Star_Uncontrolled Life Threatening Bleeding_100115
23
UNCONTROLLED LIFE-THREATENING BLEEDING Resident(s): Ava Star M.D. Attending(s): Daniel Devun M.D. Program/Dept(s): Ochsner Clinic Radiology
Transcript of Star_Uncontrolled Life Threatening Bleeding_100115
UNCONTROLLED LIFE-THREATENING BLEEDING
Resident(s): Ava Star M.D.
Attending(s): Daniel Devun M.D.
Program/Dept(s): Ochsner Clinic Radiology

CHIEF COMPLAINT & HPI
7AM urgent phone call to IR:
58yo M PMH HCV cirrhosis, ascites, CKD stage III, poorly controlled DM2 who presented to ED last night with 1 episode bright red emesis.
Pt dx HCV 2004, cirrhosis dx 2011.
Pt has had multiple prior variceal hemorrhages requiring hospitalization x 3, most recently 5 months ago.
Subsequently admitted 2 months ago for elective banding of varices, at which time also underwent paracentesis.
Currently being evaluated by hepatology for liver transplant.
Patient admitted from ED with plan for endoscopy by Gastroenterology.
During endoscopy, esophageal variceal hemorrhage was identified 34cm from incisors.
3 bands were placed on varices distal to hemorrhage site.
Hemorrhage continued unabated.
IR consulted for emergent TIPS.
RELEVANT HISTORY
LABS
WBC 19.6 / HB 8.7 / Hct 25.9 / Platelets 131 / INR 1.5 / Na 135 / K 5.2 / Creatinine 18 / GFR 40.6 / Alk Phos 108 / Total Protein 5.7 / Albumin 2.1 / Total Bili 2.3 / AST 40 / ALT 21.
PRIOR TO ADMISSION MEDS
Insulin Lispro, Insulin Pump, Nadolol 20mg daily, Lasix 20-40mg daily, Pantoprazole 40mg daily, Spironolactone 100mg daily
INPATIENT MEDS AT TIME OF PHONE CALL
Ceftriaxone 1g q 24h, Precedex gtt, Norepinephrine gtt, Ocreotide gtt, Pantoprazole gtt

DIAGNOSTIC WORKUP
Only available imaging was CT Liver Triple Phase from 5 months earlier, revealing patent portal vein at that time (arrow).

ESOPHAGEAL VARICEAL HEMORRHAGE
Hemorrhage was identified during endoscopy arising from esophageal varices, which were unsuccessfully banded.
Patient was hemodynamically unstable, maxed out on 2 pressors, and Class A Anesthesia emergency was declared.
Plan was to perform an emergent TIPS in order to control the variceal hemorrhage and allow the patient to stabilize hemodynamically.
Conversation with sister (POA) detailed procedure, and the grim prognosis. It was explained that patient could die from blood loss without the procedure.
Pt was already developing laboratory evidence of multi-organ system dysfunction.

INTERVENTION: EMERGENT TIPS
Ultrasound of PV with the patient on the table confirmed PV patency prior to TIPS.
Hepatic vein free = 15
Hepatic vein wedge = 27

EMERGENT TIPS (CONT.)
Portal vein pressure = 40
Pre-TIPS gradient = 25

EMERGENT TIPS (CONT.)
10mm diameter, 2cm covered, 6cm uncovered Viatorr ® stent
Post TIPS pressures: Portal vein 28, hepatic vein 21
Post TIPS gradient = 7

CLINICAL FOLLOW UP: 6 DAYS LATER
Pt did well s/p TIPS.
No further bleeding.
Transferred to RNF.
While using commode, patient had episode of large volume hematemesis and became unresponsive.
Code called.
Pt transferred to ICU and intubated for airway protection.
IR called emergently.
“You’ve got to help us. This patient is bleeding to death. He has received 12u PRBC and 6u FFP and he is hypotensive maxed out on pressors.”

CLINICAL FOLLOW UP (CONT.)
We went to see the patient. Pt is covered in blood, intubated, with Blakemore drain and helmet.
Hemoglobin 5.1
Hematocrit 15.6
Platelets 70
INR 3.5
Plan?
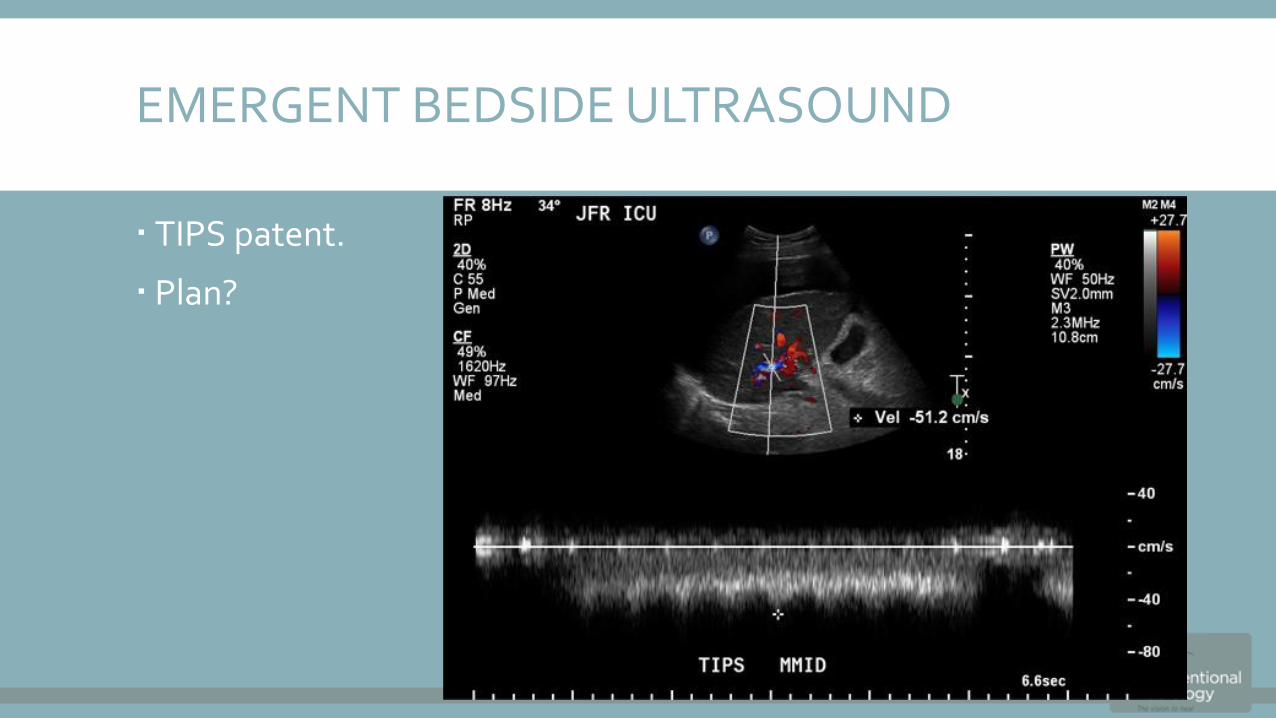
EMERGENT BEDSIDE ULTRASOUND
TIPS patent.
Plan?

PLAN
GI at bedside.
Given patency of TIPS, we requested GI to scope patient to determine if hemorrhage is arterial or venous as we did not see large varices at TIPS.
MELD 37

GI BEDSIDE UPPER ENDOSCOPY
“We can’t see anything. There is too much blood.”
“We think it is coming from a gastric band ulcer.”
“We think it is arterial based on the brisk flow and pulsatility. However, we are not certain.”
Plan?
QUESTION SLIDE
1) It is important to verify endoscopically the causes of continued or recurrent bleeding after TIPS placement or revision because nonvaricealbleeding can coexist in:
A: 2% of patients.
B: 5-10% of patients.
C: >33% of patients.
D: There is currently no evidence to support endoscopic verification of source of continued or recurrent hemorrhage post-TIPS.
CORRECT!
1) It is important to verify endoscopically the causes of continued or recurrent bleeding after TIPS placement or revision because nonvaricealbleeding can coexist in:
A: 2% of patients.
B: 5-10% of patients.
C: >33% of patients. Non-variceal bleeding can occur in >33% of post-TIPS patients, and it is important to verify the source prior to planned intervention.
D: There is currently no evidence to support endoscopic verification of source of continued or recurrent hemorrhage post-TIPS.
CONTINUE WITH CASE
SORRY, THAT’S INCORRECT.
1) It is important to verify endoscopically the causes of continued or recurrent bleeding after TIPS placement or revision because nonvaricealbleeding can coexist in:
A: 2% of patients.
B: 5-10% of patients.
C: >33% of patients. Non-variceal bleeding can occur in >33% of post-TIPS patients, and it is important to verify the source prior to planned intervention.
D: There is currently no evidence to support endoscopic verification of source of continued or recurrent hemorrhage post-TIPS.
CONTINUE WITH CASE

PLAN
Given arterial source of hemorrhage, inability of GI to control source endoscopically, and patient rapidly declining with multi-organ system dysfunction, maxed out on pressors, with transfusions unable to keep up with blood loss, decision was made to emergently embolize the left gastric artery.
Another call placed to patient’s sister (POA), again explaining the grim prognosis, the fact that the patient would almost certainly die without the procedure, and that there was no other option available to attempt to save his life.
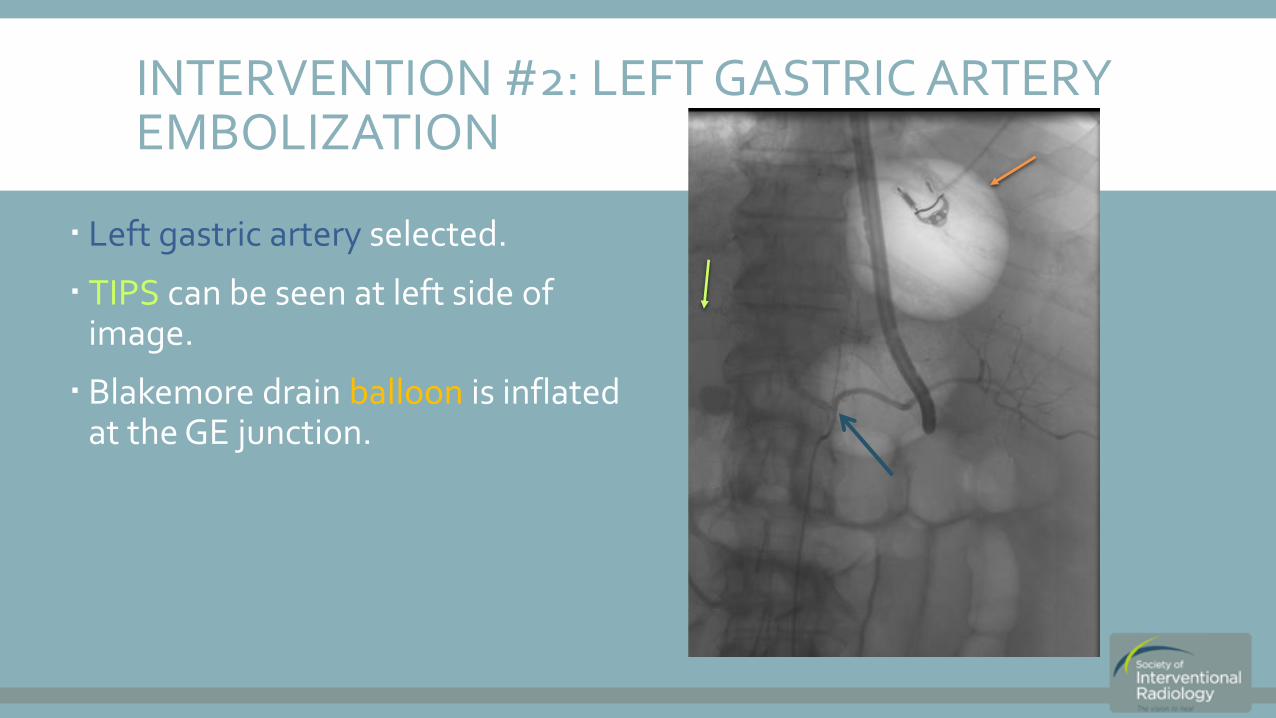
INTERVENTION #2: LEFT GASTRIC ARTERY EMBOLIZATION
Left gastric artery selected.
TIPS can be seen at left side of image.
Blakemore drain balloon is inflated at the GE junction.

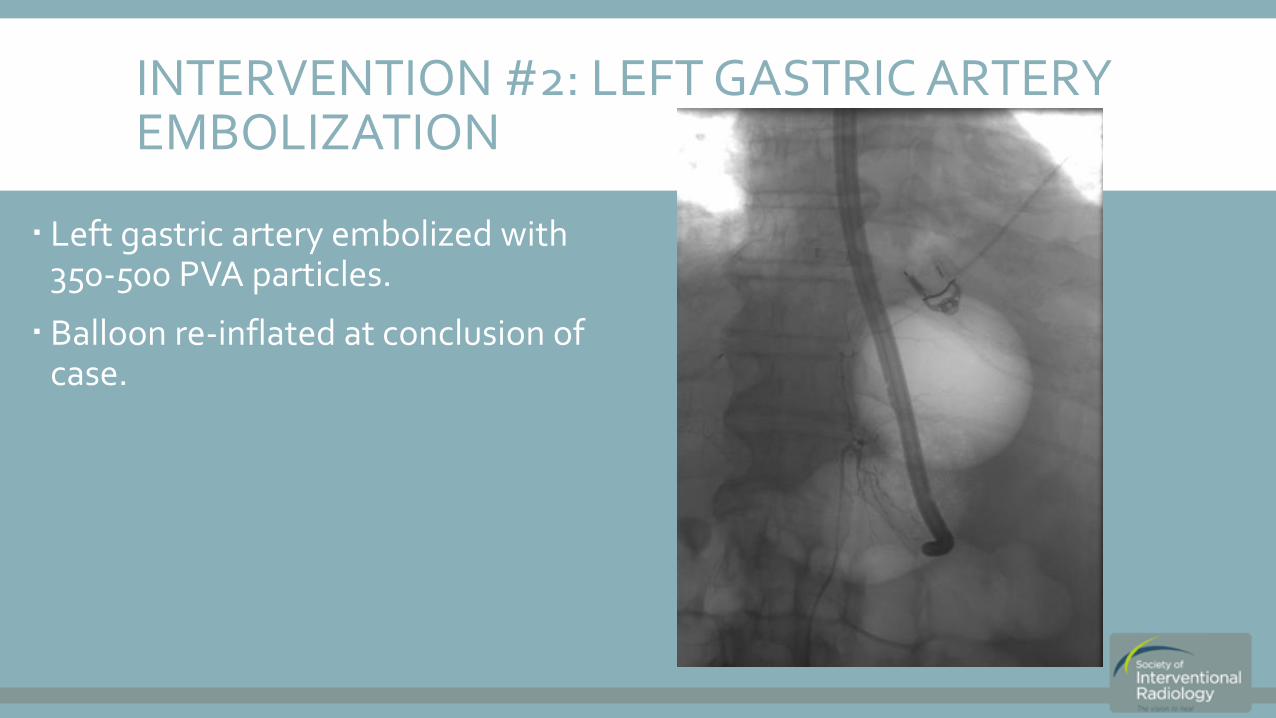
INTERVENTION #2: LEFT GASTRIC ARTERY EMBOLIZATION
Blakemore balloon deflated.
Run does not reveal active extravasation.
INTERVENTION #2: LEFT GASTRIC ARTERY EMBOLIZATION
Left gastric artery embolized with 350-500 PVA particles.
Balloon re-inflated at conclusion of case.

CLINICAL FOLLOW UP
Post-LGA embolization, Blakemore drain reinflated.
GI upper endoscopy the following day revealed no further hemorrhage.
Blakemore drain removed.
Patient did not encounter further bleeding during course of admission.
Remainder of hospital course was uneventful.
Listed for transplant.
Received liver transplant 2 weeks later.
Patient discharged in stable condition.
Patient doing well post-transplant.
SUMMARY & TEACHING POINTS
Emergent TIPS is indicated for life-threatening varicealhemorrhage unable to be otherwise controlled.
Hematemesis in cirrhotic patients is not always caused by esophageal variceal hemorrhage.
If we had performed a TIPS revision instead of a left gastric artery embolization on the patient after his 2nd episode of hematemesis, would he have survived?
REFERENCES & FURTHER READING
ACR-SIR-SPR Practice Parameters for the Creation of a Transjugular Intrahepatic Portosystemic Shunt (TIPS (2014)
Josen AS, Giuliani E, Voorhees AB, Jr., Ferrer JM, Jr. Immediate endoscopic diagnosis of upper gastrointestinal bleeding. Its accuracy and value in relation to associated pathology. Arch Surg 1976;111:980-986.
Waldram R, Davis M, Nunnerley H, Williams R. Emergency endoscopy after gastrointestinal haemorrhage in 50 patients with portal hypertension. Br Med J 1974; 4:94-96.
ACR-SIR-SPR Practice Parameters for the Creation of a Transjugular Intrahepatic Portosystemic Shunt (TIPS (2014)
Josen AS, Giuliani E, Voorhees AB, Jr., Ferrer JM, Jr. Immediate endoscopic diagnosis of upper gastrointestinal bleeding. Its accuracy and value in relation to associated pathology. Arch Surg 1976;111:980-986.
Waldram R, Davis M, Nunnerley H, Williams R. Emergency endoscopy after gastrointestinal haemorrhage in 50 patients with portal hypertension. Br Med J 1974; 4:94-96.