Spotlight 409 Repair and Reform Medicaid: Even more essential under ObamaCare
5
or Trut The John Locke Foundation is a 501(c)(3) nonprot, nonpartisan research institute dedicated to improving public policy debate in North Carolina. Viewp oints expressed by authors do not necessarily refect those o the sta or board o the Locke Foundation . 200 W. Morgan, #200 Raleigh, NC 27601 phone: 919-828-3876 ax: 919-821-5117 www.johnlocke.org n spotlight n orth Carolina state Medicaid appropriations or Fiscal Y ear (FY) 2012 will have grown about $700 million since FY 2007 without changes. 1 Federal law will make it dicult to pay or this program and other core unctions o the state, such as education. In act, ObamaCare will make as many as 888,000 more people eligible or North Carolina Medicaid in 2014. 2 Gov . Bev Perdue and the General Assembly need to make the case to Con- gress and the Obama administration o the need or greater fexibility that al- lows or reorm. Without reorm, Medicaid will provide worse care or everyone enrolled. W ith reorm, there is a chance to restrain this drag on state nances and to improve access and care or those enrolled. No. 409 – March 23, 2011 RepaiR and RefoRm medicaid Even more essential under ObamaCare k e y f a c t s : • Norh crolin unding or Mdiid will xd $3 billion in fy 2012. • Norh crolin h on o h mo xpniv Mdiid progr m in h souh, pnding pproximl $4.6 million mor pr r hn Virgini nd $2.4 million mor pr r hn tnn. • sin 1990 h Gnrl ambl h xpndd ligibili or Mdiid nd Nc Hlh choi b bou 900,000 popl. • Obmcr orbid rduing ligibili b o prviou lvl. Obm- cr will lo xpnd nrollmn rom 1.3 million popl o ponill ovr 2 million popl in 2014. • Mdiid lrd provid l o r hn priv inurn. Wih- ou h bili o rdu nrollmn mong Mdiid ripin wih highr inom, o r will dlin or vr Mdiid ripin. • Wihou rorm or ighr ligibili , h will nd o u om r- vi nd pmn o door. Boh opion will mn wor r or vr pron on Mdiid. • Gov. Bv Prdu nd h Gnrl ambl nd o puh Whingon or xmpion rom Mdiid rriion nd grr bili o innov wih prmium uppor nd nourg pin onrol o hir own r. more >>
-
Upload
john-locke-foundation -
Category
Documents
-
view
219 -
download
0
Transcript of Spotlight 409 Repair and Reform Medicaid: Even more essential under ObamaCare

8/7/2019 Spotlight 409 Repair and Reform Medicaid: Even more essential under ObamaCare
http://slidepdf.com/reader/full/spotlight-409-repair-and-reform-medicaid-even-more-essential-under-obamacare 1/5
or Trut The John Locke Foundation is a
501(c)(3) nonprot, nonpartisan researchinstitute dedicated to improving public
policy debate in North Carolina. Viewpointsexpressed by authors do not necessarily
refect those o the sta or board o the Locke Foundation.
200 W. Morgan, #200
Raleigh, NC 27601
phone: 919-828-3876ax: 919-821-5117
www.johnlocke.org n
spotlight
north Carolina state Medicaid appropriations or Fiscal Year (FY) 20will have grown about $700 million since FY 2007 without change
Federal law will make it dicult to pay or this program and othcore unctions o the state, such as education. In act, ObamaCare will make many as 888,000 more people eligible or North Carolina Medicaid in 2014.2
Gov. Bev Perdue and the General Assembly need to make the case to Cogress and the Obama administration o the need or greater fexibility that lows or reorm. Without reorm, Medicaid will provide worse care or everyoenrolled. With reorm, there is a chance to restrain this drag on state nancand to improve access and care or those enrolled.
No. 409 – March 23, 2011
RepaiR and RefoRmmedicaidEven more essential under ObamaCare
k e y f a c t s : • Norh crolin unding or Mdiid will xd $3
billion in fy 2012.
• Norh crolin h on o h mo xpniv Mdiid progrm in h
souh, pnding pproximl $4.6 million mor pr r hn Virgini
nd $2.4 million mor pr r hn tnn.
• sin 1990 h Gnrl ambl h xpndd ligibili or Mdiid n
Nc Hlh choi b bou 900,000 popl.
• Obmcr orbid rduing ligibili b o prviou lvl. Obm-
cr will lo xpnd nrollmn rom 1.3 million popl o ponill ov
2 million popl in 2014.
• Mdiid lrd provid l o r hn priv inurn. Wi
ou h bili o rdu nrollmn mong Mdiid ripin wih high
inom, o r will dlin or vr Mdiid ripin.
• Wihou rorm or ighr ligibili, h will nd o u om r-
vi nd pmn o door. Boh opion will mn wor r or vr
pron on Mdiid.
• Gov. Bv Prdu nd h Gnrl ambl nd o puh Whingon or
xmpion rom Mdiid rriion nd grr bili o innov wih
prmium uppor nd nourg pin onrol o hir own r.
more

8/7/2019 Spotlight 409 Repair and Reform Medicaid: Even more essential under ObamaCare
http://slidepdf.com/reader/full/spotlight-409-repair-and-reform-medicaid-even-more-essential-under-obamacare 2/5
2
enrollmn expnion nd co Growh sin 1990
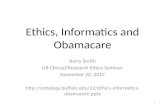
Medicaid is the largest publicly unded insurance program in the United States, with the number o averagemonthly eligibles in North Carolina increasing rom 393,593 during FY 1990 to 1,166,238 during FY 2006.3 Since 1990the number o children eligible or NC Health Choice or Children, the closely related State Child Health InsuranceProgram (SCHIP), has increased by about 600,000 and will grow again signicantly in 2014.4 During FY 2008, the estimated 1.7 million residents receiving benets in North Carolina cost nearly $10.2 billion in state and ederal unds
North Carolina’s Medicaid spending has continued to grow rapidly, increasing 9.8 percent between 2001 and 2004and 5.5 percent between 2004 and 2007.5 Although recent data refect a decline in Medicaid cost, that trend cannotcontinue with skyrocketing eligibility. Medicaid enrollment in North Carolina is expected to increase by 38.2 percentby 2019 as Medicaid expands to include people earning up to 138 percent o Federal Poverty Level (FPL), or $30,843or a amily o our, which is required by ObamaCare.6
Cost containment strategies or Medicaid have become very important to control budgets, while still encouragingimprovements in health care. However, these goals are proving extremely dicult due to ObamaCare rules that orbidchanges that tighten eligibility standards or all Medicaid populations.
th s o thing
Currently North Carolina’s Medicaid program uses state and ederal unds to provide substandard health insurance to pregnant women, low-income children, parents o dependent children, people with disabilities, and other specied groups. It also provides long-term care and some non-Medicare services or seniors and other specied groups. To
History of Average Monthly Medicaid Eligibles
and Yearly Medicaid Eligibles
393,593
467,925
573,140
657,649715,543
773,999815,276
826,725 821,671
818,136
850,811920,648
989,863
1,047,772
1,095,854
1,123,767
1,166,238
639,351
753,292
877,923
992,697
1,058,603
1,138,7861,176,589
1,192,133
1,197,173
1,176,819
1,221,266
1,354,593
1,390,0281,447,283
1,512,3601,563,751
1,602,645
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
1,800,000
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006
ELIGIBLES(Month ly Figures) ELIGIBLES(Annual Figures)
figur 1. Hior o h Norh crolin Mdiid Progrm, fy 1970 o fy 2006
Source: “History o North Carolina Medicaid Program, State Fiscal Years 1970 to 2007,” North Carolina Department o Health andHuman Services, Division o Medical Assistance, www.ncdhhs.gov/dma/pub/historyomedicaid.pd

8/7/2019 Spotlight 409 Repair and Reform Medicaid: Even more essential under ObamaCare
http://slidepdf.com/reader/full/spotlight-409-repair-and-reform-medicaid-even-more-essential-under-obamacare 3/5
3
receive Medicaid services, an individual must demonstrate that they meet specic health coverage eligibility criteriahave U.S. citizenship, and meet certain nancial requirements.
Medicaid is, ater public education, the second largest program in the state’s budget. North Carolina spends moreon Medicaid than any other state in the Southeast and is in desperate need o Medicaid reorm. Previous eorts, in-cluding implementing a preerred drug list and making greater eorts to reduce system ineciencies, are not nearlyenough to oset increasing costs or reduce the $2.4 billion decit acing North Carolina in FY 2012, even with the
gimmicks in the governor’s budget.Despite this decit, ObamaCare will make it nearly impossible or states to make economic reductions to Medicaid
due to requirements o maintaining high eligibility while imposing new costly provisions beginning in 2014.7 Secretaryo Health and Human Services Kathleen Sebelius has been all but intractable regarding state requests or fexibilityo plan design and payments to providers.8 Moreover, both Republicans and Democrats have asserted that states wilneed to nd alternatives to the strict requirements or the individual mandate imposed by ObamaCare.9, 10
Fortunately or policymakers, there are some limited options available to save the state money while encouragingMedicaid recipients to regain power over their health care options. Specic steps legislators can take or improved costcontainment are suggested below.
Rorm Long-trm cr
The most easible possibility or reorm is to make immediate changes to long-term care — e.g., nursing, adult, andhome care — through the ederal Decit Reduction Act o 2005 and to change enrollment and coverage requirementsor long-term care.11 The Decit Reduction Act has enabled states to have fexibility in how they align their respectiveMedicaid benet packages with the rest o the market.
Long-term care has been the largest portion o North Carolina’s Medicaid budget (about one-third, over $3 billionor many years. This is because o the broad range and costly services used by enrollees such as the elderly, the dis-
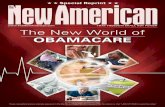
figur 2. Norh crolin Mdiid xpndiur pr nroll nd pr pir mong h high in h souh
Sources: Kaiser Family Foundation: statehealthacts.org; state demographics; author calculations

8/7/2019 Spotlight 409 Repair and Reform Medicaid: Even more essential under ObamaCare
http://slidepdf.com/reader/full/spotlight-409-repair-and-reform-medicaid-even-more-essential-under-obamacare 4/5
4
abled, and the chronically ill.12 However, less than one out o every nine dollars spent on home health care comes out othe pockets o these patients.13 Immediate remedies include encouraging private long-term care insurance and reduc-ing the number o people and services that are eligible or Medicaid payment. North Carolina, however, does not givemuch nancial incentive to people to purchase long-term care insurance, even ater the General Assembly restored thestate income tax credit or its purchase in 2007.
North Carolina does not strongly limit services covered by providers. In this area, North Carolina could ollowFlorida’s lead. In 2007 Florida set a xed-payment delivery system or nursing homes to limit the services orderedthrough the previous ee-or-service system.14 The xed-payment system limits what providers can charge or servicesand encourages adults to save early or their long-term care so they can access more elective services as they age. Thisidea is even supported by Democrats such as Sen. Ben Nelson, who conceded in a letter to constituents that privateinsurance is better than Medicaid.15 Although this recommendation would most likely be the easiest to implementthere are unresolved complications as the Decit Reduction Act, a ederal law, contradicts ObamaCare, another ederalaw.
Rdu Opionl srvi
Another alternative or reducing the Medicaid decit is to reduce the number o optional services it covers. Thisapproach has been successul in other states such as Arizona, where various transplants have been categorized as discretionary.16 The Arizona Health Care Cost Containment System has taken the stance that transplants ranging rom$263,000 (kidney) to over $1 million (intestine) are too costly.17 The Oregon Health Plan has also created a system thatprioritizes optional services and creates a dividing line based on available unds in determining what will be publiclynanced.18 Although decisions or determining who should receive unding or services are tough and oten lead to politically complex situations, services that are not required by the ederal government are an obvious place to save stateunds. North Carolina policymakers could ollow suit by determining that optional services, such as end-o-lie carerisky operations, and transplants are “optional” or “experimental,” thereby requiring private coverage. For guidancethe John Locke Foundation identied some optional services that could be reduced in its 2011 budget proposal.19
Obin Blo Grn
Lastly, and likely most infuential on the state’s Medicaid system, North Carolina could attempt to secure Medicaidunding in the orm o a block grant rom the ederal government, committing a level o ederal unding without regardto the state’s level o spending and without regulation o und usage. Thereore, block grants are an eective means orallowing each state to determine how health care related unds should be spent and are currently provided to NorthCarolina requently or mental health services and women and children’s programs. Currently, ederal payments tostates are guaranteed “as-needed,” meaning that the ederal unds are supplied as “matched unding.”20 North Carolina, or example, receives nearly two dollars in ederal unds or every dollar in state unds spent on Medicaid. A blockgrant, however, would allow the ederal government to commit a certain amount o unding no matter what the state
spends. This orm o cost-sharing enables states to know exactly how much unding will be provided and or how longremoving an incentive to expand coverage.
Rhode Island led the way or Medicaid block grants with a global Medicaid waiver in 2009. Under that waiverRhode Island receives xed payments rom the ederal government or ve years.21 Gov. Carcieri credited this waiveras the prime contributor to the state’s scal surplus in FY 2010.22 Based on that success, other states, including Michigan, Oklahoma, Washington, and Colorado, are exploring block grants in 2011 to regain fexibility and control overstate health spending.

8/7/2019 Spotlight 409 Repair and Reform Medicaid: Even more essential under ObamaCare
http://slidepdf.com/reader/full/spotlight-409-repair-and-reform-medicaid-even-more-essential-under-obamacare 5/5
5
conluion
Due to the overwhelming burden ObamaCare will place on the state o North Carolina’s budget, alternatives tothe current legislation must be explored. Legislators took an important rst step with the introduction o Health CareProtection Act (HB2), showing that a stand against ObamaCare must be taken without hesitation. The oundation oObamaCare is the Massachusetts health care law, which has resulted in a greater number o individuals with insur
ance but has also rationed health care services and greater costs or insurance and expenses or the government. NorthCarolina cannot aord current Medicaid costs and expansion o Medicaid, and the additional expenses laid out or2014 and beyond will cause urther harm. Moreover, the greater unding needed to expand Medicaid must come romother state sources like education. The most eective way to improve the state’s budget and promote individual rightswould be to repeal ObamaCare. However, in the absence o that happening in the near uture policymakers shouldseek an immediate waiver rom ObamaCare’s Medicaid provisions that destroy the state’s reedom to innovate.
Nicole Fisher is a health policy ellow at the John Locke FoundationJoseph Coletti is director o health and scal policy studies at the John Locke Foundation
end No
1. “Medicaid is the Fastest Growing Program in the State’s Budget: Growth Will Accelerate as the State’s Population Ages,” North Carolina Center or Public PolicyResearch, Jan. 29, 2010, www.nccppr.org/drupal/content/news/2010/01/29/271/medicaid-is-the-astest-growing-progam-in-the-states-budget-growth-will-.
2. John Holahan and Irene Headen, “Medicaid Coverage and Spending in Health Reorm: National and State-By-State Results or Adults at or Below 133%FPL,” Kaiser Commission on Medicaid and the Uninsured, May 2010, www.k.org/healthreorm/upload/Medicaid-Coverage-and-Spending-in-Health-Reorm-National-and-State-By-State-Results-or-Adults-at-or-Below-133-FPL.pd .
3. “History o North Carolina Medicaid Program, State Fiscal Years 1970 to 2007,” North Carolina Department o Health and Human Services, Division o MedicalAssistance, www.ncdhhs.gov/dma/pub/historyomedicaid.pd .
4. Nicole Fisher, author calculations based on 2008 data rom the U.S. Department o Health and Human Services and the Kaiser Commission on Medicaid and theUninsured.
5. See Kaiser Commission on Medicaid and the Uninsured and Urban Institute estimates based on data rom Centers or Medicare and Medicaid Services HCFA-6reports, 2010, www.statehealthacts.org/proleind.jsp?cat=4&sub=47&rgn=1.
6. Op. cit., note 2.7. Nina Owcharenko, “State Medicaid Reorm ater Obamacare,” Heritage Foundation WebMemo No. 3062, Nov. 16, 2010, www.heritage.org/research/
reports/2010/11/state-medicaid-reorm-ater-obamacare.8. “Sebelius outlines state fexibility and ederal support available or Medicaid—Full Letter,” U.S. Department o Health and Human Services, Feb. 3, 2011,
www.hhs.gov/news/press/2011pres/01/20110203c.html .
9. Sarah Kli, “Nelson says individual mandate ‘must change,’” Politico.com, Feb. 1, 2011. http://www.politico.com/blogs/glennthrush/0211/Nelson_says_individual_mandate_must_change_.html.10. “Nelson: Nebraskans want healthy and educated children, not divisive politics,” press release, oce o U.S. Sen. Ben Nelson, Aug. 30, 2010, bennelson.senate.
gov/press/press_releases/083010-01.cm.11. “Decit Reduction Act o 2005: Implications or Medicaid,” Kaiser Commission on Medicaid and the Uninsured, February 2006, www.k.org/medicaid/
upload/7465.pd .12. Jenni Owen, Lisa J. Berlin, Aimee Wall, and Linda Attarian, editors, “Medicaid Cost Containment Strategies or North Carolina and Other States,”
Center or Child and Family Policy at Duke University and School o Government at the University o North Carolina at Chapel Hill, May 24, 2005, www.amilyimpactseminars.org/s_ncs01report.pd .
13. Stephen Moses, “Long-Term Care Financing in North Carolina: Good Intentions, Ambitious Eorts, and Unintended Consequences,” John Locke Foundation,Policy Report, January 2008, johnlocke.org/research/show/policy%20reports/145.
14. Michael Bond, “Florida’s Medicaid Reorms: A Progress Report,” James Madison Institute Backgrounder No. 52, August 2007, www.jamesmadison.org/pd/materials/587.pd .
15. Op. cit., note 7.16. C. David Flower, “State Discretion in Funding Organ Transplants Under the Medicaid Program: Interpretive Guidelines in Determining the Scope o Mandated
Coverage,” Minnesota Law Review 79 (1233), May 1995.17. Milliman, Organ Procurement and Transplant Network, “The Cost O Organ Transplants,” National Public Radio, Nov. 17, 2010, www.npr.
org/2010/11/11/131215308/arizona-budget-cuts-put-organ-transplants-at-risk.18. Jonathan Oberlander, Theodore Marmor, and Lawrence Jacobs, “Rationing medical care: rhetoric and reality in the Oregon Health Plan,” Canadian Medical
Association Journal 164 (11), May 29, 2001, www.cmaj.ca/cgi/content/ull/164/11/1583.19. Joseph Coletti, “Protecting Families and Businesses: A Plan or Fiscal Balance and Economic Growth,” John Locke Foundation Spotlight No. 408, Feb. 21, 2011,
johnlocke.org/research/show/spotlights/259.20. “Medicaid and Block Grant Financing Compared,” Kaiser Commission on Medicaid and the Uninsured Policy Brie , January 2004, www.k.org/medicaid/
upload/Medicaid-and-Block-Grant-Financing-Compared.pd .21. Gary Alexander, “Rhode Island Global Consumer Choice Compact Medical Waiver: A National Model or Medicaid Reorm,” December 2010, www.galen.org/
leuploads/RIMedicaidReorm.pd .22. Pamela M. Prah, “Rhode Island’s Medicaid Gamble,” Stateline, May 11, 2010, www.stateline.org/live/details/story?contentId=483799.