
Spontaneous thrombosis of the mesenteric veins.
8
Spontaneous Thrombosis of the Mesenteric Veins CHARLES W. VAN WAY, III, M.D., STANLEY K. BROCKMAN, M.D., * Louis ROSENFELD, M.D. From the Department of Surgery, Vanderbilt University Medical Center, Nashville, Tennessee OF TliE several vascular conditions caus- ing necrosis of the intestine, the most mys- terious and least understood is spontaneous venous thrombosis. The entity is simply de- fined. If one considers all instances of thrombosis of the mesenteric veins and sub- tracts those cases in which the thrombosis has an obvious cause, such as pylephle- bitis, portal venous stasis, hypercoagulable states, or trauma, those remaining form a group which is defined as having no known cause. This group has variously been called primary mesenteric venous thrombosis,7 agnogenic venous mesenteric thrombosis,' and mesenteric venous occlusion of un- determined origin.2 Since this disease is defined in an entirely negative manner, the question arises as to whether it is a distinct clinical and patho- logic condition or simply an accident of classification. Naitove and Weismann 7 re- cently reported three cases of their own and reviewed 34 collected from the litera- ture. They concluded that there are certain characteristics which many cases shared and that the disease thus could be classed as a distinct entity. Over the past 5 years, the authors have encountered five examples of this disease. These showed the clinical features de- scribed by Naitove and Weismann7 and by others who have written about mesen- teric venous thrombosis. Three of the five Submitted for publication August 31, 1970. Supported in part by USPHS Grant No. GM- 01742. Present address: Dept. of Thoracic and Car- diovascular Surgery, Michael Reese Hospital, Chi- cago, Ill. 561 showed a peculiar pathologic finding which may serve as a further characterization and which may give a clue regarding cause. Case Reports Case 1. J. S., a 68-year-old man, was admitted to the Nashville Veterans Administration Hospital on November 3, 1964, with abdominal pain. He had been admitted twice in 1959 for thrombo- phlebitis, once in the right leg and once in the left. In 1963, he had thrombosis of the left sub- clavian and axillary veins and was successfully treated by thrombectomy. At the time of the pres- ent admission, he was taking no medication and had no other known disease. He began to have right upper quadrant and epigastric pain 5 days prior to admission with diarrhea at first, followed by constipation during the 2 days prior to admis- sion. There was no nausea or vomiting. Physical examination showed a pulse rate of 96 and mild generalized abdominal tenderness without rebound tenderness. Roentgenograms of the abdomen showed dilated loops of small bowel with fluid levels. Serum electrolytes, blood urea nitrogen, and liver function tests were normal. Abdominal pain became steadily worse over the next 24 hours. At laparotomy on November 4, 1964, an 80 cm. segment of jejunum was found to be necrotic. Arterial pulsations were present in the mesentery, and the mesenteric veins were thrombosed. A segment of bowel 150 cm. long was resected. No anticoagulants were used post- operatively. Four days later pain recurred. On November 9, 1964, re-operation again showed mesenteric venous thrombosis. A segment of bowel 140 cm. long was removed, and thrombus was extracted from the portal system proximally. He- parin was given after operation, but gastrointesti- nal bleeding developed and heparin was dis- continued. Hepatic failure ensued, and the patient died on December 17, 1964. Permission for au- topsy was not granted. The probable cause of death was intrahepatic extension of the mesenteric venous thrombosis. Microscopic examination of the two specimens showed the entire venous system engorged with
-
Upload
nguyenxuyen -
Category
Documents
-
view
222 -
download
0
Transcript of Spontaneous thrombosis of the mesenteric veins.

Spontaneous Thrombosis of the Mesenteric Veins
CHARLES W. VAN WAY, III, M.D., STANLEY K. BROCKMAN, M.D., *Louis ROSENFELD, M.D.
From the Department of Surgery, Vanderbilt University Medical Center,Nashville, Tennessee
OF TliE several vascular conditions caus-ing necrosis of the intestine, the most mys-
terious and least understood is spontaneousvenous thrombosis. The entity is simply de-fined. If one considers all instances ofthrombosis of the mesenteric veins and sub-tracts those cases in which the thrombosishas an obvious cause, such as pylephle-bitis, portal venous stasis, hypercoagulablestates, or trauma, those remaining form a
group which is defined as having no knowncause. This group has variously been calledprimary mesenteric venous thrombosis,7agnogenic venous mesenteric thrombosis,'and mesenteric venous occlusion of un-
determined origin.2Since this disease is defined in an entirely
negative manner, the question arises as towhether it is a distinct clinical and patho-logic condition or simply an accident ofclassification. Naitove and Weismann 7 re-
cently reported three cases of their own
and reviewed 34 collected from the litera-ture. They concluded that there are certaincharacteristics which many cases sharedand that the disease thus could be classedas a distinct entity.Over the past 5 years, the authors have
encountered five examples of this disease.These showed the clinical features de-scribed by Naitove and Weismann7 andby others who have written about mesen-
teric venous thrombosis. Three of the five
Submitted for publication August 31, 1970.Supported in part by USPHS Grant No. GM-
01742.Present address: Dept. of Thoracic and Car-
diovascular Surgery, Michael Reese Hospital, Chi-cago, Ill.
561
showed a peculiar pathologic finding whichmay serve as a further characterization andwhich may give a clue regarding cause.
Case ReportsCase 1. J. S., a 68-year-old man, was admitted
to the Nashville Veterans Administration Hospitalon November 3, 1964, with abdominal pain. Hehad been admitted twice in 1959 for thrombo-phlebitis, once in the right leg and once in theleft. In 1963, he had thrombosis of the left sub-clavian and axillary veins and was successfullytreated by thrombectomy. At the time of the pres-ent admission, he was taking no medication andhad no other known disease. He began to haveright upper quadrant and epigastric pain 5 daysprior to admission with diarrhea at first, followedby constipation during the 2 days prior to admis-sion. There was no nausea or vomiting. Physicalexamination showed a pulse rate of 96 and mildgeneralized abdominal tenderness without reboundtenderness. Roentgenograms of the abdomenshowed dilated loops of small bowel with fluidlevels. Serum electrolytes, blood urea nitrogen,and liver function tests were normal.
Abdominal pain became steadily worse overthe next 24 hours. At laparotomy on November 4,1964, an 80 cm. segment of jejunum was foundto be necrotic. Arterial pulsations were present inthe mesentery, and the mesenteric veins werethrombosed. A segment of bowel 150 cm. longwas resected. No anticoagulants were used post-operatively. Four days later pain recurred. OnNovember 9, 1964, re-operation again showedmesenteric venous thrombosis. A segment of bowel140 cm. long was removed, and thrombus wasextracted from the portal system proximally. He-parin was given after operation, but gastrointesti-nal bleeding developed and heparin was dis-continued. Hepatic failure ensued, and the patientdied on December 17, 1964. Permission for au-topsy was not granted. The probable cause ofdeath was intrahepatic extension of the mesentericvenous thrombosis.
Microscopic examination of the two specimensshowed the entire venous system engorged with

562 VAN WAY, BROCKMAN AND ROSENFELD
thrombus. The arteries were largely empty, al-though arterioles in the submucosa were throm-bosed. Surrounding the veins and venules in thebowel wall was a narrow zone of inflammatorycells, mostly lymphocytes and plasma cells butwith some leukocytes and eosinophiles (Fig. 1).There was necrosis in the muscular coats of thewalls of the larger veins, and the walls of thesmall veins appeared necrotic as well. This lesion,best described as necrotizing vasculitis, could beseen throughout the resected bowel.
Case 2. S. G., a 64-year-old man, was admittedon May 2, 1967 to Vanderbilt University MedicalCenter. He had adult-onset diabetes and a historyof renal stones and had never had thrombophle-bitis. He was taking no medication. A small pros-tatic nodule had been found shortly before, but ithad not as yet been biopsied and was believed bythe urologist to be benign. Two days before ad-mission, the patient developed right lower quad-rant pain with nausea and vomiting. He was ad-mitted to a local hospital and then transferred toVanderbilt University Hospital for operativetreatment.
Physical examination revealed generalized ab-dominal tenderness, most marked in the rightlower quadrant, without guarding and with onlyslight tenderness on rebound. The pulse was 124,and the blood pressure, respiratory rate, and tem-perature were normal. Bowel sounds were hyper-active at first but became hypoactive. Abdominalroentgenograms showed dilated loops of smallbowel. The packed cell volume was 52% and thewhite blood cell count was 20,300; the blood ureanitrogen, serum electrolytes, serum glutamic-oxalictransaminase, serum alkaline phosphatase, andserum amylase were within normal limits.
At operation, a segment of terminal ileum 88cm. long was resected. The veins were thrombosed.Penicillin and streptomycin were given for fourdays postoperatively. No anticoagulants were used.There were no complications.
The patient was readmitted 2 months laterwith lower abdominal pain and diarrhea, and hewas jaundiced. The diagnosis of hepatitis was sup-ported by serum enzyme determinations. Recoverywas uneventful.
In January, 1968, he had sudden epigastricand substernal pain. There was mild epigastrictenderness without rebound tenderness. Roent-genograms showed dilated small bowel loops. Ar-teriography of the aortic and superior mesentericarteries showed slow clearance of the contrastmedium from the distended loops. The leukocytecount was 11,000 and the amylase was 1914 So-mogyi units. He was operated upon and found to
Annals of SurgeryApril 1971 * Vol. 173 * No. 4
have pancreatitis with no evidence of mesentericvenous thrombosis.
He has had no subsequent intra-abdominal dif-ficulties. In October, 1968, he was found to havepelvic bone lesions suggestive of carcinoma of theprostate. Review of the earlier pelvic roentgeno-grams showed no bony lesions at the time of ve-nous thrombosis. In May, 1969, he underwent acraniotomy with excision of a solitary metastaticpoorly differentiated adenocarcinoma from the lefttemporal lobe.
Microscopic examination of the resected bowelshowed findings similar to those in case 1. Theveins, small veins, and venules were all distendedwith clot. Perivenous infiltrate of small round cellswas seen about veins of all sizes throughout theinvolved bowel and mesentery. Necrosis of themuscular layers of the vein wall was seen in largerveins. The arteries were not thrombosed, nor wasperiarterial infiltrate seen.
Case 3. V. L., a 57-year-old man, was admittedto Vanderbilt University Hospital on September26, 1967 with abdominal pain. He had no priorhistory of abdominal complaints, thrombophlebitis,or congestive heart failure, and he was taking nomedication. Periumbilical and left lower quadrantpain began 12 hours before admission. There wasno nausea or vomiting.
Physical examination showed normal vitalsigns. The abdomen was moderately distended,bowel sounds were diminished, and there wasmoderate left lower quadrant tenderness withneither spasm nor rebound tenderness. Roentgeno-grams showed dilated small bowel. The packedcell volume was 52%o and the leukocyte count was24,800. Blood urea nitrogen was 21 mg./100 ml.Serum electrolytes and amylase were normal.
Immediate laparotomy was performed, andabout 120 cm. of ileum was found to be gan-grenous and was resected. The arteries were notthrombosed. No anticoagulants were employedpostoperatively. He received cephalothin by intra-venous infusion for 4 days. He had no postopera-tive or late complications and no recurrence.
Microscopic examination of the specimenshowed thrombi in the smaller veins with patencyof the arteries. While the microscopic picture didnot show the massive engorgement of the venoussystem seen in the other four cases, the diagnosiswas felt to be mesenteric venous thrombosis. Ne-crotizing vasculitis was not seen.
Case 4. C. P., a 45-year-old man, was admittedto Vanderbilt University Medical Center on No-vember 3, 1967. He had no previous history ofthrombophlebitis. He did have a duodenal ulcer,for which he was being treated with dietary mea-sures and antacids. He had had a laparotomy for

Annals of Surgery SPONTANEOUS THROMBOSIS OF MESENTERIC VEINSApril 1971 * Vol. 173 * No. 4
ffiiS .............. ......................=.
FIG. 1. Photomicrograph of necrotizingis surrounded by infla
perforated ulcer in 1959. For 2 weeks prior toadmission he had mild epigastric and right upperquadrant pain. Upper gastrointestinal x-rays 2 daysprior to admission showed scarring of the duodenalbulb and a hiatal hernia. On the day of admission,the patient began to have more severe pain in theleft lower quadrant. He had had a similar episodeof left lower quadrant pain some months earlierwhich abated without a diagnosis having beenmade.
Physical examination showed normal vitalsigns. The upper abdomen was slightly tenderwhen first examined and became much moretender during the next two hours. Roentgenogramsshowed only one dilated loop of small bowel.Laboratory studies showed a packed cell volumeof 48%, a leukocyte count of 13,400 with a shiftto the left, normal serum electrolytes, bilirubin,and amylase, and a blood urea nitrogen of 24mg./100 ml.
vasculitis, Case 1. The thrombus-filled veinimmatory cells (200x).
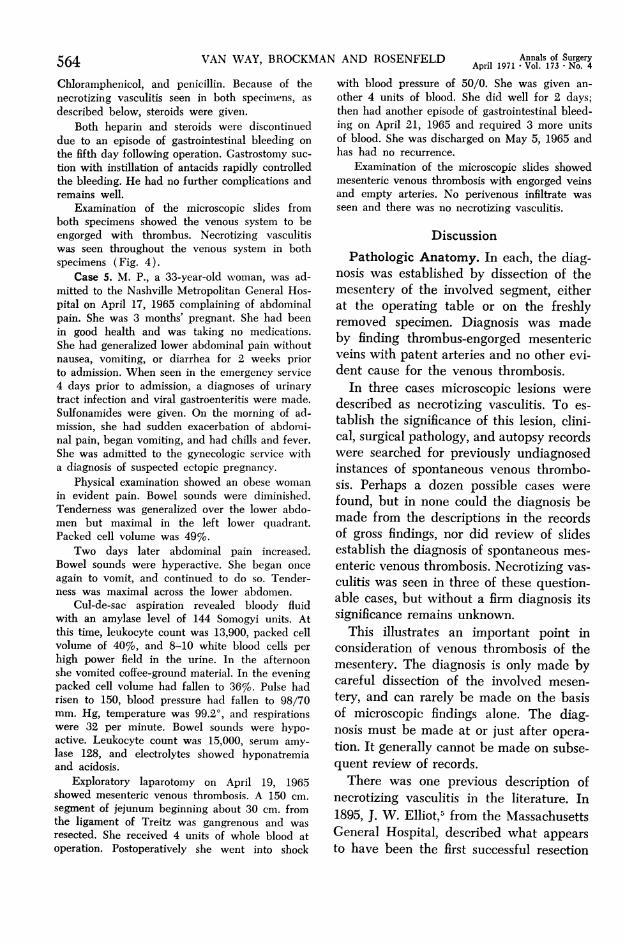
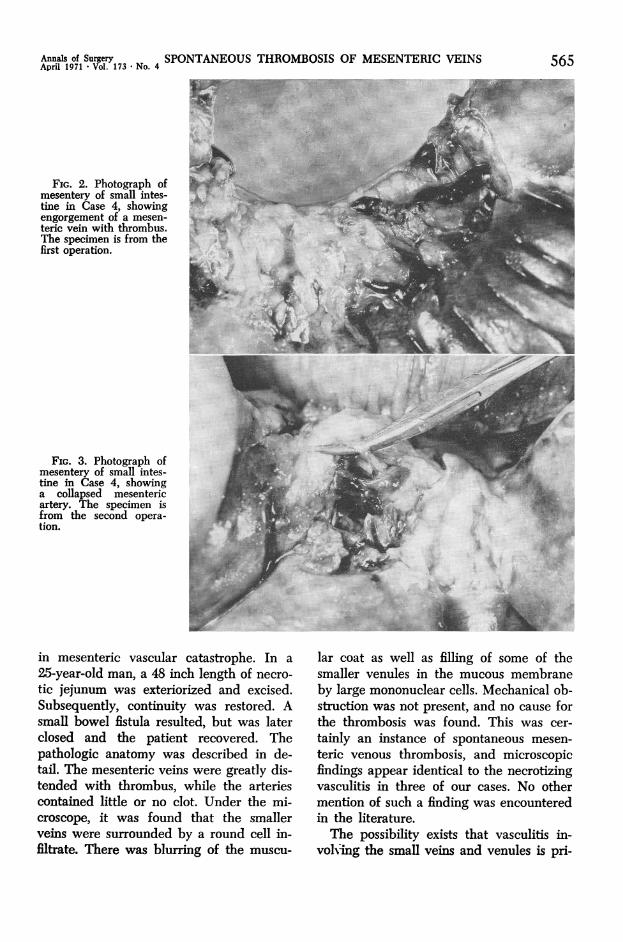
At operation, 55 cm. of mid-jejunum was re-sected. Arterial pulsations could not be seen be-cause of the massive edema of the involved mesen-tery, but the diagnosis of mesenteric venousthrombosis was easily made on inspection of thegross specimen (Fig. 2). Postoperatively, the pa-tient was treated with penicillin, Chloramphenicol,and kanamycin. On the fourth postoperative day,Coumadin was administered. The prothrombintime was prolonged into the therapeutic range bythe seventh day. On the ninth postoperative day,abdominal pain, hyperactive bowel sounds, andfever appeared. Abdominal re-operation on the10th postoperative day showed necrotic boweldistal to the old suture line. The engorged veinsand empty arteries showed the diagnosis to berecurrent mesenteric venous thrombosis (Fig. 3).About 50 cm. of bowel was resected. Since thepatient had a duodenal ulcer, a gastrostomy tubewas left in place. He was treated with heparin,
563
<.: -j
.4' is
564 VAN WAY, BROCKMChloramphenicol, and penicillin. Because of thenecrotizing vasculitis seen in both specimiiens, asdescribed below, steroids were giveni.
Both heparin and steroids were discontinueddue to an episode of gastrointestinal bleeding onthe fifth day following operation. Gastrostomy suc-tion with instillation of antacids rapidly controlledthe bleeding. He had no further complications andremains well.
Examination of the microscopic slides fromboth specimens showed the venous system to beengorged with thrombus. Necrotizing vasculitiswas seen throughout the venous system in bothspecimens (Fig. 4).
Case 5. M. P., a 33-year-old woman, was ad-mitted to the Nashville Metropolitan General Hos-pital on April 17, 1965 complaining of abdominalpain. She was 3 months' pregnant. She had beenin good health and was taking no medications.She had generalized lower abdominal pain withoutnausea, vomiting, or diarrhea for 2 weeks priorto admission. When seen in the emergency service4 days prior to admission, a diagnoses of urinarytract infection and viral gastroenteritis were made.Sulfonamides were given. On the morning of ad-mission, she had sudden exacerbation of abdomi-nal pain, began vomiting, and had chills and fever.She was admitted to the gynecologic service witha diagnosis of suspected ectopic pregnancy.
Physical examination showed an obese womanin evident pain. Bowel sounds were diminished.Tenderness was generalized over the lower abdo-men but maximal in the left lower quadrant.Packed cell volume was 49%.
Two days later abdominal pain increased.Bowel sounds were hyperactive. She began onceagain to vomit, and continued to do so. Tender-ness was maximal across the lower abdomen.
Cul-de-sac aspiration revealed bloody fluidwith an amylase level of 144 Somogyi units. Atthis time, leukocyte count was 13,900, packed cellvolume of 40%, and 8-10 white blood cells perhigh power field in the urine. In the afternoonshe vomited coffee-ground material. In the eveningpacked cell volume had fallen to 36%o. Pulse hadrisen to 150, blood pressure had fallen to 98/70mm. Hg, temperature was 99.20, and respirationswere 32 per minute. Bowel sounds were hypo-active. Leukocyte count was 15,000, serum amy-lase 128, and electrolytes showed hyponatremiaand acidosis.
Exploratory laparotomy on April 19, 1965showed mesenteric venous thrombosis. A 150 cm.segment of jejunum beginning about 30 cm. fromthe ligament of Treitz was gangrenous and wasresected. She received 4 units of whole blood atoperation. Postoperatively she went into shock
[AN AND ROSENFELD Annals of SurgeryApril 1971 * Vol. 173 * No. 4
with blood pressure of 50/0. She was given an-other 4 units of blood. She did well for 2 days;then had another episode of gastrointestinal bleed-ing on April 21, 1965 and required 3 more unitsof blood. She was discharged on May 5, 1965 andhas had no recurrence.
Examination of the microscopic slides showedmesenteric venous thrombosis with engorged veinsand empty arteries. No perivenous infiltrate wasseen and there was no necrotizing vasculitis.
Discussion
Pathologic Anatomy. In each, the diag-nosis was established by dissection of themesentery of the involved segment, eitherat the operating table or on the freshlyremoved specimen. Diagnosis was madeby finding thrombus-engorged mesentericveins with patent arteries and no other evi-dent cause for the venous thrombosis.
In three cases microscopic lesions weredescribed as necrotizing vasculitis. To es-tablish the significance of this lesion, clini-cal, surgical pathology, and autopsy recordswere searched for previously undiagnosedinstances of spontaneous venous thrombo-sis. Perhaps a dozen possible cases werefound, but in none could the diagnosis bemade from the descriptions in the recordsof gross findings, nor did review of slidesestablish the diagnosis of spontaneous mes-enteric venous thrombosis. Necrotizing vas-culitis was seen in three of these question-able cases, but without a firm diagnosis itssignificance remains unknown.
This illustrates an important point inconsideration of venous thrombosis of themesentery. The diagnosis is only made bycareful dissection of the involved mesen-tery, and can rarely be made on the basisof microscopic findings alone. The diag-nosis must be made at or just after opera-tion. It generally cannot be made on subse-quent review of records.There was one previous description of
necrotizing vasculitis in the literature. In1895, J. W. Elliot,5 from the MassachusettsGeneral Hospital, described what appearsto have been the first successful resection
Annals of Surgery SPONTANEOUS THROMBOSIS OF MESENTERIC VEINSApril 1971 Vol. 173 -No. 4
FIG. 2. Photograph ofmesentery of small intes-tine in Case 4, showingengorgement of a mesen-teric vein with thrombus.The specimen is from thefirst operation.
FIG. 3. Photograph ofmesentery of small intes-tine in Case 4, showinga collapsed mesentericartery. The specimen isfrom the second opera-tion.
in mesenteric vascular catastrophe. In a
25-year-old man, a 48 inch length of necro-
tic jejunum was exteriorized and excised.Subsequently, continuity was restored. Asmall bowel fistula resulted, but was laterclosed and the patient recovered. Thepathologic anatomy was described in de-tail. The mesenteric veins were greatly dis-tended with thrombus, while the arteriescontained little or no clot. Under the mi-croscope, it was found that the smallerveins were surrounded by a round cell in-filtrate. There was blurring of the muscu-
lar coat as well as filling of some of thesmaller venules in the mucous membraneby large mononuclear cells. Mechanical ob-struction was not present, and no cause forthe thrombosis was found. This was cer-
tainly an instance of spontaneous mesen-
teric venous thrombosis, and microscopicfindings appear identical to the necrotizingvasculitis in three of our cases. No othermention of such a finding was encounteredin the literature.The possibility exists that vasculitis in-
volving the small veins and venules is pri-
565
566 VAN WAY, BROCKMAN AND ROSENFELD
mary. In one patient (Case 2), a subse-quent episode of acute abdominal pain wasdue to pancreatitis not secondary to eitherbiliary tract disease or alcoholism. Venousthrombosis and pancreatitis might havebeen due to a similar inflammatory processacting at the level of the venule.No relationship could be established be-
tween necrotizing vasculitis and known le-sions of collagen vascular diseases. Peri-arteritis nodosa produces hemorrhagic in-farcts of the intestine, but the arteritis in-volves small arteries rather than veins.LNone of our patients showed evidence ofcollagen vascular diseases.
Clinical Considerations. Symptoms arethose of intestinal obstruction with gan-grenous bowel. All our patients had ab-dominal pain, usually with signs of peri-toneal irritation. There was leukocytosisand elevation of packed cell volume. Tem-perature on admission was between 99°and 1000 F. Nausea, vomiting, and diarrheawere inconstant. Roentgenograms usuallyindicated intestinal obstruction.Some characteristic features were seen.
All patients had been having abdominalpain without frank obstruction for severaldays. They continued to have bowel move-ments initially, becoming constipated later.This pre-obstructive phase lasted as long as2 weeks. Patients had pain out of propor-tion to abdominal tenderness. This wasnoted by Berry and Bougas,' who believedit an important differential point in diag-nosis. The tendency toward hemoconcen-tration was also seen in their patients, andprobably reflects slow progress of the dis-ease, allowing sequestration of extracellularfluid in the gut.
It is difficult to make an exact preopera-tive diagnosis. Arterial thrombosis can bedistinguished by sudden onset, but non-thrombotic occlusion often has an insidiousonset. Mechanical small bowel obstructionmay exist for several days before signs ofgangrene of bowel wall appear.
In one situation, the diagnosis of spon-
Annals of SurgeryApril 1971 * Vol. 173 * No. 4
taneous mesenteric venous thrombosis canbe made preoperatively. A patient who hashad recurrent thrombophlebitis and hassigns of intestinal obstruction with impend-ing gangrene, possibly has spontaneousmesenteric venous thrombosis. This hasbeen noted by several authors 1, 7, 8,10 andis illustrated by our Case 1. Naitove andWeismann 7 noted that 45%o of patients re-ported in the literature with primary mes-enteric venous thrombosis had histories ofprior thrombophlebitis.The difficulty of making a correct pre-
operative diagnosis is offset by the fact thattreatment is the same for any form of intes-tinal obstruction with gangrene-immedi-ate operation. Bloody fluid is commonlyseen on opening the abdomen as in all fiveof our patients. The diagnosis can be madeby the presence of arterial pulsations in thesegment of mesentery leading to the ne-crotic bowel. Often these pulsations areobscured by the gross thickening of themesentery, but careful dissection after thespecimen is removed should establish thepresence of venous thrombosis. Exclusionof other causes for thrombosis is simple.Generally other causes fall into the cate-gories of intercurrent abdominal infection;portal obstruction by tumor, cirrhosis, oradhesions; hypercoagulable states associ-ated with carcinomatosis and polycythemia;and trauma, usually operative. The opera-tion of splenectomy seems especially sub-ject to this complication, the first case beingnoted in 1895.4Treatment. Operative treatment is direct
since one of the distinguishing characteris-tics of spontaneous mesenteric venousthrombosis is that only part of the bowelis involved. This contrasts with arterial oc-clusion by thrombosis or embolus, in whichthe entire small bowel and often part ofthe colon is gangrenous, and with non-thrombotic vascular occlusion, which alsogenerally involves the entire bowel. Theinvolved segment can be resected with amargin while preserving most of the intes-

Annals of Surgery SPONTANEOUS THROMBOSIS OF MESENTERIC VEINSApril 1971 Vol. 173 No. 4 567
.Aip
't -
..**.<: *i::.., _t
rtS~~~~~~~~~~~~~~~- F---- -- -- --- --- --- ni-: ---
.. ... :4.. .. .: ...~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. .. ...
FIG. 4. Photomicrograph of necrotizing vasculitis, Case 4 (200x).
tine. This limited involvement is the rea-son for the good prognosis as comparedwith other forms of mesenteric vascularcatastrophe.The unique hazard is recurrent throm-
bosis, and is the reason for the importanceof making the diagnosis. In our cases, re-thrombosis occurred 7 to 10 days post-operatively in two patients. As proposedby Naitove and Weismann,7 postoperativeanticoagulation is essential, and heparin isthe agent of choice. The hazards of anti-coagulation are illustrated by the fact thatthree of our patients, including two whohad been receiving anticoagulants, bledpostoperatively. The method of administra-tion of heparin is controversial, but we hadgood results with continuous intravenous
administration of 5,000 to 7,500 units dur-ing each 8-hour period. The Lee-Whiteclotting time is kept at two to three timesnormal. Naitove and Weismann 7 suggestedchanging to Coumadin after 10 days, andrecommended its use for several monthspostoperatively.
Corticosteroids were administered in onecase (Case 4) and their use is questionable.If necrotizing vasculitis is evidence of anauto-immune or allergic process, cortico-steroids might prevent recurrence. On theother hand, the hazards of corticosteroidsare so serious that their use should prob-ably be reserved for recurrent episodes.The question of whether to give anti-
biotics postoperatively always arises. Noneof our patients, including the two post-
w~~~~~~~ ~~~~~~~~~~~~~ ......... Irliilil
Ai:: "i.. #S

568 VAN WAY, BROCKMAN AND ROSENFELD Annals of SurgeryApril 1971 * Vol. 173 - No. 4
operative deaths, had positive cultures ofperitoneal fluid at operation. In the ab-sence of perforation, the use of antibioticsis probably not necessary.General Considerations. Of all forms of
primary vascular occlusion of the bowel,spontaneous mesenteric venous thrombosiscarries the best prognosis. Naitove andWeismann7 found a mortality of 21% incases reported which were subjected tooperation and an overall mortality of 30%.In a recent study from the MassachusettsGeneral Hospital, Ottinger and Austen 9
reported a mortality of 92% in mesentericinfarction in general. Their cases werelargely either nonthrombotic vascular oc-clusion or arterial occlusion. Jensen andSmith6 reported a mortality of 88.6%o insuperior mesenteric artery occlusions andonly 11% in 9 venous occlusions. While nofigures are available comparing spontane-ous with secondary mesenteric venousthrombosis, the existence of a serious pri-mary disease, such as cirrhosis, tends togive the secondary form a poorer prognosis.Because of this relatively favorable out-
look, it is vital to treat these patients ag-gressively. While patients with arterial oc-clusion or nonthrombotic vascular occlu-sion may be doomed, those with spontane-ous venous thrombosis are not and can besaved by early operative treatment.
SummaryFive cases of spontaneous mesenteric ve-
nous thrombosis are reported. The clinicaland pathologic features are reviewed. Anunusual form of necrotizing vasculitis ofthe venous system was found in three of
the five cases. It should be emphasized thatthis disease, unlike other forms of vascularocclusion of the mesentery, usually in-volves only a limited segment of bowel andcarries a relatively good prognosis if promptoperative treatment is carried out and ifanticoagulation is used to prevent recur-rence of the thrombosis in the postopera-tive period.
AcknowledgmentsWe thank Dr. Robert Collins and Dr. Barton
McSwain for assistance in reviewing the pathologicand microscopic findings in these cases.
References1. Berry, F. B. and Bougas, J. A.: Agnogenic
Venous Mesenteric Thrombosis. Ann. Surg.,132:450, 1950.
2. Brown, M. J.: Mesenteric Venous Occlusion:A Clinical Entity. Amer. J. Surg., 49:242,1940.
3. Craikshank, A. H.: Venous Thrombosis in In-ternal Organs Associated with Thrombosisof Leg Veins. J. Path. Bact., 71:387, 1956.
4. De Latour, H. B.: Thrombosis of the Mesen-teric Veins as a Cause of Death after Sple-nectomy. Ann. Surg., 21:24, 1895.
5. Elliot, J. W.: The Operative Relief of Gan-grene of the Intestine Due to Occlusion ofthe Mesenteric Vessels. Ann. Surg., 21:9,1895.
6. Jensen, C. B. and Smith, G. H.: A ClinicalStudy of 51 Cases of Mesenteric Infarction.Surgery, 40:930, 1956.
7. Naitove, A. and Weismann, R. E.: PrimaryMesenteric Venous Thrombosis. Ann. Surg.,161:516, 1965.
8. North, J. P. and Wollenman, 0. J., Jr.: Ve-nous Mesenteric Occlusion in the Course ofMigrating Thrombophlebitis. Surg. Gynec.Obstet., 95:665, 1952.
9. Ottinger, L. W. and Austen, W. G.: A Studyof 136 Patients with Mesenteric Infarction.Surg. Gynec. Obstet., 124:251, 1967.
10. Quereshi, M. A. and Mansfield, R. B.: Recur-rent Mesenteric Venous Thrombosis with Re-covery. Amer. J. Surg., 108:421, 1964.
11. Wold, L. E. and Baggenstass, A. H.: Gastro-intestinal Lesions of Periarteritis Nodosa.Proc. Staff Meet. Mayo Clin., 24:28, 1949.


















