Spreecast
68
Understanding the Severe Patient What to do when CPAP fails!
-
Upload
markacruzdds -
Category
Health & Medicine
-
view
145 -
download
1
Transcript of Spreecast

Understanding the Severe Patient
What to do when CPAP fails!

Definition: Sleep Disordered Breathing
• A disorder of breathing during sleep only, or significantly affected by sleep. In general, the patient has little or no problem breathing while awake.
• Not a true sleep disorder

Categories
• Mechanical : The inappropriate collapse of the pharynx during sleep– Snoring
– Inspiratory Flow Limitation
– Obstructive sleep apnea
• Chemical : Central Sleep Apnea
• Neuromuscular : paralysis of involuntary muscle (diaphragm) or lack of adequate tidal volume requiring ventilation at night

Continuum of Sleep Disordered Breathing
Mechanical
SeverityLeast MostChemical Neuromuscular

Continuum of Sleep Disordered Breathing:Treatment
SeverityLeast Most
ChemicalCpapVpapOral AppliancesCombinationOxygen
NeuromuscularVentilatorTracheotomyCombination
MechanicalOral AppliancesCPAPCombinationSurgeryTracheostomy

Continuum of Sleep Disordered Breathing:
Treatment Success
SeverityLeast Most
Chemical?
NeuromuscularVentilator +Tracheotomy = 100%?TAP-PAP = 100%?
MechanicalCPAP <50%OA’s >50%TAP-PAP > 95%Tracheotomy 100% ?

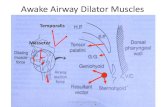
Why is the Passive Pharynx So Important???
© W. Keith Thornton D.D.S.
• Pharyngeal muscles are hypotonic during sleep
• REM sleep causes atonia of pharyngeal muscles.
• Allows the airway to collapse

Sleep Eliminates Pharyngeal Reflexes
© W. Keith Thornton DDS

Physics of Airway Collapse
• Poiseuille's Law– Size of tube and effect on negative pressure to
breath and speed of airflow
• Bernoulli’s law– Increase in speed of airflow decreases size of
flexible tube
• Pathology– Large negative Inspiratory pressure
– And/or total collapse
© W. Keith Thornton D.D.S.

Neuromuscular Factors
© W. Keith Thornton DDS
P mus –P lum > atmosphere
Pharynx Open

Neuromuscular Factors
Pharynx closed
P mus - P lumin < atmospheric
© W. Keith Thornton DDS

Genioglossal EMG in OSA
© W. Keith Thornton DDS

No Mandibular Protrusion (Oshima et al.)
© W. Keith Thornton D.D.S.

Mandibular Protrusion (Oshima et al.)
© W. Keith Thornton D.D.S.

Inspiratory Flow Limitation
© W. Keith Thornton DDS

Esophagealpressure
Inspiratory Flow Limitation : IFL
© W. Keith Thornton DDS
NormalAirflow
Normal
IFL

5 Minutes, RDI 0, T90 = approx. 80%, Severe HypoventilationSevere Inspiratory Flow Limitation, No heart rate variability
Severe IFL, no OSA90%

10 Minutes, Severe, RDI=96
16 events, RDI = 96T90 = approx 20%Little heart rate variability, 50-67

90%
67 bpm
50bpm
2 Minutes, Severe, RDI=96
16 events, RDI = 96T90 = approx 20%Little heart rate variablity 50to 67Lowest desat 83%

90%
67 bpm
50bpm
2 Minutes, Severe, RDI=96
16 events, RDI = 96T90 = approx 20%Little heart rate variablity 50to 67Lowest desat 83%

10 minutes, severe osa, RDI=66
80bpm
40bpm
90%
RDI = 66, T90= 75%, heart rate variability = 40-80Lowest desat= 63

2 minutes, severe osa, RDI=66
80bpm
40bpm
90%
RDI = 66, T90= 75%, heart rate variability = 40-80Lowest desat= 63

RDI = 66, T90= 70%, heart rate variability = 40-80Lowest desat= 63
2 minutes, severe osa, RDI=66
80bpm
40bpm
90%

Patient controlled protrusion

Dose dependent improvement of pharyngeal
collapsibility in response to mandibular advancement
-10
-5
0
5
P’close
(cmH2O)
Velopharynx
-15
-10
-5
0
5
Oropharynx
Kato et al., (2000, Chest)© W. Keith Thornton D.D.S.

0 2 4 6
0.00
0.05
0.10
0.15
0.2010 mm
8 mm
6 mm
4 mm
2 mm
0 mm
0 2 4 6
0.00
0.05
0.10
0.15
Airflow
(L/s)
Preliminary results
Oropharyngeal pressure (cmH2O)
Patient #1
No IFL at 4mm advancementPatient #2
No IFL at 10 mm advancement
(unpublished)
© W. Keith Thornton D.D.S.

Conclusions
© W. Keith Thornton D.D.S.
• Protrusion increases the cross-sectional area
• Protrusion produces a hypotonic genioglossus
• Efficacy is dose dependant

Maximum Protrusion
© W. Keith Thornton D.D.S.
Voluntary
Induced
Stretched

Treatment Position
Maximum protrusion: MP
Maximum passive protrusion: MPP

Original Maximum protrusion 8mm
Present Maximum portrusion 17mm
170% of original maximum
17 mm

23mm 185%
23mm

Macroglossia, Maxillary HypoplasiaSevere IFL
Immediate TAP CS
Increase vertical

Patient History
• Loud snoring, excessive fatigue, several wrecks
• Uncontrolled hypertension, 5 different medications per day
• Morning blood pressure on medication 175/120
• Stroke 5 years previous
• Four psg’s, no osa, no diagnosis, tried and failed cpap
• HST: RDI 3, significant upper airway resistance

Before appliance therapy

After therapy

Macroglossia, Maxillary Hypoplasia
Lateral view,Patient in occlusion
Centric Occlusion

5. Macroglossia, Maxillary Hypoplasia
Narrow arch,High palate without room for tongue
Normal mandibular arch size

Macroglossia, Maxillary Hypoplasia
Size of tongueNormal posture of tongue

Macroglossia, Maxillary Hypoplasia
Normal lip posture Freeway space

Immediate TAP CS
• Moved screw forward to compensate for maxillary hypoplasia
• Opened vertical 15 mm to accommodate tongue
• Patient titrated himself 5mm beyond maximum protrusion in first week
• Blood pressure on awakening 145/90
• No snoring, head aches, fatigue

Immediate TAP CS
15mm
5mm

TAP III from lab
Not enough vertical or protrusive Encroachment on tongue

Final TAP III appliance
Initial vertical 8mmAdded 6mm to plate, 3mm to barTotal vertical, 17mm
6mm 17mm

Neuromuscular Patients
• Post Polio
• ALS
• Muscular dystrophy
• Brain tumors affecting motor function
• Congenital
• Spinal Cord Injuries

Neuromuscular Patients
• Generally need ventilatory assistance during the day
• Paralysis of diaphragm
• Intercostal muscle deterioration
• Limited function of limbs
• Adequate dentition for retention

Neuromuscular Patients:Treatment
• Tracheotomy (medical)
• Custom mask, oral appliance combination (dental)
• No other choices except iron lung

Neuromuscular Patients:History
45 yo, post polioParalyzed from neck downMask developed by DRI using “bite block”Pressure: 45 cmwVolume ventilatorCould use intercostals during dayInserted by biting into trays

Neuromuscular Patients:History
Problems:Fabrication techniquesRetentionLeakageReparabilityBulkTechnique sensitivityCaregiver issues









Treatment of the Severe Sleep Apnic
An eight year history
2002- 2010

Patient: Ron Doe

HPI2003
• Hx of loud snoring starting in dental school
• Recent weight gain of 100 lbs (300 lbs)
• Hypersomnolence
• Acid reflux
• Htn

HPI2003
• Fibromyalgia
• Night sweats
• Joint aches
• Numb feet
• Nocturia

Family and Social Hx
• Divorced and remarried
• Father died at age 51 of HA
– Professional football player with very large neck
• Son and grandchild have osa by symptoms
• Orthodontist
– Focused on treating non-extraction and developing airways
– Very knowledgeable in tmd and occlusion

Treatment Hx
• No initial sleep study or consultation with physician
• Numerous oral appliances tried over 1 yr– Herbst
– Silencer
– Snore guard
– Silent Knight
• Failure of all appliances
• Appliances still fit

Results
Before TAP
After TAP
© 2010 Airway Management, Inc.

TAP III 2010
Plate anterior to upper incisors

PSG 2/2/2009
Diagnostic CPAP alone TAP (4/4/09)
RDI 82.2 23.6 18.2
Minimum O2 Sat 74 77 75
Sleep Efficiency 88.1 65.9 NA
PLM 99 22 NA
Tried Bilevel CPAP at 11/7 cmwCould not tolerate

TAP-PAP 2010
• TAP-PAP custom mask (TPCM)

PSG 12/28/2010TAP TAP-PAP
CustomTAP-PAPUniversal
TAP-PAPNasal
RDI/ AHI 20.7/18.9 2.5/2.5 0/0 0/0
Mean O2 Sat 92.6 % 94% 93 to 94% 94 to 98%
Lowest O2 Sat 86.0% 94% 90% 94%
Time< 90% 4.8% 0% 0% 0%
CPAP pressure 12-13 cmw 9 to 10 cmw 10 to 11 cmw
Comments Inadequately treated alone
Mask leak,Mask was not attached correctly
Sealed well,Preferred by patient