Standards of Care and Future Prosepectives in Lung Cancer ... · 1. Challenges and controversies in...
68
Spotlight: Case-based management issues in immuno-oncology Rolf Stahel Chair, Comprehensive Cancer Center Zürich 1 | Berlin, March 23, 2019 Do not duplicate or distribute without permission from author and ESO
Transcript of Standards of Care and Future Prosepectives in Lung Cancer ... · 1. Challenges and controversies in...

Spotlight:Case-based management issues in immuno-oncology
Rolf Stahel
Chair, Comprehensive Cancer Center Zürich
1 |
Berlin, March 23, 2019
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

1. Challenges and controversies in response evaluation
1. Pseudoprogression and GI toxicity
2. Hyperprogression
3. Durable clinical benefit, durable response
4. Major pathological response
5. Molecular response (ctDNA)
6. Abscopal effect and GI toxicity
7. Correlation between toxicity and response
8. Steroids and antibiotics
9. Special situations
2 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Case: 72-y/o women with lung adenocarcinoma3 |
Before nivolumab After 6 cycles nivolumab
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Guidelines for the evaluation of immune therapy activity in solid tumors:
Immune-related response criteria: Patterns of response to ipilimumab in
advanced melanoma
4 |
Wolchok, CCR 2009
Guidelines for the evaluation of immune therapy activity in solid tumors:
Immune-related response criteria: Patterns of response to ipilimumab in
advanced melanoma
3 |
Wolchok, CCR 2009
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Guidelines for the evaluation of immune therapy activity in solid tumors:
Immune-related response criteria: Patterns of response to ipilimumab in
advanced melanoma: Tumor Burden = SPDindex lesions+ SPDnew,
measurable lesions
5 |
Wolchok, CCR 2009
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Comparison of RECIST to immune-related response criteria in
patients with NSCLC treated with immune-checkpoint inhibitors
• Responses of 41 patients were
analyzed:
• Response rate:
• 29.2% assessed by RECIST v1.1
• 34.1% by irRC
• PD: 4.9% defined by RECIST but not
by irRC. The patients eventually
experienced tumor regression,
suggesting delayed
pseudoprogression.
6 |
Kim, Cancer Chemother Pharmacol, 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Pseudoprogression in previously treated patients with NSCLC who
received nivolumab monotherapy
• Retrospective cohort study in
15 centers
• Pseudoprogression:
PD at first evaluation by RECIST1.1
followed by objective response in
second evaluation
• 542 patients
• 20% typical response
• 53% progression
• 3% (14 pts) pseudoprogression
7 |
Fujimoto, JTO 2018
Tumor size in 14 pts with pseudoprogression
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Pseudo progression in previously treated patients with NSCLC who
received nivolumab monotherapy
8 |
Fujimoto, JTO 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Comparison of RECIST1.1 and iRECIST9 |
ETOP | Name Project | Title Presentation | Zurich, July 27, 2009 Seymour, Lancet Oncol 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

What happens after immune unconfirmed progressive disease (IUPD)10 |
Borcoman, Ann Oncol 2019
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Case: 72-y/o women with lung adenocarcinoma11 |
→ Biopsy of
mediastinal nodes:
Immune cells
→ Biopsy of the colon:
Colitis Grade 2
Curioni-Fonrecedro, Ann Oncol 2017
Before nivolumab After 6 cycles nivolumab
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Management of immune-related GI toxicity12 |
Haanen, Ann Oncol 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Management of immune-related GI toxicity13 |
Haanen, Ann Oncol 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Case: 72-y/o women with lung adenocarcinoma14 |
Before nivolumab After 6 cycles nivolumab After 12 cycles nivolumab
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Hyperprogressive disease: recognizing a novel pattern to improve
patient management
15 |
Champiat, Nat Rev Clin Oncl 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Hyperprogressive disease in patients with advanced NSCLC treated
with PD-1/PD-L1 inhibitors or with single-agent chemotherapy
• 406 pts treated with ICB in second line:
• 13.8% Hyperprogression*
• 4.7% Pseudoprogression
• 59 pts treated with chemotherapy in second line
• 5% Hyperprogression
• 0% Pseudoprogression
* associated with >2 metastatic sites
16 |
Ferrara JAMA Oncol 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Hyperprogressive disease in patients with advanced NDCLC treated
with PD-1/PD-L1 inhibitors or with single-agent chemotherapy
17 |
Ferrara JAMA Oncol 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Durable clinical benefit, durable response
No firm definition!
18 |
Brahmer, AACR 2017
Felip, ASCO 2018
Rizvi, Science 2015Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Neoadjuvant PD-1 blockade in resectable lung cancer with two
infusions of nivolumab 2 weeks apart: Major pathological response
19 |
Forde, ESMO 2016 and NEJM 2018
Pre-
nivo
Post-
nivo
63yo M, ex-smoker, adeno, PD-L1 2%+,
<10% viable tumor at resection
Pre-
nivo
% pathological regression:
MPR
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Pathological response after neoadjuvant chemotherapy in
resectable NSCLC: proposal for the use of major pathological
response as a surrogate endpoint
20 |
Hellmann, Lancet Oncol 2014
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Molecular response in ctDNA: Dynamics of tumor and immune
responses during immune checkpoint blockade in NSCLC
21 |
Pt 1 Pt 2
Anagnostou, CR 2019
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

47-y/o man with stage IIIB lung adenocarcinoma
• July 2014 Stage IIIB lung
adenocarcinoma (cT1pN3CM0)
• August – September 2014 3 cycles
chemotherapy with cisplatin, docetaxel
and cetuximab (SAKK 16/08)
• September – October 2014
Radiotherapy of primary tumor and
mediastinal nodes
• November 2014 resection of RUL and
mediastinal lymphadenectomy:
pT0pN0,M0
22 |
July 2014 October 2014Do n
ot duplic
ate o
r dist
ribute
with
out
permiss
ion from
auth
or and E
SO

47-y/o man with stage IIIB lung adenocarcinoma
• January – June 2015 3
cycles of carboplatin and
pemetexed followed by
pemetrexed maintenance
• June 2015 Progress in
retroperitoneal and
mediastinal nodes;
Initiation of treatment with
nivolumab
23 |
January 2015 March 2015
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

47-y/0 man with stage III lung adenocarcinoma24 |
June 2015 October 2015 January 2016 August 2017
Britschgi, Rad Oncol 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

47-y/o man with stage IIIB lung adenocarcinoma
• May 2016 admission
by ER because of
vomiting and
abdominal pain
25 |
May 2016Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

47-y/o man with stage IIIB lung adenocarcinoma
• May 2016 admission
by ER because of
vomiting and
abdominal pain
• May-July 2016
treatment with
methyprednisolone IV,
followed by
prednisone PO,
initially 100 mg, than
slowly reduced
26 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Case 1: 64-y/o man with squamous cell lung carcinoma
• June 2015:
• Squamous cell carcinoma right upper
lobe with lymph node and bone metastases
• Pathology: strong positivity of PD-L1
27 |
PD-L1 stainingDo not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Case 1: 64-y/o man squamous cell lung carcinoma
• July – September 2015: Chemotherapy with cisplatin/gemcitabine 3 cycles
• October 2015: Palliative resection of right upper lobe
28 |
June 2015 September 2015 November 2015Do n
ot duplic
ate o
r dist
ribute
with
out
permiss
ion from
auth
or and E
SO

Case 1: 64-y/o man squamous cell lung carcinoma
• November 2015: Symptomatic and radiological progression in bone
• December 2015: Radiotherapy to thoracic and sacral lesion, two applications
of nivolumab
29 |
November 2015
January 2016:
Dyspnea on exertion
PiO2 67%
CRP 115
WBC 11 G/l
Hospitalization in intensive care: O2, Methylprednisolon
250 mg IV, followed by Prednison in slowly decreasing
amounts, piperacillin and bactrim
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Case 1: 64-y/o man squamous cell lung carcinoma30 |
November 2015 February 2016 March 2017Do n
ot duplic
ate o
r dist
ribute
with
out
permiss
ion from
auth
or and E
SO

Pneumonitis in
patients treated with
anti–PD-1/PD-L1
therapy
31 |
Naidoo, JCO 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Management of immune-related pulmonary toxicity32 |
ETOP | Name Project | Title Presentation | Zurich, July 27, 2009Haanen, Ann Oncol 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Management of immune-related pulmonary toxicity33 |
ETOP | Name Project | Title Presentation | Zurich, July 27, 2009Haanen, Ann Oncol 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Time of onset of immune-related adverse events34 |
Haanen, Ann Oncol 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Pneumonitis in patients treated with anti–PD-1/PD-L1 therapy
• Of 915 patients who received
anti–PD-1/PD-L1 mAbs, pneumonitis
developed in 43 (5%; 95% CI, 3% to 6%)
• Time to onset of pneumonitis ranged
from 9 days to 19.2 months.
• The incidence of pneumonitis was higher
with combination immunotherapy versus
monotherapy (19 of 199 [10%] v 24 of
716 [3%]; P < .01
35 |
Naidoo, JCO 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Pneumonitis in patients treated with anti–PD-1/PD-L1 therapy36 |
Naidoo, JCO 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Comparison of the toxicity profile of PD-1 versus PD-L1
inhibitors in NSCLC: A systematic analysis of the literature
37 |
Pillai, Cancer 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

55-y/o man with metastatic adenocarcinoma of the lung
• March 2017 adenocarcinoma with singular brain and multiple bone
metastases, no oncogenic driver mutation, PD-L1 negative
• April 2017 SBRT of brain metastases and palliative radiotherapy to painful
sacral metastasis
• May 18 and June 1, 2017 immunotherapy with ipilimumab and nivolumab as
part of a clinical trial
• June 6 presentation at ER with muscle pain and double vision:
38 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

55-y/o man with metastatic adenocarcinoma of the lung39 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

55-y/o man with metastatic adenocarcinoma of the lung40 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

55-y/o man with metastatic adenocarcinoma of the lung41 |
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Cardiovascular toxicities associated with immune checkpoint
inhibitors: an observational, retrospective, pharmacovigilance study
42 |
Salem, Lancet Oncol, 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Cardiovascular toxicities associated with immune checkpoint
inhibitors: an observational, retrospective, pharmacovigilance study
43 |
Salem, Lancet Oncol, 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Impact of immune-related adverse events on survival in patients
with advanced NSCLC treated with nivolumab
44 |
Riciuti, WCLC 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Impact of immune-related adverse events on survival in patients
with advanced NSCLC treated with nivolumab
45 |
Riciuti, WCLC 2018
Univariate HazardRatio (95% CI)
P valueMultivariate
Hazard Ratio* (95% CI)
P value
PFS
Any 0.41 (0.3-0.57) P < 0.0001 0.48 (0.34-0.67) P < 0.0001
Lung irAEs 0.54 (0.31-0.92) P = 0.024 0.56 (0.33-0.96) P = 0.038
Gastrointestinal irAEs 0.45 (0.26-0.77) P = 0.004 0.52 (0.3-0.9) P = 0.021
Endocrine irAEs 0.5 (0.34-0.72) P < 0.0001 0.59 (0.4-0.89) P = 0.011
Skin irAEs 0.51 (0.32-0.83) P = 0.007 0.57 (0.35-0.95) P= 0.031
Hepatobiliary irAEs 0.68 (0.4-1.16) P = 0.16 0.72 (0.41-1.24) P = 0.23
OS
Any 0.33 (0.23-0.47) P < 0.0001 0.38 (0.26-0.56) P < 0.0001
Lung irAEs 0.41 (0.21-0.78) P = 0.007 0.46 (0.24-0.89) P = 0.022
Gastrointestinal irAEs 0.38 (0.2-0.73) P = 0.004 0.5 (0.26-0.98) P = 0.045
Endocrine irAEs 0.49 (0.34-0.72) P < 0.0001 0.45 (0.28-0.72) P = 0.001
Skin irAEs 0.6 (0.36-1.02) P = 0.06 0.8 (0.46-1.39) P = 0.43
Hepatobiliary irAEs 0.84 (0.48-1.47) P = 0.55 0.94 (0.53-1.66) P = 0.83
ORR: 51.4% vs. 20%, P < 0.01
DCR: 84.3% vs. 34%, P < 0.00112-weeks landmark 12-weeks landmark
6-weeks landmark 6-weeks landmark
A B
C D
P < 0.0001
HR: 0.48 (95%CI: 0.34-0.69)
P < 0.0001
HR: 0.4 (95%CI: 0.26-0.59)
P = 0.089
HR: 0.69 (95%CI: 0.45-1.05)
P = 0.021
HR: 0.55 (95%CI: 0.33-0.92)
no-irAEs (n: 67) 7.5 (4.2-10.7)irAEs (n: 78) 21..4 (15.5-27.3)
mOS, months (95%CI)
no-irAEs (n:52) 3.2 (2.8-3.7)irAEs (n: 71) 8.0 (5.2-10.9)
mPFS, months (95%CI)
no-irAEs (n: 144) 9.1 (6.1-2.3)irAEs (n: 32) 17.8 (11.4-24.5)
mOS, months (95%CI)
no-irAEs (n:144) 2.8 (2.1-3.5)irAEs (n: 32) 5.0 (1.5-8.4)
mPFS, months (95%CI)
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Outcomes of long-term responders to anti-PD-1 and antiPD-L1
when being rechallenged with the same agent at progression
• 13 patients were treated
for colorectal MSI–high
genotype (n = 5), urothelial
carcinoma
(n = 3),melanoma (n = 2),
NSCLC (n = 2) and TNB
(n = 1) for a median of
12 months (range 10.6–12)
46 |
Bernard-Tessier, EJC 2018
2 PR, 6 SD
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Impact of baseline steroids on efficacy of PD-1 and PD-L1 blockade
in patients with NSCLC
47 |
MSKCC IGR MSKCC IGR
Arbour, JCO 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Negative association of antibiotics on clinical activity of immune
checkpoint inhibitors in patients with advanced renal cell and NSCLC
48 |
Derosa, Ann Oncol 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Profiling preexisting antibodies in patients treated with anti-PD-1
therapy for advanced NSCLC
• 137 patients analyzed for preexisting rheumatoid factors, antinuclear
antibody, anti-thyreoglobulin, and anti-thyroid peroxidase
49 |
Toi, JAMA Oncol 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Safety and efficacy of PD-1 inhibitors among HIV-positive patients
with NSCLC
50 |
Ostios-Garcia, JTO 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Safety and efficacy of PD-1 inhibitors among HIV-positive patients
with NSCLC
• Partial responses to immune checkpoint inhibitors were observed in three of
seven cases. Among four patients with a programmed death ligand-1 tumor
proportion score >5 0%, three partial responses were observed. All patients
received antiretroviral therapy while on anti–PD-1 treatment. None of the
patients experienced grade 3 or 4immune-related adverse events or immune
reconstitutioninflammatory syndrome, and none required PD-1 inhibitor dose
interruption or discontinuation due to toxicity
51 |
Ostios-Garcia, JTO 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Safety and efficacy of anti-PD-1 therapy for metastatic melanoma
and non-small-cell lung cancer in patients with viral hepatitis: a
case series
• Our results indicate that patients with metastatic melanoma and NSCLC can
be treated safely with PD-1 inhibitors in the context of HBV/HCV infection.
However, we recommend that those with active viral hepatitis be monitored
closely in consultation with a hepatologist and treated with antiviral therapy if
• indicated.
52 |
Kothapalli, Melanoma Res 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Mechanisms of resistance to checkpoint inhibitors53 |
Syn, Lancet Oncol 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Key elements in biomarker development for immune-
checkpoint inhibitor therapy
54 |
Nishino, Nat Rev Clin Oncol 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

KN-001: 4-year overall survival55 |
Felip, ASCO 2018
48.1% 24.8%
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Tumor burden determined by comprehensive genomic
profiling
56 |
Chalmers, Genomic Med 2017
Comparison of comprehensive
genomic assay targeting 315 genes
with whole exome sequencing of 29
tumors
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

MSI-high – KEYNOTE-158/16257 |
Colorectal tumors
None-colorectal tumors
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

IFN-γ–related mRNA profile predicts clinical response
to PD-1 blockade
58 |
62 patients with melanomaA) Head and neck cancer (N=43),
B) gastric cancer (N=33) Ayers, JCI 2017
Baseline samples from pembrolizuma treated patients:
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

IFN-γ–related mRNA profile predicts clinical response to PD-1
blockade
59 |
Fehrenbacher, Lancet Oncol 2016
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

New strategies under evaluation60 |
IMMUNE
STATUS
1. No effective antitumorimmunity
«Cold» tumor
2. Suboptimal or exhaustedantitumor immunity
Example: PD-L+ tumor
3. Antitumor immunitysuppressed by TME
Example: CD73+ tumor
GOAL: Highly activeantitumor immunity
THERAPEUTIC
AIMPrime new response Potentiate existing response
Reverse tumor
immunosuppressionEliminate tumor
CLINICAL
PIPELINE
• Adoptive T cell therapy• CAR T-Cells• Oncolytic viruses• CD40• TLR7/8• Targeted IL2v• Targeting shared antigens• Targeting neoantigens• Personalized vaccines
• PD(L)-1• CTLA-4• PD(L)-1 + OX40• PD(L)-1 + GITR• PD(L)-1 + CD137• PD(L)-1 + CSF 1-R• PD(L)-1 + Lag3• PD(L)-1 + TIM3• PD(L)-1 + TIGIT• PD(L)-1 + T-cell bispecifics• PD(L)-1 + Radiation or chemo• NKG2A
• Adenosine metabolism pathway (A2A2), CD73
• PD(L)-1 + Anti-angiogenics• PD(L)-1 + anti-CFS 1-R• CXCR2• STAT3• Myeloid derived suppressor
cell inhibition/differentiation• Tryptophan metabolism
pathway (IDO)• Treg depletion• TGFß interaction
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

2. April
2019
Dokumentname / Autor / Abteilung61
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Efficacy of relatlimab), a monoclonal antibody that targets
LAG-3, in combination with nivolumab in patients with melanoma who
progressed during prior Anti–PD-1/PD-L1
62 |
Pink: PD-L1 ≥ 1% Blue: PD-L1 < 1% Gray: PD-L1 unknown
100
80
60
40
20
0
-20
-40
-60
-100
-80
100
80
60
40
20
0
-20
-40
-60
-100
-80
100
80
60
40
20
0
-20
-40
-60
-100
-80
45% with tumor
reduction
24% with tumor
reduction
13% with tumor
reduction
Be
st
pe
rce
nt
ch
an
ge
in s
um
of
targ
et
les
ion
dia
me
ters
fro
m b
as
eli
ne
a,b
LAG-3 ≥ 1%n = 29
LAG-3 < 1%n = 17
LAG-3
Unknownn = 8
Ascierto, ESMO 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Randomized phase II study of pembrolizumab after stereotactic
body radiotherapy (SBRT) versus pembrolizumab alone in patients
with advanced non-small cell lung cancer: The PEMBRO-RT study
63 |
Theelen, ASCO 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO
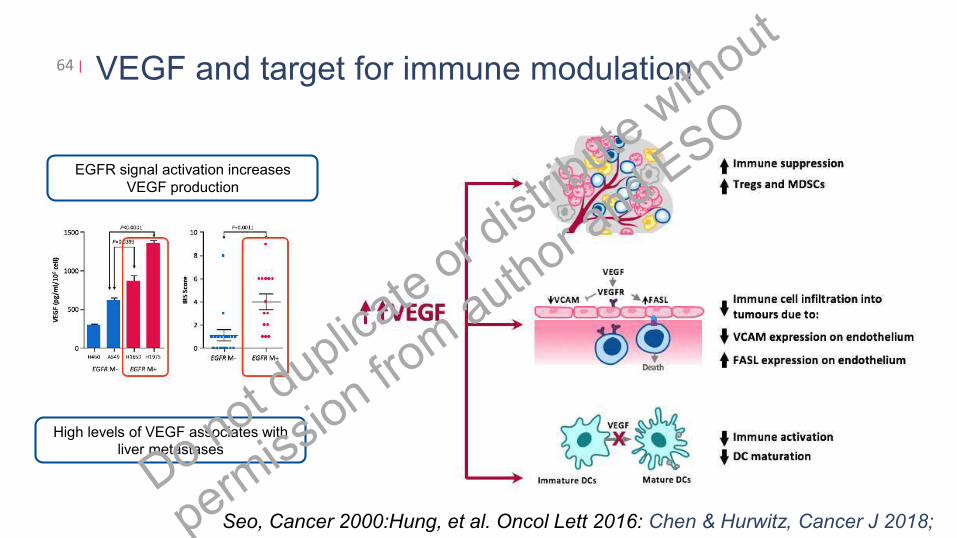
VEGF and target for immune modulation64 |
High levels of VEGF associates with
liver metastases
EGFR signal activation increases
VEGF production
Seo, Cancer 2000:Hung, et al. Oncol Lett 2016: Chen & Hurwitz, Cancer J 2018;
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Impower 150: OAS analyses of a randomized phase III study of
carboplatin and paclitaxel +/− bevacizumab, with or without atezolizumab in 1L non-squamous metastatic NSCLC:
Patients with EGFR/ALK+ tumors
65 |
Socinski, ASCO 2018
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Intrinsic Mechanisms of Resistance to Immunotherapy 66 |
Sharma, Cell 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Extrinsic Mechanisms of Resistance to Immunotherapy 67 |
Sharma, Cell 2017
Do not d
uplicate
or d
istrib
ute w
ithout
permiss
ion from
auth
or and E
SO

Impact of oncogenic
pathways on evasion of
antitumor immune
responses
68 |
Spranger and Gajewski, Nat Rev Cancer 2018
• Oncogenic WNT–β‐catenin
signalling reduces T cell
recruitment
• Gain of MYC function inhibits
T cell activation and
infiltration
• Loss of LKB1 function
decreases T cell infiltration
• Loss of PTEN reduces
efficient T cell priming
• Loss of p53 function
decreases T cell infiltration Do n
ot duplic
ate o
r dist
ribute
with
out
permiss
ion from
auth
or and E
SO