
Stages of change and stuttering: A preliminary view
26
Journal of Fluency Disorders 32 (2007) 95–120 Stages of change and stuttering: A preliminary view Jennifer Floyd a , Patricia M. Zebrowski b,∗,1 , Gregory A. Flamme c a 2392 E. 116th Ct., Thornton, CO 80233, 303-920-0471, United States b Department of Speech Pathology Audiology, University of Iowa, 127C SHC, Iowa City, IA 52245, United States c Department of Speech Pathology Audiology, Western Michigan University, Kalamazoo, MI 49008, United States Received 22 December 2006; received in revised form 7 March 2007; accepted 9 March 2007 Abstract As a way to better understand the process of change that occurs in stuttering, Craig [Craig, A. (1998). Relapse following treatment for stuttering: a critical review and correlative data. Journal of Fluency Disorders, 23, 1–30] compared the behavioral changes that people who stutter often experience with and without treatment to those that have been observed for certain (non)addictive behavior disorders such as smoking, overeating, phobia and anxiety disorder. The process underlying these behavioral changes has been described by the transtheoretical or “stages of change” model, which is a model of behavior change that can illuminate “where” a person is in the process of change, and how this may relate to the outcome of either treatment or self-change attempts [Prochaska, J. O., & DiClemente, C. C. (1986). The transtheoretical approach. In J. C. Norcross (Ed.), Handbook of eclectic psychotherapy. New York: Brunner/Mazel]. The purpose of the present study was to analyze the extent to which the responses of adults who stutter on a modified Stages of Change Questionnaire yield interrelations among questionnaire items that are consistent with a stage-based interpretation. Results of both confirmatory and exploratory factor analyses indicated that while the modified questionnaire was a relatively good fit for participant responses, the structure derived from the exploratory analysis provided a significantly better fit to the observed data. Results suggest that a questionnaire incorporating items that better reflect the unique behavioral, cognitive and affective variables that characterize stuttering may better discriminate stages of change in people who stutter as they move through therapy, or are engaged in self-directed change. Educational objectives: After reading this paper, the learner will be able to: (1) describe the transtheoretical or “stages of change” model; (2) describe the various processes that are associated with different stages of ∗ Corresponding author. Tel.: +1 319 3358735; fax: +1 319 3358851. E-mail addresses: jfl[email protected] (J. Floyd), [email protected] (P.M. Zebrowski), Greg.fl[email protected] (G.A. Flamme). 1 Tel.: +1 303 920 0471. 0094-730X/$ – see front matter © 2007 Elsevier Inc. All rights reserved. doi:10.1016/j.jfludis.2007.03.001
-
Upload
jennifer-floyd -
Category
Documents
-
view
212 -
download
0
Transcript of Stages of change and stuttering: A preliminary view
Journal of Fluency Disorders 32 (2007) 95–120
Stages of change and stuttering: A preliminary view
Jennifer Floyd a, Patricia M. Zebrowski b,∗,1, Gregory A. Flamme c
a 2392 E. 116th Ct., Thornton, CO 80233, 303-920-0471, United Statesb Department of Speech Pathology Audiology, University of Iowa, 127C SHC,
Iowa City, IA 52245, United Statesc Department of Speech Pathology Audiology, Western Michigan University,
Kalamazoo, MI 49008, United States
Received 22 December 2006; received in revised form 7 March 2007; accepted 9 March 2007
Abstract
As a way to better understand the process of change that occurs in stuttering, Craig [Craig, A. (1998).Relapse following treatment for stuttering: a critical review and correlative data. Journal of FluencyDisorders, 23, 1–30] compared the behavioral changes that people who stutter often experience with andwithout treatment to those that have been observed for certain (non)addictive behavior disorders such assmoking, overeating, phobia and anxiety disorder. The process underlying these behavioral changes hasbeen described by the transtheoretical or “stages of change” model, which is a model of behavior changethat can illuminate “where” a person is in the process of change, and how this may relate to the outcome ofeither treatment or self-change attempts [Prochaska, J. O., & DiClemente, C. C. (1986). The transtheoreticalapproach. In J. C. Norcross (Ed.), Handbook of eclectic psychotherapy. New York: Brunner/Mazel]. Thepurpose of the present study was to analyze the extent to which the responses of adults who stutter on amodified Stages of Change Questionnaire yield interrelations among questionnaire items that are consistentwith a stage-based interpretation. Results of both confirmatory and exploratory factor analyses indicatedthat while the modified questionnaire was a relatively good fit for participant responses, the structurederived from the exploratory analysis provided a significantly better fit to the observed data. Results suggestthat a questionnaire incorporating items that better reflect the unique behavioral, cognitive and affectivevariables that characterize stuttering may better discriminate stages of change in people who stutter as theymove through therapy, or are engaged in self-directed change.
Educational objectives: After reading this paper, the learner will be able to: (1) describe the transtheoreticalor “stages of change” model; (2) describe the various processes that are associated with different stages of
∗ Corresponding author. Tel.: +1 319 3358735; fax: +1 319 3358851.E-mail addresses: [email protected] (J. Floyd), [email protected] (P.M. Zebrowski),
[email protected] (G.A. Flamme).1 Tel.: +1 303 920 0471.
0094-730X/$ – see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.jfludis.2007.03.001

96 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
change; (3) summarize research findings in stages of change as they apply to a variety of clinical populations;(4) discuss the applicability of the findings from the present study to stuttering treatment, and (5) relateconventional strategies and techniques used in stuttering therapy to different stages in the process of change.© 2007 Elsevier Inc. All rights reserved.
Keywords: Stages; Change; Stuttering
In an attempt to explain the different factors that contribute to treatment responsiveness instuttering therapy, Zebrowski and Conture (1998) identified both “client independent” and “clientdependent” variables that may affect treatment outcome. So-called client independent factorsinclude observable and measurable stuttering behaviors, such as the frequency, duration, andtype of speech disfluency an individual produces, as well as environmental factors that mightinfluence the frequency, severity and variability of stuttering. Client dependent variables, on theother hand, are comprised of those affective and cognitive factors or characteristics that havebeen implicated in the development of intractable stuttering. For example, a number of studiesof stuttering treatment have shown that variables such as avoidance, external locus of control,production of learned compensatory behaviors, negative attitudes about speech, and high levelsof trait anxiety are associated with poorer long-term gains from therapy as well as relapse (e.g.,Blood, 1993; Craig, 1998; Guitar, 1976, 1998; Guitar & Bass, 1978). In a more recent study, Huincket al. (2006) showed that a pretreatment profile consisting of measures of stuttering severity andseverity of both negative emotions and cognitions yielded subgroups that experienced differenttreatment outcomes. Finally, a number of authors have argued that the client’s motivation andwillingness to change have a critical impact on stuttering treatment outcome. In particular, theclient’s readiness for change as it relates to the timing of therapy enrollment is an important factorin success; that is, beginning therapy when one is most ready for change leads to a more positiveoutcome and maintenance of therapy goals (Blood, 1993; Manning, 2001, 2006; Shapiro, 1999).
In 1998, Craig published an excellent review and extension of the research in stuttering treat-ment outcome, with a special focus on the factors that may predict relapse. He concluded thatthere are limited factors that alone can reliably predict relapse; rather a multifactorial model ofrelapse has the most validity. Craig further noted that relapse in stuttering therapy is relativelytypical, and that it is strikingly similar to the “relapse-success cycle” (p. 23) that characterizes thechange process in therapy for other behavioral and psychological disorders and addictions (e.g.,smoking, eating disorders, phobia, etc.). For example, the cyclical nature of the smoking cessationprocess, with its alternating periods of improvement and relapse over time, also characterizes themovement toward long-term change in speech fluency that individuals who stutter experience overthe course of therapy. Manning (2001, 2006) echoed this point by describing stuttering therapyas a “pattern of cyclical movement through a process of gradually more successful managementof stuttering-related behaviors and processes” (2006; p. 140). Until the new behaviors the clientis learning in therapy become stable and predictable, it is likely that he or she will move back andforth between periods of more and less fluency on the path to recovery, at times even revertingback to pre-therapy levels of stuttering (or “relapse”).
Like Craig, Manning noted that the pattern of change and relapse seen in stuttering therapyis very similar to that observed in other disorders, and suggested that previous research in thebroader area of change (e.g., Prochaska, DiClemente, & Norcross, 1992), would be a good placeto start to examine the change process in the stuttering population, with an eye toward developingeffective anti-relapse strategies.
J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 97
1. Theories of change: the theory of planned behavior and the transtheoretical orstages of change model
Research in the fields of health and sports psychology, and psychotherapy, has long beendevoted to the study of how people make durable behavioral change. Over the years, a numberof theories of change have been developed that have provided the framework for interventionapproaches designed to help people acquire positive health behaviors (e.g., smoking cessation)and optimal physical performance. In general, an individual’s beliefs and intentions have been thecornerstone of arguably the two dominant models of health behavior change: the theory of plannedbehavior (Ajzen, 1985) and the transtheoretical or “stages of change” model (Armitage, 2006;Prochaska & DiClemente, 1984). Briefly, the major premise of the theory of planned behavioris that an individual’s decisions about behavior change are rooted in predetermined intentions,and it is these intentions that are the best predictors of what people will do (Sarafino, 2006).Intention to change is a single construct that is based on a summary of three main judgmentfactors, namely the person’s perceptions of (1) how acceptable or unacceptable the behavior isto him or her (attitude), (2) how acceptable or unacceptable the behavior is to others (subjec-tive norm), and (3) the likelihood of success in changing or acquiring behavior (self-efficacy).The major focus of the theory of planned behavior is to predict and understand health-relatedchange; thus researchers investigating this model typically use prospective designs (Armitage,2006).
The transtheoretical or stages of change model is an integrated model that includes cogni-tive, affective and behavioral constructs that are described in other well-established theories ofintentional change, including the theory of planned behavior (Ajzen, 1985). The transtheoreti-cal model is based on the observation that successful change can be demonstrated through bothself-change and “professionally assisted” approaches, suggesting that there are “basic, commonprinciples that can reveal the structure underlying change occurring with and without (psycho)therapy” (Prochaska et al., 1992, p. 1102). It is a model of intentional change, in that it attempts toexplain how decision-making, rather than sociological or biological influences, impacts behaviorchange. The major focus of the transtheoretical model is to understand how people change, orthe process (not solely the outcome) of intentions to change. Most notably, the model attemptsto understand change readiness as an important piece of the entire process of behavioral change.In a series of studies, Prochaska and co-workers developed an instrument that could both delin-eate and validate the core elements, or stages of change (e.g., McConnaughy, Prochaska, &Velicer, 1983). Using responses to a 32-item scale administered to a wide range of individualsacross various clinical populations (i.e., psychotherapy clients, people in smoking cessation andweight-loss programs, etc.), Prochaska and co-workers employed a principal components anal-ysis that yielded six distinct stages of change. These stages were defined as: precontemplation,contemplation, preparation, action, maintenance, and termination. Additional analysis of partic-ipant responses demonstrated that adjacent stages (e.g., precontemplation and contemplation)were more highly correlated than nonadjacent stages (e.g., precontemplation and maintenance),suggesting that as people change, they tend to move through a predictable sequence of behaviorchange stages. Finally, subsequent work demonstrated that there are specific levels and pro-cesses of change that are associated with each stage, and that therapy is most successful whenprocesses are “matched” to their related stages (Prochaska, 1999; Prochaska & DiClemente,1984).
Since its introduction, the stages of change model has been applied in many settings to individu-als exhibiting a variety of behaviors requiring change. Numerous published articles have confirmed

98 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
the relevance of the model to the change process inherent in such areas as smoking cessation,cocaine cessation, weight control, adoption of a low-fat diet and exercise, elimination of adolescentdelinquent behavior, safer sex practices and condom use, sunscreen use, increasing frequency ofmammography screening, and treatment of a variety of eating disorders (e.g., DiClemente, 1993;Marcus & Simkin, 1994; Pallonen et al., 1994; Prochaska et al., 1994; Ruggiero, 1998; Suris,Carmen Trapp, DiClemente, & Cousins, 1998). Further, the stages of change model of inten-tional change can illuminate relationships between ‘where’ an individual is in the process ofchanging behavior, and the outcome of either therapy or self-change strategies. That is, being ina particular “stage” of behavioral change can facilitate progress in therapy if there is a “match”between stage and treatment approach, or present an obstacle to change if there is a mismatchbetween the client’s readiness for change and the treatment approach or specific techniques usedin therapy.
2. Understanding change in stuttering
As previously discussed, being able to describe the range of patterns of intentional changein people who stutter (with or without therapy) can inform the development of treatment inkey ways. The stages of change model seem most appropriate for understanding the changeprocess in stuttering for a number of reasons. First, as Craig (1998) and Manning (2001, 2006)have observed, similar to other behavioral change processes, change in stuttering is cyclical andrelapse appears to be typical. The stages model describes change as circular rather than linear,in that instead of relapse occurring in the final stage of a set sequence of stages, it can, andusually does, occur at any time over the course of the change process. And, rather than beingviewed as “the end of the line”, the stages model views relapse as a bridge back to an earlier stagein which the individual has the opportunity to strengthen the skills necessary to make changemore durable and relapse less likely to occur (Brownell, Marlatt, Lichtenstein, & Wilson, 1986).As Craig argued, understanding this pattern in people who stutter can lead to a comprehensivemodel of relapse in stuttering and the subsequent development of effective anti-relapse strategies.Second, as Manning and others have argued, assessing an individual’s readiness for change seemsparticularly important when making decisions about when to enroll in formal treatment, andwhat strategies to employ, and the stages of change model allows for the assessment of thisphenomenon.
Recently, Turnbull (2000) described the clinical applicability of the stages of change model tostuttering treatment by using case examples to argue that the model captures the change processtypically brought about by therapy. She contended that an appreciation of client stage at a particularpoint in time would assist clinicians in adjusting treatment levels and processes to meet theindividual’s needs. Turnbull further illustrated her point by discussing commonly used stutteringtherapy strategies as they might best be applied within specific stages of change. As previouslydescribed, the stage of change model has been successfully applied to a variety of disorders thatbear a striking resemblance to developmental stuttering, in terms of the cognitive and affectivelayers that constitute the disorder as a whole. These similarities suggest that the stages of changemodel can be useful as a method for determining what stage in the change process a person whostutters is in when entering therapy, and how to select the therapeutic focus that will increase theprobability of a better therapeutic outcome.
An obvious first step in any attempt to apply the stages of change model to either therapeutic orself-change in adults who stutter is to determine whether the model can be applied to the stutteringpopulation. With this initial aim in mind, the purpose of the present study was to analyze the extent

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 99
to which the responses of adults who stutter on a modified Stages of Change Questionnaire yieldinterrelations among questionnaire items that are consistent with a stage-based interpretation. Theobservation of such a factor structure could then serve as the basis for the further developmentof criteria to place an individual in any one of the stages of change that have been observed tocharacterize other clinical populations. Further, if the therapeutic change process for individualswho stutter can be described by a stage-based model, the development of optimal treatmentstrategies across various stages is possible. Alternately, if the relationships among questionnaireitems are inconsistent with the stages of change model, further work will be necessary to determinethe best way to conceptualize an individual’s status within the process of change. Overall, thelong-term goals of this research are to develop a clinically useful tool for placing an individualwho stutters into a particular stage when therapy commences, and to examine the extent to whichthe processes of change described by Prochaska and co-workers are relevant to these stages asobserved for people who stutter.
In order to provide the context for the study discussed in this paper, the following sectionpresents a more in-depth description of the stages, processes and levels that constitute the “stagesof change” model, along with the questionnaire format for determining an individual’s stage ofchange.
3. A brief description of the stages of change model: stages, processes and levels
3.1. Stages
As previously discussed, in the stages of change model, individuals move through five stageswhile changing behavior: precontemplation, contemplation, preparation, action, and maintenance.Each stage represents a different point in the “readiness” of an individual for change, and assumesboth a period of time and a set of tasks that need to be accomplished in order to move to the nextstage (DiClemente, 1993).
3.1.1. PrecontemplationBriefly, in the precontemplation stage, individuals do not recognize a need for change. People
may be in the precontemplation stage because they are denying that a problem exists, or theymay have had prior therapy experiences that have been unsuccessful. They may underestimatethe impact that change will have on their lives, and overestimate the cost involved in changing(Prochaska, 1999).
3.1.2. ContemplationProchaska (1999) described contemplation as the stage in which people “intend to change
in the next six months” (p. 229). They are still ambivalent about the cost/benefit ratio, whichcan lead to procrastination. Regardless, individuals who are in contemplation are not ready fortherapy that involves active behavioral change (e.g., treatment that focuses on behavioral speechchanges).
3.1.3. PreparationIn this stage, people have begun taking some form of action to make changes in their behav-
ior. This may take the form of so-called “bibliotherapy” (including web-surfing), obtaining thenames and contact information of relevant helping professionals, or attempting some sort ofself-therapy.

100 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
3.1.4. ActionThe action stage is characterized by tangible and deliberate changes at some level. Sometimes
these modifications can be observed and even measured (e.g., changes in speech fluency and/orstuttering behavior; changes in attitudes about talking and stuttering), and sometimes they cannot(e.g., retaining a focus in the present when starting to feel anxious about talking, or trying,successfully or not, to reduce the amount of “overthinking” listener reactions to stuttering).
3.1.5. MaintenanceThis stage involves active attempts to prevent relapse or regression. Typically, the individual
does not practice change processes as frequently as he or she did during the action stage. Mainte-nance, which can be thought of as generalization over time, requires sustained effort or attentionover a prolonged period. One of the primary reasons that people fail to maintain behavior, orrelapse, is that they are not prepared to do “what it takes” to achieve lasting change.
As previously described, the stages of change model assume that change is not an all-or-none-phenomenon, but rather a gradual movement through stages. The model assumes that regardlessof the change to be made, not all people are ready for the same type of change, and because of thisreality, individuals enter therapy at different stages (Prochaska et al., 1992). Moreover, movementthrough the stages requires the use of processes that are appropriate for each stage. In general,movement is not linear, but spiral, and most people experience relapse and regression to an earlierstage (Prochaska et al., 1992). When this occurs, however, the individual does not recycle throughthe stages endlessly, but instead uses what he or she has learned from prior mistakes, and tendsto move through each stage more quickly the “second time around.”
3.2. Processes
Prochaska and DiClemente’s (1986) analysis of different psychotherapeutic approachesrevealed 10 distinct processes that people use as they move through the stages of change. Table 1provides descriptions of these 10 processes along with their associated stages of change. In gen-eral, processes of change represent the activities a person engages in to modify a behavior, affect,or cognition, and include such actions as consciousness raising, stimulus control and developinghelping relationships with others. These processes appear to be tied to an individual stage, or tooverlap adjacent stages, in that a specific process tends to be used more often when an individualis in a particular stage of change. For example, the process of “consciousness raising” appears tobe used most often when an individual is in the precontemplation stage, and continues to be usedfrequently as he/she moves into contemplation. Consciousness raising includes such activities asinformation gathering about oneself and the problem (e.g., through reading and talking to others,including a professional), making observations and so forth. “Self-liberation”, on the other hand,is a process used most frequently in the later stage of preparation, and continues to be used asthe individual moves from preparation to action. Self-liberation includes those specific strategiesthat people use to commit to change (Prochaska et al., 1992), such as personal and interpersonalcontracts and resolutions.
3.3. Levels
Finally, levels of change represent the components of a particular problem that need to beaddressed in therapy. According to Prochaska and DiClemente (1986) there are five distinctlevels within a particular problem, organized in a hierarchical fashion. From lowest to highest

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 101
Table 1Stages of change and their associated processes
Stage Processes
Precontemplation (1) Assessing how one feels and thinks about oneself with respect to a problem: valueclarification, imagery, corrective emotional experience
Contemplation (1) Increasing information about self and problem: observations, confrontations, interpretations,bibliotherapy(2) Assessing how one feels and thinks about oneself with respect to a problem: valueclarification, imagery, corrective emotional experience
Preparation (1) Assessing how one feels and thinks about oneself with respect to a problem: valueclarification, imagery, corrective emotional experience(2) Choosing and commitment to act or belief in ability to change: decision-making therapy,New Year’s resolutions, logotherapy techniques, commitment enhancing techniques
Action (1) Choosing and commitment to act or belief in ability to change: decision-making therapy,New Year’s resolutions, logotherapy techniques, commitment enhancing techniques(2) Substituting alternatives for problem behaviors: relaxation, desensitization, assertion,positive self-statements(3) Avoiding or countering stimuli that elicit problem behaviors: restructuring one’senvironment (e.g., removing alcohol or fattening foods), avoiding high risk cues, fadingtechniques(4) Being open and trusting about problems with someone who cares: therapeutic alliance,social support, self-help groups
Maintenance (1) Substituting alternatives for problem behaviors: relaxation, desensitization, assertion,positive self-statements(2) Increasing alternatives for nonproblem behaviors available in society: advocating for rightsof repressed, empowering, policy interventions(3) Rewarding one’s self or being rewarded by others for making changes: contingencycontracts, overt and covert reinforcement, self-reward
Source: Prochaska, J. O., Diclemente, C. C., & Norcross, J. C. (1992). In search of how people change: Applications tothe cessation of smoking. Journal of Consulting and Clinical Psychology, 56(4), 520–528.
points (i.e., least to most complex and/or challenging), these include: symptom or situational,maladaptive cognitions, current interpersonal conflicts, family or system conflicts and intrap-ersonal conflicts. For the most part, the stages of change model proposes that clinicians beginwork at the symptom or situational level, because it is a more conscious level and tends to rep-resent the client’s primary reason for entering therapy. As such, change tends to occur fasterat the symptom or situational level. In stuttering therapy, for example, the main focus at thesymptom or situational level would likely be speech, so that strategies targeting either fluency(i.e., fluency shaping) or stuttering (i.e., stuttering modification) should yield positive results in arelatively short time. As the client moves up the hierarchy of levels (i.e., from the symptom to fam-ily/system and intrapersonal conflicts), those aspects or “layers” of the problem that are related tosense of self tend to be discovered. These higher levels typically require longer and more complextherapy.
The levels of change are interrelated, such that changes at one level will lead to change at otherlevels. In addition, a particular problem may be maintained at several levels, requiring a clinicianto be prepared to work at any of the five levels of change, individually or simultaneously. Mostimportantly, it is thought to be essential to the process of change that the client and clinician agreeon the level at which to work (accommodating the client’s theory of change.)

102 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
3.4. Stages of Change Questionnaire
In 1983, McConnaughy, Prochaska, and Velicer published the first study designed to developan instrument for operationally defining the five stages of change. From this investigation emergedthe “Stages of Change Questionnaire”, which they distributed to 155 outpatients across a varietyof mental health settings. The questionnaire, or scale, consisted of 32 statements and employeda five point Likert format (“1” corresponding to “strongly agree”; “5” corresponded to “stronglydisagree”). A principal components analysis yielded four distinct stages of change: precon-templation, contemplation, action and maintenance. Results indicated that preparation did notemerge as a distinct stage, leading the authors to speculate that this stage may be transitoryduring relatively fast decision making, and that it involves both contemplation and action (itstwo adjacent stages). Additional analysis demonstrated that adjacent stages (e.g., precontem-plation and contemplation; contemplation and action, etc.) were more highly correlated witheach other than they were with nonadjacent stages (e.g., precontemplation and maintenance),suggesting that as people change, they move through a predictable sequence. McConnaughyet al. (1983) concluded that the process of change is best characterized by these four adjacentstages. This work resulted in a modification of the original questionnaire into a version that con-tained the original 32 items contained within four, eight-item subscales, each related to one ofthe four distinct stages of change: precontemplation, contemplation, action, and maintenance. Inrecent studies and clinical papers, the Stages of Change Questionnaire has also been referred toas the University of Rhode Island Change Assessment (URICA) (e.g., DiClemente & Hughes,1990; Pantalon & Swanson, 2003; www.uri.edu/research/cprc/Measures/Smoking04urica.htm).
4. Summary
The stages of change or transtheoretical model has been speculated to be valid for both thedelineation of readiness for change and the description of the change process for people who stutter.Currently, however, there are no data to either support or refute this hypothesis. The purpose ofthis preliminary study, then, was to assess the validity of a stages model to characterize thechange process in the population of adults who stutter, and specifically, to examine the extentto which responses to items on a modified version of the Stages of Change Questionnaire (orURICA) would yield a factor structure similar to that which has been observed for other clinicalpopulations. If so, this factor structure could form the basis for the development of criteria to placean individual in any one of the stages of change that have been observed to characterize otherclinical populations. Alternately, if the relationships among questionnaire items are inconsistentwith the stages of change model, further work will be necessary to determine the best way toconceptualize an individual’s status within the process of change.
5. Method
5.1. Participants
Participants for this study were 44 adolescents and adults who stutter between the ages of 16 and61, with a mean age of 34.9 years. Ten participants were female and 34 were male. Participants werevolunteers recruited through speech-language pathologists and through the National StutteringAssociation (NSA). All participants reported a history of stuttering therapy.

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 103
Individual speech-language pathologists and NSA chapters (hereafter referred to as “gate-keepers”) were contacted by the investigators, and provided with a brief description of the studymethods. Gatekeepers were asked to provide this description, at their own discretion, to personswho stutter whom they knew personally, or for whom they currently provided treatment (in thecase of speech-language pathologists). Neither the purpose of the study, nor its related hypotheses,were shared with either the gatekeepers or potential participants. If and when interested partiesexpressed interest, they were given a letter describing the study methods in more detail. Subse-quently, all interested potential participants were sent a letter describing the study methods again,and what their involvement in the study would involve. Once an individual agreed to participate,he or she was given a consent form, and then a modified Stages of Change Questionnaire to com-plete and return to the first author within a predetermined period of time. The study participantscompleted the scale at their own pace and returned it to the first author in a stamped envelopeprovided by the investigators.
5.2. Procedure
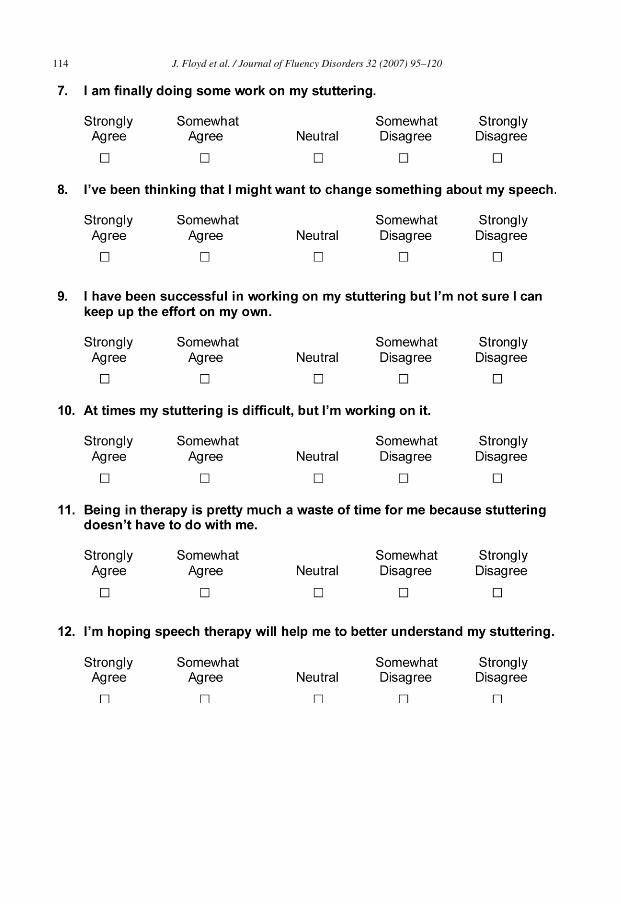
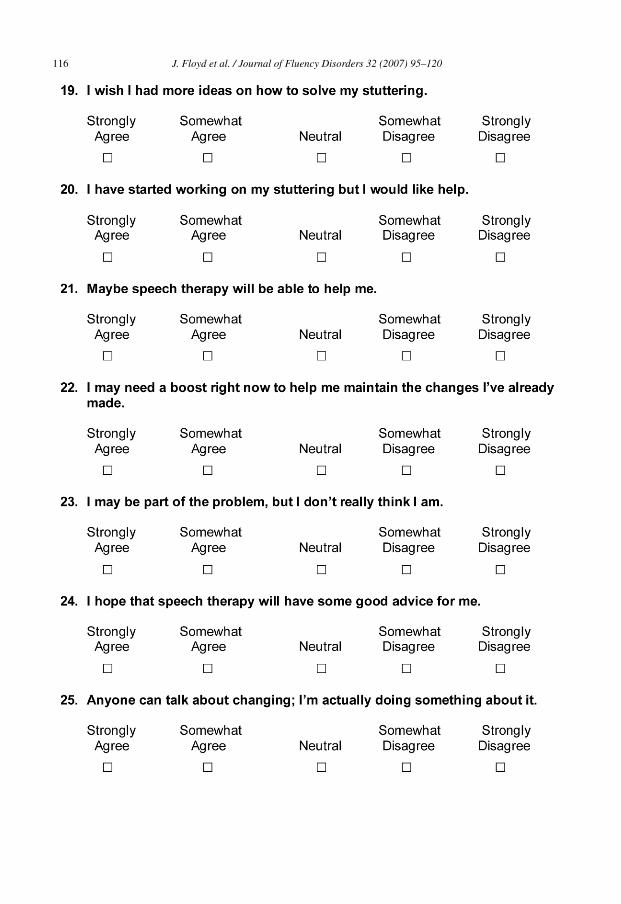
A modified Stages of Change Questionnaire (Appendix A) was developed for distribution toindividuals who consented to participate in the study. As shown in Appendix A, we modified theitems on the original questionnaire (i.e., McConnaughy et al., 1983) to make it relevant to the expe-riences of people who stutter. In most cases, this was accomplished by making minor changes inwording; for example, the specific term “stuttering” was used in place of “problem,” and “speechtherapy” was used in place of “here.” Similar to the original Stages of Change Questionnaire, thismodified version was a 32-item survey consisting of four, 8-item subscales to measure the fourdistinct stages of change: precontemplation, contemplation, action, and maintenance. Participantswere instructed to respond to each item using a 5-point Likert format, where 1 corresponded to“strongly agree” and 5 corresponded to “strongly disagree”. In accordance with McConnaughyet al. (1983), the items or statements on the modified questionnaire proposed to assess precon-templation were: 1, 5, 11, 13, 23, 26, 29, 31; items proposed to assess contemplation were: 2, 4,8, 12, 15, 19, 21, 24; items proposed to assess action were: 3, 7, 10, 14, 17, 20, 25, 30; and itemsproposed to assess maintenance were: 6, 9, 16, 18, 22, 27, 28, 32.
The psychometric properties of the Stages of Change Questionnaire have been evaluated ina number of studies across a wide variety of substance-related disorders (e.g., Pantalon, Nick,Franforter, & Carroll, 2002). In particular, it has been shown to have good concurrent and predictivevalidity (e.g., Blanchard, Morgenstern, Morgan, Labouvie & Bux, 2003; DiClemente & Hughes,1990) and internal consistency ranging from acceptable to good (Carey, Purnine, Maisto & Carey,1999; Pantalon et al., 2002).
5.3. Data analyses
The main purpose of this study was to assess the validity of a stages model to characterizethe change process in the population of adults who stutter, and specifically, to examine the extentto which responses to items on a modified version of the Stages of Change Questionnaire (orURICA) would yield a factor structure similar to that which has been observed for other clinicalpopulations. In order to allow for such an examination, both a confirmatory and exploratoryanalyses were used.
The factors in a confirmatory factor analysis are defined as a combination of related or inter-dependent variables. These underlying factors are identified through cross-correlations among

104 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
the items related to a given factor. For the present study, the modified questionnaire structure(e.g., McConnaughy et al., 1983) was used as a template; that is, the confirmatory factor analysiswas completed to assess the extent to which the 32 items on the modified questionnaire groupedtogether to form the four stages (factors) as observed in previous research (e.g., for the stutteringgroup, do questionnaire items 1, 5, 11, 13, 23, 26, and 31 form the precontemplation stage?).In addition, the confirmatory analysis allowed us to examine relationships between stages; thatis, are adjacent stages more highly correlated than non-adjacent stages? The confirmatory factoranalysis (using EQS v6.1 structural equation modeling software) was completed on the responsesobtained from the questionnaires completed by study participants. Maximum likelihood estima-tion with robust standard errors was used to adjust for the possibility of incorrect distributionalassumptions (e.g., multivariate non-normality; Bentler, 1995).
The data were also analyzed using an exploratory factor analysis (maximum likelihood esti-mation with varimax rotation). In contrast to a confirmatory analysis which uses factors (thefour stages in this case) having a predefined relationship with the questionnaire items, anexploratory factor analysis condenses the variance shared among the factors or variables, anddefines the number of factors to be used based solely on mathematical criteria. For this study,we used an exploratory factor analysis to delineate the smallest number of factors that couldaccount for the most variance in the data; therefore, the analysis was not constrained by thefour stages of change, and the manner in which the variables (the questionnaire items) werecombined to form factors was also not controlled by the investigators. We were interested infinding the best-fitting factor structure for the responses we obtained on the questionnaire (isthe four factor or stage model the “best fit” for our data, or for the population of people whostutter?).
It should be noted that while an oblique rotation method (oblimin) was initially used in themaximum likelihood analysis, we decided to report the results from an identical analysis using anorthogonal, or varimax, rotation. This was done so that we could maximize the clarity with whichthe strongest indicators of each factor could be identified. The chi square value obtained fromthe confirmatory analysis was compared to the chi square value obtained from the exploratory(maximum likelihood) analysis to determine the questionnaire structure that best fit the datagathered in this study. Eigen values were compared to Eigen values from a parallel analysis (Horn,1965; Zwick & Velicer, 1986) to determine the number of factors to be used in the exploratoryanalyses. In addition, a comparison of goodness-of-fit chi square values from vested factor models(i.e., 3- and 4-factor models) was performed to help determine the appropriate number of factorsto include.
6. Results
6.1. Confirmatory factor analysis
Table 2 contains the factor loading matrix generated by the confirmatory analysis. As shownin Table 2, 26 of the 32 items on the modified questionnaire were significantly related to theirhypothesized stages (z > 1.96). While the confirmatory analysis verified that the interpretive ques-tionnaire structure we used fit the data, a goodness of fit test indicated that it was not a perfect fit(x2 = 1213.233, d.f. = 458, p < .001; comparative fit index = .872; Satorra-Bentler scaled x2 = 572;d.f. = 458).
Confirmatory analysis results were also used to assess relationships between stages. Accordingto the stages of change model, stages are additive. This implies that stages adjacent to each

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 105
Table 2Confirmatory analysis factor loading matrix (correlations between questionnaire items and stages)
Questionnaire item # Stage of change
Precontemplation Contemplation Action Maintenance
1 .572 .43 .494 .345 .736 .847 .708 .549 .63
10 .2711 .3212 .8613 .4214 .7815 .6916 .4117 .3418 .27a
19 .4320 .6421 .7422 .7123 −.14a
24 .7825 .7026 .3427 .13a
28 .5229 .20a
30 .6731 .21a
32 .10a
Note: Correlations not reported were fixed to 0.a r values not significant (z < 1.96).
other should be more highly correlated than non-adjacent stages. This pattern was observed forcontemplation and action, and for action and maintenance (Table 3). Exceptions to this can be seenin the unexpected negative correlation between precontemplation (stage 1) and contemplation,and positive correlation between contemplation and maintenance.
6.2. Exploratory factor analysis
Table 4 shows the maximum likelihood factor loading matrix obtained from the exploratoryanalysis, containing the 32 questionnaire items and each of the four factors. Briefly, an exploratoryanalysis using maximum likelihood estimation was performed on the 32 × 32 (number ofquestionnaire items) correlation matrix to assess the extent to which an alternative interpre-tive factor structure would provide a better fit to the data (e.g., the 32 items would remain

106 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
Table 3Correlations between stages
P C A M
P −1.00a −.631 −.954C .628 1.00a
A .531
P: precontemplation; C: contemplation; A: action; M: maintenance.a Correlations set at boundaries by software during iterative model fit process. Statistical significance cannot be
estimated.
Table 4Exploratory analysis factor loading matrix (correlations between questionnaire items and factors)
Questionnaire item # Factors
1 2 3 4
1 −.33 −.18 −.11 −.662 .42 .09 −.04 .143 .13 .20 .45 .384 .09 .65 .17 .205 −.83 −.32 .12 .236 .16 .81 .06 .507 .70 .01 .24 .218 .83 .08 .28 .059 .23 .52 −.12 .17
10 .22 −.09 .54 .4311 −.18 −.61 −.19 .0512 .71 .59 −.08 .0513 −.07 −.52 −.15 −.1614 .66 .27 .56 −.1915 .70 .27 .21 .0216 .09 .37 −.15 .1917 .09 .12 .51 −.0118 .09 .11 .06 .3419 .07 .26 −.22 .7320 .74 .31 .02 .1121 .83 .35 −.22 .0722 .33 .56 −.15 .4323 .05 .16 −.54 −.0224 .61 .65 −.08 .1425 .27 .63 .48 −.4626 −.24 −.32 −.22 −.3727 −.17 .39 .39 .3928 .24 .52 −.08 .0629 −.20 .08 −.08 −.0330 .27 .04 .82 −.0831 −.34 −.06 −.08 −.1032 −.23 .43 .36 .09
J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 107
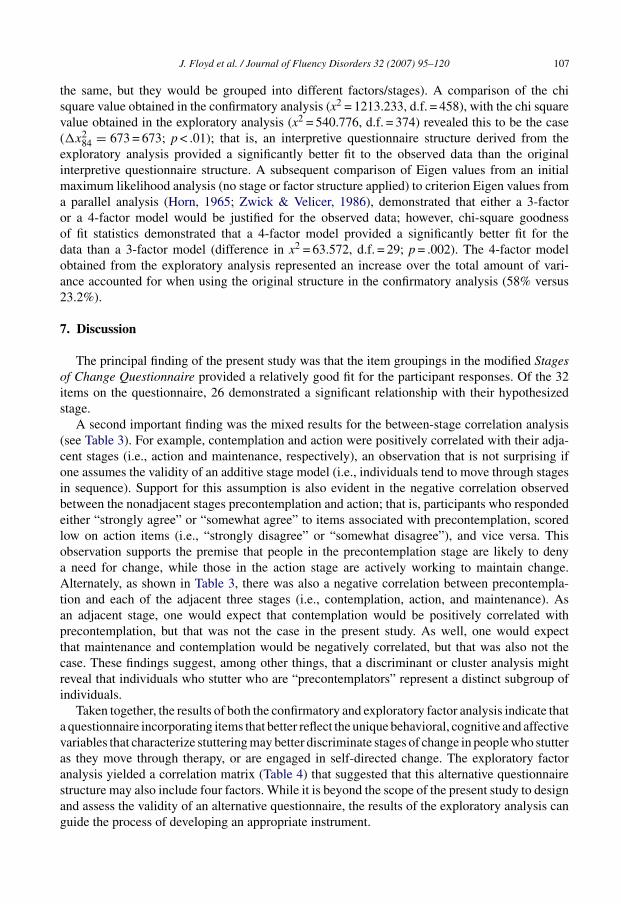
the same, but they would be grouped into different factors/stages). A comparison of the chisquare value obtained in the confirmatory analysis (x2 = 1213.233, d.f. = 458), with the chi squarevalue obtained in the exploratory analysis (x2 = 540.776, d.f. = 374) revealed this to be the case(�x2
84 = 673 = 673; p < .01); that is, an interpretive questionnaire structure derived from theexploratory analysis provided a significantly better fit to the observed data than the originalinterpretive questionnaire structure. A subsequent comparison of Eigen values from an initialmaximum likelihood analysis (no stage or factor structure applied) to criterion Eigen values froma parallel analysis (Horn, 1965; Zwick & Velicer, 1986), demonstrated that either a 3-factoror a 4-factor model would be justified for the observed data; however, chi-square goodnessof fit statistics demonstrated that a 4-factor model provided a significantly better fit for thedata than a 3-factor model (difference in x2 = 63.572, d.f. = 29; p = .002). The 4-factor modelobtained from the exploratory analysis represented an increase over the total amount of vari-ance accounted for when using the original structure in the confirmatory analysis (58% versus23.2%).
7. Discussion
The principal finding of the present study was that the item groupings in the modified Stagesof Change Questionnaire provided a relatively good fit for the participant responses. Of the 32items on the questionnaire, 26 demonstrated a significant relationship with their hypothesizedstage.
A second important finding was the mixed results for the between-stage correlation analysis(see Table 3). For example, contemplation and action were positively correlated with their adja-cent stages (i.e., action and maintenance, respectively), an observation that is not surprising ifone assumes the validity of an additive stage model (i.e., individuals tend to move through stagesin sequence). Support for this assumption is also evident in the negative correlation observedbetween the nonadjacent stages precontemplation and action; that is, participants who respondedeither “strongly agree” or “somewhat agree” to items associated with precontemplation, scoredlow on action items (i.e., “strongly disagree” or “somewhat disagree”), and vice versa. Thisobservation supports the premise that people in the precontemplation stage are likely to denya need for change, while those in the action stage are actively working to maintain change.Alternately, as shown in Table 3, there was also a negative correlation between precontempla-tion and each of the adjacent three stages (i.e., contemplation, action, and maintenance). Asan adjacent stage, one would expect that contemplation would be positively correlated withprecontemplation, but that was not the case in the present study. As well, one would expectthat maintenance and contemplation would be negatively correlated, but that was also not thecase. These findings suggest, among other things, that a discriminant or cluster analysis mightreveal that individuals who stutter who are “precontemplators” represent a distinct subgroup ofindividuals.
Taken together, the results of both the confirmatory and exploratory factor analysis indicate thata questionnaire incorporating items that better reflect the unique behavioral, cognitive and affectivevariables that characterize stuttering may better discriminate stages of change in people who stutteras they move through therapy, or are engaged in self-directed change. The exploratory factoranalysis yielded a correlation matrix (Table 4) that suggested that this alternative questionnairestructure may also include four factors. While it is beyond the scope of the present study to designand assess the validity of an alternative questionnaire, the results of the exploratory analysis canguide the process of developing an appropriate instrument.

108 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
7.1. Development of an alternative questionnaire structure
A reasonable place to start the process of alternative questionnaire development is to obtaindata from additional subjects in order to validate the current factor loadings from the exploratoryanalysis. Next, factor patterns derived from the maximum likelihood correlation matrix presentedin Table 4 should be examined. First, as shown in Table 4, there is a wide range of item loadingsfor each of the four factors (e.g., .050 (item 23) to .83 (item 8) for factor #1; .01 (item 7) to .81(item 6) for factor #2, and so on). Second, if we use r > .40 as a conservative cutoff value, wesee that of the 32 questionnaire items, 22 were correlated with a single factor. The remainingten items were either correlated with more than one factor (e.g., item 27), or were not correlatedwith any of the four factors (e.g., item 18). The reason that some items were not loaded ona single factor is unknown, but a likely explanation is that there is overlap between factors.Alternately, items that did not correlate with any of the factors suggest that there may be additionalfactors that are not adequately represented by the existing questionnaire items. It may also bethe case that these items are not representative of any salient factor and should be eliminated.Given the relatively small sample size, however, it does not seem reasonable to eliminate anyitems without additional data. Although the general structure of the factor analytic solutionspresented here can be considered reasonably stable (e.g., MacCallum, Widaman, Zhang, & Hong,1999), the confidence intervals surrounding factor loadings are quite broad and would likelylead one to discard good indicators of a factor and/or include poor indicators of a factor due tochance.
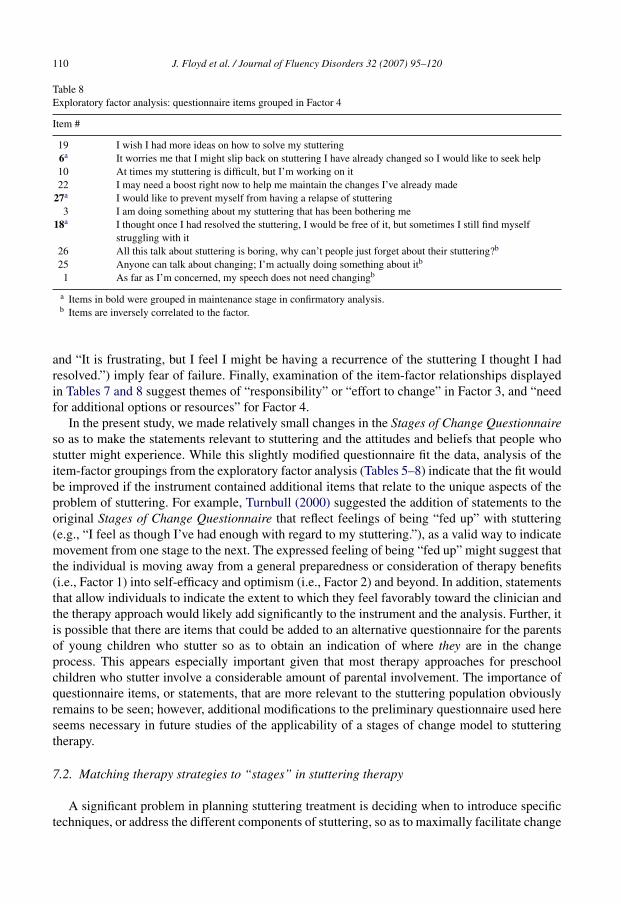
The items correlated with each factor should also be examined as a group, to determine theextent to which they suggest specific themes that may characterize different but related ‘stages’within a process of change related to stuttering. Tables 5–8 present the item-factor groupingsas determined by the results of the exploratory factor analysis presented in Table 4. Of noteis that the items in bold were also loaded on similar or “mirror” factors (i.e. stages) in theconfirmatory analysis. For example, item 1 was loaded on Factor 1 in the exploratory analysis,and precontemplation in the confirmatory analysis.
Table 5Exploratory factor analysis: questionnaire items grouped in Factor 1
Item #
8 I’ve been thinking that I might want to change something about my speech21 Maybe speech therapy will be able to help me20 I have started working on my stuttering but I would like help12 I’m hoping speech therapy will help me to better understand my stuttering
7 I am finally doing some work on my stuttering15 I have a problem and I really think I should work on it14 I am really working hard to change24 I hope that speech therapy will have some good advice for me
2 I think I might be ready to improve my speech22 I may need a boost right now to help me maintain the changes I’ve already made1a As far as I’m concerned, my speech does not need changingb
31a I would rather cope with my stuttering than try to change itb
5a I don’t have a problem with stuttering, It doesn’t make sense for me to be in therapyb
a Items in bold were grouped in precontemplation stage in confirmatory analysis.b Items are inversely correlated to the factor.
J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 109
Table 6Exploratory factor analysis: questionnaire items grouped in Factor 2
Item #
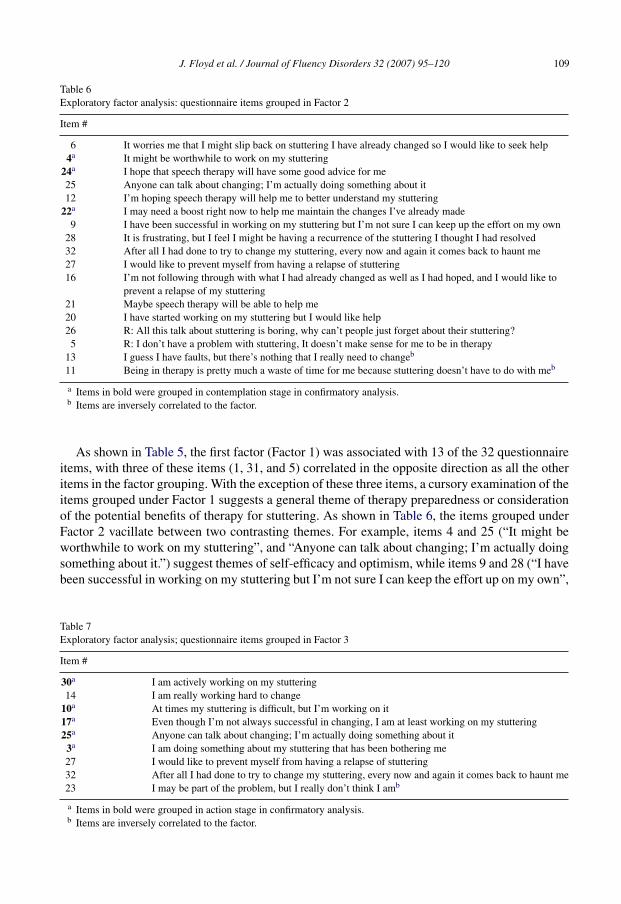
6 It worries me that I might slip back on stuttering I have already changed so I would like to seek help4a It might be worthwhile to work on my stuttering
24a I hope that speech therapy will have some good advice for me25 Anyone can talk about changing; I’m actually doing something about it12 I’m hoping speech therapy will help me to better understand my stuttering
22a I may need a boost right now to help me maintain the changes I’ve already made9 I have been successful in working on my stuttering but I’m not sure I can keep up the effort on my own
28 It is frustrating, but I feel I might be having a recurrence of the stuttering I thought I had resolved32 After all I had done to try to change my stuttering, every now and again it comes back to haunt me27 I would like to prevent myself from having a relapse of stuttering16 I’m not following through with what I had already changed as well as I had hoped, and I would like to
prevent a relapse of my stuttering21 Maybe speech therapy will be able to help me20 I have started working on my stuttering but I would like help26 R: All this talk about stuttering is boring, why can’t people just forget about their stuttering?
5 R: I don’t have a problem with stuttering, It doesn’t make sense for me to be in therapy13 I guess I have faults, but there’s nothing that I really need to changeb
11 Being in therapy is pretty much a waste of time for me because stuttering doesn’t have to do with meb
a Items in bold were grouped in contemplation stage in confirmatory analysis.b Items are inversely correlated to the factor.
As shown in Table 5, the first factor (Factor 1) was associated with 13 of the 32 questionnaireitems, with three of these items (1, 31, and 5) correlated in the opposite direction as all the otheritems in the factor grouping. With the exception of these three items, a cursory examination of theitems grouped under Factor 1 suggests a general theme of therapy preparedness or considerationof the potential benefits of therapy for stuttering. As shown in Table 6, the items grouped underFactor 2 vacillate between two contrasting themes. For example, items 4 and 25 (“It might beworthwhile to work on my stuttering”, and “Anyone can talk about changing; I’m actually doingsomething about it.”) suggest themes of self-efficacy and optimism, while items 9 and 28 (“I havebeen successful in working on my stuttering but I’m not sure I can keep the effort up on my own”,
Table 7Exploratory factor analysis; questionnaire items grouped in Factor 3
Item #
30a I am actively working on my stuttering14 I am really working hard to change
10a At times my stuttering is difficult, but I’m working on it17a Even though I’m not always successful in changing, I am at least working on my stuttering25a Anyone can talk about changing; I’m actually doing something about it
3a I am doing something about my stuttering that has been bothering me27 I would like to prevent myself from having a relapse of stuttering32 After all I had done to try to change my stuttering, every now and again it comes back to haunt me23 I may be part of the problem, but I really don’t think I amb
a Items in bold were grouped in action stage in confirmatory analysis.b Items are inversely correlated to the factor.
110 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
Table 8Exploratory factor analysis: questionnaire items grouped in Factor 4
Item #
19 I wish I had more ideas on how to solve my stuttering6a It worries me that I might slip back on stuttering I have already changed so I would like to seek help10 At times my stuttering is difficult, but I’m working on it22 I may need a boost right now to help me maintain the changes I’ve already made
27a I would like to prevent myself from having a relapse of stuttering3 I am doing something about my stuttering that has been bothering me
18a I thought once I had resolved the stuttering, I would be free of it, but sometimes I still find myselfstruggling with it
26 All this talk about stuttering is boring, why can’t people just forget about their stuttering?b
25 Anyone can talk about changing; I’m actually doing something about itb
1 As far as I’m concerned, my speech does not need changingb
a Items in bold were grouped in maintenance stage in confirmatory analysis.b Items are inversely correlated to the factor.
and “It is frustrating, but I feel I might be having a recurrence of the stuttering I thought I hadresolved.”) imply fear of failure. Finally, examination of the item-factor relationships displayedin Tables 7 and 8 suggest themes of “responsibility” or “effort to change” in Factor 3, and “needfor additional options or resources” for Factor 4.
In the present study, we made relatively small changes in the Stages of Change Questionnaireso as to make the statements relevant to stuttering and the attitudes and beliefs that people whostutter might experience. While this slightly modified questionnaire fit the data, analysis of theitem-factor groupings from the exploratory factor analysis (Tables 5–8) indicate that the fit wouldbe improved if the instrument contained additional items that relate to the unique aspects of theproblem of stuttering. For example, Turnbull (2000) suggested the addition of statements to theoriginal Stages of Change Questionnaire that reflect feelings of being “fed up” with stuttering(e.g., “I feel as though I’ve had enough with regard to my stuttering.”), as a valid way to indicatemovement from one stage to the next. The expressed feeling of being “fed up” might suggest thatthe individual is moving away from a general preparedness or consideration of therapy benefits(i.e., Factor 1) into self-efficacy and optimism (i.e., Factor 2) and beyond. In addition, statementsthat allow individuals to indicate the extent to which they feel favorably toward the clinician andthe therapy approach would likely add significantly to the instrument and the analysis. Further, itis possible that there are items that could be added to an alternative questionnaire for the parentsof young children who stutter so as to obtain an indication of where they are in the changeprocess. This appears especially important given that most therapy approaches for preschoolchildren who stutter involve a considerable amount of parental involvement. The importance ofquestionnaire items, or statements, that are more relevant to the stuttering population obviouslyremains to be seen; however, additional modifications to the preliminary questionnaire used hereseems necessary in future studies of the applicability of a stages of change model to stutteringtherapy.
7.2. Matching therapy strategies to “stages” in stuttering therapy
A significant problem in planning stuttering treatment is deciding when to introduce specifictechniques, or address the different components of stuttering, so as to maximally facilitate change

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 111
and a positive outcome. Results from the present study provide support for Turnbull’s (2000) sug-gestion that the stages of change model can provide guidelines for delineating specific strategiesor techniques that would help individuals move successfully through different stages of stutteringtherapy. While the treatment strategies or techniques conventionally used in stuttering therapydiffer from the processes used in psychotherapy and other treatment approaches used for addic-tive or socially unacceptable behaviors, they appear similar to most of the processes first definedby Prochaska and DiClemente (1986). Similar to the processes shown in Table 1, well-establishedtechniques used in stuttering intervention differentially address experiences (thoughts and emo-tions), and behaviors (speech; e.g., Healey, Trautman & Susca, 2004; Shapiro, 1999). For example,strategies that address thoughts and feelings include examining attitudes about talking and stut-tering (e.g., assessing how one feels and thinks about oneself with respect to a problem: valueclarification, corrective emotional experience, or precontemplation; see Table 1), desensitization,and self-disclosure.
Perz, DiClemente and Carbonari (1996), describing the processes related to successful cessa-tion from smoking, discovered that it was more appropriate to use experiential processes duringparticular stages of change, and behavioral processes during others. Experiential processes addressaffective and cognitive components, whereas behavioral processes are ones that teach the specificbehaviors necessary for change to come about. Examples of experiential processes are conscious-ness raising, self re-evaluation, and self and social liberation (see Table 1). Perz et al. (1996)found that it was more beneficial to treatment progress if clients in the precontemplation and con-templation stages used the experiential processes of consciousness-raising and self re-evaluation.On the other hand, individuals in the action stage benefited more from such behavioral processesas counter conditioning and stimulus control. Using processes at the “right” time were shown tofacilitate movement from one stage to another.
The work of Perz et al. (1996) and Turnbull (2000) provide direction for matching stut-tering therapy techniques or tools to “where” a person who stutters might be in the changeprocess. For example, if it is determined that a person who stutters is in the “thinking abouttherapy” stage, he or she would likely benefit from “bibliotherapy”, or reading information per-taining to talking and stuttering. This is an experiential activity that serves as a mechanismfor raising consciousness. Such experiential processes could also be used by those who arepreparing for therapy, or those who are considering the potential benefits of therapy. These indi-viduals are likely to benefit from activities such as exploring the implications of change, andweighing the advantages and disadvantages of both staying the same and of changing (self re-evaluation).
For those who are making an active effort to change, Turnbull again borrows from the pro-cesses believed to support movement through action to maintenance. For example, individualswho stutter, who are actively involved in the change process would be primed, or ready to engagein the use of techniques or strategies for changing speech behaviors (i.e., strategies specific toeither fluency shaping or stuttering modification; “substituting alternatives for problem behaviors”(see Table 1). In addition, in this “action” stage, strategies to facilitate thoughts and feelings thatpromote change would be important, and include, among other things, relaxation and assertive-ness training, desensitization work, and enlisting others to provide support and encouragement,such as one receives from support groups or self-help organizations. These are all commonlyused strategies in therapy for stuttering. Looking at self-help organizations from a different per-spective, however, it might be the case that participation in a support group, while intuitivelyhelpful, has the opposite effect on those people who believe that there is no problem, or thattherapy or change is not presently needed. For these individuals, attending a support group may

112 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
be a confrontational or intimidating experience in that they do not share (or see) common expe-riences with other group members. In these cases, the individual likely has nothing to shareand may come away frustrated and “turned-off” to stuttering intervention of any kind. Finally,Turnbull suggests that individuals in the “maintenance” stage of change, or who are lookingfor additional options for change that extend beyond therapy, need to develop a “tool box” ofstrategies to help maintain change. Using the processes associated with the “maintenance” stageof change (see Table 1), this “tool box” might include the expansion of support networks, self-advocacy, rewarding oneself for making changes, and consideration of relapse with an openmind.
7.3. Limitations of the present study
As previously discussed, the most obvious limitation of the present study is the relativelysmall number of participants, especially given the nature of factor analysis. Undoubtedly futureresearch should attempt to collect additional data from a larger number of subjects. While somestatisticians suggest a minimum of 5–15 participants per variable to increase the reliability offactor analyses, others have disagreed that this is necessary. For example, MacCallum et al.(1999) and others have argued that subject to item ratio is not necessarily a valid indicator ofthe reliability of an individual factor analytic solution. In their Monte Carlo study, MacCallum etal. observed that the congruence of a factor analytic solution from a sample to a population wasa complex function of sample size, communalities (i.e., the sum of squared factor loadings fora variable), and factor overdetermination (i.e., the number of items serving as indicators of thefactor). Among these three, communalities were the most important. Using this observation, theresults of the present study have wide communalities (mean: .52; 5th to 95th %ile; range: .13–.88),and high factor overdetermination (with eight items per factor, compared with 6.66 items perfactor in McCallum et al.’s study). With the present sample size of 44, we expect that the resultsof the exploratory factor analysis would therefore have high congruence (>.8) with populationvalues.
Besides sample size, another potential limitation of this study is the population from whichparticipants were drawn, and the extent to which this may have influenced the results ofthe analysis, particularly the confirmatory factor analysis. Recall that the confirmatory anal-ysis yielded relatively strong correlations between the maintenance stage and the other threestages (precontemplation, contemplation and action). This correlation pattern was unexpected,as typically, nonadjacent stages (e.g., maintenance and precontemplation, or maintenance andcontemplation) are not correlated. In the present study, subjects were recruited from eitherspeech-language pathologists or self-help organizations (i.e., NSA), and all reported a historyof stuttering therapy (as might be expected from their association with so-called gatekeepers).For this reason it is safe to say that a disproportionate number of subjects may be represen-tative of either action or maintenance stages of change, and such unequal distribution acrossstages may make it unreasonable to expect sphericity (i.e., higher correlations between adja-cent stages) in the confirmatory factor analysis. We cannot know if this is the case basedon one data set, but this possibility can be ruled out in future research by comparing thefactor inter-correlation matrices from separate confirmatory factor analyses, one of which isobtained from subjects who are “therapy graduates” and one from subjects who have neverhad formal stuttering therapy (or have not been enrolled in therapy for an extended period oftime).

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 113
Appendix A. Modified “Stages of Change” Questionnaire (after McConnaughy et al.,1983)
114 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 115
116 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 117

118 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
CONTINUING EDUCATION
Stages of change and stuttering: A preliminary view
QUESTIONS
1. The underlying premise of the “stages of change” or “transtheoretical model” isa. that there are various components to stuttering treatmentb. that there are commonalities across treatment approaches in the processes people use to
change their behaviorc. that change is inevitabled. that some treatment approaches are better than otherse. that change processes are only seen in nonaddictive behaviors
2. The “stages of change” can be seen ina. individuals enrolled in treatment programsb. so-called “self-changers”c. both individuals enrolled in therapy, and self-changersd. primarily femalese. primarily males
3. In general, movement through the “stages of change” isa. linearb. nonadjacentc. uncorrelatedd. spirale. random
4. Results from the present study suggest thata. the stages of change are not validb. adjacent stages of change are not correlatedc. change can be predicted by stuttering severityd. measurements of stuttering are not reliablee. a modified Stages of Change Questionnaire structure provides a relatively good fit to the
responses obtained from people who stutter5. “Self-liberation” is a
a. level of changeb. confounding element to changec. degree of changed. way to describe people who stutter who make progress in therapye. process of change
References
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhl & J. Beckman (Eds.), Action control:From cognition to behaviour (pp. 11–39). New York: Springer-Verlag.
Armitage, C. J. (2006). Evidence that implementation intentions promote transitions between the stages of change. Journalof Consulting and Clinical Psychology, 74, 141–151.
Bentler, P. M. (1995). EQS Structural Equations Program Manual. Encino, CA: Multivariate Software, Inc.

J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120 119
Blanchard, K., Morgenstern, J., Morgan, T., Labouvie, E., & Bux, D. (2003). Motivational subtypes and continu-ous measures of readiness for change: Concurrent and predictive validity. Psychology of Addictive Behaviors, 17,56–65.
Blood, G. W. (1993). Treatment efficacy in adults who stutter: Review and recommendations. Journal of Fluency Disorders,18, 303–318.
Brownell, K., Marlatt, G., Lichtenstein, E., & Wilson, T. (1986). Understanding and preventing relapse. AmericanPsychologist, 41(7), 765–782.
Carey, K., Purnine, D., Maisto, S., & Carey, M. (1999). Assessing readiness to change substance abuse: A critical reviewof instruments. Clinical Psychology: Science and Practice, 6, 245–266.
Craig, A. (1998). Relapse following treatment for stuttering: A critical review and correlative data. Journal of FluencyDisorders, 23, 1–30.
DiClemente, C. C. (1993). Changing addictive behaviors: A process perspective. Current directions in PsychologicalScience, 29(4), 101–106.
DiClemente, C., & Hughes, S. (1990). Stages of change profiles in outpatient alcoholism treatment. Journal of SubstanceAbuse, 2, 217–235.
Guitar, B. (1976). Pretreatment factors associated with the outcome of stuttering therapy. Journal of speech and hearingResearch, 19, 590–600.
Guitar, B. (1998). Stuttering: An integrated approach to its nature and treatment (2nd ed.). Baltimore: Williams &Williams.
Guitar, B., & Bass, C. (1978). Stuttering therapy: The relation between attitude change and long-term outcome. Journalof Speech and Hearing Disorders, 43, 392–400.
Healey, E. C., Trautman, L. S., & Susca, M. (2004). Clinical applications of a multidimensional approach for the assessmentand treatment of stuttering. Contemporary Issues in Communication Science and Disorders, 31, 40–48.
Horn, J. L. (1965). A rationale and test for the number of factors in factor analysis. Psychometrika, 30, 179–185.Huinck, W. J., Langevin, M., Kully, D., Graamans, K., Peters, H. F. M., & Hulstijn, W. (2006). The relationship between
pre-treatment clinical profile and treatment outcome in an integrated stuttering program. Journal of Fluency Disorders,31(1), 43–63.
MacCallum, R. C., Widaman, K. F., Zhang, S., & Hong, S. (1999). Sample size in factor analysis. Psychological Methods,4, 84–99.
Manning, W. H. (2001). Clinical decision making in fluency disorders (2nd ed.). Vancouver, Canada: Singular.Manning, W. H. (2006). Therapeutic change and the nature of our evidence: Improving our ability to help. In N. Bernstein
Ratner & J. A. Tetnowski (Eds.), Current issues in stuttering research and practice. Mahwah, NJ: Lawrence ErlbaumAssoc.
Marcus, B. H., & Simkin, L. R. (1994). The transtheoretical model: Applications to exercise behavior. Medicine andScience in Sports and Exercise, 26(11), 1400–1404.
McConnaughy, E. A., Prochaska, J. O., & Velicer, W. F. (1983). Stages of change in psychotherapy: Measurement andsample profiles. Psychotherapy: Theory, Research, and Practice, 20(3), 368–375.
Pallonen, E., Leskinen, L., Prochaska, J. O., Willey, J., Kaariainen, R., & Salonen, J. T. (1994). Self-help smoking cessa-tion manual intervention among middle-aged Finnish men: An application of the transtheoretical model. PreventiveMedicine, 23(4), 507–514.
Pantalon, M., Nich, C., Frankforter, T., & Carroll, K. (2002). The URICA as a measure of motivation to change amongtreatment-seeking individuals with concurrent alcohol and cocaine problems. Psychology of Addictive Behaviors,16(4), 299–307.
Pantalon, M., & Swanson, A. (2003). Use of the Rhode Island Change Assessment to measure motivational readiness tochange in psychiatric and dually diagnosed individuals. Psychology of Addictive Behaviors, 17(2), 91–97.
Perz, C. A., DiClemente, C. C., & Carbonari, J. P. (1996). Doing the right thing at the right time? The interaction of stagesand processes of change in successful smoking cessation. Health Psychology, 15(6), 462–468.
Prochaska, J. O. (1999). How do people change and how can we change to help many more people? In M. A. Hubble, B.L. Duncan, & S. D. Miller (Eds.), The heart & soul of change: What works in therapy (pp. 227–255). Washington,D.C.: American Psychological Association.
Prochaska, J. O., & DiClemente, C. C. (1984). The transtheoretical approach: Crossing traditional boundaries of therapy.Homewood, IL: Dow Jones-Irwin.
Prochaska, J. O., & DiClemente, C. C. (1986). The transtheoretical approach. In J. C. Norcross (Ed.), Handbook of eclecticpsychotherapy. New York: Brunner/Mazel.
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how people change: Applications to addictivebehaviors. American Psychologist, 47(9), 1102–1114.

120 J. Floyd et al. / Journal of Fluency Disorders 32 (2007) 95–120
Prochaska, J. O., Velicar, W. F., Rossi, J. S., Goldstein, M. G., Marcus, B. H., Rakowski, W., et al. (1994). Stages ofchange and decisional balance for 12 problem behaviors. Health Psychology, 13(1), 39–46.
Ruggiero, L. (1998). Transtheoretical model: Applications in the prevention and treatment of cancer. Medical and PediatricOncology supplement, 1(69), 74.
Sarafino, E. (2006). Health Psychology:Biopsychosocial Interactions. Hoboken, NJ: Wiley & Sons, Inc.Shapiro, D. A. (1999). Stuttering intervention: A collaborative journey to fluency freedom. Austin: TX: Pro-Ed.Suris, A. M., Carmen Trapp, M., DiClemente, C. C., & Cousins, J. (1998). Application of the transtheoretical model of
behavior change for obesity in Mexican-American women. Addictive Behaviors, 23(5), 655–668.Turnbull, J. (2000). The transtheoretical model of change: Examples from stuttering. Counseling Psychology Quarterly,
31(1), 13–21.Zebrowski, P. M., & Conture, E. G. (1998). Influence of nontreatment variables on treatment effectiveness for school-age
children who stutter. In A. K. Cordes & R. J. Ingham (Eds.), Treatment efficacy for stuttering: A search for empiricalbases (pp. 293–310). San Diego, CA: Singular Publishing Group, Inc.
Zwick, W. R., & Velicer, W. F. (1986). Comparison of five rules for determining the number of components to retain.Psychological Bulletin, 99(3), 432–442.
Jennifer Floyd graduated from the University of Colorado at Boulder with majors in Psychology and Biology. Sheattained her MA in speech-language pathology from the University of Iowa in 2001. Since then, Jennifer has worked inthe elementary school system in Illinois, and is currently in private practice in Colorado.
Patricia M. Zebrowski is an associate professor in Speech Pathology and Audiology at the University of Iowa. She isa Fellow of the American Speech-Language and Hearing Association, and a Board Recognized Fluency Specialist. Herinterests are in the area of stuttering, with specific emphasis on children who stutter.
Gregory A. Flamme is an assistant professor in Speech Pathology and Audiology at Western Michigan University. Heearned a PhD in Audiology (University of Memphis) and completed postdoctoral studies in Epidemiology and Biostatistics(University of Iowa). His research focuses on hearing loss prevention and treatment.


















