Stable Ischemic Heart Disease - okpa.org · Aneesh Venkat Pakala, M.D. Assistant Professor,...
69
Stable Ischemic Heart Disease Aneesh Venkat Pakala, M.D. Assistant Professor, Department of Medicine, Cardiovascular diseases section, University of Oklahoma Health Sciences Center.
Transcript of Stable Ischemic Heart Disease - okpa.org · Aneesh Venkat Pakala, M.D. Assistant Professor,...

Stable Ischemic Heart
Disease
Aneesh Venkat Pakala, M.D.
Assistant Professor,
Department of Medicine,
Cardiovascular diseases section,
University of Oklahoma Health Sciences Center.

Objectives
Overview of coronary artery disease
(CAD)
Pathogenesis of atherosclerosis
Risk factors associated with CAD
Stable ischemic heart disease
Definition of CAD
Coronary artery atherosclerosis or
CAD (coronary artery disease) refers
to the presence of atherosclerotic
changes within the walls of the
coronary arteries, which causes
impairment or obstruction of normal
blood flow with resultant myocardial
ischemia.

Epidemiology of CAD
No. 1 cause of death in the US and a
major cause of morbidity.
380,000 deaths in 2010.
Over 1 million MIs per year.
30% of MI patients don’t return to work.
>13 million with coronary artery disease.
10 million with angina pectoris.
25% men over 75 years of age have
CAD.
Cost for Ischemic heart
disease
177.1 Billion dollars in 2010 for
management of ischemic heart disease.
Over 900 million a year spent in outpatient
visits.
Over 200 million a year spent for ER visits.
Over 200 million a year for prescription
drugs for ischemic heart disease.
Over 1 million PCIs and over 400,000 CABG
in 1 year.

Epidemiology continued…
In 2001, prevalence of CHD by gender
& race:
White males: 6.9%
AA males: 7.1%
Hispanic males: 7.2%
White females: 5.4%
AA females: 9.0%
Hispanic females: 6.8%

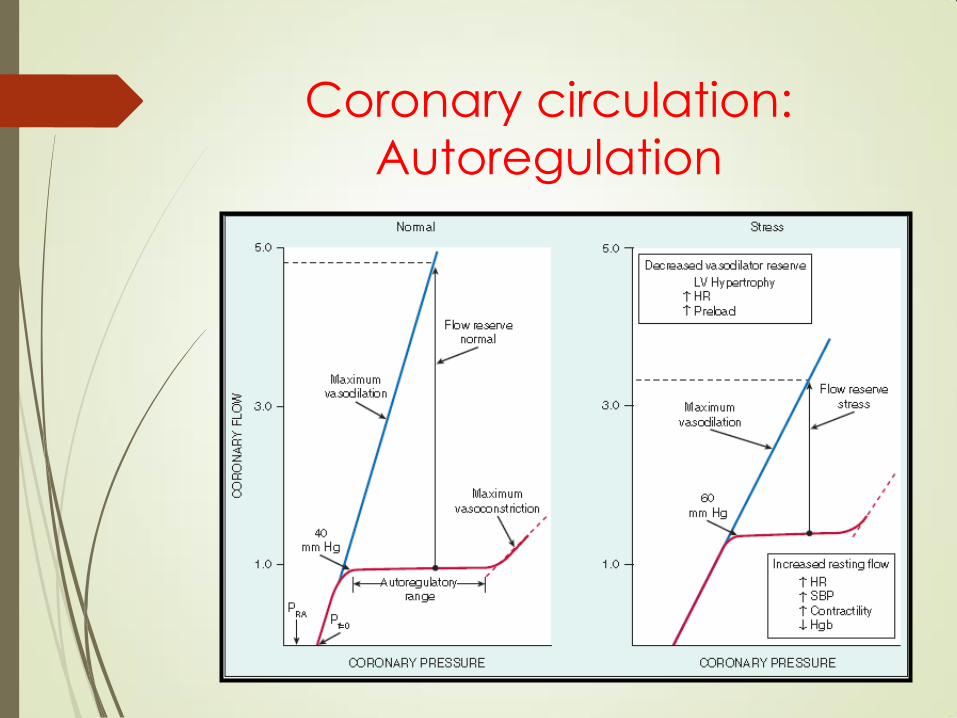
Coronary circulation:
Autoregulation

Coronary circulation: Effect
of stenosis on coronary flow.

Atherosclerosis
“Athero”: wax; sclerosis: hardening
Process in which deposits of fatty
substances, cholesterol, cellular
waste products, calcium, and other
substances build up in the inner
lining of an artery eventually leading
to plaque formation.



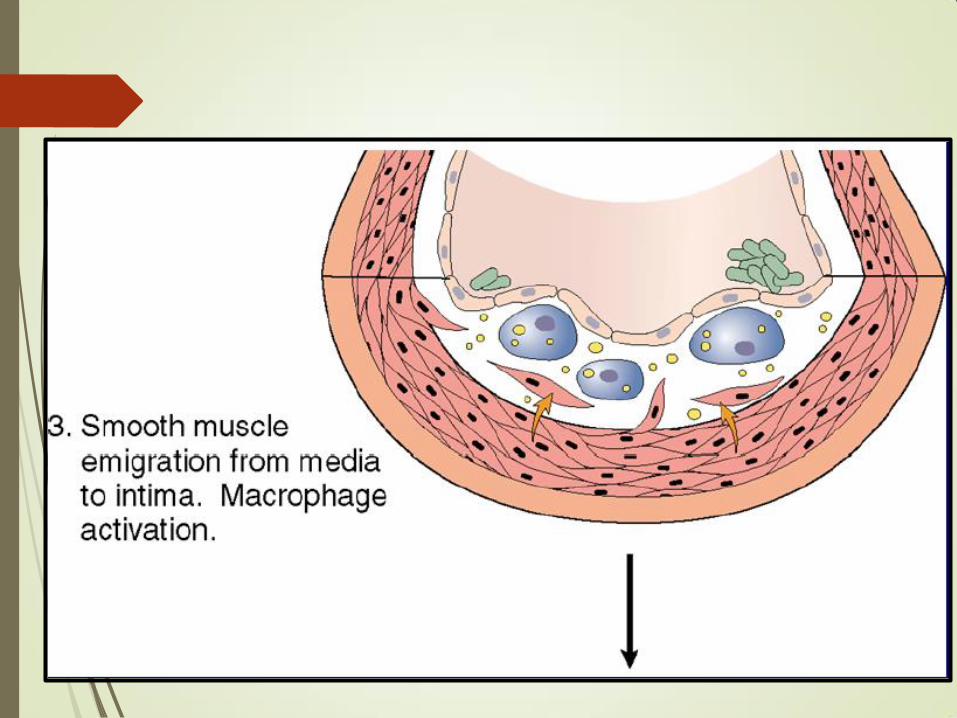

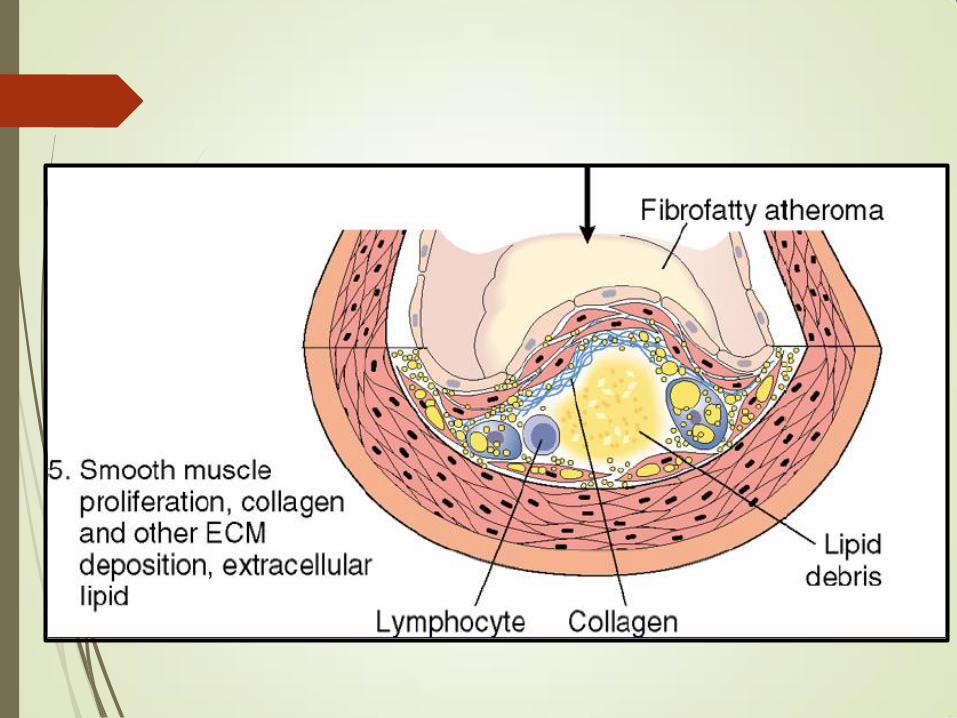

Atherosclerotic plaque




Clinical Manifestations of
CAD
A chronic disorder that typically cycles
in and out of clinically defined phases:
asymptomatic
Stable ischemic heart disease
Acute Coronary Syndrome:
unstable angina, NSTEMI, & STEMI

Stable ischemic heart
disease (SIHD)
Pertains to adults with known or
suspected ischemic heart disease
with stable chest discomfort (angina)
for over 2 months without worsening
frequency, severity or duration.
Definition: Stable Angina
Angina pectoris or angina is the result
of myocardial ischemia caused by an
imbalance between myocardial blood
supply and oxygen demand
STABLE as opposed to UNSTABLE
angina is when the symptoms are
reproducible after a fixed amount of
exertion.

SIHD: Aims of evaluation
Distinguish anginal chest pain due to
gradual worsening of obstructive
coronary artery disease (CAD) from
that due to atherosclerotic plaque
rupture.
Provide risk assessment in patients
with stable ischemic CAD.

Evaluation
Detailed symptom history
Focused physical examination
RISK ASSESSMENT

Evaluation/History: “chest pain”
Quality - "squeezing," "griplike," "pressurelike," "suffocating" and "heavy”; or a "discomfort" but not "pain." Angina is almost never sharp or stabbing, and usually does not change with position or respiration.
Duration - anginal episode is typically minutes in duration. Fleeting discomfort or a dull ache lasting for hours is rarely angina
Location - usually substernal, but radiation to the neck, jaw, epigastrium, or arms is not uncommon. Pain above the mandible, below the epigastrium, or localized to a small area over the left lateral chest wall is rarely anginal.
Provocation - angina is generally precipitated by exertion or emotional stress and commonly relieved by rest. Sublingual nitroglycerin also relieves angina, usually within 30 seconds to several minutes.


Major Risk Factors for CAD
Age
Gender
Family history of premature CAD
Elevated total or LDL cholesterol
Reduced HDL cholesterol
Tobacco use
Hypertension
Diabetes mellitus
Obesity
Sedentary Lifestyle
Metabolic Syndrome

Evaluation: Symptoms/Signs
Chest pain
Dyspnea
Orthopnea
PND (paroxysmal noctural dyspnea)
Dizziness
Diaphoresis
Palpitations
Syncope

Evaluation: Physical Exam
Check vital signs: temperature, BP, HR, RR
For most patients with stable angina, physical examination findings might be normal.
Other signs of atherosclerosis: carotid bruits, decreased/absent peripheral pulses,
Left heart failure: S3/S4, bibasilar rales, displaced apical impulse
Right heart failure: JVD, ascites, hepatomegaly, edema
Auscultate for aortic stenosis.
Pain produced by chest wall pressure is usually of chest wall origin.

Differential Diagnosis of Chest
Pain
Non-Ischemic CV
aortic dissection
pericarditis
Pulmonary
pulmonary embolus
pneumothorax
pneumonia
pleuritis
Chest Wall
costochondritis
fibrositis
rib fracture
sternoclavicular
arthritis
herpes zoster
Gastrointestinal
Esophageal
esophagitis
spasm
reflux
Biliary
colic
cholecystitis
cholangitis
Peptic ulcer
Pancreatitis
Psychiatric
Anxiety disorder
Hyperventilation
panic disorder
primary anxiety
Affective disorders
depression
Diagnosis
CBC (check hemoglobin)
BMP (check glucose, electrolytes, Cr)
Fasting lipid panel
Resting ECG.
Chest x-ray in patients with signs or symptoms of CHF.

Diagnosis: 12 Lead Resting
ECG
Should be recorded in all patients with
symptoms suggestive of angina
pectoris
Normal in 50% of patients with stable
angina
A normal ECG does not exclude
severe CAD


Class 1 (Level of Evidence: B). A
resting ECG is recommended in
patients without an obvious,
noncardiac cause of chest pain.
Electrocardiogram.


Diagnosis: Stress Test
Exercise stress EKG
Exercise or pharmacologic stress with Echocardiogram
Exercise or pharmacologic stress with Myocardial perfusion
imaging.
Exercise stress is the test of
choice if patient can
exercise.
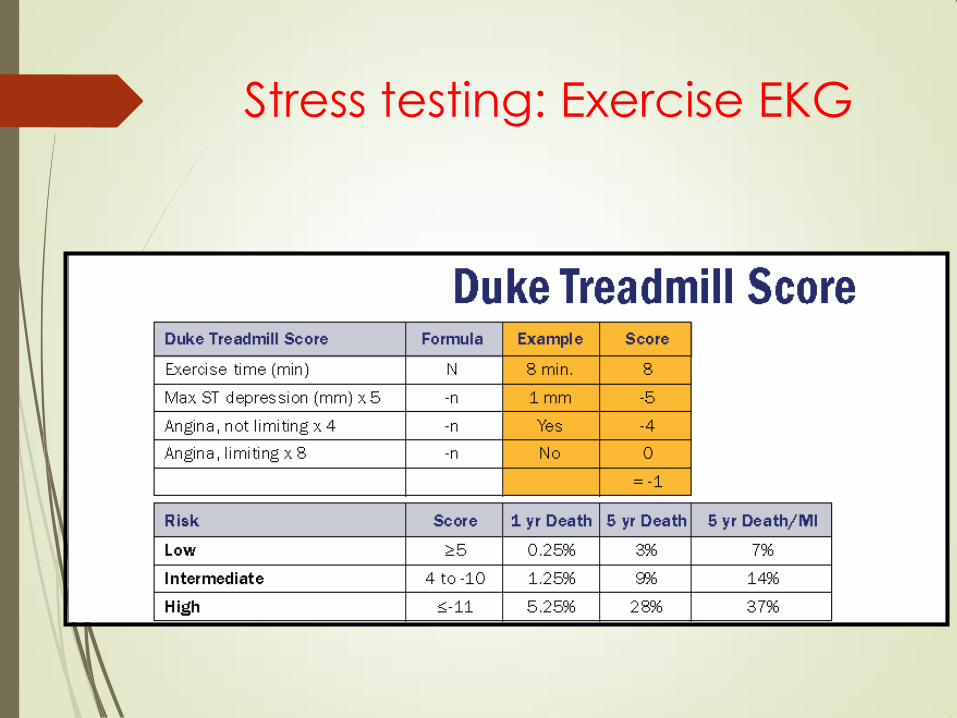
Stress testing: Exercise EKG

Stress testing: Stress imaging.
Stress Imaging

Myocardial Perfusion
Imaging
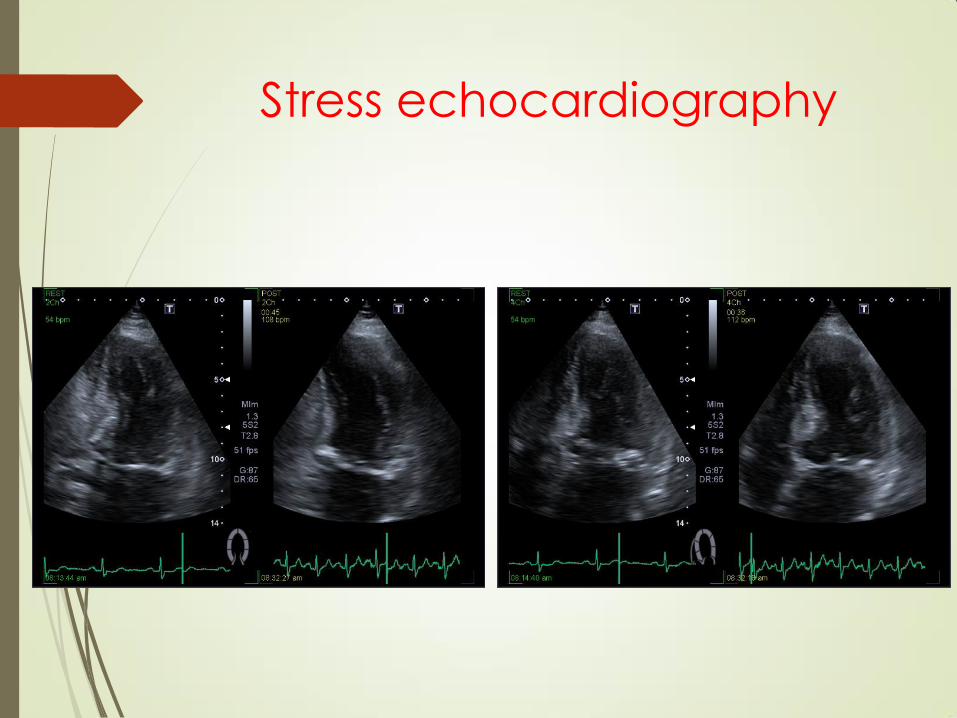
Stress echocardiography

Able to exercise.
Class1 (Level of Evidence: A). Standard exercise
ECG testing is recommended for patients with an
intermediate pretest probability of IHD who have an
interpretable ECG and at least moderate physical
functioning or no disabling comorbidity.
Class 1 (Level of Evidence: B) Exercise stress with
nuclear MPI or echocardiography is recommended for
patients with an intermediate to high pretest probability
of IHD who have an uninterpretable ECG and at least
moderate physical functioning or no disabling
comorbidity .
Stress testing in suspected
SIHD.

Able to exercise.
Class III (Level of Evidence: C). Pharmacological
stress with nuclear MPI, echocardiography, or CMR is
not recommended for patients who have an
interpretable ECG and at least moderate physical
functioning or no disabling comorbidity.
Class III (Level of Evidence: C). Exercise stress with
nuclear MPI is not recommended as an initial test in
low-risk patients who have an interpretable ECG and
at least moderate physical functioning or no disabling
comorbidity.
Stress testing in suspected
SIHD.
Stress testing in suspected
SIHD.
Unable to exercise.
Class I : Pharmacological stress with
nuclear MPI or echocardiography is
recommended for patients with an
intermediate to high pretest probability of
IHD who are incapable of at least
moderate physical functioning or have
disabling comorbidity.
Stress testing in suspected
SIHD.
Unable to exercise.
Class III: Standard exercise ECG testing
is not recommended for patients who
have an uninterpretable ECG or are
incapable of at least moderate physical
functioning or have disabling comorbidity.
(Level of Evidence: C).

Resting imaging to detect
cardiac structure and function
Class 1(Level of Evidence: B).
Assessment of resting LV systolic and
diastolic ventricular function and
evaluation for abnormalities of
myocardium, heart valves, or pericardium
are recommended with the use of
Doppler echocardiography in patients
with known or suspected IHD and a prior
MI, pathological Q waves, symptoms or
signs suggestive of heart failure, complex
ventricular arrhythmias, or an
undiagnosed heart murmur.

Class III (Level of Evidence: C) Echocardiography,
radionuclide imaging, CMR, and cardiac CT are not
recommended for routine assessment of LV function
in patients with a normal ECG, no history of MI, no
symptoms or signs suggestive of heart failure, and no
complex ventricular arrhythmias.
Class III (Level of Evidence: C) Routine reassessment
(1 year) of LV function with technologies such as
echocardiography radionuclide imaging, CMR, or
cardiac CT is not recommended in patients with no
change in clinical status and for whom no change in
therapy is contemplated.
Resting imaging to detect
cardiac structure and function

Diagnosis: Angiography
Depending on stress test results can
either consider medical therapy or
consider sending patient for a
coronary angiography.

Coronary Angiography


Coronary angiography
continued…

To assess risk after non invasive
testing is done:
Class I (Level of Evidence C).
Coronary arteriography is
recommended for patients with
SIHD whose clinical characteristics
and results of noninvasive testing
indicate a high likelihood of
severe IHD and when the benefits
are deemed to exceed risk
Coronary angiography

Class III:
Coronary angiography for risk assessment is not recommended in
patients with SIHD who elect not to undergo revascularization or who
are not candidates for revascularization because of comorbidities
or individual preferences (306,366). (Level of Evidence: B)
Coronary angiography is not recommended to further assess risk in
patients with SIHD who have preserved LV function (EF 50%) and
low-risk criteria on noninvasive testing (306,366). (Level of
Evidence: B)
Coronary angiography is not recommended to assess risk in patient
who are at low risk according to clinical criteria and who have not
undergone noninvasive risk testing. (Level of Evidence: C)
Coronary angiography is not recommended to assess risk in
asymptomatic patients with no evidence of ischemia on noninvasive
testing. (Level of Evidence: C)
Coronary angiography with
known SIHD

Risk assessment
High risk features:
Low EF <35%
High risk Duke treadmill score.
High risk stress imaging features.
High risk stress echocardiographic
features.

CLASS I (Level of Evidence: C)
Choices about diagnostic and
therapeutic options should be made
through a process of shared decision
making involving the patient and
provider, with the provider explaining
information about risks, benefits, and
costs to the patient.
Patient information
Chronic Stable Angina
Treatment Objectives
Reduce the risk of mortality and morbid events
Reduce symptoms
Medical therapy first!!!

Treatment
Class I:
Introduction to self-monitoring skills (Level of
Evidence: C);
Information on how to recognize worsening
cardiovascular symptoms and take appropriate
action. (Level of Evidence: C)
Educated about the following lifestyle elements:
maintenance of a BMI of 18.5 to 24.9 kg/m2, and
waist circumference less than 40 inches in men and
less than 35 inches in women; lipid management; BP
control; smoking cessation and avoidance of
exposure to secondhand smoke(Level of Evidence:
C)

Treatment
Risk factor modification:
Class I:
Lifestyle modifications, including daily physical
activity and weight management, are strongly
recommended for all patients with SIHD. (Level of
Evidence: B)
Dietary therapy for all patients should include
reduced intake of saturated fats (to 7% of total
calories), trans fatty acids (to 1% of total calories),
and cholesterol (to 200 mg/d). (Level of Evidence:
B)

Treatment
Smoking cessation:
Class 1. Smoking cessation and avoidance of
exposure to environmental tobacco smoke at work
and home should be encouraged for all patients with
SIHD. Follow-up, referral to special programs, and
pharmacotherapy are recommended, as is a stepwise
strategy for smoking cessation (Ask, Advise, Assess,
Assist, Arrange, Avoid). (Level of Evidence: B)

Antiplatelet Agents
Aspirin
Aspirin 81mg daily should be used routinely in all
patients with acute and chronic ischemic heart
disease with or without manifest symptoms in the
absence of contraindications
in >3,000 patients with stable angina, aspirin
reduced the risk of adverse cardiovascular
events by 33%
in patients with unstable angina, aspirin
decreases the short and long-term risk of
fatal and nonfatal MI

Statins

Treatment: Medical therapy to relieve symptoms
Class I:
Beta blockers should be prescribed as initial therapy for relief
of symptoms in patients with SIHD (Level of Evidence: B)
Calcium channel blockers or long-acting nitrates should be
prescribed for relief of symptoms when beta blockers are
contraindicated or cause unacceptable side effects in patients
with SIHD (Level of Evidence: B)
Calcium channel blockers or long-acting nitrates, in combination
with beta blockers, should be prescribed for relief of symptoms
when initial treatment with beta blockers is unsuccessful in
patients with SIHD. (Level of Evidence: B)
Sublingual nitroglycerin or nitroglycerin spray is
recommended for immediate relief of angina in patients with
SIHD (Level of Evidence: B)

Elimination of anginal chest pain
Return to normal activities
Functional capacity of CCS class I
angina
Good patient compliance - minimal
side effects of therapy, cost-effective
Definition of Successful
Therapy
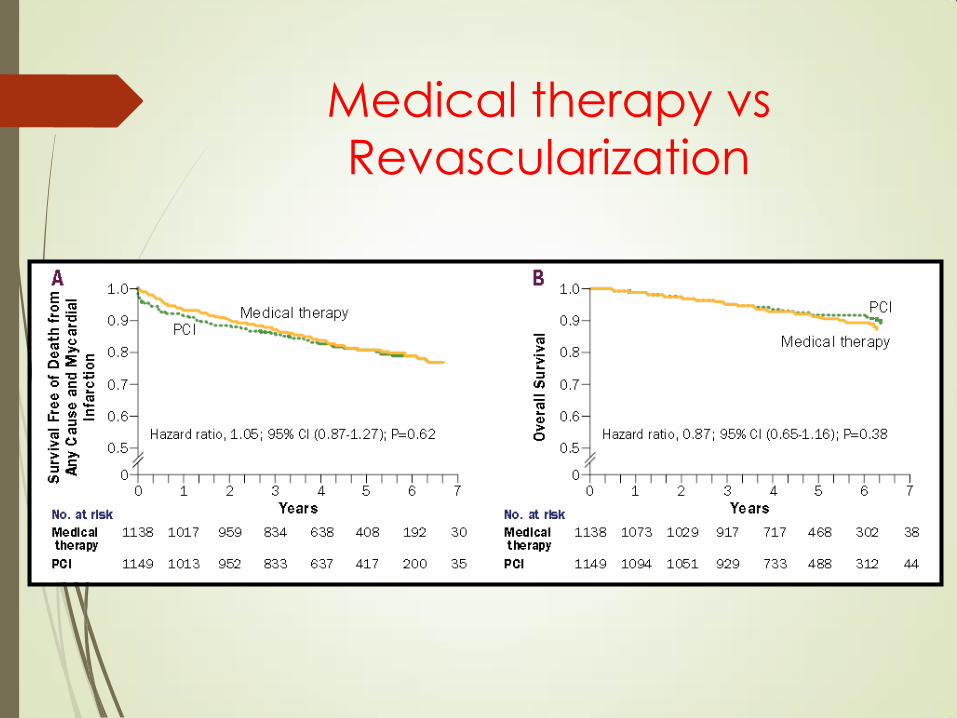
Medical therapy vs
Revascularization

Revascularization
Revascularization :
PCI (percutaneous coronary intervention)
CABG (coronary artery bypass grafting)
Indications:
High grade coronary lesions (Left main,
multivessel disease involving prox LAD)
High risk stress test features.
Severe symptoms despite medical therapy.

Follow up
Class I:
Patients with SIHD should receive periodic follow-up, at least
annually, that includes all of the following (Level of Evidence:
C):
a. Assessment of symptoms and clinical function;
b. Surveillance for complications of SIHD, including heart
failure and arrhythmias;
c. Monitoring of cardiac risk factors; and
d. Assessment of the adequacy of and adherence to
recommended lifestyle changes and medical therapy.
Assessment of LVEF and segmental wall motion by
echocardiography or radionuclide imaging is recommended in
patients with new or worsening heart failure or evidence of
intervening MI by history or ECG. (Level of Evidence: C)

Questions Thank you!