
Spectera Network Administration Manual
66
Network Administration Manual | Notice of Updates Spectera Network Administration Manual
Transcript of Spectera Network Administration Manual

Network Administration Manual | Notice of Updates
Spectera Network Administration Manual

Network Administration Manual | Notice of Updates
2
Disclaimer:
This manual remains the sole and exclusive property of Spectera. The information contained in this manual is confidential and proprietary, and the UnitedHealthcare Vision Network / Spectera Vision Network provider is granted a limited personal and non‐transferrable license for use of the content of this manual during, and for the provider’s participation on our networks. This manual is considered a part of your Provider Agreement. Revised 7/1/2021. Network Administration Manual Notice of Updates Effective July 2021:
Section 5 – Administering Member Benefits • 5.1 – Updated UnitedHealthcare and Spectera member ID card images
Section 7 – Lab Network Warranty & Policies • 7.3 – Added updated information on frames and warranty • 7.8 – Removed “Note” section • 7.9 – Changed “frames” to “materials” • 7.16 – Removed reference to the lab supply option
Section 10 – Quality • 10.3 – Added URL for users who may not have access to click the link directly through the NAM
Section 13 – Codes • 13.1 – Updated list of diagnosis codes for necessary contact lenses and fittings • 13.4 – Added 3600 exception code and description

Network Administration Manual | About the Network Administration Manual
3
About this Manual
This Network Administration Manual (this “Manual”) applies to services you provide to UnitedHealthcare vision plan members as a part of our vision network, unless otherwise noted.
Except when specified, this manual is effective on July 1, 2021.
Terms used in this manual include the following:
“Enrollee” refers to a person eligible and enrolled to receive coverage from us for covered services as defined or referenced in your agreement with us (we sometimes refer to Enrollees as “members” or “patients”).
“You”, “your”, or “provider” refers to any provider subject to this Manual (we sometimes refer to providers as “associates”).
“Us”, “we”, “our” refers to Spectera and/or UnitedHealthcare Vision Network / Spectera Vision Network for those products and services subject to this manual.
This manual is part of your contract. It is available to all participating providers online, or you can request a copy by contacting Customer Service. It is confidential and proprietary and should not be shared.
The purpose of this document is to make you aware of the policies held by Spectera. To find training guides and educational material, log in to spectera.com. The spectera.com training center is available to you 24/7 and is where you will find instructions for submitting claims, administering benefits and more!
For additional questions go to spectera.com Contact Us

Network Administration Manual | Table of Contents
4
Section 1: Online Resources.................................. 6 1.1 spectera.com ...................................................... 6 1.2 Password Requirements .................................... 6 1.3 News & Updates ................................................. 6 1.4 Online Training ................................................... 6 Section 2: Practice Changes .................................. 7 2.1 New Provider Application ................................... 7 2.2 Updating Provider Records ................................ 7 2.4 How to Change an Existing Tax Identification Number (TIN) ....................................... 8 Section 3: Communicating Benefits ...................... 9 3.1 Interactive Voice Response System .................. 9 3.2 Vision Benefits Faxback ..................................... 9 3.3 Language Interpretation Services ...................... 9 California Language Assistance Program ................. 9 Section 4: Benefit Overview ................................. 11 4.1 Minimum Prescription Requirements ............... 11 4.2 Full Service (Comprehensive) Plans ................ 11 4.3 Vision Benefits Included in UnitedHealthcare Medical Plans ............................. 12 4.4 Discount Benefit Plans ..................................... 13 4.5 Safety Eyewear Benefit Plans .......................... 13 4.6 Senior Care Options Members – Massachusetts Providers ONLY ............................. 13 4.7 Children’s Eye Care Program .......................... 13 4.8 Maternity Benefit .............................................. 14 4.9 Post-Laser Non-Prescription Sunglass Frame Benefit .......................................................... 14
4.10 Formularies .................................................... 14 4.11 Provider Warranty – For Providers Who Do Not Use The Lab Network ......................... 16 4.12 Eye Health & Wellness .................................. 17 4.13 HEDIS / Star Performance Reporting ............ 17 Section 5: Administering Member Benefits .................................................................. 20 5.1 Member Identification Cards ............................ 20 5.2 Product Brands ................................................. 21 5.3 Eligibility and Benefits Verification ................... 22 5.4 Determining Member Responsibility ................ 22 5.5 Sales Tax ......................................................... 22 Section 6: Materials Ordering .............................. 23 6.1 Materials Ordering ............................................ 23 6.2 What to Do When a Member Returns Materials .................................................................. 23
Section 7: Lab Network Warranty & Policies – For Providers Who Use the Lab Network ........................ Error! Bookmark not defined. 7.1 One-Time Doctor Redo Request or Changes to Orders .................................................. 25 7.2 Laboratory Error or Defective Materials ........... 26 7.3 Lab Network Supplied Frames ........................ 26 7.4 Provider Supplied Frames ............................... 26 7.5 Cancel Order Policy ......................................... 26 7.6 Anti-Reflective Coatings .................................. 26 7.7 Scratch Resistant Coating ............................... 27 7.8 Progressive Lenses Patient Satisfaction ......... 27 7.9 Materials Sent by the Provider’s Office ............ 27 7.10 Member Materials .......................................... 27 7.11 Product Liability .............................................. 27 7.12 Drilled Rimless and Metal-Grooved Frames .................................................................... 27 7.13 Uncut or Edged “Lenses-Only” Orders .......... 28 7.14 Contact Lenses .............................................. 28 7.15 Prescription Change ...................................... 28 7.16 The Laboratory Network's Right to Cancel Orders ......................................................... 28 7.17 Material Returns ............................................. 28 Section 8: Claims .................................................. 29 8.1 How to File a Claim .......................................... 29 8.2 Clean Claims .................................................... 29 8.3 National Provider Identification (NPI) ............... 30 8.4 Electronic Claims Submission ......................... 30 8.5 Coordination of Benefits .................................. 31 8.6 Provider Remittance Advice ............................ 31 8.7 Electronic Payments and Statements (Optum Pay) ............................................................ 32 Section 9: Standards of Care ............................... 33 9.1 Clinical Practice Guidelines ............................. 33 9.2 Access Standards ........................................... 36 9.3 Telemedicine .................................................... 37 Section 10: Quality ............................................... 38 10.1 Quality Management Program ....................... 38 10.2 Credentialing & Re-credentialing ................... 38 10.3 Cultural Competency ..................................... 39 Section 11: Policies .............................................. 40 11.1 Provider Disputes ........................................... 40 11.2 Provider Fair Hearing Policy .......................... 40 11.3 New Jersey Golden Rule ............................... 42 11.4 Rhode Island Providers: Notice of Member Vision Complaint and Appeal Rights ........ 43 11.5 Non-Covered Services ...................................... 44 11.6 Additional Medicare Advantage Requirements .......................................................... 44

Network Administration Manual | Table of Contents
5
11.7 General Compliance and Fraud, Waste and Abuse .................................................... 45 11.8 Terminations for Inactivity .............................. 47 11.9 Provider Directory Requirements ................... 47 Section 12: Forms ................................................. 48 12.1 Patient Care Forms ........................................ 48 12.2 Patient Frames - Waiver Form for Patients Who Use the Lab Network ........................ 48 12.3 Referral Forms ............................................... 49 Section 13: Codes ................................................. 57 13.1 Spectera Vision Network Billing Guide ........... 57 13.2 Spectera Vision Network Modifier Codes ...................................................................... 64 13.3 Vision Diagnosis Codes ................................. 65 13.4 Commonly Used Provider Remittance Advice Remark Codes ............................................ 66

Network Administration Manual | Section 1: Online Resources
6
Section 1: Online Resources 1.1 spectera.com
Our website is available 24/7 and is designed to provide a wealth of information while minimizing the time you spend on administration. Use spectera.com to find member benefit information, to educate yourself and your staff using our training center, and to submit claims and orders.
1.2 Password Requirements When you log in to spectera.com, you will be prompted to update your password using the following requirements:
• Must be at least 8 characters in length • Must be a mix of upper and lower case characters • Must contain at least one numeric character • Must contain at least 1 special character(!,#,$,%,* or ~) • Cannot contain the user login ID • Cannot be one of the previous 10 passwords
We require that your password be changed every six months. If you forget it, you can reset it on the website.
We allow you to create additional user IDs and passwords for your office staff at spectera.com, but require you to keep them secure. If you have created passwords for employees who later leave your company, you can call Customer Service to have their user ID and password terminated. The termination will take place within 48 hours.
1.3 News & Updates You’ll find the latest news and information at spectera.com Home Page Provider Connection. You’ll receive our newsletter monthly via email. To receive these important communications, make sure that your email address in your profile is current at all times.
1.4 Online Training
We offer short and pre-recorded training (that you can listen to 24/7) as well as printable “how to” guides so that you understand how to submit claims, look up benefits, and more. At times we offer live training sessions and may require that you and your staff attend these sessions. Specialized training is also available upon request through Customer Service or your Provider Relations Advocate.
spectera.com Home Page Online Training Center
Network Administration Manual | Section 2: Practice Changes
7
Section 2: Practice Changes
2.1 New Provider Application Adding a new provider to your practice is easy! Simply request an application through spectera.com, or call Customer Service. Remember: Providers are not considered to be participating until they’ve been credentialed by us.
Proactive Notification of Changes Please notify us of changes to your demographic information at least 30 calendar days prior to the effective date of the change.
2.2 Updating Provider Records Part of your responsibility as a provider in our vision network is to make sure that the information we have about you and your practice is up to date. Review your information, including the details listed below, at least quarterly.
The information that you are required to review quarterly includes, but is not limited to: • the address(es) of the office locations where you currently practice • the phone number(s) of the office locations where you currently practice • your email address • if you’re still affiliated with listed provider groups • your specialty • your license(s) • your tax identification number • your NPI(s) • any languages you or your staff are able to speak or write • ages you serve • office hours
If the information changes or isn’t correct, submit corrections to us at spectera.com, by fax (855-250-8162), or by email ([email protected]).
Send notice of the following occurrences to the address noted in your provider agreement. This is needed within 10 calendar days of it occurring.
• Material changes to, cancellation or termination of liability insurance. • Bankruptcy or insolvency. • Any indictment, arrest or conviction fora felony or any criminal charge related to your practice or
profession. • Any suspension, exclusion, debarment or other sanction from a state or federally funded
healthcare program. • Loss, suspension, restriction, condition, limitation, or qualification of your license to practice. For
physicians, any loss, suspension, restriction, condition, limitation or qualification of staff privileges at any licensed hospital, nursing home, or other facility.
• Relocation or closure of your practice, and, if applicable, transfer of member records to another physician/facility.

Network Administration Manual | Section 2: Practice Changes
8
2.3 How to Change an Existing Tax Identification Number (TIN) You must include your W-9 form in order to request a TIN change. To submit the change, complete the Provider Profile Update Form by logging in at spectera.com Plan Resources Provider Profile Update Form or document your change on office letterhead.

Network Administration Manual | Section 3: Communicating Benefits
9
Section 3: Communicating Benefits
3.1 Interactive Voice Response System Our Interactive Voice Response (IVR) system is available 24/7 by calling (800) 638-3120. When you call, use your office phone number, NPI or other basic provider information to identify yourself. Make sure your practice telephone number is updated in your provider profile atspectera.com.
3.2 Vision Benefits Faxback Once you’ve verified if a member is eligible for services, you can have a fax immediately sent to you with the member’s benefits. If we have your fax number in your Provider Profile, you’ll just need to verify it. If the IVR can’t find your fax number, it will ask you to enter the number.
3.3 Language Interpretation Services We want to make sure that we’re communicating to you and your patients in the way that’s easiest to understand. We provide both written and spoken translation services to you and your patients. If you or your UnitedHealthcare vision patients need translation services, call Customer Service at (800) 638-3120 to be connected with the Language Line.
California Language Assistance Program Vision providers and other health plans (including their network providers) regulated by the California Department of Insurance (CDI) are required to offer language assistance services to members with limited English proficiency. The legislation outlines specific requirements of the plans and the contracted network when working with Limited English Proficient (LEP) members. The Language Assistance Program includes:
• Surveying members to determine language preferences. • Making the information collected about members language preferences available to network
providers upon request via Customer Service representatives. • Informing members and providers of the availability of free language services. • Free interpreter services in the caller’s language of choice via the language line to any member who
requires language assistance by calling Customer Service at (800) 638-3120. • Written member documents interpreted via the Language Line for all relevant documents
according to the regulations. • Written translation of member documents will be provided if spoken interpretation is refused.
What is required of you?
• Offer free interpretation services through Spectera to members with limited English proficiency, even when the member is accompanied by a family member or friend who can interpret.
• Document the acceptance or denial of interpreter services in the member’s treatment record.

Network Administration Manual | Section 3: Communicating Benefits
10
If language assistance is required, call Customer Service at (800) 638-3120. You will be connected with the Language Line via a Customer Service Representative, and certified interpreters will provide telephonic interpretation services.

Network Administration Manual | Section 4: Benefit Overview
11
Section 4: Benefit Overview Benefit designs will vary within our vision plans, so it is important that you always check each member’s eligibility and benefits before you render services. Some benefit plans include multiple exams. Additional exams are not available until 60 days have passed from the date of the most recent exam. Verify eligibility and benefits by calling Customer Service or online at spectera.com Home PagePatient InformationSelect Patient.
Note: Materials that are not for the purpose of correcting vision are excluded from coverage (Non-prescription eyeglasses, non-prescription contact lenses and frames without lenses) unless otherwise indicated in the members’ benefits and eligibility. A valid ICD-10 code associated with vision correction is required on all claims.
4.1 Minimum Prescription Requirements
United Healthcare's vision benefits apply to prescription lenses that aid in the correction of vision and have a minimum of 0.25 diopters in either the sphere or cylinder unless otherwise indicated in the members’ benefits and eligibility.
4.2 Full Service (Comprehensive) Plans Our comprehensive vision plans usually include coverage for an eye exam, eyeglasses, or contact lenses (in lieu of eyeglasses), as well as lens options and extras.
Exams A comprehensive eye examination must be performed for all members. The examination should include the components we describe in the Standards of Care section of this manual. A Dilated Fundus Examination should be performed when indicated. Some benefit plans include multiple exams. Additional exams must occur at least 60 days from the most recent exam.
Materials Our vision plans usually include prescription lenses and coverage of a frame up to a fixed dollar amount. Our plans also usually include coverage for prescription contact lenses in lieu of eyeglasses. Remember to verify your member’s coverage before providing any services or materials. Member out-of-pocket costs, for example copays, may apply and can vary plan by plan.
• Frames Members are not restricted to a specific frame selection. Members have an allowance that is based on either the wholesale frame price or the retail frame price. The frame allowance can be applied to any frame you have in your office or any frame you are willing to order. Actual allowances may vary by member and should be confirmed on spectera.com before serving your patient. Check the fee schedule in your contract for frame benefit discount amounts.
• Lenses and Lens Options
You should prescribe prescription lenses. Standard lenses include single vision, lined bifocal, lined trifocal, glass or lenticular lenses. Lenses or lens options not covered by the plan are typically offered at a discounted price.

Network Administration Manual | Section 4: Benefit Overview
12
If a member requires a multifocal prescription in only one eye and selects a progressive lens, the member is responsible for any material copay and surcharge associated with a pair of progressive lenses. Members should be charged the lesser of your charges or the published lens options pricing, not to exceed the lens option pricing.
For order entry, the lens style that should be entered in the order shall be the lens style that utilizes the richest benefit for the member. In these instances, you must contact the laboratory in order to clarify the order has mixed styles.
• Contact Lenses Most plans provide coverage for elective contact lenses in lieu of eyeglasses. Some plans will use a formulary (selection) contact lens list for covered-in-full contact lenses; others may apply an allowance towards a member’s contact lens purchase as well as fit and evaluation fees.
Non-formulary (non-selection) contact lens benefits typically include a fixed dollar allowance to be used towards the purchase of contact lenses that are not on the formulary. When you supply non-selection contact lenses, use only the full contact lens allowance for contact lens materials.
If a member requires both selection and a non-selection lenses (because they have a different contact lens prescription for each eye and they are fitted with a formulary lens for one eye and a non-formulary lens for the other eye), the non-selection contact lens benefit and reimbursement will apply. In these instances, you are responsible for sourcing the contact lenses (including the selection/formulary lenses). Refer to the claims instructions in the billing guide which can be found in the appendix to this manual.
NOTE: If a member is not eligible for contact lenses, the fitting and evaluation is not reimbursable.
• Necessary Contact Lenses Necessary contacts are covered in full for members after any applicable copay. Claims for necessary contacts must be submitted per the instructions in the billing guide in this manual.
Reimbursement rates for necessary contact lens fitting and evaluation services are capped at $500.
Reimbursement rates for necessary contact lenses are capped at $1,500. If your costs exceed the contracted reimbursement amount, complete the Supporting Documentation Form– Necessary Contact Lenses and Services and include documentation of your actual acquisition cost. An invoice or order form receipt is acceptable documentation. Total payment will not exceed 125% of acquisition cost of the necessary contact lenses, less any member expenses. Approvals will be based on review of the completed form and the original claim.
4.3 Vision Benefits Included in UnitedHealthcare Medical Plans Some UnitedHealthcare medical plans include routine vision benefits in order to comply with Affordable Care Act (ACA) requirements. We administer this vision care benefit, which generally includes a comprehensive eye exam including dilation and/or refraction as appropriate; eyeglasses including frame and lenses; or contact lenses in lieu of eyeglasses; as a part of the medical plan for pediatric members. Some members have access to multiple benefits, and some benefits include multiple exams. Subsequent exams must be performed at least 60 days after the previous exam. Coverage typically aligns with medical plan designs and may include copays, coinsurance amounts and particularly in Consumer Driven Health Plans, the application of the vision benefit to the plan deductible. The annual deductible is the amount the member must pay out of pocket each plan year for covered health services before the plan begins paying for eligible expenses. In all plans, out-of-pocket amounts will accumulate to members’ out-of-pocket maximums.

Network Administration Manual | Section 4: Benefit Overview
13
4.4 Discount Benefit Plans Discount vision plans typically include a comprehensive eye examination and discounts on eyeglasses or contact lenses (in lieu of eyeglasses) as well as discounts on lens options. Discount plans may be offered to UnitedHealthcare medical members in addition to their medical benefit. When you verify eligibility, you may find that some members have both a discount and a comprehensive vision plan. To accommodate these members, review the benefits and select the plan that allows the best coverage for the member.
• Materials
Benefits typically include discounts on prescription lenses, frames, and lens options. Benefits may also include discounts on formulary and non-formulary contact lenses. Review the member’s coverage before providing materials. Member expenses may apply, and out-of-pocket amounts vary.
4.5 Safety Eyewear Benefit Plans Safety eyewear benefits are provided by some employer groups. The benefit includes coverage for prescription, polycarbonate lenses with side shields as well as a fixed dollar allowance toward approved safety frames.
Safety lenses must meet ANSI Z-87 standards.
4.6 Senior Care Options Members – Massachusetts Providers ONLY For providers in our vision networks in the state of Massachusetts, you may see UnitedHealthcare vision members with Senior Care Options Plans. Senior Care Options (SCO) is a comprehensive health plan that covers all services usually covered by Medicare and MassHealth. SCO is a fully integrated dual eligible special needs plan and is offered to individuals who have Medicaid (MassHealth Standard) and are over the age of 65. The majority of members have dual eligibility.
UnitedHealthcare was selected to provide vision benefits to Senior Care Options (SCO) members beginning on January 1, 2016. Benefits include a $0 copay for routine eye exams and a $0 copay for contact lenses or 1 pair of frames up to $200 every year.
Through SCO, members are able to select two pairs of glasses in lieu of bifocals. For SCO members to receive this second pair benefit, the member must have one or more of the following conditions. The condition(s) must be documented:
1. The member’s prescription cannot satisfactorily be made into bifocal lenses. 2. The member has shown an inability to adjust to bifocals. 3. The member has a physical disability (for example, severe arthritis) that
would preclude or impede adjustment to bifocals. 4. The member’s advanced age would make adjustment to bifocals unduly difficult. 5. The member’s occupation would make bifocals hazardous. 6. The member has a marked facial asymmetry.
If a SCO member has one or more of the conditions listed above, you must submit the “Two Pairs of Glasses in Lieu of Bifocals Form” (found in this manual) with a claim according to the instructions provided.
4.7 Children’s Eye Care Program The Children’s Eye Care Program offers an additional benefit to Commercial vision members up to age 13 that includes a second eye exam and replacement eyeglass benefit each benefit period. The benefit

Network Administration Manual | Section 4: Benefit Overview
14
would include a second eye exam that would follow the same copay as the core benefit and follow the below requirements for the replacement eyeglass benefit:
1. There is a cumulative change of 0.50 diopters or greater in sphere and/or cylinder power 2. There is a shift in cylinder axis that results in an increase in visual acuity 3. Follows the same copays, frame allowance, and price protections as the core plan 4. The 60-day window of time between initial pair and replacement to ensure the need for materials
is based upon the applicable change in prescription.
4.8 Maternity Benefit The Maternity Benefit offers an additional benefit to Commercial vision members who are pregnant or breastfeeding that includes a second eye exam and replacement eyeglass benefit during their pregnancy or while breastfeeding. The benefit would follow the below requirements:
1. The additional exam and replacement materials must occur at least 60 days from the most recent use of the member’s benefit.
2. The additional exam and replacement materials must be billed with the diagnosis codes Z33.1 or Z39.1 for claim processing.
3. Coverage of the glasses is dependent upon a cumulative change of 0.50 diopters or greater in sphere and/or cylinder power
4. There is a shift in cylinder axis that results in an increase in visual acuity 5. Follows the same copays, frame allowance, and price protections as the core plan
4.9 Post-Laser Non-Prescription Sunglass Frame Benefit Some members are eligible to use an allowance toward non-prescription sunglasses after laser correction surgery. The members’ eligibility for this benefit will show on their benefit summary. This benefit offers eligible members a once-per-lifetime frame allowance to use toward non-prescription sunglass frames in lieu of prescription eyewear following laser correction surgery.
1. Verify member eligibility at spectera.com 2. Use diagnosis code Z98.890 and procedure code S0518 on your claim 3. Claims must be filed via hardcopy or EDI
4.10 Formularies Contact Lens Formularies We refer to the contact lenses on our formulary as “selection” contact lenses. Our formularies include a variety of contact lenses, including planned replacements.
Contact lenses not listed on the formulary are referred to as "non-selection." Claims for non-selection contact lenses can be submitted at spectera.com. All non-selection contact lenses must be supplied by your office.
Note: Not all plans use the same contact lens formulary. When you verify member benefits at spectera.com, you can confirm which formulary to use in the Contact Lens section of the benefit summary. It's important to check the formulary when you verify benefits. Provide the maximum benefit to your members by directing them to materials that are covered by their plan.
Progressives Lens Formulary The progressive lenses on our formulary are classified in five categories.
Anti-Reflective Coating Formulary The anti-reflective lenses on our formulary are classified in four categories.

Network Administration Manual | Section 4: Benefit Overview
15
Non-Formulary Progressives and Anti-Reflective Coatings Non-formulary progressive or anti-reflective products will default to the “All Other Ophthalmic Lens Options” category on your fee schedule for reimbursement. Products with brands not included on the formularies must be administered as non-formulary. If you have questions about non-formulary products, please contact your Provider Relations Advocate.
Our formularies can be found online at spectera.com Formulary Lists

Network Administration Manual | Section 4: Benefit Overview
16
4.11 Provider Warranty – For Providers Who Do Not Use The Lab Network Prescription Change
If you made an error when prescribing eyeglass lenses, or if the member has a condition that might cause the prescription to change, we require you to offer a one-time prescription change at no charge if it occurs within 90 days from the time the glasses were dispensed. However, if your policy to offer changes for longer than 90 days, your policy should be used instead.
Manufacturer’s Defects on Frames and/or Lenses
If a member received materials that are deemed “defective,” we require you to extend a one- time replacement of the frame and/or lenses at no charge. The member must return the eyewear within one year of initial dispensing to the provider or within the time specified by the manufacturer’s warranty, whichever is longer. This includes replacing defective frames without charging a fee to the member or to us, and replacing all materials when the defective frame is discontinued or no longer available to be replaced.
Reinstating Member Benefits and Processing Refunds to Member and Lab Network When a member requests a refund because of cancellation of an order or because you have exhausted all alternatives and cannot satisfy the member, send the request to [email protected], fax the request to (888) 751-0933, or call Customer Service.
Include the following details on the request: your provider number, member name, member ID number, and date of service, requested refund amount, and reason for the refund (i.e., member returned glasses). We will reinstate the member benefits once the request has been processed.

Network Administration Manual | Section 4: Benefit Overview
17
4.12 Eye Health & Wellness As a valued network eye care professional, you are part of UnitedHealthcare’s unique approach to eye health and wellness. UnitedHealthcare helps you to provide care to your patients, which in turn helps them make better decisions about their health.
UnitedHealthcare’s integrated approach represents the critical partnerships between health care professionals, patients and insurance providers. You help patients identify and manage chronic health conditions that may affect their eyes, and we offer educational experiences that empower patients to manage their ongoing health care needs.
UnitedHealthcare’s approach offers: • Proactive outreach, motivating patients with chronic conditions to actively monitor their eye
health. • Dilation recommendations triggered by patients’ medical diagnoses to help you plan the extra
time you may need to spend with the patients. • Patient education materials available at spectera.com. • Easy referral forms to communicate relevant health information to the patient’s PCP or Specialist. • Care integration that is possible because of the patient diagnosis data you provide to support an
interactive disease management approach.
Dilated Fundus Examination (DFE) Recommendation When we are made aware of a condition with the potential for ocular complications, you will receive a DFE recommendation when you check eligibility and benefits at spectera.com. The DFE recommendation serves as a reminder to help you deliver excellent ongoing care to our members.
Glaucoma Screenings In order to support the collection of data for HEDIS quality measure reporting, you are required to tell us if a glaucoma screening was performed when submitting your claims online.
The Centers for Medicare and Medicaid Services (CMS) states that a glaucoma screening includes tonometry and a dilated examination of the optic nerve head. The CMS requirements are met if both the dilation and the glaucoma boxes are checked “Yes” when submitting a claim online.
4.13 HEDIS / Star Performance Reporting Because Spectera administers benefits for UnitedHealthcare and other medical plans, we are invested in improving members overall health care quality and cost. When you include appropriate CPTII and ICD-10 codes on your claims, it helps us support our health plan partners as they manage members’ medical conditions and identify candidates for disease management programs. The inclusion of appropriate codes also helps to improve plan quality as measured by HEDIS and Stars ratings. Appropriate coding also limits requests for HEDIS and Star chart reviews, which allow your practice to spend more time on patient care.
Spectera only requires CPTII coding for diabetic retinopathy screening at this time. However, you may include additional codes on your claims. • Claims for members who have diabetes and present without evidence of retinopathy should
include appropriate ICD-10 diagnosis codes and the applicable CPTII code: 2023F, 2025F or 2033F
• Claims for members who have diabetes and present with evidence of retinopathy should include the appropriate ICD-10 diagnosis code and the applicable CPTII code: 2022F, 2024F or 2026F

Network Administration Manual | Section 4: Benefit Overview
18
• Claims for members who have diabetes and present with low risk for retinopathy (no evidence of retinopathy in the prior year) should include the appropriate ICD-10 diagnosis code and the applicable CPT II code: 3072F
Important: • Always bill the appropriate ICD-10 code, including any medical diagnosis codes, at the highest level of
specificity. • A patient’s medical record should always support the CPTI, CPTII and ICD-10 codes billed.
Normal billing rules apply. The requirements listed here should be included in your billing process.
ICD-10 Diagnosis Codes**
Nonproliferative Diabetic Retinopathy (NPDR)
Type 1 Type 2
E10.3211, E10.3212, E10.3213, E10.3291, E10.3292, E10.3293, E10.3311, E10.3312, E10.3313, E10.3391, E10.3392, E10.3393, E10.3411, E10.3412, E10.3413, E10.3491, E10.3492, E10.3493
E11.3211, E11.3212, E11.3213, E11.3291, E11.3292, E11.3293, E11.3311, E11.3312, E11.3313, E11.3391, E11.3392, E11.3393, E11.3411, E11.3412, E11.3413, E11.3491, E11.3492, E11.3493
Proliferative Diabetic Retinopathy (PDR)
Type 1 Type 2
E10.3511, E10.3512, E10.3513, E10.3521, E10.3522, E10.3523, E10.3531, E10.3532, E10.3533, E10.3541, E10.3542, E10.3543, E10.3551, E10.3552, E10.3553, E10.3591, E10.3592, E10.3593
E11.3511, E11.3512, E11.3513, E11.3521, E11.3522, E11.3523, E11.3531, E11.3532, E11.3533, E11.3541, E11.3542, E11.3543, E11.3551, E11.3552, E11.3553, E11.3591, E11.3592, E11.3593
CPTII Code* Description
2022F Dilated retinal eye exam with interpretation by an ophthalmologist or optometrist documented and reviewed.
2023F Dilated retinal eye exam with interpretation by an ophthalmologist or optometrist documented and reviewed; without evidence of retinopathy.
2024F Seven standard field stereoscopic photos with interpretation by an ophthalmologist or optometrist.
2025F Seven standard field stereoscopic retinal photos with interpretation by an ophthalmologist or optometrist documented and reviewed; without evidence of retinopathy.
2026F Eye imaging validated to match diagnosis from seven standard field stereoscopic photos results documented and reviewed.
CPTII Code* Description
2033F Eye imaging validated to match diagnosis from seven standard field stereoscopic retinal photos results documented and reviewed; without evidence of retinopathy.
3072F Low risk for retinopathy (no evidence of retinopathy in the prior year)

Network Administration Manual | Section 4: Benefit Overview
19
* CPTII codes are tracking codes used for performance measurement. They should be billed in the CPT/HCPCS field on your claim form and submitted on the same claim as the CPTI codes. CPTII codes do not have relative value and can be billed with a $0 charge amount. ** This list contains the most common ICD-10 codes.

Network Administration Manual | Section 5: Administering Member Benefits
20
Section 5: Administering Member Benefits 5.1 Member Identification Cards
Our members can print personalized ID cards (shown below) from the member website. However, an ID card is not required for our members to receive services. Additionally, an ID card does not guarantee eligibility.
SAMPLE ID CARDS:

Network Administration Manual | Section 5: Administering Member Benefits
21
5.2 Product Brands Today’s health care environment can be hard for patients to understand. As a UnitedHealthcare Vision Network / Spectera Vision Network health care professional, you can help patients avoid confusion by referencing their insurance benefits by the correct brand names.
Patients may not be familiar with our network names and will typically use their insurance plan name to identify themselves. As a health care professional in our networks, you’ll see patients who are UnitedHealthcare members and other patients with a variety of plan names. Get to know the plans we serve to better support your patients and their eye care experience
© 2021 United HealthCare Services, Inc. All Rights Reserved

Network Administration Manual | Section 5: Administering Member Benefits
22
5.3 Eligibility and Benefits Verification Our members may have benefits under a variety of product brands. Be advised that the benefit summary is not a guarantee of payment.
Note: Some members’ networks may be restricted to certain providers. If you are not in a member’s network, you will receive this message when checking eligibility: “Not Eligible for Location/Provider. Instruct the member to visit their insurance website or call Customer Service to find a provider that participates in their network.”
5.4 Determining Member Responsibility Members are responsible to pay you for their member expenses as defined in their vision plans. Member expenses include, but are not limited to, copays, coinsurance and deductibles. In addition to member expenses, you may also collect payment for non-covered services, such as additional pairs of glasses.
When you submit your claim or order on spectera.com, the claim is auto-adjudicated and the member out of pocket is calculated for you in real time.
5.5 Sales Tax In states where the retail sale of prescription eyeglasses are subject to sales tax, the provider is responsible for charging the appropriate amount of sales tax to the member as well as remitting the sales tax to the state taxing authority. Refer to your state’s tax laws and regulations for specific guidance.

Network Administration Manual | Section 6: Materials Ordering
23
Section 6: Materials Ordering
FOR PROVIDERS WHO USE THE LAB NETWORK: Material orders should be submitted online at spectera.com. Your claim will be processed automatically once the order has been received. The lab network consists of ‘integrated’ and ‘non-integrated’ laboratories. All labs operate identically, however for non-integrated labs, you must call the lab directly to create an account if you do not have one already with that lab. After creating the account with the non-integrated lab, allow 24 hours prior to associating with the lab within the portal and submitting an order. Refer to the online documentation and training for more information including a list of integrated and non-integrated labs.
Note: A provider- or member-supplied frame must be received at the chosen lab before the order can be started. The lab may cancel an order when the provider-supplied frame has not been received within 45 days. In the event this occurs, you will be contacted with instructions on how to re-enter the order once the frame is available to be sent in.
To ensure the fastest turnaround times possible, enter orders on spectera.com.
6.1 Materials Ordering Online Orders You are required to utilize the Lab Network for all member orders. Use our online order entry service at spectera.com >Home Page>Get Started to submit your material orders.
Lab Exceptions for Urgent Member Needs The Lab Network fulfills all orders for eyewear materials. In the unlikely event of an urgent situation, you can request approval to use a non-network lab to meet the member’s need. You may request approval by calling the Provider Services Departmentat1-800-638-9382.
Requests should only be made in urgent situations when the member does not have other serviceable glasses or contact lenses and their well-being is at risk unless the materials are delivered more quickly than the Lab Network can supply them. For example:
• Member is unable to drive or function at home or work • Student cannot function at school • Member has an immediate military deployment deadline
Non-network lab approval cannot be considered for reasons of convenience or preference such as vacations, business trips, or other life events.
Your office will be paid in accordance with the terms of the fee schedule in your contract. Your payment will appear on your next remittance advice.
Your lab bill must match the approved prescription. Any change or add-on product will void the approval. In all cases, lab errors and remakes are the responsibility of the fabricating lab. Members may not bear any cost in addition to what is required by their in-network benefit.
6.2 What to Do When a Member Returns Materials When a member returns materials, you are responsible for:
• Requesting that member benefits be reinstated • Requesting that the claim be reprocessed so your payment is recouped

Network Administration Manual | Section 6: Materials Ordering
24
• Reimbursing the member for any monies paid for materials, including copays and coinsurance
Note: A member returning of materials does not guarantee a reinstatement of benefits. Please refer to Order Cancellation Policy section of this manual for more information.

Network Administration Manual | Section 7: Lab Network Warranty & Policies
25
Section 7: Lab Network Warranty & Policies – For Providers Who Use the Lab Network Our materials replacement and warranty will apply in the following instances: Re-dos will be limited to one per order and will also include changes requested when the order is in process at the lab. A provider redo includes changes to the original prescription lens order regardless if the order has shipped from the lab or not. For example, a change in prescription request would be honored for an order that has not shipped; however, subsequent replacement requests will not be honored. After the one-time replacement has been used, the provider is responsible for any additional replacement requests. All associated charges will be subsequently handled between you and the lab as a private transaction.
7.1 One-Time Doctor Redo Request or Changes to Orders We will replace prescription lenses under the following conditions and limitations:
• The redo must be requested within 90 days of shipment • The redo must be for the same patient and same provider as the original order. • The original materials and packing slip must be sent back to the original laboratory • Any and all enhancements or upgrades after the order has been shipped which deviate from the original
order must be handled as a private transaction between you and the lab. • Below are some examples of redo request scenarios. This list is not exhaustive, and any questions should
be directed towards the lab network customer service:
Allowed by one-time redo policy, but subject to price difference charges for upgrades as
applicable
Not Allowed by one-time redo policy
• Change or addition of tint or coatings • Change or addition of any lens treatment
such as polarized lenses, photochromic, blue treatment
• Change from plastic to high-index • Any change in Rx such as but not limited to
power, segment height, axis, etc. • A change in lens style or brand such as
changing a style from one manufacturer to another
• Redo is requested after 90 Days of Shipment
• A redo is requested to a lab which is different than the original lab
• Loss, Abuse and misuse by provider or member
• Lab errors or warranties (lab warranty, lens manufacturer warranty, or frame manufacturer warranty) will not
count against you as the one-time redo and should be submitted to the originating lab for replacement • A redo of lenses for a frame change or restyle will count as the one-time redo as long as the replacement
frame is supplied by the provider or member. • Some examples of when you will be charged for upgrades after an order has been shipped include:
o RX change to initiate the redo, but AR is added. The upgrade to AR will be charged o Material change from plastic to high index initiates the redo. The difference in price from plastic to
high index will be charged by the lab o A change from bifocal to trifocal initiates the redo and blue treatment is requested. The difference
in price from bifocal to trifocal AND the upgrade to blue treatment will be charged by the lab o A change from single vision to progressive initiates the redo. The difference in price from single
vision to progressive would be charged by the lab.

Network Administration Manual | Section 7: Lab Network Warranty & Policies
26
o Add AR to an original order and no other change will initiate the one-time redo. The difference in price for adding AR will be charged by the lab.
• Pricing for any enhancements or upgrades are dictated by the lab or by your own established rates with the lab.
• Non-Adapt situations with progressive lenses follow the manufacturer’s progressive warranty and are not counted against you as the one-time redo. Please contact the laboratory for information regarding these redo requests.
7.2 Laboratory Error or Defective Materials We are committed to supplying a quality product. In the case of a lab error or defective materials, new lenses will be processed immediately. Laboratory error or defective materials do not count against you as the one- time redo. Requests must be within 6 months of shipment to your office, and all materials should be returned to the originating laboratory for evaluation. Replacement lenses will be made to the exact specifications of the original prescription. The price difference for any additions or changes to enhancements or upgrades to materials or lens type will be charged by the laboratory.
7.3 Lab Network Supplied Frames As of 5/1/2021, all frames are provider supplied. The following information is supplied for warranty of lab supplied frames for orders prior to 5/1/2021. All frames purchased from Vendor are guaranteed against defects in material and workmanship for one year. Defective frames replaced under warranty by our lab must be returned to the lab to make the frame replacement. Should a frame be discontinued during the warranty period, the lab will replace the frame with a new one of equal or lesser value. Defective frames are defined as: 1. Separation of metal/zyl attachments, 2. Separation along solder points, 3. Visual cosmetic defects upon initial inspection before dispensing, 4. Visual defects in workmanship upon initial inspection before dispensing.
Non-Defective frames are defined as: 1. Error during adjustments causing separation, 2. Bubbles or rolled eyewear due to excessive heat generated by salt pan, 3. Undue stress on frame material during insertion of lenses by the provider’s office, 4. Excessive twisting of pad arm in nose pad adjustments, 5. Frame abuse by customer, 6. Any problem that has occurred after obvious prolonged wear by a consumer.
7.4 Provider Supplied Frames Whenever a frame is supplied by your office, it will be your responsibility to contact the lab network directly to obtain a prepaid shipping label. It will also be your responsibility to honor the one-year frame warranty or the manufacturer’s warranty. This includes replacing defective frames without a fee charged to our member or to us. It also includes replacing the lenses when the defective frame is discontinued and cannot be replaced. When the frame is supplied by your office, the lab network will bear the shipping cost to the lab; however, the lab is not responsible for frames lost in transit that do not have a tracking number. Please ensure that you keep a copy of your tracking numbers.
7.5 Cancel Order Policy To cancel or replace an order that is in process at the lab but not yet shipped, call the Essilor Customer Care Center directly at 800-638-9382. Either a cancelation or a redo/replacement will consume the allowed one-time redo. The member’s benefit will not be reinstated, so out-of-pocket amounts should not be refunded.
7.6 Anti-Reflective Coatings Please contact the laboratory about specific anti-reflective coating warranties. Warranties may vary. Instructions for anti-reflective warranty claims and associated charges will be provided by the originating laboratory

Network Administration Manual | Section 7: Lab Network Warranty & Policies
27
7.7 Scratch Resistant Coating All scratch resistant coated lenses are guaranteed for one year from date of order and will be replaced at no charge during that one year if damaged due to scratching. Lenses must be replaced in identical form. To qualify, please return lenses along with a copy of original invoice or packing list. A maximum of one replacement per Rx order is allowed. Front surface scratches through normal use will be covered; however, abuse of the lens will not be covered.
7.8 Progressive Lenses Patient Satisfaction Please refer to the manufacturer's specific warranty first before reverting to the following warranty policy as a manufacturer's warranty may be more comprehensive. If requested within 90 days of shipment, the lab network will replace non-adapt progressive lenses with single vision or standard multifocal lenses. The progressive lenses must be returned to the lab upon receipt of the replacement lenses. New lenses will be made to the original prescription and edged to the original frame shape. There is a one-time replacement for non-adapt members, and the progressive lens option fee is non-refundable.
7.9 Materials Sent by the Provider’s Office Please do not send materials to the lab unless specifically requested to do so by a lab representative or website messaging. Spectera Lab Network nor our network labs assume liability for unsolicited materials that are lost or damaged in transit. Unsolicited materials sent to a lab will be returned to your office without risk or liability to the lab.
Demo Lenses are handled as carefully as possible; however, the network laboratories are not responsible for the integrity and/or return of unsolicited sample lenses. Please retain demo lenses at your office unless they are required to fulfill the prescription.
7.10 Member Materials When forwarding a member’s own frame and lenses, please have the member sign the Patient Waiver Form, located on spectera.com. You may enclose a copy of the form with the materials. A member’s frame and lenses are handled as carefully as possible; however, the lab assumes no liability for the existing materials, and may refuse to fabricate lenses if the member’s frame is in unacceptable condition. Our laboratories are not responsible for the integrity of previously worn frames or for the integrity and return of the member’s existing lenses. Our network laboratories are not responsible for materials lost in shipment to them. Lost or damaged materials that are shipped via the laboratory’s pre-paid return labels are not the responsibility of the laboratory and do not result in Spectera filing a claim for the loss
7.11 Product Liability Our lab network cannot supply standard dress thickness lenses in a frame marked with a Z87 stamp. These frames require safety thickness lenses. Our lab network does not fabricate lenses for non-ophthalmic quality frames or frames deemed as “Not Rx Adaptable” by the manufacturer. Lens thickness requests that are outside the tolerance of our laboratory’s processing standards cannot be honored.
7.12 Drilled Rimless and Metal-Grooved Frames For Safety and lens integrity reasons, drilled rimless mountings are not permitted in CR 39 material. Orders for drilled rimless frames utilizing Polycarbonate, Trivex, Plastic 1.60 Index, 1.66 Index, 1.67 Index and 1.74 Index

Network Administration Manual | Section 7: Lab Network Warranty & Policies
28
materials have a one time, 1-year warranty against splitting and cracking. Please contact the originating lab for warranty claims.
7.13 Uncut or Edged “Lenses-Only” Orders If preferred, your office may request “lenses only” (edged or uncut) for a specified frame. Please refer to the instructions on spectera.com for proper ordering instructions and exclusions. Uncut lenses must be examined at your office before edging. Once edged, the lenses cannot be remade chargeable to lab error. Redo requests after edging will be applied to a warranty, unless the lab verifies a manufacturer’s defect. Please refer to the instructions on spectera.com for accurate ordering instructions and exclusions. Uncut lenses that are processed incorrectly by the lab must be returned for evaluation with the original invoice before new lenses will be processed.
7.14 Contact Lenses Contact Lenses can be returned one time for any reason, within 60 days of shipment to your office. When you receive a contact lens order, always confirm the order and prescription accuracy before opening or marking the box or vials. Boxes or vials that have been opened, marked, damaged or otherwise altered may not be returned. Returns must include a tracking number and be placed in a box to avoid damage during transit. All contact lenses must be returned to ABB Optical Group at:
UHC/Spectera Vision Network Returns
c/o ABB Optical Group [Insert your invoice number]
12301 NW 39th St. Coral Springs, FL 33065
Contact lenses mailed directly to the member that are lost in shipment will be replaced and shipped directly to your office.
7.15 Prescription Change In the event that your office made an error when prescribing the eyeglass lenses, or if the member has a condition that might cause the prescription to change, we require you to offer a one-time prescription change at no charge if it occurs within 90 days from the time the glasses were dispensed.
7.16 The Laboratory Network's Right to Cancel Orders The laboratory network reserves the right to cancel an order after 45 days if the lab has not received a required frame from the provider’s office.
7.17 Lab Material Returns Materials should be returned to the processing lab only when requested or required for a redo or warranty. Neither the lab nor UHC is responsible for materials lost or damaged during shipping. The return of materials does not constitute the reinstatement of member benefits nor the return of surcharges. Initial charges are non-refundable with the exception of orders canceled within 90 minutes of entry. If returned glasses are not requested by the lab or required for a redo or warranty, the materials are not guaranteed to be returned back to you.
Network Administration Manual | Section 8: Claims
29
Section 8: Claims
8.1 How to File a Claim We strive to make filing a claim as easy as possible for you and your practice. Whether you submit claims electronically using spectera.com or on paper, reference the information outlined in the Billing Guide in this Manual. All claims must be submitted within 90 days of the date of service as described in your contract.
Our vision plans cover only routine eye exams and materials. Services and procedures that you perform to treat and manage an eye injury or ocular disease should be billed to the member’s medical plan.
Our proprietary Billing and Code Modifier Guide will help you to accurately bill us for your services and materials.
• Enter the procedures, services or supplies using Current Procedural Terminology (CPT) and Healthcare
Common Procedure Coding System (HCPCS) codes. • A Modifier Code should be added to the procedures, services, or supplies field for contact lenses and
member lens options as appropriate. • Refractions are not separately reimbursable when filed along with HCPCS codes for routine
ophthalmological exams (S-codes). • Enter the appropriate diagnosis codes on all claims, including claims for materials only. Valid diagnosis
codes are required on all claims. Always code to the highest degree of specificity when indicating diagnosis. A partial diagnosis code list can be found in the Appendix to this Manual.
• Always include the Subscriber/Member 2-digit suffix on your claim. This will ensure that the claim will process for the correct family member.
Example: Subscriber/Member: 123456789 00
IMPORTANT INFORMATION ABOUT EXAM CLAIMS
When you submit a claim for an exam, you must include the rendering practitioner’s NPI code. We strongly encourage the submission of all other NPIs to allow efficient claims processing and avoid delays or denials.
8.2 Clean Claims A “clean claim" is a claim that includes all the information required for processing (as described in this Manual or other instructions provided by us) and does not include claims pended for investigation of potential fraudulent or abusive billing practices. However, if a claim is subject to state claims payment regulation and the applicable state regulation uses a conflicting definition of "complete claim" or "clean claim," the state definition will be used to determine whether that state-regulated claim is a "clean claim" for the purposes of this section.
Whether you submit your claim online, electronically or on paper, a clean claim includes the following information. Additional information may be required for particular types of services, circumstances, or state requirements: • Member’s name, address, gender, date of birth • Primary member’s name and ID number (always include the Subscriber/Member 2-digit suffix on
your claim. This will ensure that the claim will process for the correct family member.)

Network Administration Manual | Section 8: Claims
30
• Name, signature, ‘remit to’ address, and phone number of the practitioner or health care provider performing the service described in your contract; practitioner or health care provider’s NPI; and federal tax id number
• Date of service(s), place of service(s) and number of services(units) rendered • Current CPT-4 and HCPCS procedure codes with modifiers where appropriate • ICD-10 diagnosis codes to the highest level of specificity • Referring physician’s name and tax id number (if applicable) • Charges per service and total charges • Electronic claims must be HIPAA-compliant in order to be considered clean claims, using the
applicable format that complies with all federal laws related to electronic health care claims, including applicable implementation guides, companion guides, and trading partner agreements.
Submitting Corrected Claims and Claims Adjustments Many corrected claims and claims adjustments may be submitted through your normal EDI process. For more information about this functionality, please see Section 8.4, Electronic Claims Submission. You can also submit corrected claims and claims adjustments by sending us the original claim marked with “CORRECTED” at the top. You may also submit your corrected claims and claims adjustments using the Optional Corrected Claim – Standard Cover Sheet in this manual.
Fax or email your corrected claim and form, if applicable to: Fax: (888) 751-0933 Email: [email protected].
8.3 National Provider Identification (NPI) The Health Insurance Portability and Accountability Act (HIPAA), federal Medicare regulations, and many state Medicaid agencies mandate the adoption and use of a standardized National Provider Identifier (NPI) for all health care professionals. In compliance with HIPAA, all covered health care providers and organizations must obtain an NPI for identification purposes in standard electronic transactions. In addition, based on state-specific regulations, NPI may be required on paper claims. HIPAA defines a covered health care provider as any provider who transmits health information in electronic form in connection with a transaction for which standards have been adopted. These covered health care providers must obtain an NPI and use this number in all HIPAA transactions in accordance with the instructions in the Implementation Guides.
• To avoid payment delays or denials, we require a valid Billing NPI code be submitted on both paper and electronic claims. In addition, we strongly encourage the submission of all other required NPIs.
• The NPI information that you report to us is essential in allowing us to efficiently process claims and to avoid delays or denials.
8.4 Electronic Claims Submission
We accept initial filing of claims through EDI submission via the UnitedHealth Group Corporate EDI connection. EDI files are sent to Optum Insight and processed by Spectera. Our payer ID is 00773.
The following EDI transactions may be performed in batch or real-time mode, based on your connectivity method:
• 270/271 Eligibility and Benefit Inquiry and Response transaction provides ability to inquire on eligibility and benefits associated with a subscriber or dependent.

Network Administration Manual | Section 8: Claims
31
• 276/277 Claim Status Inquiry and Response transaction allows inquiry on the status of a claim after it has been sent to a payer, whether submitted on paper or electronically.
The following EDI transactions must be submitted in batch: • 837/835 Claim submission and resulting payment details. • 999 and 277CA: File and claim-level acknowledgment responses.
We are able to receive transactions from all major clearinghouses, such as TriZetto, Relay Health, Change Healthcare, Next Gen, Ability, Networks, SSI Group and many more.
If you are interested in a clearinghouse connection, you or your clearinghouse can directly contact the EDI Sales Team at Optum Insight, at (800) 341-6141, option 2. For service and support, call 877-309-4256 or 800-341-6141, option 1. Submitting Corrected Claims and Claims Adjustments Electronically Many corrected claims may be submitted through your normal EDI process. For file format detail, see the complete EDI companion guide, found on spectera.com. At this time, an adjustment needed as a result of a member returning materials must be submitted on paper. Submitting claim corrections and adjustments through EDI is an optional feature. If you wish to continue to submit corrections via paper, see Section 8.2 of this manual, Clean Claims – Submitting Corrected Claims and Claims Adjustments.
8.5 Coordination of Benefits As a rule, we do not coordinate benefits with other insurance plans or payers and you should always bill us as the primary payer for routine vision claims. Exceptions to this policy are for participants of the Office of Personnel Management Federal Dental/Vision Program (OPMFEDVIP).
When a member visits a provider who participates with both the Federal Employees Health Benefits Program (FEHBP) medical plan and the Federal Employees Dental/Vision Program (FEDVIP) plan, the FEHBP medical plan is primary and Spectera is secondary.
Spectera will initially process claims for FEDVIP participants as primary. Claim service lines for members known to have vision coverage through their medical FEHBP plans will be reviewed and benefits will be coordinated with Spectera as secondary for services covered by both medical and vision.
If you filed a claim with Spectera and it was denied with a 1046 exception (No Primary Insurer EOB Present), fax the medical carrier’s EOB/proof of denial, the claim and the corrected claim coversheet to (888) 751-0933. If you filed the claim with the member’s medical carrier before submitting to Spectera, fax the medical EOB/proof of denial and the claim on a CMS1500 form to (248) 733-6060.
8.6 Provider Remittance Advice If you are enrolled in OptumPay then your Provider Remittance Advice (PRA) is available online. If you receive paper checks, the PRA will be mailed with each payment.

Network Administration Manual | Section 8: Claims
32
Your PRA is included with each and every payment and is a statement of your activity with our plans.
All balances owed to us must be submitted no later than 30 days after receipt of PRA. Please return the bottom portion of the PRA with your payment. The PRA shows the amounts being paid to you, minus any amounts due to us for expenses collected from the member for materials. If the amount on your statement is a positive balance, payment to you will be enclosed or wired electronically to your bank account on file. If the amount on your statement is a negative balance, no check will be enclosed, nor will any payment be wired electronically to your bank account on file. A negative balance on your statement indicates you collected more money than the contracted amounts due to you for service that you provided. Those amounts may be in the form of member copays, lens options charges, and/or overage amounts for frames and lenses. Submit payments to: ATTN: Accounts Receivable Spectera, Inc. PO Box 645469 Pittsburgh, PA 15264-5252
Note: A list of commonly used Provider Remittance Advice remark codes and definitions can be found in the billing guide in the appendix.
Payments are issued weekly and can be viewed at spectera.com. They are available when you receive a payment from us. If you did not receive a check with your PRA that means you have a negative balance on your statement. A negative balance means that you collected more money than the contracted amounts due to you for services that you provided. The negative amount is due to us no later than 30 days after the receipt of the PRA.
8.7 Electronic Payments and Statements (Optum Pay)
We have partnered with OptumHealth Financial Services to offer electronic payments and statements (Optum Pay) to you. Optum Pay allows you to receive payments from us electronically. It also gives you online access to payment information for easy billing and payment reconciliation. By enrolling in Optum Pay, you can reduce paperwork, save time and receive payments faster. You can use Optum Pay whether you submit claims electronically or on paper.
Instead of checks arriving in the mail, your payments are deposited directly into your office’s checking account. You receive a payment notification via e-mail one business day in advance, and you can view the amount of the payment and the corresponding PRAs online.
There is no fee for enrolling in Optum Pay, and no special software or licensing is required. Optum Pay offers some premium features for a monthly fee. All you need is a computer with Internet access. Optum Pay cannot be used in debit transactions to your account. To enroll, go to spectera.com Home PageLog into EPS.

Network Administration Manual | Section 9: Standards of Care
33
Section 9: Standards of Care
9.1 Clinical Practice Guidelines We recommend the following clinical practice guidelines for a comprehensive eye examination and refraction in order to ensure that plan members receive services consistent with the guidelines established by the American Optometric Association (AOA). You can find the AOA’s Clinical Practice Guidelines here. Care Standards: Eye Health Examinations Comprehensive eye exams are critical, not only to correct and preserve vision, but also for the early detection of systemic disease.1 To support our commitment to quality care for all patients, we have developed Care Standards for eye health examinations. Developed by our Chief Eye Care Officer and our Peer Committee, these guidelines reflect our focus on early detection and prevention. The following elements are required for all comprehensive eye health examinations: Element 1: Reason for Visit What is expected: The patient should be directly questioned as to why they presented for the encounter. The patient should also be asked about issues with their eyes and vision or other problems that may be related to the visual system. The answers to these questions should be documented in the medical record. Element 2: Review of Systems What is expected: Each of the following systems should be queried and the patients’ response recorded. For all positive responses, additional questioning may be indicated.
• Cardiovascular • Constitutional • Endocrine • Gastrointestinal • Head • Hematologic/Lymphatic • Immunologic • Integumentary • Musculoskeletal • Neurological • Psychiatric • Respiratory
Element 3: Medications and Allergies What is expected: Medication name and dosage for all drugs or supplements the patient is taking should be recorded. If no medication, this should be indicated on the chart as none and not left blank. For allergies related to medications, the name should be listed as well as the adverse effect the member experienced. If the patient experiences environmental or food allergies, these should be noted as well. If no allergies are reported, the chart should indicate this. Element 4: Ocular History; Family History; Orientation, Mood and Affect What is expected: A detailed list of the patient’s previous eye problems and procedures should be listed. The family history should query medical problems including diabetes, hypertension, thyroid problems and cancer in addition to eye problems such as cataracts, glaucoma, and macular degeneration. The patients should be

Network Administration Manual | Section 9: Standards of Care
34
asked if they know the day, date and their current location. The clinician should note the validity and assess whether the patient’s mood or affect is normal or abnormal. Element 5: Entering Visual Acuity at Distance and Near What is expected: A measurement of visual acuity both uncorrected and with the patient’s habitual correction should be performed at both distance and near. Element 6: Entering Tests, Including Vital Signs and External Examination What is expected:
Measurement of the following: • Height • Weight • Body mass index • Blood pressure for patients age 13 and older • Pulse • Testing of pupil response • Direct • Consensual • Swinging flashlight • Extra ocular muscle testing • Cover test • Visual field • Confrontation or • Automated test
Element 7: Refraction What is expected: The refraction is the subjective test that allows for the patient’s visual perception of the physical refractive error. Auto-refraction, by itself, is not an acceptable measurement Element 8: Near Point Testing What is expected: Testing may include measurements of accommodation and/or convergence as well as additional testing as determined by the provider (e.g. evaluation of saccadic eye movements). Element 9: Current Optical Prescriptions What is expected: The current glasses prescription should be measured and recorded in the refractive testing area. Element 10: Corneal Curvature What is expected: The measurement should be recorded in the refractive testing area when indicated. Element 11: Biomicroscopy What is expected: Use of the slit lampbiomicroscope to inspect all anterior segment eye structures including the lids and lashes, tear film, cornea, anterior chamber, angle grade, iris and lens. The documentation must be individualized based on the findings of the examination. Cloned language in electronic health records should be carefully reviewed and revised to be consistent with the rest of the documentation in the record. Element 12: Intraocular Pressure What is expected: The type of instrument used as well as the time of measurement should be included with the numerical finding. Element 13: Optic Nerve Head Evaluation What is expected: The optic nerve must be visualized, and details recorded at each visit. The details of the evaluation of the Optic nerve should include all aspects of the nerve itself, including cup to disc ratio, disc

Network Administration Manual | Section 9: Standards of Care
35
margin, disc size, color, thickness and vessel caliber. The exam may be performed with a minimum of a fundus lens, or a direct ophthalmoscope, indirect ophthalmoscope, or photographically. Element 14: Dilated Fundus Examination What is expected: A thorough inspection of the optic nerve, macula, vascular tree and retinal surface with a fundus lens and biomicroscope, a binocular indirect ophthalmoscope and/or a wide-angle retinal imaging system. Document the method of examination. Although retinal imaging is acceptable in some cases, it is not a substitute for a binocular physical retina examination. All providers must be licensed and capable to dilate the pupil and perform the physical retina examination. Element 15: Diagnosis What is expected: These can be a refractive diagnosis such as Myopia, Astigmatism, Emmetropia, Hyperopia, or Presbyopia or medical eye diagnoses such as Cataract, Corneal Dystrophy, Choroidal Nevus or Glaucoma. Pertinent systemic medical diagnoses such as diabetes should also be listed. Element 16: Assessment, Management and Treatment Plan What is expected: In this section, the provider should summarize the overall examination, and clarify the points that need to be managed. The treatment/management plan should spell out the steps to be taken to address the chief concerns identified in the clinical findings. In healthy patients, this can be as simple as, “Normal Exam, return in 1 year for re-examination.” For a patient with refractive error, the verbiage can include the diagnosis and be stated as “Myopia, order glasses to be used for distance only, return in 1 year.” For patients with pathology, this section should be more specific and address patient education, glasses, contact lenses, low-vision aids, medications prescribed with directions for use, referrals, recommended testing, time frames and follow-up schedules. Other clinicians, reviewers, and any party evaluating this clinical encounter will look to this section to determine the important clinical points of the case and identify the plan of action and recommended follow-up. Element 17: Legible Records What is expected: Records that are easily deciphered, following a consistent examination sequence, that are complete and document all findings, clinical decisions and any continuity of care recommendations. If using electronic medical records, it is important to review any “pre-populated” and/or “cloned” default data for accuracy, attest to the doctor personally reviewing history and medications and review all recorded data to ensure it reflects the examination findings and recommendations. A signature is required on all charts, if electronic it needs to be time and date stamped.
Care Standards: Diabetes Dilation of the pupil for fundus examination is required for members with diabetes. All providers must be licensed and capable to dilate the pupil and perform the physical retina examination.
• New Patients
o All new patients require a detailed examination of the fundus. This can be accomplished with the pharmacological dilation of the pupil and examination with a binocular indirect ophthalmoscope and a slit lamp fundus lens or the professional review of a wide-angle fundus image (Optos or equivalent).
• Established Patients o Patients who have been diagnosed with diabetes require dilation every year at a minimum, more
often if they have retinopathy. o Although the retinal imaging method is acceptable in some cases, it is not a substitute for a
physical binocular retina examination.
Care for patients with diabetes • The following actions will assure the care required for patients with diabetes:
Network Administration Manual | Section 9: Standards of Care
36
o The history should include the name and, if available, contact information of the Primary Care Physician (PCP), or the provider managing the diabetes.
o The history should include a list of all diabetes medications. o The HA1c should be documented in the chart. This may come from the patient, a lab report, or the
PCP. o Dilation is required every year. o All common eye changes that result from diabetes should be documented in the medical record.
These include, but are not limited to, retinopathy, dry eye, blepharitis, cataract, and low-tension glaucoma.
o The retina examination must be detailed, and subtle background changes should be noted. o Education and counseling about blood sugar control and the required numbers to prevent vision
loss should be emphasized. • Communication and coordination with the PCP is required.
o Send a full report of the dilated eye examination results to the PCP and/or diabetes provider. You may contact the Health Plan or PCP to coordinate additional medical needs as identified while providing vision services.
• Correct Coding and Billing is required o Include the correct codes for retinopathy on your claim: the appropriate ICD-10 code related to the
diagnosis of diabetes and CPTII (2022F, 2023F, 2024F, 2025F, 2026F, 2033F or 3072F).
Contact Lens Evaluation/Fitting will include, but is not limited to: • A detailed evaluation of the cornea • Precise measurement of the curvature of the cornea • Determination of the health of the eye tissue via microscopic examination • Placement of diagnostic lenses on the eye to check fit and refraction • Check for tearing: Adequacy of tearing, tear flow under contact lenses, etc.
Eyeglass Dispensing should include: • Fitting measurements • Ordering of glasses from laboratory • Adjustments when indicated • Discussion of proper lens use, as indicated
Contact lens patients should receive the following: • Examination & fitting • Dispensing • Patient training
o Proper instruction on solutions, wearing schedule and risk factors o Contact lens “starter kit” with proper solutions o Instructions to member on how to properly insert and remove contact lenses o Instructions to member on how to properly care for and handle contact lenses
• Up to two follow-up visits when indicated
9.2 Access Standards We require that our members receive timely access to care; therefore, members should be scheduled for appointments within 15 business days of their requests.

Network Administration Manual | Section 9: Standards of Care
37
When it is necessary for you or a member to reschedule an appointment, the appointment must be promptly rescheduled in a manner that is appropriate for the member’s vision care needs and ensures continuity of care consistent with good professional practice.
The applicable waiting time for a particular appointment may be extended if the referring or treating licensed vision care professional providing triage or screening services, as applicable, acting within the scope of his or her practice and consistent with professionally recognized standards of practice, has determined and noted in the relevant record that a longer waiting time will not have a detrimental impact on the health of the member.
9.3 Telemedicine If telemedicine is acceptable in your state, you must be approved in advance in order to submit claims for telemedicine exams. Please contact your Provider Relations Advocate for instructions. Additional credentialing may be required, including verification of licensure in states where members are located. Once approved to submit claims, you may use Place of Service Code 02 with exam codes 92002, 92004, 92012, or 92014 on your electronic (EDI) or paper claim or via the portal. Claims for materials must be filed separately with the appropriate Place of Service Code. Members must be informed in advance when exams are performed via telemedicine technology.
FOR CALIFORNIA PROVIDERS:
For patients who are unable to obtain a timely appointment, please contact Customer Service. Your patient may also call Customer Service directly. If you would like to file a complaint because a patient is unable to obtain a timely appointment, please contact the DMHC Help Center at 888-466-2219.

Network Administration Manual | Section 10: Quality
38
Section 10: Quality
10.1 Quality Management Program Our Quality Management Program provides a planned, systematic and comprehensive approach to measure access and improve delivery of eye care services. The scope of the program applies to the member experience with participating network providers including:
• Clinical services • Plan Administrative services • Access to care
The Quality Management Program monitors trends in grievances and appeals related to materials and clinical service quality. The goals and objectives of the Quality Management Program are to:
• Ensure the review of quality of care and quality of service • Identify opportunities for improvement and monitor successful and complete execution of action
plans • Address quality of service elements, including accessibility, availability, member and provider
satisfaction
10.2 Credentialing & Re-credentialing We are proud of our provider community and we support your efforts in maintaining the high-quality service our members have come to expect. We follow NCQA guidelines for initial credentialing, as well as re-credentialing which typically occurs every 3 years. We will support you through the process. Credentialing is typically completed within 30 days once it's been routed to our Credentialing Verification Office (CVO) Unless use of another credentialing application source is required by your state regulations, CAQH Proview™ will be used to obtain the necessary information to complete your credentialing, as well as checking various state systems. You will be notified when the review has been completed.
Up-to-date versions of the following items are needed on CAQH Proview™:
• CAQH Application Release to Spectera Eyecare Networks • CAQH Attestation within the last 3 months • Certificate of Insurance showing Professional Liability Coverage (Malpractice Insurance) • State License including Diagnostic Pharmaceutical Agent (DPA) License or Therapeutic Pharmaceutical
Agent (TPA) License • Copy of DEA and CDS* • Board Certification* • State Medicaid ID* • Vitae/Resume, including work history (only needed for your initial credentialing) • Copy of W9
*If applicable

Network Administration Manual | Section 10: Quality
39
*In order to be credentialed, our credentialing plan requires that you:
• Aren’t ineligible, excluded or debarred from participation in the Medicare and /or Medicaid and related state and federal programs
• Are without any sanctions levied by the office of Inspector (OIG), the CMS Preclusion* List or other disciplinary action by any federal state entities identified by CMS
*Precluded provider claims will no longer be paid. A precluded provider must hold Medicare beneficiaries harmless from financial liability for services or items provided on or after the claim-rejection date.
10.3 Cultural Competency Our vision network expects all members to receive services and treatment in an equitable and effective manner. As a health care provider, you are expected to be sensitive to the diverse populations and to effectively provide covered services in a manner that recognizes the cultural diversity of all our members.
Cultural Competency Online Resource(s):
U. S. Department of Health & Human Services: Information related to key considerations, basic principles and other resources related to identifying & understanding how to effectively serve in a culturally competent manner
(://thinkculturalhealth.hhs.gov/about)
Network Administration Manual | Section 11: Policies
40
Section 11: Policies
11.1 Provider Disputes Our dispute resolution mechanism only accepts provider disputes submitted in writing. Letters of appeal must include:
• Member name • Claim ID • Nature of the appeal including identification of the service
Unless otherwise prescribed by state regulation, we accept provider disputes regarding claims or unfavorable resolutions to quality of care issues within 90 days following the date of a (n):
• Claim denial • Unsatisfactory resolution of member benefit issue or appeal • Notification of unfavorable resolution to quality of care issue
We accept provider disputes regarding plan policies and procedures or quality of care guidelines at any time unless the provider disputes impacts a particular claim.
The Appeals and Grievance Department responds and resolves all provider disputes within state mandated timeframes upon completion of all necessary information. PR actioners will then be notified of the final determination within two (2) business days unless otherwise prescribed by state law, statute, or act.
Send all disputes, including all accompanying documentation, to:
Spectera Vision Network Appeals and Grievance Department PO Box 30978 Salt Lake City, UT 84130
11.2 Provider Fair Hearing Policy In addition to those rights set forth in your provider contract and those provisions under applicable state and federal law governing termination, in the event that we are presented with cause, we reserve the right to investigate a provider’s behavior, which may lead to corrective action, monitoring, full or partial suspension of network privileges, request for voluntary resignation and termination from the provider network. Suspensions may be automatic or probationary in nature.
Automatic Suspension Circumstances • Threat of imminent harm to the general public • Sanctions by Medicare or Medicaid • Revocation, suspension, restriction, lapse or probationary status of state license or hospital
privileges • Failure to maintain malpractice insurance

Network Administration Manual | Section 11: Policies
41
• Failure to complete credentialing/re-credentialing application • Failure to appear for an interview (if requested by the Peer Review Committee or directors) • Revocation, suspension, restriction or probationary status of DEA certificate
Notification of Automatic Suspension You will be notified in writing, by certified mail, of an automatic suspension from the network by us within 10 days of suspension. A review of your status will be made by the Peer Review Committee within 45 days of suspension. Notification of the Committee’s interim decision will also be sent to you in writing, by certified mail, within 10 days of the decision. The interim decision will set forth conditions and timeframes, if any, that must be met in order for us or the Committee to consider a reversal or modification of the suspension.
Appeal of Automatic Suspension Independent of any conciliations and/or timeframes set forth in the interim decision, you have the right to appeal the Peer Review Committee’s interim decision in writing within 45 days of the date of the decision and request a hearing by the Committee within 45 days of the date of the written appeal. The interim decision will become final if the committee does not receive a written appeal within 45 days of the date of the interim decision.
Notification of Final Decision You will be notified in writing, by certified mail, of the final decision of the Peer Review Committee within 10 days of the decision. You may reapply for participation in our network in writing after a 12-month period. The request must be substantiated with documentation that the appropriate behavior has been corrected.
• Probationary Suspension Circumstances • Notification of pending malpractice litigation or adverse judgment against a provider, or
settlement offers by provider pertaining to same • Notification by the general public or other network providers that the provider is participating in an
activity which may harm the general public or is against a Spectera, Inc. or the applicable state’s licensing board’s standards of care
• Repeated or egregious failure of the provider to comply with this Administration Manual • Repeated negligence by the provider in submitting claims for services and /or materials • Repeated egregious failure of the provider to submit records requested by Spectera, Inc. • Failure of the provider to comply with provider’s contract with Spectera, Inc., including, but not
limited to, balance billing enrolled members for covered services • Notification from another insurance group that the provider has been placed on corrective action
or received an administrative revocation of privileges • Repeated complaints against the provider from either members, groups or other network providers • Misappropriation of Spectera, Inc. property or submission of intentionally inaccurate records by
the provider • Any violation by the provider of the HIPAA or applicable state privacy and security rules in effect • Refusal of the provider to use the required laboratory or use by the provider of a facility other than
that required laboratory(if applicable) • Action or omission by the provider that subjects us to a lawsuit or otherwise subjects Spectera,
Inc. to liability
Notification of Probationary Status You will be notified in writing, by certified mail, of our intent to impose a probationary suspension upon you. You are required to respond to us within 15 days from the date of the notification letter. If we have not received a satisfactory response within this 15-day period, you will be placed on probationary suspension. You will be notified in writing, by certified mail, of the probationary suspension within 10 days

Network Administration Manual | Section 11: Policies
42
of the decision. This interim decision will set forth conditions and timeframes, if any, that must be met in order for us to consider a reversal or modification of the suspension.
Appeal of Probationary Suspension Independent of any conditions and/or timeframes set forth in the interim decision, you have the right to appeal the interim decision in writing within 45 days of the date of the decision and request a hearing by the committee within 45 days of the date of the written appeal. The interim decision will become final if the committee does not receive a written appeal within 45 days of the date of the interim decision.
Notification of Final Decision You will be notified in writing, by certified mail, of the final decision of the Peer Review Committee within 10 days of the decision. You may reapply for participation, in writing, after a 12-month period. The request must be substantiated with documentation that the appropriate behavior has been corrected.
Peer Review Committee Actions All Peer Review Committee actions will be based upon a majority vote
Appeal Hearing Criteria • You may provide pertinent documentation to support your case. • The committee will allow the provider to offer alternate solutions, within reason for consideration. • The committee will not require that you be present for an appeal hearing, but you may be present
at the hearing.
Adoption and Amendment Policy The fair hearing plan may be adopted, amended or replaced, in whole or in part, by the Senior Vice President, Product and Provider Solutions.
11.3 New Jersey Golden Rule THE BELOW PROCEDURES ARE SPECIFIC TO GOLDEN RULE POLICYHOLDERS
New Jersey Complaint Resolution Process for Golden Rule Members
New Jersey law requires us to provide network providers with a description of the complaint resolution process for covered persons.
Applicability: For vision rider products, complaints may be filed by covered persons and providers regarding our contracts or policies, choice and accessibility of network providers, and network adequacy. A complaint may be submitted in writing to:
Golden Rule Insurance Company 7440 Woodland Drive Indianapolis, IN 46278-1719 (800) 657-8205
A complaint submission does not require a special form. Upon request, we will make a representative available to assist you with complaint procedures.
Complaint Resolution: We will notify you in writing of the decision as soon as possible but in no case later than 30 days after receipt of the written complaint.

Network Administration Manual | Section 11: Policies
43
If you are dissatisfied with the results of the resolution reached through our complaint system, you may contact the Department at the following address and phone number:
Office of Managed Care Consumer Protection Services Department of Banking and Insurance P.O Box 329 Trenton, NJ 08625-0329 Fax: (609) 633-0807 Phone: (888) 393-1062
We will not discontinue coverage for or otherwise penalize any covered person or provider for exercising his or her right to file a complaint.
11.4 Rhode Island Providers: Notice of Member Vision Complaint and Appeal Rights
What if You Have a Complaint? Contact Customer Service at 1-800-638-3120. Representatives are available to take your call during regular business hours, Monday through Friday. If you would rather send your complaint to us in writing, the representative can provide you with the address. If the representative cannot resolve the issue over the phone, he/she can help you prepare and submit a written complaint. We will notify you of our decision regarding your complaint within 30 calendar days of receiving it.
How to Request an Appeal If you disagree with either claim determination or a rescission of coverage determination, you can contact us in writing to request an appeal. Your request for an appeal should include:
• The patient's name and Policy number. • The date(s) of vision service(s). • The provider's name. • The reason you believe the claim should be paid. • Any documentation or other written information to support your request for claim payment. Your
appeal request must be submitted to us within 180 days after you receive claim denial.
Appeal Process A qualified individual who was not involved in the decision being appealed will be chosen to decide the appeal. You consent to this referral and the sharing of needed vision claim information. Upon request and free of charge, you have the right to reasonable access to and copies of all documents, records and other information related to your claim for benefits. If any new or additional evidence is relied upon or generated by us during the determination of the appeal, we will provide it to you free of charge and in advance of the due date of the response to the adverse benefit determination.
Appeals Determinations You will be provided written or electronic notification of the decision on your appeal as follows:

Network Administration Manual | Section 11: Policies
44
• For appeals of pre-service request for Benefits, the appeal will take place and you will be notified of the decision within 30 days from receipt of a request for appeal of a denied request for Benefits.
• For appeals of post-service request for Benefits, the appeal will take place and you will be notified of the decision within 60 days from receipt of a request for appeal of a denied request for Benefits.
11.5 Non-Covered Services In accordance with current applicable state laws and regulations, which may be subject to change, you are not required to provide services to a Member at a fee set by or subject to our approval unless the services are Covered Services under the Agreement. If you provide services that are Non-Covered Services to members, you must first obtain the member’s written consent. The consent must be signed and dated by the member prior to rendering the specific service(s) and a copy must be retained in the member’s record. The consent must (a) disclose to the Member that such services are Non-Covered Services, (b) inform the member of the fees or additional amounts Member will be required to pay for that service, and (c) state that the member agrees to be solely responsible for the non-covered charges.
When allowed and appropriate for your practice, we ask that you extend a 20% discount on materials purchased after plan benefits have been exhausted. Examples of these materials would include non-covered replacement or second pairs of eyeglasses and additional boxes of contact lenses.
11.6 Additional Medicare Advantage Requirements If you participate in the network for our Medicare Advantage products, you must comply with the following additional requirements (as applicable) for services you provide to our Medicare Advantage members.
• You may not discriminate against members in any way based on health status. • You must make sure that members have adequate access to Covered Services. • You must make sure that your hours of operation are convenient to members and do not
discriminate against members and that medically necessary services are available to members 24 hours a day, 7 days a week.
• You may only make available or distribute plan marketing materials to members in accordance with CMS requirements.
• You must provide services to members in a culturally competent manner, taking into account limited English proficiency or reading skills, hearing or vision impairment and diverse cultural and ethnic backgrounds.
• You must cooperate with our procedures to inform members of health care needs that require follow-up and provide necessary training to members in self-care.
• You must provide Covered Services in a manner consistent with professionally recognized standards of health care.
• You must make sure that any payment and incentive arrangements with subcontractors are specified in a written agreement, that such arrangements do not encourage reductions in medically necessary services, and that any physician incentive plans comply with applicable CMS standards.
• You must cooperate with our processes to disclose to CMS all information necessary for CMS to administer and evaluate the Medicare Advantage Program, and all information

Network Administration Manual | Section 11: Policies
45
determined by CMS to be necessary to assist members in making an informed choice about Medicare coverage.
• You must cooperate with our processes for notifying members of network participation agreement terminations.
• You must comply with our Medicare Advantage medical policies, quality improvement programs and medical management procedures.
• You must cooperate with us in fulfilling our responsibility to disclose to CMS quality, performance and other indicators as specified by CMS.
• You must cooperate with our procedures for handling grievances, appeals and expedited appeals.
11.7 General Compliance and Fraud, Waste and Abuse
Our organization uses the terms: delegates; delegated entities; vendor; first-tier, downstream entity and related entity (FDR); subcontractor; and, occasionally, others interchangeably to name the parties with whom we contract with to support administration of benefits, access to care and other services performed on our behalf.
As a delegated entity of our organization, we expect you to comply with all state and federal laws as described in your contract, including those that are designed to prevent and eliminate fraud, waste and abuse. Therefore, at minimum, you need to have implemented the following compliance program requirements.
Standards of Conduct Awareness and Distribution
You are required to provide a copy of your own or UnitedHealth Group’s Code of Conduct to all employees (including temporary or contract workers, sub-delegates, volunteers, etc.), within 90 days of hire and annually thereafter (by the end of each year), or when the Code of Conduct is updated. You must maintain distribution standards (i.e. in an email, website portal or contract, etc.) for 10 years. Documentation may be requested by us or a regulatory agency to verify compliance with this requirement.
Education and Training The Centers for Medicare and Medicaid Services (CMS) requires that all organizations and their delegates working with our Medicare Advantage Parts C and D or Medicaid programs to provide FWA and general compliance training.
You must provide FWA and general compliance training to your employees (includes temporary or volunteers) and contractors that support the delivery and administration of program benefits or services. The FWA and general compliance training must be completed within 90 days of hire and annually thereafter (by end of each year).
To ensure that you and/or your organization has assess to training, CMS provides resources related to compliance and fraud and abuse at:
https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/ProviderCompliance
It is your responsibility to administer and track the completion of this training for all employees and contractors within your organization that support the delivery and administration of program benefit or services. You must maintain a record of completion (i.e. method, training materials, employee sign-in

Network Administration Manual | Section 11: Policies
46
sheets, attestations or electronic certifications that include the date of the training) for 10 years. Documentation may be requested by us, CMS or a regulatory agency to verify compliance with this requirement.
Exclusion Checks All delegates working with our Medicare Advantage Parts C and D or Medicaid programs must review the federal exclusion lists maintained by the U.S. Department of Health and Human Services – Office of the Inspector General (HHS-OIG) and the General Services Administration (GSA). These exclusion lists name individuals or organizations that are suspended or otherwise excluded from participation in Medicare and Medicaid programs.
Delegates must review all employees and/or subcontractors (including if temporary and volunteers) that support Medicare Advantage Parts C and D and/or Medicaid plans and membership against OIG and GSA federal exclusion lists prior to hiring or contracting with them, and on a monthly basis thereafter.
For more information or access to publicly accessible excluded party online databases, refer to: • Health and Human Services-Office of the Inspector General (https://oig.hhs.gov/exclusions/index.asp) • General Services Administration (GSA) System for Award Management (https://www.sam.gov)
Many states maintain state-based sanction/exclusion databases that are in addition to, but do not replace, the OIG and GSA federal exclusion databases. A provider may not participate in the network of a state if the specific state is listed on that state’s exclusion list, even if the provider is not listed on a federal exclusion list. State Exclusion List Resource:
• Verify Comply® (https://www.verifycomply.com)
What you need to do for Exclusion Checks You must review the applicable exclusion lists as outlined, document and retain proof of the method used, date performed, employee list and results found for 10 years. Documentation of the exclusion checks may be requested by us or regulatory agency to provide documentation upon request. Failure to comply may result in any of a series of regulatory enforcement actions and our remediation activities.
Offshoring Reporting & Downstream Delegates Delegates must report to us prior to moving services offshore that involve sharing of protected health information (PHI) or personal identifiable information (PII) and must hold their downstream entities or subcontractors that support the delivery or administration of program benefits or services accountable for the same compliance program requirements.
Reporting suspected FWA If you identify suspected fraud, waste, or abuse, it is your right and responsibility to report it to us immediately so that we can detect, correct and prevent FWA in the health care system. We expressly prohibit retaliation if a suspected issue is reported in good faith.
You can report suspected fraud, waste, or abuse to UnitedHealthcare online at uhc.com/fraud or by calling (844) 359-7736.

Network Administration Manual | Section 11: Policies
47
For questions or to reference more about the UnitedHealth Group Compliance Program, refer to: http://www.unitedhealthgroup.com/Suppliers/ComplianceProgram.aspx
*Our vision networks are not affiliated with any independent websites mentioned in the section above.
11.8 Terminations for Inactivity
It is imperative that our Provider Directory is kept up to date so our members have the information they need to manage their eye health. In order to accurately reflect providers in our Provider Directory who are actively seeing our members, we will take the following actions:
1. Terminate contracts with providers who have not submitted claims for a period of one year on the basis that they are not actively rendering services to members and have voluntarily ended participation in our network.
2. Inactivate any TINs under which there have been no claims submitted for a period of one year on the basis that they are not in active use. Because other TINs associated with a particular agreement have been active, this is not a termination of your contract. You may contact us to reactive an inactivated TIN.
11.9 Provider Directory Requirements We require our provider network to review and verify the accuracy of their provider directory information on a regular basis, or every 90 days, to ensure our provider directory is current and meets regulatory requirements to best serve our members.
You have 24/7 access to log on to spectera.com and verify your location and provider demographic information is current and accurate. To do so, go to spectera.com, log-on using your payee or location level credentials, go to entity management to review and if alerted, verify accuracy, or if applicable, use the entity management function to submit updates to the location’s demographic information or active provider(s). Failure to verify or update a locations demographic and provider information may result in removal from the directory.
California :
In accordance with California Senate Bill 137, we are required to perform ongoing updates to our provider directories, both online and hardcopy. We are required to contact all contracted providers every six months. The provider outreach will include a summary of the information that we have on record and require you to respond confirming information is accurate, or with applicable changes. The notice will inform you that failure to respond to our request and provide accurate information may result in your removal from the provider directory. If we do not receive a response within 30 business days from you either confirming that the information on file is correct, or by providing the necessary updates, we have 15 business days to make attempts to verify the information. If subsequent attempts are unsuccessful, we will notify you that, after 10 business days you will be removed from the directory if you continue to be non-responsive"
If the final 10-business day period lapses with no response from you, we will remove you from the directory. We retain the right to terminate provider contracts if there is a pattern or repeated failure to provide the information required for us to comply with this regulatory requirement.

Network Administration Manual | Section 12: Forms
48
Section 12: Forms
12.1 Patient Care Forms We can now accept your post-cataract claims via EDI, HCFA, or through spectera.com without the Confirmation of Cataract Surgery Form. When submitting claims via this new process, please refer to the Billing Guide, specifically the “Additional Billing Instructions”, to ensure proper processing of the claim. Please continue to use the form if you are submitting your claim via paper.
You can verify eligibility of the member’s post-cataract benefits at spectera.com or by calling Customer Service.
Note: The member’s benefit is a lifetime benefit based on surgery performed once per eye. Members can obtain one material benefit after each post-cataract surgery. For post-cataract claims submitted via paper:
The completed Confirmation of Cataract Surgery form can be faxed or mailed as follows:
Attention: Vision Advocates 6200 Northwest Parkway San Antonio, TX 78249 Fax : (877) 410-2519
The forms described below can be found below or at spectera.com.
Confirmation of Cataract Surgery Form: This form is for Medicare members who require new eyeglasses or contact lenses after cataract surgery.
Upon receipt, Customer Service will call you to confirm benefits and you can submit your claim via your normal process.
12.2 Patient Frames - Waiver Form for Patients Who Use the Lab Network
If a member chooses to keep their current frame and have it sent to the network laboratory for new lenses, they must complete a Patient Waiver Form. Include the completed form (including the member’s name, order tracking number, and your provider account number) when you ship the frames to the network laboratory. We recommend that you contact the lab network to obtain a pre-paid shipping label. You can find the waiver form on spectera.com or in this manual.

Network Administration Manual | Section 12: Forms
49
12.3 Referral Forms Communicating relevant information helps to integrate eye care into your patient's overall health and wellness.
We encourage you to use the referral forms located at spectera.com when you refer members for recommended treatment and follow-up care. You may give the form to the member to take to their Primary Care Physician or you can fax or mail it directly. Keep a copy of the referral in the member's chart for future reference.
• The Eye Examination Report is designed to help communicate the identification of chronic disease or eye disease, or for monitoring previously identified conditions between eye care providers, the patients, and other care providers.
• The Diabetic Eye Exam Report is used to share information between health care providers regarding a member’s condition, exam findings, treatment plans, and any additional referral/support required.

Network Administration Manual | Section 12: Forms
50

Network Administration Manual | Section 12: Forms
51
REFERRAL/REPORT FORM

Network Administration Manual | Section 12: Forms
52
REFERRAL/REPORT FORM

Network Administration Manual | Section 12: Forms
53
Confirmation of Cataract Surgery Form
Patient Name:
/ /
Date of Service
/ /
Member ID # D.O.B.
I, _____________________________________________________hereby certify the above patient had (Print Dispensing Provider Name)
Cataract surgery performed.
/ /
Dispensing Provider Signature Date:
Please submit completed form to:
• Vision Advocates FAX: (877)410-2519 • Or mail to the address below: Spectera
Attention: Vision Advocates 6200 Northwest Parkway San Antonio, TX 78249
Spectera, Inc. is the contracting entity for Spectera Eyecare Networks providers.
M54978 2/15 © 2015Spectera, Inc. M12345
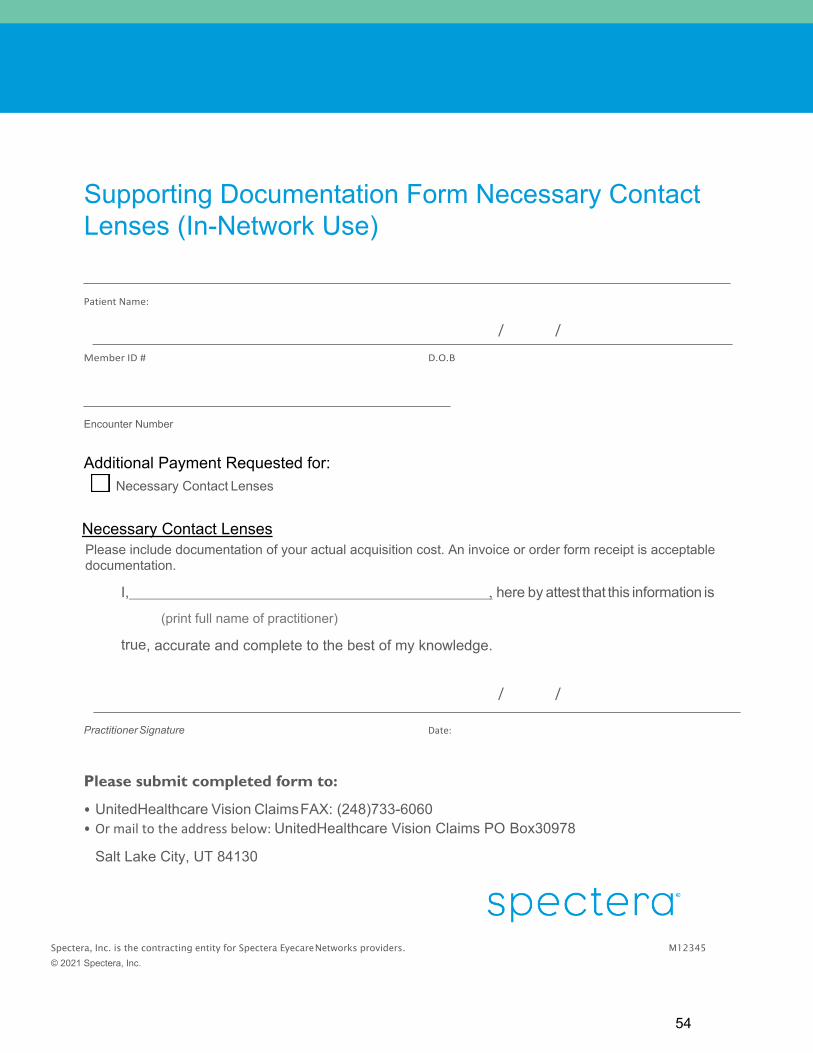
Network Administration Manual | Section 12: Forms
54
Supporting Documentation Form Necessary Contact Lenses (In-Network Use)
Patient Name:
/ /
Member ID # D.O.B
Encounter Number
Additional Payment Requested for: Necessary Contact Lenses
Necessary Contact Lenses Please include documentation of your actual acquisition cost. An invoice or order form receipt is acceptable documentation.
I, , here by attest that this information is
(print full name of practitioner)
true, accurate and complete to the best of my knowledge.
/ /
Practitioner Signature Date:
Please submit completed form to:
• UnitedHealthcare Vision Claims FAX: (248)733-6060 • Or mail to the address below: UnitedHealthcare Vision Claims PO Box30978
Salt Lake City, UT 84130
Spectera, Inc. is the contracting entity for Spectera Eyecare Networks providers. M12345
© 2021 Spectera, Inc.

Network Administration Manual | Section 12: Forms
55
Spectera Claim ID Number: _________________________________________________
Please supply a brief explanation of the corrected claim changes:
Provider Office Contact Information:
Name: _______________________________________________________
Phone Number: ________________________________________________
Email: _______________________________________________________
© 2021 Spectera Eyecare Networks
OPTIONAL CORRECTED CLAIM – STANDARD COVER SHEET
Instructions:
1.) You can fill out this form in its entirety and use it as your cover sheet or just submit your corrected claim with “corrected claim” written at the top.
2.) You MUST include the corrected claim. 3.) Fax or email your corrected claim and form, if applicable to:
Fax: (888) 751-0933
Email: [email protected]
This form should NOT be used for benefit questions, eligibility issues, or payment discrepancy issues – please contact Customer Service if you have questions
related to benefits, eligibility or payment discrepancies.

Network Administration Manual | Section 12: Forms
56
FOR MA PROVIDERS ONLY
Two Pairs of Glasses in Lieu of Bifocals Form
Member Name:
Member ID #: DOB:
Doctor Name: Provider #:
Doctor Phone#: Doctor Fax#:
Doctor NPI#: Date of Service:
The prescribing doctor determines if two pairs of glasses in lieu of bifocals is necessary based on Spectera Vision guidelines. The conditions that allow a member to get two pairs of glasses in lieu of bifocals are below. Check all that apply:
The member's prescription cannot satisfactorily be made into bifocal lenses. The member has shown an inability to adjust to bifocals. The member's advanced age would make adjustment to bifocals unduly difficult. The member’s occupation would make bifocals hazardous.
The member has a marked facial asymmetry. The member has a physical disability (for example, severe arthritis) that would preclude or impede adjustment
to bifocals.
Additional information:
Please submit this form together with your claim paperwork via the adjustments email: Email: [email protected] Subject: MA Two Pairs in Lieu of Bifocals
11292016_HL

Network Administration Manual | Section 13: Codes
57
Section 13: Codes 13.1 Spectera Vision Network Billing Guide Revised 7/1/21
Examination and Ophthalmic Lenses
Accepted CPT / HCPC Codes
Required Modifier
(if blank, no modifier required)
Description
Eye Examination 92002 92004 92012 92014
Refraction 92015 Diabetic Care Reporting 2022F
2024F 2026F 3072F
Dilated retinal eye exam in Diabetic patient 7 standard field stereoscopic photos for Diabetic patient eye exam Eye imaging validated to 7 standard field stereoscopic phots-Diabetic eye exam Low risk for retinopathy (no evidence of retinopathy in prior year)
Frames S0516 Safety Frame S0518 Sunglass Frame V2020 V2025 Frame
Single Vision Lenses V2100 to V2115 V2121 V2199
Standard
V2100 to V2115 V2121 V2199
FF Free Form
V2410 Aspheric (See Additional Billing Instructions below) Bifocal Lenses V2200 to V2215
V2218 to V2221 V2299
Standard (Lined)
V2200 to V2215 V2218 to V2221 V2299
BB Blended
V2430 Aspheric (See Additional Billing Instructions below) V2786 Occupational Double Segmented
Trifocal Lenses V2300 to V2315 V2318 to V2320 V2399
Standard (Lined)
Progressive Lenses V2781 P1 Progressive Lenses: Tier I
V2781 P2 Progressive Lenses: Tier II
V2781 P3 Progressive Lenses: Tier III
V2781 P4 Progressive Lenses: Tier IV
V2781 P5 Progressive Lenses: Tier V
V2781 P6 Progressive Lenses: Non-Formulary
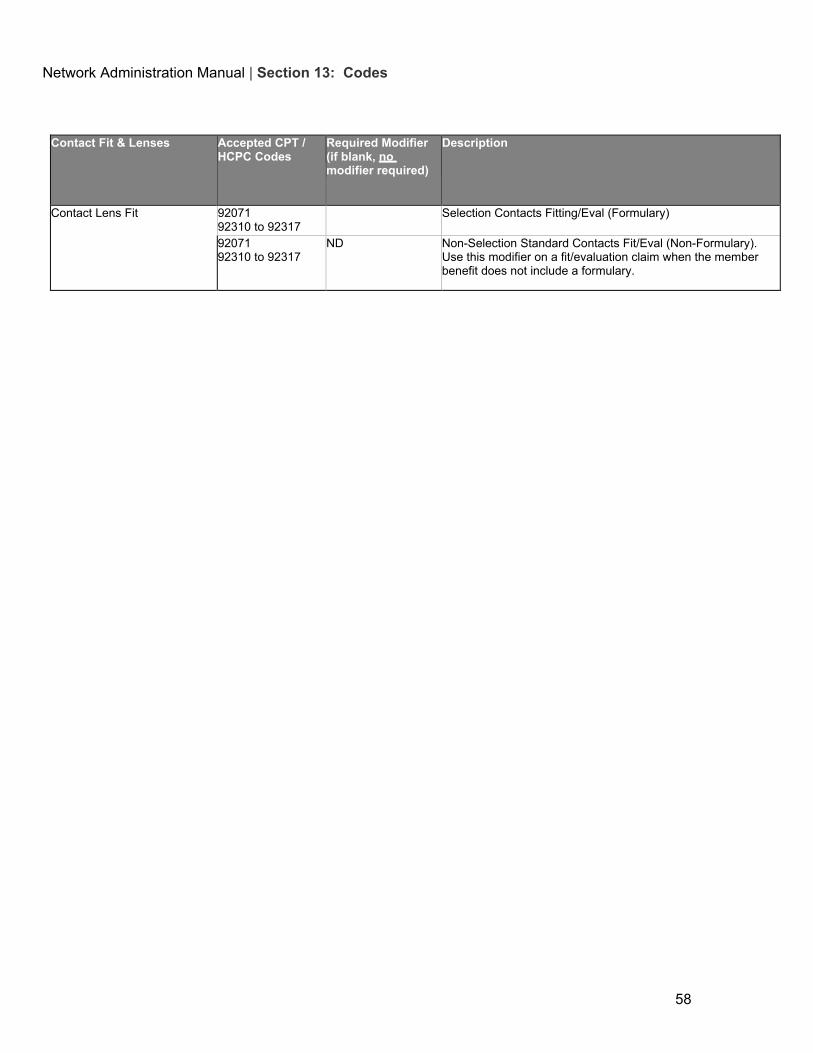
Network Administration Manual | Section 13: Codes
58
Contact Fit & Lenses Accepted CPT / HCPC Codes
Required Modifier (if blank, no modifier required)
Description
Contact Lens Fit 92071 92310 to 92317
Selection Contacts Fitting/Eval (Formulary)
92071 92310 to 92317
ND Non-Selection Standard Contacts Fit/Eval (Non-Formulary). Use this modifier on a fit/evaluation claim when the member benefit does not include a formulary.

Network Administration Manual | Section 13: Codes
59
92071 92310 to 92317
XC Necessary Contact Lenses Fit/Eval In order to process a Necessary Contact Lens Fit, you must bill with the XC modifier and the member must have one or more of the conditions noted below. Always code to the highest degree of specificity when indicating diagnosis. A list of acceptable diagnosis codes can be found below. Keratoconus: H18.601 thru H18.629 Irregular Corneal Astigmatism: H52.211 thru H52.219 Aphakia: H27.00 thru H27.03, Q12.3 Anisometropia or Aniseikonia: H52.31, H52.32 Corneal Deformity: Q13.3, Q13.4, H18.70, H18.721 thru H18.799 Corneal Opacity: H17.00 thru H17.13, H17.811 thru H17.829, H17.89, H17.9 Corneal Degeneration: H18.40, H18.421 thru H18.469, H18.49 Corneal Ectasia: H18.711 thru H18.719 Corneal Transplant: Z94.7, T86.8401 thru T86.8499 Disorder of Refraction: H52.7 (This covers cases where vision is less than 20/70 with glasses but can be improved to better than 20/70 with contact lenses ) Facial deformity: M95.0, M95.2, Q67.0, Q67.1, Q18.0 thru Q18.9, Q75.0 thru Q75.9 Hereditary Corneal Degenerations: H18.501 thru H18.599 Order Specified Corneal Disorders: H18.811 thru H18.829 Other Corneal Disorders: H18.011 thru H18.019

Network Administration Manual | Section 13: Codes
60
Contact Lenses V2500 to V2503 V2510 to V2513 V2520 to V2523 V2530 to V2531 V2599
CD Selection Bi-Weekly and Daily Wear Disposable Contact Lenses (Formulary)
V2500 to V2503 V2510 to V2513 V2520 to V2523 V2530 to V2531 V2599
CM Selection Planned Replacement Monthly Wear Contact Lenses (Formulary)
V2500 to V2503 V2510 to V2513 V2520 to V2523 V2530 to V2531 V2599
ND Non-Selection Disposable Contact Lenses (Non- formulary). Use this modifier on the elective contact lenses claim when the benefit plan does not include a formulary.

Network Administration Manual | Section 13: Codes
61
V2500 to V2503 V2510 to V2513 V2520 to V2523 V2530 to V2531 V2599
XC Necessary Contact Lenses In order to process Necessary Contact Lenses, you must bill with the XC modifier and the member must have one or more of the conditions noted below. Always code to the highest degree of specificity when indicating diagnosis. A list of acceptable diagnosis codes can be found below. Keratoconus: H18.601 thru H18.629 Irregular Corneal Astigmatism: H52.211 thru H52.219 Aphakia: H27.00 thru H27.03, Q12.3 Anisometropia or Aniseikonia: H52.31, H52.32 Corneal Deformity: Q13.3, Q13.4, H18.70, H18.721 thru H18.799 Corneal Opacity: H17.00 thru H17.13, H17.811 thru H17.829, H17.89, H17.9 Corneal Degeneration: H18.40, H18.421 thru H18.469, H18.49 Corneal Ectasia: H18.711 thru H18.719 Corneal Transplant: Z94.7, T86.8401 thru T86.8499 Disorder of Refraction: H52.7 (This covers cases where vision is less than 20/70 with glasses but can be improved to better than 20/70 with contact lenses ) Facial deformity: M95.0, M95.2, Q67.0, Q67.1, Q18.0 thru Q18.9, Q75.0 thru Q75.9 Hereditary Corneal Degenerations: H18.501 thru H18.599 Order Specified Corneal Disorders: H18.811 thru H18.829 Other Corneal Disorders: H18.011 thru H18.019

Network Administration Manual | Section 13: Codes
62
Lens Options CPT / HCPC
Codes Required Modifier (if blank, no modifier required)
Description
Anti-Reflective V2750 R1 Anti-Reflective Coating: Tier I V2750 R2 Anti-Reflective Coating: Tier II V2750 R3 Anti-Reflective Coating: Tier III V2750 R4 Anti-Reflective Coating: Tier IV V2750 R5 Anti-Reflective Coating: Non-Formulary
Edge Coating V2799 ED Edge Coating
High Index (Single Vision or Multifocal, Plastic or Glass)
V2782 Index lens, < (less than) 1.66 V2783 High Index, 1.66 to 1.73 V2783 HI High Index >= 1.74 V2782 Index lens, < (less than) 1.66
Photochromic (Including Transitions)
V2744 PS Glass Photochromic V2744 Non-Glass Photochromic
Polarized V2762 Polarized Lens
Polished Edges V2799 PP Polished Edges / Roll & Polish Polycarbonate V2784 Polycarbonate Lenses
Prism V2715 Prism Lens Premium Scratch Coating V2799 PC Premium Scratch Coating Scratch Warranty V2799 SW One Year Scratch Warranty Blue Light Filter V2799 BL Embedded Blue Light Filter (non-AR) Slab Off V2710 Slab Off Lens Tint V2745 Solid Tint
V2745 GL Gradient Tint - Glass Lens
V2745 GT Gradient Tint - Plastic Lens
V2745 RS Rose Tint I & II
UV Coating V2755 UV 400 - Plastic Lens
V2755 GL UV 400 - Glass Lens
Lens Options CPT / HCPC Codes
Required Modifier (if blank, no modifier required)
Description
Miscellaneous / Other V2797 Miscellaneous Lens Accessories -- For any lens or option(s) not listed above, bill one line with V2797, charges bundled.
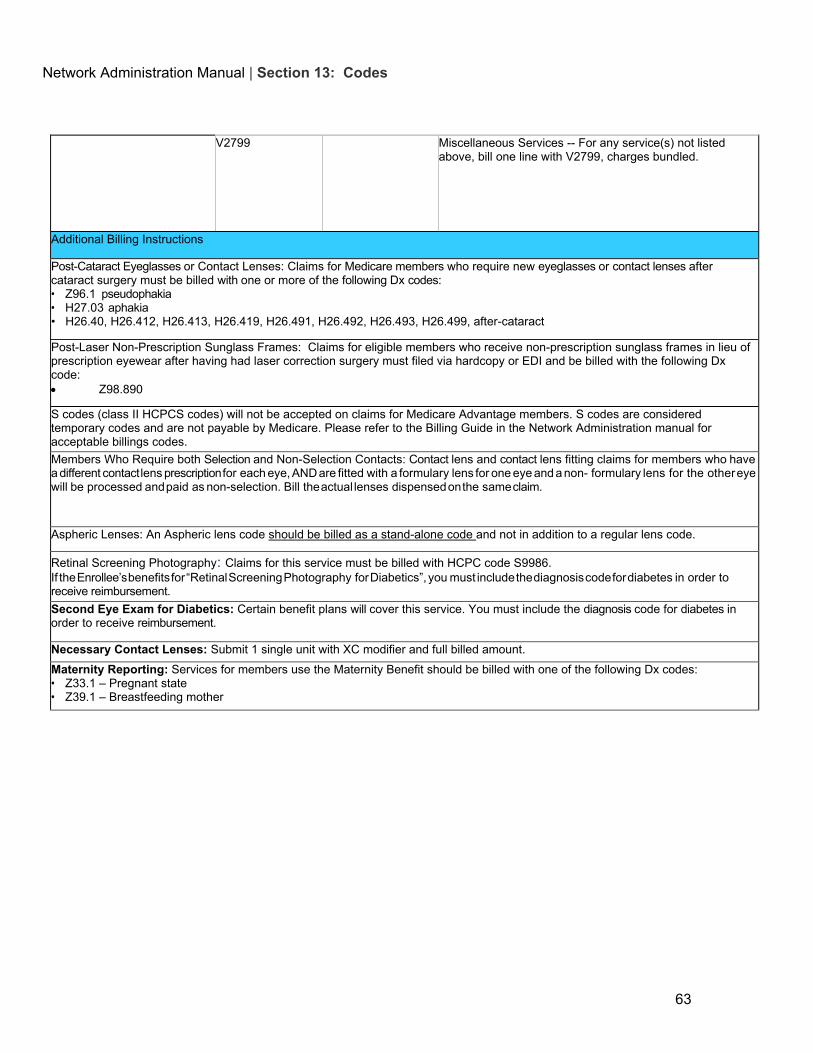
Network Administration Manual | Section 13: Codes
63
V2799 Miscellaneous Services -- For any service(s) not listed above, bill one line with V2799, charges bundled.
Additional Billing Instructions
Post-Cataract Eyeglasses or Contact Lenses: Claims for Medicare members who require new eyeglasses or contact lenses after cataract surgery must be billed with one or more of the following Dx codes: • Z96.1 pseudophakia • H27.03 aphakia • H26.40, H26.412, H26.413, H26.419, H26.491, H26.492, H26.493, H26.499, after-cataract
Post-Laser Non-Prescription Sunglass Frames: Claims for eligible members who receive non-prescription sunglass frames in lieu of prescription eyewear after having had laser correction surgery must filed via hardcopy or EDI and be billed with the following Dx code: • Z98.890
S codes (class II HCPCS codes) will not be accepted on claims for Medicare Advantage members. S codes are considered temporary codes and are not payable by Medicare. Please refer to the Billing Guide in the Network Administration manual for acceptable billings codes. Members Who Require both Selection and Non-Selection Contacts: Contact lens and contact lens fitting claims for members who have a different contact lens prescription for each eye, AND are fitted with a formulary lens for one eye and a non- formulary lens for the other eye will be processed and paid as non-selection. Bill the actual lenses dispensed on the same claim.
Aspheric Lenses: An Aspheric lens code should be billed as a stand-alone code and not in addition to a regular lens code.
Retinal Screening Photography: Claims for this service must be billed with HCPC code S9986. If the Enrollee’s benefits for “Retinal Screening Photography for Diabetics”, you must include the diagnosis code for diabetes in order to receive reimbursement. Second Eye Exam for Diabetics: Certain benefit plans will cover this service. You must include the diagnosis code for diabetes in order to receive reimbursement.
Necessary Contact Lenses: Submit 1 single unit with XC modifier and full billed amount. Maternity Reporting: Services for members use the Maternity Benefit should be billed with one of the following Dx codes: • Z33.1 – Pregnant state • Z39.1 – Breastfeeding mother

Network Administration Manual | Section 13: Codes
13.2 Spectera Vision Network Modifier Codes
Revised 5/1/2021 CONTACT LENS MODIFIER CODES CM Covered Selection Monthly Planned Replacement (Formulary)
CD Covered Selection Disposable Contacts/Bi-Weekly and Daily Wear (F l ) ND Non-Selection Disposable Contacts (Non-Formulary)
XC Necessary Contacts
LENS AND LENS OPTION MODIFIER CODES R1 Anti-Reflective Coating: Tier I R2 Anti-Reflective Coating: Tier II R3 Anti-Reflective Coating: Tier III R4 Anti-Reflective Coating: Tier IV R5 Anti-Reflective Coating: Non-Formulary BB Blended Bifocal BL Blue Light Filter ED Edge Coating FF Free Form Single Vision Lens GL UV Glass GT Gradient Tint HI High Index - greater than or equal to 1.74 (for V2783) P1 Progressive Lenses: Tier I P2 Progressive Lenses: Tier II P3 Progressive Lenses: Tier III P4 Progressive Lenses: Tier IV P5 Progressive Lenses: Tier V P6 Progressive Lenses: Non-Formulary PC Premium Scratch Coat PP Roll & Polish PS Photochromic Glass Lens RS Pink Tint I & II
SW Scratch Warranty

Network Administration Manual | Section 13: Codes
63
13.3 Vision Diagnosis Codes

Network Administration Manual | Section 13: Codes
66
13.4 Commonly Used Provider Remittance Advice Remark Codes
Code
Description 1027 Invalid service for covered benefit; patient is responsible for these charges
1039 Service Not a Covered Benefit
1036 Invalid Specialty for Procedure
1042 Duplicate Service
1043 Duplicate Service Previously Paid
1044 Untimely Filing
1045 Patient Ineligible 1051 Service exceeds frequency limit; patient is responsible for these charges 1052 Duplicate Service Being Processed 1055 Invalid Modifier (1st Modifier) 1062 Service Not a Covered Benefit According to Rules 1067 Provider Contract Not Effective on Date of Service 1069 No Reimbursement Information Found For Service 1105 Member has exceeded their maximum benefit. Patient responsible for all charges 1116 Internal Use Only; this service has been separated into individual service lines 3100 Refraction included with exam 3400 Bundled service for lens and lens option pairs 3600 At least one service line has an Invalid Modifier based on date of service 3900 Denied under patient's benefit; patient is responsible for entire purchase 1046 No Primary Insurer EOB Present


















