Staging and Therapeutic Regimen Wilm’s Tumor Neuroblastoma Hydronephrosis Sacrococcygeal teratoma.
42
Staging and Therapeutic Regimen • Wilm’s Tumor • Neuroblastoma • Hydronephrosis • Sacrococcygeal teratoma
-
Upload
jonatan-menear -
Category
Documents
-
view
217 -
download
0
Transcript of Staging and Therapeutic Regimen Wilm’s Tumor Neuroblastoma Hydronephrosis Sacrococcygeal teratoma.
Staging and Therapeutic Regimen
• Wilm’s Tumor• Neuroblastoma• Hydronephrosis• Sacrococcygeal teratoma

Wilm’s Tumor: Staging
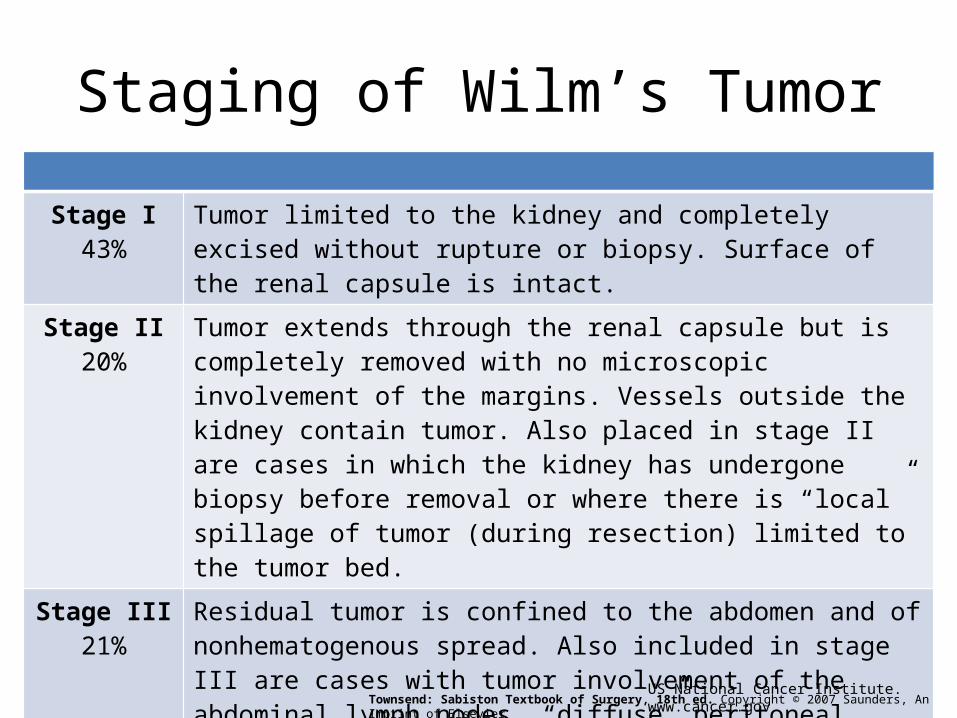
Staging of Wilm’s Tumor
Stage I43%
Tumor limited to the kidney and completely excised without rupture or biopsy. Surface of the renal capsule is intact.
Stage II20%
Tumor extends through the renal capsule but is completely removed with no microscopic involvement of the margins. Vessels outside the kidney contain tumor. Also placed in stage II are cases in which the kidney has undergone biopsy before removal or where there is “local” spillage of tumor (during resection) limited to the tumor bed.
Stage III21%
Residual tumor is confined to the abdomen and of nonhematogenous spread. Also included in stage III are cases with tumor involvement of the abdominal lymph nodes, “diffuse” peritoneal contamination by rupture of the tumor extending beyond the tumor bed, peritoneal implants, and microscopic or grossly positive resection margins.
Stage IV 11% Hematogenous metastases at any site.
Stage V 5% Bilateral renal involvement.
Townsend: Sabiston Textbook of Surgery, 18th ed. Copyright © 2007 Saunders, An Imprint of Elsevier US National Cancer Institute. www.cancer.gov

Staging of Wilm’s Tumor
• Stage I or Stage II – The 4-year survival is 94%
• Stage III – The 4-year survival is 76%
US National Cancer Institute. www.cancer.gov

Wilm’s Tumor: Therapeutic Regimen

Treatment of Wilm’s Tumor
* Infants <11 mo are given half the recommended dose of all drugs. Full doses lead to prohibitive hematologic toxicity in this age group. Full doses of chemotherapeutic agents should be administered to those >12 mo.
NWTS-5 Treatment Recommendations for Wilms' Tumor
Stage I (FH) Surgery, no radiotherapy, dactinomycin + vincristine for 18 wk
Stage I focal anaplasia Surgery, no radiotherapy, dactinomycin + vincristine for 18 wk
Stage II (FH) Surgery, no radiotherapy, dactinomycin + vincristine for 18 wk
Stage II focal anaplasia Surgery, 1080 cGy to tumor bed, dactinomycin +vincristine + doxorubicin for 24 wk
Stage III (FH) Surgery, 1080 cGy to tumor bed, dactinomycin +vincristine + doxorubicin for 24 wk
Stage III focal anaplasia
Surgery, 1080 cGy to tumor bed, dactinomycin +vincristine + doxorubicin for 24 wk
Townsend: Sabiston Textbook of Surgery, 18th ed. Copyright © 2007 Saunders, An Imprint of Elsevier
National Wilms Tumor Study (NWTS) GroupUS National Cancer Institute. www.cancer.gov
Treatment of Wilm’s Tumor
* Infants <11 mo are given half the recommended dose of all drugs. Full doses lead to prohibitive hematologic toxicity in this age group. Full doses of chemotherapeutic agents should be administered to those >12 mo.
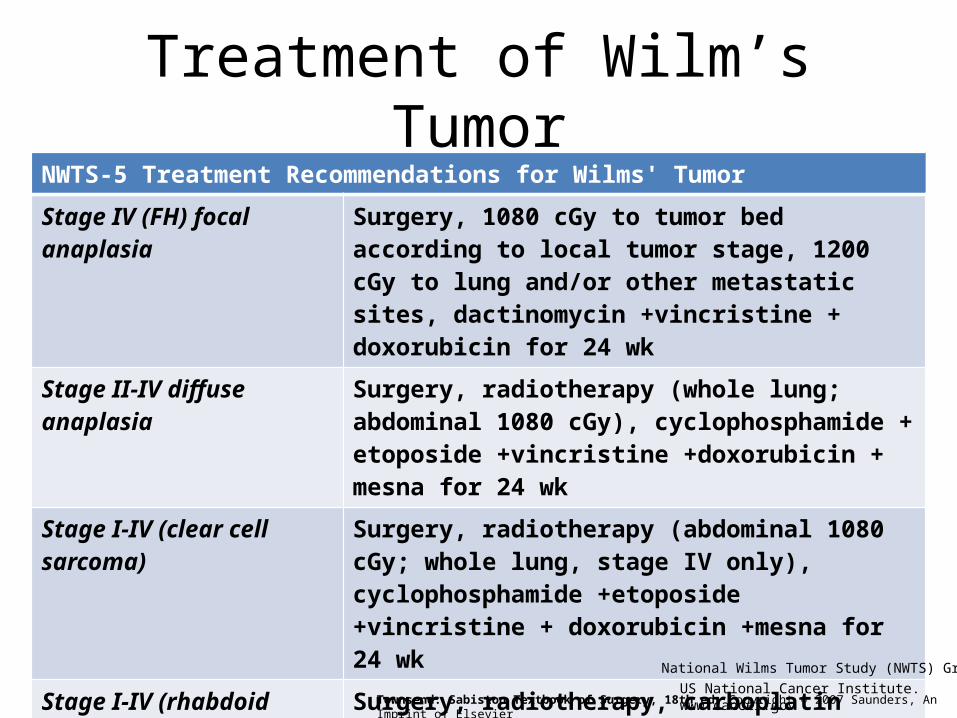
NWTS-5 Treatment Recommendations for Wilms' Tumor
Stage IV (FH) focal anaplasia Surgery, 1080 cGy to tumor bed according to local tumor stage, 1200 cGy to lung and/or other metastatic sites, dactinomycin +vincristine + doxorubicin for 24 wk
Stage II-IV diffuse anaplasia Surgery, radiotherapy (whole lung; abdominal 1080 cGy), cyclophosphamide + etoposide +vincristine +doxorubicin + mesna for 24 wk
Stage I-IV (clear cell sarcoma)
Surgery, radiotherapy (abdominal 1080 cGy; whole lung, stage IV only), cyclophosphamide +etoposide +vincristine + doxorubicin +mesna for 24 wk
Stage I-IV (rhabdoid tumor): Surgery, radiotherapy, carboplatin +etoposide +cyclophosphamide +mesna for 24 wk
Townsend: Sabiston Textbook of Surgery, 18th ed. Copyright © 2007 Saunders, An Imprint of Elsevier
National Wilms Tumor Study (NWTS) GroupUS National Cancer Institute. www.cancer.gov
Resectable Tumors
• Procedure of choice: Radical nephrectomy and lymph node sampling via a transabdominal incision
• Preoperative biopsy should not be performed• Most important role of the surgeon
– to ensure complete tumor removal without rupture and perform an assessment of the extent of disease
National Wilms Tumor Study (NWTS) GroupUS National Cancer Institute. www.cancer.gov

Surgery: Nephrectomy
Radical• Removal of the kidney, the
ipsilateral adrenal gland, and all the fat contained within Gerota's fascia.
• If there is no evidence of adrenal involvement by the tumor on the CT scan, the adrenal gland can be spared
Partial • Controversial; not recommended except for bilateral tumors
National Wilms Tumor Study (NWTS) GroupUS National Cancer Institute. www.cancer.gov
Massive, Nonresectable Unilateral Tumors, Bilateral Tumors
• Candidates for preoperative chemotherapy because of the risk of initial surgical resection.
National Wilms Tumor Study (NWTS) GroupUS National Cancer Institute. www.cancer.gov
Neuroblastoma: Staging
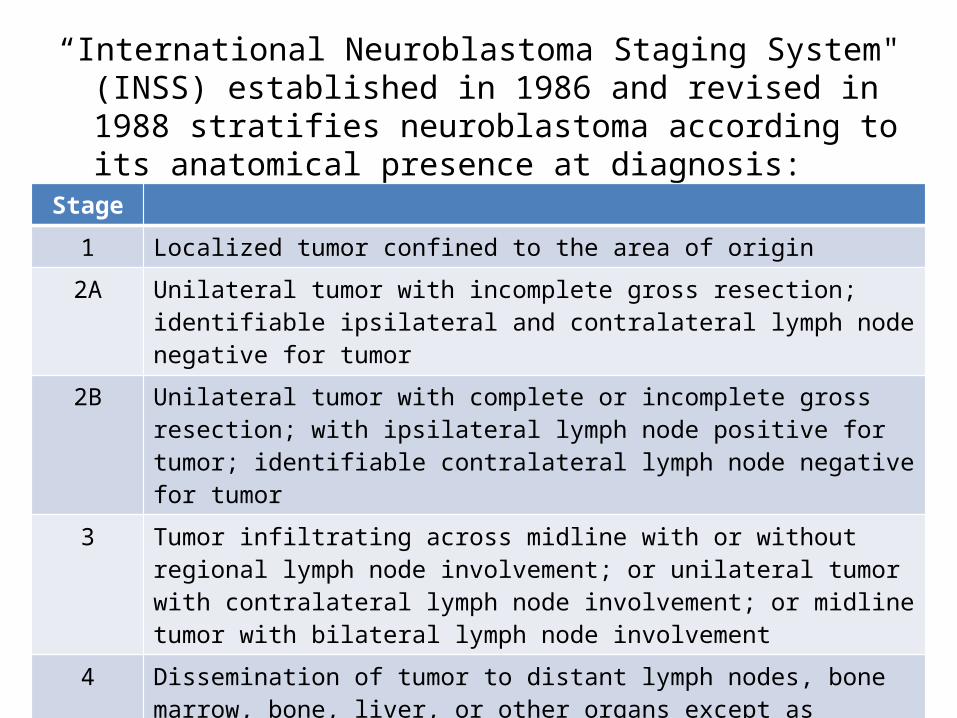
“International Neuroblastoma Staging System" (INSS) established in 1986 and revised in 1988 stratifies neuroblastoma according to its anatomical presence at diagnosis:
Stage
1 Localized tumor confined to the area of origin
2A Unilateral tumor with incomplete gross resection; identifiable ipsilateral and contralateral lymph node negative for tumor
2B Unilateral tumor with complete or incomplete gross resection; with ipsilateral lymph node positive for tumor; identifiable contralateral lymph node negative for tumor
3 Tumor infiltrating across midline with or without regional lymph node involvement; or unilateral tumor with contralateral lymph node involvement; or midline tumor with bilateral lymph node involvement
4 Dissemination of tumor to distant lymph nodes, bone marrow, bone, liver, or other organs except as defined by Stage 4S
4S Age <1 year old with localized primary tumor as defined in Stage 1 or 2, with dissemination limited to liver, skin, or bone marrow (less than 10 percent of nucleated bone marrow cells are tumors)
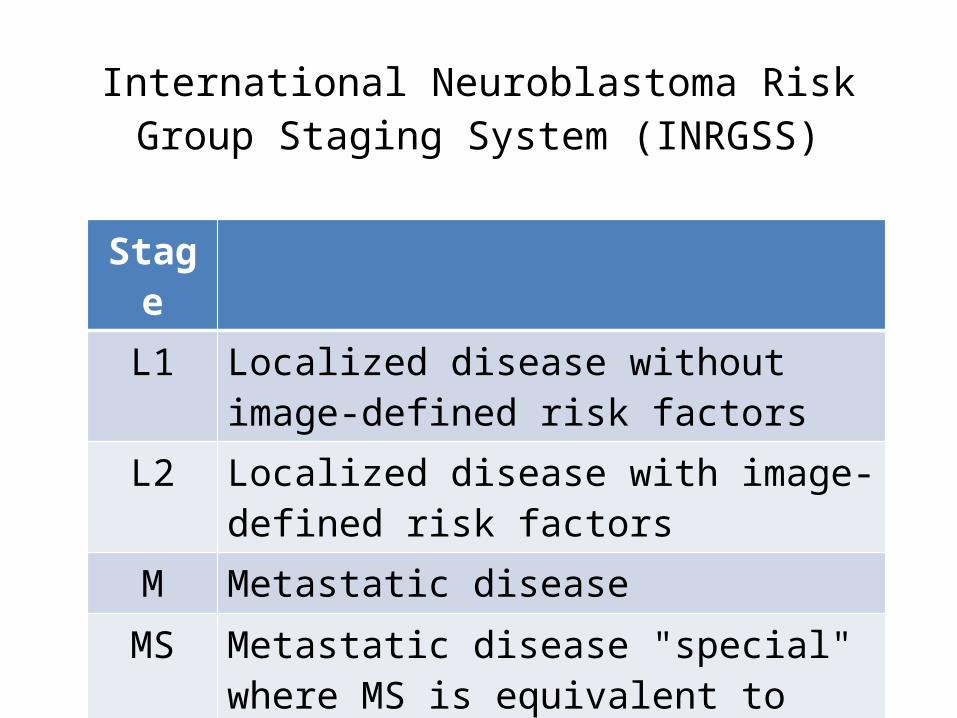
International Neuroblastoma Risk Group Staging System (INRGSS)
Stage
L1 Localized disease without image-defined risk factors
L2 Localized disease with image-defined risk factors
M Metastatic disease
MS Metastatic disease "special" where MS is equivalent to stage 4S

Shimada Histopathologic Classification System
• Describes tumors as either favorable or unfavorable histology based on the degree of differentiation, mitosis-karyorrhexis index, schawannian stroma
• In general, children of any age with localized neuroblastoma and infants <1yr with advanced disease and favorable disease characteristics have a high likelihood of disease free survival
• By contrast, older children with advanced stage disease have significantly decreased chance for cure despite intensive therapy
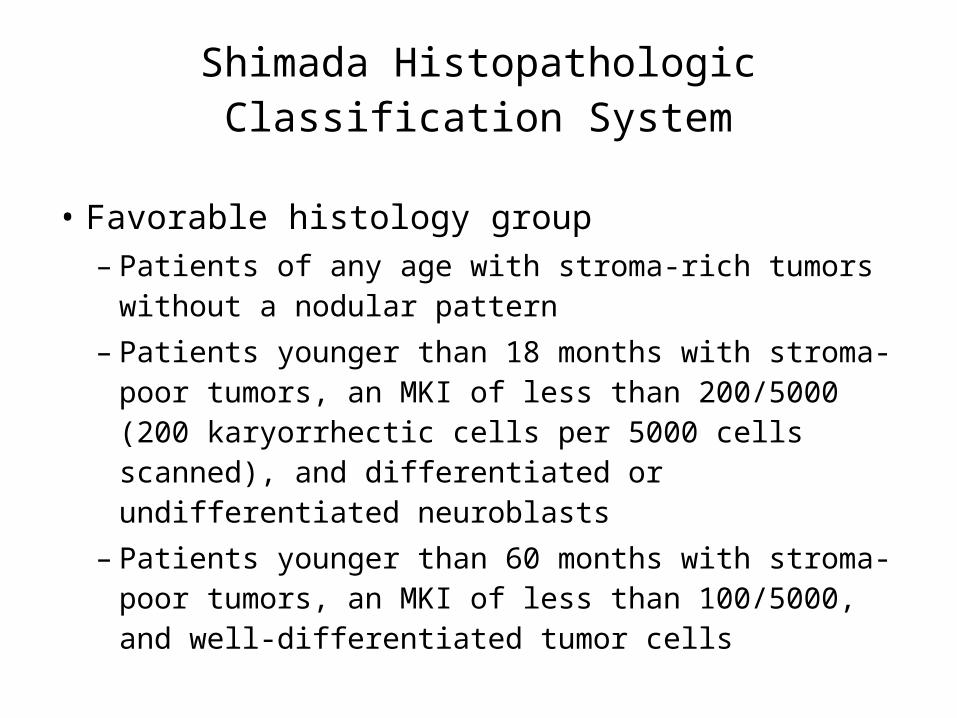
Shimada Histopathologic Classification System
• Favorable histology group– Patients of any age with stroma-rich tumors
without a nodular pattern– Patients younger than 18 months with stroma-
poor tumors, an MKI of less than 200/5000 (200 karyorrhectic cells per 5000 cells scanned), and differentiated or undifferentiated neuroblasts
– Patients younger than 60 months with stroma-poor tumors, an MKI of less than 100/5000, and well-differentiated tumor cells
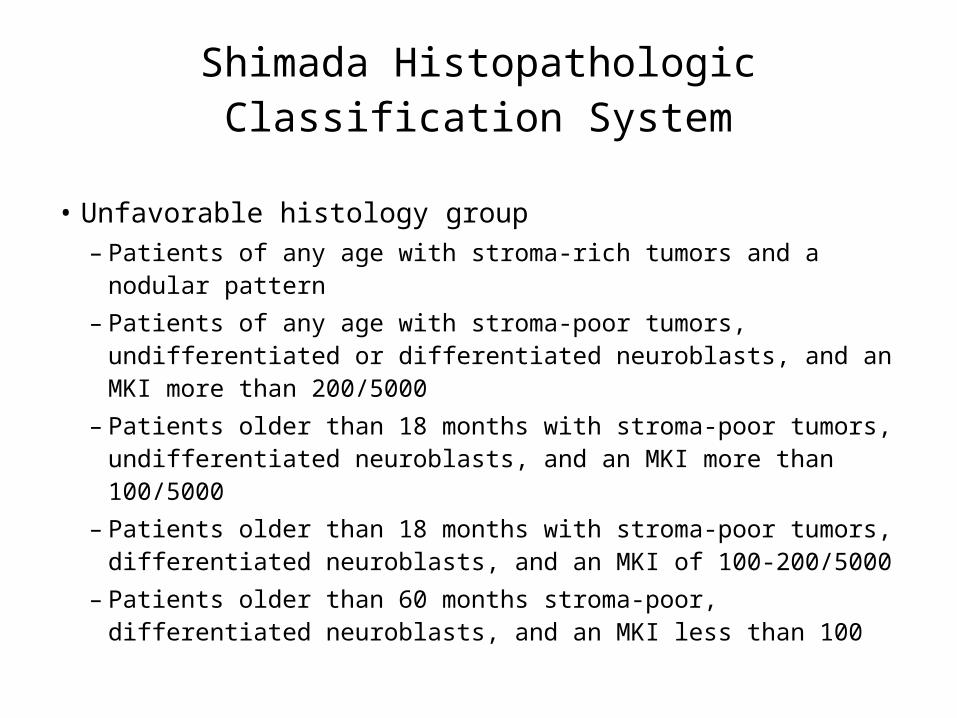
Shimada Histopathologic Classification System
• Unfavorable histology group– Patients of any age with stroma-rich tumors and a nodular
pattern– Patients of any age with stroma-poor tumors, undifferentiated
or differentiated neuroblasts, and an MKI more than 200/5000– Patients older than 18 months with stroma-poor tumors,
undifferentiated neuroblasts, and an MKI more than 100/5000– Patients older than 18 months with stroma-poor tumors,
differentiated neuroblasts, and an MKI of 100-200/5000– Patients older than 60 months stroma-poor, differentiated
neuroblasts, and an MKI less than 100

Neuroblastoma: Therapeutic Regimen
• Stage of the cancer• Child's age• Prognostic markers (hyperdiploid tumor DNA,
N-myc, H-ras)• Chemotherapy• Surgery• Radiation therapy• Retinod therapy
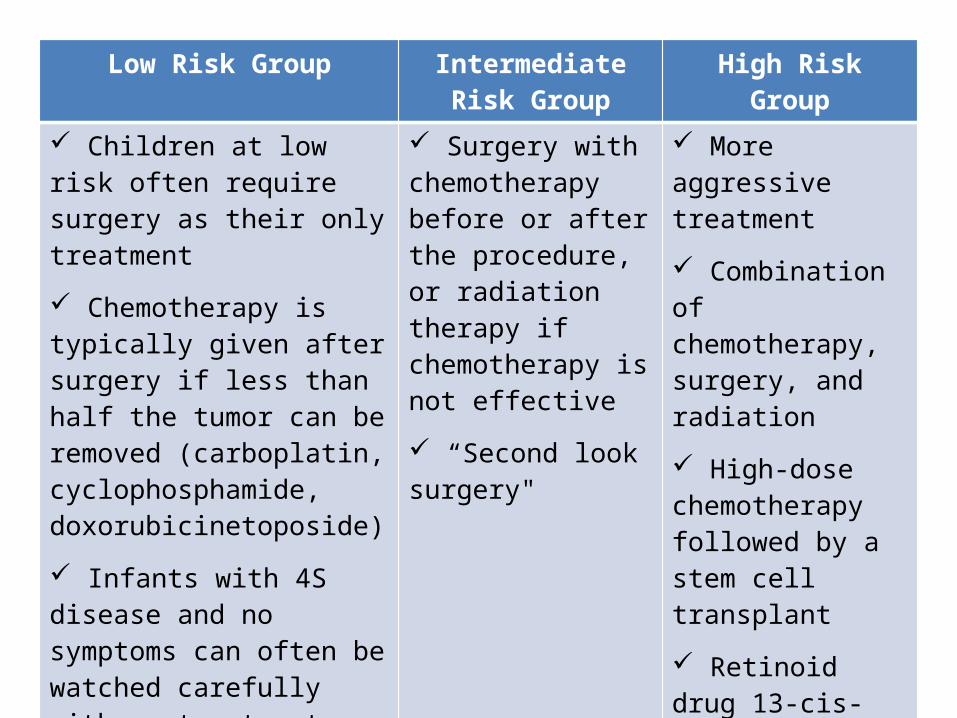
Low Risk Group Intermediate Risk Group
High Risk Group
Children at low risk often require surgery as their only treatment
Chemotherapy is typically given after surgery if less than half the tumor can be removed (carboplatin, cyclophosphamide, doxorubicinetoposide)
Infants with 4S disease and no symptoms can often be watched carefully with no treatment, because these cancers often mature or go away on their own
Surgery with chemotherapy before or after the procedure, or radiation therapy if chemotherapy is not effective
“Second look surgery"
More aggressive treatment
Combination of chemotherapy, surgery, and radiation
High-dose chemotherapy followed by a stem cell transplant
Retinoid drug 13-cis-retinoic acid (isotretinoin) is often given for 6 months after other treatments are completed.
Recurrent Neuroblastoma
• For low- and intermediate-risk neuroblastomas that recur in the same area where they started, surgery with or without chemotherapy may be appropriate
• For higher-risk cancers or those that recur in distant parts of the body, treatment is usually more intense, and may include a combination of chemotherapy, surgery, and radiation therapy
• intensive treatment with high-dose chemotherapy/radiation therapy, followed by a donor stem cell transplant

Chemotherapy
Anti-neoplastic agents• cyclophosphamide or
ifosfamide• cisplatin or carboplatin• vincristine• doxorubicin (Adriamycin)• etoposide• teniposide• topotecan
Side effects• hair loss• mouth sores• loss of appetite• nausea and vomiting• increased chance of
infections (due to low white blood cell counts)
• easy bruising or bleeding (due to low blood platelet counts)
• fatigue

Surgery
• Diagnosis and treatment• Complete resection• Use of adjuvant therapies
Radiation Therapy
• Uses high-energy rays or particles to kill cancer cells– External beam radiation therapy– MIBG radiotherapy

External beam radiation therapy• uses radiation focused on the cancer from a source outside the body• to destroy neuroblastoma cells that remain behind after surgery and
chemotherapy• to try to shrink tumors before surgery, making them easier to
remove at the time of surgery• to treat larger tumors that are causing serious problems (such as
trouble breathing) and do not respond quickly to chemotherapy• as part of the treatment regimen (along with high-dose
chemotherapy) before a stem cell transplant in children with high-risk neuroblastoma
• to help relieve pain caused by advanced neuroblastoma• mild skin reactions, nausea, diarrhea, or fatigue
MIBG radiotherapy
• chemical similar to norepinephrine• Once injected into the bloodstream, the MIBG
goes to the sites of tumors anywhere in the body, where it delivers its radiation
• child will need to stay in a special room for a few days
• nausea and vomiting, lower blood cell counts
Retinoid Therapy
• chemically related to vitamin A• “differentiating agents”• 13-cis-retinoic acid (isotretinoin) reduces the
risk of recurrence after high-dose chemotherapy and stem cell transplant
• 6 month therapy• drying and cracking of the lips, dry skin or
eyes, nosebleeds and changes in the nails

Hydronephrosis: Grading
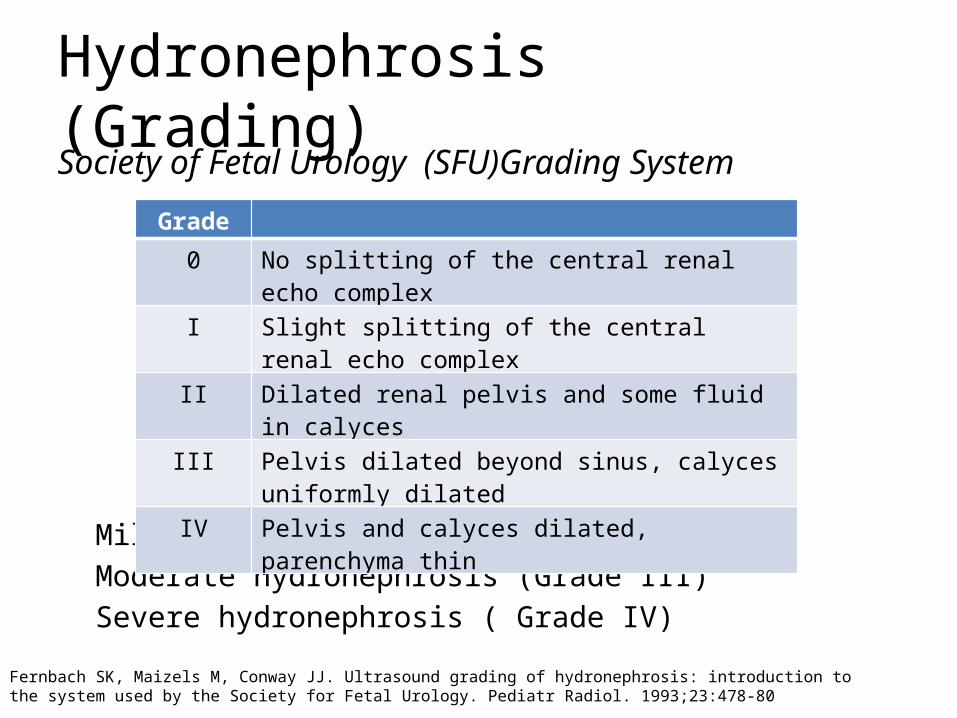
Hydronephrosis (Grading)Society of Fetal Urology (SFU)Grading System
Mild hydronephrosis (Grade I or II)Moderate hydronephrosis (Grade III)Severe hydronephrosis ( Grade IV)
Fernbach SK, Maizels M, Conway JJ. Ultrasound grading of hydronephrosis: introduction to the system used by the Society for Fetal Urology. Pediatr Radiol. 1993;23:478-80
Grade
0 No splitting of the central renal echo complex
I Slight splitting of the central renal echo complex
II Dilated renal pelvis and some fluid in calyces
III Pelvis dilated beyond sinus, calyces uniformly dilated
IV Pelvis and calyces dilated, parenchyma thin
Hydronephrosis: Therapeutic Regimen
Treatment (Medical)
• The role of medical treatment is limited to pain control and treatment or prevention of infection
• Most conditions require either minimally invasive or open surgical treatment.
• Two notable exceptions are (1) oral alkalinization therapy for uric acid stones and (2) steroid therapy for retroperitoneal fibrosis
Vourganti, S. (2008). Hydronephrosis and Hydroureter: Treatment & Medication
Treatment (Medical)
• Neonates with hydronephrosis are at high risk for pyelonephrosis
• Therefore, all neonates diagnosed with unilateral or bilateral hydronephrosis should be started on antibiotic prophylaxis– Example: Amoxicillin 10 mg/kg per 24 h
Schwartz’s Manual of Surgery 8th Ed.

Treatment (Surgical)
• The specific treatment of a patient with hydronephrosis depends on the etiology of the process
• Any signs of infection within the obstructed system warrant urgent intervention because infection with hydronephrosis may progress rapidly to sepsis
• The potential for loss of renal function also adds to the urgency
Vourganti, S. (2008). Hydronephrosis and Hydroureter: Treatment & Medication

Treatment (Surgical)
• Urethral catheterization to help rule out a lower tract cause for hydronephrosis and hydroureter – Difficulty in placing a Foley catheter may suggest
urethral stricture or bladder neck contracture
• Ureteral stent placement in cases of intrinsic and extrinsic causes of hydronephrosis.– Stents can bypass an obstruction and dilate the
ureter for subsequent endoscopic treatment
Vourganti, S. (2008). Hydronephrosis and Hydroureter: Treatment & Medication
Treatment (Surgical)
• Nephrostomy tube– Using the Seldinger technique, a tube ranging from
8-12F can be placed– Placed when a retrograde stent cannot be passed
because of anatomic changes in the bladder or high-grade obstruction in the ureter
Vourganti, S. (2008). Hydronephrosis and Hydroureter: Treatment & Medication
Treatment (Surgical)
• Advances in endoscopic and percutaneous instrumentation have decreased the role of open or laparoscopic surgery for hydronephrosis.
• However, extrinsic causes of hydropnephrosis (retroperitoneal fibrosis, retroperitoneal tumors, and aortic aneurysms) still require treatment with open surgery.
• Some stones that cannot be treated endoscopically or with extracorporeal shockwave lithotripsy require open removal
Vourganti, S. (2008). Hydronephrosis and Hydroureter: Treatment & Medication
Sacrococcygeal Teratoma: Staging

AAPSS Staging Classification of Sacrococcygeal Teratomas
Type DescriptionI Completely external, no presacral componentII External component and internal pelvic
componentIII External component and internal component
extending into abdomenIV Completely internal and no external
component
Fetology: diagnosis & management of the fetal patient By Diana W. Bianchi, Timothy M. Crombleholme, Mary E. D'Alton
Sacrococcygeal Teratoma: Therapeutic Regimen
Treatment
• Chemotherapy– Cisplastin– Bleomycin– If serum AFP levels remain elevated,
chemotherapy containing cisplastin for four cycles is recommended
– Carboplatin– Etoposide
Avery's diseases of the newborn By H. William Taeusch, Roberta A. Ballard, Christine A. Gleason, Mary Ellen Avery

Treatment
• JEB Regimen– Etoposide 120 mg/m2i.v. over 1 hour– Carboplatin i.v. over one hour on day 2 in a dose
calculated as 600 mg/m2
– Bleomycin 15 mg/m2 i.v. over 15 minutes
S.N. Huddart Æ J.R. Mann Æ K. Robinson Æ F. Raafat J. Imeson Æ P. Gornall Æ M. Sokal Æ E. GrayP. McKeever Æ A. Oakhill Sacrococcygeal teratomas: the UK Children’s Cancer Study Group’s experience. I. Neonatal

Treatment
• Surgery– complete surgical excision through a chevron-
shaped buttock incision– most tumors can be completely removed using a
sacral approach• If preoperative imaging demonstrates
significant intra-abdominal extension of the tumor– combined abdominal-sacral approach
Townsend: Sabiston Textbook of Surgery, 18th ed.

• Care must be taken to individually ligate the vessels supplying the tumor, including the middle sacral artery and branches of the hypogastric arteries
• After the tumor is excised, the levator muscle complex is secured to the presacral fascia, and the remaining wound is closed in layers
Townsend: Sabiston Textbook of Surgery, 18th ed.Mature sacrococcygeal teratoma: case reportJN Legbo, WEk Opara, and JF Legbo Department of Surgery, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria