Stabilization with the Dynamic Cervical Implant: a novel ... · eration of the facet joints,...
9
SPINE J Neurosurg Spine Volume 22 • March 2015 CLINICAL ARTICLE J Neurosurg Spine 22:237–245, 2015 ABBREVIATIONS ACDF = anterior cervical discectomy and fusion; ASD = adjacent-segment disease; DCI = Dynamic Cervical Implant; DDD = degenerative disc disease; FSU = functional spinal unit; HO = heterotopic ossification; NDI = Neck Disability Index; ROM = range of motion; TDR = total disc replacement; VAS = visual analog scale. SUBMITTED December 3, 2013. ACCEPTED October 13, 2014. INCLUDE WHEN CITING Published online January 2, 2015; DOI: 10.3171/2014.10.SPINE131089. DISCLOSURE Clinical data collection and statistical analysis were financially supported by Paradigm Spine GmbH, the manufacturer of the Dynamic Cervical Implant. Dr. Matgé is a patent holder for, and consultant to, Paradigm Spine GmbH. Stabilization with the Dynamic Cervical Implant: a novel treatment approach following cervical discectomy and decompression Guy Matgé, MD, Christophe Berthold, MD, Vimal Raj Nitish Gunness, MD, Ardian Hana, MD, and Frank Hertel, MD National Neurosurgical Department, Centre Hospitalier de Luxembourg, Luxembourg City, Luxembourg OBJECT Although cervical total disc replacement (TDR) has shown equivalence or superiority to anterior cervical discectomy and fusion (ACDF), potential problems include nonphysiological motion (hypermobility), accelerated degen- eration of the facet joints, particulate wear, and compromise of the mechanical integrity of the endplate during device fixation. Dynamic cervical stabilization is a novel motion-preserving concept that facilitates controlled, limited flexion and extension, but prevents axial rotation and lateral bending, thereby reducing motion across the facet joints. Shock absorp- tion of the Dynamic Cervical Implant (DCI) device is intended to protect adjacent levels from accelerated degeneration. METHODS The authors conducted a prospective evaluation of 53 consecutive patients who underwent DCI stabiliza- tion for the treatment of 1-level (n = 42), 2-level (n = 9), and 3-level (n = 2) cervical disc disease with radiculopathy or myelopathy. Forty-seven patients (89%) completed all clinical and radiographic outcomes at a minimum of 24 months. Clinical outcomes consisted of Neck Disability Index (NDI) and visual analog scale (VAS) scores, neurological function at baseline and at latest follow-up, as well as patient satisfaction. Flexion-extension radiography was evaluated for device motion, implant migration, subsidence, and heterotopic ossification. Cervical sagittal alignment (Cobb angle), functional spinal unit (FSU) angle, and range of motion (ROM) at index and adjacent levels were evaluated with WEB 1000 soft- ware. RESULTS The NDI score, VAS neck and arm pain scores, and neurological deficits were significantly reduced at each postoperative time point compared with baseline (p < 0.0001). At 24 months postoperatively, 91% of patients were very satisfied and 9% somewhat satisfied, while 89% would definitely and 11% would probably elect to have the same surgery again. In 47 patients with 58 operated levels, the radiographic assessment showed good motion (5° –12°) of the device in 57%, reduced motion (2° –5°) in 34.5%, and little motion (0–2°) in 8.5%. The Cobb and FSU angles improved, showing a clear tendency for lordosis with the DCI. Motion greater than 2° of the treated segment could be preserved in 91.5%, while 8.5% had a near segmental fusion. Mean ROM at index levels demonstrated satisfying motion preservation with DCI. Mean ROM at upper and lower adjacent levels showed maintenance of adjacent-level kinematics. Heterotopic ossification, including 20% minor and 15% major, had no direct impact on clinical results. There were 2 endplate subsid- ences detected with an increased segmental lordosis. One asymptomatic anterior device migration required reoperation. Three patients underwent a secondary surgery in another segment during follow-up, twice for a new disc herniation and once for an adjacent degeneration. There was no posterior migration and no device breakage. CONCLUSIONS Preliminary results indicate that the DCI implanted using a proper surgical technique is safe and fa- cilitates excellent clinical outcomes, maintains index- and adjacent-level ROM in the majority of cases, improves sagittal alignment, and may be suitable for patients with facet arthrosis who would otherwise not be candidates for cervical TDR. Shock absorption together with maintained motion in the DCI may protect adjacent levels from early degeneration in longer follow-up. http://thejns.org/doi/abs/10.3171/2014.10.SPINE131089 KEY WORDS dynamic cervical implant; dynamic cervical stabilization; cervical arthroplasty; cervical arthropathy; shock absorption; adjacent-level protection 237 ©AANS, 2015 Unauthenticated | Downloaded 10/19/20 09:39 PM UTC
Transcript of Stabilization with the Dynamic Cervical Implant: a novel ... · eration of the facet joints,...

spine
J Neurosurg Spine Volume 22 • March 2015
cliNical articleJ Neurosurg Spine 22:237–245, 2015
abbreviatioNS ACDF = anterior cervical discectomy and fusion; ASD = adjacent-segment disease; DCI = Dynamic Cervical Implant; DDD = degenerative disc disease; FSU = functional spinal unit; HO = heterotopic ossification; NDI = Neck Disability Index; ROM = range of motion; TDR = total disc replacement; VAS = visual analog scale.Submitted December 3, 2013. accepted October 13, 2014.iNclude wheN citiNg Published online January 2, 2015; DOI: 10.3171/2014.10.SPINE131089.diScloSure Clinical data collection and statistical analysis were financially supported by Paradigm Spine GmbH, the manufacturer of the Dynamic Cervical Implant. Dr. Matgé is a patent holder for, and consultant to, Paradigm Spine GmbH.
Stabilization with the Dynamic Cervical Implant: a novel treatment approach following cervical discectomy and decompressionguy matgé, md, christophe berthold, md, vimal raj Nitish gunness, md, ardian hana, md, and Frank hertel, md
National Neurosurgical Department, Centre Hospitalier de Luxembourg, Luxembourg City, Luxembourg
obJect Although cervical total disc replacement (TDR) has shown equivalence or superiority to anterior cervical discectomy and fusion (ACDF), potential problems include nonphysiological motion (hypermobility), accelerated degen-eration of the facet joints, particulate wear, and compromise of the mechanical integrity of the endplate during device fixation. Dynamic cervical stabilization is a novel motion-preserving concept that facilitates controlled, limited flexion and extension, but prevents axial rotation and lateral bending, thereby reducing motion across the facet joints. Shock absorp-tion of the Dynamic Cervical Implant (DCI) device is intended to protect adjacent levels from accelerated degeneration.methodS The authors conducted a prospective evaluation of 53 consecutive patients who underwent DCI stabiliza-tion for the treatment of 1-level (n = 42), 2-level (n = 9), and 3-level (n = 2) cervical disc disease with radiculopathy or myelopathy. Forty-seven patients (89%) completed all clinical and radiographic outcomes at a minimum of 24 months. Clinical outcomes consisted of Neck Disability Index (NDI) and visual analog scale (VAS) scores, neurological function at baseline and at latest follow-up, as well as patient satisfaction. Flexion-extension radiography was evaluated for device motion, implant migration, subsidence, and heterotopic ossification. Cervical sagittal alignment (Cobb angle), functional spinal unit (FSU) angle, and range of motion (ROM) at index and adjacent levels were evaluated with WEB 1000 soft-ware.reSultS The NDI score, VAS neck and arm pain scores, and neurological deficits were significantly reduced at each postoperative time point compared with baseline (p < 0.0001). At 24 months postoperatively, 91% of patients were very satisfied and 9% somewhat satisfied, while 89% would definitely and 11% would probably elect to have the same surgery again. In 47 patients with 58 operated levels, the radiographic assessment showed good motion (5°–12°) of the device in 57%, reduced motion (2°–5°) in 34.5%, and little motion (0–2°) in 8.5%. The Cobb and FSU angles improved, showing a clear tendency for lordosis with the DCI. Motion greater than 2° of the treated segment could be preserved in 91.5%, while 8.5% had a near segmental fusion. Mean ROM at index levels demonstrated satisfying motion preservation with DCI. Mean ROM at upper and lower adjacent levels showed maintenance of adjacent-level kinematics. Heterotopic ossification, including 20% minor and 15% major, had no direct impact on clinical results. There were 2 endplate subsid-ences detected with an increased segmental lordosis. One asymptomatic anterior device migration required reoperation. Three patients underwent a secondary surgery in another segment during follow-up, twice for a new disc herniation and once for an adjacent degeneration. There was no posterior migration and no device breakage.coNcluSioNS Preliminary results indicate that the DCI implanted using a proper surgical technique is safe and fa-cilitates excellent clinical outcomes, maintains index- and adjacent-level ROM in the majority of cases, improves sagittal alignment, and may be suitable for patients with facet arthrosis who would otherwise not be candidates for cervical TDR. Shock absorption together with maintained motion in the DCI may protect adjacent levels from early degeneration in longer follow-up.http://thejns.org/doi/abs/10.3171/2014.10.SPINE131089Key wordS dynamic cervical implant; dynamic cervical stabilization; cervical arthroplasty; cervical arthropathy; shock absorption; adjacent-level protection
237©AANS, 2015
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC

g. matgé et al.
J Neurosurg Spine Volume 22 • March 2015
The gold standard treatment for cervical disc dis-ease is anterior cervical decompression and fusion (ACDF). The well-documented potential complica-
tions of ACDF, including symptomatic adjacent-segment disease (ASD), pseudarthrosis, graft donor site morbid-ity, and instrumentation-related problems have led to the search for motion-preserving alternatives that will provide adequate motion segment stabilization while eliminating the problems encountered with ACDF.4,10,14,15,18,19 Recent results of several multicenter, prospective, randomized trials comparing cervical total disc replacement (TDR) implants with ACDF have demonstrated equivalence or superiority over ACDF with respect to clinical outcomes, reduced reoperation rates at the index level, and lower rates of revision for symptomatic ASD.12,21,22,30 Conser-vative estimates suggest that as many as 47% of patients requiring cervical spine surgery meet the strict inclusion criteria to be candidates for TDR.2
Although TDR has been shown to reduce adjacent-level intradiscal pressures and provide a more physiological over-all cervical but also index- and adjacent-level range of mo-tion (ROM) while maintaining sagittal alignment, recent studies have also highlighted the potential limitations of TDR.1,3,5–8 Device subsidence with keel- and flange-based devices has led to the search for optimal interface mechan-ics between the device and bony endplate.6,17 Furthermore, clinical and finite element analysis kinematic studies have revealed that certain TDR designs may actually increase the loads experienced by the facet joints.9,16 As such, pa-tients with facet arthrosis are currently not candidates for TDR devices. Facet joint stresses can also be exacerbated with poor implant positioning, thus highlighting how tech-nical error in device placement may lead to a suboptimal outcome due to facet joint arthrosis despite excellent neu-ral decompression.9,25 Consequently, there may be a role for a motion-preserving strategy that acts as a bridge be-tween rigid fixation achieved with fusion and potentially nonphysiological, position-dependent motion provided by TDR that may exacerbate facet degeneration.28
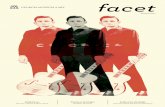
The concept of dynamic cervical stabilization was in-troduced by the first author (G.M.) in 2004 as a treatment approach that aimed to facilitate controlled, limited index-level motion to prevent transfer of stresses to adjacent lev-els, while also aiming to minimize motion that may ex-acerbate facet joint stresses.13,28 By limiting axial rotation and lateral bending, motion that significantly contributes to facet forces, and by only allowing limited subaxial flexion and extension, the Dynamic Cervical Implant (DCI; Para-digm Spine) allows for motion-preservation while limiting stresses applied to the posterior elements.28 In contrast to other motion-preserving implants, the device functions as a shock absorber and allows for axial compression in flex-ion and limited extension and is protected from fatigue overload via its mechanical stop during maximal flexion (Fig. 1). Thus, the DCI is capable of segmental stabiliza-tion and protecting the posterior elements from excessive motion.28 The DCI is a single-piece, titanium U-shaped implant, with no polyethylene core, that is placed into the disc space and secured to the endplate with serrated teeth, thus obviating the need for fixation via vertebral body screws or keels that may compromise the mechanical in-
tegrity of the vertebral endplate. The single metallic piece with no polyethylene/metallic articulation eliminates par-ticulate wear and the potential for wear debris–induced osteolysis.17 The current second-generation device with a more rectangular shape and ancillary technical improve-ments has been used since 2008 in more than 9500 spinal levels worldwide to date.
methodspatient population
Fifty-three consecutive patients with 1-, 2-, or 3-level cervical disc disease from C-3 to C-7, with neck and arm pain recalcitrant to at least 6 weeks of conservative treat-ment, underwent anterior cervical discectomy and sta-bilization with the second-generation DCI device by the first author (G.M) between May 2008 and March 2011, as-sisted by coauthors during follow-up. Forty-seven patients (89%) completed clinical and radiographic outcomes at 24 months. Six patients (11%), 5 with 1-level and 1 with 3-lev-el surgeries, were lost to follow-up before 24 months were completed: 1 emigrated, 2 had another serious health con-dition (ongoing Parkinson disease, and lymphoma), and 2 did not want to continue the full study after 12 months. All had an uneventful postoperative outcome and a functional device at 12 months. One patient experienced device mi-gration requiring removal, without further therapy and a good outcome. The indication to operate was primarily an overlap of disc herniation (43%), degenerative disc dis-ease (DDD; 39%), and stenosis (18%). In 12 patients, the DCI was indicated to treat DDD that had developed at a level adjacent to a prior ACDF. In 2 patients, surgery was performed at the level adjacent to a previous cervical disc arthroplasty. The remaining 39 patients were index-level surgeries. There were 27 women and 26 men in the study with an average age of 50 years (range 25–79 years). For-ty-two (79%) of the 53 treated patients were implanted for single-level cervical disc disease, 9 (17%) for 2-level, and 2 (4%) for 3-level contiguous cervical disc disease. The 58 treated levels in 47 patients who completed follow-up represent the basis of this study.
Fig. 1. Lateral radiographs showing the shock-absorbing capabilities of the DCI implant during movement.
238
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC

Stabilization with the dynamic cervical implant
J Neurosurg Spine Volume 22 • March 2015
clinical outcomesAll patients included in this series were symptom-
atic for radiculopathy or beginning myelopathy. Patients with chronic myelopathy and pure discogenic neck pain were excluded from this study. Clinical outcomes were assessed using Neck Disability Index (NDI) scores at baseline and at each available postoperative time point (3, 6, 12, and 24 months). Visual analog scale (VAS) scores for neck and arm pain as well as neurological function were also collected at each available postoperative time point. At 24 months postoperatively, patients were also asked whether they would undergo the surgery again, and to rate their postoperative satisfaction as very satisfied, somewhat satisfied, somewhat dissatisfied, or very dissat-isfied. Data analysis was performed with GraphPad Prism software (version 5.0d, GraphPad Software). A paired t-test (2-tailed) was applied with the significance level set at p = 0.05.
radiographic outcomesFunctional and neutral radiographs were documented
and assessed preoperatively and postoperatively to ana-lyze motion and/or any abnormality. Postoperative exami-nation concentrated on the variables of motion, heterotop-ic ossification (HO), and device subsidence or migration. Cervical alignment from C-2 to C-7 (Cobb angle), func-tional spinal unit (FSU) angle, and the ROM of the index level and adjacent cervical levels were measured by the site with Web 1000 software (AGFA). For overall cervical curvature of C2–7, patients were classified as lordotic (≥ 10°), neutral (0°–10°), or kyphotic (< 0°). For FSU angle, patients were classified as lordotic (≥ 5°), neutral (0°–5°), or kyphotic (< 0°).
Surgical techniqueA standard Smith-Robinson approach was made to the
anterior cervical spine. Placement of the patient in slight cervical lordosis while maintaining his or her shoulders downward is routinely used under lateral fluoroscopy. A discectomy sparing the cartilage and foraminal decom-pression using a combination of curettes, pituitary ron-geurs, and high-speed bur are used. The anterior vertebral osteophytes are not removed so as to not promote HO. With respect to the posterior disc–osteophyte complex, care is taken to remove this osteophyte to fully seat the U-shaped part of the device (Fig. 2). Failure to remove the poste-rior osteophyte may lead to suboptimal decompression and device placement, but also lack of required fixation. Complete excision of the posterior longitudinal ligament is routinely performed to complete neural decompres-sion. Osseous and epidural bleeding (promotion of HO) is controlled with hemostatic glue, avoiding bone wax and microcoagulation near neural structures. Trial inserts are used to identify the proper implant size. Device undersiz-ing may lead to poor fixation and implant migration. The largest possible device that can be safely placed should be selected to maximize device-endplate contact and to gain support from the apophyseal rim. The trial insert is ad-vanced under fluoroscopic guidance to ensure safe place-ment. A depth-controlled stop mechanism allows for safe
and controlled device placement in the anterior-posterior direction (Fig. 3). The implant should be placed as poste-riorly as possible with the apex of the U-shaped part of the device lining up with the posterior cortical rim, as visual-ized using intraoperative fluoroscopy. The teeth of the im-plant are optimally fixated to the endplate via Caspar pin compression following device insertion. The device may be replaced or changed using the same insertion instru-ment if final imaging demonstrates suboptimal position-ing. Rinsing the implanted disc space removes remaining blood and bone dust, all potentially promoting HO. Per-fect hemostasis is required while closing the wound in 2 layers. Postoperative management consists of unrestricted but careful neck ROM, along with antiinflammatory med-ications for a 10-day period to reduce the potential for HO.
resultsclinical outcomes
The VAS pain scores for the neck and affected arm were significantly reduced at each postoperative time point compared with baseline (p < 0.0001; Fig. 4). Neurological function improved in 73.3% and was maintained in 26.7% without deterioration at 24 months (Table 1). Similarly, NDI scores were significantly reduced from baseline at each postoperative time point (Fig. 5A). Excellent clinical outcomes were maintained at 24 months postoperatively: Patients reported being very satisfied in 91% or somewhat satisfied in 9% of all cases. Similarly, at the 24-month postoperative time point, patients reported that they would definitely choose to undergo the same procedure again in 89% and probably in 11% of all cases.
Fig. 2. Perioperative fluoroscopy showing implantation of the DCI. Note the DCI positioning with optimal endplate coverage, respecting the anterior and posterior safety zone using an implantation tool with depth control. The center of rotation is in the posterior third of the disc space.
Fig. 3. Photograph of the DCI implantation tool (lower) with a central knob for depth control, lateral knob for compression of the implant allow-ing easier insertion, and a trial sleeve (upper) for the final DCI position. Reproduced with permission from Paradigm Spine LLC.
239
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC

g. matgé et al.
J Neurosurg Spine Volume 22 • March 2015
radiographic outcomesIn 47 patients with 58 implanted levels and a mini-
mum follow-up of 24 months, the radiographic assess-ment showed the following (as compared with preopera-tive dynamic views): good motion (ROM 5°–12°) of the implanted disc space in 33 levels (57%), reduced motion (ROM 2°–5°) in 20 levels (34.5%), and no significant mo-tion (ROM 0–2°) in 5 levels (8.5%). Thus, using the DCI, motion could be preserved in 91.5% at a minimum of 24 months follow-up, in which 8.5% of patients experi-enced near-complete fusion and 34.5% had reduced but ongoing motion over 24 months. ROM at index levels was measured as 0.5°–14.8° (mean 6.0°) preoperatively and 0.6°–12.2° (mean 5.3°) at 24-months follow-up, i.e., sat-isfying motion preservation (-5.5%) with DCI (Fig. 5B). Evolution of mean ROM at upper (from 6.2° to 6.1°, or
-1.7%) and lower (from 5.6° to 5.4°, or -4.1%) adjacent lev-els showed a protective effect for ASD with DCI, without any hypermobility. Global cervical alignment measured by the Cobb angle ranged from -24.8° to 29° (mean 9.9°) preoperatively and from -8.3° to 35.7° (mean 16.3°) at 24 months follow-up, with, respectively, 23 and 27 cases of lordotic angulations, 22 and 19 neutral angulations, and 2 and 1 kyphotic angulations, showing a clear tendency (31.7% improvement) for lordosis with DCI (Fig. 5C). This coincides with FSU angulation improving from a mean of 3.8° to 5.2° (38.8% improvement). We noticed some HO in 21 patients (35%, according to McAfee et al.;20 see Table 2) from 58 implanted levels: minor (nonbridging) Grade I in 7 (12%), Grade II in 5 (8%), major Grade III in 5 (8%), and Grade IV in 4 (7%), in which 2 of these 4 levels were in the same patient (Table 2). HO had no direct impact on
table 1. development of neurological functionDeficits (%) Neurological Function (%)
Time Period No Neurological w/ Neurological Motor Sensory Improved Maintained Deteriorated
Preop (n = 53) 28.3 71.7 56.7 69.8Postop (n = 47) 3 mos 70.8 29.2 0 6 mos 68.1 31.9 0 12 mos 67.4 32.6 0 24 mos 73.3 26.7 0
Fig. 4. Bar graph of the VAS scores for neck pain (upper) and arm pain (lower) preoperatively and at each follow-up evaluation.
240
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC

Stabilization with the dynamic cervical implant
J Neurosurg Spine Volume 22 • March 2015
clinical results, but major HO (Grade III or IV) resulted in less motion. There was 1 asymptomatic anterior device migration detected (1.7%), and 2 cases of asymptomatic endplate subsidence (3.5%) with a focal incidence on lor-
dosis. Only 1 (2%) of 47 patients had symptomatic acceler-ated ASD after 24 months, and 2 patients (4%) had a new disc herniation detected at different levels. No posterior device displacement or material breakage occurred.
Fig. 5. Bar graphs showing preoperative and follow-up scores for the NDI (a), ROM of index and adjacent segments (AS; b), and sagittal alignment of the cervical spine and the index segments (c).
TABLE 2. Classification of HO in TDR according to McAfee et al.
Grade Description
0 No HO present.I HO present in islands of bone w/in soft tissue but not influencing the ROM of the vertebral motion segment.II HO possibly affecting the vertebral ROM. HO present btwn the 2 planes formed by the vertebral endplates but not
blocking or articulating btwn adjacent vertebral endplates or osteophytes.III The ROM of the vertebral endplates is blocked by the formation of HO &/or postoperative osteophytes on flexion-
extension or lateral bending radiographs.IV HO causing inadvertent arthrodesis. Bone ankylosis. Bridging trabecular bone continuous btwn adjacent end-
plates & <3° of motion on lateral flexion-extension radiographs.
241
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC

g. matgé et al.
J Neurosurg Spine Volume 22 • March 2015
complications and reoperationsOne patient (2%) experienced an asymptomatic anterior
device migration that required implant removal. The mi-gration was detected during the scheduled 6-month follow-up examination. Because the disc space was nearly fused in the posterior part, no further stabilization was required and final outcome has been good to date, more than 3 years following surgery. Three patients underwent a second-ary surgery in another segment during follow-up (6.5%), twice with a DCI for a new, not directly adjacent-level disc herniation (4.3%), and once with a DCI for an accelerated adjacent-disc degeneration (2.2%). This last patient already had DDD when undergoing an operation more than 2 years previously for 2-level disc herniation below this new level and would now be treated at 3 levels in 1 session. All 4 reoperations (9%) had a satisfying evolution. One patient experienced dysphonia, and recovered at 6 months.
illustrative caseThis 49-year-old woman complained of pain in the
neck and right arm in a C-5 radicular pattern for more than 1 year, and conservative treatment was unsuccessful. The pain was worse in extension, where dynamic radiog-raphy showed degenerative retrolisthesis at C4–5 (chronic instability). She had previously undergone an ACDF with intervertebral cage fusion at C5–6 in 2006 for cervical disc herniation. The surgery consisted of decompression and dynamic stabilization with a DCI at C4–5. The 7-mm disc space distraction (no overdistraction) allowed restabi-lization of the unstable segment. The patient’s clinical out-come was excellent with good restoration of disc height, sagittal balance, and motion (Fig. 6).
discussionWhile ACDF provides excellent, reliable short-term
outcomes, the long-term health of the adjacent discs may be compromised as a result of increased loads and transfer of stresses leading to symptomatic ASD.14,15 Motion-pres-ervation with TDR produces a physiological distribution of ROM and stresses at operative and adjacent levels, thereby reducing the risk for developing ASD.7,8,29 In fact, the re-sults of recent randomized, prospective multicenter trials comparing TDR with ACDF have confirmed the purport-ed biomechanical rationale for motion preservation and have shown significantly reduced reoperation rates at the adjacent levels with TDR compared with ACDF.12,21–23,30
Despite the excellent initial clinical record, TDR is not a panacea for all cervical disc disease. Auerbach et al.2 reported that as many as 47% of patients undergoing sur-gery for the cervical spine could qualify for TDR using the strict inclusion criteria from the US FDA Investiga-tional Device Exemption randomized prospective trials comparing ACDF with TDR; however, 53% of patients possessed contraindications that precluded candidacy for TDR. Among the most common contraindications ob-served were 3 or more diseased levels (28.1%), fused adja-cent level (10.2%), and the presence of facet degeneration (8.3%). Other limitations of TDR include: increased load-ing of the facet joints; potential vertebral body fracture or compromise of the mechanical integrity of the vertebral
endplate with keel- or flange-based devices; and issues re-lated to long-term wear between the polyethylene core and metal bearing surfaces.9,24
Dynamic cervical stabilization with the DCI is a novel treatment approach for cervical disc disease that was initial-ly conceived as a method to combine the potential advan-tages of fusion and TDR. Dynamic cervical stabilization is predicated on limited index-level motion preservation to reduce the rate of ASD, while precluding lateral bending and axial rotation motion, and thus theoretically protecting the facet joints from excessive stresses.13,28 Along the spec-trum of motion, the DCI is intended to provide controlled, limited flexion and extension—the primary motions in the subaxial cervical spine—that is greater than that seen with fusion, but less than that achieved with TDR. By protect-ing the facet joints from lateral bending and axial rotation forces, the DCI is a potential treatment option for patients with facet arthrosis who would otherwise be contraindicat-ed for TDR.2,12,21,22,28 Another unique feature is the ability of the device to function as a shock absorber, which allows axial compression in flexion, and limited extension from the neutral position, thereby protecting the adjacent levels from excessive stresses.28 Furthermore, because fixation of the DCI does not require vertebral body screws, keels, or flanges, and is instead secured to the endplate via serrated edges, this implant may potentially treat multilevel disease without compromising the vertebral endplate architecture and increase the risk for subsidence. Finally, the lack of a metal–polyethylene articulating surface, as noted with several TDR designs, precludes the development of wear debris and the potential for wear-induced osteolysis.17
Fig. 6. Preoperative (a and b) and 1-year postoperative (c and d) functional radiographs of DDD at C4–5 with retrolisthesis in extension above cage–fusion at C5–6, dynamically stabilized with an M7 DCI (12 × 14 × 7 mm).
242
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC

Stabilization with the dynamic cervical implant
J Neurosurg Spine Volume 22 • March 2015
Our initial results indicate that the DCI is able to facili-tate and maintain excellent neurological decompression and motion-segment stabilization. Clinical outcomes as assessed by the NDI, VAS neck and arm pain scores, and satisfaction indicate that the DCI provides results com-parable to ACDF and TDR.12,13,19,21–23,26 The current series included patients undergoing treatment for symptomatic ASD and with the presence of facet arthrosis, both contra-indications to receiving TDR. One patient had experienced an acceleration of a radiographic but asymptomatic ASD already present 2 years previously when operated on using a DCI 2 levels below this level. This patient would now be treated at 3 levels in 1 session. A longer follow-up pe-riod will be needed to determine the extent to which DCI protects against ASD. Preservation of motion as long as possible was a request when starting with DCI, although slow fusion appears to protect against ASD as neighboring cervical spine structures may adapt over time if we try to maintain or to restore lordosis.1,11 Global cervical align-ment as measured by the Cobb angle improved from mean of 9.9° preoperatively to 16.3° at 24 months follow-up, with, respectively, 23 and 27 cases of lordotic angulations, 22 and 19 neutral angulations, and 2 and 1 kyphotic angu-lations, showing a clear tendency for lordosis with DCI, in agreement with FSU angulations improving from a mean of 3.8° to 5.2°. Motion of the device could be preserved in 91.5% at a minimum follow-up of 24 months, in which 8.5% of patients had near fusion, and 34.5% had reduced but ongoing motion over 24 months. Mean ROM at index levels was measured as 6° before surgery and 5.3° after 24 months of follow-up, i.e., satisfying motion preserva-tion (-5.5%) with DCI. Evolution of mean ROM at upper (from 6.2° to 6.1°) and lower (from 5.6° to 5.4°) adjacent levels shows a protective effect for ASD with DCI, without any hypermobility as noted rapidly following segmental immobilization with ACDF. We observed approximately 35% of HO (20% minor HO and 15% major HO), which is in the low range of TDR publications, and probably also related to our perioperative care avoiding blood and bone dust.3,12,21,22,26 An interesting paper by Tu et al. analyzed the effects of carpentry on HO and mobility with the Bryan artificial disc using CT scanning, which is much more sensitive to detecting ossification. Shell kyphosis and in-adequate endplate coverage had adverse effects in the for-mation of HO and segmental mobility after arthroplasty, and appropriate carpentry was the more important factor in maintaining segmental motion.27
While the DCI is intended to provide another treatment option for cervical disc disease and serve as a complement to ACDF and TDR in the spine surgeon’s armamentarium, there are certain biomechanical advantages with DCI by providing limited, controlled flexion-extension while lim-iting axial rotation and lateral bending motions.28 A recent finite element analysis study compared load sharing on facet joints with Bryan, Prestige LP, and ProDisc-C TDR, in which the unconstrained Bryan disc imposed the great-est stress on the facet joints during flexion and extension, but all 3 TDR-cervical (TDR-C) systems showed increased loads at the joints in lateral bending, attributable to direct impinging contact force.16 Rousseau et al. performed an in vivo kinematic evaluation of 26 patients treated using
the Prestige LP and 25 with the ProDisc-C and found that both disc systems produced flexion-extension centers of rotation located more anteriorly and superiorly, which may consequently increase load in the facet joints, as has been shown in similar lumbar spine models.16,24,25 Galbusera et al. used a finite element analysis model to evaluate a ball-and-socket TDR-C design and found that anteroposterior positioning of the device affected not only flexion and ex-tension motion, but also affected the facet joint forces in lateral bending and axial rotation.9 In contrast, by limiting subaxial lateral bending and axial rotation, the DCI may significantly reduce facet joint forces and protect the facet joints from excessive stress, while maintaining index level motion.13,28
Another potentially advantageous feature of the DCI design is the use of serrated teeth to fixate the device to the endplate, and the lack of vertebral body screws, flanges, or the need to chisel and place a keeled device. A recent finite element analysis study compared fixation methods and bone-implant interface strain of 3 TDR-C systems and reported that anchorage design is a factor that may con-tribute to the subsidence. The authors found high contact stresses at the endplate flanges in the Prestige LP device, and at the midline keel fixation of the ProDisc-C, which may initiate bone resorption.17 In an in vitro cadaver study, Cunningham et al. reported that despite the presence of a keel and taller teeth, “[Prestige LP and Kineflex/C de-vices] did not demonstrate inordinately greater fixation strength than those configurations with lower profiles.”6
The DCI, due to its nonkeeled, nonflange design that is fixated by serrated teeth alone, does not violate the endplate and potentially increase the risk for fracture or subsidence. Highlights of the current second-generation design, which was first implanted in 2008, include a full spectrum of footprint sizes and a change in the shape of the device foot-print from square to rectangular to better accommodate patient anatomy. The serrated teeth allow for adequate de-vice fixation when surgical technique is respected. In this series, only 1 of the 66 devices experienced asymptomat-ic anterior migration in a hyperactive patient at 6 months follow-up, although dynamic views at 3 months showed an adapted device to treated disc space. Stabilization was probably not adequately achieved at this time in an athletic patient. In only these cases, we now would recommend a cervical collar for 6 weeks during sports participation, al-though the compliance of the patients is rather difficult if this is not well explained before the procedure. From inter-national feedback of DCI users, we found out that anterior migrations occurred due to surgeon error in device size se-lection (undersizing), inadequate posterior decompression, or aberrant device positioning (positioned too anteriorly). There have been no reported posterior migrations.
Limitations of this study include a small series with only a 2-year follow-up and no randomization to ACDF or TDR. Longevity of the device has been proven in pa-tients who received the first generation implanted in 2004. There has been no material breakage in more than 150 patients who underwent operations performed personally by the first author (G.M.). There is a bias in the study, as all patients were operated on and followed by the first author, assisted by coauthors.
243
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC

g. matgé et al.
J Neurosurg Spine Volume 22 • March 2015
conclusionsThe initial clinical and radiographic results with the
DCI appear promising as an alternative to TDR and ACDF in the treatment of cervical disc disease. The DCI affords maximal neurological improvement, along with maintenance of excellent clinical outcomes. The potential biomechanical advantages of DCI over ACDF and TDR-C include the ability to maintain device-level motion and minimize the development of ASD, while protecting the facet joints from excessive stresses noted with other mo-tion-preserving devices during lateral bending, axial ro-tation, and extension. Fixation of the device to the bone via serrated teeth precludes the need for a central keel or flanges, which reduces the mechanical competency of the endplate, and possibly protects against subsidence or fracture. The presence of only 1 symptomatic ASD at 24 months with DCI in the current study is encouraging, but requires a longer follow-up period to determine the extent to which ASD can be prevented. Proper surgical technique with improved biomechanical understanding could further improve results with this device.
references 1. Anakwenze OA, Auerbach JD, Milby AH, Lonner BS,
Balderston RA: Sagittal cervical alignment after cervical disc arthroplasty and anterior cervical discectomy and fu-sion: results of a prospective, randomized, controlled trial. Spine (Phila Pa 1976) 34:2001–2007, 2009
2. Auerbach JD, Jones KJ, Fras CI, Balderston JR, Rushton SA, Chin KR: The prevalence of indications and contraindica-tions to cervical total disc replacement. Spine J 8:711–716, 2008
3. Bertagnoli R, Yue JJ, Pfeiffer F, Fenk-Mayer A, Lawrence JP, Kershaw T, et al: Early results after ProDisc-C cervical disc replacement. J Neurosurg Spine 2:403–410, 2005
4. Boden SD, Balderston RA, Heller JG, Hanley EN Jr, Zigler JE: An AOA critical issue. Disc replacements: this time will we really cure low-back and neck pain? J Bone Joint Surg Am 86-A:411–422, 2004
5. Chang UK, Kim DH, Lee MC, Willenberg R, Kim SH, Lim J: Range of motion change after cervical arthroplasty with ProDisc-C and prestige artificial discs compared with an-terior cervical discectomy and fusion. J Neurosurg Spine 7:40–46, 2007
6. Cunningham BW, Hu N, Zorn CM, McAfee PC: Compara-tive fixation methods of cervical disc arthroplasty versus conventional methods of anterior cervical arthrodesis: ser-ration, teeth, keels, or screws? Laboratory investigation. J Neurosurg Spine 12:214–220, 2010
7. DiAngelo DJ, Roberston JT, Metcalf NH, McVay BJ, Davis RC: Biomechanical testing of an artificial cervical joint and an anterior cervical plate. J Spinal Disord Tech 16:314–323, 2003
8. Dmitriev AE, Cunningham BW, Hu N, Sell G, Vigna F, McAfee PC: Adjacent level intradiscal pressure and segmen-tal kinematics following a cervical total disc arthroplasty: an in vitro human cadaveric model. Spine (Phila Pa 1976) 30:1165–1172, 2005
9. Galbusera F, Anasetti F, Bellini CM, Costa F, Fornari M: The influence of the axial, antero-posterior and lateral positions of the center of rotation of a ball-and-socket disc prosthesis on the cervical spine biomechanics. Clin Biomech (Bristol, Avon) 25:397–401, 2010
10. Goffin J, van Loon J, Van Calenbergh F, Plets C: Long-term results after anterior cervical fusion and osteosynthetic stabi-
lization for fractures and/or dislocations of the cervical spine. J Spinal Disord 8:500–508, 1995
11. Guérin P, Obeid I, Gille O, Bourghli A, Luc S, Pointillart V, et al: Sagittal alignment after single cervical disc arthro-plasty. J Spinal Disord Tech 25:10–16, 2012
12. Heller JG, Sasso RC, Papadopoulos SM, Anderson PA, Fes-sler RG, Hacker RJ, et al: Comparison of BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion: clinical and radiographic results of a randomized, controlled, clinical trial. Spine (Phila Pa 1976) 34:101–107, 2009
13. Herdmann J, Buddenberg P, Trautwein F, Rhee S, Piltz A, Floeth F: Does maintenance of physiologic kinematics in the adjacent segment prevent adjacent segment degeneration following cervical dynamic stabilization? Paradigm Spine. (Abstract) (http://int.paradigmspine.com/sites/default/files/Does%20maintenance%20of%20physiologic%20kinematics %20in%20the%20adjacent%20prevent%20adjacent%20 segment%20degeneration%20following%20dynamic%20 cervical%20stabilization.pdf) [Accessed October 15, 2014]
14. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohl-man HH: Radiculopathy and myelopathy at segments adja-cent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am 81:519–528, 1999
15. Ishihara H, Kanamori M, Kawaguchi Y, Nakamura H, Kimura T: Adjacent segment disease after anterior cervical interbody fusion. Spine J 4:624–628, 2004
16. Kang H, Park P, La Marca F, Hollister SJ, Lin CY: Analysis of load sharing on uncovertebral and facet joints at the C5-6 level with implantation of the Bryan, Prestige LP, or ProDisc-C cervical disc prosthesis: an in vivo image-based finite ele-ment study. Neurosurg Focus 28(6):E9, 2010
17. Lin CY, Kang H, Rouleau JP, Hollister SJ, Marca FL: Stress analysis of the interface between cervical vertebrae end plates and the Bryan, Prestige LP, and ProDisc-C cervical disc prostheses: an in vivo image-based finite element study. Spine (Phila Pa 1976) 34:1554–1560, 2009
18. Matgé G: Approaches to cervical spine, in Sindou M (ed): Practical Handbook of Neurosurgery From Leading Neu-rosurgeons. Vienna: Springer, 2009, pp 1141–1160
19. Matgé G: Cervical cage fusion with 5 different implants: 250 cases. Acta Neurochir (Wien) 144:539–550, 2002
20. McAfee PC, Reah C, Gilder K, Eisermann L, Cunningham B: A meta-analysis of comparative outcomes following cervi-cal arthroplasty or anterior cervical fusion: results from 4 prospective multicenter randomized clinical trials and up to 1226 patients. Spine (Phila Pa 1976) 37:943–952, 2012
21. Mummaneni PV, Burkus JK, Haid RW, Traynelis VC, Zde-blick TA: Clinical and radiographic analysis of cervical disc arthroplasty compared with allograft fusion: a randomized controlled clinical trial. J Neurosurg Spine 6:198–209, 2007
22. Murrey D, Janssen M, Delamarter R, Goldstein J, Zigler J, Tay B, et al: Results of the prospective, randomized, con-trolled multicenter Food and Drug Administration investi-gational device exemption study of the ProDisc-C total disc replacement versus anterior discectomy and fusion for the treatment of 1-level symptomatic cervical disc disease. Spine J 9:275–286, 2009
23. Robertson JT, Papadopoulos SM, Traynelis VC: Assessment of adjacent-segment disease in patients treated with cervical fusion or arthroplasty: a prospective 2-year study. J Neuro-surg Spine 3:417–423, 2005
24. Rousseau MA, Cottin P, Levante S, Nogier A, Lazennec JY, Skalli W: In vivo kinematics of two types of ball-and-socket cervical disc replacements in the sagittal plane: cranial ver-sus caudal geometric center. Spine (Phila Pa 1976) 33:E6–E9, 2008 [Erratum in Spine (Phila Pa 1976) 33:829, 2008]
25. Rundell SA, Auerbach JD, Balderston RA, Kurtz SM: Total disc replacement positioning affects facet contact forces and
244
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC

Stabilization with the dynamic cervical implant
J Neurosurg Spine Volume 22 • March 2015
vertebral body strains. Spine (Phila Pa 1976) 33:2510–2517, 2008
26. Sasso RC, Smucker JD, Hacker RJ, Heller JG: Artificial disc versus fusion: a prospective, randomized study with 2-year follow-up on 99 patients. Spine (Phila Pa 1976) 32:2933–2942, 2007
27. Tu TH, Wu JC, Huang WC, Wu CL, Ko CC, Cheng H: The effects of carpentry on heterotopic ossification and mobility in cervical arthroplasty: determination by computed tomog-raphy with a minimum 2-year follow-up. Clinical article. J Neurosurg Spine 16:601–609, 2012
28. Welke B, Hurschler C, Schwarze M, Packheiser A, Tak S, Richter B, et al: Biomechanical comparison between fusion, TDR and dynamic stabilization. Paradigm Spine. (Abstract) (http://int.paradigmspine.com/sites/default/files/Biomechan ical%20Comparison%20between%20Fusion,%20TDR%20and%20Dynamic%20Stabilization_0.pdf) [Accessed October 15, 2014]
29. Wigfield C, Gill S, Nelson R, Langdon I, Metcalf N, Robert-son J: Influence of an artificial cervical joint compared with fusion on adjacent-level motion in the treatment of degenera-tive cervical disc disease. J Neurosurg 96 (1 Suppl):17–21, 2002
30. Zigler JE, Delamarter R, Murrey D, Spivak J, Janssen M: ProDisc-C and anterior cervical discectomy and fusion as surgical treatment for single-level cervical symptomatic de-generative disc disease: five-year results of a Food and Drug Administration study. Spine (Phila Pa 1976) 38:203–209, 2013
author contributionsConception and design: Matgé. Acquisition of data: all authors. Analysis and interpretation of data: Matgé. Drafting the article: Matgé. Critically revising the article: all authors. Reviewed sub-mitted version of manuscript: all authors. Approved the final ver-sion of the manuscript on behalf of all authors: Matgé. Statistical analysis: Matgé. Administrative/technical/material support: Matgé. Study supervision: Matgé.
correspondenceGuy Matgé, 25 Rue de la Gare, L-8229 Mamer, Luxembourg. email: [email protected].
245
Unauthenticated | Downloaded 10/19/20 09:39 PM UTC