----......;..;,;~.....;;;.;:~.::..:.._--------------
Citation42 CER 431.17AT-79-29
4.7 Maintenance of Records
The Medicaid agency maintains or supervisesthe maintenance of records necessary for theproper and efficia~t operation of ~~e plan,including records regarding afP1ications,determination of eligibility, the provision ofmedical assistance, and administrative casts,and statistical, fiscal and other recordsnecessary for reporting am ac:countabili ty ,and retains ~~ese records in accordance withFederal require.'11e!1ts. .ill require.'11ents of 42CPR 431.17 are met.
." ..
'IN # 77 "ItSupersedes'IN *74 -II
Approval Date I -1/-71 Effective Date /tJ-/-77

"evision:
39
ECFA-AT-SO-38 (BPF)May 22, 1980 .::. "•• -! ••..; • -'~
::..:.. :;.:.~~
NEt~ JERSEYState-------------------------Citaticn42 ern 431.18 (b)M-79-29
'IN if 24 - 4Supersedes'IN # 74 - I
4.8 Availability of Agenc{ Program Manuals
Program manuals and other policy issuances thataffect the public, including the Medicaidagency I s rules and regulations governingeligibility, need arrl arrount of assistance,recipient rights and responsibilities, andservices offered by the agencj are maintainedin the State office and in each local anddistrict orfice for examination, upon request,by individuals fer review, study, orreprcduction. All I:'=Cl'.1ir2JTlents of 42 CM431.18 are met.
Afproval Date~ - I~- 75' Effective Date$"- /4-14
",,-. ' .. ".
," ",-r....•· _,. ~'.. '
:..:....... ~ '.
40
Revision: r.c?A-AT-80-38 (BFP)~.ay 22, 1980
State. N_E\_,J_J_E_RS_E_y _
Citatim42 ern 433.37Kr-78-90
'IN # 74 -4Supersedes
........ 'IN # 7+-/
4.9 RePOrtino Provider Payments to Interr~
Revenue Service
There are procedures imple.'11ented inaccordance with 42 CFR 433.37 foridentification of providers of services bysccial secur i ty number or by employeridentification number and for reportingthe informati01 required by the InternalRevenue,Code (26 U.S.C. 6041) with respectto payment ror services under the plan.
Afproval Date 4- IS'- 75 Effective DateS"-J4 -74
..; .•..
; ~--'-" ---.~.i::"·.~·_ .,..~.~~',~.' 't: .
41
New: HCFA-PM-99-3JUNE 1999
State: N~ew..:.:.....oJ:..>::e~rs""e.L_y _
OFFICIAL
Citation42 CFR 431.51AT 78-9046 FR4852448 FR 232121902(a)(23)P.L. 100-93(section 8(t)P.L. 100-203(Section 4113)
--"ection 1902(a)(23)of the SocialSecurity ActP.L. 105-33
Section I932(a)(l )Section 1905(t)
4.10 Free Choice ofProviders(a) Except as provided in paragraph (b), the Medicaid agencyassures that an individual eligible under the plan may obtainMedicaid services from any institution, agency, pharmacyperson, or organization that is qualified to perform the services,including of the Act an organization that provides these services orarranges for their availability on a prepayment basis.
(b) Paragraph (a) does not apply to services furnished to anindividual -
(1) Under an exception allowed under 42 CFR 431.54, subject tothe limitations in paragraph (c), or
(2) Under a waiver approved under 42 CFR 431.55, subject to thelimitations in paragraph (c), or
(3) By an individual or entity excluded from participation inaccordance with section 1902(p) of the Act,
(4) By individuals or entities who have been convicted of a felonyunder Federal or State law and for which the State determines thatthe offense is inconsistent with the best interests of the individualeligible to obtain Medicaid services, or
~ ~. ~
(5) Under an exception allowed under 42 CFR 438.50 or42 CFR 440.168, subject to the limitations in paragraph (c).
(c) Enrollment of an individual eligible for medical assistance in a primary carecase management system described in section 1905(t), 1915(a), 1915(b)(1), or1932(a), or a managed care organization, prepaid inpatient health plan, a prepaidambulatory health plan, or a similar entity shall not restrict the choice of thequalified person from whom the individual may receive emergency services orservices under section 1905 (a)(4)(c).
03-07-MA (NJ)
TN # ~03,,---,,-07-,--· _Supersedes TN #--'9"-:9:.....--"-.19"-- _
Effective Date 1 3 20Approval Date MAR 1 1 2~
42
Revision: H~~-AT-80-38{BPP)
~-1ay 22, 1980
NEH JERSEYState-------------------------Citatim42 ern 431. 610KJ:-78-90AT-80-34
4.11 Relations with Standard-SettitH and SurveYhJencies
(a) The State agency utilized by theSecretary to determine qualifications ofinstitutions and suppliers of services toparticipate in Medicare is responsiblefor establishing and maintaining heal~,
standards for private or publicinstitutions (exclusive of ChristianScience sanatoria) that provide servicesto y~dicaid reci~ients. T~is asencyis DEPARH1ENT OF HEALTH
(b) The State authority (ies) respcnsible forestablishing and maintaining standards,other than these relating to health, forpublic or private institutions G,atprovide services to Medicaid recipientsis (are): DEPARTMENT OF HU~1AN SERVI CES
(c) A'IT...£:Hl1ENI' 4.11-A descr ibes the standardsspecified in paragraphs (a) and (b)above, that are kept on file and madeavailable to the Health Care FinancingAdministration on request.
.... : -'.:'-. ~
, .. " ....... : ...
~y~:,-", ,.: ..
'IN # 7te.- 2.1SUp2rsedes
·....... 'IN#74-4Approval Date P-/I- 77 Effective Date II -/-}(;,

NEVI JERSEY
43
Re'lision: B:7A-~-80-38 (3PP)May 22, 1980
State-------------------------
r:~r,.,;-~
~;::-~~-;!:
,....., .. - ..---
Citaticn42 ern 431. 610Nr-78-90Nr-89-34
4.11(d) The DEPARTMENT OF HEALTH
(agency)wnich is the State agencj responsiblefor licensing health institutions,determines if institutions andagencies meet the requirements forparticipation in the Medicaidprogram. The requirements in 42 CFR431. 610 (e), (f) and (g) are met.
'....:< ... -:: ...
. '4:-,:':.
'IN # 7'-2./SupersedesW- *74 - 4
Approval Date I-JI- 77 Effective Date 11-/-7(;,

44
Revision: EC'A-AT-80-38 (BFP)May 22, 1980
State N_Ev_J,-:J-=E,;.;;RS:..;;E;;.:.y _, _....
...--'---
Citaticn42 CFR 431.105 (b)Nr-i8-90
4.12 Consultation to Medical Facilities
(a) Consultative services are providedby healL' and other afPropriateState agencies to hospitals, nursingfacili:.ies, hone health agercies,clinics and laboratories inaccordance with 42 CFR 431.105 (b) .
(b) SL'1lilar servico--s are provided toother types of facilities 9rovidingmediC3l care to individualsreceiving ser'lices :J..'l.cer t:;eprograms spec ified in 42 CPR431.105 (b) .
!JJ Yes, as listed 'c€10H':
Other appropriate institutions,such as mental hospitals, ICF/MR's,etc.
U Not applicable. Similarservices are rot provided toother types of medicalfacili ties.
~. ,
~- .'. . .r;:"-::":~;':-';:._~~ ....
'IN # 74 .. ISupersedes'IN .:.:.# _
Approval Date .3 -/9- 70S' Effective Date /-1-74
..-
Revision: HCFA-PM-91- 4AUGUST 1991
(BPD)
450ff\C\AlOMB No.: 0938-
State/Territory: New Jersey
Citation 4.13 Reguired Provider Agreement
With respect to agreements between the Medicaid agencyand each provider furnishing services under the plan:
42 CFR 431.107
42 CFR Part 4831919 of theAct
42 CFR Part 483,Subpart 0
1920 of the Act
( a)
(b)
(c)
(d)
For all providers, the requirements of 42 CFR431.107 and 42 CFR Part 442, Subparts A and B (ifapplicable) are met.
For providers of NF services, the requirementsof 42 CFR Part 483, Subpart B, and section1919 of the Act are also met.
For providers of 1CF/MR services, therequirements of participation in 42 CFR Part 483,Subpart D are also met.
For each provider that is eligible underthe plan to furnish ambulatory prenatalcare to pregnant women during a presumptiveeligibility period, all the requirements ofsection 1920(b)(2) and (c) are met.
L-/ Not applicable. Ambulatory prenatal care isnot provided to pregnant women during apresumptive eligibility period.
TN No. 91-£ DECSupersedes q 'IJ Approval Date 5 1991TN No. I-e?>.
Effective Date 'OCT 11991
HCFA 1D: 7982E

45(a)
OFFICIALOMBNo.:(MB)Revision: HCFA-PM-91-9October 1991
~ Staterrerritory: ----'N~e~w~Je~rs_""e"'Jyt._._ _
(e)
(c)
(d)
(b)
Hospitals, nursing facilities,providers ofhome health care orpersonal care services, hospiceprograms, managed care organizations,prepaid inpatient health plans, prepaidambulatory health plans (unless the PAHPexcludes providers in 42 CFR 489.102), andhealth insurIng organizations are required to do thefollowing:(a) Maintain written policies and
procedures with respect to alladult individuals receivingmedical care by or through theprovider or organization abouttheir rights under State taw tomake decisions concerning medicalcare, including the right toaccept or refuse medical orsurgical treatment and the rightto formulate advance directives.Provide written information to alladult individuals on theirpolicies concerning implementationof such rights;Document in the individual'smedical records whether or not theindividual has executed an advancedirective;Not condition the provision ofcare or otherwise discriminateagainst an individual based onwhether or not the individual hasexecuted an advance directive;Ensure compliance withrequirements of State Law (whether
For each provider receiving funds underthe plan, all the requirements foradvance directives of section 1902(w) aremet:(1)
4.13 (e)
Citation1902 (a)(58)1902(w)
TN # ~O~3-~O-"--7 _....... Supersedes TN #--'9~1'--~3~8 _
Effective DateAUG 1 3 2003Approval DateMAR 1 7 2OlJ4
03-07-MA (NJ)

Revision: HCFA-PM-91-9~ October 1991
45(b)
(MB) OMBNo.: Off\C\Staterrerritory: ~N~e~w'_'J~e:!..:rse~y _
(2)
(3)
statutory or recognized by thecourts) concerning advancedirectives; and
(f) Provide (individually or withothers) for education for staffand the community on issuesconcerning advance directives.
Providers will furnish the writteninfonnation described in paragraph(1)(a) to all adult individuals atthe time specified below:(a) Hospitals at the time an
individual is admitted as aninpatient.
(b) Nursing facilities when theindividual is admitted as aresident.
(c) Providers of home health care orpersonal care services before theindividual comes under the care ofthe provider;
(d) Hospice program at the time ofinitial receipt of hospice care bythe individual from the program;and
(e) Managed care organizations, health insuringorganizatiori's, prepaid inpatient health plans, and prepaidambulatory health plans (as applicable) at the time ofenrollment of the individual with the organization.
Attachment 4.34A describes law of theState (whether statutory or asRecognized by the courts of theState) concerning advance directives.
Not applicable. No State lawor court decision exists regardingadvance directives.
TN # _O=3'--O"'-'7e- _Supersedes TN #_.-o9'-'1'--=::-38oe- _
~
Effective DateAUG 13 2003Approval Date MAR 1 1 200t
03-07-MA (NJ)

Revision: HCFA-PM-91-10DECEMBER 1991
(MB)46
Staterrerritory: .......o...N'-"'ec:..:wc...:J"-"e::..:rs::,::e:.,L.y _
Citation42 CFR 431.6042 CFR456.250 FR 153121902(a)(30)(C) and1902(d) of theAct, P.L. 99-509(Section 9431)
1932(c)(2)and 1902(d) of theACT, P.L. 99-509(section 9431)
4.14(a)
Utilization/Quality ControlA Statewide program of surveillance andutilization control has been implemented thatsafeguards against unnecessary or inappropriateuse of Medicaid services available under thisplan and against excess payments, and thatassesses the quality of services. Therequirements of 42 CFR Part 456 are met:X Directly
By undertaking medical and utilization reviewrequirements through a contract with a Utilization andQuality Control Peer Review Organization (PRO)designated under 42 CFR Part 462. The contract with thePRO-
(1) Meets the requirements of §434.6(a):(2) Includes a monitoring and evaluation plan to
ensure satisfactory performance;(3) Identifies the services and providers subject to
PRO review;(4) Ensures that PRO review activities are not
inconsistent with the PRO review of Medicareservices; and
(5) Includes a description of the extent to whichPRO determinations are considered conclusivefor payment purposes.
A qualified External Quality Review Organizationperforms an annual External Quality Review that meetsthe requirements of 42 CFR 438 Subpart E of eachmanaged care organization, prepaid inpatient healthplan, and health insuring organizations under contract,except where exempted by the regulation.
TN # --"-'03"---"-07'"- _Supersedes TN #---,9",,2,,--~04--,-- _
J.\UG 13 20QlEffective Date -.-.....-=--..".-"..-......,..,
Approval Date MAR 1 7 2004
03-07-MA (NJ)
46(a)
TITLE XIX STATE PLAN- NEW JERSEY
4.14 Utilization/Quality Control Con't
Clinical Audit Process for Nursing Facilities
Clinical audit is a method of utilization control under section 1902(a)(30) of theSocial Security Act.
The goal is to monitor continued utilization of and payment for nursing facility(NF) care and services reimbursable under Title XIX.
The focus on clinical audit review (the review) shall be on the following areas:
1. Comparative analysis of NF claim reporting to recipient's identified careneeds;
2. Appropriate utilization and provision of required services; and
3. Effectiveness and quality of provided services.
The review will also evaluate a NF claim reporting of nursing service acuities.
97-15-MA(NJ)
~~ ~-2-:~_Approval OatedUl] 1 1997
SupersedEs ((J ili\~eW-EfF2ctive Date APR QI :;~:~.. ,.. .
Revision: HCFA-PM-85-3KAY 1985
state:
47
(SERC)
NEW JERSEY
OKS NO. 0938-0193
Citation42 CFR 456.250 FR 15312
4.14 (b) The Medicaid agency meets the requirementsof 42 CFR Part 456, Subpart C, forcontrol of the utilization of inpatienthospital services.
4/
LI
utilization and medical review areperformed by a Utilization and QualityControl Peer Review Organization designatedunder 42 CFR Part 462 that has a contractwith the agency to perform those reviews.
Utilization review is performed inaccordance with 42 CFR Part 456, Subpart H,that specifies the conditions of a waiverof the requirements of Subpart C for:
LI All hospitals (other than mentalhospitals) .
LI Those specified in the waiver.
LI No waivers have been granted.
TN No.~SupersedesTN No. '15-1/
JUN 2 1 1985ApPl:"oval Date _ JAN 1 1985
Effective Date
HCFA ID: 0048P/0002P

; ,
OffiCIAL
48
Revision: HCFA-PK-85-7JULY 1985
State/Territory:
(BERC)
NEW JERSEY
OKB NO.: 0938-0193
(
Citation42 CFR 456.250 FR 15312
4.14 (c) The Medicaid agency meets the requirementsof 42 CFR Part 456, Subpart 0, for controlof utilization of inpatient services in mentalhospitals.
L-/ Utilization and medical review areperformed by a Utilization and QualityControl Peer Review Organization designatedunder 42 CFR Part 462 that has a contractwith the agency to perform those reviews.
L-/ Utilization review is performed inaccordance with 42 CFR Part 456, Subpart H,that specifies the conditions of a waiverof the requirements of Subpart 0 for:
L-I All mental hospitals.
L-/ Those specified in the waiver.
L-ff No waivers have been granted.
L-/ Not applicable. Inpatient services in mentalhospitals are not provided under this plan.
nJ No. H::L08upereedeeTH No. gs-"4
Approval Date OCT. 1 0 1985 Effective Date OCT. 1 1985
HCFA 10: 0048P/0002P
Revision: HCrA-PH-85-3KAY 1985
state:
49
(BERC)
NEW JERSEY
OHB NO. 0938-0193
Citation42 CrR 456.250 rR 15312
4.14 (d) The Hedicaid agency meets the requirements of42 crR Part 456, Subpart E, for the control ofutilization of skilled nursing facilityservices.
L-' Utilization and medical review areperformed by a Utilization and QualityControl Peer Review Organization designatedunder 42 crR Part 462 that has a contractwith the agency to perform those reviews.
,]/ Utilization review is performed inaccordance with 42 CrR Part 456, Subpart H,that specifies the conditions of a waiverof the requirements of Subpart E for:
'X, All skilled nursing facilities.
L-' Those specified in the waiver.
L-' No waivers have been granted.
"NNo.~upersedes
.'N No. 1'S~'1
JUN 21 1985Approval Date _ JAN 11985Effective Date __
HCFA 1D: 0048P'0002P
---------------~~~--
(Revision: HCFA-PM-85-3~.AY 1985
state:
(BERC)
NE\~ JERSEY
50
~.
OH3 ~O. 0938-0193
(
Citation42 CFR 456.250 FR 15312
4.14 IX/(e) The Medicaid agency meets the ~e~ui~e~ents
of 42 eFR Pa~t 456, Subpa~t F, fo. cont~ol
of the utilization of inteLrnediate ca~e
facility services. Utilizatio~ ~evie~ infacilities is p~ovided th~ough:
L-I Facility-based review.
IXI Di~ect ~eview by pe~sonnel of the ~edical
assistance unit of the State agency.
IXI Pe~sonnel unde~ cont~act to the medicalassistance unit of the State agency.
I I Utilization and Quality Co~t.ol Pee~ Revie~
O~ganizatio:is.
I I Anothe~ method as desc~ibed in ATTAe~~~~~
4.14-A.
I I Two o~ no~e of the above ~et~~cs.
ATTAC~E:~;-r c. .14-B descrices theci~c~~stances unde~ ~hich each method isused.
I I !:ot applicable.ser-vices a.e not
Inte~ediate ca~e facilityp~ovided unce. this ?l~~.
Reviews are conducted by personnel employed by the Department of Healthand Senior Services (DHSS), or personnel under contract to DHSS. Reference;s made to approved State Plan Amendment 96-31-MA at Attachment 4.16A-5.
lIN No •. "\;.. - \~Supe~sedes
IN No. 'f35-trApp~oval Date ,~Jl'11l9g1 Effective Date __~l'__~__~
HerA IO: 0048P/0002P

Revision: HCFA-PM-91-10December 1991
(MB)
50a
Citation
Staterrerritory: --.o..;N:..:::e..:..:w..."J:..:::e""'rs""e.,J....y _
4.14 Utilization/Quality Control (Continued)
42 CFR 438.356(e)
42 CFR 438.35442 CFR 438.356(b) & (d)
TN # --"'03"'--=.07.<.- _Supersedes TN #--'90..=2=---=-04--'-- _
For each contract, the State must follow an open,competitive procurement process that is in accordancewith State law and regulations and consistent with 45CFR part 74 as it applies to State procurement ofMedicaid services.
The State ensures that an External Quality ReviewOrganization, and its subcontractors performing theExternal Quality Review or External Quality Reviewrelated activities, meet the competence andindependence requirements.
Not applicable.
03-07-MA (NJ)
Effective Date AUG 1 3 200lApprova1Date ~MITA=-R--":-t-;7;;;-"1'!2004I1'Vn-
51 OFFI··CIALRevision: HCFA-PM-92-2
HAReR 1992(HSQB)
New Jerseystate/Territory: _~:""-'''---'~L->L'-3- _
Citation 4.15 Inspection of Care in Intermediate Care Facilities for theMentally Retarded, Facilities Providing Inpatientpsychiatric Services for Individuals Under 21, and MentalHospitals
42 CFR Part456 SubpartI, and1902(a}(31)and 1903(g}of the Act
The State has contracted with a PeerReview organization (PRO) to performinspection of care for:
ICFs/MR;
Inpatient psychiatric facilities forrecipients under age 21; and
42 CFR Part456 SubpartA and1902(a)(30}of the Act
Ment~l Hospitals.
__X_ All applicable requirements of 42 CFR Part456, Subpart I, are met with respect toperiodic inspections of care and services.
Not applicable with respect to intermediate carefacilities for the mentally~etarded services; suchservices are not provided under this plan.
Not applicable with respect to services forindividuals age 65 or over in institutions for mentaldisease; such services are not provided under thisplan.
Not applicable with respect to inpatient psychiatricservices for individuals under age 21; such servicesare not provided under this plan.
TN No. '1=1-10SupersedesTN No. '7' -;).
Approval Date MAY 2 1 .,. Effective Date JAN 1- 1993
52
Revision: HCFA-AT-80-38(BPP)May 22, 1980
State. N~e::.!w~Je~r!_.::s~e:..Ly _
Citation42CFR 431.615(c)AT-l8-90
4.16 Relations with State Health and VocationalRehabilitation Agencies and Title VGrantees
The Medicaid agency has cooperativearrangements with State health andvocational rehabilitation agencies and withtitle V grantees, that meet therequirements of 42 CFR 431.615.
The Medicaid agency will provide forcoordination of the operations under TitleXIX with the State's operations under thespecial supplemental food program forwomen, infants and children (WIC) underSection 17 of the Child Nutrition Act of1966 as specified by amendment to Section1902 (a) (11) of the Social Security Act.
ATTACHMENT 4.16-A describes the cooperativearrangements with the health and vocationalrehabilitation agencies, and with theSupplemental Food Programs for women,infants and children (WIC).
TN' pn-/ISupersedesTNII ,fc-i
Approva1 Date APR t 9 1991 Effective Oate JA_N O_1 19_9_1 ___
53
Revision: HCFA-PM-95-3 (Ma)MAY 1995
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
OFFICIAL
State/Territory: Ne\'/ Jersey
Citation42 CFR 433.36(c)1902(a)(18) and19l7(a) and (b) ofthe Act
4.17 Liens and Adjustments or Recoveries
(a) Liens
The State imposes liens against anindividual's real property on account ofmedical assistance paid or to be paid.
The State complies with the requirementsof section 19l7(a) of the Act andregulations at 42 CFR 433.36(c)-(g) withrespect to any lien imposed against theproperty of any individual prior to hisor her death on account of medicalassistance paid or to be paid on his orher behalf.
__X__ The State imposes liens on real propertyon account of benefits incorrectly paid.
The State imposes TEFRA liens19l7(a)(l)(B) on real property of anindividual who is an inpatient of anursing facility, IeF/MR, or othermedical institution, where theindividual is required to contributetoward the cost of institutional care
~i all but a minimal amount of incomerequired for personal needs.
x
The procedures by the State fordetermining that an institutionalizedindividual cannot reasonably be expectedto be discharged are specified inAttachment 4.l7-A. (NOTE: If the Stateindicates in its State plan that it isimposing TEFRA liens, then the State isrequired to determine whether aninstitutionalized individual ispermanently institutionalized and afford
·-these individuals notice, hearingprocedures, and due processrequirements.)
The State imposes liens on both real andpersonal property of an individual afterthe individual's death.
TN No. 9S-a.;( AUG 0 I _Supersedes Approval DateTN No. gS-~
Effective Date APR 1- 1995
R'C'J'l.8 :"on: EC:'.>,-?X-95-) (1-'.3) Hl\X 19~5
5T'\1':S P"'....)J{ UHDE:R TITLZ XIX Of T~Z: socrAL so;C\.:'"RI'rY AC-:
Ne'tl Jerseys::"t:e/Ter::: itcr;: ~~--------_.
(t) J\Ci~.st.:nC'·,::'5 0:- ?,eCC""O(2:' :..e~.....--oI:----~_.. h _~
The St.l.te ccmelier; ..... ith the rec;.:~:e:::er,tG ot Bec~ion 1917(b) of t~ Ac~ a~d-ce7~la~~c~s a~ 42 CoR 433.J6(h)-(i),
Acj\J6t.:nen~g c=, recover iell tor ~ec ~c J..~ c 1.a;.;:.s cor~ectly paid are as fo1.10 .....s:
(l) for permanently institutionalized individuals, adjus~ent3 or recoveries a..re oade fr:OII1 the indiv idual' s estate or upon sale of the property subject to a lien imposed because of medical agaLatance paid on behalf of the individual for services provided in a nursing :facility, ICY!lffi, 0::- other medical in~titution.
Adjust.:nen't3 or recoveries are made for all other medical a9sistance paid on behalf of the ~odividual.
(2 ) The St ate detel.-nlinea "perm.a..nent institutioTlo'l.l status" of individualo under·the age o! S5 other:. than thoge wLth re:lpeet to ~hom it, imposes liens on real property under S1917(a)(1){B) (even if it does .no't. impose those liens).
(3) For any individual who re~eived medical Aasistance at age 55 or older, adjustments Q~ recoveries of payments are m.u.de 'from tne ind.ividua.1' s e!ltate for nursing facility services, heme and co~munity-based'service5, ~~d related hospital and prescription d--ug services.
x In addition to adjustment 0=
recovery of payments for 5ervices li~ted above, payments are adjusted or,r~Qvered £or oth~· nervic8s under the State plan as listed
-..' balO'",; ',"': ':'_.' ..
------'·-~"····~"-·F~~"·~·;y individual who received ". '. : '''-:~'ined i ca 1 "a 5S i stance'; a t age55-' or
.- -':.01 der,.' a'djustrnents 'or recover; es of payments are 'made from the' individual's estate for all services covered under the State Plan]
except for Medicare cost sharing identified at 4,17(b)(3-- Continued)
Tt1 110." /O-).!{_ MAR 0 1 2011Super8edeb Approval Date i:ffective Date .iO/.JJ..~OI0 TIl }Ie. __ 1,~ 'f '3 _
Page 53a-l
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
State: New Jersey
4.17(b) Adjustments or Recoveries (continued)
L(3) (Continued) Limitations on Estate Recovery - Medicare Cost Sharing:
(i) Medical assistance for Medicare cost sharing is protected from estate recovery for the following categories of dual eligibles: QMB, SLMB, QI, QDWI, QMB+, SLMB+. This protection extends to medical assistance for fOUf Medicare cost sharing benefits: (Part A and B premiums, deductibles, coinsurance, co-payments) with dates of service on or after January I) 2010. The date of service for deductibles, coinsurance, and co-payments is the date the request for payment is received hy the State Medicaid Agency. The date of service for premiums is the date the State Medicaid Agency paid the premium.
(ii) In addition to being a qualified dual eligible the individual must also be age 55 or over. The above protection from estate recovery for Medicare cost sharing benefits (premiums, deductibles, coinsurance, co-payments) applies to approved mandatory (i.e., nursing facility, home and community-based services, and related prescription drugs and hospital services) as well as optional Medicaid services identi tied in the State plan, which are applicable to the categories of duals referenced above.
TN No.: 10-14 Effective Date: October 1, 20] 0
Supersede1l.. Approval Date: I1AR 0 1 lnnTNNo.:N''WeW
Revision: HCFA-PM-95-3MAY 1995
(KB)
53b
OFFICIALSTATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
State/Territory: New Jersey
(4) The State disregards assets orresources for individuals who~eceive or are entitled to receivebenefits under a long term careinsurance policy as provided for inAttachment 2.6-A, Supplement 8b.
X The State adjusts or recovers from---- the individual's estate on account
of all medical assistance paid fornursing facility and other long termcare services provided on behalf ofthe individual. (States other thancalifornia, Connecticut, Indiana,Iowa, and New York which providelong term care insurance policybased asset or resource disregardmust select this entry. These fiveStates may either check this entryor one of the following entries.)
The State does not adjust or recover---- from the individual's estate on
account of any medical assistancepaid for nursing facility or otherlong term care services provided onbehalf of the individual.
The State adjusts or recovers fromthe assets or resources on accountof medical assistance paid fornursing facility or other long termcare services provided on behalf ofthe individual to the extentdescribed below:
TN No.Superse Approval Date AUG 0 2 1995TN No. ~"'~N-
Effective Date APR 1- 1995

53b - \
1917 (b) 1 (Cl
•
STATE PLAN UNDER TITLE XIX 0, THE SOCIAL SECURITY ACT
State, NtA!tJ :fers-e.j _
(4) X If an individual covered under a long-term careinsurance policy received benefits for whichassets or resources were disregarded asprovided for in Attachment 2.6-A, Supplement 8c(State Long-Term Care Insurance Partnership) I
the State does not seek adjustment or recoveryfrom the individual's estate for the amount ofassets or resources disregarded .
• TN No. 01-,"Supersedes
TN No. ~\ .....
\fEB 1 q",. ~llApproval Date Effective Date NOV 2 3 LUU
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT-.
Revision: HCFA-PM-95-3MAY 1995
State/Territory:
53c
New Jersey
(Ma) OFFICIAL
x
(c) Adjustments or Recoveries: Limitations
The State complies with the requirements ofsection 1917(b)(2) of the Act and regulationsat 42 CF~S433.36(h)-(i).
x(1) Adjustment or recovery of medical
assistance correctly paid will be madeonly after the death of the individual'ssurviving spouse, and only when theindividual has no surviving child who iseither under age 21, blind, or disabled.
(2) With respect to liens on the home of anyindividual who the State determines ispermanently institutionalized and whomust as a condition of receiving servicesin the institution apply their income tothe cost of care, the State will not seekadjustment or recovery of medicalassistance correctly paid on behalf ofthe individual until such time as none ofthe following individuals are residing inthe individual's home:
(a) a sibling of the individual (who wasresiding in the individual's homefor at least one year immediatelybefore the date that the individualwas institutionalized), or
(b) a child of the individual (who wasresiding in the individual's homefor at least two years immediatelybefore the date that the individualwas institutionalized) whoestablishes to the satisfaction ofthe State that the care the childprovided permitted the individual toreside at horne rather than becomeinstitutionalized.
(3) No money payments under another programare reduced as a means of adjusting orrecovering Medicaid claims incorrectlypaid.
:~~~ ....--J.:~::::.Ji:"'--ApprovalDate AUG 0r f99!iTN No.
Effective Date APR 1 - 1995

Revision: HCFA-PM-95-3MAY 1995
(MB)
53d
OFFICiALSTATE PLAN ONDER TITLE XIX OF THE SOCIAL SECURITY ACT
State/Terri tory: __.....uN.t:e:¥\rJI--l.,lJJe::.r~s.t:e:.:ly'-- _
(d) ATTACHMENT 4.17-A
(1) Specifies the procedures for determiningthat an institutionalized individualcannot reasonably be expected to bedischarged from the medical institutionand return home. The description of theprocedure meets the requirements of 42CFR 433.36(d).
(2) Specifies the criteria by which a son ora daughter can establish that he or shehas been providing care, as specifiedunder 42 CFR 433.36(f).
(3) Defines the following terms:
o estate (at a minimum, estate asdefined under State probate law).Except for the grandfathered Stateslisted in section 4.l7(b)(3), if theState provides a disregard for assetsor resources for any individual whoreceived or is entitled to receivebenefits under a long term careinsurance policy, the definition ofestate must include all real, personalproperty, and assets of an individual(inclUding any property or assets inwhich the individual had any legaltitle or interest at the time of deathto the extent of the interest and alsoincluding the assets conveyed throughdevices such as joint tenancy, lifeestate, living trust, or otherarrangement),
o individual's home,
o equity interest in the home,
o residing in the home for at least 1 or2 years,
o on a continuous basis,
o discharge from the medical institutionand return home, and
o lawfully residing.
TN No. 9S-9\asuperse1f, ApprovalTN No. -PteW--
DateAUG 82" Effective Date APR 1 - 1995
Revision: HCFA-PM-9S-3MAY 1995
(ME)
53e OffiCiAlSTATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
State/Territory: New Jersey
(4) Describes the standards and proceduresfor waiving estate recovery when it wouldcause undue hardship.
6
(5) Defines when adjustment or recovery isnot cost-effective. Defines costeffective and includes methodology orthresholds used to determine costeffectiveness.
(6) Describes collection procedures.Includes advance notice requirements,specifies the method for applying for awaiver, hearing and appeals procedures,and the time frames involved.
TN No. qS-~~ AUsupersedes . Approval Date G02 1995TNNO.~
Effective Date APR 1- 1995

Revision: HCFA-AT-91-4(BPD)AUGUST 1991
54
OMBNo.: 0938-0FflCIAStatefferritQry: --'-'N""e~w_"Jc:erse=y.L_. _
Citation 4.1842 CFR 447.51through 447.58 (a)
1916(a) and (b) (b)of the Act
Recipient Cost Sharing and Similar Charges
Unless a waiver under 42 CFR 431.55(g) applies,deductibles, coinsurance rates, and copayments donot exceed the maximum allowable charges under42 CFR447.54.
Except as specified in items 4. 18(b)(4), (5),and (6) below, with respect to individuals coveredas categorically needy or as qualified Medicarebeneficiaries (as defmed in section 1905(p)(1) ofthe Act) under the plan:
(I) No enrollment fee, premium, or similar charge is imposed under theplan.
(2) No deductible, coinsurance, copayment, or stmilar charge is imposedunder the plan for the following:
(i) Services to individuals under age 18, orunder--
[ ] Age 19
[ ] Age 20
[X] Age 21 ".
Reasonable categories of individuals whoare age 18 or older, but under age 21, towhom charges apply are listed below, ifapplicable.
(ii) Services to pregnant women related to thepregnancy or any other medical conditionthat may complicate the pregnancy.
03-07-MA (NJ)
TN # ~-,O=3__-0",-,7 _Supersedes TN # 91-34
Effective Date Allr, 1 3 2003Approval Date}AM{' 1 'f ~
Revision: HCFA-PM-91-4AUGUST 1991
(BPD)
55
OMB No.: 0938-
Statefferritory: ~N~e~w'_=J~e~rse~y _
Citation 4. 18(b)(2) (Continued)
42 CFR 447.51through 447.58
(iii) All services furnished to pregnant women.
Not applicable. Charges apply for services topregnant women unrelated to the pregnancy.
(iv) Services furnished to any individual who is an inpatientin a hospital, long-term care facility, or other medicalinstitution, if the individual is required, as a condition ofreceiving services in the institution to spend for medicalcare costs all but a minimal amount ofhis or her incomerequired for personal needs.
(v) Emergency services if the services meet therequirements in 42 CFR 447.53(b)(4).
\
(vi) Family planning services and supplies furnished toindividuals of childbearing age.
(vii) Services furnished by a managed care organization,health insuring organization, prepaid inpatient healthplan, or prepaid ambulatory health plan in which theindividual is enrolled, unless they meet the requirementsof 42 CFR 447.60.
42 CFR438.10842 CFR 447.60
[ ] Managed care enrollees are chargeddeductibles, coinsurance rates, and copaymentsin an amount equal to the State Plan servicecost-sharing.
1916 of the Act,P.L. 99-272,(Section 9505)
[X] Managed care enrollees are not chargeddeductibles, coinsurance rates, and copayments.
(viii) Services furnished to an individual receivinghospice care, as defined in section 1905(0) ofthe Act.
03-07-MA (NJ)
~ TN # ~03,,---=07-,-- _Supersedes TN #----'9"-'1'--=:..34-'- _
AUG 13 2003Effective Date MAR 1 7 z664Approval Date _
Revision: HCFA-PM-9l- 4AUGUST 1991
State/Territory:
(BPD)
56
New Jersey
OFF tALOMB No.: 0938-
Citation 4.l8(b) (Continued)
42 CFR 447.51through447.48
(3 ) Unless a waiver under 42 CFR 43l.55(g)applies, nominal deductible, coinsurance,copayment, or similar charges are imposed forservices that are not excluded from such chargesunder item (b)(2) above.
LX/ Not applicable. No such charges areimposed.
(i) For any service, no more than one type ofcharge is imposed.
(ii) Charges apply to services furnished to thefollowing age groups:
1-/ 18 or older
1-/ 19 or older
1-/ 20 or older
1-/ 21 or older
1-/ Charges apply to services furnished to thefollowing reasonable categories ofindividuals listed below who are 18 years ofage or older but under age 21.
HCFA ID: 7982E
TN No. ql-39 1992supersedes Approval Date __J_A_N__1__5 _TN No. 8b-/1
Effective Date OCT 0 1 1991
Revision: HCFA-PM-91- 4 (BPD)AUGUST 1991
State/Territory:
56a
New Jersey
OfHt\OMB No.: 0938-
Citation42 CFR 447.51through 447.58
4.l8(b)(3) (Continued)
(iii) For the categorically needy and qualifiedMedicare beneficiaries, ATTACHMENT 4.18-Aspecifies the:
(A) Service(s) for which a charge(s) isapplied;
(B) Nature of the charge imposed on eachservice;
(C) Amount(s) of and basis for determiningthe charge(s);
(D) Method used to collect the charge(s);
(E) Basis for determining whether anindividual is unable to pay the chargeand the means by which such an individualis identified to providers;
(F) Procedures for implementing and enforcingthe exclusions from cost sharingcontained in 42 CFR 447.53(b); and
(G) Cumulative maximum that applies to alldeductible, coinsurance or copaymentcharges imposed on a specified timeperiod.
L-/ Not applicable. There is nomaximum.
HCFA 1D: 7982E
TN No. 91- 34 JAt;~p:~~ede~1) _( ~Approval Date l~ 1 5 1!i92 Effective Date OCT 0 1 1991

Revision: HCFA-PM-91-4 (BPD)AUGUST 1991
56b
OMB No.: 0938-
state/Territory: New Jersey
Citation1916(c) ofthe Act
1902(a)(52)and 1925(b)of the Act
1916(d) ofthe Act
4.18(b)(4) 1-/ A monthly premium is imposed on pregnantwomen and infants who are covered undersection 1902(a)(lO)(A)(ii)(IX) of the Actand whose income equals or exceeds 150 percentof the Federal poverty level applicable to afamily of the size involved. The requirementsof section 1916(c) of the Act are met.ATTACHMENT 4.18-D specifies the method thestate uses for determining the premium and thecriteria for determining what constitutes unduehardship for waiving payment of premiums byrecipients.
4.18(b)(5) 1-/ For families receiving extended benefitsduring a second 6-month period undersection 1925 of the Act, a monthly premiumis imposed in accordance with sections1925(b)(4) and (5) of the Act.
4.18(b)(6) 1-/ A monthly premium, set on a sliding scale,imposed on qualified disabled and workingindividuals who are coveredunder section 1902(a)(10)(E)(ii) of the Act andwhose income exceeds 150 percent (but does notexceed 200 percent) of the Federal povertylevel applicable to a family of the sizeinvolved. The requirements of section 1916(d)of the Act are met. ATTACHMENT 4.18-Especifies the method and standards the Stateuses for determining the premium.
TN No. 9 I ?j q: JAN 15 1992Supersedes Approval Date _TN No. R (z-( 7
Effective Date aCT 01 1991
HCFA ID: 7982E

Revision: HCFA-PM-91- 4 (BPD)AUGUST 1991
State/Territory:
56c OFFICIALOMS No.: 0938-
New Jersey
Citation
42 CFR 44 7 . 51through 447.58
4.18(c) LXI Individuals are covered as medically needy underthe plan.
(1) 1-/ An enrollment fee, premium or similar charge isimposed. ATTACHMENT 4.l8-B specifies theamount of and liability period for such chargessubject to the maximum allowable charges in 42CFR 447.52(b) and defines the State's policyregarding the effect on recipients ofnon-payment of the enrollment fee, premium, orsimilar charge.
447.51 through447.58
( 2 ) No deductible, coinsurance, copayment,or similar charge is imposed under the plan forthe following:
(i) Services to individuals under age 18, orunder--
L/ Age 19
L/ Age 20
LJ/ Age 21
Reasonable categories of individuals whoare age 18, but under age 21, to whomcharges apply are listed below, ifapplicable:
TN No. en -34 .Supersedes Approval Date JAN l!i 1992TN No. ~"-11
Effective Date OCT 0 1 1991
HCFA ID: 7982E
56d
Revision: HCFA-PM-91- 4 (SPD)AUGUST 1991
Off\&\AlOMS No.: 0938-
State/Territory: New Jersey
Citation
42 CFR 447.51through447.58
4.18 (c)(2) (Continued)
(ii) Services to pregnant women related to thepregnancy or any other medical conditionthat may complicate the pregnancy.
(iii) All services furnished to pregnant women.
1-/ Not applicable. Charges apply forservices to pregnant women unrelated tothe pregnancy.
(iv) Services furnished to any individual who is aninpatient in a hospital, long-term carefacility, or other medical institution, if theindividual is required, as a condition ofreceiving services in the institution, to spendfor medical care costs all but a minimal amountof his income required for personal needs.
(v) Emergency services if the services meet therequirements in 42 CFR 447.53(b)(4).
(vi) Family planning services and supplies furnishedto individuals of childbearing age.
1916 of the Act,P.L. 99-272(Section 9505)
44 7 . 51 through447.58
(vii) Services furnished to an indiVidualreceiving hospice care, as defined insection 1905(0) of the Act.
(viii) Services provided by a health maintenanceorganization (HMO) to enrolled individuals.
LJV Not applicable. No such charges areimposed.
TN No. l' .3<7supersede Approval DateTN No. ~n-17
JAN'Ll. 1992 Effective DateOCT 0 1 1191
HCFA ID: 7982E
Revision: HCFA-PM-9l-4 (BPD)AUGUST 1991
State/Territory:
56e
New Jersey
OMB No.: 0938-
Citation 4.l8(c)(3) Unless a waiver under 42 CFR 431.55(g) applies,nominal deductible, coinsurance, copayment, orsimilar charges are imposed on services that arenot excluded from such charges under item (b)(2)above.
LX/ Not applicable. No such charges areimposed.
(i) For any service, no more than one type ofcharge is imposed.
(ii) Charges apply to services furnished to thefollowing age group:
1-/ 18 or older
1-/ 19 or older
1-/ 20 or older
1-/ 21 or older
Reasonable categories of individuals who are 18years of age, but under 21, to whom chargesapply are listed below, if applicable.
TN No. 9/-.:3 #Supersedes Approval DateTN No. 86-'1
Effective Date
HCFA In: 7982E
OCT 0 1 1991

Revision: HCFA-PM-91- 4 (BPD)AUGUST 1991
56f
Off\~., 0938-
State/Territory: r~ew Jersey
Citation 4.18(c)(3) (Continued)
447.51 through (iii) For the medically needy, and other optionalgroups, ATTACHMENT 4.l8-C specifies the:
447.58(A) Service(s) for which charge(s) is
applied;
(B) Nature of the charge imposed on eachservice;
(C) Amount(s) of and basis for determiningthe charge(s);
(D) Method used to collect the charge(s);
(E) Basis for determining whether anindividual is unable to pay the charge(s)and the means by which such an individualis identified to providers;
(F) Procedures for implementing and enforcingthe exclusions from cost sharingcontained in 42 CFR 447.53(b); and
(G) Cumulative maximum that applies to alldeductible, coinsurance, or copaymentcharges imposed on a family during aspecified time period.
1-/ Not applicable. There is no maximum.
TN No. q I -;3 if ... 1992supersede~ Approval Date JAN~;t.TN No. <5C9-/7 -------
Effective Date
HCFA 1D: 7982E
OCT 0 1 1991

Revision: HCFA-PM-91- 4AlCl'ST 1991
State/Territory:
(SPD) OMS No.: 0938-
New Jersey
Citation
42 CFR 447.2521902(a)(13)and 1923 ofthe Act
4.19 Payment for Services
(a) The Medicaid agency meets the requirements of42 CFR Part 447, Subpart C, and sections1902(a)(13) and 1923 of the Act with respect topayment for inpatient hospital services.
ATTACHMENT 4.l9-A describes the methods andstandards used to determine rates for payment forinpatient ho~pital services.
~/ Inappropriate level of care days are covered andare paid under the State plan at lower rates thanother inpatient hospital services, reflecting thelevel of care actually received, in a mannerconsistent with section 186l(v)(1)(G) of the Act.
L-/ Inappropriate level of care days are not covered.
HCFA ID: 79B2E
TN No. o/l-'9JSupersedes APproval DateTN No. ,'('7-/4
FEB ! ~ 1'~') Effective Date OCT ] 1991

58
State/Ter::-:..tory:
Revision::\ugus t
HCFA-PM-93- 61993
NevJ Jersey
(MB) OMS No.: 0938-
OFFICIALCitation42 CFR 447.20142 erR 447.30252 :R 286481902 (a) ( 13 ) (:.:)1903(a)(1) and(n), 1920, and1926 of the Act
4.19(b) In addition to the se~~ices specified in_paragraphs 4.19(<1)", (dl. (k), (1),. and tm),theMedicaid agency meets the followingrequirements:
(1) Section 1902(a)(1J)(E) of the Act regardingpayment for services furnished by Federallyqualified health centers (FQHCs) under section1905(a)(2)(C) of the Act. The agency meetsthe requirements of section 6303 of the StateMedicaid Manual (HCFA-Pub. 45-6) regardingpayment for FQHC serv ices. ATTACHMENT 4.19-6describes the method of payment and how theagency determines the reasonable costs of theservices (for example, cost-reports, cost orbudget reviews, or sample surveys).
(2) Sections 1902(a) (13) (E) and 1926 of the Act,and 42 CFR Part 447, Subpart 0, with respectto payment for all other types of ambulatoryservices prOVided by rural health clinicsunder the plan.
ATTACHMENT 4.19-6 describes the methods andstandards used for the payment of each of theseservices except for inpatient hospital, nursingfacility services and services in intermediate carefacilitie. for the mentally retarded that aredescribed in other attachments.
1902(41) (10) and1902(41)(30) ofthe Act
SUPPLEMENT 1 to ATTACHMENT 4.19-8 describeSgeneral methOde and standarda used torestablishing payment tor Medicare Part A and Bdeductible/coinsurance.
Effective Dat~OC_l_1__1_993__TN-'!rwft---------------:-:--:-:--W'1'~
Approval Date \
Nn~ JERSEY
59
;risicn: HCFA-AT-80-38 (BPF)~ May 22, 1980
State-------~~==-=~------------
Citatim42 CPR 447.40"Kr-78-90
4.19 (c) Payment is made to reserve a bed duringa recipient's temporary absence from an"inpatient facility.
Yes. The State's policy isdescr ibed in A'IT~..cHMENI' 4.19-<:.
u No.
," ', ..,",- ~- ;
.~ IN it 77 - /rSupersedes'IN if ?,-,IS'
Afproval Date /- '/1- 7'1 Effective Date /,i?;jf-77
..
. l
60 -Revision: HCFA-PM-87- 9
AUGUST 1987(BERC) OMB No.: 0938-0193
state/Territory: NEW JERSEY
". 1-:.',"':'; ....
" .-
Citation42 CFR 447.25247 FR 4796448 FR 5604642 CFR 447.28047 FR 3151852 FR 28141
4.19 (d)
/1/ (1) The Medicaid agency meets the requirements of42 CFR Part 447, Subpart C, with respect topayments for skilled nursing and intermediatecare facility services.
ATTACHMENT 4.19-0 describes the methods andstandards used to determine rates for paymentfor skilled nursing and intermediate carefacility services.
(2) The Medicaid agency provides payment forroutine skilled nursing facility servicesfurnished by a swing-bed hospital.
L-/ At the average rate per patient day paid toSNFs for routine services furnished duringthe previous calendar year.
L-/ At a rate established by the state, whichmeets the requirements of 42 CFR Part 447,Subpart C, as applicable.
/~ Not applicable. The agency does notprovide payment for SNF services to aswing-bed hospital.
(3) The Medicaid agency provides payment forroutine intermediate care facility servicesfurnished by a swing-bed hospital.
L / At the average rate per patient day paid torCFs. other than rCFs for the mentallyretarded, for routine services furnishedduring the previous calendar year.
L-I At a rate established by the State. whichmeets the requirements of 42 CFR Part 447.Subpart C. as applicable.
I~ Not applicable. The agency does notprovide payment for rCF services to aswing-bed hospital.
L/ (4) Section 4.19(d)(1) of this plan is notapplicable with respect to intermediate carefacility services; such services are notprovided under this State plan.
TN No. ~OSupersedesTN No. i4~ y
. JAH 29 1990Approval Date _ Effective Date
HCFA 10: 1010P/0012P
Revisicn:
61
HCFA-AX-SO-38 (BPP)May 22, 1980 :. . ;. .~ '.---
NEVi JERSEYState------------------------Citation42 CPR 447.45 (c)AT-79-50
4.19 (e) The Medicaid agency meets all requirementsof 42 CPR 447.45 for timely payment ofclaims.
~ACHMENT 4.19-E specifies, for eachtype of service, the definition of aclaim for puq:x:ses of meeting theserequirements.
: .. '.
'IN !..1~-/.3~Superc;Pdes'IN .t77-1£
Effective Datef6 ..,;./-1J

(BERC)Revision: HCFA-PM~87-4
KARCH 1987
State/Territory: NEW JERSEY
No.: 0938-0193
Citation42 CFR 447.15AT-78-90AT-80-3448 FR 5730
4.19 (f) The Medicaid agency limits participation toproviders who meet the requirements of42 CFR 447.15.
No provider participating under this plan may denyservices to any individual eligible under the planon account of the individual's inability to pay acost sharing amount imposed by the plan inaccordance with 42 CFR 431.55(g) and 447.53. Thisservice guarantee does not apply to an individualwho is able to pay, nor does an individual'sinability to pay eliminate his or her liability forthe cost sharing change.
Approval Date SEP. 2 1987 Effective Date APR. 1 1987
HCFA 1D: 1010P/0012P
63
....
f~:i$~f-·
RevisiQi: HCFA-AT-80-38(BPP)~ May 22, 1980
: ... .- ...-.
NEvi JERSEYState------------------------Citatien42 CPR 447.20142 CPR 447.202NJ:-78-90
4.19(g) The Medicaid agency assures appropriateaudit of records wilen payment is based encosts of services or en a fee pluscost of materials.
'IN # 77-/2~ Supersedes
'IN * 71' - 9Afproval Date /1)-.2 - 79 Effective Datei-~-79

NEW JERSEY
'-
64
Revision: HCFA-AT-80-60 (BPP)August 12, 1980
State--------------------------
t · I' :co__:,;;,.,c~~~..~..
Citation42 CFR 447.20142 CFR 447.203AT-78-90
4.19 (h) The Medicaid agency meets the requirementsof 42 CPR 447.203 for documentation andavaiJabi1ity of payment rates.
-
lit·:··~ ,("...10.~~It·~, ....~ ~.
Jo. ... \\
'IN # 7?-12Supersedes'IN # 7p· 9
Awroval Date /0"'2. - 7'1 Effective Date i--b" 79
• ~ ,_ •."1,
- ,-----.-- -----: _~._- ---,.-'fi - - _t y ... ,
f - • \' ,. ~ . ~ - ... ~ .

Revisicn:
65
HCFA-AX-80-38 (SPP)May 22, 1980
NEW JERSEYState-------------------------Citaticn42 CPR 447.20142 c...~ 447.204AX-78-90
4.19 (i) The Medicaid agency's payments aresufficient to enlist enough providers sothat services under the plan areavailable to recipients at least to theexta~t that those services are available tothe general population.
'IN # 79-12~ Supersedes
'IN # 71 -?AH?rov~~e/6-;2. -77
/ ~
,_.'F.
Effective DateJ'-~-7'7
Revision: HCFA-PM-91- 4AUGUST 1991
State:
Citation
(BPD)
New Jersey
66 OFFICIALOMS No.: 0938-
42 CFR 4.19(j)447.201and 447.205
1903(v) of the (k)Act
The Medicaid agency meets the requirementsof 42 CFR 447.205 for public notice of any changes inStatewide method or standards for setting paymentrates.
The Medicaid agency meets the requirementsof section 1903(v) of the Act with respect to paymentfor medical assistance furnished to an alien who isnot lawfully admitted for permanent residence orotherwise permanently residing in the United Statesunder color of law. Payment is made only for careand services that are necessary for the treatment ofan emergency medical condition, as defined in section1903(v) of the Act.
TN No. 'i 1- 47-Supersedes tlD Approval DateTN No. :J._ -Dl
DEC 5 1991Effective Date ~O~C~T~_1_1~99_' __
HCFA 1D: 7982E
Rev isi on: HCFA-A'l'-8l-34 (BPP) 10-81
t applicable. TheMe 'caid agency does notall payment under theplan physicians foroutside laboratoryservices.
Payments to Physicians t~~Clinical Laboratory Sefvices
7
For services perfor~d by anoutside laborator for a physicianwho bills for t service, payment
oes not excee the amount thatuld be aut rized under Medicare
in ccorda e with 42 CFR405. l5(b , (c) and (d).
NEW JERSEY
~itation
~2 CFR 447.34246 FR 42669
~_.~
:::.ir...;c.~ .
-
II(
TN # ~ \...- )-c£SupersedesTN -::..# _
Approval Date/:l./'6 vbr Effective Date 16/1 /1(
~
[lt
.... -------~-
::c:?>-:?:!-54-2. (H3)CCTOBER 199~
<C~'''n/7e--1"'o-y'-- ... --~ ... ---'- - .
66 (b)
HE~ JEP.sEY Or~.,~.. f:~,L
'. t·· '..'./* F...:. rio g.•... 1;\ ,.f; .... .. Ii ~~l ,~ ,'; 'j1 .
Ii~Hlli
":.19 (~) ~ec~caid "Rel..::-.b\J"::"ae::-.ent\"-:cr ;;"cLTl!n'l.'3,:-::a:.~on of Vacc:":-.<!~ \::"".ce:~he ?edia~ric l~\:~i=~~ion PrEc~~~~
1928(c)(2)(C)(ii) 0:the r.c'::
( i) r.. F::cvic.er oay Gp:::ae:;.,z.. c~~S\~ ..fo:: :.h::_aC=i~!.st::::-ation of a. C".i'a.1,j..fiec. ~c.!..a.t=~c ;VaCC~1:e
~! stated in 1928 (c-y"p )="(C) (ii) or"- ~"'e . r.ct.. ;';i..~~:":1 :":--:"'5o·/e=a.ll 'O"::"ovi5icn, Y.ec.ica..:..c'. ·=e,:,:::::\:::se=.ent: to "!J:::C'(:"C~::S -..::"'llce c..c.~i.:1is::.e=ed as fcllc'-;~ . .J" ....
( i i) 'Il:e Stat:e:
sets ~ "!Jay=.'e:'1t =a.t'e a:: t~e le'/el of the :::-es:"c::a.l ::-.;:.:::::..::-....:::-.est:2..blishec'. by ~I:e DE:-:S Sec=eta.:-!.
"'C2V'::'.e::7: =G.~£
~S~~'!..~5::~~:-..:::c':-.a5e St.ate c.:1C s et5 2.
-t::e :::-egionc.l :::a;:;~-..:::-.
Stat:e la.,":_
:"5 2. Unive:::-salt:"1e level ofa(;:(;:o:::-c.a::ce ..... ith
r;::- .~.
"f set.s ~ 1?ay;=e~t ::z..t:e belc.... the level cf ~::e =e-::-:"'::::-.2.l":::.a.xi,:::.u::. est:abli~hec. b:y 'the n::::.-:s Sec:::-eta:::-y.
is 2. Unive=sal :1.::::-chase state anc.. sets1::elo...... the level of the :=eSicnal r..;:';=:=-=.\:~t:~e Unive::sal ?-..:::chase St.at:e.
':'~e Stat:e :pavs\t~e =ollo......i~c =o.te .::0:: the ac..::1i::is-::::at:ic:-.of a vacci..""e~: ~·i.5·b· if t:.he pr<:r'1iaer receives, free. v:;;.cc~... e..
J526 of~he ?ct:.
(iii) ::e.c!.caid. .ceneI::l.C~"" ~ccrrs-.to i:"':.1:.~i:::ations isc.g~-..::::-ec. tr..:::-?\:gh th~· tcll'c!:":~g··'t=.etbccolc<;;{:
Other
==-~=..c= " ~-'. ~'., ....---~
APR 0 7 117
67~. < • ~
~~i:;;~;:F
Revision: HCFA-AT-80-38 (BPP)....... May 22, 1980
N[l'J JERSEYState-----~::.:.:..~;.:.:.;:;:.:;;..:...------'-----------
Citation42 CPR 447.25 (b)AT-78-90
4.20 Direct Pavments to Certain Recipients forPhvsicia~' or Dentists' Services
Direct payments are made to certain recipientsas specified by, arrl in accordance with, therequirements of 42 CPR 447.25.
L-I Yes, for L-I physicians' services
L-I dentists' services
ATl'JlCl-<J.lEN1' 4. 20-A specifies theconditions under 'Nhich such payments aremade.
!..Jj Not applicable. No direct payments aremade to recipients.
.c,.r:-,..--.. ,'.:.
'-" 'N # 71'- /~'Jupersedes'IN # 7'" -I&'
Approval Date Effective Date 1.e-31-77
I"'""'\~e\,~;;jion: HCFA-AT-81-311 (BPP) !(,I!'I
kia.!l...' \~.,
,;~l:~~:t_$ ~ _,¥'~
lU-81
Payment for Medicaid servicesfurnished by any provider under thisplan is made only in accordance withthe requirements of 42 CFR 447.10.
NEW JERSEY
4.21 ~~ohi~ition_~9_ainstReassignment ofProvider Claims
State--------,- --- ..----.--------,-,---!!!:-i+'!-~~-.'-'-"-"- ......
'tation
~2 CFR 447.10(c)AT-78-9046 FR 42699
~
r~'' ....
,Irr~, ..
(:~1' .~':, ",
t .. 't, •
I'· .f""'-
:" ..
~.
~
I -
,-----._---- --- -'-'-"- --------------- --_._._--_.-------- -~ ..---.-.-_._-
TN ! ,~LlB__Supersedes
~TN L7i~__..-
l\ppcoval Date /;2,/6 V/'i I Effective Date ID /1 ('if
!r
~t\~~ '"~.:~':~~
,....,..I\I,!r,
1ft

Revision: HCFA-PM-94-1FEBRUARY 1994
(MB) 69 OFFICIALStatefferritory: ;.;,.Ne::..:w.;......:;J..::.e.:..:rs=-::e::..£y _
Citation4.22 Third Party Liability
42 CFR 433.137
1902(A)(25)(H) and (I)of the act
42 CFR 433.138(f)
42 CFR 433.138(g)(1 )(ii)and (2)(ii)
42 CFR 433. 138(g)(3)(i)and (iii)
42 CFR 433.138(g)(4)(i)through (iii)
(a)
(b)
The Medicaid agency meets all requirements of:
(1) 42 CFR 433.138 and 433.139,(2) 42 CFR 433.145 through 433.148,(3) 42 CFR 433.151 through 433.154,(4) Sections 1902(a)(25)(H) and (I) of the Act.
ATIACHMENT 4.22~A--,
(1) Specifies the frequency with which the dataexchanges required in 433.138(d)(1), (d)(3) and(d)(4) and the diagnosis and trauma code editsrequired in 433.138~ are conducted;
(e)(2) Describes the methods the agency uses formeeting the followup requirements contained in433.138(g)(1 )(i) and (g)(2)(i);
(3) Describes the methods the agency uses forfollowing up on information obtained through theState motor vehicle accident report file dataexchange required under 433.138(d)(4)(ii) andspecifies the time frames for incorporation into theeligibility case file and into its third party data baseand third party recovery unit of all informationobtained through the followup that identifies legallyliable third party resources; and
(4) Describes the methods the agency uses forfollowing up on paid claims identified under433.138(e) (methods include a procedure forperiodically identifying those trauma codes thatyield the highest third party collections and givingpriority to following up on those codes) andspecifies the time frames for incorporation into theeligibility case file and into its third party data baseand third party recovery unit of all informationobtained through the followup that identifies legallyliable third party resources.
;;.~
Revision: HCFA-PM-94-1 (MB)FEBRUARY 1994
StateITerritory:
Citation
69a
New Jersey OFFICIAL
42 CFR 433.139(b)(3)(ii)(A)
42 CFR 433.139(b)(3)(ii)(C)
42 CFR 433.139(f)(2)
42 CFR 433.139(f)(3)
42 CFR 447.20
__ (c)
(d)
(e)
Providers are required to bill liable thirdparties when services covered under theplan are furnished to an individual on whosebehalf child support enforcement is beingcarried out by the State IV-D agency
ATTACHMENT 4.22-8 specifies thefollowing:
(1) The method used in determining aprovider's compliance with the third partybilling requirements at433.139(b)(3)(ii)(C),
(2) The threshold amount or other guidelineused in determining whether to seekrecovery of reimbursement from a liablethird party, or the process by which theagency determines that seeding recovery ofreimbursement would not be cost effective,
(3) The dollar amount or time period theState uses to accumulate billings from aparticular liable third party in making thedecision to seek recovery ofreimbursement.
The Medicaid agency ensures that theprovider furnishing a service for which athird party is liable follows the restrictionsspecified in 42 CFR 447.20.
TN'
Supersedes TN qO':" kJ
FEB 2 0 1996
Effective D2,te APR 0 11995-
Revision: HCFA-PM-94-1FEBRUARY 1994
StatefTerritory:
Citation
70
New Jersey
4.22 (continued)
OFFICIAL
42 CFR 433.151(a)
1902(a)(60) of the Act
1906 of the Act
(g)
(h)
(f) The Medicaid agency has written cooperativeagreements for the enforcement of rights to andcollection of third party benefits assigned to theState as a condition of eligibility for medicalassistance with the following: (Check asappropriate.)
__ State title IV-D agency. The requirements of42 CFR 433.152(b) are met.
-X- Other appropriate State agency(s) --New Jersey Department of Law and PublicSafety, Division of Law
__ Other appropriate agency(s) of another State
Gourts and law enforcement officials.
The Medicaid agency assures that the State has ineffect the laws relating to medical child supportunder section 1908 of the Act.
The Medicaid agency specifies the guidelines usedin determining the cost effectiveness of anemployer-based group health plan by selecting oneof the following:
The Secretary's method as provided in theState Medicaid Manual, Section 3910.
X The State provides methods for determiningcost effectiveness on ATTACHMENT 4.22Q..
:'Ji",,~5-tf~__, . 00 .'J;.A!,prOV~I"Yil\;f;~EB2 0 1990
Super:st?d€~ TN qL-~S__ ~fffective Datt'PR011&

OMB No. 0938-019371
Revision: HCFA-AT-84-2 (BERC)01-84
Staterrerritory:. ~N~e~w~J~e'"_!rse=.l_y _
V",.,
Citation
42 CFR434.448 FR 54013
42 CFR Part 438
4.23 Use of Contracts
The Medicaid agency has contracts of thetype(s) listed in 42 CFR Part 434. Allcontracts meet the requirements of42 CFR Part434.
L/ Not applicable. The State has no suchcontracts.
The Medicaid agency has contracts of thetype(s) listed in 42 CFR Part 438. Allcontracts meet the requirements of42 CFR Part 438. Risk contracts are procuredthrough an open procurement process that is co~istent with45 CFR Part 74. The State does not use a competitive bid process, butcontracts with any willing and qualified provider that meets the State'scontract standards for managed care organizations. The risk contract iswith (check all that apply): . ,
a Managed Care Organization that meets the definition of1903(m) ofthe Act and 42 CFR 438.2
a Prepaid Inpatient Health Plan that meets the definition of 42CFR438.2
a Prepaid Ambulatory Health Plan that meets the definition of 42CFR438.2.
Not applicable.
03-07-MA (NJ)
.,--, TN # ~03,,--~07"-- _Supersedes TN #..--'8"--.4'---0=5"-- _
. AUG 13 2003EffectIve Date MAR 1 I 2994Approval Date _

OFFICIAL72
Revision: HCFA-PH-94-2APRI:' 1994
State/~err~tory:
(BPD)
New Jersey
Ci'.:ation42 eFR ~42.10
and 442.100AT-78-90AT-79-18AT-80-25AT-80-3452 FR 32544P.:' 100-203(Sec. 4211)S4 FR 531656 FR 48826
4.24 Standards ~or payments for ~ursing Facilitvand Intermed~ate Care Fac~l~ty for t~e ~encallyRetarded Serv~ces
With respect to nursing facilities andintermediate care facilities for the mentallyretarded, all applicable requirements of42 erR Part 442, Suoparts Band e are met.
Not applicaole to intermediate carefac~lit~es for t~e mentally retarded;9UC~ serVlces are not prov~ded under thisplan.
•
TN No. q If-qSupersedesTN No. 'gO-IS
Approval Date JUL t 5 1994 Effective Date APR 1 - 1994
',sion:
73
HCFA-AT-SO-38 (BPP)May 22, 1980
(~,•• :::-: -;-:-<
':":-'.; ...
~-~ , ..
state, N_EW_J_E_RS_E_Y _
Citation42 ern 431. 702AT-78-90
4.25 Prooram for Licensing Administrators of NursingHanes
The State has a program that, except withrespect to Chr istian SCience sanatoria, meetsthe requirements of 42 CPR Part 431, SubpartN, for the licensing of nursing horneadministrators.
'IN # 74- J...... Supersedes
'IN .::..# _
Effective Date /-1-1'4-
Revision: HCFrt-?X- (H3) OFFICIALState/7erritory: STArt OF NEW JERSEY (DMA&HSY
Citation
1927(g)42 CFR 456.700
1927(g)(1)(rt)
4.26 Drug Ut~lizatior. Re~~~w ?rcgram
A.l. T~e Medicaid ag;~c: meets the requiremen~s o~Section 1927(g) 0: the Act for a drug usereview (OUR) program for outpatient crug
1 •c_al.ms.
2. The OUR prcgr~~ assures that prescriptionsfor outpatien~ c~~gs are:
-Appropriate-Xedically necessary-Are not likel~ to result in adverse mecicalresults -
1927{g) (1) (a)42 CFR 456.705(b) and456.709(b)
1927{g) (I) (8)42 CFR 456.703(d)and(!)
B.
C.
T~e OUR pr:gr~~ is designed to educa~e
physicians anc ?ha~acists to identify andrecuce the fre~~ency of patterns of frauc,abuse, gross ove~~se, or inappropriate ormecically unnecessarf care among physicia~s,
pr.a~acists, and patients or associated withspecific'crugs as well as:
-?otential and ac~~al adverse d~g
=eac-:;icns-7heraDeu~ic a:~rooriateness
-overu~ilizati;n and underutilization-Appropriate use 0: generic prcducts-The=a:eutic d~:lica~icn
-Drug disease c;~t=ai~dications-D=ug-d~g interactions-Incorrect dr~g ccsage or duraticn 0= drug
treat:nent-~=ug-aller;y interactions-clinical abuse/misuse
The DUR p=og=~ shall assess data use agains~
predete~ined standares whose sourcematerials for their ceve100ment areconsisten~ with peer-revie~ed cedicalliterature which. has been critically reviewedby unbiased indepencent eXFe~s ~,d thefollowing-ccmpencia:
-American Hosoital Fc~ula=y Service DrugInformation -
-Unitec States Pha--=acopeia-DrugIn=o~ation
-American Hedical Association D=~g
Evaluations
...... :...--~_ .."
!.'?$.1':.ets~;::;:'
~..
I~-:-·,~
TN No. 16-10SuoersedesTN- No. 9.3-c)""
rtpproval DateNAY' 02 1996 Effective Date .MAR 1 8 1996
... , ..... _. ~ I _ .- -
74anevi4ion: HCFA-?~- (HB)
State/~e::ritory: STATE OF NEW JERSEY (DMA&HS4 Off\t\-
Citation
1927(9) (1) (0)42 CFR 456.703(b) O. DU~ is not re~~i::ed for druss d~spensed to
residents of nu::si~g facilities ~~at are i~
c::.:lpliance •... i~:: dr...:g regimen re·... .:..eworocecures se~ fort~ in 42 CFR 423.60. Tr.eState has neve::-the-less chosen ~~ i~cludenu::sing home crugs i~:
P::-ospect: i ·... e OURRetrospe~~ive OUR.
-
-1927(g) (2) (A)42 CFR 456.705(b)
1927(g) (2) (A) (i)42 crR 4S6.705(b),(1)-(7) )
1927(9) (2) (A) (E)42 CFR 456.705 (c)and (d)
1927(g) (2) (3)42 CFR 456.709(a)
E.1. The OUR prog::-a~ includes prospec~ive re'lie~
of drug thera;y at the point of sale or pci~~
cf distri=uti~~ be:~re each pres==iptic~ isfilled cr deli'lere~ to tr.e Hedic~id
reci?ient.
2. Prospective O~~ incluces screer.i~~ eac~
~rescri~tion filled or delivered co anindivid~al receivi~g benefits fer potentialc::-ug therapy problems cue to:
-Thera~eutic d~~lication
-Drug-disease contra':"~dications-Drug-drug i,,~eractions
-Jrug-inte=ac~ic~s~ith n::~-?re~==i?~i~~ c=cver-the-ccu~~er dr~gs
-I~CO:=2C~ c=~; ccsase c= ci~=a~~~~ c= c=~c
treat::lent-Jrug alle=~y i~~er~cticns
-Clinical abuse/~is~se
3. Prospective OUR inc~~des counse~i~g ~~_
~edicaic reci=ients based on st~~dards
established by State law and rnai~tenance c:patie~t p=ofiles.
:.~. The OUR prcgra::l incluces ret=os~ective OURth:::ough i~s ~echani~ec crug clai=s pr~cessi~~
and infcr~aticn re~=ieval syste~ or ot~e:::~ise
which u~ce=~a~es c~soi~g pe=~cc~~ exa~i~a~ic~
0: claims data and-c~her records to icer.~i:::
-?atterns of fraud and abuse-· ----Gross cve:::use-~na~~ro=ria~e or ~edicallv un::e~essary ca=~
- - - • -; '\l •• ••among phys:"cians, pnarmac::.s-::s, •.e01..ca::.c.reci?ients, or associated wit~ s~ecific
d:::ugs or g:::oups 0: drugs.
TN No. 9?)-/DSupersed~
TN No. '13- fit
.........
Date MAY 02 1996 .MAR 18 1996

: _'\evis-ion: HCF;>'-?~-
state/-:e==itory:
Citation
(HB)
STATE OF NEW JERSEY (DMA&HS) OFFlC\Al927(g) (2) (C)42 C?R 456.709(b)
1927(g) (2) (D)42 C?R 456.711
1927(g) (3) (A)42 CFR 456.716(a)
:.2. 7he DUR prog=~~ assesses data on c=~g ~se
agatnst ex?lic:= precete=~i~ed s~a~darcs
i~c~~ding but cc~ li~i:ed to moni=cri~g for:
-:herape~tic appropria:eness-Overutilizaticn and u~derutili=a~icn
-Appropriate usc of ge~eric prcd~~~s
-:herapeutic duplication-~rug-disease cc~trai~dicatiens
-Drug-drug interactie~s
-Incorrect drug dosage/duration 0: dr~g
t=eat~e~t
-Clinical abuge/~is~se
J. The DUR progra= t~rc~g~ its State CUR Bea=c,~sing data provided =: the Beard, p=ovicesfor ac=ive and cr.goi~g educational c~t=eac~
prcgrams to ed~cate prac~itieners en ccr.~en
d=~g therapy p=c~le~s to L~~rove Fre9c=i~i~g
a~d dispensing practi~es.
G.l. -:~e DUR p=eg=~~ has established a State DG~
Soa=d eithe:::
Di::ectly, c=U~der cont=actorga~i=atic~
'0; _,"-.... __ ...
1927(g) (3) (3)42 CFR 456.716(A) l\.'\i) (3)
--927(g){3)(C)42 C?~ 4S5.716(rl)
2. T~e OUR Eoard ~e~~e=s~io includes tealt~
p=ofessionals (c~e-t~ir~ licensed activelyp=actici~g p~a~aCist5 and cr.e-t~i=d c~t nc~o=e than 51 ~er=ent lice~sed a~d acti.elyp=actici~g physicia~s) with &~ewledge a~dexperience in c~e 0:: core 0= the !ollc~i~g:
- Clinically a~prc?=iate presc=i~ing cf. cove=ed outpatient drugs.
- Clinically apprcp=iate dispensing andmenite::i~g of cove::ed cut?atie~: C=~gs.
- D::ug use revie~, evaluation a~c
i:lte::'/entic~.- Hedical ~~ality ass~::an=e.
3. L~e ac~ivi~ies of ~~e DU~ Boa== i~c~~de:
- Ret=os~ective Dv~,
- App1ica~ion of S~a~dards as definec i~sec~ion 1927(g)(2)(C), a~d
- ongoing interven~ions to:: physicia~s a~d
pha=macists ~a=;e~ed teward the::apyp~oblems 0:: indivicuals ider.~itied i~ t~e
course 0= re:=os~ec~ive OU~.
TN No. q"-/DSu~e=sedes
TN" No. 93-;)..Approval Date MAY 0 2 1995 Ef:ect:'ve Da~e .aIAR 1 8 1996

~~~~~
Revision:
Citation
He
HCFA-?~- (HB) OHB
State/Te::ritory: STATE OF NEW JERSEY (OMA&HS).'
No·OfflC\Al
"'!I!'"~:;:.,...,
~
, ~: ;,..,-~~~~
~
~~~::~,
~
1927(g) (3) (C)42 CFR 456.711(a)-(d)
1927(g) (3) (D)42 CFR 456.712(A) and (B)
1927(h)(1)42 CFR 450.722
G.4 The interven~:cr.s i~elude in a~or~o::ia~e
ins·.:ances:
Information cisse~ination
- Written, oral, anc elec~ronic remi~cers
Face-to-Face discussionsIntensified canitoring/revie~0:prescribe::s/dispensers
H. The State assures that it will prepare ancsubmit an annual re~ar~ to the Secreta~l,
which incoroorates a renort f=cm t~e StateOUR Board, anc that the-State wi~l achere tothe plans, s~e?s, procedures as cescri=ed inthe report.
I.l. The State est~lishes, as its principal meansof processing claL~s for cove=ec cutpatien~
drugs uncer this ti~le, a point-of-saleelectronic cla~~s management system toperfo~ on-line:
Ii!i.....
~~
~
1927(g) (2) (A) (i)42 CFR 456.705{b)
1927(j)f2-L4 2 CF1(~$9.:.'7 0 3 ( c )
...... ~ l:' .~ , .~. •.. ", - ..If '.' "....' 1. ,
...-.
: .=!• . ...
.'...- ..-;
,X- 2.
J.
real t~e eligibility verifica~ion
-claims data caot~re
adjudication of c~aL~sassistance to pha~acists, e~=. a~?lying
for and receiving payment.
Prosnective D~ is ce=fo~ed usi~; anelectronic point at-sale drug c~aL~sprecessing syst~.
Hospitals whic~ dispense coveree outoatientdrugs are ex~pted from the drug utiiiza~ion::eview recuir~~ents of this se~ian whenfacilities use drug fo~ulary systems andbill the ~edicaid program no more than thehospital's pu::chasing cost fo:: s~ch eC7e::ecoutpatient c~gs.
• U.s. G.P.O.:1993-J4Z-2J9:80043
TN No. 11;.-10Suoersedes AoorovalT.N-Na. -New-- -- 'Date MAY e2 1996 Effec-:.ive Date.IIAR 1 8 1996

75
. ~ sion: HCFA-~-aO-38(BPP)
May 22, 1980
NEW JERSEYState------------------------Citatioo42 CPR 431.115 (c)AT-78-90M-79-74
4.27 Disclosure of Survey Information and Provideror COntractor Evaluation
The Medicaid agency has established proceduresfor disclosing pertinent findings obtainedfrom surveys and provider and contractorevaluations that meet all the require.rnents in42 CPR 431.115.
,~# 7'1-/7--- ~upersedes
'IN # 7h- +Approval Date 1~-#1?O - 71 Effective Date /O-J~7f

Revision: HCFA-PM-93-lJanuary 1993
State/Terri.tory:
76
(BPD)nfHt\~l
New Jersey
Citation
42 CFR 431.152;AT-79-1852 FR 22444;Sees.1902(a) (28) (0) (i)and 1919(e)(7) ofthe Act; P.L.100-203 (Sec. 4211(c)).
4.28 Appeals Process
(a) The Medicaid agency hasestablished appeals proceduresfor NFs as specified in 42 CFR431.153 and 431.154.
(b) The State provides an appeals systemthat meets the requirements of 42 CFR431 Subpart E, 42 CFR 483.12, and42 CFR 483 Subpart E for residents whowish to appeal a notice of intent totransfer or discharge from a NF and fori.ndividuals adversely affected by thepreadmission and annual resident reviewrequirements of 42 CFR 483 Subpart C.
/
TN No. 91f-lQ:OO m---"'Supersedes Approval Date 14I\N t '.\ 'l:I9~TN No. 3<g-3L
Effective Date APR 1 - 1994

77
New: HCFA-PM-99-3JUNE 1999
State: ~N~e~w~Je~rse=.,.l.y _
Citation
OFFICIAL
1902(a)(4)(C) of theSocial Security ActP.L. 105-33
1902(a)(4)(D) of theSocial Security ActP.L. 105-331932(d)(3)42 CFR 438.58
TN # _0,,-,,3~-O,,-,7,-- _~ Supersedes TN #.-29-19 _
4.29 Conflict of Interest Provisions
The Medicaid agency meets the requirements ofSection 1902(a)(4)(C) of the Act concerning theprohibition against acts, with respect to any activityunder the plan, that are prohibited by section 207or 208 oftitle 18, United States Code.
The Medicaid agency meets the requirements of1902(a)(4)(D) of the Act concerning the safeguardsagainst conflicts of interest that are at least asstringent as the safeguards that apply under section27 of the Office of Federal Procurement Policy Act(41 U.S.c. 423).
03-07-MA (NJ)
Effective Date AUG 13 Z003Approval Date MAR 1 120M
Revision: HCFA-PK-87-14OCTOBER 1987
78
(BERC) OMB No.: 0938-0193
State/Terr'itory: NEW JERSEY
Citation42 CFR 1002.203AT-79-5448 FR 374251 FR 34772
4.30 Exclusion of Providers and Suspension ofPractitioners and Other Individuals
(a) All requirements of 42 CFR Part 1002, Subpart Baremet.
~ The agency, under the authority of State law,imposes broader sanctions.
No. 'BB-.5ersedesNo . .M::llf
Approval Date Effective Date
HCFA ID: 1010P/0012P
Revision: HCFA-AT-87-l4OCTOBER 1987
(BERC)
78a
OMB No.: 0938-01934.30 continued
StatefTerritory: N~ew.:..:...:J'-"'ers=ey~ _
Citation
1902(P) of the Act
42 CFR 438.808
1932(d)(l)42 CFR 438.610
(b) The Medicaid agency meets the requirements of-
(1) Section 1902(P) of the Act by excluding fromparticipation-
(A) At the State's discretion, any individual or entity for anyreason for which the Secretary could exclude theindividual or entity from participation in a programunder title xvru in accordance with sections 1128,ll28A, or 1866(b)(2).
(B) Any MCO (as defined in section 1903(m) of the Act), oran entity furnishing services under a waiver approvedunder section 1915(b)(1) of the Act, that -
\
(i) Could be excluded under section 1128(b)(8)relating to owners and managing employees whohave been conyi.cted of certain crimes orreceived other sanctions, or
(ii) Has, directly or indirectly, a substantialcontractual relationship (as defined by theSecretary) with an individual or entity that isdescribed in section 1128(b)(8)(B) of the Act.
(2) An MCO, PiliP, PAHP, or PCCM may not haveprohibited affiliations with individuals (as definedin 42 CFR 438.610(b)) who are suspended, or otherwiseexcluded from participating in procurement activities underthe Federal Acquisition Regulation or from participating innon-procurement activities under regulations issued underExecutive Order No.12549 or under guidelinesimplementing Executive Order No. 12549. If the State findsthat an MCO, PCCM, PiliP, or PAHP is not in compliance,the State will comply with the requirements of 42 CFR438.610(c)
03-07-MA (NJ)
...... TN # --"-03"'---"-07-'-- _Supersedes TN #---,8~8e---"-0,,,-5 _
Effective Date AUG 1 3 2003Approval Date MAR 1 7 2004

Revision: HCFA-AT-87-14OCTOBER 1987
(BERC)
78b
OMB No.: 0938-01934.30 continued
Statetrerritory: ~N:.::e'-'-'w_'J'_"erse='_'_y _
Citation1902(a)(39) of the Act (3) Section 1902(a)(39) of the Act by-
(A) Excluding an individual or entity from participation forthe period specified by the Secretary, when required bythe Secretary to do so in accordance with sections 1128or 1128A of the Act; and .
(B) Providing that no payment will be made with respect toany item or service furnished by an individual or entityduring this period.
(c) The Medicaid agency meets the requirements of_
(1) Section 1902(a)(41) of the Act with respect to promptnotification to CMS whenever a pro\,ider is terminated,suspended, sanctioned or otherwise excluded fromparticipating under this State plan; and
(2) Section 1902 (a)(49) ofth~ Act with respect to providinginformation and access to information regarding sanctionstaken against health care practitioners and providers by Statelicensing authorities in accordance with section 1921 of theAct.
03-07-MA (NJ)
...... TN # -"-'03"---"-07-'-- _Supersedes TN #-..-:.8='.-'8"---"-05"-- _
. AUG 13 2003Effecttve Date
-.,..,.~-.,--,--=""..,..-
Approval Date MAR 1 7 20~

Revision: HCFA-PM-87-14 (BERC)October 1997
OMB No: 0938-0193
Citation455.10344 FR 416441902(a)(38)of the ActP.L. 100-93(sec, 8(f))
435.940through435.96052 FR 59671903(rlof theAct1137 of theAct
State/Territory: NEW JERSEY
4.31 Disclosure of Information by Providers and Fiscal AgentsThe Medicaid agency has established procedures for the disclosureof information by providers and fiscal agents as specified in 42 CFR455.104 through 455.106 and sections 1128(b)(9) and 1902(a)(38) ofthe Act.
4.32 Income and Eligibility Verification System
(a) The Medicaid agency has established a system for income andeligibility verification in accordance with the requirements of Section1137 of the Act and 42 CFR 435.940 through 435.960.
(b) ATTACHMENT 4.32-A describes, in accordance with 42 CFR435.948{a)(6) the information that will be requested in order to verifyeligibility or the correct payment amount and the agencies and theState(s) from which that information will be requested.
TNNo.: 12-03
SupersedesTN No.: 88-5
Approval Date:
Effective Date:
0 6 2012-
0 1 2012
Revision: HCFA-PM-87-14OCTOBER 1987
(BERC)
79a
OHa No.: 0938-0193
State/Terdtory: NEW JERSEY
Citation1902(a)(48)of the Act,P.L. 99-570(Section 11005)P.L 100-93(sec. 5(a)(3»
4.33 Medicaid Eligibility Cards for Homeless Individuals
(a) The Medicaid agency has a method for making cardsevidencing eligibility for medical assistanceavailable to an individual eligible under theState's approved plan who does not reside in apermanent dwelling or does not have a fixed home ormailing address.
(b) ATTACHMENT 4.33-A specifies the method for issuanceof Medicaid eligibility cards to homelessindividuals.
TN No. B~-5
SupersedesTN No. ~q>
Approval Date _ Effective Date
HCFA ID: 1010P/0012P
-(r u.s. GOVERNMENT PRINTING OFFICE: 1987- 2 0 1 - 8 1 8 / 6 0 '+ 3 7

OFACIAl79b
Revision: HCFA-PM-88-10 (BERC)SEPTEMBER 1988
OKS No.: 0938-0193
State/Territory: New .Jersey
~ n~
TIII~!;:;i!
Citation1137 ofthe Act
P.L. 99-603(see. 121)
TN No . .m5...::...:9\SupersedesTN Yo. -
4.34 Systematic Alien Verification for EntitlementsThe State Medicaid agency has established proceduresfor the verification of alien status through theImmigration & Naturalization Service (INS) designatedsystem, Systematic Alien Verification for Entitlements(SAVE), effective October 1, 1988.
L-/ The State Medicaid agency has elected toparticipate in the option period of October 1, 1987to September 30, 1988 to verify alien statusthrough the INS designated system (SAVE).
L-/ The State Medicaid agency has received thefollowing type(s) of waiver from participation inSAVE.
L-/ Total waiver
L-/ Alternative system
L-/ Partial implementation
Approval oat.JAffT91989 Effective Date OCT 1 1988
HcrA 10: 1010P/0012P
state/Territory:
~~
Revision: HCFA-PM-95-4JUNE 1995
(HSQB)
79c.1
New Jersey
'~
~
Citation
42 CFRS488.402(f)
42 cnS488.434
42 cnS488. 402-< f) (2 )
42 eFRS488.456(c) (d)
42 CFRS488.488.404(b)(1)
4.35 Enforcement of Compliance for Nursing Facilities
(a) Notification of Enforcement Remedies
When taking an enforcement action against a nonstate operated NF, the State providesnotification in accordance with 42 CFR488.402(f).
(i) The notice (except for civil money penaltiesand State monitoring) specifies the:
(1) nature of noncompliance,(2) which remedy is imposed,(3) effective date of the remedy, and(4) right to appeal the determination
leading to the remedy.
(ii) The notice for civil money penalties is inwriting and contains the informationspecified in 42 cn 488.434.
(iii) Except for civil money penalties andState monitoring, notice is given at least 2calendar days before the effective date ofthe enforcement remedy for immediate jeopardysituations and at least 15 calendar daysbefore the effective date of the enforcementremedy when immediate jeopardy does notexist.
(iv) Notification of termination is given to thefacility and to the public at least 2calendar days before the remedy's effectivedate if the nonco~pliance constitutesimmediate jeopardy and at least 15 calendardays before the remedy's effective date ifthe noncompliance does not constituteimmediate jeopardy. The State must terminatethe provider agreement of an NF in accordancewith procedures in parts 431 and 442.
(b) Factors to be Considered in Selecting Remedies
(i) In determining the seriousness ofdeficiencies, the State considers the f~ctors
specified in 42 CFR 488.404(b)(1) & (2).
The State considers additional factors.Attachment 4.3S-A describes the State'sother factors.
. JUl. 0 1 1995Effective Date:-------
Revision: HCFA-PM-95-4.r'::iE 1995
(HSQB)
79c.2
State/Terri~ory:
Citatio::
New Jersev
c) Aoolication of Remedies
42 CFRS~88.410
42 CFRS488.417(b)S1919(h)(2)(C)of the Act.
42 CFRS488.414S1919(h) (2) (D)of the Act.
~2 C?:l5~88.~03
19l9(h) (2) (A)0: ~he Ac~.
~2 C=?.S483.4l2(c.)
(i)
(ii)
(iii)
(-.. )
If there is immediate jeopardy to residenthealth or safety, the State terminates theNF's provider agreeme~~ within 23 calendardavs from the date cf ~he last su=vey cr:_:e~~a·ely irnooses -D-jO-a-y rnanace~e~~ ~o~~c;; ;he th~~at ~~;;;; 23-days. -
The State impbses the c~nial of payme~t
(or its approved al~ernative) with respec~
to any individual a~itted to an NF thathas not come into substantial compliancewithin 3 months after the last day of thesu-vey.
The State imposes the denial of payment fornew admissions remedy as specified inS488.417 (or its approved alternative) anda State monitor as s~cified at 5488.422,when a facility has been found to haveprovided substandard ~ality of ~are on thelast three consecutive standard surveys.
:~e S~a=e fellows t~e =riteria speci:ie= a~
42 C??. S~38.40S(c)(2:, S4S8.~C5(d)(2), c~~
54~=.~08(e)(2), ~he:: i~ ~~?osp.s re~e~ie5 .?~a=e of or in addi~i=:: tc te~ina~ic::.
t·;::e:: i.::'".::1edi2.~e j eo;::c.=::;" c.oes nc-:. exis-:, :.=-~e
S-:.=::e ~e~':'n2:.es 2.:: ~;:' s ~=c....,..i.c.e= a:;=2e=.e:-.-:.~= ~~~e= ~~c~ E ~~~~~~ :==~ ~~e :~~~~~~ ::~=~===~~~2~~e, ~= ~~= ==~=~~~~~S c: ~= =:~
4==.~:2(a) ~=e ~c~ ~e~.
42 C??5 48 2.42':0(::;)Sl'?l5'(~) (2) p.)0: ~he Ac-=..
t ~ \\ -/
_x_ (l) Termination(2) Temporary Mana~e=e~t
(3) Denial of Payme~~ :or New Admissicr.s(4) Civil Money Penal~ies
(S) Transfer of Residents; Transfer 0:Residents with Closure of Facility
(6) State Mo~itorin;
A~tachments 4.3S-B through 4.35-G describe the crite=iafor applying the above remedies.
x (7)X (8)
Directed Plan of CorrectionDirected Inservice Training
TN No; "'5 - ~ '5
;~~~~~~.pproval Dat~'t.J.N--.1-W997 E::ective Date: l,lUl. 0 1 1995

Revision: HCFA-PK-95-4JUNE 1995
(HSQB)
79c.3
citation
state/Territory: New .Jersey
Attachments 4.35-B through 4.35-G describe thealternative remedies and the criteria for applying them.
(e) L State Incentive Programs
42 CFRS488.406(b)S1919(h)(2)(B)(ii)of the Act.
42 cnS488.303(b)1910(h)(2)(F)of the Act.
(il) _
(1)(2)(3)(4)
(5)
x (1)=(2)
Of~ l
The State uses alternative remedies.The state has established alternativeremedies that the State will impose inplace of a remedy specified in 42 CFR488.406(b) •
Temporary ManagementDenial of Payment for New AdmissionsCivil Money Penalties _Transfer of Residents, Transfer ofResidents with Closure of FacilityState Monitoring.
Public RecognitionIncentive Payments
TN No. " S - ...,SSupersedes Approval Date: If ftl , 1 1991TNNO.~ ~
Effective Datel'-JUL 0 1 1995
Revision: HCFA-PM-91- 4AUGUST 1991
State/Territory:
(BPD)
79d
New Jersey
OFFICIALOMB No.: 0938-
Citation
1902(a)(1l)(C)and 1902(a)(53)of the Act
4.36 Reguired Coordination Between the Medicaid and WICPrograms
The Medicaid agency provides for the coordinationbetween the Medicaid program and the SpecialSupplemental Food Program for Women, Infants, andChildren (WIC) and provides timely notice andreferral to WIC in accordance with section 1902(a)(53)of the Act.
TN No. q 1-$"superse~lr~ ••• ApprovalTNNO.~
Date Effective Date __~O~C~T 1~19~9_1 _
HCFA 10: 7982E

Revision: HCFA-PM-91- 10DECEMBER 1991
State/Territory:
79n
(BPD)
New Jersey
OFFICIAL
Citation42 CFR 483.75; 42CFR 483 Subpart 0;Secs. 1902(a)(28),1919(e)(1) and (2),and 1919 ( f) (2 ) ,P.L. 100-203 (Sec.4211(a) (3»; P.L.101-239 (Secs.6901(b) (3) and(4»; P.L. 101-508(Sec. 4801(a»).
4.38
x
Nurse Aide Training and com~tency
Evaluation for Nursing Faci~ties
(a) The state assures that therequirements of 42 CFR483.1S0(a), which relate toindividuals deemed to meet thenurse aide training andcompetency evaluationrequirements, are met.
(b) The State waives the competencyevaluation requirements forindividuals who meet therequirements of 42 CFR483.150(b) (1).
(c) The State deems individuals whomeet the requirements of 42 CFR483.150(b)(2) to have met thenurse aide training andcompetency evaluationrequirements.
(d) The State specifies any nurseaide training and competencyevaluation programs it approvesas meeting the requirements of42 CFR 483.152 and competencyevaluation programs it approvesas meeting the requirements of42 CFR 483.154.
x (e) The State offers a nurse aidetraining and competencyevaluation program that meetsthe requirements of 42 CFR483.152.
(f) The State offers a nurse aidecompetency evaluation programthat meets the requirements of42 CFR 483.154.
TN No. u.::s=superse··_
WTN No.~ 1
Approval Date _A1'RTU1992_ Effective Date 'JAN 1"- 1992
Revision: HCFA-PM-91- 10DECEMBER 1991
state/Territory:
790(BPD)
New Jersey
OfflC\AlCitation42 crR 483.75; 42CFR 483 Subpart D;Secs. 1902(a)(28),1919(e)(1) and (2),and 1919 ( f) (2 ) ,P.L. 100-203 (Sec.4211 (a) (3) ); P. L.101-239 (Secs.6901(b) (3) and(4)); P.L. 101-508(Sec. 4801(a)).
(g)
(h)
If the State does not choose tooffer a nurse aide training andcompetency evaluation program ornurse aide competency evaluationprogram, the State reviews allnurse aide training andcompetency evaluation programsand competency evaluationprograms upon request.
The State survey agencydetermines, during the course ofall surveys, whether therequirements of 483.75(e) aremet.
fi) Before approving a nurse aidetraining and competencyevaluation program, the Statedetermines whether therequirements of 42 CFR 483.152are met.
(j) Before approving a nurse aidecompetency evaluation program,the State determines whether therequirements of 42 CFR 483.154are met.
(k) For program reviews other thanthe initial review, the Statevisits the entity providing theprogram.
(1) The State does not approve anurse aide training andcompetency evaluation program orcompetency evaluation programoffered by or in certainfacilities as described in 42CFR 483.151(b)(2) and (3).
TN No. ~SupersedesTN No. 'Me'll;
Approval Date "APR 3 0 1992 Effective Date J~A~N~1 1~99~2~
Revision: HCFA-PM-91-10DECEMBER 1991
79p(BPD) OFFICIAL
State/Territory: New ,Jerse,)'
The State, within 90 days ofreceivinq a request for approvalof a nurse aide traininq andcompetency evaluation proqram orcompetency evaluation proqram,either advises the requestorwhether or not the proqram hasbeen approved or requestsadditional information from therequestor.
(n)
(m)
The State does not qrantapproval of a nurse aidetraininq and competencyevaluation proqram for a periodlonqer than 2 years.
(0) The State reviews programs whennotified of substantive changes(e.q., extensive curriculummodification) •
Citation42 CFR 483.75; 42CFR 483 Subpart 0;Secs. 1902(a)(28),1919(e)(1) and (2),and 1919(f~(2),
P.L. 100-203 (Sec.4211 (a)(3»; P.L.101-239 (Secs.6901(b) (3) and(4»; P.L. 101-508(Sec. 4801(a».
( q)x
(p) The State withdraws approvalfrom nurse aide training andcompetency evaluation programsand competency evaluationprograms when the program isdescribed in 42 CFR483.151(b)(2) or (3).
The State withdraws approval ofnurse aide training andcompetency evaluation programsthat cease to meet therequirements of 42 CFR 483.152and competency evaluationprograms that cease to meet therequirements of 42 CFR 483.154.
(r) The State withdraws approval ofnurse aide traininq andcompetency evaluation proqramsand competency evaluationproqrams that do not permitunannounced visits by the State.
TN No.SuperseTN No. ..a...a.l~W
Approval Date 1992 Effective Date JAN t -. 1992
Revision: HCFA-PM-91-10DECEMBER 1991
State/Territory:
79q(BPD)
New Jersey
Off\&\~l
Citation42 CFR 483.75; 42CFR 483 Subpart 0;Secs. 1902(a)(28),1919(e)(1) and (2),and 1919 ( f) (2) ,P.L. 100-203 (Sec.4211(a) (3»; P.L.101-239 (Secs.6901(b)(3) and(4»; P.L. 101-508(Sec. 4801(a».
(s)
(t)
When the state withdrawsapproval from a nurse aidetraining and competencyevaluation program or competencyevaluation program, the Statenotifies the program in writing,indicating the reasons forwithdrawal of approval.
The State permits students whohave started a training andcompetency evaluation programfrom which approval is withdrawnto finish the program.
(u) The State provides for thereimbu~sement of costs incurredin completing a nurse aidetraining and competencyevaluation program or competencyevaluation program for nurseaides who become employed by orwho obtain an offer ofemployment from a facilitywithin 12 months of completingsuch program.
(v) The State provides advancenotice that a record ofsuccessful completion ofcompetency evaluation will beincluded in the State's nurseaide registry.
(w) Competency evaluation programsare administered by the State orby a State-approved entity whichis neither a skilled nursingfacility participating inMedicare nor a nursing facilityparticipating in Medicaid.
(x) The state permits proctoring ofthe competency evaluation inaccordance with 42 CFR483.154(d).
(y) The State has a standard forsuccessful completion ofcompetency evaluation programs.
TN No. !El::!)supersedjf •TN No. -flew. Approval Date~ Effective Date JAN 1.... 1992------
Revision: HCrA-PM-91-10DECEMBER 1991
State/Territory:
79r(aPD)
New Jersey
OFFICIAL
(z) The State includes a record ofsuccessful completion of acompetency evaluation within 30days of the date an individualis found competent.
(aa) The State imposes a lr.aximum uponthe number of times anindividual may take a competencyevaluation program (any maximumimposed is not less than 3).
Citation42 cta 483.75; 42crR 483 Subpart 0;Secs. 1902(a)(28),1919(e)(1) and (2),and 1919 (f) (2 ) ,P.L. 100-203 (Sec.4211(a) (3»; P.L.101-239 (Secs.6901(b) (3) and(4»; P.L. 101-508(Sec. 4801(a».
(bb)
(cc)
(dd)
(ee)
(ff)
The State maintains a nurse aideregistry that meets therequirements in 42 crR 483.156.
The State includes home heal~h
aides on the registry.
The State contracts theoperation of the registry to anon State entity.
ATTACHMENT 4.38 contains theState's description of registryinformation to be disclosed inaddition to that required in 42crR 483.156(c)(1)(iii) and (iv).
ATTACHMENT 4.38-A contains theState's description ofinformation included on theregistry in addition to theinformation required by 42 CFR483.156(c).
TN No. qfl.-....') -APR 3 a 1992supersec:rvl ,.. Approval DateTN No. -PIe...., Effective DateJAN 1- 1992
State/Te:::: :..::or"/:
nC:A-?~-7:;-l
Janua::-y i.99J(3?S)
7?s
New Jersey
OFFICi;\l
C:"':.3.t:..o;-:Sees.1902 (a) (23) (D) ( i)
and :919(e)(7) oft::e Act;? 1:... 100-203(Sec. 4211(e));i?:". 101-508{Sec. 4801(b)).
4.39 ?::eadm~s~:..=n Se::een:..ng and Annual~es~dent ~ev:..ew :..n Nurs:..nc :ae:..l:..~:..es
(a) 7he Mediea~d agency has in effec~ awr:..tten agreement with t::e State mentalhealth and mental retardat~on authorit:..esthat meet the requirements of 42 (CFR)431.622.(c) .
(b) The State operates a preadmission andannual res~dent rev lew program that meet5the requirements of 42 CFR 483.100-138.
(C) The State aoes not claim as "medicalassi.stance under the State ?lan" the costof services to individuals who shouldrece:..ve preadmission screenlng or annualresident review until such ind~viduals arescreened or reviewed.
(dl With the exception of NF serv£cesfurn:..shed to certain NF res:..dents definedin 42 CFR 483.118(c)(1), the State doesnot cla~m as "medical aSSlst.anee under theStat.e plan" the cost of NF serv~ces toindlvlduals who are found not to requireNF services.
(e) ATTACHMENT 4.39 specifies the State'sdef:..nition of spec~alized serVlces.
:-~l ~o. gLf-! 0 JII. 3 A'"su perseca.5g .- ..... ~ Approval Date IlL\N 1 ''d9ST:J ;.10.~
Effective Date APR 1 - 1994

791
Revision: HCFA-PM-93- 1 (BPO) January 1993 ClAl
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURTTY ACT SunefTemtory: -!-N..!.!E~W~J..!e<E~R~SE~Y~ _
4.39 Preadmission Screening and Annual resident Review in Nursing Facilities (Continued)
(f) Except for residents identified in 42 CFR 483.118(c) (I), the Slate mental health or mental retardation authority makes categorical determinations rnat individuals with certain mental cooditions or levels of severity of mental i!loess would nonnally require specialized services of such an intensity that a specialized services program could not be delivered by the State in most, if not all, NFs and that a more appropriate placement sbould be utilized,
-.A- (g) The State describes any categorical detenninatiohs it applies in ATIACHMENT 4.39-A.
10-08-MA (NJ)
TN: 10-08 Effective: July 1, 2010
Supersedes 94-10 Approved: DEC__2_2._'_Ola _

Revision: HCFA-PM-91-3 (HSQB)APRIL 1992
79u
OMB No.:
State/Territory: New Jersey...
4.40 Survey & Certification Process
(a) The State assures that the requirements ot1919(g) (1) (A) through (C) and section1919(g)(2)(A) through (E)(111) of ~he Actwh1ch relate to the survey andcertification of non-State ownedfacilities based on the requirements ofsection 19~9(b), (c) and (d) of the Act,are met.
CitationSections1919(g)(1)thru (2) and1919(g)(4)thru (5) ofthe Act P.L.100-203(sec.4212(a) )
1919(g)(1)(B) of theAct-
(b) The State conducts periodic educationprograms for staff and residents (andtheir representatives). Attachment 4.40-Adescribes the survey and certificationeducational program.
1919(g)(1)(C) of theAct
19l9(g) (1)(C) of theAct
1919(g) (1)(C) of theAct
1919(g) (1)(C) of theAct
(c) The State provides for a process for thereceipt and timely review andinvestigation of allegations of neglectand abuse and misappropriation of residentproperty by a nurse aide of a resident ina nursing facility or by anotherindividual used by the facility.Attachment 4.40-8 describes the State'sprocess.
(d) The State agency responsible for surveysand certification of nursing facilities oran agency delegated by the State surveyagency conducts the process for thereceipt and timely review andinvestigation of allegations of neglectand abuse and misappropriation of residentproperty. If not the State survey agency,what agency?
(e) The State assures that a nurse aide, foundto have neglected or abused a resident ormisappropriated resident property in afacility, is notified of the finding. Thename and finding is placed on the nurseaide registry.
(f) The State notifies the appropriatelicensure authority of any licensedindividual found to have neglected orabused a resident or misappropriatedresident property in a faci11ty.
TN No. t\ -\ -'tSupersedesTN No.
Approval Dattt!UN 1 1 \~ :JAN t) 1 1993Effective Date _
HCFA ID:
Revision: HCFA-PM-92-3APRIL 1992
State/Territory:
79v
(HSQS)
New Jersey
OMS No:
..1919(g)(2) (g)(A) (i) ofthe Act
1919(g) (2) (h)(A) (ii) ofthe Act
1919(g)(2) (i)(A)(iii)(I)of the Act
1919(g)(2) (j)(A)(iii)(II)of the Act
1919(g)(2) (k)(8) of theAct
1919(g)(2) (1)(C) of theAct
OFFIC~Al
The State has procedures, as provided for atsection 1919(g)(2)(A)(i), for the scheduling andconduct of standard surveys to a.sure that theState has taken all reasonable steps ~o avoidgiving notice through the. scheduling proceduresand the conduct of the surveys themselve••Attacbment 4.40-<: describes the State'sprocedure••
The State assures that each facility shall havea standard survey which includes (for a case-mixstratified sample of residents) a survey of thequality of care furnished, as measured byindicators of medical, nursing andrehabilitative care, dietary and nutritionalservices, activities and social participation,and sanitation, infection control, and thephysical environment, written plans of care andaudit of resident's assessments, and a review ofcompliance with resident's rights not later than15 months after the date of the previousstandard survey.
The State assures that the Statewide averageinterval between standard surveys of nursingfacilities does not exceed 12 months.
The State may conduct a special standard orspecial abbreviated standard survey within 2months of any change of ownership,administration, management, or director ofnursing of the nursing facility to determinewhether the change has resulted in any declinein the quality of care furnished in thefacility.
The State conducts extended surveys immediatelyor, if not practicable, not later that 2 weeksfollowing a completed standard survey in anursing facility which is found to have providedsubstandard care or in any other facility at theSecretary's or State's discretion.
The State conducts standard and extended surveysbased upon a protocol, i.e., survey forms,methods, procedures and guidelines developed byHCFA, using individuals in the survey team whomeet minimum qualifications established by theSecretary.
TN No. L\:s~q;
SupersedesTN No.
Approval Date JUN 11 1997 Effective Date :IAN 0 1 1993;
HeFA IO:
Revision: HCFA-PM-92- 3APRIL 1992
State/Territory:
79w
(HSQB)
New Jersey
OMB No:
1919(g)(2)(D) of theAct
1919(g)(2)(E)(i) ofthe Act
1919(g)(2)(E) (ii) ofthe Act
1919 (9) (2)(E)(iii) ofthe Act
1919(9) (4)of the Act
1919(9) (5)(A) of theAct
1919(9) (5)(8) of theAct
1919(9) (5)(e) of theAct
1919(9)(5)(D) of theAct
(m)
(n)
(0)
(p)
(q)
(r)
(s)
(t)
(u)
The State provides for programa to measure andreduce inconsistency in the application ofsurvey results among surveyors. Attachment4.40-D describes the State·s programs.
The State uses a multidisciplinary team ofprofMssionals including a registeredprofessional nurse..The State assures that members of a survey teamdo not serve (or have not served within theprevious two years) as a member of the staff orconsultant to the nursing facility or has nopersonal or familial financial interest in thefacility being surveyed.
The State assures that no individual shall serveas a member of any survey team unless theindividual has successfully completed a trainingand test program in survey and certificationtechniques approved by the Secretary.
The State maintains procedures and adequatestaff to investigate complaints of violations ofrequirements by nursing facilities and onsitemonitoring. Attachment 4.40-& describes theState's complaint procedures.
The State makes available to the publicinformation respecting surveys and certificationof nursing facilities including statements ofdeficiencies, plans of correction, copies ofcost reports, statements of ownership and theinformation disclosed under section 1126 of theAct.
The State notifies the State long-term careombudsman of the State's finding of noncompliance with any of the requirements ofsubsection (b), (c), and (d) or of anyadverseactions taken against a nursing facility.
If the State finds substandard quality of carein a facility, the State notifies the attendingphysician of each resident with respect to whichsuch finding is made and the nursing facilityadministrator licensing board.
The State provides the State Medicaid fraud andabuse agency access to all informationconcerning survey and certification actions.
·-HCFA 10:
;;;;TN....-:;N'=""O-.-:,,::-:.s~_-r\{"""'---------J'7:U-:-N:-:--]-]-1~9~9~'J~------AMft 0 1 1993supersediS Approval Dat , Effective Date _TN N0~Jl~".,
~,~,;;;; VJ"'V :

Revision: HCFA-PH-92"': 2~lo\RCH 1992
79x
.(HSQB)
State/TerritorY: N_e_w__J_e_r_s_e~y __
Citation 4.41 Resident Assessment for Nursing Facilities
Sections1919(b) (3)and 1919(e)(5) ofthe Act
1919(e)(5)(A) of theAct
( a)
(b)
The State specifies the instrument to be used bynursing facilities for conducting acomprehensive, accurate, standardized,reproducible assessment of each resident'sfunctional capacity as required inS19l9(b)(3)(A) of the Act.
The State is using:
the resident assessment instrumentdesignated by the Health Care FinancingAdministration (see Transmittal 1241 ofthe State Operations Manual)[S1919(e)(S)(A»); or
1919(e)(5)(B) of theAct
TN No.SuperTN No
Approval Date
x a resident assessment instrumentthat the Secretary has approved as beingconsistent with the minimum data set ofcore elements, common definitions, andutilization guidelines as specified by theSecretary (see Section 4470 of the State .Medicaid Manual for the secretary's-----~approval criteria) [S19l9(e) (5) (B)].
Effective DateHCFA 10: _
79y(1)
TATE PLAN UNDER TiTLE XIX OF THE SOCIAL SECURITY ACT
taterrerritory: Of Jersey
Citation
1902(a)(68) of the ActP.L. 109-171 (section 6032)
4.42 t.mp}oyee Education About False ClaimsRecoveries.
(a) The Medicaid ag~ney meets therequirements regarding establishment of policiesand procedures for the education of employees ofentities covered by section 1902(a)(68) of theSocial Secwity Act (the Act) regarding false claimsrecoveries and methodologies for oversight ofentities' compliancewlth these requirements.
(1) Definitions.
(A) An "entity includes a governmental agellcy,organization, unit corporation. partnership, orother bllsiness arrangement (including anyMedicaid managed care organization, irrespectiveof the form of business structure or arrangement bywhich it exists) whether for-profit or not-forprofit, which receives or makes payments, under aState Plan approved under title XIX or under anywaiver of such plan, totaling at least $5,000,000annually.
If an entity furnishes items or services at more thana single location or under more than onecontractual or other payment arrangement, theprovisions of section 1902(a)(68) apply if theaggregate payments to that entity meet theS5,000 000 annual threshold. This applies whetherthe entity submits claims for payments using one ormore provider identifitation or tax identificationnumbers.
A govenunental component providing Medicaidhealth care items or services for which Medicaidpayment') are made would qualify as an "entity"(e.g., a state mental health f!lcility or school district
T' 07-03- ~A (N.D'upersedes -r :~
Appro,,'a DateEffective Date
07-03-MA (NJ)
DEC 2 0 2007
JAN 0 I 2Q07
79y(2) 01;""1'-' ....,j ~~,." •.
< rrH,J'~;iLSTATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
Staterrerritory: New Jersey
4.42 Employee Education About False Claims Recoveries (continued)
providing school-based health services). A governmentagency which merely administers the Medicaidprogram, in whole or part (e.g., managing the claimsprocessing system or determining beneficiaryeligibility), is not, for these pLlrposes, considered to bean entity.
An entity will have met the 55,000,000 annualthreshold as ofJanuary I, 2007, if it received or madepayments in that amount in Federal fiscal year 2006.Future detenninations regarding an entity~s
responsibility stemming From the requirements ofsection 1902(a)(6K) will be made by January 1 of eachsubsequent year, based upon the amount of pa)Ulentsan entity either received or made under the State Planduring the preceding Federal fiscal year.
(8) An "employee" includes any ot1icer or employee ofthe entity.
eC) A "contractor" or "agent" includes any contractor,subcontractor, agent, or other person which Or who, onbehalf of the entity, furnishes, or otherwise authorizesthe fumishing ot; Medicaid health care items orservices. perf0n11S billing or coding functions, or isinvolved in the monitoring of health care provided bythe entity.
07-03-MA (N,J)
TN 07-03-MA ( 'J)Supersedes T!'i: NEW
Approval Date~:rfectiveDate
ut.C 'l. \) t0lj?
JIHJ () 1 zg07
79y(3) 'WA~
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY AC~tt\~~~;Statcrrerritory: New Jersey
4.42 Employee Education About False Claims Recoveries (continued)
(2) The entity must establish and disseminatewritten policies which mllst also be adopted by itscontractors or agents. Written policies may be on papcror in electronic form, but mllst be readily available toall employees, contractors, or agents. The entity neednot create an employee handbook ifnone alreadyexists.
(3) An entity shall establish written policies for011 employees (includinll management), and of anycontractor or agent of the entity, that include detailedinformation about the False Claims Act and the otherprovisions named in section J902(a)(68)(A). The entityshall include in those written policies detailedinformation about the entity's policies and proceduresfor detecting and preventing waste, fraud, and abuse.The entity shall also include in any employeehandbook a specific discussion of the laws described inthe written policies, thc rights of employees to bcprotected as whistleblowers and a spccific discussionofthe entity's policies and procedures for detectingand preventing fraud, waste, and abusc.
(4) The requirements of this law should beincorporated into each State's provider enrollmentagreements.
(5) The State will implement this State Planamendment on January 1, 2007.
(b) ATTACHMENT 4.42-A describes, in accordance withsection 1902(a)(68) of the Act, the methodology of complianceoversight and the frequency with which the State will re-assesscompliance on an ongoing basis.
07-03-MA (NJ)
TN 07-03-MA (NJ)Supersedes TN: NEW
Approval DllteEffective Oate
DEC 2 0 2001
JAN 0 1 7007

Jff\fAM.Section 4Page 79y
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
State/Territory: New Jersey
Citation1902(a)(69) of theAc\.PI 109-171(section 6034)
4.43 Cooperation with Medicaid Integrity Program EffortsThe Medicaid agency assures it complies with suchrequirements determined by the Secretary to be necessaryfor carrying out the Medicaid Integrity Program establishedunder section 1936 of the Act.
TN No. 08-08-MA (NJ)Supercedes NTN No New ew
Jl.I~; ~ ~ ZC~BApproval Date. _
Effective Date: I-_.I'_R_O_l_Z_0_0B__

4.44
79z
STATE PLAN UNDER TITLE XIX OF THE SOCIAL SECURITY ACT
STATE: NEW JERSEY
SECTION 4 - GENERAL PROGRAM ADMINISTRATION
Medicaid Prohibition on Payments to Institutions or Entities Located Outside of the United States
Citation Section 1902(a)(80) of the l The State shall not provide any payments for Social Security Act, P.l. 111-148 items or services provided under the State plan (Section 6505) or under a waiver to any financial institution
or entity located outside of the United States.
TN No. 11-02 Effective Date: January 1, 2011
Supersedes TN No. NEW ~,t~ Approval Date: APR 0 5 zun
jJj ~!, !~'P' '''ur

80
icn: HCFA-AT-80-38 (BFP)~1ay 22, 1980 ...... -."
---~..
State N_Ev_'_J_E_RS_E_Y _
SEX:TICN 5 PERSONNEL AIMINISI'RATIQ1
Citation42 CPR 432.10 (a)AT-78-90AT-79-23AT-80-34
5.1 Standards of Personnel Administration
(a) The Medicaid agency has established andwill maintain methcds of personreladministration in conformity withstandards prescribed by the U.S. CivilService Ccmmission in accordance withSection 208 of the IntergovernmentalPersonnel Act of 1970 and the regulationson ~nministrationof the Standards for aMerit System of Personnel Administration,5 CFR Part 900, Subpart F. Allrequirements of 42 CPR 432.10 are met.
U The plan is locally administered andState-supervised. The requirementsof 42 CPR 432.10 with respect tolocal agency administraticn are met.
- (b) Affirmative Action Plan
The Medicaid agency has in effect anaffirmative action plan for equalen"q?loyment ofPOl=tunity that includesspecific action steps and timetables andmeets, all other requirements of 5 CPRPart 900, Subpart F•
........ ~N * 77-11Supersedes'IN # 74 -/~
Approval Date ,,-2'-77 Effective Date 7 -/-77

·ision:
81
HCFA-AT-80-38 (BPP)May 22, 1980
State NEW JERSEY
5.2 [Reserved]
~iijl~?~~~~'·.
ft~~~::~,:/
I #........ sup-"-e-rs-ed--:;""e-s--
W#~----
Approval Date _ Effective Date----
82
iiorl: HCFA-AT-80-38 (BPP)May 22, 1980
State N_E_W~JE.....;.R...:;.S..:;;.EY~ _
\::..,'- ::.·,\•..-··c-_~·~~;:::-::".~"~-
Citaticn42 CFR Part 432,Sul:part BAT-78-90
5.3 Trainina Proorams; Sub?rofessional andVolunteer prbgrarrs
The Medicaid agency meets the requirements of42 CFR Part 432, Subpart B, with respect to atraining program for agency personnel and thetraining and use of subprofessional staff andvolunteers.
"';--'-':'.-..;,-.
.......... 'IN # 73-1Supersedes'IN * 77 -/1
Effective Date 3 -/-It'
83
ision: HCFA-AT-SO-38 (BPP)~ May 22, 1980
c ." _ . ~.,
State~ NE_\t_J_J_ER_S_E_Y _
SECTICN 6 FJNAN:IAL ArMINISTRATICl'l
Citaticn42 CPR 433.32AT-79-29
6.1 Fiscal Policies and Accountabilitv
The Medicaid agency and, where applicable,local agencies administering the plan,mai~tains an accounting system and supportingfiscal records adequate to assure that claimsfor Federal funds are in accord withapplicable Federal requirements. Therequirements of 42 CPR 433.32 are met. .'.,: .. ~:.
;: ~:" .. :.~'
. d #: 74-/1.......supersedes
'IN ~ 7t> -'}Approval Date 7-27- 7~ Effective Date£- -sa-1"

Effective Date, 1-/fs. -%~
'!here is an afProved cost allocationplan en file with the Department inacrordance with the requirementscontained in 45 CFR Part 95, Subpart E.
6.2 Cost Allocatien
AQ;?roval Date
84
HCFA-AT-82.- 10 (BPI')
State__N_E..;.W.....;..JE.;;..R.;.;S;.;;E..;.Y _
Citatioo42 CFR 433.3447 FR 17490
· . . ~
'IN i i't!. - {i
Supersedes'IN t 7,,-n
(t Revisioo:
~-'
.~.i'.-.. '.,-

85
ision: HCFA-AT-80-38 (BPP)May 22, 1980
'-'State N_E_\~_J_E_R_SE_Y _
.....".
ation~'R 433.3379-2980-34
--~
6.3 State Financial Participatim
(a) State funds are used in !:::oth assistanceand administration.
U State funds are used to pay all ofthe non-Federal share of totalexpenditures under the plan.
I.lJ There is lccal participation. Statefunds are used to pay not less than40 percent of the non-Feder~l shareof the total experrlitures under theplan. There is a method ofapportioning Federal and State fundsamong the political subdivisions ofthe State on an equalization or otherbasis which assures that lack ofadequate func1s fran local sourceswill not result in lcwer ing thearrount, duration, srope or quality ofcare and services or level ofadministration under the plan in anypart of the State.
(b) State and Federal funds are awortionedarrong the polltical subdivisions of theState on a basis consistent with equitabletreatment of individuals in similarcircumstances throughout the State.
.:.. - ........~ - -
n::S~
!fi. -,Approval Date 7- c.'7-7l. Effective Date '-3(;j-J~
OFFICIAL86
Revision: HCFA-PM-91- 4AUGUST 1991
State/Territory:
(BPD)
New Jersey
OMS No. 0938-
Citation
42 CFR 430.12(c)
7.1
SECTION 7 - GENERAL PROVISIONS
Plan Amendments
The plan will be amended whenever necessary toreflect new or revised Federal statutes orregulations or material change in State law,organization, policy or State agency operation.
TN No. g/-31Supersedes 7 / Approval DateTN No. 7_- b
DEC 5 1991 Effective Date
HCFA ID: 7982E
OCT 1199J
Revision: HCFA-PM-9l- 4AUGUST 1991
State/Territory:
87
(BPD)
New Jersey
OMB No. 0938-
Citation
45 CFR Parts80 and 84
7.2 Nondiscrimination
In accordance with title VI of the Civil Rights Actof 1964 (42 U.S.C. 2000d et. seg.), Section 504 of theRehabilitation Act of 1973 (29 U.S.C. 70b), and theregulations at 45 CFR Parts 80 and 84, the Medicaidagency assures that no individual shall be subject todiscrimination under this plan on the grounds of race,color, national origin, or handicap.
The Medicaid agency has methods of administration toassure that each program or activity for which itreceives Federal financial assistance will be operatedin accordance with title VI regulations. These methodsfor title VI are described in ATTACHMENT 7.2-A.
TN No. j/-0$1 JAN 1 5 1992Supersedes ::: Approval Date _TN No. _1.1..9..1..--...;lQ....-__
Effective Date OCT 1 1991
HCFA ID: 7982E
Revision: HCFA-PM-91- 4AUGUST 1991
(BPD)
88
OMB No. 0938-
State/Territory: Ne_w__J_e_r__se_y _
<;:itation 7.3 Maintenance of AFDC Efforts
1902(c) ofthe Act
L!7 The State agency has in effect under its approvedAFDC plan payment levels that are equal to or more thanthe AFDC payment levels in effect on May I, 1988.
HCFA ID: 7982E
TN No. 97-90supersedr~'~'U'j~pproval DateTN No. d 3;, 'I'; t~rj1{
JAN 15 1992 Effective Date OCT () 1 1991

Off\C'~l89
7.4 StocR Goyernor', Review
Revision: HCFA-PM-91-4AUGUST 1991
State/Territory:
(8Po)
Hew Jersey
OKS No. 0938-
,.,2 eFR 430.12(b) The Medicaid agency will provide opportunity for the
Office of the GOvernor to review State plan amendmenta.long-ren9@ proqr~ pl~nnin9 projection., and other -.periodic report. thereon, excluding periodic.tati.tical, budget and fiscal report.. Any comment.made will be tran••itted to the Health Care FinancingAdmini.tration with .uch document••
JaV Not applicable. The Governor--
~ Doe. not wi.h to review any plan material.
L-/ Wi.he. to review only the plan material•• pecified in the enclo.ed document.
I hereby certify that I o. outhorized to .ub=it thi. plan on behalf of
oepartment of Hu.an Services(oe.ignated Single State Agency)
Date: .lIme 22. 1993
0J~J~ ~J----(Signature)
William Waldman, Co~nissioner
(Title)
HeFA ID: 79822:
::N No. 93-#7 SEP 1 - 1993Supersedes Approvol Dote-;NNo. 91-34
...
Effective Dote APR 1 - 1993

r';p' " '.'I)) f. J j,
1< ) ."j, I.) i /.:.
J,r l <[I." ,
Stelle of j;,\, ,-_. -_ .• - -~---
"
fl '")1
=-.-.J
1I
IJ,
, ~
Tbe: leu1 (n;.tl:')i':;.~y 'll~'.'l' \:);:\('11 t,]lC
the pJi.:n all a S~:::Lc',,·j.d :;~'.~ :i.sC~'S
:;"
, ;.. l
'~J
D ElllJc:r-\,rj"3j_r,~ tL(: ~J2""';(:~t-:.i~~L},::,"tiorl of th·::; rll~:n Lj' 10(:·1pJlitic2.l ::mb~E'\::~,iC'n:j,
The legal i,11Lll:Jl«,:,' ,11)':,.1' \;113 ell LL,:: ,::[;c:Jcy ~L:::':T'::~~>~::;
the ncl::llni;::,(,r'iiL:'i.O;; of the pJ.e<11 on 2. StdC'.;.U:..~ 'cds::'", isconl,,~:il1(d in
-.----->--~-';.~,.. -:-,-;... :(~--7'j-~..;:.;':..:-).---~-'~-"-'.'\ .,l'llLL,U"~. C.!.vul. .lC)l
The CJ LC}l}~~:/ t~) 1 c L~Jl.1. Cl111~,}:') ::.~j_-t / to ri:"; 1~,=: ruJ_ (; s 2.r-::Jthc.t (11'C bir::iin..; Oil the-: }JJliLic::-:l :'ut~::i'y:',-c:~c'n',
in£!, tIL: pl"Ij is
1" c: L.~:~,) l c~ t :.i. ':"~ ~-"..~L:. (~.~:J ~~~~~ ~_ ::~ ~ c :"'-~
1!.~,11
.~
December 1976
Ji lIttoJ:)H"<' (,(')1('1';)1 of 1;"",; :J(;::(~""
TiLle:
-