SPOTLIGHT CLE: THE OPIOID EPIDEMIC IN KENTUCKY€¦ · THE OPIOID EPIDEMIC IN KENTUCKY . Sponsor:...
60
SPOTLIGHT CLE: THE OPIOID EPIDEMIC IN KENTUCKY Sponsor: Supreme Court of Kentucky CLE Credit: 1.0 Thursday, June 22, 2017 10:50 a.m. - 11:50 a.m. West Ballroom C-D Owensboro Convention Center Owensboro, Kentucky
Transcript of SPOTLIGHT CLE: THE OPIOID EPIDEMIC IN KENTUCKY€¦ · THE OPIOID EPIDEMIC IN KENTUCKY . Sponsor:...

SPOTLIGHT CLE: THE OPIOID EPIDEMIC IN
KENTUCKY
Sponsor: Supreme Court of Kentucky CLE Credit: 1.0
Thursday, June 22, 2017 10:50 a.m. - 11:50 a.m.
West Ballroom C-D Owensboro Convention Center
Owensboro, Kentucky

A NOTE CONCERNING THE PROGRAM MATERIALS
The materials included in this Kentucky Bar Association Continuing Legal Education handbook are intended to provide current and accurate information about the subject matter covered. No representation or warranty is made concerning the application of the legal or other principles discussed by the instructors to any specific fact situation, nor is any prediction made concerning how any particular judge or jury will interpret or apply such principles. The proper interpretation or application of the principles discussed is a matter for the considered judgment of the individual legal practitioner. The faculty and staff of this Kentucky Bar Association CLE program disclaim liability therefore. Attorneys using these materials, or information otherwise conveyed during the program, in dealing with a specific legal matter have a duty to research original and current sources of authority.
Printed by: Evolution Creative Solutions 7107 Shona Drive
Cincinnati, Ohio 45237
Kentucky Bar Association

TABLE OF CONTENTS The Presenters ................................................................................................................. i Inside Opioid Addiction .................................................................................................... 1 The Heroin Epidemic: There's a New Drug of Choice in Kentucky: Heroin. Fentanyl ........................................ 7 State Strategies for Combatting Heroin and Illicit Fentanyl ............................................ 11 Creating a Region-wide Response to the Opioid Crisis in Western Kentucky ................ 15 Maintenance Medication for Opiate Addiction: The Foundation of Recovery ................ 19 Here's What Trump's New Executive Order Means for Opioid Addiction ....................... 43 Jefferson Foster Care Facts .......................................................................................... 47 Adverse Childhood Experience (ACE) Questionnaire – Finding Your ACE Score ......... 49


THE PRESENTERS
Dr. Allen Brenzel Kentucky Department for Behavioral Health,
Developmental & Intellectual Disabilities 275 East Main Street 4W-F Frankfort, Kentucky 40621
(502) 564-4527 [email protected]
DR. ALLEN J. BRENZEL was appointed the Medical Director for the Kentucky Department for Behavioral Health, Developmental & Intellectual Disabilities with the Cabinet for Health and Family Services in 2010. Prior to 2010 he served as the Medical and Psychiatric Consultant for the Department of Community Based Services (DCBS) and as the Director of the Division of Child and Adolescent Psychiatry at the University of Kentucky. He attended the University of Louisville School of Medicine and completed a combined residency in Pediatrics, Adult Psychiatry and Child Psychiatry at the University of Kentucky. He also completed his Master in Business Administration in 2006. He joined the UK faculty in 1993 where he is an Associate Professor of Psychiatry and Pediatrics. Dr. Brenzel is actively involved in healthcare services reform in Kentucky. This has included working to modernize the State Medicaid Plan to include a full continuum of behavioral health substance abuse services including targeted case management, mobile and residential crisis and peer supports. In partnership with other state agencies, Dr. Brenzel has worked on reducing prescription drug abuse, addressing buprenorphine utilization and diversion, disseminating naloxone rescue kits, and developing guidelines for Kentucky's recently approved Harm reduction and needle exchanges. He is also the CO-PI on the Kentucky MAT-PDOA grant which is providing coordinated care to woman with an opiate use disorder who are pregnant or parenting. In 2017, Dr. Brenzel was actively involved in the submission of Kentucky's SAMHSA response to the Opioid STR grant. This will bring 10.5 million dollars to Kentucky for each of the next two years to address the opioid use disorder crisis in Kentucky.
i

Van Ingram Kentucky Office of Drug Control Policy Justice & Public Safety Cabinet 125 Holmes Street Frankfort, Kentucky 40601 (502) 564-9564 [email protected] VAN INGRAM is the Executive Director for the Kentucky Office of Drug Control Policy. He joined ODCP in November 2004, shortly after it was created with the mission of coordinating Kentucky's substance abuse efforts in enforcement, treatment and prevention/education. Mr. Ingram served with the Maysville Kentucky Police Department for more than twenty-three years, the last six as Chief of Police. He is a former President of the Kentucky Association of Chiefs of Police, and was named "Kentucky Chief of the Year" in 2001. He is the 2004 recipient of the Governor's Award for Outstanding Contribution to Law Enforcement, as well as, the Melvin Shein Award for distinguished service to Kentucky law enforcement. Mr. Ingram is a certified law enforcement instructor and has trained officers across the state on a variety of topics, including community oriented policing, case management, and "Kentucky Substance Abuse Issues" for Chiefs, Sheriff's and command staff. He is a frequent speaker on a variety of substance abuse issues both in Kentucky and nationally.
Chief Justice John D. Minton, Jr. Supreme Court of Kentucky
Warren County Justice Center 1001 Center Street, Suite 305
Bowling Green, Kentucky 42101 [email protected]
CHIEF JUSTICE JOHN D. MINTON, JR. was elected to the Supreme Court of Kentucky in 2006 and re-elected to another eight-year term in 2014. His fellow justices elected him for a four-year term as Chief Justice in 2008, 2012 and 2016. In July 2016, Chief Justice Minton was elected by his fellow chief justices to serve a one-year term as president of the Conference of Chief Justices and chair of the National Center for State Courts Board of Directors. He is also a member of the board of directors for the State Justice Institute, a federal nonprofit corporation that awards grants to improve the quality of justice in state courts. President Obama nominated him to the SKI board and the U.S. Senate confirmed the nomination in December, 2016. Chief Justice Minton was in private practice for fifteen years before serving as a circuit judge from 1992 to 2003 and a Kentucky Court of Appeals judge from 2003 to 2006. He holds degrees from Western Kentucky University and the University of Kentucky College of Law. Chief Justice Minton previously served on the boards of the Conference of Chief Justices and the Council of State Governments and is a 2010 alumnus of the prestigious Toll Fellowship Program, one of the nation's top leadership development programs for state government officials. In 2003, the Kentucky Bar Association honored him with its Outstanding Judge Award. He was named Distinguished Jurist in 2012 by the University of Kentucky College of Law Alumni Association, and was inducted into the Western Kentucky University Hall of Distinguished Alumni in 2013.
ii

Judge Paula F. Sherlock Jefferson Family Court Judicial Center 700 West Jefferson Street Louisville, Kentucky 40202 (502) 595-2232 [email protected] JUDGE PAULA F. SHERLOCK serves as Chief Judge of the Jefferson Family Court. She is a graduate of the University of Northern Colorado and received her J.D. from Washington & Lee University. Judge Sherlock is admitted to practice before the United States District Courts for the Eastern and Western Districts of Kentucky and the United States Supreme Court. She is a member of the Louisville, Kentucky and American Bar Associations, a Master in the Brandeis Inn of Court and serves on the Child Fatality and Near Fatality External Review Panel. Judge Sherlock is the recipient of numerous awards including the Women Lawyers' Association's 2016 Outstanding Judge; Louisville Bar Association's 2015 Outstanding Judge; American Academy of Matrimonial Lawyers' 2014 Outstanding Judge and the 2012 Kosair Outstanding Child Advocate.
Judge David A. Tapp 28th Judicial Circuit
Post Office Box 1324 Somerset, Kentucky 42503
(606) 677-4091 [email protected]
JUDGE DAVID A. TAPP serves as Judge of the 28th Circuit of the Kentucky Court of Justice. He is a frequent presenter on a wide variety of civil and criminal issues and has authored numerous articles and columns associated with justice related issues. Judge Tapp received his J.D. from the University of Louisville, Brandeis School of Law, a M.S. degree from Chaminade University of Honolulu, and his B.A. degree from Morehead State University. In 2011, he received the All Rise Award from the National Association of Drug Court Professionals for his work involving funding issues for substance abuse treatment courts. Most recently, his drug court team became one of only fifteen drug courts (out of 2,700 worldwide) to receive the NADCP's Community Transformation Award for his team's continuing efforts to provide meaningful substance abuse treatment. Judge Tapp is the lead judge for Kentucky's efforts to explore the use of extended release injectable Naltrexone (Vivitrol) as part of a comprehensive opiate drug treatment strategy. He is also the newest appointee to the federal Coordinating Council on Juvenile Justice and Delinquency Prevention. Judge Tapp serves on Kentucky's Criminal Justice Policy Assessment Council which is currently tasked with penal code reform. He currently serves as the chair of Kentucky's Circuit Judges Education Committee and until 2017 served as co-chair of the Judicial Child Fatality Task Force. Judge Tapp has served previously as an adjunct professor at the University of Louisville Brandeis School of Law and currently serves on the University of Louisville Law Alumni Council.
iii

iv

INSIDE OPIOID ADDICTION: 10 QUESTIONS WITH DR. ANDREW KOLODNY Justin Allen
Reprinted from https://www.ket.org/opioids/inside-opioid-addiction-10-questions-with-dr-andrew-kolodny/ (9/9/16)
"With very highly addictive drugs, it's not that there are risky people, it's that the drug itself is inherently addictive." Dr. Andrew Kolodny, a leading expert on opioid addiction, spoke with KET about the opioid epidemic as part of an upcoming one-hour documentary on the crisis in Kentucky and possible solutions. Kolodny is chief medical officer of Phoenix House, a nonprofit addiction treatment organization, and senior scientist at the Heller School for Social Policy and Management at Brandeis University. He is also the executive director and co-founder of Physicians for Responsible Opioid Prescribing (PROP). As a public health official in New York City, he helped to implement overdose prevention, medication-assisted treatment, and other intervention and referral programs. Parts of this interview will be featured in the KET documentary directed by Justin Allen, scheduled to air in early 2017. What Are Opioids and Opiates? What's the Difference? When you hear the term opiate, that's referring to drugs that exist naturally inside opium. Inside opium, morphine exists naturally and codeine exists naturally. When you hear people use the term opioid, that's referring to drugs that come from opium. Heroin comes from opium. Hydrocodone and oxycodone are synthesized from opium, but they've been treated chemically to make them more potent. And the effects that hydrocodone and oxycodone produce in the brain are indistinguishable from the effects produced by heroin. So, when we talk about opioid pain medicine, we're essentially talking about heroin pills. Which doesn't mean that you should never prescribe them. Opioids are very important medicines for treating pain at the end of life. They play a very important role when used after a major surgery for a few days. Unfortunately, the bulk of our prescribing in the United States, and the bulk of our consumption, is for common conditions where opioids may be more likely to harm patients than help them. Heroin Epidemics Are not a New Thing. What Is Different about this One? The opioid addiction epidemic really began in the late 1990s with the introduction of OxyContin. Purdue Pharma, when they put that drug on the market, they were interested in a drug that would bring in lots of revenue on sales. But, when they were introducing OxyContin they had a problem, which was that the medical community understood at that time that opioids are highly addictive drugs.
1

We knew that if you treated common conditions with long term opioids, many patients would get addicted. We knew that patients would develop a tolerance to the pain-relieving effect rapidly, meaning they'd need higher and higher doses. The medical community understood that opioids were not appropriate drugs for these common conditions. What Purdue Pharma did when they were launching OxyContin was to reframe these very good reasons for being concerned about opioids as barriers to compassionate pain care. And they sponsored 20,000 educational programs across the country with messages for the medical community that we were allowing patients to suffer needlessly because of an overblown fear of addiction. … And as the medical community responded to this brilliant marketing campaign, and as the prescribing began to take off, it led to parallel increases in addiction and overdose deaths that led to a public health crisis. Since 1997, we've had a 900 percent increase in opioid addiction in the United States from exposure to opioid pain medicine. What Groups Are at Risk for Opioid Addiction? Do You See any General Characteristics? We have two groups of Americans who have become addicted, an older group and a younger group. The younger group are people who are getting addicted either through medical use of opioid pain medicines or from recreational use, or sometimes from both. That young group, when they get addicted, even if their addiction developed through medical treatment, they have a hard time getting enough pills from doctors to maintain their addiction. So they have turned to the black market, once addicted, to maintain their supply. And the pills are very expensive on the black market. So, if the young person was in a region of the country where heroin was available, they switched, because the heroin produced the same effect and cost much less. And what we've seen happen over the past fifteen years is that heroin has spread across the country into places it was never previously available to meet the demand for it by these young people who first became addicted to prescription opioids. But what's really important to understand, and which doesn't really get reported on very much, is that there's this older group – people over forty who developed opioid addiction, usually through medical treatment for a chronic pain problem. When that older group gets addicted, they don't need to switch to the black market. They can usually find a doctor who will prescribe them all of the opioid pain medicine that they would want. What's not well known is that the overdose death rate is actually significantly higher in the older group than it is in the younger group that's been switching to heroin. The age group with the highest rate of overdose death in the United States is forty-five to fifty-four years old. Yet, many of us think of the opioid crisis as something that's exclusive to young adults. Why Are Opioids not Recommended for Long-Term Use? The problem with using opioids long-term is that tolerance to the pain-relieving effect develops very quickly. So, in order for a patient to continue getting pain relief, the dose has to start going up. And as the dose gets higher and higher, what you often see is that
2

the patient's functioning begins to decline, and patients who may have had all sorts of interests and activities that they had been engaged in, they stop engaging in them. What we now know, especially with data that has come from workers' comp – if you treat an injured worker's chronic pain with long-term opioids, that worker is far less likely to ever go back to work again compared to any other intervention you could have offered them. What we know is that, for most patients with a chronic pain problem, taking opioids on a daily basis for weeks and months and years not only does not help them, it can even make pain worse. It's a phenomenon called hyperalgesia. At the leading pain centers in the United States, at the Cleveland Clinic, at the Mayo Clinic, they treat people who suffer with chronic pain by getting them off of their opioids. How Should We Treat Chronic Pain? Are There Alternatives? There's a tendency to think about chronic pain as a single problem, or to think about chronic pain even as a disease – in fact, the pharmaceutical companies would like us to think about all sorts of common conditions as diseases. Chronic pain isn't a disease, it's a symptom. It can be a sign of a serious disease, and it can be a sign of an underlying problem that needs medical treatment. So, if a patient has a chronic pain problem, the first thing that a clinician should do is try to identify the cause of that pain and treat the underlying condition. The approach really depends on the patient. For some patients, it's necessary to prescribe medicine. And medications that can be just as effective as – or even more effective than opioids, depending on the pain – would be a combination of drugs like Advil and Tylenol. Advil and Tylenol work differently, so it's safe to take them together. It's not as though Advil and Tylenol don't have their own risks – they do. All medicines have risks. But they're sold over the counter for a reason: They really are safer than opioids, and we sometimes forget how helpful they can be. It's almost a rite of passage in the United States to take out wisdom teeth, and dentists prescribe Vicodin to teenagers every time they take out their wisdom teeth. In other parts of the world, in Western Europe, dentists don't give out Vicodin. They give out drugs similar to Advil when they remove wisdom teeth. And drugs like Advil can work just as well, if not better, because they're anti-inflammatory. We've Gotten Ourselves into this as a Country and as a Culture. How Do We Treat this Epidemic? The way that we should handle this disease epidemic is very similar to the way you would handle other disease epidemics – even an infectious disease epidemic. Think about how you would tackle an Ebola outbreak or a measles epidemic. There are really two things you have to do if you're tackling a disease epidemic. First, you have to contain it, meaning prevent new cases of the disease. And then, you have to see that the people who already have the disease are accessing effective treatment so the disease doesn't kill them. And that's basically the approach for the opioid addiction epidemic.
3

We have to prevent new people from getting addicted, and to do that there are different strategies, but the most important are those that will lead to more cautious prescribing. But for the millions of Americans now who are already addicted, we have to see that they can access effective treatments. If we don't, if we just focus on curtailing the overprescribing, we'll succeed in reducing new cases of addiction. But the generation of people who have already developed addiction will continue to suffer a very high rate of overdose deaths, and heroin will continue to flood the market to meet the demand for it. So, we've got to see that those individuals are accessing the right treatment. Talk about Prescription Drug Monitoring Programs. How Do They Fit into Preventing New Cases? Kentucky was at the forefront in mandating that their doctors use a database before writing controlled substance prescriptions. So these prescription drug monitoring programs, or PDMPs, are fantastic tools in addressing our opioid crisis, and they are underutilized. In states where the doctors haven't been made to use the PDMP, very few doctors actually bother to check. Many doctors think they can tell by looking at a patient who may or may not have a problem or who may or may not be visiting multiple prescribers to get pills. And of course they can't. Being able to identify a patient who is visiting multiple prescribers is really important, because if the patient is addicted and you don't know that, your prescription could wind up leading to a loss of life. It's also important to see if the patients are visiting multiple doctors, because they could be somebody who is out there selling the pills on the black market. So, mandatory use of PDMP is one very helpful intervention. After Kentucky mandated that their doctors use the PDMP, Tennessee and New York state also passed similar laws and they've been very helpful. Are There Ways that Doctors Can Identify a Person as Being at Risk for Transitioning from an Opioid to Heroin, or for Developing an Addiction of any Kind? As the opioid addiction epidemic has gotten worse, some states are making their doctors take educational programs on opioids, and unfortunately the content in many of these educational programs is not good. What doctors are not being taught is that opioids are lousy drugs for chronic pain. Instead of being taught not to use opioids for low back pain, chronic headache, fibromyalgia, etc., they're being taught how to use opioids for these conditions. And that teaching is seriously flawed. The idea behind these programs is that these aren't really risky drugs, it's that there's just a subset of our population that's prone to addiction, and we should figure out who they are and be careful with them, and everybody else we don't have to worry about. And that's not true with highly addictive drugs. … With very highly addictive drugs, it's not that there are risky people, it's that the drug itself is inherently addictive. "When most people get an opportunity for treatment, what we often provide them with is detox. We give them tapering doses of methadone over a few days and send them home. And that doesn't work. That's treating the acute withdrawal, and most individuals will relapse and they'll relapse pretty quickly."
4

We've Heard a lot about Addiction Being a Disease, However, There Are Still People Who Aren't Getting that Message. Could You Clarify Why Addiction Is Classified as a Disease, Or Why It Should Be in People's Minds? How Does that Change the Way We Treat It? I think there is a tendency to think about our opioid crisis as a drug abuse problem. I think that suggests that the problem is, we've got a group of people out there behaving badly, taking dangerous drugs because it feels good to take those drugs, and some of them are accidentally killing themselves in the process. That's not what's going on. What we have is a very large increase in the number of people who've developed addiction. Once you've developed addiction – either because you made bad choices or because you were following a doctor's recommendation – once you have that condition, you're not just taking a drug to get a high from it. Without using the drug you're feeling very sick, and it's not just a flu-like illness. When you're going into withdrawal, it's also very, very severe anxiety. It feels like a panic attack. There's this sense of impending doom. People feel like they're truly going to die, like they're losing their mind. It's why they will do very desperate things to maintain their opioid supply. So the idea that people are out there having a good time with these drugs isn't true. The people who are opioid-addicted have a horrible quality of life. Unfortunately, when most people get an opportunity for treatment, what we often provide them with is detox. We give them tapering doses of methadone over a few days and send them home. And that doesn't work. That's treating the acute withdrawal, and most individuals will relapse and they'll relapse pretty quickly. Talk about Medication-Assisted Treatment for Opioid Addiction. What Is the Difference between What Methadone Does and What Buprenorphine and Suboxone Do? Buprenorphine and methadone are similar in that they're both opioids. Methadone is more like the opioid pain medicines that are prescribed in that if you take too much of it, you'll stop breathing and you can die of an overdose. So, it's a dangerous drug, which is why when you're using it to treat opioid addiction, it is almost always given to a patient who's visiting the clinic. In general, it's not prescribed. Buprenorphine is much safer, and works a little differently. It's very hard to overdose on it – it has what we would call a ceiling on its effect. It doesn't slow breathing the way methadone or other opioids will. Buprenorphine has this other unique property, in that it blocks the brain's opiate receptor, so if a patient is taking their buprenorphine or Suboxone – which is another name for it – if they're taking their buprenorphine and they run into a friend who offers them heroin and they try to use the heroin, they won't feel the effect of the heroin, it's blocked. This is very nice when you're treating a condition where people are prone to relapsing. There's very good evidence supporting the use of methadone and buprenorphine. And with buprenorphine, we also have evidence from France that when the drug was released and widely prescribed without the same restrictions we have in the United States, within six years of the release the overdose death rate in France dropped by 80 percent. So, there's good reason to believe that with better access to buprenorphine we could reduce overdose deaths in the United States.
5

This KET article is part of the Inside Opioid Addiction initiative (https://www.ket.org/health/opioids), funded in part by the Foundation for a Healthy Kentucky (www.healthy-ky.org).
6

THE HEROIN EPIDEMIC THERE'S A NEW DRUG OF CHOICE IN KENTUCKY: HEROIN. FENTANYL.
Reprinted from http://odcp.ky.gov/Pages/The-Heroin-Epidemic.aspx Addiction has reached epidemic levels in Kentucky, where painkiller and heroin abuse are rampant. Kentucky is all too familiar with heroin overdoses. Especially hit hard have been Northern Kentucky, Louisville, and Lexington raising fears that the heroin scourge will soon ravage the entire Commonwealth. Heroin—known by the nicknames such as Black Tar, Big H. Dog, Horse, and Puppy Chow, is a highly addictive drug derived from morphine, which is obtained from the opium poppy. Heroin can be injected, smoked in a water pipe, inhaled as smoke through a straw, or snorted as powder through the nose. Heroin is especially deadly because it is both highly addictive and unpredictable. It is also dangerous because there is no way to know exactly what you're buying. A key driver behind the uptick in heroin abuse was the reformulation of two widely abused prescription pain drugs, making them harder to crush and snort. Drug manufacturers reformulated OxyContin in 2010 and Opana in 2011. The growing number of people who began abusing expensive prescription drugs are switching to heroin, which is cheaper and easier to buy. The reason may come down to basic economics: illegally obtained prescription pain killers have become more expensive and harder to get, while the price and difficulty in obtaining heroin have decreased. An 80 mg OxyContin pill runs between $60 to $100 on the street. Heroin costs about $9 a dose. Even among heavy heroin abusers, a day's worth of the drug is cheaper than a couple hits of Oxycontin. Increasingly, heroin is being laced with fentanyl, a deadly and powerful synthetic drug. To impact the problem, the Kentucky Office of Drug Control Policy will continue to work towards increased public education, increased access to treatment, enhanced penalties for major traffickers, and greater access to Narcan (also referred to as Naloxone). FENTANYL Because of its potency and toxicity, fentanyl can kill quickly. It's critical that people call 911 immediately when they suspect someone is having a drug overdose so they can receive a potentially life-saving medication called naloxone. WHAT IS IT? According to the National Institute on Drug Abuse (NIDA), fentanyl is a powerful synthetic opiate analgesic similar to but much more potent than morphine. It is typically used during anesthesia, to treat patients with severe pain, or to manage pain after surgery. It is sometimes used to treat people with chronic pain who are physically tolerant to opiates. It is a schedule II prescription drug. However, recent overdoses have
7

been connected to illegally produced and trafficked fentanyl, not diverted pharmaceutical fentanyl. NAMES* In its prescription form, fentanyl is known as Actiq, Duragesic and Sublimaze. Street names for the drug include: Apache, China girl, China white, dance fever, friend, goodfella, jackpot, murder 8, TNT, or Tango and Cash. EFFECTS* Like heroin, morphine and other opioid drugs, fentanyl works by binding to the body's opiate receptors, highly concentrated in areas of the brain that control pain and emotions. When opiate drugs bind to these receptors, they can drive up dopamine levels in the brain's reward areas, producing a state of euphoria and relaxation—and in some people, the urge to use the drug again and again. Medications called opiate receptor antagonists act by blocking the effects of opiate drugs. Naloxone is one such antagonist. Overdoses of fentanyl should be treated immediately with an opiate antagonist. When prescribed by a physician, fentanyl is often administered via injection, transdermal patch or in lozenge form. However, the type of fentanyl associated with recent overdoses was produced illegally in underground laboratories and sometimes mixed with (or substituted for) heroin in a powder form. Mixing fentanyl with street-sold heroin or cocaine markedly amplifies their potency and potential dangers, including the risk of death. Effects include: euphoria, drowsiness/respiratory depression and arrest, nausea, confusion, constipation, sedation, unconsciousness, coma, tolerance and addiction. SENATE BILL 192 ~ "THE HEROIN BILL" The most talked-about issue of the General Assembly's 2015 session was also a main focus of the late-night closing hours of the session as lawmakers struck an agreement on a comprehensive bill to battle the state's heroin epidemic. Heroin is devastating Kentucky families in a number of ways, and the legislation approved strikes back against the deadly drug on a number of fronts. The multi-prong approach includes stronger penalties for dealers and traffickers and better treatment options for addicts seeking help. Lawmakers approved the legislation, Senate Bill 192, just hours before adjourning the 2015 session in the early morning of March 25. The bill was signed into law later that morning by Gov. Steve Beshear. Since the bill contained an emergency clause, it took effect as state law as soon as the governor signed it. Under the new law, importing heroin into Kentucky with intent to distribute or sell is a crime punishable by up to ten years in prison. Those convicted of selling between 2 grams and 100 grams of heroin will not be eligible for parole before serving at least half of their five to ten years sentences. Those caught selling even more would face sentences of up to twenty years.
8

The new law also recognizes the health crisis that heroin poses and provides new funds to make treatment more widely available to those seeking help. The state's addiction treatment system will receive an immediate $10 million boost followed by $24 million annually. Another newly established tool in the fight against the health problems associated with heroin will permit clean needle exchanges at health departments, if a local jurisdiction approves. Supporters say the needle exchange programs show success in curbing the spread of Hepatitis C and HIV infection from shared needles. The programs also bring addicts into health departments where they'll be closer to the state's network of care and more likely to seek help for their addictions. SB 192 will increase the availability of naloxone, a drug that can reverse the effects of a heroin overdose if promptly administered. The bill also encourages people to call for help when overdose victims need it by including a "Good Samaritan" provision. That will shield people from prosecution when they seek help for someone who overdoses. http://www.lrc.ky.gov/record/15RS/SB192.htm
9

10

STATE STRATEGIES FOR COMBATTING HEROIN AND ILLICIT FENTANYL NGA Center for Best Practices Learning Lab
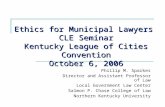
Description of Current Challenge The above DEA map from the period of 1999 to 2001 denotes those areas of the country having the highest numbers of opioid pain killer prescriptions. As you can see, Kentucky has been struggling with the consequences of over exposure to opioids for over fifteen years. Our Commonwealth was the first to pass a number of major policy initiatives that have been replicated in many states. The good news is those policies are working. Overdose deaths caused by legitimate prescription drugs have declined. However, the number of total overdose deaths has risen 16 percent in one year. There were 1,071 deaths in 2014 compared to 1,248 in 2015. The cause of this horrendous increase is clear, illicit fentanyl was present in the toxicology of 420 decedents (34 percent) compared to 121 in 2014. Heroin also remained a major factor being present in 28 percent of all deaths. The largest age demographic in 2015 was 45-54 years old and the second highest was 35-44 years old. These are people that have long struggled with an opioid use disorder. Most started with prescription painkillers, graduated to heroin and then fentanyl in many cases not realizing that the heroin or prescription pill they purchased was actually illicit fentanyl. While it is important to pass laws that slow the number of people exposed to prescription opioids, those efforts do not address the tens of thousands of Kentuckian's already addicted.
11

Like many states, Kentucky cleared the way for liberal naloxone prescribing by physicians, nurse practitioners, as well as pharmacists in 2015. That liberal prescribing has been slow to occur. Cost of naloxone has been a challenge especially in our small rural areas. A lack of understanding of this disease and the view by some that Narcan distribution is enabling drug use also is a barrier. As a state and a nation, we have a lot of work to do to reduce stigma, prejudice and misperception about this disease. Another challenge our state faces is the inability to meet the demand for substance abuse treatment. Although things have improved in recent years, providing treatment on demand is rarely possible. Residential programs have long waiting lists and many areas of the state have limited access to quality medication assisted treatment. Description of Kentucky's Efforts to Address the Opioid Epidemic Kentucky has passed a number of policy measures to address the opioid epidemic. Kentucky was the first state to mandate a prescription drug monitoring query prior to prescribing any controlled substance as well as the first southern state to allow for syringe exchange programs. The Kentucky Injury Prevention Research Center has and continues to assist state government agencies in collecting and interrupting health care data to guide public policy and agency actions. We have worked with the National Governor's Association since 2012 in the first opioid centered policy academy as well as presenting material at subsequent academies. The policy initiative highlights are as follows: House Bill 1: Passed in a special session of the General Assembly in 2012, the bill contained fourteen chapters. The underlying intent of the bill was to ensure that when an opioid is prescribed for chronic non-cancer pain, that the decision is a careful, deliberate, measured choice between prescriber and patient. Highlights of the bill include: 1. Required prescribers use our prescription monitoring program, KASPER. 2. Required CEUs on addiction, treating pain, KASPER etc. 3. Changed requirements for ownership and operation of pain clinics. 4. Required coordination between licensing boards and law enforcement. 5. Required licensing boards to promulgate regulations for the prescribing of
controlled substances. House Bill 217: Passed in the 2013 Regular Session this bill was largely a cleanup bill to HB 1 that placed some items into regulation rather than statute. Senate Bill 192: Passed in the 2015 Regular Session this bill focused on harm reduction strategies and refocused penalties for heroin trafficking. 1. The law created a Good Samaritan provision for persons possessing small
amounts of drugs or paraphernalia that call 911 and stay with an overdose victim.
12

2. The bill also allows for local option syringe exchange and expanded access to naloxone.
3. Tougher penalties were added for traffickers while at the same time creating
avenues for treatment over incarceration for addicts. 4. In addition to the policy reforms, $10 million were allocated for eight programs.
The bill permitted the Department of Corrections to increase substance abuse treatment in state facilities as well as local jails and in the community. In addition, it increased funding for Community Mental Health Centers and organizations that provide treatment for expecting mothers with a substance use disorder. Funds were allocated for local community anti-drug organizations that focus on prevention and treatment programs in their community. Additionally, funds were awarded for the Department of Public Advocacy and the Prosecutor's Advisory Council so defendants in the criminal justice system who would benefit from treatment in lieu of incarceration could be more easily identified. This funding continued and was increased by $12 million in Governor Bevin's 2016-2018 budgets.
In addition to the legislative efforts, Kentucky has done the following: 1. Created seventeen credit hours of online prescriber training on opioids. We will
create twelve additional hours over the next year. Over 3,000 have attended and/or viewed these trainings.
2. Over 193 permanent prescription drug disposal sites in 116 counties have been
created across the Commonwealth to dispose of unused medication. 3. Awarded $375,000 to communities in 2015 in the form of grants to address
overdose prevention at the local level. Those grants will continue and be increased in 2016.
4. Established a program to distribute naloxone kits in the ER (emergency room) of
several major Kentucky hospitals. 5. Partnered with the Kentucky Harm Reduction Coalition to distribute naloxone
kits. 6. Worked with traditional media sources along with social media, town hall
meetings, and statewide trainings to increase awareness. 7. $32 million awarded through a settlement agreement with the Attorney General
and was distributed through grants and direct awards for substance abuse treatment for adolescents and adults.
8. $24 million awarded in an Attorney General settlement with Purdue Pharma and
distributed by the Kentucky General Assembly to substance abuse treatment providers.
13

14

CREATING A REGION-WIDE RESPONSE TO THE OPIOID CRISIS IN WESTERN KENTUCKY
Patrick Reed Reprinted from https://www.ket.org/opioids/creating-a-region-wide-response-to-the-opioid-crisis-
in-western-kentucky/ (3/15/17) The opioid abuse epidemic roiling Kentucky over the past quarter-century has affected different regions in different ways, and with varying degrees of intensity. Eastern Kentucky, the first region in the commonwealth to be crippled by widespread opioid abuse, has been Ground Zero for policy makers as they work to find solutions. In recent years, spikes in opioid abuse in Louisville and Northern Kentucky have motivated government offices to direct more resources to those communities. But there is no part of Kentucky that is untouched by the opioid crisis. Western Kentucky has its own unique set of problems, and community leaders in the Jackson Purchase have banded together to form region-specific solutions to the epidemic under the auspices of the McCracke n County Agency for Substance Abuse Policy (ASAP). As part of KET's Inside Opioid Addiction (www.ket.org/health/opioids) initiative, a production team visited the McCracken County ASAP during their board meeting to learn more about the roots of the opioid abuse epidemic in Western Kentucky, and what measures are being taken to bolster prevention and treatment efforts for at-risk populations. Characteristics of the Epidemic in Western Kentucky The McCracken County ASAP is one of over seventy ASAP groups in Kentucky that gather stakeholders from a community's medical, education, government, and nonprofit sectors to develop programs that curb alcohol, tobacco, and drug use. The county ASAPs grew out of Kentucky's Agency for Substance Abuse Policy, created in 2000 and now operated through the state's Office of Drug Control Policy. County ASAPs receive funding through ODCP, but the individual ASAP boards have the authority to design and implement strategic programs that best fit the needs of their communities with regard to substance abuse. The McCracken County ASAP is organized by the United Way of Paducah, headed by Monique Zuber. During a meeting of the McCracken County ASAP, several members discussed the main aspects of opioid addiction in the Jackson Purchase region. Most agreed that, unlike other areas in the state that have seen a precipitous rise in heroin overdoses, drug cases in far Western Kentucky have to date mainly been a result of prescription painkiller abuse. This is due in part to the larger percentage of older people in the region who may receive opioids for chronic conditions, and to the traditional prescribing habits of area physicians, said several ASAP members. Hydrocodone and oxycodone are still prescribed heavily in the region, often from doctors to patients with whom they have had a decades-long relationship. At the board meeting, Samantha Powell, prevention specialist for Four Rivers Behavioral Health, provided early 2016 data from a Kentucky Incentives for Prevention (KIP) Study.
15

Collecting responses from the nine counties in the Jackson Purchase region served by Four Rivers, the data indicated that outreach efforts to warn teenagers about the dangers of heroin use were effective, but that prescription opioid abuse was still common, as addicts often divert drugs prescribed for illness or injury to recreational uses. Several guests stated during the meeting that, as prescribing opioid painkillers becomes harder, heroin abuse will spike as it has in other regions in Kentucky. "It's happened across the state, and it's going to happen here, too," said Dr. Patrick Withrow, a retired cardiologist and the director of health outreach for Baptist Health Paducah who is a committed advocate for drug prevention and treatment. "There are opioid addicts out there whose supply will dry up from prescription drugs, so they will go to heroin. . . . Some of them have already done it, I'm sure of it. It's probably much worse than we know right now." Emerson Goodwin is the corporate regional director for KentuckyCare, which operates four federally qualified health centers (FQHC) in the region. He said there is a trend among persons who exhibit "pain-seeking behavior" when they visit his clinics – that is, they will engage in risky acts in order to obtain an opioid prescription that allows them to continue using. "We have seen that people will travel," he said. "If they can't get what they want from Clinic A, they will go to Clinic B." The Jackson Purchase's proximity to Missouri poses a problem, according to one ASAP member. Missouri's government does not have a prescription drug monitoring system, unlike Kentucky's, whose KASPER (Kentucky All Schedule Prescription Electronic Recording) online system served as a national model when it was introduced in 2005. Persons seeking to obtain an opioid prescription thus have an easier time if they are willing to make a short trip. Overall, Goodwin said that important steps have been taken to curb painkiller prescriptions, but also cautioned that "I just think we have to do a better job in communicating how difficult it is, once an opioid is prescribed, to manage what happens to it after that." Varied Treatment Programs Prove Effective Later in the meeting, Goodwin discussed KentuckyCare's project that introduces medication-assisted treatment (MAT) programs in each of the region's four FQHCs. He acknowledged that in Western Kentucky there is a reluctance to embrace MAT as a modality for those trying to overcome their opioid use disorder, and several other ASAP members agreed. After studying data on long-term treatment and success rates, Goodwin came to a different conclusion. "Some people may prefer abstinence, and that's okay. For the longest time, we preferred abstinence," he said. "But, as we kept looking at the data and kept talking to experts in this area, we thought – and the need is there – we need to really look seriously at medication-assisted treatment. And that's why we're bringing MAT to market, because we think the data's there that it will help some people. Does it help everybody? No. But, I don't think we know of one thing that helps everybody."
16

Aside from medication-assisted treatment, Goodwin said his KentuckyCare programs also offers behavioral services in association with Four Rivers. He said the programs design an individualized treatment model for each patient, which may incorporate MAT and/or counseling and will "meet each patient where they are." Other treatment facilities in the region include Centerpoint Recovery, which treats men and uses a peer-based approach where successful enrollees can become counselors. Ladies Living Free, a division of Paducah Lifeline Ministries, offers an abstinence-based program for women rooted in Christian principles. The Merryman House in Paducah, which offers comprehensive services to abuse victims, coordinates with area treatment programs to serve its patients when needed. And additionally, ASAP members from both the Paducah Independent School District and Paducah Public Schools also coordinate with Four Rivers and other facilities to help students with issues ranging from their own drug use to how to cope with parents who are addicted to drugs. These programs are succeeding, but more needs to be done to help those suffering from substance use disorder in the face of a persistent stigma about addiction, according to the ASAP members. "People are hesitant to come forward and admit they have a problem because other people continue to look down on addicts," said Ellen Walsh, director of prevention services at Four Rivers. "There's still a lot of controversy, I think, over whether addiction is a disease or not, or if it's a choice. We still hear arguments about that." Bolstering Prevention Going forward, the ASAP members agreed that they and other stakeholders in the Jackson Purchase need to devise and implement comprehensive drug prevention models that help all at-risk groups, starting in the schools and reaching out to families in need. "What I think is really wonderful about Paducah is that we've come together to really provide the kind of wraparound services to families in crisis, to children in crisis, so their futures can look different," said Monique Zuber. "What we're really looking at is prevention, and how can we combat the problem before it gets started. Because we just don't want to treat a symptom. We want to look at the root problem." Ultimately, such a prevention model for the region will be a holistic one that addresses the social conditions that may lead a person to develop behavioral health issues and then turn to opioids for relief. Catherine Fuller, an attorney with Kentucky Legal Aid in Paducah, observed that "every day stressors" such as economic and social instability are triggers for such downward spiral, and that it will take a community-wide effort to assist persons for whom rent, food, and everyday needs are not secure. "People don't know how to cope with it, so they turn their coping skills to drug usage, to try to escape," Fuller said. "And unfortunately, children are affected by it." Dr. Withrow, whose outreach program in conjunction with other prevention advocates has reached more than 2,000 people in area schools and correctional facilities, offered his own perspective on addiction's allure in a broken social system.
17

"One of the things we're having to battle with – you've heard me say it before – is nurture. We're dealing with a lot of families where there's a single parent, not enough money, not enough support, not enough structure, not enough role modeling – the kids are really just behind the 8-ball when they first start," he said. "And if you're dealing with kids like that, that's trouble… The social situation of our families and kids pre-disposes these kids to use. They have a hole in their soul that they're filling with drugs." Jason Amyx, who works with area children through the Necco foster care and social services branch in Paducah, said that he has a constant focus on prevention, which will only succeed if kids know that there is a network of support to help them deal with personal issues when they arise. "We start planting seeds now, that way, if something happens, kids know what to do. They know where to go, they know that there's hope, we've exposed them to alternatives, dealing with stress, seeking out resources, how to choose friends, and the list goes on," he said. "Hopefully, we prevent their situation from getting worse. And if it does get worse, we've given them the tools they need." Several members of the McCracken County ASAP attended KET's Inside Opioid Addiction Forum (https://www.ket.org/opioids/opioid-addiction-forum/) in February 2017 to offer more insight into the opioid crisis in Western Kentucky and their evolving programs in treatment and prevention.
18

MAINTENANCE MEDICATION FOR OPIATE ADDICTION: THE FOUNDATION OF RECOVERY∗
Gavin Bart MD, FACP, FASAM∗∗,∗∗∗ (2012) Journal of Addictive Diseases, 31:3, 207-225, DOI: 10.1080/10550887.2012.694598
Reprinted by permission of Taylor & Francis, LLC (http://www.tandfonline.com).
Illicit use of opiates is the fastest growing substance use problem in the United States, and the main reason for seeking addiction treatment services for illicit drug use throughout the world. It is associated with significant morbidity and mortality related to human immunodeficiency virus, hepatitis C, and overdose. Treatment for opiate addiction requires long-term management. Behavioral interventions alone have extremely poor outcomes, with more than 80% of patients returning to drug use. Similarly poor results are seen with medication-assisted detoxification. This article provides a topical review of the three medications approved by the Food and Drug Administration for long-term treatment of opiate dependence: the opioid-agonist methadone, the partial opioid-agonist buprenorphine, and the opioid-antagonist naltrexone. Basic mechanisms of action and treatment outcomes are described for each medication. Results indicate that maintenance medication provides the best opportunity for patients to achieve recovery from opiate addiction. Extensive literature and systematic reviews show that maintenance treatment with either methadone or buprenorphine is associated with retention in treatment, reduction in illicit opiate use, decreased craving, and improved social function. Oral naltrexone is ineffective in treating opiate addiction, but recent studies using extended-release naltrexone injections have shown promise. Although no direct comparisons between extended-release naltrexone injections and either methadone or buprenorphine exist, indirect comparison of retention shows inferior outcome compared with methadone and buprenorphine. Further work is needed to directly compare each medication and determine individual factors that can assist in medication selection. Until such time, selection of medication should be based on informed choice following a discussion of outcomes, risks, and benefits of each medication. KEYWORDS. Review, opiate, addiction, methadone, buprenorphine, naltrexone, pharmacotherapy Opiate dependence (hereafter referred to as addiction) is a major public health problem with global reach.1 The illicit use of opiates contributes to the global burden of disease and can result in premature disability and death.2 Overdose is a significant cause of
∗ This work was supported in part by NIH-NIDA K23 DA024663. Address correspondence to Gavin Bart, MD, FACP, FASAM, Department of Medicine, Hennepin County Medical Center, 701 Park Avenue, Minneapolis, MN 55415. E-mail: [email protected] ∗∗ Division of Addiction Medicine, Hennepin County Medical Center, Minneapolis, Minnesota, USA. ∗∗∗ Department of Medicine, University of Minnesota, Minneapolis, Minnesota, USA.
19

death and the incidence and prevalence of blood-borne viruses (e.g., human immunodeficiency virus [HIV], hepatitis B, and hepatitis C) are higher in illicit opiate users, especially injection drug users, than the general population.3-7 In the United States, deaths related to opiate analgesic overdose now exceed those caused by heroin and cocaine combined.8 Access to, adherence to, and outcomes for the treatment of general medical illness and infectious diseases such as HIV, viral hepatitis, and tuberculosis are reduced in opiate addicts. Globally, between 24 and 35 million adults aged 15-64 years used an illicit opiate in 2010.9 Throughout Europe and Asia, opiate use is the primary reason for seeking treatment for illicit drugs.9 Although relative global stability has been seen in prevalence of illicit opiate use, the United States has seen a significant increase in the illicit use of prescription opiates despite stable levels in heroin use.9,10 In 2009, in the United States, opiates were second only to alcohol as the primary reason for treatment admission.11
From 1999 to 2009, annual treatment admissions for opiates increased from approximately 280,000 to 421,000 individuals.11 The increase in prescription opiate use, overdose deaths, and treatment admissions parallels increases in production and distribution of prescription opiates.8
The addiction liability of opiates is high, with 50% and 11% of people who used heroin or prescription opiates, respectively, last year meeting addiction criteria.12 The focus of this review is on the pharmacologic treatment options for individuals addicted to opiates. A brief discussion of the neurobiology of opiate addiction will be followed by description of the role current Food and Drug Administration (FDA)-approved treatments for opiate addiction have in facilitating recovery. Economic, ethical, and regulatory issues surrounding these medications are beyond the scope of this review and will not be discussed. NEUROBIOLOGY OF OPIATE ADDICTION The risk for developing opiate addiction is a complex interaction between genetics, environmental factors, and the pharmacological effects of opiates. For example, selective breeding in rodents has produced strains prone to opiate self-administration; multiple genetic loci associated with opiate self-administration have been identified; and selective disruption of the gene encoding the mu opioid receptor, the principal target of opiates, can eliminate opiate self-administration and conditioned place preference.13
Human family and twin studies have identified increased genetic risk for addiction in the first-degree relatives of addicts but also that the genetic risk specific to opiate addiction is second only to that for alcoholism.14,15 Environmental factors such as availability of opiates, perceived risk of opiate use, psychosocial stressors, and learned coping strategies influence the risk of developing opiate addiction. For example, the incidence of opiate addiction has paralleled the increased availability opiates. Although 75% of high school seniors perceive using heroin once or twice as dangerous, only 40% perceive similar use of prescription opiates as dangerous.16 Traumatic lifetime experience may increase the risk for opiate addiction. In rodent models, maternal separation early in life increases vulnerability to opiate addiction for the pup and the dam and, in humans, weak parental bonds increase the risk for illicit drug use during adulthood.17-19 In humans, an association exists between posttraumatic stress disorder and opiate addiction, with an overrepresentation in the
20

prevalence of this disorder in opiate addicts compared with the general population and to those with other substance use disorders.20
The euphoria and abuse liability of an opiate is related to its pharmacokinetic and pharmacodynamic properties. The rapidity with which a drug enters and then exits the brain is positively correlated with its rewarding and reinforcing effects.21-23 This principal is clinically apparent in the transition from oral or intranasal to smoked or intravenous routes of drug administration and through the practice of crushing extended-release tablets to achieve more immediate opiate absorption. Once in the brain, the primary target for abused opiates is the mu opioid receptor. This receptor is present throughout the brain, with highest density in areas modulating pain and reward (e.g., thalamus, amygdala, anterior cingulated cortex, and striatum). Activation of mu opioid receptors inhibits gamma-aminobutyric acid (GABA)-mediated tonic inhibition of dopaminergic neurons in the ventral tegmental area.24 This initiates a cascade of effects in diverse brain regions, including the striatum, amygdala, and prefrontal cortex, that are not only related to reward but also influence the risk for repeated opiate use by heightening the saliency of drug-related cues and the incubation of drug craving.25,26 Repeat opiate administration induces tolerance and imparts the potential for a withdrawal syndrome upon cessation. The unpleasant physical and psychological symptoms of withdrawal produce negative reinforcement whereby opiates continue to be used, often in escalating doses, to avoid their onset.27 Furthermore, short-acting opiates modulate stress responsive pathways causing dysregulation and further stress-induced negative reinforcement. This stress dysregulation can continue long after a person has discontinued opiate use and, therefore, is a contributing factor to the risk for relapse during stress. Long-term approaches to the treatment of opiate addiction are required because of persistent alterations in dopaminergic, opioidergic, and stress responsive pathways. Human imaging studies have identified ongoing reductions in dopamine D2 receptor binding potential in opiate addicts and that this reduction correlates with the duration of opiate use.28,29 Animal models of opiate addiction and post-mortem studies in human opiate addicts have identified alterations in opioid gene expression in specific brain areas related to reward and behavior.13 Finally, stress response is exaggerated in former heroin addicts who are not taking methadone pharmacotherapy.30 Although pharmacotherapy may not correct alterations in dopamine receptor availability and opioid gene expression, it does appear to normalize several aspects of stress responsiveness.31-33 The advent of epigenetics has allowed us to gain understanding as to how genetic expression is modified by environmental and pharmacological inputs, linking all three main contributors to the risk for addiction. For example, environmental inputs such as maternal care or social hierarchy modulate expression of neuroreceptors that, in turn, influence drug selfadministration.34,35 Opiate administration also modulates expression of several genes including those in opioidergic, dopaminergic, and stress responsive pathways.13 The details of how the interaction between genes, environment, and drugs contributes to the development, persistence, and relapse to addiction have yet to be elucidated. This interaction forms the hypothesized foundation for the persistence of addiction vulnerability even in those who have discontinued drug use and indicates that long-term relapse prevention strategies need to include environmental and pharmacological interventions beyond the immediate period of withdrawal.
21

PSYCHOSOCIAL INTERVENTION ONLY Although this review does not comprehensively address non-pharmacological interventions for opiate addiction, when used alone, these approaches should be considered to lie outside the domain of first-line evidence-based treatment. Historical data indicate poor outcome in patients provided only psychosocial interventions. Whether compelled or voluntary, return to opiate use approaches 80% within 2 years of intensive residential treatment.36,37 Although a systematic review by the Cochrane collaboration indicates some psychosocial interventions may be superior to others, a separate review found that psychosocial intervention alone was inferior to methadone maintenance for outcomes such as retention in treatment and reduction in opiate-positive urine toxicology tests.38,39 This later review also indicated a trend for greater mortality in psychosocial versus methadone treatment, a finding supported in other reports from populations that receive no treatment, psychosocial treatment only, or those who voluntarily discontinue pharmacotherapy.40-44 MEDICALLY ASSISTED DETOXIFICATION The negative reinforcement of withdrawal is a primary driver of ongoing drug use. Several strategies to relieve opiate withdrawal symptoms have been evaluated. The short-term (first 30 days) effect on relief of symptoms and return to illicit opiate use between alpha adrenergic agonists such as clonidine and lofexidine (and presumably dexmedetomidine) and opiate-based regimens are similar.45 Rapid withdrawal and sedation-assisted transition to opioid antagonist therapy has an increased risk of serious adverse events when performed under heavy sedation and is too resource intensive to endorse given the limited benefit when performed under light sedation.46,47 A longer period of detoxification (1 to 6 months) with methadone or buprenorphine are also ineffective in promoting abstinence beyond the initial stabilization period.48,49 MEDICATIONS USED TO TREAT OPIATE ADDICTION BEYOND THE WITHDRAWAL PERIOD Methadone, buprenorphine, and naltrexone are each FDA approved for the long-term treatment of opiate addiction (Tables 1 and 2). Methadone has been used for the longest period of time and thus has a large body of research supporting its effectiveness. Buprenorphine is similar to methadone in mechanism of action (partial agonist versus full agonist) and effectiveness and thus will be discussed in a slightly abbreviated manner. Naltrexone, an opiate antagonist, has a less of an historical basis for effectiveness but newly evolving literature warrants attention. Methadone Methadone is a synthetic mu opioid receptor agonist originally synthesized in the late 1930s as a congener of atropine.50 In the treatment of opiate addiction, methadone is administered orally in liquid, tablet, or dispersible tablet formulation and is a racemic mixture whose R- entantiomer is responsible for the opioid effect and both R- and S-entantiomers are N-methyl-D-aspartic acid (NMDA) antagonists. Following oral administration, it is rapidly absorbed, undergoes little first pass metabolism, and has moderate bioavailability of 70% to 80%. Methadone is approximately 90% bound to plasma proteins such as albumin, globulin fragments, and α1-acid-glycoprotein. Methadone is also distributed throughout various tissues, such as the liver, intestine,
22

lung, muscle, and brain, with an apparent volume of distribution during steady state of 3.6 L/kg. Following oral administration, peak plasma levels are reached within 2 to 4 hours, and the elimination half-life at steady state is approximately 28 hours, allowing for once-daily dosing. Methadone is hepatically metabolized into inactive compounds primarily by cytochrome P450 3A4 and 2B6 enzymes and is eliminated through both renal and fecal routes. The use of certain medications that induce (e.g., phenytoin, rifampin, efavirenz) or inhibit (e.g., azole based antifungals) these enzymes may affect plasma methadone levels, although the clinical effect in terms of precipitating withdrawal or inducing sedation are variable. Methadone safety is well established.52 Like other opiate agonists, methadone has the potential to induce lethal respiratory suppression when given in doses that exceed an individual's tolerance. Recent increases in methadone-associated deaths are primarily related to its minimally regulated use in the treatment of pain and not due to its use in the treatment of opiate dependence.53 This may be due to too rapid dose escalations and a differential rate in development of tolerance to the analgesic and respiratory suppressive effects of methadone. In the setting of addiction treatment, higher levels of dosing supervision reduce mortality rates.54 Recent concern exists regarding potential cardiac safety of methadone. Although methadone will increase the electrocardiographic QTc interval, this appears minimal in magnitude and rarely exceeds the 500 msec threshold associated with cardiac arrhythmia and sudden death in those with heart disease.55,56 Evidence that preventing cardiac events through electrocardiographic monitoring or use of buprenorphine, which likely does not prolong the QTc, is lacking.57 Therefore, it appears that the greatest risks in mortality associated with methadone maintenance occur during the induction period because of multiple drug ingestion (e.g., benzodiazepines) or due to the loss of tolerance with subsequent overdose on methadone discontinuation.43
Methadone's ability to relieve the opiate withdrawal syndrome was noted as early as 1947, and within 2 years it became the preferred medication for detoxification at the national narcotics hospital in Lexington, Kentucky.58 On taking methadone, opiate addicts in withdrawal found their symptoms relieved; those with active addiction did not experience euphoria or request their usual and available doses of injected morphine and, after chronic administration, sudden cessation of methadone produced a milder, albeit longer in duration, withdrawal syndrome than following morphine cessation.59
23

TABLE 1. Clinical Characteristics of Methadone, Buprenorphine, and Naltrexone Methadone Buprenorphine Naltrexone Controlled substance Yes Yes No Availability OTP OTP or DATA
Waived practitioner
Any prescribing practitioner
1-year retention 60% 60% 20% (53% 6-months ER)
Direct expense $ $$ $$-$$$$ Dosing frequency Daily Daily Daily or monthly (ER) Narcotic blockade Yes, at
steady-state Yes, at
steady-state Yes
Can induce withdrawal No Yes Yes Overdose potential Yes Yes No Withdrawal upon cessation Yes Yes No Loss of tolerance upon cessation Yes Yes Yes Complicates treatment of moderate-severe pain
No No Yes
OTP = opiate treatment program; DATA = Drug Addiction Treatment Act of 2000; ER = extended-release formulation It was not until 1964 when scientists at the Rockefeller Medical Research Institute (now University) began to evaluate methadone maintenance as a means of long-term medication-assisted treatment for opiate addiction. This work helped establish that not only did methadone relieve opiate withdrawal but, when at steady-state, it also blocked the euphoric and sedating effects of superimposed opiates.60,61 Thus, with methadone, major components of both the positive and negative reinforcing effects of short-acting opiates were reduced and craving subsided, allowing the addict to concentrate on non-drug-related activities. Methadone response appears to be dose related, with most patients stabilizing at doses between 60 and 120 mg daily.62 Response is most frequently measured in terms of retention in treatment and reduction in illicit opiate use, although improvements in psychosocial function and medical status have also been documented.63 Mean 1-year retention in treatment is approximately 60% and can vary based on adherence to evidence-based dosing practices.64–67 In terms of retention in treatment and adherence to treatment regimen, the results of methadone maintenance are similar to or exceed results for other medically managed diseases, such as hypertension, dyslipidemia, and diabetes mellitus.68 At any given time during treatment, approximately 15% of patients in methadone maintenance will have ongoing illicit opiate use. Although some associations are found between treatment outcome and age, medical comorbidity, criminal justice involvement, ongoing non-opiate drug use, and patient satisfaction with treatment, predicting and then preventing treatment failure has not proved successful.67,69-72 Providing intensive psychosocial services and counseling may improve treatment outcomes during the initial 6 months of methadone maintenance but its benefit diminishes through time such that patients receiving intensive services have similar incidences of drug use at 1 year as those receiving standard counseling.73
24

TABLE 2. Pharmacological Profile of Methadone, Buprenorphine, and Naltrexone Methadone Buprenorphine Naltrexone Main effect Mu full agonist, NMDA
antagonist Mu partial agonist Mu antagonist
Bioavailability 70%-80% 50% <50% (approximately 100% ER)
Half-life 28 hours 37 hours 9 hours (4.95 days ER) Clinically apparent drug interactions
Rifampin, phenytoin, several ART
Select ART Opioids, NSAIDS (?)
Active metabolites None Nor-buprenorphine 6-beta-naltrexol ART = antiretroviral therapy; NSAID = non-steroidal anti-inflammatory; ER = extended-release formulation; NMDA = N-methyl-D- aspartic acid. Methadone maintenance is not the replacement of an illegally used opiate for a legally supervised opiate. Unlike abused opiates, once a stabilization dose is achieved (generally between 60 and 120 mg daily), rarely is it needed to increase the dosage due to tolerance development. The reason for this is unknown but may be related to its NMDA antagonist properties.74 In addition, at stabilization, methadone binds approximately 30% of mu opioid receptors, allowing the remaining receptors to perform their usual physiological function in modulation of pain, reward, and mood.75 In addition, the psychosocial problems inherent in opiate addiction are also relieved during methadone maintenance. Regulation of stress response is one such function that tends to normalize with methadone stabilization. For example, suppression of adrenocorticotropic hormone (ACTH) and corisol caused by administration of short-acting opiates, blunted diurnal variation in their release in active addicts, and the increase in these hormones during opiate withdrawal are all corrected during methadone maintenance (Table 2).52,76,77 Perhaps most importantly, many of the abnormal hormonal responses to stressors during addiction and even following abstinence-based treatment are corrected once patients are stabilized on methadone.78 Thus although methadone relieves withdrawal and blocks the effect of superimposed opiates, it may more importantly be thought of as a relapse prevention drug in that it normalizes many of the physiological stress-related responses that precede and contribute to relapse (Table 3). Buprenorphine Buprenorphine is a semi-synthetic mu opioid partial agonist with weak partial agonist effects at delta and kappa opioid receptors. It was first synthesized in the late 1960s by Bentley et al.79 as part of analgesic explorations of thebaine congeners. In the treatment of opiate addiction, buprenorphine is administered sublingually in tablet or film formulations. A new subdermal implant that delivers buprenorphine for 6 months is in development and showing promise in the treatment of opiate addiction.80 Buprenorphine undergoes extensive first-pass metabolism and oral administration results in poor bioavailability. However, following sublingual administration, bioavailability is approximately 50%.81 Buprenorphine is extensively protein bound to globulin fragments and is distributed to various tissues with an apparent volume of distribution during steady state of 3.7 L/kg. Following sublingual administration, peak plasma levels are reached within 1 to 3 hours and the elimination half-life at steady state is approximately 37 hours, allowing for once daily, and in some instances every other day, dosing. Buprenorphine is hepatically metabolized by cytochrome P450 3A4 and possibly 2C8 into the weak opioid partial agonist norbuprenorphine, which is eliminated through glucuronidation.82 Both buprenorphine and norbuprenorphine are eliminated through renal and fecal routes. The
25

use of certain medications that induce or inhibit cytochrome P450 3A4 may affect plasma buprenorphine levels, although the clinical effect of this is minimal possibly due to buprenorphine's partial agonism, high receptor affinity or because of the weak opioid effects of norbuprenorphine.51
The literature on safety evaluation of buprenorphine maintenance is less developed than that of methadone, but phase III research reports indicate that buprenorphine maintenance is safe, with equivalent adverse events to methadone and placebo.64,66,83 Although buprenorphine is a partial agonist at mu opioid receptors, it may induce respiratory suppression but to a lesser extent than full agonists.84 In addition, as a partial agonist with high receptor affinity and modest efficacy, many of buprenorphine's effects plateau after approximately 16 mg, although doses of up to 32 mg are used clinically.84
Thus, although it may have similar rewarding properties as methadone in nontolerate opiate addicts, attempts to increase this effect or achieve intoxication through dose escalation beyond this ceiling are of little avail.85 Nevertheless, deaths associated with buprenorphine have been reported following its more rapid delivery through injection or when combined with benzodiazepines.86 To reduce the harm associated with buprenorphine injection, it is available in formulations that combine buprenorphine with the opioid antagonist naloxone in a 4:1 ratio. Naloxone undergoes extensive first-pass metabolism and is not absorbed into the systemic circulation when taken orally or sublingually. However, injection allows naloxone to enter systemic circulation and compete with buprenorphine for receptor occupancy. This competition reduces the initial effects of buprenorphine, lowering its rewarding properties and the risks of lethal respiratory suppression.87 As with methadone, deaths in buprenorphine maintenance patients are more likely to occur during the initial induction period or due to loss of tolerance following its discontinuation.43
TABLE 3. Stress Response Hormones
Adrenocorticotropic hormone
Cortisol
Short-acting opiates ↓
↓
Opiate withdrawal ↑
↑
Methadone ↔ ↔ Buprenorphine ↔ ↔ Naltrexone (oral) ↑ ↑
Naltrexone (extended release) ? ? ↑= stimulate; ↓= suppress; ↔ = no change.
Buprenorphine's ability to both induce and relieve opiate withdrawal was observed by Martin et al.88 in 1976, and within 2 years Jasinski et al.89 hypothesized that it may be used in the treatment of opiate dependence. Because buprenorphine is a high affinity and moderate efficacy mu opioid partial agonist, it will displace other high efficacy opiates, if present, and induce withdrawal symptoms. On the other hand, when a patient has stopped using opiates and is in withdrawal, buprenorphine will bring relief through its partial agonist effect. Because of this dual effect, induction onto buprenorphine has the potential to precipitate withdrawal. It is, therefore, generally advised that the first dose of buprenorphine be given no sooner than 12 hours after the last use of a short-acting
26

opiate and 24 hours after a long-acting opiate, which may be difficult for many patients to achieve. Various induction protocols ranging from inpatient to outpatient monitoring for withdrawal symptoms prior to first dose to patient-driven home induction are available to help clinicians safely induce patients onto buprenorphine.90,91 Following chronic administration, sudden cessation of buprenorphine produces a mild yet prolonged withdrawal syndrome.89 Although several early reports found that buprenorphine could relieve opiate withdrawal and block the effect of superimposed opiates, it was not used as a maintenance treatment until 1985.89,92,93 As with methadone, on relief of withdrawal and craving, patients on buprenorphine maintenance turn their focus to nonaddiction-related activities. Unlike methadone, buprenorphine is not highly regulated so most studies have evaluated buprenorphine maintenance in a primary care setting. Buprenorphine response is dose related, with most patients stabilizing at doses between 12 and 16 mg daily.64,94 When adequate doses are used, treatment outcome in terms of retention and reduction in illicit opiate use is similar to that of methadone maintenance.95 Unlike methadone, where the dose can be increased to facilitate treatment response, buprenorphine's ceiling effect may limit its effectiveness in patients with ongoing opiate use.96 In these individuals, transitioning from buprenorphine to methadone may allow for an improved treatment outcome. Also, the role of intensive counseling does not appear to improve the outcome of office-based treatment compared with standard counseling.96,
97 Little difference is found in outcome between office-based and opiate treatment program settings, although direct comparison of a randomized population has yet to be performed. A weakness in the buprenorphine literature is that most study follow-up periods are between 12 and 24 weeks. In these studies, retention rates are similar to that of methadone over the same period of time.98 Whether this similarity persists for 1 year is uncertain. One small but dramatic program-based placebo-controlled study found 1 year retention of 75% and 0% for buprenorphine and placebo, respectively.41 In addition, all patients receiving the placebo dropped out by 3 months and 4 of 20 patients had died by the end of the year, whereas no patients receiving buprenorphine died. Aside from ongoing opiate use, predictors of buprenorphine treatment outcome may include depression, income, and ongoing cocaine use.69 Recent attention has been placed on the use of buprenorphine for the treatment of prescription opiate addiction.97 During maintenance treatment, patients have reduced illicit opiate use, but following buprenorphine taper, more than 90% of patients return to illicit opiate use.97 In another study comparing heroin addicts to prescription opiate addicts, the heroin addicts had more severe medical and addiction severity and did not do as well with buprenorphine as the less ill prescription opiate addicts.99 Caution in interpreting this finding is warranted because these two populations are not comparable, and the difference in outcome may be more related to addiction severity than to the patient's opiate of choice. No neurobiological or pharmacological reason exists for why, after adjusting for these factors, heroin addicts and prescription opiate addicts would have different treatment outcomes and require separate consideration in medication choice. The neurobiological effect of buprenorphine in the treatment of opiate addiction is presumed to be mediated through partial agonism of the mu opioid receptor. The effect at delta and kappa receptors is likely too weak to contribute to its treatment
27

effectiveness. Buprenorphine binds extensively to mu opioid receptors, with more than 90% occupancy following doses of 16 mg or more.100 Buprenorphine can suppress stress-responsive hormones such as adrenocorticotropic hormone and cortisol when administered acutely to healthy control patients.101 When stabilized methadone-maintained patients were transitioned to buprenorphine, basal levels of beta-endorphin remained normal.102 It appears that most stress-responsive markers are normalized in buprenorphine-maintained patients, and that failure to normalize correlates with craving and relapse.103,104 Thus, as with methadone, the role of buprenorphine in the treatment of opiate addiction is not simply the replacement of an illicitly used opiate for a medically supervised opiate, but rather as a medication that corrects many of the neurobiological processes contributing to relapse. Naltrexone Naltrexone is a semi-synthetic mu and kappa opioid receptor antagonist synthesized in the mid-1960s as a congener of oxymorphone.105 In the treatment of opiate addiction, naltrexone is administered either orally in tablet formulation or intramuscularly in an extended-release formulation. Following oral administration, it is rapidly absorbed but undergoes significant first-pass metabolism with a bioavailability less than 50%.106
Naltrexone has a low protein binding capacity and an apparent volume of distribution of approximately 19 L/kg. Peak plasma levels following oral administration are reached within 4 hours, and the elimination half-life at a steady state is approximately 9 hours.107 Naltrexone is reduced to the weak opioid antagonist 6β-naltrexol in the liver. Naltrexone, 6β-naltrexol, and their conjugates are renally eliminated, with less than 3% recovered in the feces.107 No known drug interactions exist that would alter naltrexone metabolism and thus limit its use. Naltrexone safety is well established. Some reports have been made of hepatotoxicity following high-dose naltrexone and caution is advised in prescribing naltrexone in the setting of acute hepatitis or end-stage liver disease.108 Unlike methadone and buprenorphine, naltrexone is not behaviorally reinforcing in individuals without opiate tolerance and does not induce respiratory suppression. Because it is an opioid antagonist, naltrexone may precipitate withdrawal in patients with physical dependence on opioids. The initial hypothesis for the use of opioid antagonists in the treatment of opiate addiction was as a means of eliminating a conditioned response to use opiates.109 Based on this hypothesis, return to opiate use following detoxification is caused by negative reinforcement of environmental stimuli (e.g., cues and social stressors), and if an antagonist prevented the addict from relieving this negative state through opiate use, then the behavior of turning to opiates in these situations would eventually cease. Indeed, naltrexone can block the effect of superimposed opiates for approximately 24 to 48 hours after oral dosing.110 The plasma levels sufficient to block 25 mg of heroin are approximately 1 to 2 ng/mL, a level maintained for 21 to 28 days following 380 mg of the intramuscular extended release formulation.111 As early as 1976, National Institute on Drug Abuse convened a workgroup to study and promote the development of oral and extended-release naltrexone as a treatment for opiate addiction.112 Early and successive work found that naltrexone was well tolerated with few adverse effects other than mild nausea. Patients taking naltrexone reported fewer days of heroin use and had few opiate-positive urine drug tests.113 Patient
28

adherence and drop out has been a major stumbling block for oral naltrexone. In multiple studies of either daily or thrice weekly dosing, fewer than 20% of patients remain in treatment for 6 months.113-115 A Cochrane collaboration meta-analysis found that due to extensive drop-out rates, oral naltrexone maintenance with or without psychotherapy was no better than placebo treatment.116 Extended-release naltrexone may improve treatment outcome because nonadherence to daily oral regimens is reduced by delivery of a once monthly injection. Currently, limited data exist regarding the extended-release intramuscular injection. In a 2-month randomized placebo controlled trial, only 70% of patients were retained for 8 weeks.117 A larger trial in Russia retained 53% of patients at 6 months compared with 38% for placebo.118 Patients receiving extended-release naltrexone also had significantly fewer days of illicit opiate use. Although intramuscular naltrexone is the only FDA-approved extended-release formulation, literature on subdermal implants capable of maintaining naltrexone plasma levels between 1 to 2 ng/mL for 6 months may also contribute to our understanding of the role naltrexone may play in the treatment of opiate addiction. These studies have shown retention of approximately 60% at 6 months, exceeding that of oral naltrexone.119,120 Illicit opiate use was also significantly reduced; however, in one study, patients receiving the implants had a higher rate of non-opiate drug use than those receiving methadone.121 The use of naltrexone in the treatment of opiate addiction is mechanistically different from that of methadone and buprenorphine. Each medication can block the effect of superimposed opiates and, following steady-state oral administration, naltrexone achieves approximately 95% mu opioid receptor occupancy.122 Unlike methadone and buprenorphine, naltrexone is without intrinsic opiate activity and poses minimal risk of abuse or diversion. What may be most compelling about naltrexone comes from the literature on its use in the treatment of alcoholism, where it reduces craving, a frequent predecessor to relapse. In fact, reduction in base-line craving is correlated with its effectiveness.123 Naltrexone's effect on craving in opiate addicts is less clear. Oral naltrexone may not reduce craving more than a placebo and, if it does, this reduction does not necessarily correlate with abstinence.124,125 Failure of oral naltrexone to prevent relapse in opiate addicts may be related to ongoing stress dysregulation and is supported by animal research showing its failure to suppress stress-induced relapse.126
Although methadone and buprenorphine can normalize stress response, naltrexone may not. In fact, oral naltrexone administration stimulates adrenocorticotropic hormone and cortisol, even following chronic administration.127 This stimulation mimics the hormonal response during opiate withdrawal. It also mimics the response to acute administration of alcohol, which may explain oral naltrexone's effectiveness for alcohol but not opiate addiction.128 Whether extended-release naltrexone has a similar effect on stress response remains unknown, but its ability to reduce craving is promising.118
Methadone, Buprenorphine, Naltrexone Direct Comparisons No randomized double-blind controlled trials exist comparing all three medications. One randomized trial comparing each of the medications found 24-week retention rates of 84%, 59%, and 21% for 50 mg of methadone, 5 mg of buprenorphine, and 50 mg of naltrexone, respectively, despite suboptimal doses of methadone and buprenorphine.129 A comparative study between buprenorphine and oral naltrexone found naltrexone response to be inferior.130 No comparative outcome studies exist between extended-release naltrexone and either methadone or buprenorphine. It has been observed that
29

the 6-month retention rates following extended-release naltrexone are similar to the 1-year retentions in methadone maintenance and thus non-inferiority studies of extended-release naltrexone are needed.131 Special Populations End-Stage Liver Disease Decreased hepatic metabolism and plasma protein can lead to increased methadone clearance,132 which may result in the onset of withdrawal symptoms and can be prevented by increasing methadone dose. Because this will also increase methadone peak levels, it may result in sedation. If this occurs, the methadone dose may be split into two doses taken during the course of the day. No formal studies exist of buprenorphine pharmacokinetics in end-stage liver disease. Given the long half-life and active metabolites of buprenorphine, it is unclear whether a dose adjustment is needed for patients with end-stage liver disease. FDA labels for both oral and intramuscular naltrexone recommended against their use in the setting of end-stage liver disease. Pregnancy The placenta is metabolically active and can increase clearance of both methadone and buprenorphine. Because methadone does not have active metabolites, patients may experience early withdrawal and may require increases in or splitting of methadone dose during the second and third trimesters.133 It is recommended that neither naloxone nor naltrexone be administered during pregnancy, although each are Category C drugs, thus buprenorphine should be administered as the mono product and naltrexone should be avoided. Methadone and buprenorphine are associated with improved maternal and fetal outcomes compared to abstinence based approaches. Although the recent MOTHER trial found that the length, but not intensity, of neonatal abstinence syndrome and the neonates' need for morphine relief was lower in women taking buprenorphine compared with methadone, lower retention was found in the buprenorphine treated group.134
Adolescents Opiate addiction is often a disease of pediatric onset. Early interventions can prevent the associated consequences of addiction, such as HIV and hepatitis C.135 Because adolescents often have shorter addiction history, it is not known whether they would require maintenance pharmacotherapy. Several reports compare short-term detoxification to buprenorphine maintenance but show better results with longer periods of medication and high rates of relapse following discontinuation of medication.136
Comparative research to guide maintenance medication selection in adolescents is needed. Until such research is available, the choice of maintenance medication should be based on available evidence and informed choice. Chronic Pain A significant number of patients in maintenance pharmacotherapy complain of chronic pain.137 Many of these patients may require daily or intermittent opioid analgesics. Methadone and buprenorphine have been used in the treatment of moderate to severe pain, and their chronic use for opiate addiction does not preclude the regular use of opioid analgesics. Naltrexone can prevent the effectiveness of opioid analgesics. Its antagonist effect can be overridden in setting of acute pain but caution is advised.138 It is not clear whether naltrexone maintenance can be recommended for the patient requiring ongoing opioid analgesia.
30

Criminal Justice Methadone and buprenorphine have been used with success in criminal justice populations.139, 140 Each can reduce recidivism and illicit opiate use. Oral naltrexone requires close supervision for adherence and trials of extended-release naltrexone in criminal justice populations are forthcoming.141 No direct comparisons of these medications have been performed in a criminal justice setting. Although legal precedent exists for compulsory addiction treatment and medication in offenders, this precedent does not extend to a specific medication and the criminal justice system must avoid requiring one medication in favor of others and respect the informed choice of decisions made between a physician and patient.142 Health Professionals Health professionals who are opiate addicts have excellent treatment outcomes compared with the general population.143 Behavioral interventions alone have retention rates approaching 80%.144 Although some have reported successful use of naltrexone as an adjuvant treatment in health professionals who are opiate addicts, in the absence of controlled trials, it is difficult to know whether it provides added benefit to behavioral interventions alone.145,146 Without clear benefit of naltrexone over methadone or buprenorphine, the selection of specific pharmacotherapy should be between a physician and patient and based on evidence and informed choice. CONCLUSION: MEDICATION AND RECOVERY Extensive research shows that each of the three available medications used to treat opiate addiction have superior treatment outcomes to nonmedication-based therapies. Increased retention reduces mortality, improves social function, and is associated with decreased drug use and improved quality of life. Thus, these medications help patients achieve recovery, as it is currently defined. Although methadone and buprenorphine appear to have superior outcomes to oral and intramuscular naltrexone, more direct comparisons are needed. Further work is needed to identify and predict treatment response to help individualize medication choice. Until such data are available, it is prudent, and within a patient's right to informed choice, for treatment professionals to provide information regarding these standard treatment options, their expected outcomes, and their potential adverse effects and to allow the patient to choose the medication that best suits his or her need. REFERENCES 1. Degenhardt L, Bucello C, Calabria B, et al. What data are available on the extent
of illicit drug use and dependence globally? Results of four systematic reviews. Drug Alcohol Depend 2011; 117:85-101.
2. World Health Organization. Global health risks: mortality and burden of disease
attributable to selected major risks. Geneva, Switzerland: WHO Press; 2009. 3. Salomon N, Perlman DC, Friedmann P, Ziluck V, Des J. Prevalence and risk
factors for positive tuberculin skin tests among active drug users at a syringe exchange program. Int J Tuberc Lung Dis 2000; 4:47-54.
4. Nelson PK, Mathers BM, Cowie B, et al. Global epidemiology of hepatitis B and
hepatitis C in people who inject drugs: results of systematic reviews. Lancet 2011; 378:571-83.
31

5. Mathers BM, Degenhardt L, Phillips B, et al. Global epidemiology of injecting drug use and HIV among people who inject drugs: a systematic review. Lancet 2008; 372:1733-45.
6. Paulozzi LJ, Budnitz DS, Xi Y. Increasing deaths from opioid analgesics in the
United States. Pharmacoepidemiol Drug Saf 2006; 15:618-27. 7. Degenhardt L, Bucello C, Mathers B, et al. Mortality among regular or dependent
users of heroin and other opioids: a systematic review and meta-analysis of cohort studies. Addiction 2011; 106:32-51.
8. Centers for Disease Control and Prevention. Vital signs: overdoses of
prescription opioid pain relievers – United States, 1998-2008. MMRW 2011; 60:1487-92.
9. UNODC. World drug report 2011. 2011. United Nations Publication Sales No.
E.11.XI.10. 10. Substance Abuse and Mental Health Services Administration. Results from the
2010 National Survey on Drug Use and Health: summary of national findings. DHHS Publication No. SMA 11-4658. 2011. Rockville, MD, Office of Applied Studies. NSDUH Series H-41.
11. Substance Abuse and Mental Health Services Administration. Treatment episode
data set. 2011. http://www.dasis.samhsa.gov/webt/quicklink/us09.htm (accessed December 21, 2011).
12. Substance Abuse and Mental Health Services Administration. National survey on
drug use and health 2010. 2011. http://www.icpsr.umich.edu/cgi-bin/SDA/SAMHDA/hsda?samhda+ 32722- 0001 (accessed December 21, 2011).
13. Kreek MJ, Bart G, Lilly C, Laforge KS, Nielsen DA. Pharmacogenetics and
human molecular genetics of opiate and cocaine addictions and their treatments. Pharmacol Rev 2005; 57:1-26.
14. Merikangas KR, Stolar M, Stevens DE, et al. Familial transmission of substance
use disorders. Arch Gen Psychiatry 1998; 55:973-9. 15. Tsuang MT, Lyons MJ, Meyer JM, et al. Co-occurrence of abuse of different
drugs in men: the role of drug-specific and shared vulnerabilities. Arch Gen Psychiatry 1998; 55:967-72.
16. Monitoring the Future. 2011 data from in-school surveys of 8th-, 10th, and 12th-
grade students. 2011. http://monitoringthefuture.org/data/11data.html#2011data-drugs (accessed December 21, 2011).
17. Kalinichev M, Easterling KW, Holtzman SG. Long-lasting changes in morphine-
induced locomotor sensitization and tolerance in long-evans mother rats as a result of periodic postpartum separation from the litter: a novel model of increased vulnerability to drug abuse? Neuropsychopharmacology 2003; 28:317-28.
32

18. Vazquez V, Giros B, Dauge V. Maternal deprivation specifically enhances vulnerability to opiate dependence. Behav Pharmacol 2006; 17:715-24.
19. Brook JS, Brook DW, Zhang C, Cohen P. Pathways from adolescent parent-child
conflict to substance use disorders in the fourth decade of life. Am J Addict 2009; 18:235-42.
20. Mills KL, Teesson M, Ross J, Peters L. Trauma, PTSD, and substance use
disorders: findings from the Australian National Survey of Mental Health and Well-Being. Am J Psychiatry 2006; 163:652-8.
21. Volkow ND, Ding YS, Fowler JS, et al. Is methylphenidate like cocaine?
Studies on their pharmacokinetics and distribution in the human brain. Arch Gen Psychiatry 1995; 52:456-63.
22. Volkow ND, Wang GJ, Fischman MW, et al. Effects of route of administration on
cocaine induced dopamine transporter blockade in the human brain. Life Sci 2000; 67:1507-15.
23. Marsch LA, Bickel WK, Badger GJ, et al. Effects of infusion rate of intravenously
administered morphine on physiological, psychomotor, and self-reported measures in humans. J Pharmacol Exp Ther 2001; 299:1056-65.
24. Johnson SW, North RA. Opioids excite dopamine neurons by hyperpolarization of local interneurons. J Neurosci 1992; 12:483-8.
25. Volkow ND, Wang GJ, Fowler JS, Tomasi D, Telang F. Addiction: beyond
dopamine reward circuitry. Proceedings of the National Academy of Sciences. 2011; 108:15037-42.
26. Pickens CL, Airavaara M, Theberge F, Fanous S, Hope BT, Shaham Y.
Neurobiology of the incubation of drug craving. Trends in Neurosciences 2011; 34:411-20.
27. Koob GF, Volkow ND. Neurocircuitry of addiction. Neuropsychopharmacology
2010; 35:217-38. 28. Wang GJ, Volkow ND, Fowler JS, et al. Dopamine D2 receptor availability in
opiate-dependent subjects before and after naloxone-precipitated withdrawal. Neuropsychopharmacology 1997; 16:174-82.
29. Zijlstra F, Booij J, van den Brink W, Franken IHA. Striatal dopamine D2 receptor
binding and dopamine release during cue-elicited craving in recently abstinent opiate-dependent males. European Neuropsychopharmacology 2008; 18:262-70.
30. Kennedy JA, Hartman N, Sbriglio R, Khuri E, Kreek MJ. Metyrapone-induced
withdrawal symptoms. Br J Addict 1990; 85:1133-40. 31. Schluger JH, Borg L, Ho A, Kreek MJ. Altered HPA axis responsivity to
metyrapone testing in methadone maintained former heroin addicts with ongoing cocaine addiction. Neuropsychopharmacology 2001; 24:568-75.
33

32. Bart G, Borg L, Schluger JH, Green M, Ho A, Kreek MJ. Suppressed prolactin response to dynorphin A1-13 in methadone-maintained versus control subjects. J Pharmacol Exp Ther 2003; 306:581-7.
33. Schluger JH, Bart G, Green M, Ho A, Kreek MJ. Corticotropin-releasing factor
testing reveals a dose-dependent difference in methadone maintained vs control subjects. Neuropsychopharmacology 2003; 28:985-94.
34. Hackman DA, Farah MJ, Meaney MJ. Socioeconomic status and the brain:
mechanistic insights from human and animal research. Nat Rev Neurosci 2010; 11:651-9.
35. Morgan D, Grant KA, Gage HD, et al. Social dominance in monkeys: dopamine
D2 receptors and cocaine self-administration. Nat Neurosci 2002; 5:169-74. 36. Pescor MJ. Follow-up study of treated narcotics addicts. Publ Health Rep 1943;
Suppl 170:1-18. 37. Vaillant GE. A 20-year follow-up of New York narcotic addicts. Arch Gen
Psychiatry 1973; 29:237-41. 38. Mayet S, Farrell M, Ferri M, Amato L, Davoli M. Psychosocial treatment for opiate
abuse and dependence. Cochrane Database Syst Rev 2005; CD004330. 39. Mattick RP, Breen C, Kimber J, Davoli M. Methadone maintenance therapy
versus no opioid replacement therapy for opioid dependence. Cochrane Database Syst Rev 2003; CD002209.
40. Hser YI, Hoffman V, Grella CE, Anglin MD. A 33-year follow-up of narcotics
addicts. Arch Gen Psychiatry 2001; 58:503-8. 41. Kakko J, Svanborg KD, Kreek MJ, Heilig M. 1-year retention and social function
after buprenorphine-assisted relapse prevention treatment for heroin dependence in Sweden: a randomised, placebo- controlled trial. Lancet 2003; 361:662-8.
42. Woody GE, Kane V, Lewis K, Thompson R. Premature deaths after discharge
from methadone maintenance: a replication. J Addict Med 2007; 1:180-5. 43. Cornish R, Macleod J, Strang J, Vickerman P, Hickman M. Risk of death during
and after opiate substitution treatment in primary care: prospective observational study in UK General Practice Research Database. BMJ 2010; 341:c5475.
44. Cushman P, Dole VP. Detoxification of rehabilitated methadone-maintained
patients. JAMA 1973; 226:747-52. 45. Amato L, Davoli M, Minozzi S, Ali R, Ferri M. Methadone at tapered doses for the
management of opioid withdrawal. Cochrane Database Syst Rev 2005; CD003409.
34

46. Gowing L, Ali R, White JM. Opioid antagonists under heavy sedation or anaesthesia for opioid withdrawal. Cochrane Database Syst Rev 2010; CD002022.
47. Collins ED, Kleber HD, Whittington RA, Heitler NE. Anesthesia-assisted vs
buprenorphine- or clonidine-assisted heroin detoxification and naltrexone induction. JAMA 2005; 294:903-13.
48. Sees KL, Delucchi KL, Masson C, et al. Methadone maintenance vs 180-day
psychosocially enriched detoxification for treatment of opioid dependence: a randomized controlled trial. JAMA 2000; 283:1303-10.
49. Ling W, Hillhouse M, Domier C, et al. Buprenorphine tapering schedule and illicit
opioid use. Addiction 2009; 104:256-65. 50. Kleiderer EC, Rice JB, Conquest V, Williams JH. Pharmaceutical activities at the
I.G. Farbenindustrie plant, Hochst am Main. 981. Washington, DC: Office of the Publication Board Department of Commerce; 1945.
51. McCance-Katz EF, Sullivan LE, Nallani S. Drug interactions of clinical importance
among the opioids, methadone and buprenorphine, and other frequently prescribed medications: a review. Am J Addict 2010; 19:4-16.
52. Kreek MJ. Medical safety and side effects of methadone in tolerant individuals.
JAMA 1973; 223:665-8. 53. Center for Substance Abuse Treatment. Methadone mortality – a reassessment.
2007. http://www.dpt.samhas.gov/pdf/methadonereport10%2018%2007brief% 20attch.pdf.
54. Strang J, Hall W, Hickman M, Bird SM. Impact of supervision of methadone
consumption on deaths related to methadone overdose 1993-2008: analyses using OD4 index in England and Scotland. BMJ 2010; 341:c4851.
55. Martin JA, Campbell A, Killip T, et al. QT interval screening in methadone
maintenance treatment: report of a SAMHSA expert panel. J Addict Dis 2011; 30:283-306.
56. Martell BA, Arnsten JH, Krantz MJ, Gourevitch MN. Impact of methadone
treatment on cardiac repolarization and conduction in opioid users. Am J Cardiol 2005; 95:915-8.
57. Bart G. CSAT's QT interval screening in methadone report: outrageous fortune or
sea of troubles? J Addict Dis 2011; 30:313-7. 58. Isbell H, Wikler A, Eddy NB, Wilson JL, Moran CF. tolerance and addiction
liability of 6-dimethylamino-4–4-diphenylheptanone-3 methadon. JAMA 1947; 135:888-94.
35

59. Isbell H, Vogel VH. The addiction liability of methadone amidone, dolophine, 10820 and its use in the treatment of the morphine abstinence syndrome. Am J Psychiatry 1949; 105:909-14.
60. Dole VP, Nyswander ME, Kreek MJ. Narcotic blockade. Arch Intern Med 1966;
118:304-9. 61. Dole VP, Nyswander M. A medical treatment for diacetylmorphine heroin
addiction. A clinical trial with methadone hydrochloride. JAMA 1965; 193:646-50. 62. National Institutes of Health. Effective medical treatment of opiate addiction.
National Consensus Development Panel on Effective Medical Treatment of Opiate Addiction. JAMA 1998; 280:1936-43.
63. Ball JC, Ross A. The effectiveness of methadone maintenance. New York:
Springer-Verlag; 1991. 64. Johnson RE, Chutuape MA, Strain EC, Walsh SL, Stitzer ML, Bigelow GE. A
comparison of levomethadyl acetate, buprenorphine, and methadone for opioid dependence. N Engl J Med 2000; 343:1290-7.
65. Strain EC, Bigelow GE, Liebson IA, Stitzer ML. Moderate- vs high-dose
methadone in the treatment of opioid dependence: a randomized trial. JAMA 1999; 281:1000-5.
66. Ling W, Wesson DR, Charuvastra C, Klett CJ. A controlled trial comparing buprenorphine and methadone maintenance in opioid dependence. Arch Gen Psychiatry 1996; 53:401-7.
67. Simpson DD, Joe GW, Broome KM, Hiller ML, Knight K, Rowan-Szal GA.
Program diversity and treatment retention rates in the drug abuse treatment outcome study DATOS. Psychol Addict Behav 1997; 11:279-93.
68. McLellan AT, Lewis DC, O'Brien CP, Kleber HD. Drug dependence, a chronic
medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA 2000; 284:1689-95.
69. Marsch LA, Stephens MA, Mudric T, Strain EC, Bigelow GE, Johnson RE.
Predictors of outcome in LAAM, buprenorphine, and methadone treatment for opioid dependence. Exp Clin Psychopharmacol 2005; 13:293-302.
70. Kelly SM, O'Grady KE, Mitchell SG, Brown BS, Schwartz RP. Predictors of
methadone treatment retention from a multi-site study: a survival analysis. Drug Alcohol Depend 2011; 117:170-5.
71. Belding MA, McLellan AT, Zanis DA, Incmikoski R. Characterizing
"nonresponsive" methadone patients. J Subst Abuse Treat 1998; 15:485-92. 72. Villafranca SW, McKellar JD, Trafton JA, Humphreys K. Predictors of retention in
methadone programs: a signal detection analysis. Drug Alcohol Depend 2006; 83:218-24.
36

73. Kraft MK, Rothbard AB, Hadley TR, McLellan AT, Asch DA. Are supplementary services provided during methadone maintenance really cost-effective? Am J Psychiatry 1997; 154:1214-9.
74. Davis AM, Inturrisi CE. d-Methadone blocks morphine tolerance and N-methyl-D-
aspartate-induced hyperalgesia. J Pharmacol Exp Ther 1999; 289: 1048-53. 75. Kling MA, Carson RE, Borg L, et al. Opioid receptor imaging with positron
emission tomography and[sic] [18F]cyclofoxy in long- term, methadone-treated former heroin addicts. J Pharmacol Exp Ther 2000; 295:1070-6.
76. Kreek MJ, Wardlaw SL, Hartman N, et al. Circadian rhythms and levels of beta-
endorphin, ACTH, and cortisol during chronic methadone maintenance treatment in humans. Life Sci 1983; 33:409-11.
77. Facchinetti F, Grasso A, Petraglia F, Parrini D, Volpe A, Genazzani AR. Impaired
circadian rhythmicity of beta-lipotrophin, beta-endorphin and ACTH in heroin addicts. Acta Endocrinol Copenh 1984; 105:149-55.
78. Kreek MJ, Borg L, Zhou Y, Schluger J. Relationships between endocrine
functions and substance abuse syndromes: heroin and related short-acting opiates in addiction contrasted with methadone and other long-acting opioid agonists used in pharmacotherapy of addiction. In: Pfaff D, Arnold A, Etgen A, et al., eds. Hormones, brain and behavior. San Diego, CA: Academic Press, 2002:781-830.
79. Bentley KW, Hardy DG. Novel analgesics and molecular rearrangements in the
morphine-thebaine group. 3. Alcohols of the 6,14-endoethenotetrahydrooripavine series and derived analogs of N-allylnormorphine and -norcodeine. J Am Chem Soc 1967; 89:3281-92.
80. Ling W, Casadonte P, Bigelow G, et al. Buprenorphine implants for treatment of
opioid dependence: a randomized controlled trial. JAMA 2010; 304:1576-83. 81. Schuh KJ, Johanson CE. Pharmacokinetic comparison of the buprenorphine
sublingual liquid and tablet. Drug Alcohol Depend 1999; 56:55-60. 82. Picard N, Cresteil T, Djebli N, Marquet P. In vitro metabolism study of
buprenorphine: evidence for new metabolic pathways. Drug Metab Dispos 2005; 33:689-95.
83. Fudala PJ, Bridge TP, Herbert S, et al. Office-based treatment of opiate addiction
with a sublingual-tablet formulation of buprenorphine and naloxone. N Engl J Med 2003; 349:949-58.
84. Walsh SL, Preston KL, Stitzer ML, Cone EJ, Bigelow GE. Clinical pharmacology
of buprenorphine: ceiling effects at high doses. Clin Pharmacol Ther 1994; 55:569-80.
37

85. Comer SD, Sullivan MA, Walker EA. Comparison of intravenous buprenorphine and methadone self-administration by recently detoxified heroin-dependent individuals. J Pharmacol Exp Ther 2005; 315:1320-30.
86. Kintz P. Deaths involving buprenorphine: a compendium of French cases.
Forensic Sci Int 2001; 121:65-9. 87. Comer SD, Sullivan MA, Vosburg SK, et al. Abuse liability of intravenous
buprenorphine/naloxone and buprenorphine alone in buprenorphine-maintained intravenous heroin abusers. Addiction 2010; 105:709-18.
88. Martin WR, Eades CG, Thompson JA, Huppler RE, Gilbert PE. The effects of
morphine- and nalorphine-like drugs in the nondependent and morphine-dependent chronic spinal dog. J Pharmacol Exp Ther 1976; 197:517-32.
89. Jasinski DR, Pevnick JS, Griffith JD. Human pharmacology and abuse potential
of the analgesic buprenorphine: a potential agent for treating narcotic addiction. Arch Gen Psychiatry 1978; 35:501-16.
90. Center for Substance Abuse Treatment. Clinical guidelines for the use of
buprenorphine in the treatment of opioid addiction. DHHS Publication Number SMA 04–3939. Rockville, MD, Substance Abuse and Mental Health Services Administration. Treatment Improvement Protocol TIP Series 40; 2004.
91. Lee JD, Grossman E, DiRocco D, Gourevitch MN. Home
buprenorphine/naloxone induction in primary care. J Gen Intern Med 2009; 24:226-32.
92. Mello NK, Mendelson JH. Buprenorphine suppresses heroin use by heroin
addicts. Science 1980; 207:657-9. 93. Reisinger M. Buprenorphine as new treatment for heroin dependence. Drug
Alcohol Depend 1985; 16:257-62. 94. Ling W, Charuvastra C, Collins JF, et al. Buprenorphine maintenance treatment
of opiate dependence: a multicenter, randomized clinical trial. Addiction 1998; 93:475-86.
95. Mattick RP, Kimber J, Breen C, Davoli M. Buprenorphine maintenance versus
placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev 2008; CD002207.
96. Fiellin DA, Pantalon MV, Chawarski MC, et al. Counseling plus buprenorphine-
naloxone maintenance therapy for opioid dependence. N Engl J Med 2006; 355:365-74.
97. Weiss RD, Potter JS, Fiellin DA, et al. Adjunctive counseling during brief and
extended buprenorphine-naloxone treatment for prescription opioid dependence: a 2-phase randomized controlled trial. Arch Gen Psychiatry 2011; 68:1238-46.
38

98. Mattick RP, Ali R, White JM, O'Brien S, Wolk S, Danz C. Buprenorphine versus methadone maintenance therapy: a randomized double-blind trial with 405 opioid-dependent patients. Addiction 2003; 98:441-52.
99. Moore BA, Fiellin DA, Barry DT, et al. Primary care office-based buprenorphine
treatment: comparison of heroin and prescription opioid dependent patients. J Gen Intern Med 2007; 22:527-30.
100. Greenwald MK, Johanson CE, Moody DE, et al. Effects of buprenorphine
maintenance dose on mu-opioid receptor availability, plasma concentrations, and antagonist blockade in heroin-dependent volunteers. Neuropsychopharmacology 2003; 28:2000-9.
101. Rolandi E, Marabini A, Franceschini R, Messina V, Bongera P, Barreca T.
Changes in pituitary secretion induced by an agonist-antagonist opioid drug, buprenorphine. Acta Endocrinol Copenh 1983; 104:257-60.
102. Kosten TR, Morgan C, Kreek MJ. Beta endorphin levels during heroin,
methadone, buprenorphine, and naloxone challenges: preliminary findings. Biol Psychiatry 1992; 32:523-8.
103. Kakko J, von WJ, Svanborg KD, Lidstrom J, Barr CS, Heilig M. Mood and
neuroendocrine response to a chemical stressor, metyrapone, in buprenorphine-maintained heroin dependence. Biol Psychiatry 2008; 63:172-7.
104. Fatseas M, Denis C, Massida Z, Verger M, Franques-Rénéric P, Auriacombe M.
Cue-induced reactivity, cortisol response and substance use outcome in treated heroin dependent individuals. Biol Psychiatry 2011; 70:720-7.
105. Blumberg H, Pachter I, Matossian Z, inventors. 14-hydroxydihydronormorphinone
derivatives. US Patent 3,332,950. 1967. 106. Verebey K, Volavka J, Mule SJ, Resnick RB. Naltrexone: disposition,
metabolism, and effects after acute and chronic dosing. Clin Pharmacol Ther 1976; 20:315-28.
107. Wall ME, Brine DR, Perez-Reyes M. Metabolism and disposition of naltrexone in
man after oral and intravenous administration. Drug Metab Dispos 1981; 9:369-75.
108. Pfohl DN, Allen JI, Atkinson RL, et al. Naltrexone hydrochloride Trexan: a review
of serum transaminase elevations at high dosage. NIDA Res Monogr 1986; 67:66-72.
109. Martin WR. Realistic goals for antagonist therapy. Am J Drug Alcohol Abuse
1975; 2:353-6. 110. Volavka J, Resnick RB, Kestenbaum RS, Freedman AM. Short-term effects of
naltrexone in 155 heroin ex-addicts. Biol Psychiatry 1976; 11:679-85.
39

111. Dunbar JL, Turncliff RZ, Dong Q, Silverman BL, Ehrich EW, Lasseter KC. Single- and multiple-dose pharmacokinetics of long-acting injectable naltrexone. Alcohol Clin Exp Res 2006; 30:480-90.
112. National Institutes of Health. Narcotic antagonists: naltrexone progress report.
Julius, D and Renault, P. 1976. Virginia, DHEW. National Institute on Drug Abuse research Monograph Series 9.
113. O'Brien CP, Greenstein RA, Mintz J, Woody GE. Clinical experience with
naltrexone. Am J Drug Alcohol Abuse 1975; 2:365-77. 114. Hollister LE, Schwin RL, Kasper P. Naltrexone treatment of opiate-dependent
persons. Drug Alcohol Depend 1977; 2:203-9. 115. Judson BA, Carney TM, Goldstein A. Naltrexone treatment of heroin addiction:
efficacy and safety in a double-blind dosage comparison. Drug Alcohol Depend 1981; 7:325-46.
116. Minozzi S, Amato L, Vecchi S, Davoli M, Kirchmayer U, Verster A. Oral
naltrexone maintenance treatment for opioid dependence. Cochrane Database Syst Rev 2011; CD001333.
117. Comer SD, Sullivan MA, Yu E, et al. Injectable, sustained-release naltrexone for
the treatment of opioid dependence: a randomized, placebo-controlled trial. Arch Gen Psychiatry 2006; 63:210-8.
118. Krupitsky E, Nunes EV, Ling W, Illeperuma A, Gastfriend DR, Silverman BL.
Injectable extended-release naltrexone for opioid dependence: a double-blind, placebo-controlled, multicentre randomised trial. Lancet 2011; 377:1506-13.
119. Hulse GK, Morris N, Arnold-Reed D, Tait RJ. Improving clinical outcomes in
treating heroin dependence: randomized, controlled trial of oral or implant naltrexone. Arch Gen Psychiatry 2009; 66:1108-15.
120. Kunøe N, Lobmaier P, Vederhus JK, et al. Naltrexone implants after in- patient
treatment for opioid dependence: randomised controlled trial. Br J Psychiatry 2009; 194:541-6.
121. Ngo HTT, Tait RJ, Hulse GK. Comparing drug-related hospital morbidity following
heroin dependence treatment with methadone maintenance or naltrexone implantation. Arch Gen Psychiatry 2008; 65:457-65.
122. Weerts EM, Kim YK, Wand GS, et al. Differences in delta- and mu-opioid
receptor blockade measured by positron emission tomography in naltrexone-treated recently abstinent alcohol-dependent subjects. Neuropsycho-pharmacology 2008;33:653-65.
123. Volpicelli JR, Clay KL, Watson NT, O'Brien CP. Naltrexone in the treatment of
alcoholism: predicting response to naltrexone. J Clin Psychiatry 1995; 56:39-44.
40

124. Krupitsky EM, Zvartau EE, Masalov DV, et al. Naltrexone with or without fluoxetine for preventing relapse to heroin addiction in St. Petersburg, Russia. J Subst Abuse Treat 2006; 31:319-28.
125. Dijkstra BAG, De Jong CAJ, Bluschke SM, Krabbe PFM, van der Staak CPF.
Does naltrexone affect craving in abstinent opioid-dependent patients? Addiction Biology 2007; 12:176-82.
126. Shaham Y, Funk D, Erb S, Brown TJ, Walker CD, Stewart J. Corticotropin-
releasing factor, but not corticosterone, is involved in stress-induced relapse to heroin-seeking in rats. J Neurosci. 1997; 17:2605-14.
127. Kosten TR, Kreek MJ, Ragunath J, Kleber HD. Cortisol levels during chronic
naltrexone maintenance treatment in ex-opiate addicts. Biol Psychiatry 1986; 21:217-20.
128. O'Malley SS, Krishnan-Sarin S, Farren C, Sinha R, Kreek MJ. Naltrexone
decreases craving and alcohol self-administration in alcohol-dependent subjects and activates the hypothalamo-pituitary-adrenocortical axis. Psychopharma-cology Berl 2002; 160:19-29.
129. Ahmadi J, Ahmadi K, Ohaeri J. Controlled, randomized trial in maintenance
treatment of intravenous buprenorphine dependence with naltrexone, methadone or buprenorphine: a novel study. Eur J Clin Invest 2003; 33:824-9.
130. Schottenfeld RS, Chawarski MC, Mazlan M. Maintenance treatment with
buprenorphine and naltrexone for heroin dependence in Malaysia: a randomised, double-blind, placebo-controlled trial. Lancet 2008; 371:2192-200.
131. Bart G. Promise of extended-release naltrexone is a red herring. Lancet 2011;
378:663-4. 132. Kreek MJ, Bencsath FA, Field FH. Effects of liver disease on urinary excretion of
methadone and metabolites in maintenance patients: quantitation by direct probe chemical ionization mass spectrometry. Biomed Mass Spectrom 1980; 7:385-95.
133. Pond SM, Kreek MJ, Tong TG, Raghunath J, Benowitz NL. Altered methadone
pharmacokinetics in methadone-maintained pregnant women. J Pharmacol Exp Ther 1985; 233:1-6.
134. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after
methadone or buprenorphine exposure. N Engl J Med 2010; 363:2320-31. 135. Piccolo P, Borg L, Lin A, Melia D, Ho A, Kreek MJ. Hepatitis C virus and human
immunodeficiency virus-1 co-infection in former heroin addicts in methadone maintenance treatment. J Addict Dis 2002; 21:55-66.
136. Minozzi S, Amato L, Davoli M. Maintenance treatments for opiate dependent
adolescent. Cochrane Database Syst Rev 2009; CD007210.
41

137. Rosenblum A, Joseph H, Fong C, Kipnis S, Cleland C, Portenoy RK. Prevalence and characteristics of chronic pain among chemically dependent patients in methadone maintenance and residential treatment facilities. JAMA 2003; 289:2370-8.
138. Gastfriend DR. Intramuscular extended-release naltrexone: current evidence.
Ann N Y Acad Sci 2011; 1216:144-66. 139. Kinlock TW, Gordon MS, Schwartz RP, Fitzgerald TT, O'Grady KE. A
randomized clinical trial of methadone maintenance for prisoners: results at 12 months postrelease. J Subst Abuse Treat 2009; 37:277-85.
140. Magura S, Lee JD, Hershberger J, et al. Buprenorphine and methadone
maintenance in jail and post-release: a randomized clinical trial. Drug Alcohol Depend 2009; 99:222-30.
141. Coviello DM, Cornish JW, Lynch KG, Alterman AI, O'Brien CP. A randomized trial
of oral naltrexone for treating opioid-dependent offenders. Am J Addict 2010; 19:422-32.
142. Richard J. Judicially mandated naltrexone use by criminal offenders: a legal
analysis. Journal of Substance Abuse Treatment 2006; 31:121-7. 143. Domino KB, Hornbein TF, Polissar NL, et al. Risk factors for relapse in health
care professionals with substance use disorders. JAMA 2005; 293:1453-60. 144. Skipper GE, Campbell MD, Dupont RL. Anesthesiologists with substance use
disorders: a 5-year outcome study from 16 state physician health programs. Anesth Analg 2009; 109:891-96.
145. Ling W, Wesson DR. Naltrexone treatment for addicted health-care
professionals: a collaborative private practice experience. J Clin Psychiatry 1984; 45:46-8.
146. Merlo LJ, Greene WM, Pomm R. Mandatory naltrexone treatment prevents
relapse among opiate-dependent anesthesiologists returning to practice. J Addict Med 2011; 5:279-83.
147. What is recovery? A working definition from the Betty Ford Institute. J Subst
Abuse Treat 2007; 33:221-8.
42

HERE'S WHAT TRUMP'S NEW EXECUTIVE ORDER MEANS FOR OPIOID ADDICTION
Laura Santhanam∗ Reprinted from http://www.pbs.org/newshour/rundown/heres-trumps-new-executive-order-means-
opioid-addiction/ (March 29, 2017) New Jersey Gov. Chris Christie will lead a new national opioid commission created Wednesday by an executive order from President Donald Trump that also maps out his administration's latest strategy to combat the public health crisis. The fight against the opioid epidemic is "one that's incredibly important to every family in every corner of this country," Christie said Wednesday in an interview with The Today Show, adding he and Trump "both care passionately about this issue and we want to save lives." "Addiction is a disease, and no life is disposable. We can help people by giving them appropriate treatment," Christie said. Trump tweeted (https://twitter.com/realdonaldtrump/status/847201455165624320) late Wednesday that his signed executive order would create a presidential commission designed to combat opioid addiction and the opioid crisis. According to Trump's signed order, the commission is designed to: Identify existing federal dollars to combat drug addiction, including opioids; Assess availability and access to addiction treatment centers and overdose
reversal and identify underserved areas; Measure the effectiveness of state prescription drug monitoring programs; Evaluate public messaging campaigns about prescription and illegal opioids, and
identify best practices for drug prevention. In ninety days, the commission will submit an interim report to Trump with its findings. It will submit a final report by October 1, unless more time is needed, according to the executive order. The commission will dissolve a month later. On the campaign trail, Trump promised to tackle the nation's opioid crisis. But in February, the New York Times reported the Trump Administration planned to eliminate the White House Office for National Drug Control Policy, a three-decades-old office that President Ronald Reagan and Congress created to orchestrate the country's drug policy and strategies. The report concerned public health officials who worried about lost resources in the middle of nationwide opioid epidemic.
∗ Laura Santhanam is the Data Producer for the PBS NewsHour.
43

The executive order signed Wednesday by Trump asks that office to help the commission carry out some of its tasks. It does not make mention of what will happen to the "drug czar," a leadership position created by President Ronald Reagan. President Barack Obama's most recent appointee, Michael Botticelli, promoted expanded access to naloxone and other kinds of treatment, and shepherded a prescription drug monitoring program that is active in all states except Missouri. He also made headlines for being the first person in the position to be openly recovering from addiction. The national drug control policy office referred questions from the NewsHour to the White House, which did not respond to requests for comment. In January, Christie promised New Jerseyans that he would devote his final year in office to making headway in the state's own fight against opioid addiction, the Associated Press reported (https://www.nytimes.com/2017/01/10/nyregion/new-jersey-chris-christie-drug-crisis-state-of-the-state-address.html?_r=2). This policy work continues efforts he launched in 2011, as detailed by NJ.com (http://www.nj.com/politics/index.ssf/2016/12/ christie_wants_you_to_know_you_can_buy_naloxone_at.html). By the end of 2016, the state had expanded access to naloxone—an opioid antidote that reverses potentially fatal overdoses within minutes—and created a program that uses electronic data to track how often doctors and pharmacists doll [sic] out prescription drugs. Christie's administration also devoted more resources to the state's drug courts, which allows defendants who face drug charges to choose between treatment or jail time. Christie attended a White House meeting to discuss strategies to address opioid addiction, intervention and treatment Wednesday morning along with Trump and several members of the administration, including Attorney General Jeff Sessions, Education Secretary Betsy DeVos, Homeland Security Secretary Michael Kelly and Veterans Affairs Secretary David Shulkin, among others. The meeting also included some representatives of the law enforcement and health communities, as well as advocates and those recovering from addiction. "Stopping this epidemic is an issue that every American regardless of political background can and must get behind," White House Press Secretary Sean Spicer told reporters Wednesday, adding that the day's announcement was the first step in bringing stakeholders together. Trump's decision to form the commission is a step in the right direction, says Mary Bassett, who leads the New York City Department of Health and Mental Hygiene. In November, she co-signed a letter sent to the Trump transition team by ten other public health officials from the across the country asking for attention to the issue. "Opioid overdose deaths are preventable but have claimed too many American lives, and the growing presence of more potent drugs is exacerbating the problem," she says in a written statement from the department. "This executive order for an opioid commission seems to be an important step toward addressing the opioid epidemic at a national level."
44

Preventing further tragedy requires "all hands on deck," echoed Sen. Claire McCaskill, who earlier in the week launched an investigation into drugmakers who make the nation's top-five selling prescription opioids. "Drug overdose deaths, the majority of which are from heroin and prescription opioids, are a national crisis," McCaskill said in a written statement. "We'll need the help of Governor Christie, President Trump, and others at all levels of government, from any party affiliation, if we're going to make progress and save lives." The announcement arrives the same day a new report revealed the changing profile of Americans who use and abuse heroin. According to Silvia Martins and researchers at Columbia University Mailman School of Public Health, heroin use has become more prevalent over the last decade, increasing across all measures for age, race, gender, education, income and marital status—especially among white, uneducated men. "The nonmedical use of prescription opioids preceding heroin use increased among white individuals, supporting a link between the prescription opioid epidemic and heroin use in this population," the report said. Researchers analyzed more than 79,000 respondents who were asked about drug use in 2002-2003 and 2012-2013 for the National Epidemiologic Survey on Alcohol and Related Conditions. Their findings were released in JAMA Psychiatry Wednesday. "Heroin use has become more normative over time," Martins told the NewsHour. The commission's task is, in part, to stop that.
45

46

Jefferson Foster Care FACTS
Based on all children in OOHC on May 7, 2017 Source TWS-W058 Statewide Total Demographic Indicator Number Percent
Within Region
Number Percent Within State
Total Number of Children in OOHC with Active Placements (note E, F)
973 8,375
Placed in PCC Foster Homes 485 49.8 3,650 43.6 Placed in PCC Residential 112 11.5 1,002 12.0 Placed in Relative Placement 17 1.7 327 3.9 Total Number placed in DCBS Foster Homes all types (note A)
260 26.7 2,863 34.2
Placed in DCBS Basic and Advanced Foster Homes 232 23.8 2,462 29.4 Placed in DCBS Care Plus or Medically Fragile Homes
3 0.3 143 1.7
Placed in DCBS Adoptive Home 25 2.6 258 3.1 Placed in Detention Center 10 1.0 28 0.3 Placed in Independent Living or Education Setting 25 2.6 126 1.5 Placed in Psychiatric Hospitals 26 2.7 134 1.6 Placed out of state (note B) 14 1.4 57 0.7
Age at First Entry into Foster Care Age at First Entry into Foster Care: Less than 1 year 196 20.1 1,606 19.2 Age at First Entry into Foster Care: 1 to < 3 years 125 12.8 1,263 15.1 Age at First Entry into Foster Care: 3 to < 6 years 145 14.9 1,417 16.9 Age at First Entry into Foster Care: 6 to < 12 years 245 25.2 2,068 24.7 Age at First Entry into Foster Care: 12 to < 18 years 261 26.8 2,013 24.0
Demographics African American Children 482 49.5 1,534 18.4 Children with a Goal of Adoption 389 40.0 2,359 28.2 Children with a Goal of Reunification (note C) 314 32.3 4,204 50.2 Children with a Goal of Emancipation 43 4.4 304 3.6 Average Age of Entry into foster care 7.1 6.8 Average Age Now 10.3 9.8 Average # Months in Care at this Point in Time 24.5 22.2 Average Percent of Life in Care 30.9 29.4 Average Number of Days to Re-enter for those with any Re-Entry
989.5 852.1
Average Number of Placements this Removal Episode 3.9 3.1 Cost Data
Number of Children with Per Diem payments listed 837 7,310 Average Cost Per Day for Child with Per Diem Payments $81.27 $77.67 Average Cost per Child for Average Months in Care (note D)
$60,495.03 $52,567.84
A. Includes DCBS adoptive homes, basic and advanced, medically fragile homes. B. Includes relative placements, adoptive homes, treatment facilities, and homes just over the border. C. Other goals include placement with relatives, planned permanent living or the goals have not been determined. D. Total costs per child will be higher because children in this number have not exited care. E. Includes 32 Statewide duplicate placements as 'bed held' during hospital, detention or other short term stays. F. Includes 6 Regional duplicate placements as 'bed held' during hospital, detention or other short term stays.
47

48

Adverse Childhood Experience (ACE) Questionnaire Finding your ACE Score ra hbr 10 24 06
While you were growing up, during your first 18 years of life:
1. Did a parent or other adult in the household often …
Swear at you, insult you, put you down, or humiliate you?
or Act in a way that made you afraid that you might be physically hurt?
Yes No If yes enter 1 ________
2. Did a parent or other adult in the household often …
Push, grab, slap, or throw something at you?
or Ever hit you so hard that you had marks or were injured?
Yes No If yes enter 1 ________
3. Did an adult or person at least 5 years older than you ever…
Touch or fondle you or have you touch their body in a sexual way?
or
Try to or actually have oral, anal, or vaginal sex with you?
Yes No If yes enter 1 ________
4. Did you often feel that …
No one in your family loved you or thought you were important or special?
or Your family didn’t look out for each other, feel close to each other, or support each other?
Yes No If yes enter 1 ________
5. Did you often feel that …
You didn’t have enough to eat, had to wear dirty clothes, and had no one to protect you?
or
Your parents were too drunk or high to take care of you or take you to the doctor if you needed it?
Yes No If yes enter 1 ________
6. Were your parents ever separated or divorced?
Yes No If yes enter 1 ________
7. Was your mother or stepmother:
Often pushed, grabbed, slapped, or had something thrown at her?
or Sometimes or often kicked, bitten, hit with a fist, or hit with something hard?
or Ever repeatedly hit over at least a few minutes or threatened with a gun or knife?
Yes No If yes enter 1 ________
8. Did you live with anyone who was a problem drinker or alcoholic or who used street drugs?
Yes No If yes enter 1 ________
9. Was a household member depressed or mentally ill or did a household member attempt suicide?
Yes No If yes enter 1 ________
10. Did a household member go to prison?
Yes No If yes enter 1 ________
Now add up your “Yes” answers: _______ This is your ACE Score
49

50

51

52