
‘Stakeholder Involvement’ - who.int · Stakeholders and partners The key stakeholders, the...
41
‘Stakeholder Involvement’ Background paper prepared for the WHO/WEF Joint Event on Preventing Noncommunicable Diseases in the Workplace (Dalian/ China, September 2007) Authors: John Griffiths Hayley Maggs Emma George Contact author: John Griffiths work2health ltd E: [email protected] T: +44 (0) 2920 388 477 M: +44 (0) 7798 502 548 F: +44 (0) 8707 626 208 W: www.work2health.org.uk
Transcript of ‘Stakeholder Involvement’ - who.int · Stakeholders and partners The key stakeholders, the...
‘Stakeholder Involvement’ Background paper prepared for the WHO/WEF Joint Event on Preventing Noncommunicable Diseases in the Workplace (Dalian/ China, September 2007) Authors: John Griffiths Hayley Maggs Emma George
Contact author: John Griffiths work2health ltd E: [email protected] T: +44 (0) 2920 388 477 M: +44 (0) 7798 502 548 F: +44 (0) 8707 626 208 W: www.work2health.org.uk
1
© World Health Organization 2008
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
The named authors alone are responsible for the views expressed in this publication.
2
Section Page
1. 1.1 1.2 1.3 1.4
Introduction Preamble Historical perspective The strengths and weaknesses of the setting The business case and other drivers for workplace health promotion
3 3 5 6 6
2. 2.1 2.2 2.3 2.4 2.5 2.6
Promoting healthy diets and physical activity in the workplace – who are the stakeholders? Rationale for stakeholder involvement Stakeholders and partners The key stakeholders, the rationale for their involvement, their role and competency A model of stakeholder engagement Stakeholders as enablers and resistors Promoting good nutrition and physical activity in the workplace – the resource implications for stakeholders
9
9 9
10
18 20 23
3. 3.1 3.2
Interaction between stakeholders Mechanisms of interaction between different stakeholders Barriers to the stakeholder interaction and possible ways to overcome these barriers
24 24 29
4. 4.1 4.2 4.3 4.4
Examples of multi stakeholder activities / programmes / experiences: Regional example Country examples NGO led example Company led examples
30 39 31 33 34
5. Conclusions and recommendations
36
6.
Limitations of the paper 38
7. References
39

3
1. Introduction Preamble Being in employment is health enhancing, with people in employment enjoying better levels of health than those who are unemployed (Waddell, 1). In addition to providing an income, work can also lead to improved self image, a sense of purpose to life, social interaction and personal development (Waddell, 1). The workplace has long been considered a suitable setting in which to promote health and well being. There are several reasons for this, not least of which is that the workplace is a setting in which a large proportion of the adult (working aged) population can be reached with messages about health and well-being. Associated with this is that many people who make up the workforce come from groups who are traditionally hard to reach with messages about health, wellbeing and lifestyle, such as males and lower socio-economic groups. A second major driver for workplace health promotion (WHP hereafter) is that it has a positive impact on the economic well-being of an organisation and, in turn, the creation of wealth in the community as a whole. Key reasons that provide a rationale for WHP activity include:
• The aging population in many countries and the need to have older people who can remain healthy and economically active
• The increasing diversity of the workforce • The requirement for high levels of workability among employees • The need to recruit and retain high quality employees
To have a workforce that is fit, flexible and efficient (workability) requires an organisation to have policies and approaches that:
• Enable and equip people to remain in work later in life • Reduce the loss of experienced workers from the workforce i.e.
improve retention • Improve the quality of life both inside and outside work for all
workers especially older workers Given the known benefits that accrue to organisations (and their employees) that implement workplace health promotion initiatives, the considerable potential of workplace health promotion can clearly be seen. However employer engagement in the promotion of employee health and well being is far from high. The key question then is how can more employers be encouraged to become involved and what systems and measures need to be in place in order for this to happen? The immediate need for action to be taken is made more pressing by demographic change and the continuing rise in lifestyle related chronic diseases such as obesity, Type II mature onset diabetes, CHD and stroke, the statistics for which are alarming. In 2006 the World
4
Health Organisation estimated that there were 1.6 billion adults (aged 15+) who were overweight and at least 400 million adults who were clinically obese, predicting that by 2015 approximately 2.3 billion adults will be overweight and more than 700 million obese (WHO, 2). Similar statistics relating to Type II diabetes and CHD are of equal concern with an estimated 120 million people world-wide affected by type 2 diabetes which is predicted to almost double to 215 million by 2010 (British Nutrition Foundation, 3) and an estimated 17 million people each year dying of cardiovascular diseases, in particular heart attacks and strokes (WHO, 4).
As this paper will describe, the workplace provides an ideal setting in which to raise awareness and promote behaviour change in terms of nutrition and physical activity, but that to achieve the considerable potential of the workplace all stakeholders must be completely committed and fully involved.
In order to aid our understanding two complementary definitions of workplace health promotion should be examined. The first, from Wynne (5) states that WHP, “is directed at the underlying causes of ill health; combines diverse methods of approach; aims at effective worker participation; and is not primarily a medical activity, but should be part of work organisation and working conditions”. The second definition was developed by the European Network for Workplace Health Promotion (ENWHP) in 1997. This states that, “WHP is the combined efforts of employers, employees and society to improve the health and well-being of people at work” (6). This is achieved through a combination of:
• Improving the work organisation and the working environment • Promoting the active participation of employees in health activities • Encouraging personal development (6)
The ENWHP statement goes on to note that WHP involves an organisational commitment to improving the health of the workforce; providing employees with appropriate information; having policies and practices which help employees to make healthy choices; and recognising that organisations have an impact on people. Using the WHO Ottawa Charter (7) as a basis, a template for WHP activity can be developed. This shows that WHP is based on:
• the building of healthy corporate policy • the creation of a supportive working environment • the development of employee skills (and knowledge) which are
conducive to health • the strengthening of workforce action towards health • the re-orienting of occupational health services
Many countries, and indeed notable WHO documents, set out clear public health targets. These range in scope from specific targets on
5
lifestyle issues such as a reduction in the levels of morbidity and mortality linked to certain behaviours e.g. tobacco and alcohol use, to more general targets focusing on the health consequences of socio-economic factors such as a reduction in inequalities in health.
It can be reasonably concluded that WHP offers considerable potential in terms of the achievements of these targets and consequently bring about improvements in levels of public health. This statement is born out by research findings focusing on the outcomes of workplace interventions. The vielife / IHPM Health and Performance Research Study (8) was the first prospective controlled study that explored the link between health and productivity in the workplace. The findings of the research highlight how health promotion programmes within the workplace can significantly improve the health status of individuals and enhance quality of life, as well as improve work performance by 8.5 % and reduce short term sickness absence. If this effect were to be multiplied across all the employers in a country then the impact on overall employee wellbeing would be considerable, with benefits to health at a population level being experienced for many years in the future.
1.2 Historical perspective One of the first, if not the first report, to identify the workplace as a setting in which people’s health could be improved was the Lalonde Report published by the Canadian Ministry of National Health and Welfare in 1974. The purpose of the Report was, ‘to unfold a new perspective on the health of Canadians and to thereby stimulate interest and discussion on future health programs for Canada’ (9). In setting out a possible health promotion strategy several courses of action were identified, including those that relate to the workplace and to the importance of stakeholder involvement in the promotion of employee health and well being e.g. ‘Enlistment of the support of employers of sedentary workers in the establishment of employee exercise programs’; and ‘Enlistment of the support of trade unions representing sedentary workers in obtaining employee exercise programs.’ Lalonde(9). The issue of stakeholder involvement was also referred to in the Ottowa Charter (7), where it is stated that, ‘health promotion demands coordinated action by all concerned: by governments, by health and other social and economic sectors, by nongovernmental and voluntary organisations, by local authorities, by industry and by the media’ and on the specific issue of work it is noted that, ‘Work and leisure should be a source of health for people. The way society organizes work should help create a healthy society (Ottowa Charter, 7). Since Ottowa a number of international and national developments have taken place and workplace health promotion has developed rapidly in many countries. Arguments supporting WHP particularly in the
6
context of the business case and return-on-investment have grown in strength as more evidence and data has become available.
1.3 The strengths and weaknesses of the setting
It is widely acknowledged that the workplace offers a setting that is conducive with the promotion of health activities. The identification of the workplace as an appropriate vehicle to effectively promote health is recognised by writers such as Fielding et al (10) who perceive that the workplace is an advantageous setting not only because of the significant proportion of time spent at work by the large majority of the population, but also because it offers an opportunity to utilise peer pressure to encourage employees to make desirable alterations to their health habits. Chu et al (11) echo such sentiment, recognising that the workplace offers the ideal infrastructure to support the promotion of health to a wide audience as its impact upon the physical, economic and social well-being of the workers will in turn impact upon their families, communities and thus wider society, therefore ensuring that the benefit is far reaching. The WHO (12) perceive that such a strategy can impact not only upon the health of people living in developed countries, but also upon those living in the developing world, through their assertion that a fundamental strategy in poverty alleviation will be to get healthy workers to raise healthy families. Further strengths that are notable for the promotion of health within a workplace setting are attained by both the organisations and individuals involved. From an organisational perspective, the promotion of health within the workplace can be advantageous as it offers an improvement in staff morale, a positive corporate image, a reduction in turnover, absenteeism, health care costs and risk of litigation and an improvement in morale and productivity (WHO, 12). Equally, the employees of an organisation that embarks upon a health promotion programme benefit too from a safe and healthy working environment, improved health, well being, self-esteem and job satisfaction, and a reduction in stress (WHO, 12). However health promotion activities in the workplace may encounter some difficulties which need to be addressed at the outset of any programme in order that adaptations can be implemented accordingly. Key feasibility and sustainability considerations in the implementation of workplace health initiatives can include seasonal, temporary, irregular, mobile, migrant and shift workers (Peltomaki et al, 13), whilst acknowledgment that labour management mistrust can impact upon the success of WHP programmes is also an important consideration (Janer et al, 14).
1.4 The Business case and other drivers for workplace health promotion Workplace health promotion (with particular reference to non communicable disease prevention addressing nutrition and physical activity) is being presented on an international platform by economic,
7
as well as societal drivers . Within the developed countries of the world, there is a substantial economic cost directly relating to a lack of physical activity and poor nutrition. The Canadian Fitness and Lifestyle Institute (15) estimate the cost of physical inactivity in Canada to amount to $5.3 billion ($1.6 billion of which are direct costs and $3.7 billion of which are indirect), whilst the cost of obesity is placed at $4.3 billion ($1.6 billion of which are direct costs and $2.7 billion of which are indirect) annually in health care expenditures. In England, the cost of inactivity is estimated to be £8.2 billion annually which accounts for both the direct costs of treating the lifestyle diseases that result, as well as the indirect costs of sickness absence (Department of Health, 16). Further, America suffers excessive costs with the price of obesity in 2000 estimated at $117 billion ($61 billion direct and $56 billion indirect), mostly associated with the diagnosis and treatment of type 2 diabetes, coronary heart disease, and hypertension (United States Department of Health & Human Services, 17) whilst an estimated 9.4% of U.S. health care expenditures are directly related to physical inactivity and obesity. (Centers for Disease Control and Prevention, 18). The economic ramifications of poor nutrition are equally eminent in the developing world. Horton (19) suggests that micronutrient deficiencies alone cost India US$2.5 billion, whilst the productivity losses (for manual workers) that surmount from stunting and deficiencies in iodine and iron, are responsible for a 2.95 percent total loss of the countries GDP. Such costs however are not reflective of the impact that non communicable diseases can have upon organisations and it is important to stress that employers may absorb a significant amount of the costs as detailed above through sickness absence, staff turnover and reduced productivity (Adeyi et al, 20). These reasons outlined above, coupled with an ageing workforce, globalisation and the need to remain competitive, have meant that many organisations have recognised the value of introducing workplace health promotion programmes, particularly which aim to directly tackle the nutrition and physical inactivity of their workforces. Within the developed world, interventions have been introduced within the workplace that are concerned with physical activity and nutrition, in recognition of the benefits that can be attained at both organisational and individual level. In Sweden, AstraZeneca (formerly Astra AB), a pharmaceutical company, has introduced a regular breakfast meeting at which nutritional food options are served, whilst also making provision to improve the health of its staff through the introduction of seminars on health related subjects, keep fit exercises at the workplace and sports programmes (European Network for Workplace Health Promotion, 21) Similarly in Greece, ElaÏs, a food production company, provides its staff with a gymnasium and professional trainers and a canteen and restaurant that provide healthy, high quality food European Network for Workplace Health Promotion, 22).

8
Within the developing countries, there is evidence of large scale interventions being introduced in workplaces that attempt to alleviate the problems associated with nutritional deficiency in the adult populations. Doak (23) highlights a large scale intervention in India that has been introduced in multiple worksites and which incorporates exercise, counselling in family nutrition and healthier menu options in the cafeteria, whist also making reference to South Korea which has programmes at worksites that offer health and nutrition counselling and education services. Further, on a smaller scale, Doak (23) draws attention to selected work site programmes in Tanzania that emphasise the importance of exercise to their staff.
9
2. Promoting healthy diets and physical activity in the workplace – who are the stakeholders? A broad range of stakeholders have a legitimate interest in diet and physical activity interventions in the workplace. In addition to those that might naturally be considered to be stakeholders in workplace health activities – employers, employees, trades unions, company insurance funds and ministries of health and labour for example, other stakeholder groups need to be involved. These include private sector organisations representing the agricultural industry, food producers and retailers, and transport and leisure interests.
2.1 Rationale for stakeholder involvement The fundamental question to be asked when considering these issues is, ‘Why should any potential stakeholder wish to become involved in the promotion of health and well being in, and through, the workplace?’ Several answers are possible, and in reality stakeholder involvement may well be based on a mixture of some or all of them. They include:
• altruism – we do it because we believe it is the right thing to do irrespective of cost
• investment – we do it because we perceive that there will be a return on our investment. This can be tangible e.g. an employer might expect that sickness absence costs will diminish, and / or intangible – the workforce will see that we are a caring employer and commitment and morale might rise as a consequence
• compulsion – we do it because we have been told we have to. The significant risk with this approach is that we will do the absolute minimum
• lost opportunity – we do it because the potential benefits are so great that we cannot afford not to, or that our competitors are doing it, thus we must do the same to maintain our market position
2.2 Stakeholders and partners
With multi-agency involvement it is sometimes difficult to distinguish between stakeholders and those agencies who may not be ‘stakeholders’ in the full sense of the word but who are working as partners in the intervention. To clarify the situation it is necessary to examine the meaning of the terms ‘stakeholder’ and ‘partner’. The term ‘stakeholder’ has numerous definitions, many of which are linked to the context in which the term is being used. Two general definitions are useful in the context of this paper – the first of these is that a stakeholder is a person or group with an interest, involvement or investment in something; (http://www.nchsd.org/uploadedfiles/Keys%20to%20Successful%20Request%20Legislation.ppt#277) ,and, in the second the word is used to describe people who will be affected by a project, or who can influence it, but who are not directly involved in doing the work. (http://www.lse.co.uk/FinanceGlossary.asp?searchTerm=&iArticleID=927&definition=stakeholder)

10
A partnership on the other hand is defined as a relationship between individuals or groups that is characterized by mutual cooperation and responsibility, as for the achievement of a specified goal: http://www.answers.com/topic/partnership?cat=biz-fin Can different stakeholders work in partnership to promote diet and physical activity? – The answer is an unequivocal ‘Yes’ and the ideal conditions for such working are explored later in Sections 2 and 3. Do all partners have to be stakeholders? – The answer is, ‘theoretically no, but in reality more often than not, yes’.
2.3 The key stakeholders, the rationale for their involvement, their role and
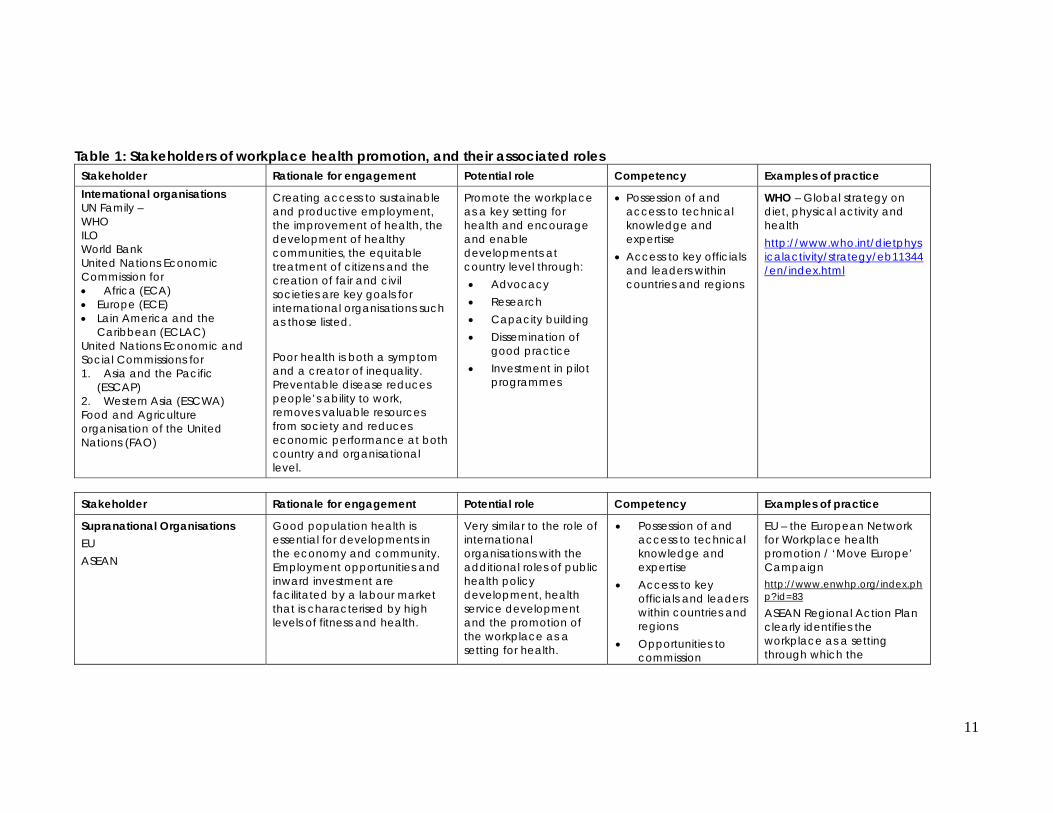
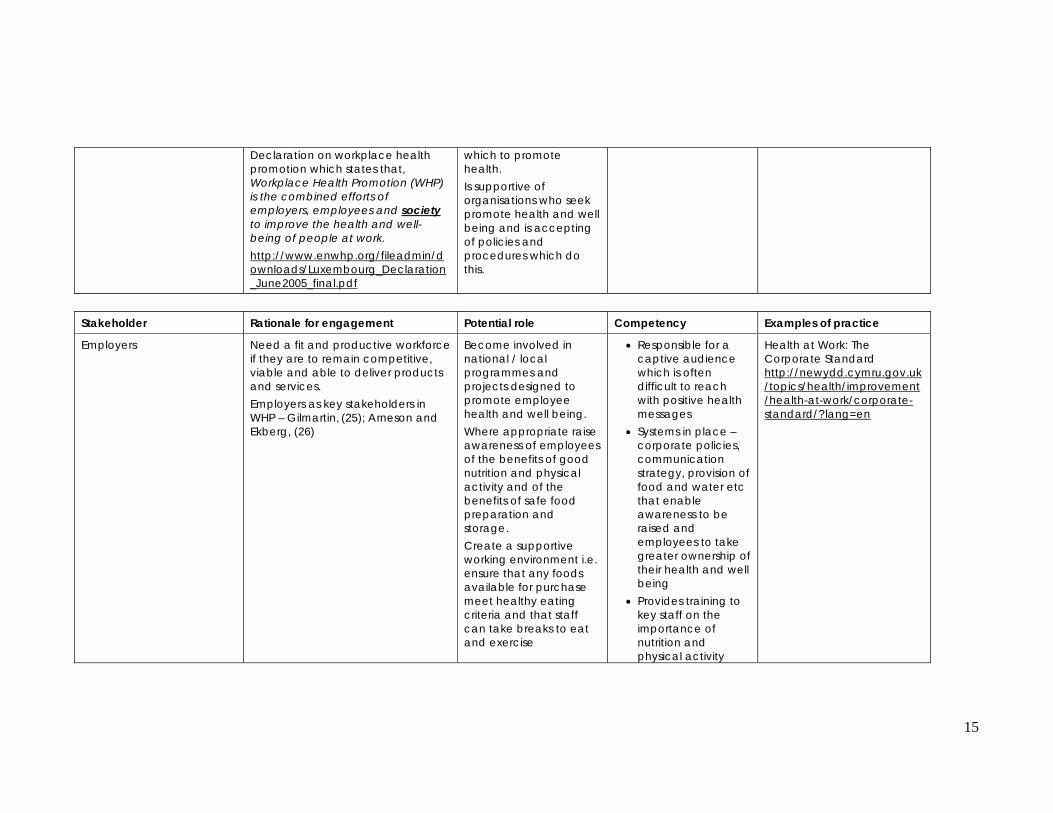
competency. Table 1 provides examples of the stakeholder groups and describes their potential role and competency in the context of workplace health promotion and diet and physical activity interventions in particular. In considering the information set out in the table we need to bear in mind that the overarching reason for the involvement of any of the stakeholders is the beneficial outcomes that their involvement brings to them or to those they represent, examples of these outcomes are set out in the table. In the case of governments this may well be improvements in public health, the creation of a healthy society etc. But this will not be a legitimate reason for other stakeholders to become involved. For these, employee productivity, organisational efficiency and increase in profit will be the driving force. The roles of individual stakeholders can vary in different circumstances, e.g., the role of the Trade Unions may initially be reluctant participant but having seen the benefits of workplace health promotion they may become proactive champions. This also means that roles can be interchangeable. The exception of this principle is the leadership role. Whilst all stakeholders can take the lead in workplace health initiatives, certain groups of stakeholders, such as employees, can never manifest true leadership as they do not possess the organisational authority necessary to act in a full leadership role. Where there is mutual respect for one another’s goals, and an understanding that the achievement of positive outcomes will mean different things for different stakeholders, then significant progress can be made in developing and implementing nutrition and physical activity programmes that will protect and improve health.
11
Table 1: Stakeholders of workplace health promotion, and their associated roles Stakeholder Rationale for engagement Potential role Competency Examples of practice International organisations UN Family – WHO ILO World Bank United Nations Economic Commission for • Africa (ECA) • Europe (ECE) • Lain America and the
Caribbean (ECLAC) United Nations Economic and Social Commissions for 1. Asia and the Pacific
(ESCAP) 2. Western Asia (ESCWA) Food and Agriculture organisation of the United Nations (FAO)
Creating access to sustainable and productive employment, the improvement of health, the development of healthy communities, the equitable treatment of citizens and the creation of fair and civil societies are key goals for international organisations such as those listed. Poor health is both a symptom and a creator of inequality. Preventable disease reduces people’s ability to work, removes valuable resources from society and reduces economic performance at both country and organisational level.
Promote the workplace as a key setting for health and encourage and enable developments at country level through: • Advocacy • Research • Capacity building • Dissemination of
good practice • Investment in pilot
programmes
• Possession of and access to technical knowledge and expertise
• Access to key officials and leaders within countries and regions
WHO – Global strategy on diet, physical activity and health http://www.who.int/dietphysicalactivity/strategy/eb11344/en/index.html
Stakeholder Rationale for engagement Potential role Competency Examples of practice
Supranational Organisations EU ASEAN
Good population health is essential for developments in the economy and community. Employment opportunities and inward investment are facilitated by a labour market that is characterised by high levels of fitness and health.
Very similar to the role of international organisations with the additional roles of public health policy development, health service development and the promotion of the workplace as a setting for health.
• Possession of and access to technical knowledge and expertise
• Access to key officials and leaders within countries and regions
• Opportunities to commission
EU – the European Network for Workplace health promotion / ‘Move Europe’ Campaign http://www.enwhp.org/index.php?id=83
ASEAN Regional Action Plan clearly identifies the workplace as a setting through which the
12
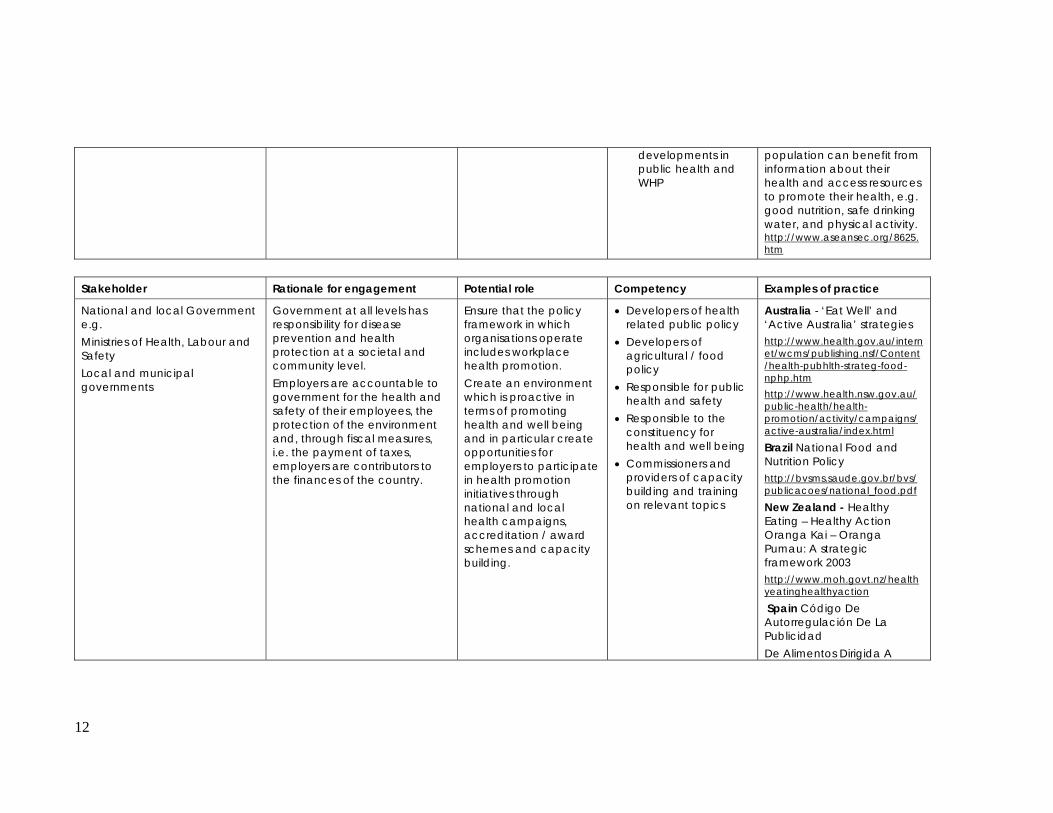
developments in public health and WHP
population can benefit from information about their health and access resources to promote their health, e.g. good nutrition, safe drinking water, and physical activity. http://www.aseansec.org/8625.htm
Stakeholder Rationale for engagement Potential role Competency Examples of practice
National and local Government e.g. Ministries of Health, Labour and Safety Local and municipal governments
Government at all levels has responsibility for disease prevention and health protection at a societal and community level. Employers are accountable to government for the health and safety of their employees, the protection of the environment and, through fiscal measures, i.e. the payment of taxes, employers are contributors to the finances of the country.
Ensure that the policy framework in which organisations operate includes workplace health promotion. Create an environment which is proactive in terms of promoting health and well being and in particular create opportunities for employers to participate in health promotion initiatives through national and local health campaigns, accreditation / award schemes and capacity building.
• Developers of health related public policy
• Developers of agricultural / food policy
• Responsible for public health and safety
• Responsible to the constituency for health and well being
• Commissioners and providers of capacity building and training on relevant topics
Australia - ‘Eat Well’ and ‘Active Australia’ strategies http://www.health.gov.au/internet/wcms/publishing.nsf/Content/health-pubhlth-strateg-food-nphp.htm http://www.health.nsw.gov.au/public-health/health-promotion/activity/campaigns/active-australia/index.html Brazil National Food and Nutrition Policy http://bvsms.saude.gov.br/bvs/publicacoes/national_food.pdf
New Zealand - Healthy Eating – Healthy Action Oranga Kai – Oranga Pumau: A strategic framework 2003 http://www.moh.govt.nz/healthyeatinghealthyaction
Spain Código De Autorregulación De La Publicidad De Alimentos Dirigida A
13
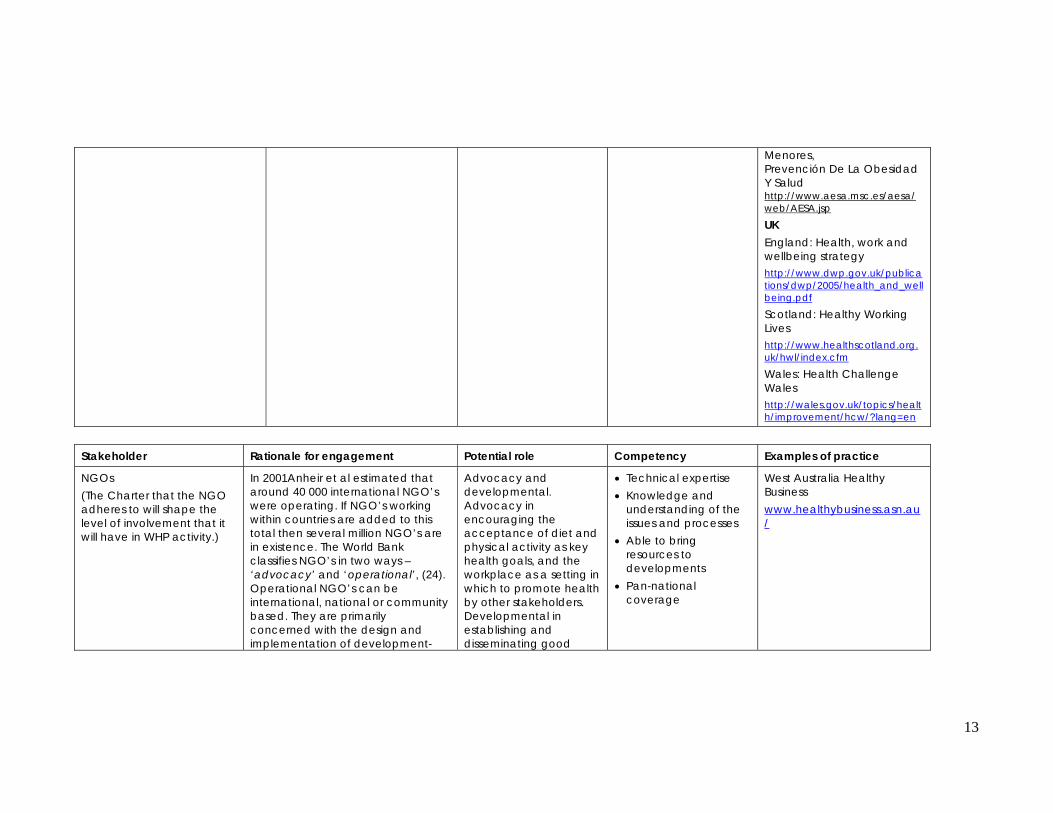
Menores, Prevención De La Obesidad Y Salud http://www.aesa.msc.es/aesa/web/AESA.jsp
UK England: Health, work and wellbeing strategy http://www.dwp.gov.uk/publications/dwp/2005/health_and_wellbeing.pdf
Scotland: Healthy Working Lives http://www.healthscotland.org.uk/hwl/index.cfm
Wales: Health Challenge Wales http://wales.gov.uk/topics/health/improvement/hcw/?lang=en
Stakeholder Rationale for engagement Potential role Competency Examples of practice
NGOs (The Charter that the NGO adheres to will shape the level of involvement that it will have in WHP activity.)
In 2001Anheir et al estimated that around 40 000 international NGO’s were operating. If NGO’s working within countries are added to this total then several million NGO’s are in existence. The World Bank classifies NGO’s in two ways –‘advocacy’ and ‘operational’, (24). Operational NGO’s can be international, national or community based. They are primarily concerned with the design and implementation of development-
Advocacy and developmental. Advocacy in encouraging the acceptance of diet and physical activity as key health goals, and the workplace as a setting in which to promote health by other stakeholders. Developmental in establishing and disseminating good
• Technical expertise • Knowledge and
understanding of the issues and processes
• Able to bring resources to developments
• Pan-national coverage
West Australia Healthy Business www.healthybusiness.asn.au/
14
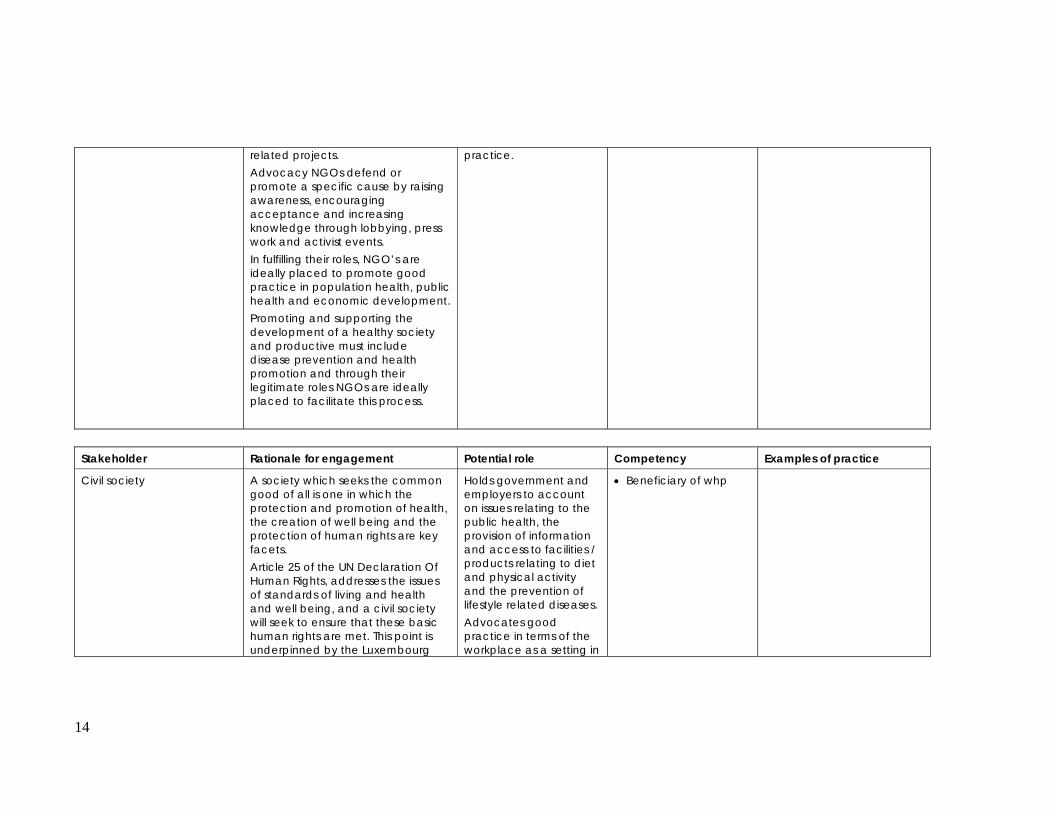
related projects. Advocacy NGOs defend or promote a specific cause by raising awareness, encouraging acceptance and increasing knowledge through lobbying, press work and activist events. In fulfilling their roles, NGO’s are ideally placed to promote good practice in population health, public health and economic development. Promoting and supporting the development of a healthy society and productive must include disease prevention and health promotion and through their legitimate roles NGOs are ideally placed to facilitate this process.
practice.
Stakeholder Rationale for engagement Potential role Competency Examples of practice
Civil society A society which seeks the common good of all is one in which the protection and promotion of health, the creation of well being and the protection of human rights are key facets. Article 25 of the UN Declaration Of Human Rights, addresses the issues of standards of living and health and well being, and a civil society will seek to ensure that these basic human rights are met. This point is underpinned by the Luxembourg
Holds government and employers to account on issues relating to the public health, the provision of information and access to facilities / products relating to diet and physical activity and the prevention of lifestyle related diseases. Advocates good practice in terms of the workplace as a setting in
• Beneficiary of whp
15
Declaration on workplace health promotion which states that, Workplace Health Promotion (WHP) is the combined efforts of employers, employees and society to improve the health and well-being of people at work. http://www.enwhp.org/fileadmin/downloads/Luxembourg_Declaration_June2005_final.pdf
which to promote health. Is supportive of organisations who seek promote health and well being and is accepting of policies and procedures which do this.
Stakeholder Rationale for engagement Potential role Competency Examples of practice
Employers Need a fit and productive workforce if they are to remain competitive, viable and able to deliver products and services. Employers as key stakeholders in WHP – Gilmartin, (25); Arneson and Ekberg, (26)
Become involved in national / local programmes and projects designed to promote employee health and well being. Where appropriate raise awareness of employees of the benefits of good nutrition and physical activity and of the benefits of safe food preparation and storage. Create a supportive working environment i.e. ensure that any foods available for purchase meet healthy eating criteria and that staff can take breaks to eat and exercise
• Responsible for a captive audience which is often difficult to reach with positive health messages
• Systems in place – corporate policies, communication strategy, provision of food and water etc that enable awareness to be raised and employees to take greater ownership of their health and well being
• Provides training to key staff on the importance of nutrition and physical activity
Health at Work: The Corporate Standard http://newydd.cymru.gov.uk/topics/health/improvement/health-at-work/corporate-standard/?lang=en
16
(such groups would include OH staff, catering staff and managers)
Stakeholder Rationale for engagement Potential role Competency Examples of practice
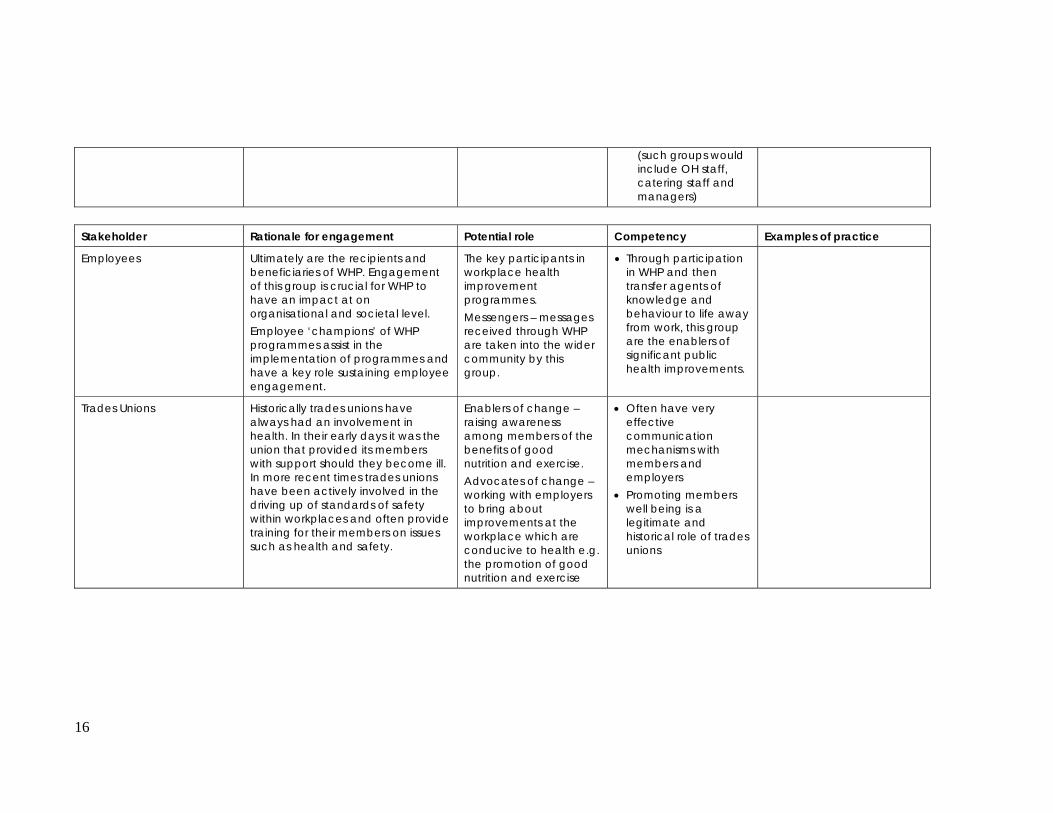
Employees Ultimately are the recipients and beneficiaries of WHP. Engagement of this group is crucial for WHP to have an impact at on organisational and societal level. Employee ‘champions’ of WHP programmes assist in the implementation of programmes and have a key role sustaining employee engagement.
The key participants in workplace health improvement programmes. Messengers – messages received through WHP are taken into the wider community by this group.
• Through participation in WHP and then transfer agents of knowledge and behaviour to life away from work, this group are the enablers of significant public health improvements.
Trades Unions Historically trades unions have always had an involvement in health. In their early days it was the union that provided its members with support should they become ill. In more recent times trades unions have been actively involved in the driving up of standards of safety within workplaces and often provide training for their members on issues such as health and safety.
Enablers of change – raising awareness among members of the benefits of good nutrition and exercise. Advocates of change – working with employers to bring about improvements at the workplace which are conducive to health e.g. the promotion of good nutrition and exercise
• Often have very effective communication mechanisms with members and employers
• Promoting members well being is a legitimate and historical role of trades unions
17
Stakeholder Rationale for engagement Potential role Competency Examples of practice
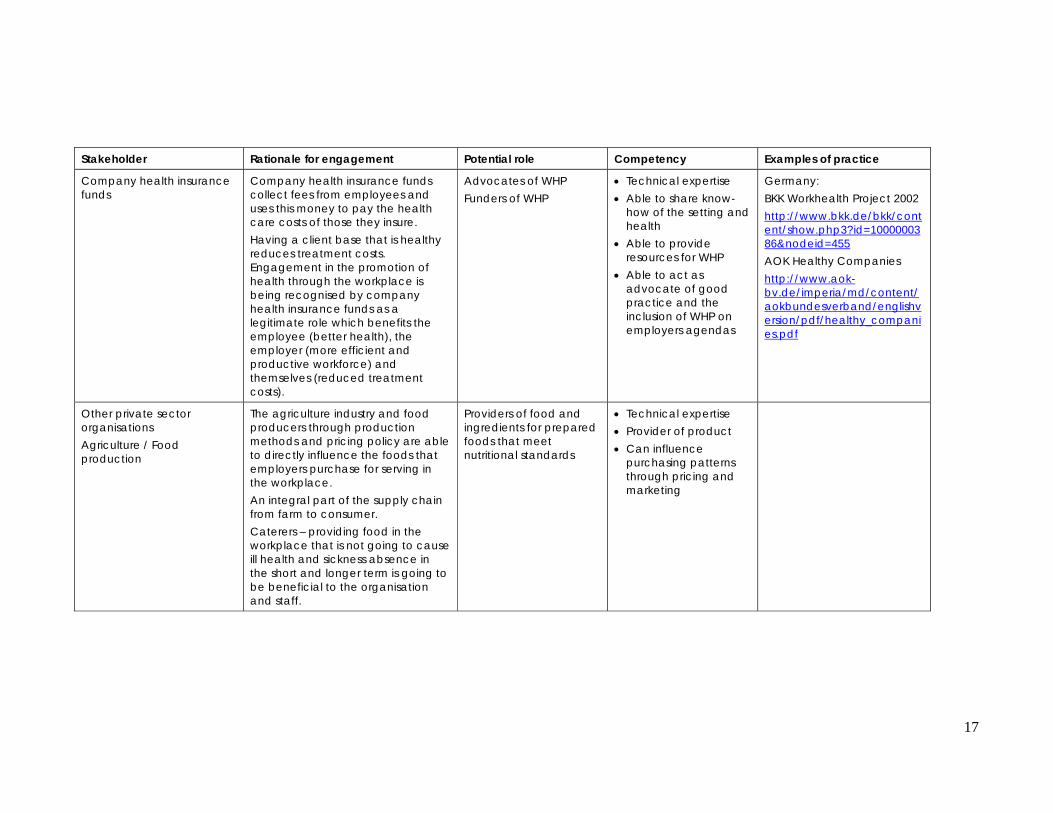
Company health insurance funds
Company health insurance funds collect fees from employees and uses this money to pay the health care costs of those they insure. Having a client base that is healthy reduces treatment costs. Engagement in the promotion of health through the workplace is being recognised by company health insurance funds as a legitimate role which benefits the employee (better health), the employer (more efficient and productive workforce) and themselves (reduced treatment costs).
Advocates of WHP Funders of WHP
• Technical expertise • Able to share know-
how of the setting and health
• Able to provide resources for WHP
• Able to act as advocate of good practice and the inclusion of WHP on employers agendas
Germany: BKK Workhealth Project 2002 http://www.bkk.de/bkk/content/show.php3?id=1000000386&nodeid=455 AOK Healthy Companies http://www.aok-bv.de/imperia/md/content/aokbundesverband/englishversion/pdf/healthy_companies.pdf
Other private sector organisations Agriculture / Food production
The agriculture industry and food producers through production methods and pricing policy are able to directly influence the foods that employers purchase for serving in the workplace. An integral part of the supply chain from farm to consumer. Caterers – providing food in the workplace that is not going to cause ill health and sickness absence in the short and longer term is going to be beneficial to the organisation and staff.
Providers of food and ingredients for prepared foods that meet nutritional standards
• Technical expertise • Provider of product • Can influence
purchasing patterns through pricing and marketing

18
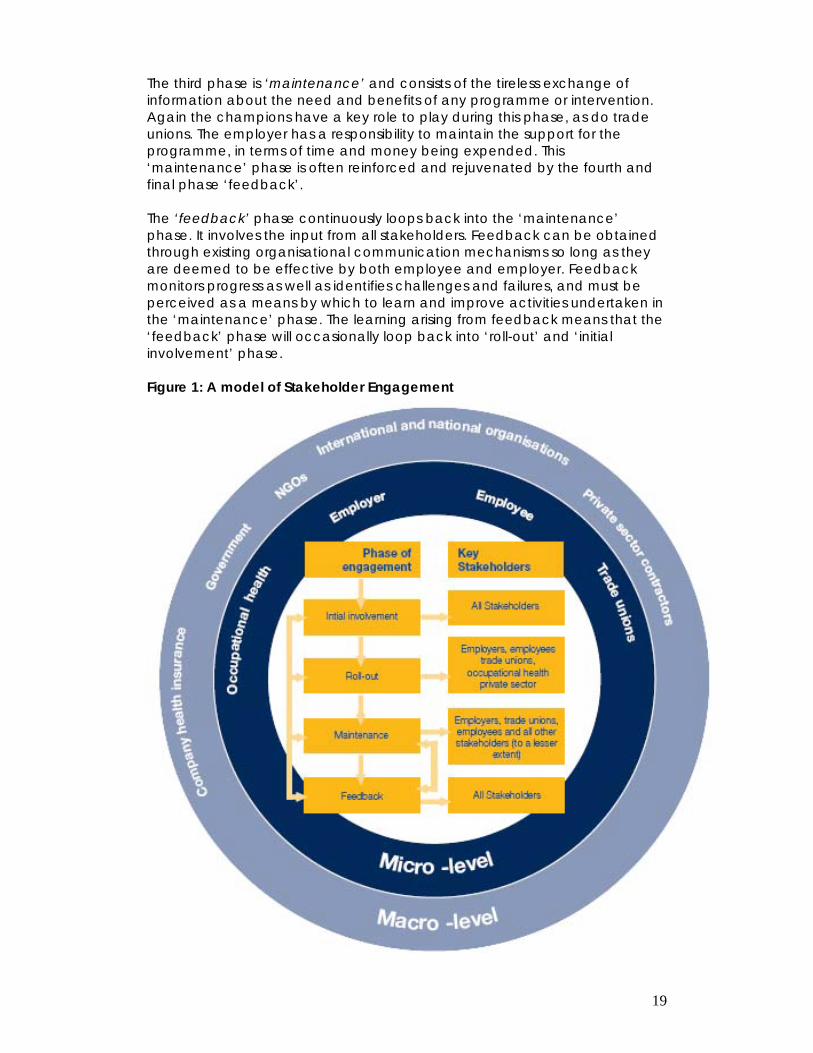
2.4 A model of stakeholder engagement The success of a programme that tackles chronic disease in the workplace relies heavily in the involvement of the stakeholders identified above. The following model has been developed to provide a framework of stakeholder engagement to be used by those responsible for implementing health promotion programmes. The model describes 4 phases during which different stakeholders are primarily involved. The model illustrates how the dynamic involvement of stakeholders can change through the phases of engagement. The 4 phases presented in the model are qualitatively different from each other, pose different challenges for successful implementation and have different key stakeholders. Drawing on Figure 1, generally, the closer the stakeholder is to the centre of the circle the greater their overall involvement to a workplace health programme. Therefore, we can see that typically employees and employers have a greater role in an intervention than do agencies such as NGOs or international organisations. In other words, stakeholders in the micro-environment often have a greater role in the realisation of an intervention than do those in the macro-environment. There are exceptions to this principle, for example, government initiatives to raise population health through a workplace programme. Clearly, in such circumstances the role of the government is absolutely key. It is important to note that all stakeholders have the ability to interact with one another in order to facilitate the implementation of an intervention. However, some stakeholders are more likely to interact than others. It is clear that an employer and a NGO are more likely to be in dialogue than an occupational health provider and the government. See Section 3 for more discussion on interaction of stakeholders. Dialogue between stakeholders should be promoted at all times to ensure the intervention is optimally implemented, overcoming any resistors (see section 2.4). The first phase of engagement is termed ‘initial involvement’. This phase may involve all stakeholders, but it is characterised by the involvement of ‘champions’ or a group of organisational representatives (both employer, employees, and occupational health) that are highly motivated to drive forward the workplace health agenda within the organisation. During this phase the goals of the ‘champions’ and the workplace health programme are set out, and a strategy for the second phase, ‘dissemination’, is decided. The ‘dissemination’ phase is led by the champions but aims to engage the entire workforce. The importance of the influence that trade unions can have on the uptake of the workforce of any interventions must not be under-estimated. In the macro-environment, the private sector, such as insurance providers, may have an input during this phase. ‘Dissemination’ involves the roll-out of interventions and programmes that address chronic disease in the workplace. This phase is strongly dependent upon large amounts of information being provided to the audience of the intervention that is both clear and easily understood and that explains the need to become engaged in such programmes.
19
The third phase is ‘maintenance’ and consists of the tireless exchange of information about the need and benefits of any programme or intervention. Again the champions have a key role to play during this phase, as do trade unions. The employer has a responsibility to maintain the support for the programme, in terms of time and money being expended. This ‘maintenance’ phase is often reinforced and rejuvenated by the fourth and final phase ‘feedback’. The ‘feedback’ phase continuously loops back into the ‘maintenance’ phase. It involves the input from all stakeholders. Feedback can be obtained through existing organisational communication mechanisms so long as they are deemed to be effective by both employee and employer. Feedback monitors progress as well as identifies challenges and failures, and must be perceived as a means by which to learn and improve activities undertaken in the ‘maintenance’ phase. The learning arising from feedback means that the ‘feedback’ phase will occasionally loop back into ‘roll-out’ and ‘initial involvement’ phase. Figure 1: A model of Stakeholder Engagement

20
2.5 Stakeholders as enablers and resistors Each of the stakeholders described so far in this paper has the potential to play a significant role in the development of good practice in the promotion of diet and physical activity where the workplace is concerned. But, are all the relevant stakeholders actively engaged in a positive way, and, if not, are they adopting a neutral position or may they even be operating in a negative way i.e. actively resisting developments within the setting? Positive stakeholder engagement is not guaranteed – vested interests, maintenance of the status quo and a failure to recognise the potential of the setting are among the many reasons why this might be so. Table 2 describes the characteristics that might be shown by a stakeholder at different positions on the spectrum of stakeholder involvement. Table 2: The enablers/resistors spectrum
The spectrum of stakeholder involvement Resistor Enabler
Severe resistors
Moderate resistors
Mild resistors / Mild enablers
Moderate enabler
Very proactive enabler
Unable or unwilling to change
Unlikely to change without compelling evidence
Easily moved from one
position to another
Is involved through
signposting to interventions
Convinced of the benefits of
involvement and assumes an
ambassadorial role
Cannot see any benefits of becoming involved
Lack of awareness of the benefits of involvement
Awareness of the benefits of
involvement and takes action
Has identified clear role in
terms of own involvement
Position may be influenced by vested interests
Facilitates access to
interventions
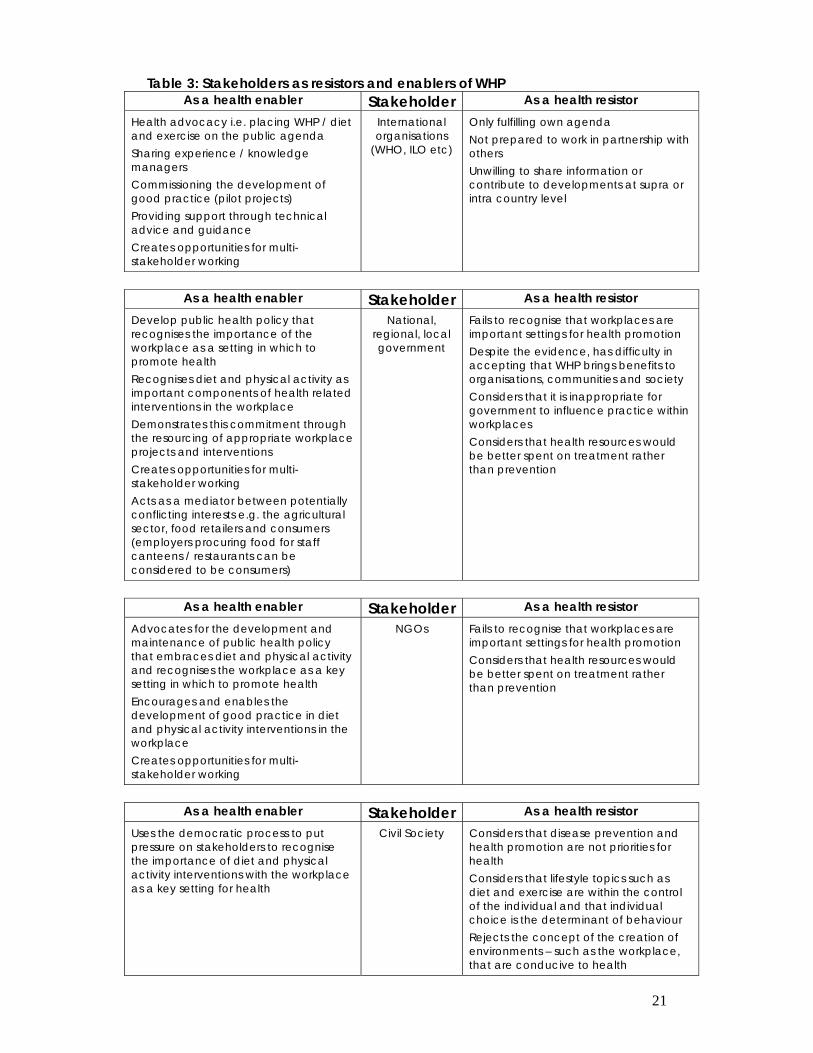
Given the strength of the business case and the health case for the involvement of workplaces in the promotion of diet and physical activity programmes, advocates and champions of change must make all stakeholders aware of the benefits that can be achieved through the positive and active engagement, and, if they do not become positively engaged, of the increase in premature death and preventable disease and the burden this places on themselves, the wider society, on efficiency and profit, and on individual workers and citizens. Table 3 briefly describes how stakeholders can act as enablers of workplace health and conversely, how they can act as resistors to workplace health. In some circumstances the strength of a resistor is sufficiently strong to result in inactivity of a stakeholder. It is the function of health advocates and those stakeholders who have adopted this proactive approach towards WHP to move remaining stakeholders from the right hand column of the table to the left.
21
Table 3: Stakeholders as resistors and enablers of WHP As a health enabler Stakeholder As a health resistor
Health advocacy i.e. placing WHP / diet and exercise on the public agenda Sharing experience / knowledge managers Commissioning the development of good practice (pilot projects) Providing support through technical advice and guidance Creates opportunities for multi- stakeholder working
International organisations
(WHO, ILO etc)
Only fulfilling own agenda Not prepared to work in partnership with others Unwilling to share information or contribute to developments at supra or intra country level
As a health enabler Stakeholder As a health resistor
Develop public health policy that recognises the importance of the workplace as a setting in which to promote health Recognises diet and physical activity as important components of health related interventions in the workplace Demonstrates this commitment through the resourcing of appropriate workplace projects and interventions Creates opportunities for multi- stakeholder working Acts as a mediator between potentially conflicting interests e.g. the agricultural sector, food retailers and consumers (employers procuring food for staff canteens / restaurants can be considered to be consumers)
National, regional, local government
Fails to recognise that workplaces are important settings for health promotion Despite the evidence, has difficulty in accepting that WHP brings benefits to organisations, communities and society Considers that it is inappropriate for government to influence practice within workplaces Considers that health resources would be better spent on treatment rather than prevention
As a health enabler Stakeholder As a health resistor
Advocates for the development and maintenance of public health policy that embraces diet and physical activity and recognises the workplace as a key setting in which to promote health Encourages and enables the development of good practice in diet and physical activity interventions in the workplace Creates opportunities for multi- stakeholder working
NGOs Fails to recognise that workplaces are important settings for health promotion Considers that health resources would be better spent on treatment rather than prevention
As a health enabler Stakeholder As a health resistor
Uses the democratic process to put pressure on stakeholders to recognise the importance of diet and physical activity interventions with the workplace as a key setting for health
Civil Society Considers that disease prevention and health promotion are not priorities for health Considers that lifestyle topics such as diet and exercise are within the control of the individual and that individual choice is the determinant of behaviour Rejects the concept of the creation of environments – such as the workplace, that are conducive to health
22
As a health enabler Stakeholder As a health resistor
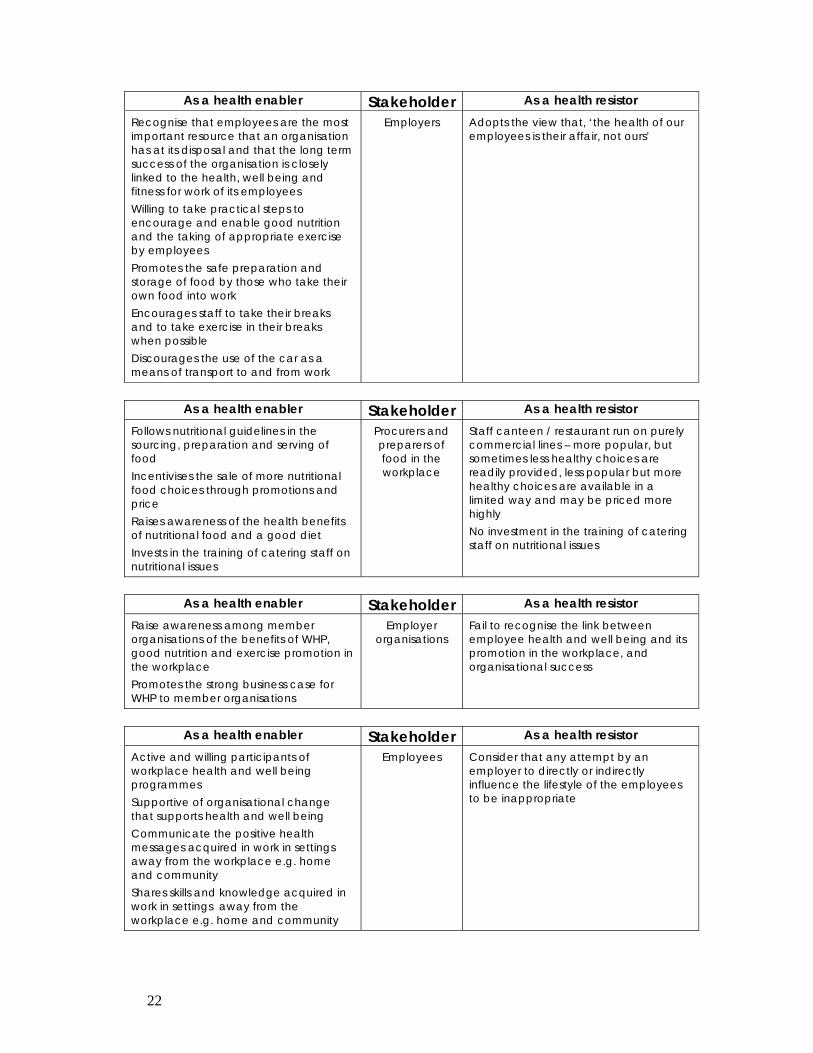
Recognise that employees are the most important resource that an organisation has at its disposal and that the long term success of the organisation is closely linked to the health, well being and fitness for work of its employees Willing to take practical steps to encourage and enable good nutrition and the taking of appropriate exercise by employees Promotes the safe preparation and storage of food by those who take their own food into work Encourages staff to take their breaks and to take exercise in their breaks when possible Discourages the use of the car as a means of transport to and from work
Employers Adopts the view that, ‘the health of our employees is their affair, not ours’
As a health enabler Stakeholder As a health resistor
Follows nutritional guidelines in the sourcing, preparation and serving of food Incentivises the sale of more nutritional food choices through promotions and price Raises awareness of the health benefits of nutritional food and a good diet Invests in the training of catering staff on nutritional issues
Procurers and preparers of food in the workplace
Staff canteen / restaurant run on purely commercial lines – more popular, but sometimes less healthy choices are readily provided, less popular but more healthy choices are available in a limited way and may be priced more highly No investment in the training of catering staff on nutritional issues
As a health enabler Stakeholder As a health resistor
Raise awareness among member organisations of the benefits of WHP, good nutrition and exercise promotion in the workplace Promotes the strong business case for WHP to member organisations
Employer organisations
Fail to recognise the link between employee health and well being and its promotion in the workplace, and organisational success
As a health enabler Stakeholder As a health resistor
Active and willing participants of workplace health and well being programmes Supportive of organisational change that supports health and well being Communicate the positive health messages acquired in work in settings away from the workplace e.g. home and community Shares skills and knowledge acquired in work in settings away from the workplace e.g. home and community
Employees Consider that any attempt by an employer to directly or indirectly influence the lifestyle of the employees to be inappropriate
23
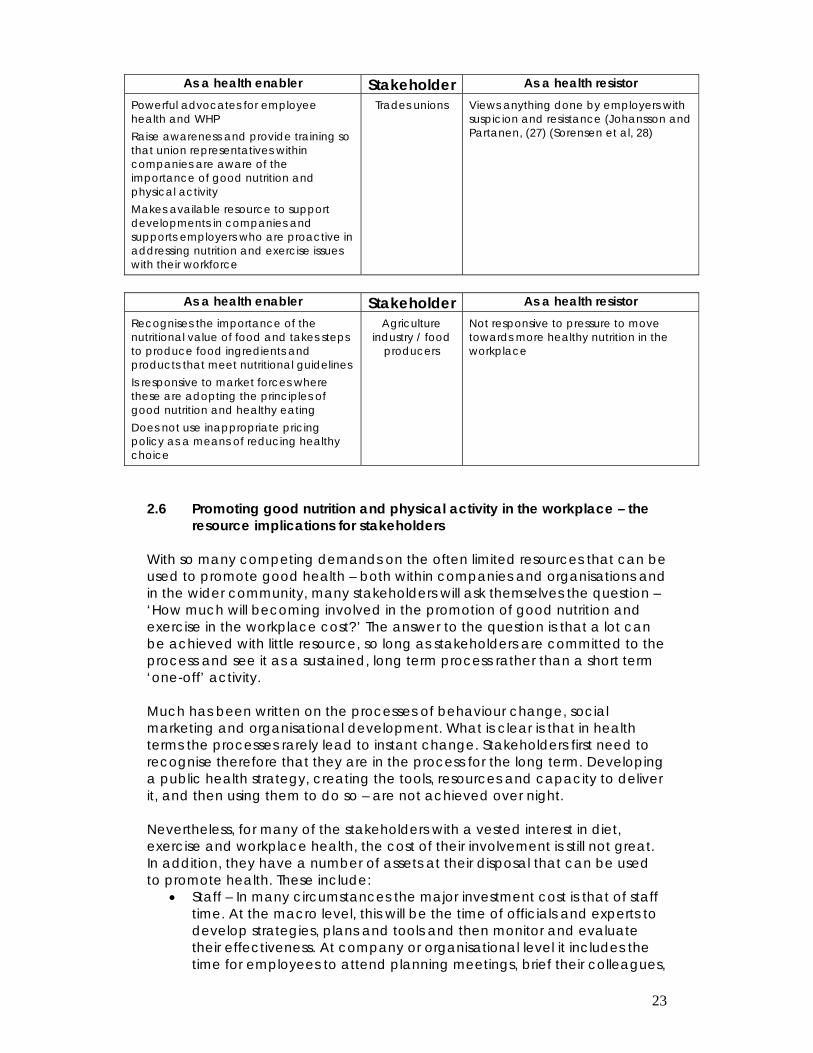
As a health enabler Stakeholder As a health resistor Powerful advocates for employee health and WHP Raise awareness and provide training so that union representatives within companies are aware of the importance of good nutrition and physical activity Makes available resource to support developments in companies and supports employers who are proactive in addressing nutrition and exercise issues with their workforce
Trades unions Views anything done by employers with suspicion and resistance (Johansson and Partanen, (27) (Sorensen et al, 28)
As a health enabler Stakeholder As a health resistor
Recognises the importance of the nutritional value of food and takes steps to produce food ingredients and products that meet nutritional guidelines Is responsive to market forces where these are adopting the principles of good nutrition and healthy eating Does not use inappropriate pricing policy as a means of reducing healthy choice
Agriculture industry / food
producers
Not responsive to pressure to move towards more healthy nutrition in the workplace
2.6 Promoting good nutrition and physical activity in the workplace – the
resource implications for stakeholders With so many competing demands on the often limited resources that can be used to promote good health – both within companies and organisations and in the wider community, many stakeholders will ask themselves the question – ‘How much will becoming involved in the promotion of good nutrition and exercise in the workplace cost?’ The answer to the question is that a lot can be achieved with little resource, so long as stakeholders are committed to the process and see it as a sustained, long term process rather than a short term ‘one-off’ activity. Much has been written on the processes of behaviour change, social marketing and organisational development. What is clear is that in health terms the processes rarely lead to instant change. Stakeholders first need to recognise therefore that they are in the process for the long term. Developing a public health strategy, creating the tools, resources and capacity to deliver it, and then using them to do so – are not achieved over night. Nevertheless, for many of the stakeholders with a vested interest in diet, exercise and workplace health, the cost of their involvement is still not great. In addition, they have a number of assets at their disposal that can be used to promote health. These include:
• Staff – In many circumstances the major investment cost is that of staff time. At the macro level, this will be the time of officials and experts to develop strategies, plans and tools and then monitor and evaluate their effectiveness. At company or organisational level it includes the time for employees to attend planning meetings, brief their colleagues,
24
attend training (training does not necessarily mean participating in expensive courses many miles from base, it can include shadowing, benchmarking and mentoring, and use e-learning, desk research and individual learning), and leading, supporting and participating in the interventions.
• Knowledge, skills and understanding - one of the great benefits of partnership working is that different stakeholders bring different assets to the project. For example in a country based nutrition programme, officials from the ministry of health and public health professionals will have a clear appreciation and understanding of the nutrition goals, while representatives of business community will know what is needed to make the programme work in companies. The sharing of these assets and the pooling of knowledge and skills can prevent expensive mistakes being made and inappropriate and unworkable programmes being developed.
• Technical resources – research, marketing, project management, resource design etc are all technical skills which can be shared as stakeholders work in partnership.
• Economic resources – In a world where the demands on health funding are strong and the level of resources is often limited economic resources need to be used with care and with justification. However, some financial commitment is required to initiative and sustain programmes. Some stakeholders will be more able to allocate these resources than others, but ‘in kind’ resourcing can prove to be as valuable as direct financial support.
The issue of stakeholders working in partnership is more fully discussed in Section 3. 3. Interaction between stakeholders
As the previous section outlined, action by individual stakeholders can bring about positive health benefits. However there is little doubt that even greater benefit (the synergistic effect) can be obtained through stakeholders working in partnership with one another for their mutual benefit. Such partnerships profit from having clear and achievable goals and realistic plans. During the lifetime of an intervention stakeholders may become more or less involved, so a flexibility principle should underpin any interaction between stakeholders. Several modes of stakeholder interaction are set out below.
3.1 Mechanisms of stakeholder interaction i. Public Private Partnership - is a system in which a government service or private business venture is funded and operated through a partnership of government and one or more private sector organisations. These schemes are sometimes referred to as PPP or P3.
In some types of PPP, the government uses revenues derived from taxation to provide capital to the project (on occasion resourcing may be of the ‘in kind’ type). Resources may be used as an initial capital investment or as maintenance funding. The actual programmes or services are run jointly with the private
25
sector or under contract. In other types of PPP, capital investment is made by the private sector on the strength of a contract with government to provide agreed services. Examples of PPP being used in a public health context are rare, most health related PPP projects being concerned with the development and operation of major capital projects such as hospitals. However the lack of PPP projects in public health does not mean that this mechanism of joint working is invalid; rather it is just few public health PPP’s have been formed yet! One example of project which might be considered to be a PPP project in which WHO (Euro) was involved) was the WHO European Partnership Project to Reduce Tobacco Dependence. Set up in 1999, for an initial three-year period, the objective of the project was to bring about a reduction in tobacco-related death and disease. The Partnership Project comprised private, non-commercial and public sector partners, including the pharmaceutical sector at the European level and in four target countries, France, Germany, Poland and the United Kingdom. In 2001, the Czech Republic joined the project. A wide range of technical reports, professional and lay resources and guidance documents were produced as a result of the work of the project.
ii. Platform lead by government The development of an enterprise culture within a society provides another means of tackling health issues. To remain competitive, societies need to demonstrate to potential investors that the population from whom the workforce is drawn is fit and able to work. Being able to work requires potential, certain levels of educational attainment and training as well as a level of health that enables the individual to meet the physical and mental requirements of the job. Ministries of Finance, together with enterprise and inward investment agencies also need to give serious consideration to population health. Government (both national and local) is ideally placed to take a lead / be an enabler of diet and physical activity programmes in the workplace. In the first instance it is a major employer in its own right, and can and should lead by example promoting good nutrition and the incorporation of appropriate exercise into its own employees’ daily routine. It also has the opportunity to influence actions at organisational and individual company level in a number of ways. These include:
a. Public health policy In setting the agenda for developments at both a national and local level, public authorities should identify the role of the workplace as a setting in which to promote health. Public health policy – especially where it addresses disease prevention, health promotion and rehabilitation – should provide a framework for health development within the context of employment and the
26
workplace. Developments at company / organisational level should therefore dovetail with national and local policy and contribute to the achievement of health goals and targets. To enable this to happen national public health strategies need be developed in a way that engages with and involves other national and local stakeholders. An example of this approach is that adopted by the Welsh Assembly Government in its Health Challenge Wales initiative, available at http://new.wales.gov.uk/subsite/healthchallenge/?lang=en . Health Challenge Wales is a call by the Government of Wales to people and organisations to work together for a healthier nation. Health Challenge Wales is the national focus of efforts to improve health and well-being. It recognises that a wide range of factors - economic, social and environmental - have an impact on health, so that action in all these areas can help create a healthier nation. Several workplace initiatives are funded by the Government but are branded Health Challenge Wales, and each of the major projects requires that companies who become involved evidence their workplace health efforts with an action plan that addresses nutrition and physical activity as well as other lifestyle related health topics.
b. Seed funding / pump priming Making available limited resources – usually in the form of grants or time limited pump priming (regular amount of project funding for a fixed period) – to facilitate the development of projects and programmes can be of great benefit. Care needs to be taken to ensure the viability of the project / programme, and in agreeing to fund specific activities it a requirement should be that all applicants set out the aim and objectives of their project together with a detailed plan on how these will be achieved and how resources will be managed. Good communication is essential between the funding body as is good governance on the part of the giver and receiver of the funds and resources.
c. Project development A third way in which government can stimulate and promote action within organisations is through the development of national and local initiatives such as campaigns and award schemes. A high profile media led campaign addressing health related behavior that has elements designed for use in workplaces and for people in employment makes it easy for employers to become involved. When the message that people see on TV, hear about on the radio or read about in their newspapers is also presented to them in the workplace then employees are more likely to recognise and act on the message and make the change to their behavior that will result in health benefits. Messages about

27
food hygiene, preparation and storage of food, the importance of good nutrition and the benefits of exercise are ideal topics for this type of campaign. Other types of national / local workplace projects include accreditation and award schemes. Here companies receive advice and guidance from external agencies such as ministries of health, employment, labour on how to meet specified health criteria. Evidence if offered by the company on how this has been achieved and if the evidence is satisfactory then an award and the recognition and positive PR that comes from possessing such an award is gained by the company. Award schemes provide a positive incentive for companies to develop workplace health programmes, reinforce the idea that such companies ‘care’ for their employees and enables the company to be recognised as an ‘employer of choice’.
d. Fiscal measures In a limited number of circumstances government support for local action can be demonstrated through fiscal practice. Examples of this type of support could include tax incentives for companies who are able to prove that they are investing in the health and well being of their employees. Proof would need to be measured against a pre determined set of criteria and would need to be independently and objectively assessed.
e. Dissemination of good practice
One of the ways of developing good practice at company level is to identify and disseminate models of good practice. This is often done in the context of business excellence, but less frequently in terms of investing in the health and well being of employees. National and local government in partnership with employer and employee organisations is in a position to promote good practice and excellence in this way.
f. Capacity building The development of sustainable interventions at company level is often dependent on just one or two people – usually enthusiasts who fulfill the role of ‘championing’ the process because of their personal commitment and enthusiasm. Yet, what happens when one of these people is promoted, moves to another site, or is given new responsibilities – the workplace health promotion programmes are quickly under threat. More people within companies need to be provided with basic knowledge and skills on health and well being issues – for some e.g. human resources, health and safety and occupational health, employee health and well being naturally forms part of their role anyway, but the full potential (for both the company and its employees) of promoting health may not have yet been provided to them.

28
The development of a reservoir of skills within organisations is a vital way of ensuring a long term sustainable approach and local and national government together with training providers has a key role to play in facilitating this process.
iii. Employer and employee led initiatives The links between work and health are clear with those in employment enjoying better levels of health than those who are unemployed. However the world of work can still jeopardise a persons health and well being. Unsafe working practices, high levels of stress and inflexible working arrangements provide examples of the negative factors which can have a detrimental effect on employee health and consequently on the health and well-being of their families.
Therefore it is very much in the interest of employers and employees to ensure that work is a healthy rather than a health damaging aspect of life. However the relationship between the two in terms of leadership is interesting. Employers can exert leadership because in most circumstances they hold a position of power and authority, although how that is used will determine whether or not the leadership is positive. In promoting diet and physical activity they therefore have the opportunity to use this power and authority in a beneficial way so far as the employees are concerned. Employees on the other hand clearly have more than a slight interest in their own health and well being, are consequently stakeholders in workplace health promotion, may even display evidence of leadership in planning and organising the approach – but do so under the (tacit) authority of the employer. In other words employees might, in some circumstances be considered to be leaders without power. Employers and employees (and those who represent them) must work to optimise this relationship, and where possible employers and society should empower employees so that they become leaders with power, champions of change.
Currently many joint activities often focus on health and safety issues, but there is equal legitimacy in exploring the potential to influence lifestyle and health. It is easier to do this where a framework for action exists, be it health and safety legislation, or a national public health strategy. However the lack of these does not prevent joint action being taken. Common goals need to be sought, trust between partners needs to be created and maintained, and actions need to be underpinned by clear stakeholder commitment – demonstrated though active and public support, and the allocation of resources (people, time, materials and money).
iv. International Organisations (e.g. the EU, WHO, ILO) Through research the development of priority actions and an understanding of the health challenges faced by countries, international organisations have the opportunity to view the strategic situation and then identify potential stakeholders at the
29
national and local level with whom they can collaborate. In some circumstances the support of an international organisation will mean that other agencies are prepared to commit resource to the intervention.
3.2 Barriers to the stakeholder interaction and possible ways to overcome these barriers
Partnership and collaborative working are often presented as a panacea with which to solve particularly complex issues and problems that exist within the fields of policy, politics, strategy and planning, in a wide range of international contexts (Armistead et al, 29). Partnerships within the context of health promotion focus specifically upon health outcomes rather than goals and thus partnerships / collaborative working within this sphere can be defined as “a voluntary agreement between two or more partners to work cooperatively towards a set of shared health outcomes” (Gillies, 30). Proponents of partnership suggest that its benefits offer mutual gains for all stakeholders involved (Kochan and Osterman, 31) however there can also be significant barriers to stakeholder collaborative working which will be discussed within an international setting. There are various prerequisites that can ensure successful partnership working, and Gillies (30) recognises good practice partnerships to place emphasis upon the sharing of power, responsibility and authority for change. However it is vital that these are addressed at the outset of any collaboration to avoid any issues that could arise, resulting in barriers to effective interaction between the stakeholders. Huxham (32) identifies the key significant barriers to such interaction to include common aims, distribution of power, issues relating to trust, membership structures and leadership.
30
4. Examples of multi stakeholder activities / programmes / experiences In seeking to identify examples of good practice the following have been chosen as they are well established, that is they have been sustained for some time, and they draw on the support and commitment of several stakeholders. In each case information has been obtained from the programme / company website or the organisation itself.
4.1 Regional example a. The European Network for Workplace Health Promotion ‘Move Europe’ Campaign
Stakeholders: The European Union Commission, The ENWHP Members (An informal network of national occupational health and safety institutes, public health, health promotion and statutory social insurance institutions), Companies
Description: The initiative is designed as a campaign which sets quality standards for Good Practice in WHP, identifies complying models and disseminates these results throughout Europe.
i. Based on an intensive review of other quality models and existing literature, the ENWHP members have developed together a high level quality standard ("quality model"), which results in the production of corresponding tools.
ii. Companies from participating countries can fill out an online questionnaire for the "Company Health Check" available in their national languages, and assess the quality of lifestyle-related health promotion programmes.
iii. A gradual status and selection model enables companies to participate and identifies good models on different levels: Companies can participate as "Move-Europe Companies" and can qualify for selection as Models of Good Practice. Exemplary Models which are considered particularly suitable for transfer in other countries will be invited to present their activities in health promotion on a European Conference to be held in Rome in the beginning of 2009.
iv. An advocacy and alliance building strategy will tie national interest and expert groups to the campaign and thus increase its impact. Using a dual-level-partnership model, with opening meetings in every country and on European level, relevant stakeholders and experts will be recruited, helping to further widen the scope for participation and to deepen the penetration in national WHP markets.
v. Marketing and PR instruments (e.g. contest, "labels", media work, concluding conference) will be employed to create added value for participating companies, members and partners, helping to raise the campaign’s awareness.
31
vi. National dissemination symposiums in every country, (organised by the NCOs with national stakeholder communities) and a European conference (organised by the secretariat) will facilitate the process of a Europe-wide exchange of knowledge and experiences, support the dissemination process.
The results of the campaign will be thoroughly documented, evaluated, elaborated and made accessible in all countries via reports and distribution, translated and adapted recommendations, fact sheets and guidelines. (Text taken from the ENWHP website: http://www.enwhp.org/index.php?id=83 )
4.2 Country Examples
The examples in this category are all award / accreditation schemes. Examples have been selected from Singapore and the United Kingdom.
a. The Singapore HEALTH (Helping People Achieve Life-Time Health Award)
Stakeholders: The Singapore Government, participating companies Description: The Singapore HEALTH Award is presented by the Health Promotion Board to give national recognition to organisations with commendable Workplace Health Promotion (WHP) programmes. It is an important way of showing appreciation to organisations that strive to help their employees lead healthy and vibrant lives. The award addresses 4 key areas, namely physical activity, nutrition, mental health, and tobacco control. It is assessed on the following criteria:
o Programme Positioning and Organisation o Programme Planning o Programme Evaluation and Results o Programme Comprehensiveness
Programme Comprehensiveness examines the programme focus and the elements incorporated in the WHP programme to enable and support a healthy workplace. The key elements in this category are ‘A Balanced Approach’, i.e. that the organisation puts equal emphasis on each of the three components: • Lifestyle and Personal Health Skills:
o Provides information and education to increase awareness and knowledge about health (e.g. disseminate information and organise workshops and courses).
o Incorporate strategies to encourage attitude and behavioural changes (e.g. motivation and incentive
• Environmental Supports: o Creates a supportive physical environment (e.g.
canteen that serves healthier food choices and provision of water coolers).
• Organisational Policies:

32
o Establishes rules and guidelines to ensure a healthy workforce and safe environment.
For further information visit: http://www.hpb.gov.sg/hpb/default.asp?pg_id=2115
b. UK – Wales, Health at Work: The Corporate Standard Stakeholders: The Welsh Assembly Government, participating organisations (the programme is endorsed by a wide variety of organisations including the Wales Trades Union Congress, The Health and Safety Executive, The EEF Wales (Manufacturing Employers organisation), The British Heart Foundation Wales and the Food Standards Agency) Description: The Corporate Health Standard, run by the Welsh Assembly Government, is the quality mark for workplace health promotion in Wales. It is presented in Bronze, Silver, Gold and Platinum categories to public and private sector-organisations implementing practices to promote the health and well-being of their employees. Like other workplace quality initiatives, it is a progressive programme and organisations are reassessed every three years. The work to achieve the Standard is consistent with the Business Excellence Model, which drives quality and organisational development in many organisations. Sections on nutrition and physical activity are included in the assessment process and to gain an award an organisation will have to show that criteria appropriate to the level of award the organisation is seeking are being met, e.g. for an organisation with a catering provision the following criteria must be met.
Bronze 1. Provision of a healthy balanced menu using the balance of Good Health Model
2. Participation in national events e.g. 5 a day
3. Clearly identified healthy food choices
4. Provision of information about healthy eating
5. Suitable facilities for breast feeding mothers
6. 4 of the Health Choice criteria are incorporated into menus
Silver 1. Active marketing of healthy choices
2. Healthy vending
3. Training for catering staff
4. Healthy choices at corporate functions and social events
5. Minimum of 1 event held per year to highlight/raise awareness of healthy choices
6. Extend policy to contract/catering providers used by organisation
33
7. A minimum of 8 Healthy Choice criteria are incorporated into menus
Gold 1. Links with lifestyle screening and support being available for staff wanting to lose weight
2. A minimum of 12 healthy choice criteria are incorporated into menus
(Text taken from: http://newydd.cymru.gov.uk/topics/health/improvement/health-at-work/corporate-standard/?lang=en )
4.3 NGO led examples Western Australia Healthy Business Stakeholders: The Cancer Council Western Australia, National Heart Foundation of Australia (WA Division), Diabetes WA and Healthway (Note: Healthway was established in 1991 under the Tobacco Control Act as a statutory body. One of its roles being to, ‘fund activities that promote health, particularly that of young people, and provide research grants to organisations engaged in health promotion programs and research’). Description: The WA Healthy Business originated from a pilot project developed by a partnership between the charities mentioned above and funded by Healthway. From July 2003 until August 2005, seven WA workplaces participated in the study. This study enabled these organisations to identify the main health areas of concern for employees and observe their working environment for physical activity, nutrition, smoking and sun protection. The seven organisations developed, ran and evaluated their own workplace health promotion programs with support from the pilot project. WA Healthy Business is primarily aimed at blue collar workplaces to improve the long term health outcomes of their employee's, however it is also available to a range of workplaces The aim of the project is to support Western Australian workplaces and their staff in the delivery of workplace health promotion (WHP) through a range of strategies. This includes:
• Capacity building workshops for organisation employees
• Information and resources through the WA Healthy Business website
• Education sessions on health issues • Health information kits • E-newsletters • Healthy Business Coordinator • Workplace case studies
34
The project is focused on the leading causes of death and disability in Australia and the factors associated with them, two of the leading ones being diet and physical activity. For further information visit: http://www.healthybusiness.asn.au/
4.4 Company led examples
a. Caixa Geral de Depositos Stakeholder: Company and employees Description: Caixa Geral de Depositos is an international banking and finance organisation based in Lisbon, Portugal employing just under 20 000 people. Given the links that exist between diet, exercise and wellbeing, the occupational health team at Caixa Geral de Depositos has placed nutrition and exercise at the centre of the well being activities. The corporate approach to healthy nutrition has involved an analysis of long term absenteeism and the development of a multifactoral intervention consisting of three elements – consultations on nutrition issues with at risk groups, the provision of information and the greater involvement of occupational health services and an enhancement of the quality of food on offer.
The first aspect of the intervention involved the provision of 1:1 consultations on the theme of healthy nutrition, with the goal of ‘promoting health through an adequate food regimen and reducing the prevalence of nutrition related diseases’. In 2005 440 consultations were carried out and results indicate that, both men and women who participated in the programme were able to reduce their weight – with men showing greater levels of weight loss.
In terms of the workforce as a whole, the internet is used disseminate information on the calorific content of the staff restaurant menu, and a number of key recommendations have been implemented. These include making the ambience of the restaurant more pleasant – provision of music, flowers and attractive décor, presenting the healthier options in a more attractive way, implementing theme weeks, providing free yoghurt or fruit and incentivising the purchase of healthy food choices by pricing them more competitively. In addition a process of continuously raising awareness of the benefits of a healthy diet has been put in place. (For further information visit http://www.enterprise-for-health.org/fileadmin/texte/EfH_Healthy_Lifestyle.pdf)
b. Torun Energa (Poland) Stakeholder: Company and employees Description: Torun Energa is an electricity supply company based in the town of Torun in Poland and employs approximately 1450 staff. Promoting the health and well being of employees has long been a priority corporate goal, and wherever possible links have been made to family and community life as well.

35
Diet and physical activity have been identified as action areas for the WHP programme. Awareness raising materials were produced for employees using information received from the Scientific Council of the Institute of Mediterranean Diet and Functional Nutrition appointed by the Polish Association of Research on Sclerosis, the Council of Healthy Diet Promotion and the Institute of Food and Nutrition in Warsaw. Wherever possible employees are encouraged to modify their diets and take appropriate exercise. To facilitate the taking of exercise, the company purchases subscription for employees to a wellness centre where the instructors offer advice on exercise and diet and use of the centre is increasing.
36
5. Conclusions and recommendations 1. Stakeholder commitment
This paper has demonstrated that the major stakeholders have a key role to play in the continuing development of workplace initiatives to tackle lifestyle related disease. If the potential of the workplace is to be realised as a setting in which diet and exercise issues can be addressed then first and foremost stakeholders need to recognise that their commitment should be public and sustained. Public, because this demonstrates a conviction that action is needed, and sustained, because changing attitudes, beliefs and behaviours be it at the individual or the organisational level, takes time.
2. Stakeholder collaboration
It is usual for several stakeholders to be involved in WHP programmes. Different stakeholders bring different perspectives, skills, understanding, and resources to the relationship and this must be recognised as a strength. In working together, stakeholders should utilise these differences in the building of strong and effective interventions. However it may be necessary for historically held positions to be moderated, for example at the local level, trade unions working in partnership with company managers to create a healthy working environment in which opportunities to exercise and consume a healthy diet are readily available to all staff; and at the national level, government working with private sector organisations to bring about improvements in population health. The basic principles of collaborative working need to be in place – sharing of power, responsibility and authority for change. The successful adoption of these principles requires trust between stakeholders, good communication and an absence of blame when progress becomes difficult.
3. Stakeholder engagement
The improvement of population health, making private and public sector organisations more effective and successful are goals that many stakeholders possess independently of one another. Their ability to influence these goals in isolation is not as great as their ability to influence them when working collaboratively with others. Given the commonality of goals and the beneficial health, business and community outcomes, potential stakeholders need to identify ways in which they can collaborate, and means by which they can do so. The engagement of stakeholders is facilitated when they are ‘buying in’ i.e. committing to, a clear plan of action which has
37
objectives which they can relate to and agree with. Leaders at all levels of workplace health promotion development need to consider how to gain this buy in by stakeholders as plans and proposals are created and consulted on. Having clear strategies whether they relate to health, enterprise development or regeneration etc provide a good starting point. When these are backed up by sound action plans, clear and deliverable goals and when the all the benefits of the intervention are clearly stated for each of the stakeholders, then engagement of the full range of potential stakeholders is more likely.
4. Involving other stakeholders Tackling the issues of diet and physical activity comprehensively can often require the involvement of range of stakeholders and other organisations. In the context of nutrition and diet for example all organisations in the supply chain from farm to consumer should be involved if at all possible. This means that food is produced to the highest possible nutritional standards, is transported in the least environmentally harmful way and is prepared in ways that meet standards of hygiene and nutritional content.
5. Evidence based interventions
A great deal of evidence is now available on the effectiveness and benefits of workplace health promotion. In order to maximise the impact of their involvement stakeholders should ensure that programmes are planned and developed using the evidence base as a foundation.
6. Resources
WHP in general and lifestyle interventions in particular do not normally require huge capital outlay. Companies do not need to install multi-suite gymnasia, swimming pools and tennis courts etc for their staff in order to promote exercise. The key message is not that all staff should become elite athletes, rather that all staff should incorporate the appropriate amount of exercise into their daily routines so that their risk of developing CVD, Type 2 diabetes etc are reduced. All stakeholders have something to contribute to WHP and as has been stated previously this does not need to be in the form of direct financial aid. The contribution of all stakeholders (financial and in kind, knowledge, skills and experience) should therefore be valued and appreciated.
38
6. Limitations of this paper 1. Whilst this paper has identified stakeholders in WHP programmes and detailed their respective roles, it is beyond the scope of this paper to establish definite and sophisticated criteria for action to implement WHP programmes. Stakeholders obviously have a hugely significant role in putting a programme into action, and Table 1 demonstrates the potential roles, and thus actions, that each stakeholder can become involved with. Future research should seek to establish practical criteria for stakeholders to move WHP programmes forward. 2. The theoretical model of stakeholder engagement presented in
Section 2 is as yet untested. Further work in this area should look to evaluate the accuracy and validity of the model through observed application of the model.
3. In developing the paper we sought to include examples of practice
from both the Developed and the Developing World. Finding examples from the Developing World was very difficult and their absence is an indicator of the disparity which exists. Care needs to be taken in simply transferring the experience of stakeholders in the Developed World and assuming that it can be directly applied in the Developing World. Transfer of experience and knowledge needs to be undertaken sensitively with due regard to political, social and cultural contexts.
39
References 1. Waddell, G. & Burton, K. Is Work Good for you Health and Wellbeing? London: TSO, 2006 2. World Health Organisation, Obesity and overweight, Fact sheet no. 311, available [online] http://www.who.int/mediacentre/factsheets/fs311/en/index.html 3. British Nutrition Foundation, Diabetes, available [online] http://www.nutrition.org.uk/home.asp?siteId=43§ionId=405&subSectionId=321&parentSection 4. World Health Organisation, The Atlas of Heart Disease and Stroke, available [online] http://www.who.int/cardiovascular_diseases/resources/atlas/en/ 5. Wynne R., Workplace Action for health: a selective review and a framework for analysis. Working paper No. EF/WP/89/30/EN. European Foundation for the Improvement of Living and Working Conditions,1989 6. The European Network for Workplace Health Promotion, The Luxembourg Declaration, available [online] http://www.enwhp.org/fileadmin/downloads/Luxembourg_Declaration_June2005_final.pdf 7. The World Health Organization, The Ottawa Charter for Health Promotion available [online] http://www.who.int/hpr/NPH/docs/ottawa_charter_hp.pdf 8. The vielife/IHPM Health and Performance Research Study (2005), Sponsored by Standard Life Healthcare, Philips and Unilever. Available [online] http://www.vielife.com/our_research/vielife_Research_Report.pdf 9. Lalonde M., A new perspective on the health of Canadians – a working document, Ministry of National health and Welfare, Ministry of Supply and Services, 1981 10. Fielding, J.E. & Piserchia, P.V., Frequency of worksite health promotion activities, American Journal of Public Health, 1983, 79:16–20 11. Chu, C., Breucker, G., Harris, N., Stitzel, A., Gan X., Gu, X. & Dwyer, S., Health-promoting workplaces - international settings development, Health Promotion International, 2000, 15:155-167
12. World Health Organisation, Workplace Health Promotion - Benefits, available [online] http://www.who.int/occupational_health/topics/workplace/en/index1.html
13. Peltomäki, P., Johansson, M., Ahrens, W., Sala, M., Wesseling, C., Brenes, F., Font, C., Husman, K., Janer, G., Kallas-Tarpila, T., Kogevinas, M., Loponen, M., Dolors Solé, M., Tempel, J., Vasama-Neuvonen, K. & Partanen, T., Social context for workplace health promotion: feasibility considerations in Costa Rica, Finland, Germany, Spain and Sweden, Health Promotion International 2003, 18:115-126
14. Janer, G., Sala, M., & Kogevinas, M., Health promotion trials at worksites and risk factors for cancer, Scandinavian Journal of Work and Environmental Health, 2002, 28:141-157
15. Canadian Fitness and Lifestyle Institute, Cost of Physical Inactivity, available [online] http://www.cflri.ca/eng/provincial_data/information/cost_inactivity.php 16. Department of Health, 2004, Promoting Physical Activity in the Workplace, Available [online] http://64.233.169.104/search?q=cache:zpfh1URy9tgJ:guidance.nice.org.uk/download.aspx%3Fo%3D424936+workplace+physical+activity+interventions+outcomes&hl=en&ct=clnk&cd=2&gl=uk 17. United States Department of Health & Human Services, The Surgeon General’s Call to Action, Available [online] http://www.sdchip.org/pdfs/G-nutrition%20edited.pdf
40
18. Centers for Disease Control and Prevention, Press Release: Twin Epidemics of Diabetes and Obesity Continue to Threaten the Health of Americans CDC Says,, available [online] http://www.sdchip.org/pdfs/G-nutrition%20edited.pdf
19. Horton, S., The Economics of Nutritional Interventions, Nutrition and Health in Developing Countries, ed. Semba, R.D. and Bloem, M. W., Totowa, NJ: Humana Press, Inc., 1999 20. Adeyi, O., Smith, O., Robles, R., Public Policy and the Challenge of Chronic Noncommunicable Diseases. Available [online] http://siteresources.worldbank.org/INTPH/Resources/PublicPolicyandNCDsWorldBank2007FullReport.pdf 21. European Network for Workplace Health Promotion, Astra, available [online] http://www.enwhp.org/fileadmin/downloads/models/Project%20Success%20Factors/Sweden/Astra%20AB.pdf 22. European Network for Workplace Health Promotion, ElaÏs S.A, Greece, available [online] http://www.enwhp.org/fileadmin/downloads/models/Project%20Success%20Factors/Greece/Elais%20S.A..pdf 23. Doak, C., Large-scale interventions and programmes addressing nutrition related chronic diseases and obesity: examples from 14 countries, Public Health Nutrition, 2002 5:275–277 Available [online] http://journals.cambridge.org/download.php?file=%2FPHN%2FPHN5_1a%2FS1368980002000381a.pdf&code=bc9ad6f128be6697d69390f92ddf4fcd 24. Duke University Libraries, NGO Research Guide, available [online] http://library.duke.edu/research/subject/guides/ngo_guide/ngo_wb.html 25. Gilmartin S., Wellness programs hit the attraction and retention mark, Workspan, 2002, 45:46–48. 26. Arneson, H., & Ekberg, K., Evaluation of empowerment processes in a workplace health promotion intervention based on learning in Sweden, Health Promotion International, 2005 20:351–359. 27. Johansson, M. & Partanen, T., Role of trade unions in workplace health promotion, International Journal of Health Services, 2002, 32:179-193 28. Sorensen et al., 1997, “Labour positions on worksite tobacco control policies: A review of arbitration cases, Journal of Public Health Policy, 18, 433-452. 29. Armistead, C. & Pettigrew, P., Effective partnerships: building a sub-regional network of reflective practitioners, International Journal of Public Sector Management, 2004, 17: 571-585 30. Gillies, P., Effectiveness of alliances and partnerships for health promotion, Health Promotion International, 1998, 13:99-120 31. Kochan, T.A., Osterman, P., 1994, The Mutual Gains Enterprise: Forging a Winning Partnership among Labor, Management and Government, Harvard Business School Press, Cambridge, MA., 2002 32. Huxham, C., Theorizing Collaboration Practice, Public Management Review, 2003, 5:401-423


















