Stacy C. Zimmerman MD FACP FAAP - Internal Medicine · PDF file... have discussed the...
55
“A PCMH Model” Stacy C. Zimmerman MD FACP FAAP
Transcript of Stacy C. Zimmerman MD FACP FAAP - Internal Medicine · PDF file... have discussed the...

“A PCMH Model”
Stacy C. Zimmerman MD FACP FAAP

AFMC board of directors
CMS Technical expert panel 2016-2017

Importance of practice transformation
Outline basis of Population Management
Outline Patient Centered Medical Home (PCMH)
Basic practice transformation activities
Align measures and activities for the PCMH programs
Practice and patient outcomes


Smarter
Spending
Healthier
People
Better
Care

Quadruple
Aim
Better Care
Smarter
Spending
Healthier
People
Physician
Satisfaction



Van Buren County Courthouse



Red River Family Medicine
Location: Clinton, AR Providers: 2 Empanelment: 3370 EHR: eMDs Contact Info: Stacy Zimmerman, MD [email protected]



Assets to assist in physician recruitment and retention for the small practice.
Employee recruitment and retention, options for temporary staffing??
Practical care management options for the small practice to replace the expensive cost(s) of the patient care coordinator.
Incentives to develop specialist care coordination agreements for seamless exchange of patient information.
Innovative practice efficiency and patient care strategies / techniques that do not increase physician workload.
Vendors to support EMR’s with affordable seamless population management and data exchange functions.
IT support systems to combine provider/payer data for multiple initiatives
Development of an Arkansas Practice registry for the small to large practice. (For practices to access information for collaboration with state and federal initiatives).
Competition barriers between practices

The Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) is a bipartisan legislation signed into law on April 16, 2015. ◦ What does Title I of MACRA do?
Repeals the Sustainable Growth Rate (SGR) Formula
Changes the way that Medicare rewards clinicians for value over volume
Streamlines multiple quality programs under the new Merit-Based Incentive Payments System (MIPS)
Provides bonus payments for participation in eligible alternative payment models (APMs)

MIPS changes how Medicare links performance to payment :
MACRA streamlines those programs into MIPS: (Merit-Based
Incentive Payment System (MIPS)
Value-Based Payment Modifier Medicare EHR Incentive Programs: CPC Plus
ACO’s and qualifying private payer incentive programs Physician Quality Reporting Program (PQRS)
These quality and value programs for physicians and practitioners are known as Alternative Payment Models (APM).
Medicaid Value-Based Incentive Programs:
Arkansas Medicaid PCMH

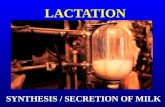
How much can MIPS adjust your Medicare payments? Based on the MIPS composite performance score, physicians and practitioners will receive positive, negative, or neutral adjustments based on the percentages below.
MAXIMUM Adjustments
Adjustment to provider’s base rate of Medicare Part B payment Merit-Based Incentive Payment System (MIPS)
+/- 4% 2019 +/- 5% 2020 +/- 7% 2021 +/- 9% 2022 and onward MIPS composite performance score is based on the following: (Data collection to begin 2017)
Quality Resource use Clinical practice improvement activities Meaningful use of certified EHR technology


Patient access
Care coordination
Care management
Physician champion

Clinical Leader
(physician
champion)
Technical expertise
Day to Day
Leadership Project sponsor
Effective
Team

Patient Family Advisory Counsel PFAC (the value of patient feedback)
Alternative visits or extended office hours, Same day access and 24hr access
Patient Portal
Patient-centered processes Team-based care Population health management Pre and post visit planning Medical neighborhood collaboration
Transition of care protocol for ER and Hospital follow ups Performance measurement and quality improvement

PCMH Practice Transformation Goals
Annual wellness visits Emergency room and Hospital utilization reduction Care management with Care Coordination Decreased pharmacy costs Access to providers and specialists Improvement in Population health outcomes

EMR
Population Risk
Stratification
Model
PCMH

RISK STRATIFICATION MODEL:
Create ICD codes to track your population: RS4 EHR HEALTH MANAGEMENT (this would be the sickest 5% of pts) RS3 HR HEALTH MANAGEMENT (the next 25%) RS2 MR HEALTH MANAGEMENT (the next 30%) RS1 LR HEALTH MANAGEMENT (the remaining 40%)

Reduction in ER Utilization
Providers must educate patients during office visits about proper ED utilization Identify frequent users of the ED with claims data “Gold Pass” card for “frequent fliers” to encourage them to call the clinic BEFORE going to the ER. Posters on appropriate ED use placed in exam rooms.


NCQA PCMH
Medicaid
PCMH
CPC Plus
MU
PQRS



Patient Care
Gap
Team
member
action
EMR tracking
process
triggered
Overdue alerts
Team
member
reconciliation

Red pop up reminders for staff
to address care gaps



Ozark Internal Medicine & Pediatrics: Patient:_______________ PCP: Zimmerman
DOB:_________________ Care Mgr.: Yates LPN I, the patient and care team mgr, have discussed the following care plan
and the patient has received a copy.
_______________________________ _______________________________
Patient signature & date Care Manager signature
Assessment/Nursing DX
Medications associated with Care Plan:
_______________________________________
_______________________________________
_______________________________________
_______________________________________
_______________________________________
___________________________________
_______________________________________
_______________________________________
_______________________________________
_______________________________________
_______________________________________
_______________________________________
_______________________________________
_______________________________________
_________________________________ COPD
Ineffective Airway Clearance
r/t: increased production of secretions, decreased energy & fatigue
AEB: Patient states “I am having difficulty breathing”.
I will work on: Staying active (within level of activity)
Use my oxygen Use my inhalers as prescribed
Attempt to stop Smoking
*Call my PCP at 501-745-3033 or 501-253-8534 (after hours) if any changes in respirations or mentation
Patient Goals
Patient demonstrates behaviors to improve airway clearance, such as; coughs effectively and expectorates secretions, maintains a Sp02 of >90% on a daily basis. First aid and emergency care as needed.
Patient Actions
Increase fluid intake to 2000 ml/day. Keep environmental pollutants to a minimal, including cigarette smoke. Will stay current with pneumonia vaccine.
Expected Outcome
Hydration helps decrease the viscosity of secretions, facilitating expectoration. Precipitators of allergic type of respiratory reactions that can trigger onset of acute episode
This vaccine lowers your risk of pneumococcal pneumonia and its complications. People who have COPD are at higher risk of pneumonia than people who don't have COPD.
Medications associated with Care Plan:
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
**

Front office intake
and update of
patient care
reminders
PATIENT CHECK IN
Nursing
updates
reminders
EXAM ROOM
Provider
reviews
reminders
VISIT





Medicaid Attributed Beneficiaries 844 for 2014
Our 2014 Benchmark TCOC (total cost of care) $1,906
Final TCOC for 2014 was $1,572
Shared savings for 2014 >25K

CPC PCMH initiative $102,108
PCMH medicaid managed PMPM $2,045
Medicaid PCP supplemental payment $55,413
Medicaid PCMH Shared Savings 2014 $26,000
PQRS $497
PCIP (multipayer initiative payments) $5,468







Access and continuity of care: Track 1 with 24/7 patient access and Track 2 e-visits and expanded hours
Care Management: Track 1 risk stratification and Track 2 care plans for high risk patients
Clinical and Community Coordination: Track 1 focus on TOC and Track 2 will add BHS
Patient and caregiver engagement: Track 1 PFAC and Track 2 increase self management of high risk conditions
Planned care and population health: Track 1 analysis of payer reports with process of improvement and Track 2 care team review of population health data

PCMH
success
Check data
frequently to
adapt change to
your practice. Don’t expect
huge
improvements.
Create reliable
workflows.
Use PDSA’s to
drive sustainable
change.
Don’t depend on
“local heroes”.
Make it a team
effort. Allow
customization
provided core
elements to
improvements
are clear.
Team strategic
review of the
scope of the
change .
Team tracking
and monitoring
process.
Sustain gains
with an
infrastructure of
staff to support
them.

PCMH