ACRIN 6673: RF Ablation in HCC Patients - PowerPoint Presentation
Upload
gray-shieldsCategory
view
40download
0description

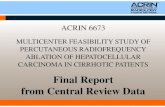
Staging Strategy and Treatment for Patients With HCC
Liver transplant RFA/PEI
Curative treatments
TACE
Single
Increased Associateddiseases
Normal No Yes
Terminalstage
PST 0-2, Child-Pugh A-B
Multinodular, PST 0
Sorafenib
Portal pressure/bilirubin
3 nodules ≤ 3 cm
N1, M1, PST 1-2≤ 3 cm, PST 0
Intermediate stage
PST > 2,Child-Pugh C
Very early stageSingle < 2 cm
Early stageSingle or 3 nodules
Advanced stagePortal invasion,
PST 0, Child-Pugh A
Resection
Symptomatic
HCC
Palliative treatments
Forner A, Reig ME, de Lope CR, Bruix J. Current strategy for staging and treatment: the BCLC update and future prospects.Semin Liver Dis. 2010;30(1):61-74

Liver transplantation RFA/PEI
Curative treatments (30%); 5-yr survival: 40%-70%
TACE
Single
Increased Associateddiseases
Normal No Yes
Sorafenib
Portal pressure/bilirubin
3 nodules ≤ 3 cm
Resection Symptomatic (20%); survival <
3 mosRCTs (50%); 3-yr survival: 10%-40%
Terminalstage (D)
Okuda 1-2, PS 0-2, Child-Pugh A-B
Multinodular, PS 0 N1, M1, PS 1-2< 3 cm, PS 0
Intermediate stage (B)
Okuda 3, PS > 2,Child-Pugh C
Very early stage (0)Single < 2 cmCarcinoma in situ
Early stage (A)Single or 3 nodules
Advanced stage (C)Portal invasion,
PS 0, Child-Pugh AHCC
BCLC Staging and Treatment Strategy
Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10):698-711, by permission of Oxford University Press.

BCLC Staging System
Terminalstage (D)
Okuda 1-2, PS 0-2, Child-Pugh A-B
Multinodular, PS 0 N1, M1, PS 1-2< 3 cm, PS 0
Intermediate stage (B)
Okuda 3, PS > 2,Child-Pugh C
Very early stage (0)Single < 2 cmCarcinoma in situ
Early stage (A)Single or 3 nodules
Advanced stage (C)Portal invasion,
PS 0, Child-Pugh A
HCC
Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10):698-711, by permission of Oxford University Press.
Stage 0 Stage A-C Stage D

Liver Transplantation for HCC:Milan Criteria (Stage 1 and 2)
• 5-yr survival with transplantation: ~ 70%• 5-yr recurrent rates: < 15%
+Absence of macroscopic vascular invasion,
absence of extrahepatic spread
Single tumor, not > 5 cm Up to 3 tumors, none > 3 cm
Mazzaferro V, et al. N Engl J Med. 1996;334:693-699.Llovet JM. J Gastroenterol Hepatol. 2002;17(suppl 3):S428-S433.

Candidates for RFA/PEI
• Includes individuals who are not candidates for surgery
• Radiofrequency ablation generally preferred over percutaneous ethanol injection– Necrotic effect more predictable across tumor
sizes– Meta-analyses suggest survival benefit with
radiofrequency ablation vs percutaneous ethanol injection
Bruix J, et al. AASLD HCC guidelines. July 2010.

Liver transplantation RFA/PEI
Curative treatments (30%); 5-yr survival: 40%-70%
TACE
Single
Increased Associateddiseases
Normal No Yes
Sorafenib
Portal pressure/bilirubin
3 nodules ≤ 3 cm
Resection Symptomatic (20%); survival <
3 mosRCTs (50%); 3-yr survival: 10%-40%
Terminalstage (D)
Okuda 1-2, PS 0-2, Child-Pugh A-B
Multinodular, PS 0 N1, M1, PS 1-2< 3 cm, PS 0
Intermediate stage (B)
Okuda 3, PS > 2,Child-Pugh C
Very early stage (0)Single < 2 cmCarcinoma in situ
Early stage (A)Single or 3 nodules
Advanced stage (C)Portal invasion,
PS 0, Child-Pugh AHCC
Unresectable HCC
BCLC Staging and Treatment Strategy
Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10):698-711, by permission of Oxford University Press.

Llovet JM, et al. Hepatology. 2003;37:429-442.
Arterial Embolization for HCCMeta-analysis of 6 RCTs (2-Yr Survival)
Random Effects Model,OR (95% CI)
Author, Journal Yr Patients, n
Lin, Gastroenterology 1988 63
GETCH, NEJM 1995 96
Bruix, Hepatology 1998 80
Pelletier, J Hepatol 1998 73
Lo, Hepatology 2002 79
Llovet, Lancet 2002 112
Overall 503
Median survival: ~ 20 mos
0.01 0.1 0.5 1 2 10 100
Z = -2.3P = .017
Favors Treatment Favors Control

Contraindications to TACE
• Extrahepatic tumor spread• Lack of portal blood flow
– Portal vein thrombosis, portosystemic anastomoses or hepatofugal flow
• Advanced liver disease (Child-Pugh Class B or C)
• Clinical symptoms of end-stage cancer
Bruix J, et al. AASLD HCC guidelines. July 2010.

Liver transplantation RFA/PEI
Curative treatments (30%); 5-yr survival: 40%-70%
TACE
Single
Increased Associateddiseases
Normal No Yes
Sorafenib
Portal pressure/bilirubin
3 nodules ≤ 3 cm
Resection Symptomatic (20%); survival <
3 mosRCTs (50%); 3-yr survival: 10%-40%
Terminalstage (D)
Okuda 1-2, PS 0-2, Child-Pugh A-B
Multinodular, PS 0 N1, M1, PS 1-2< 3 cm, PS 0
Intermediate stage (B)
Okuda 3, PS > 2,Child-Pugh C
Very early stage (0)Single < 2 cmCarcinoma in situ
Early stage (A)Single or 3 nodules
Advanced stage (C)Portal invasion,
PS 0, Child-Pugh AHCC
BCLC Staging and Treatment Strategy
Llovet JM, et al. Design and endpoints of clinical trials in hepatocellular carcinoma. Journal of the National Cancer Institute. 2008;100(10):698-711, by permission of Oxford University Press.


















