Spatio-temporal parameters and lower-limb kinematics of turning gait in typically developing...
6
Spatio-temporal parameters and lower-limb kinematics of turning gait in typically developing children Philippe C. Dixon a , Julie Stebbins b, *, Tim Theologis b , Amy B. Zavatsky a a Department of Engineering Science, University of Oxford, Oxford, UK b Nuffield Orthopaedic Centre, Oxford University Hospitals NHS Trust, Oxford, UK 1. Introduction Turning is a common feature of community and in-home ambulation accounting for approximately 20% of steps taken during daily activity [1] and up to 50% of steps indoors [2]. Turning is challenging for a number of populations with limited gait ability [3–5], including children with cerebral palsy (CP) who have compromised balance and are known to trip and fall more often than their typically developing peers. Regardless, gait analysis predominantly focuses on straight walking. Turning is achieved using either a step (outside leg) or spin (inside leg) strategy [6–8]. Step turns maintain the center of mass (COM) within the base of support and may require less muscular effort. Yet, spin turns may be better for facilitating turning as the COM is shifted outside the foot toward the turning direction [6]. In adults, both techniques require modification of biomechanical variables from those of straight walking, such as spatio-temporal [9] and kinematic quantities (frontal and transverse planes) [6]. To date, little is known about the adaptations required for typically developing children to turn; however, preliminary data indicate that decreased velocity, maintenance of cadence, and minimal kinematic sequencing characterize turning in this population [8]. A comprehensive study of turning in children will yield greater insight into the biomechanical requirements of this task and may lead to the development of improved diagnostics, rehabilitation programs, and surgical outcomes in pathological populations such as children with CP. Thus, the aims of this study were to investigate the spatio- temporal and lower limb kinematic adaptations required for typically developing children to navigate 908 step and spin turns. We hypothesized that for the step turn, velocity and stride length would decrease while stance time and stride width would increase compared to straight walking [9]. We expected similar changes in velocity, stride length and stance time for the spin turn, but a decreased stride width (based on the increased ipsilateral hip adduction reported in adults [6]). Finally, we hypothesized that the majority of kinematic changes would occur in the coronal and transverse planes [6]. Gait & Posture 38 (2013) 870–875 A R T I C L E I N F O Article history: Received 23 November 2012 Received in revised form 22 March 2013 Accepted 17 April 2013 Keywords: Turning Gait Kinematics Oxford foot model Children A B S T R A C T Turning is a requirement for most locomotor tasks; however, knowledge of the biomechanical requirements of successful turning is limited. Therefore, the aims of this study were to investigate the spatio-temporal and lower-limb kinematics of 908 turning. Seventeen typically developing children, fitted with full body and multi-segment foot marker sets, having performed both step (outside leg) and spin (inside leg) turning strategies at self-selected velocity, were included in the study. Three turning phases were identified: approach, turn, and depart. Stride velocity and stride length were reduced for both turning strategies for all turning phases (p < 0.03 and p < 0.01, respectively), while stance time and stride width were increased during only select phases (p < 0.05 and p < 0.01, respectively) for both turn conditions compared to straight gait. Many spatio-temporal differences between turn conditions and phases were also found (p < 0.03). Lower-limb kinematics revealed numerous significant differences mainly in the coronal and transverse planes for the hip, knee, ankle, midfoot, and hallux between conditions (p < 0.05). The findings summarized in this study help explain how typically developing children successfully execute turns and provide greater insight into the biomechanics of turning. This knowledge may be applied to a clinical setting to help improve the management of gait disorders in pathological populations, such as children with cerebral palsy. ß 2013 Elsevier B.V. All rights reserved. * Corresponding author. Tel.: +44 1865227609; fax: +44 1865227949. E-mail address: [email protected] (J. Stebbins). Contents lists available at SciVerse ScienceDirect Gait & Posture jo u rn al h om ep age: ww w.els evier.c o m/lo c ate/g aitp os t 0966-6362/$ – see front matter ß 2013 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.gaitpost.2013.04.010
Transcript of Spatio-temporal parameters and lower-limb kinematics of turning gait in typically developing...

Gait & Posture 38 (2013) 870–875
Spatio-temporal parameters and lower-limb kinematics of turning gaitin typically developing children
Philippe C. Dixon a, Julie Stebbins b,*, Tim Theologis b, Amy B. Zavatsky a
a Department of Engineering Science, University of Oxford, Oxford, UKb Nuffield Orthopaedic Centre, Oxford University Hospitals NHS Trust, Oxford, UK
A R T I C L E I N F O
Article history:
Received 23 November 2012
Received in revised form 22 March 2013
Accepted 17 April 2013
Keywords:
Turning
Gait
Kinematics
Oxford foot model
Children
A B S T R A C T
Turning is a requirement for most locomotor tasks; however, knowledge of the biomechanical
requirements of successful turning is limited. Therefore, the aims of this study were to investigate the
spatio-temporal and lower-limb kinematics of 908 turning. Seventeen typically developing children,
fitted with full body and multi-segment foot marker sets, having performed both step (outside leg) and
spin (inside leg) turning strategies at self-selected velocity, were included in the study. Three turning
phases were identified: approach, turn, and depart. Stride velocity and stride length were reduced for
both turning strategies for all turning phases (p < 0.03 and p < 0.01, respectively), while stance time and
stride width were increased during only select phases (p < 0.05 and p < 0.01, respectively) for both turn
conditions compared to straight gait. Many spatio-temporal differences between turn conditions and
phases were also found (p < 0.03). Lower-limb kinematics revealed numerous significant differences
mainly in the coronal and transverse planes for the hip, knee, ankle, midfoot, and hallux between
conditions (p < 0.05). The findings summarized in this study help explain how typically developing
children successfully execute turns and provide greater insight into the biomechanics of turning. This
knowledge may be applied to a clinical setting to help improve the management of gait disorders in
pathological populations, such as children with cerebral palsy.
� 2013 Elsevier B.V. All rights reserved.
Contents lists available at SciVerse ScienceDirect
Gait & Posture
jo u rn al h om ep age: ww w.els evier .c o m/lo c ate /g ai tp os t
1. Introduction
Turning is a common feature of community and in-homeambulation accounting for approximately 20% of steps takenduring daily activity [1] and up to 50% of steps indoors [2]. Turningis challenging for a number of populations with limited gait ability[3–5], including children with cerebral palsy (CP) who havecompromised balance and are known to trip and fall more oftenthan their typically developing peers. Regardless, gait analysispredominantly focuses on straight walking.
Turning is achieved using either a step (outside leg) or spin(inside leg) strategy [6–8]. Step turns maintain the center of mass(COM) within the base of support and may require less musculareffort. Yet, spin turns may be better for facilitating turning as theCOM is shifted outside the foot toward the turning direction [6]. Inadults, both techniques require modification of biomechanicalvariables from those of straight walking, such as spatio-temporal
* Corresponding author. Tel.: +44 1865227609; fax: +44 1865227949.
E-mail address: [email protected] (J. Stebbins).
0966-6362/$ – see front matter � 2013 Elsevier B.V. All rights reserved.
http://dx.doi.org/10.1016/j.gaitpost.2013.04.010
[9] and kinematic quantities (frontal and transverse planes) [6]. Todate, little is known about the adaptations required for typicallydeveloping children to turn; however, preliminary data indicatethat decreased velocity, maintenance of cadence, and minimalkinematic sequencing characterize turning in this population [8]. Acomprehensive study of turning in children will yield greaterinsight into the biomechanical requirements of this task and maylead to the development of improved diagnostics, rehabilitationprograms, and surgical outcomes in pathological populations suchas children with CP.
Thus, the aims of this study were to investigate the spatio-temporal and lower limb kinematic adaptations required fortypically developing children to navigate 908 step and spin turns.We hypothesized that for the step turn, velocity and stride lengthwould decrease while stance time and stride width would increasecompared to straight walking [9]. We expected similar changes invelocity, stride length and stance time for the spin turn, but adecreased stride width (based on the increased ipsilateral hipadduction reported in adults [6]). Finally, we hypothesized that themajority of kinematic changes would occur in the coronal andtransverse planes [6].
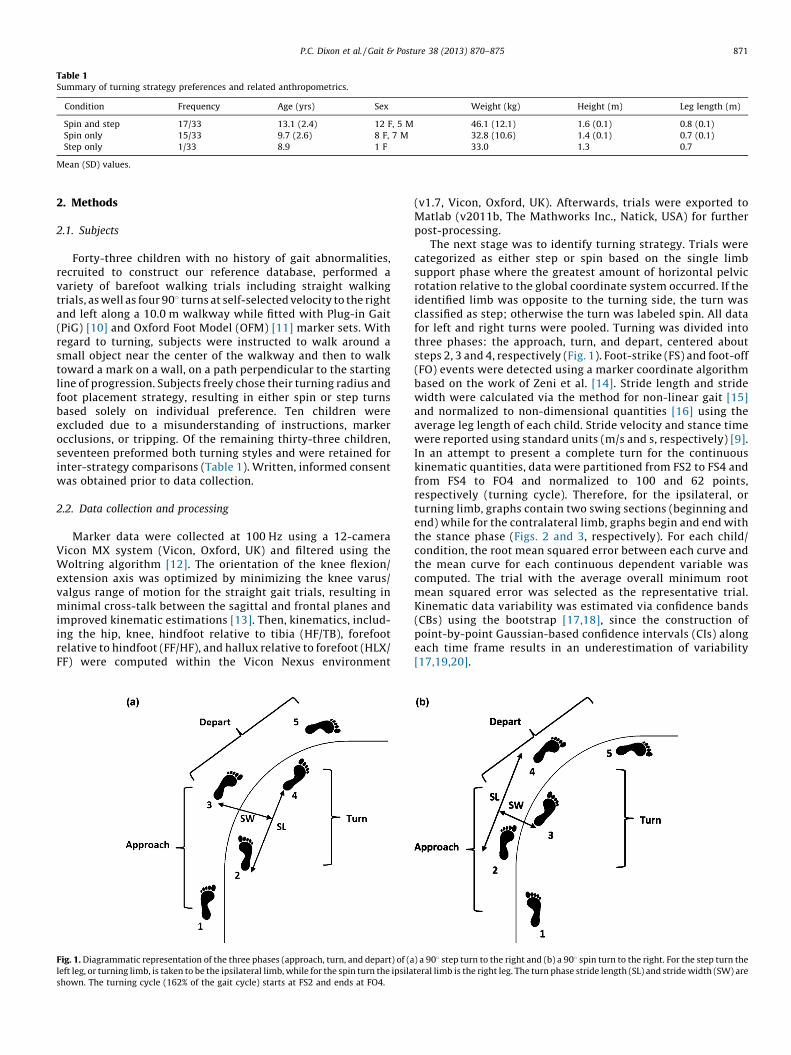
Table 1Summary of turning strategy preferences and related anthropometrics.
Condition Frequency Age (yrs) Sex Weight (kg) Height (m) Leg length (m)
Spin and step 17/33 13.1 (2.4) 12 F, 5 M 46.1 (12.1) 1.6 (0.1) 0.8 (0.1)
Spin only 15/33 9.7 (2.6) 8 F, 7 M 32.8 (10.6) 1.4 (0.1) 0.7 (0.1)
Step only 1/33 8.9 1 F 33.0 1.3 0.7
Mean (SD) values.
P.C. Dixon et al. / Gait & Posture 38 (2013) 870–875 871
2. Methods
2.1. Subjects
Forty-three children with no history of gait abnormalities,recruited to construct our reference database, performed avariety of barefoot walking trials including straight walkingtrials, as well as four 908 turns at self-selected velocity to the rightand left along a 10.0 m walkway while fitted with Plug-in Gait(PiG) [10] and Oxford Foot Model (OFM) [11] marker sets. Withregard to turning, subjects were instructed to walk around asmall object near the center of the walkway and then to walktoward a mark on a wall, on a path perpendicular to the startingline of progression. Subjects freely chose their turning radius andfoot placement strategy, resulting in either spin or step turnsbased solely on individual preference. Ten children wereexcluded due to a misunderstanding of instructions, markerocclusions, or tripping. Of the remaining thirty-three children,seventeen preformed both turning styles and were retained forinter-strategy comparisons (Table 1). Written, informed consentwas obtained prior to data collection.
2.2. Data collection and processing
Marker data were collected at 100 Hz using a 12-cameraVicon MX system (Vicon, Oxford, UK) and filtered using theWoltring algorithm [12]. The orientation of the knee flexion/extension axis was optimized by minimizing the knee varus/valgus range of motion for the straight gait trials, resulting inminimal cross-talk between the sagittal and frontal planes andimproved kinematic estimations [13]. Then, kinematics, includ-ing the hip, knee, hindfoot relative to tibia (HF/TB), forefootrelative to hindfoot (FF/HF), and hallux relative to forefoot (HLX/FF) were computed within the Vicon Nexus environment
Fig. 1. Diagrammatic representation of the three phases (approach, turn, and depart) of (a
left leg, or turning limb, is taken to be the ipsilateral limb, while for the spin turn the ipsila
shown. The turning cycle (162% of the gait cycle) starts at FS2 and ends at FO4.
(v1.7, Vicon, Oxford, UK). Afterwards, trials were exported toMatlab (v2011b, The Mathworks Inc., Natick, USA) for furtherpost-processing.
The next stage was to identify turning strategy. Trials werecategorized as either step or spin based on the single limbsupport phase where the greatest amount of horizontal pelvicrotation relative to the global coordinate system occurred. If theidentified limb was opposite to the turning side, the turn wasclassified as step; otherwise the turn was labeled spin. All datafor left and right turns were pooled. Turning was divided intothree phases: the approach, turn, and depart, centered aboutsteps 2, 3 and 4, respectively (Fig. 1). Foot-strike (FS) and foot-off(FO) events were detected using a marker coordinate algorithmbased on the work of Zeni et al. [14]. Stride length and stridewidth were calculated via the method for non-linear gait [15]and normalized to non-dimensional quantities [16] using theaverage leg length of each child. Stride velocity and stance timewere reported using standard units (m/s and s, respectively) [9].In an attempt to present a complete turn for the continuouskinematic quantities, data were partitioned from FS2 to FS4 andfrom FS4 to FO4 and normalized to 100 and 62 points,respectively (turning cycle). Therefore, for the ipsilateral, orturning limb, graphs contain two swing sections (beginning andend) while for the contralateral limb, graphs begin and end withthe stance phase (Figs. 2 and 3, respectively). For each child/condition, the root mean squared error between each curve andthe mean curve for each continuous dependent variable wascomputed. The trial with the average overall minimum rootmean squared error was selected as the representative trial.Kinematic data variability was estimated via confidence bands(CBs) using the bootstrap [17,18], since the construction ofpoint-by-point Gaussian-based confidence intervals (CIs) alongeach time frame results in an underestimation of variability[17,19,20].
) a 908 step turn to the right and (b) a 908 spin turn to the right. For the step turn the
teral limb is the right leg. The turn phase stride length (SL) and stride width (SW) are
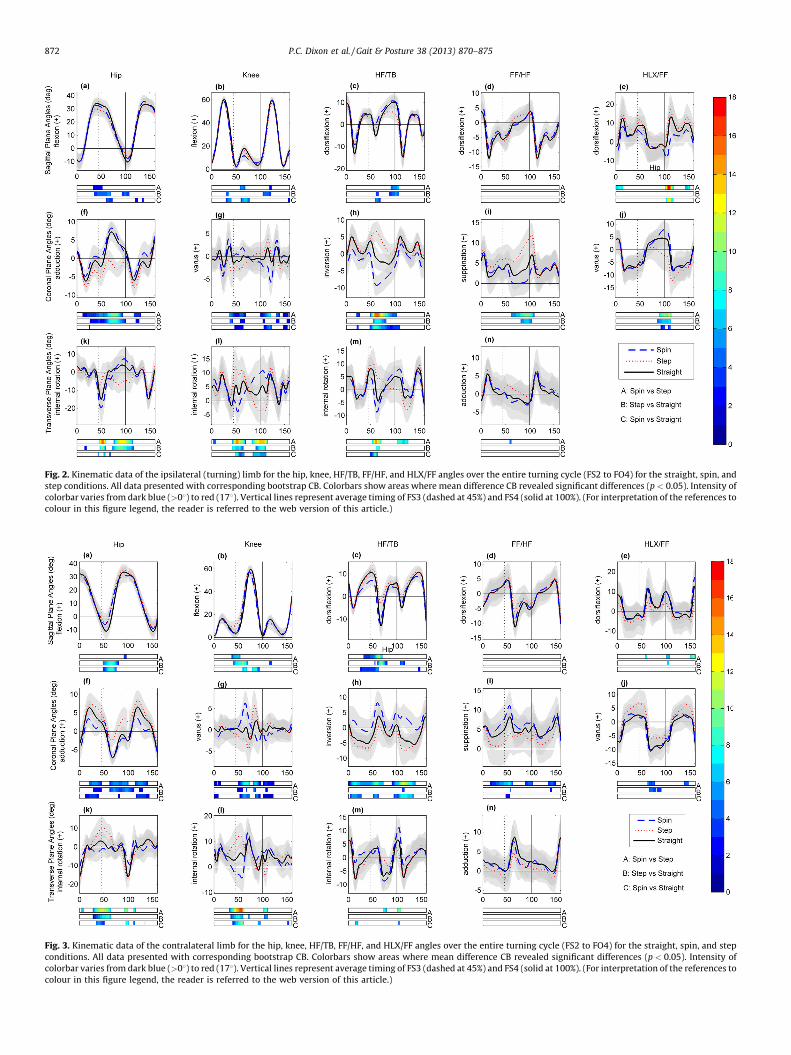
Fig. 2. Kinematic data of the ipsilateral (turning) limb for the hip, knee, HF/TB, FF/HF, and HLX/FF angles over the entire turning cycle (FS2 to FO4) for the straight, spin, and
step conditions. All data presented with corresponding bootstrap CB. Colorbars show areas where mean difference CB revealed significant differences (p < 0.05). Intensity of
colorbar varies from dark blue (>08) to red (178). Vertical lines represent average timing of FS3 (dashed at 45%) and FS4 (solid at 100%). (For interpretation of the references to
colour in this figure legend, the reader is referred to the web version of this article.)
Fig. 3. Kinematic data of the contralateral limb for the hip, knee, HF/TB, FF/HF, and HLX/FF angles over the entire turning cycle (FS2 to FO4) for the straight, spin, and step
conditions. All data presented with corresponding bootstrap CB. Colorbars show areas where mean difference CB revealed significant differences (p < 0.05). Intensity of
colorbar varies from dark blue (>08) to red (178). Vertical lines represent average timing of FS3 (dashed at 45%) and FS4 (solid at 100%). (For interpretation of the references to
colour in this figure legend, the reader is referred to the web version of this article.)
P.C. Dixon et al. / Gait & Posture 38 (2013) 870–875872

P.C. Dixon et al. / Gait & Posture 38 (2013) 870–875 873
2.3. Statistical analysis
For the spatio-temporal parameters, each of the three strides(approach, turn, and depart) of the two turning conditions (stepand spin), along with a single stride chosen from the straightwalking trials were analyzed using a one-way repeated measuresANOVA (1 � 7) with a Bonferroni post hoc correction (IBM SPSSv20. IBM Corp., Armonk, NY, USA). All data were considered normalthrough Q–Q plot analysis, but showed unequal variance. Thus, aGreenhouse–Geisser correction was implemented. For the kine-matics, statistical analyses were conducted over the entire turningcycle by investigating the mean difference 95% CB between pairs ofconditions. Any portion of the CB of paired differences that did notcontain zero was said to be significantly different at the selectedalpha level (a = 0.05) [17,21].
3. Results
3.1. Turning frequency
Overall, children favored turning using either a combination ofstrategies or the spin technique, with only a single child choosingto perform solely step turns. Younger children tended to choose asingle turning style (Table 1). The seventeen children performingboth strategies were retained for analyses.
3.2. Spatio-temporal parameters
All spatio-temporal parameters had a significant main effectdifference (p < 0.001) (Table 2). Stride velocity was reduced for allturning phases compared to the straight condition (p < 0.027). Forboth turn types, the turn and depart phases were slower than theapproach (p < 0.001) with the step condition showing the slowestdepart phase. Stance time for the spin (turn phase) and step (turnand depart phases) were longer than for straight (p = 0.002, 0.058and <0.001, respectively). For the spin condition, the turn phasewas longer than the approach (p < 0.001). Stride length wasshorter for all turning strides compared to straight (p < 0.008). Thestep condition turn stride was shorter than the spin turn stride aswell as the step approach and depart strides (p < 0.001). Finally,stride width for the spin (approach and depart) and step (turn)were increased compared to straight (p < 0.003). The turn stride ofthe step turn was wider than for the spin turn (p < 0.001);however, both the approach and depart strides of the step turnwere narrower than their spin counterparts (p < 0.001). For thestep condition, the turn stride was wider than both the approachand depart strides (p < 0.001) while for the spin, the depart stridewas wider than the approach (p = 0.027).
3.3. Kinematics
The average variation of the bootstrap CBs for all kinematicparameters was approximately 1.6 times larger than the
Table 2Spatio-temporal parameters for healthy children during straight and turning condition
Stride velocity (m/s) Stance time (
Straight 1.30 [1.21, 1.38] 0.59 [0.56, 0.
Spin approach 1.16 [1.07, 1.24]* 0.61 [0.57, 0.
Spin turn 0.99 [0.91, 1.01]*a 0.66 [0.61, 0.
Spin depart 0.97 [0.91, 1.04]*a 0.62 [0.59, 0.
Step approach 1.16 [1.07, 1.25]* 0.62 [0.57, 0.
Step turn 0.99 [0.91, 1.06]*a 0.63 [0.59, 0.
Step depart 0.92 [0.85, 0.99]*at 0.64 [0.61, 0.
Mean [95% confidence interval]. Statistical difference from straight (*), approach stride sa
same phase (s).
point-by-point Gaussian CI width. In the sagittal plane, only afew significant differences were seen at the hip, knee, HF/TB, andHLX/FF angles of the ipsilateral (Fig. 2a–c and e) and contralateral(Fig. 3a–c and e) sides.
Numerous significant differences occurred in the coronal plane,most notably for the ipsilateral limb. At the hip, the step conditioninvolved an abduction angle, while the spin and straight conditionsshowed an adduction resulting in a difference of up to 108 near 80%of the turning cycle. For the knee, differences ranging from 2 to 78were detected, mainly between turn conditions and between spinand straight. For the HF/TB, differences of up to 168 were identifiedduring the stance phase of FS3 arising from large inversion for thestep condition and increased eversion for the spin compared tostraight. Increased supination for the FF/HF of the step conditionoccurred in comparison to spin and straight. A slightly increasedHLX/FF varus resulted for spin (compared to straight) while thestep condition presented hallux valgus (Fig. 2f–j). For thecontralateral side, significant differences at the hip were expressedas increased adduction for the step and decreased adduction forthe spin compared to straight. At the knee, both turning stylesshowed out of phase increased varus peak angles compared tostraight walking. For the HF/TB, spin presented consistentlygreater inversion (2–118) compared to both step and straight.For the FF/HF, consistent increased supination (2–78) was seen forthe spin condition compared to step. Finally, the step turn HLX/FFvalgus was decreased compared to both spin and straightconditions (Fig. 3f–j).
In the transverse plane, large differences were found for bothlimbs. For the ipsilateral side, the hip had external rotationcentered about FS4 for the step condition, while internal rotationwas present for the spin and straight conditions (10–138differences). The knee revealed an out-of-phase angular patternthroughout the middle of the turning cycle between conditions.Similarly, the HF/TB presented oppositely directed anglesbetween turning conditions (8–168 differences) during the stancephase of FS3 and FS4 (Fig. 2k–m). On the contralateral side,differences were mainly apparent at the hip and knee. For the hip,all conditions differed from each other with the greatestdifferences occurring about FS3 between the spin and step. Atthe knee, differences were again centered about FS3 with the spincondition in external rotation and the step presenting increasedinternal rotation compared to straight (Fig. 3k and l). Alldifferences noted above were significantly different at p < 0.05level.
4. Discussion
This study investigated the spatio-temporal and lower-limbkinematics of typically developing children during 908 step andspin turns and compared the results to straight walking. The 908turn is easy to implement within a gait laboratory and is relevantsince the majority of turning maneuvers in daily activity result in achange in direction between 768 and 1208 [1]. The kinematic
s (n = 17).
s) Stride length Stride width
62] 1.56 [1.49, 1.62] 0.09 [0.08, 0.11]
65] 1.40 [1.32, 1.48]* 0.17 [0.15, 0.20]*
70]*a 1.35 [1.29, 1.41]* 0.17 [0.14, 0.21]
66] 1.33 [1.25, 1.40]* 0.27 [0.23, 0.30]*a
66] 1.44 [1.37, 1.52]* 0.07 [0.05, 0.10]s
68]* 1.18 [1.11,1.24]*sa 0.35 [0.32, 0.37]*sa
68]* 1.38 [1.31, 1.45]*t 0.07 [0.04, 0.11]st
me turn condition (a), turn stride same condition (t), and between conditions for the

P.C. Dixon et al. / Gait & Posture 38 (2013) 870–875874
analysis procedure represents a rarely used, yet effective,conservative statistical approach that succinctly summarizeddifferences throughout the turning cycle. To the knowledge ofthe authors, this is the first study to describe the kinematics ofturning in typically developing children, the spatio-temporalparameters for the 908 spin turn, and the kinematics based on theOFM multi-segment foot model for both turning strategies in anypopulation. This study also presents a novel way to identify turningstrategy based on pelvic motion. In general, this investigation hasdemonstrated that turning requires numerous lower-limb bio-mechanical adaptations and may be challenging for populationswith a variety of gait disorders.
For the kinematic data, bootstrap CBs were used to representthe variability and conduct statistical analyses. In terms ofvariability, bootstrap CBs result in the maintenance of thetheoretical coverage (95%) over the entire curve, whereas point-by-point CIs produce narrow bands leading to increased type Ierror rates [17,19,20]. When conducting statistical analysis usingdiscrete points, specific curve features that are often notreproducible or have a different temporal component betweentrials/individuals must be correctly identified. This difficulty isavoided with the bootstrap CBs; however, the current approach issensitive to loss of information from ensemble averaging. Althoughother continuous data analysis procedures, such as functional dataanalysis [22], nonlinear model fitting [23], and statisticalparameter mapping [24] may be more powerful, the currentmethod was chosen as it addresses the weaknesses of point-by-point analysis and is relatively easy to implement and interpret.Importantly, the bootstrap CBs do not allow for the identification ofspecific sources of variability in the data (e.g. variability arisingfrom unidentified covariates) [25] while the statistical approach ofanalyzing the CB difference may be limited to research designswith relatively few paired-comparisons. We attempted to mini-mize variability by testing similar children during a single session,without removing markers between conditions, and by optimizingPiG kinematic data [13]. Despite its limitations, we believe thatbootstrap CBs represent a robust option for the representation ofvariability, especially when used to build a normal database, and toprovide statistical analysis in continuous gait data.
Our results for straight walking are in agreement with previousdata [26]. With regard to the turning conditions, as hypothesized,stride length and stride velocity were found to decrease comparedto straight walking in agreement with step turn data presented byStrike and Taylor [9], while stance time generally increased.Moreover, also in agreement with Strike and Taylor [9], increasedstride width was found during the turn phase of the step condition.Contrary to our hypothesis, no significant changes in stride widthwere observed for the turn phase of the spin turn, while theapproach and depart phases revealed increased stride widthcompared to straight walking. This phenomenon may haveoccurred due the positioning of the approach (FS2) and depart(FS4) steps in an attempt to maintain balance through widening ofthe base of support. These assertions may be supported by thedecreased hip adduction seen for the contralateral limb. Finally, ashypothesized, coronal and transverse plane angles showedimportant differences from straight walking. These results aresimilar to those found by Taylor et al. [6]; however, caution mustbe exercised when making comparisons between the two studiesas populations sampled, protocols implemented, and biomechani-cal models computed differ. A major disparity between this studyand the research of Taylor et al. [6] is that here, a single spin turnstrategy was identified. In a group of healthy adults (n = 10), Tayloret al. [6] divided the spin technique into two sub-categories: theipsilateral pivot (n = 4) where the foot rotates with respect to thesurface during the turning stance phase and the ipsilateral cross-over (n = 6), where the turning foot is rooted as the contralateral
limb is swung into the new direction. This subdivision of spin turnshas not been confirmed by other authors [7]. It is likely that theemergence of the ipsilateral pivot is dependent on increased gaitvelocity. The approach speed from the Taylor et al. [6] study was1.38 m/s, while here, children approached the spin turn with amean velocity of 1.16 m/s. Alternatively, although the presentcohort seem to possess a mature straight gait pattern, it is possiblethat the increased demands of turning might expose remaininggait immaturity leading to a fusion of the more complex turningsub-strategies identified in adults. A further point to make is thathere the PiG model outputs were optimized [13], whereas Tayloret al. [6] presented data that may be subject to error due tomisaligned thigh wand markers. Finally, as Taylor et al. [6] onlyinvestigated a portion of the turning cycle for the ipsilateral limb,important information over the entire turn and the role of thecontralateral limb are not available for comparison.
The present cohort predominantly chose to perform turns usingthe spin strategy, regardless of an increased risk of tripping [6].This disagrees with previous pilot data in which sample size mayhave been too small (n = 9) to discern a consistent trend [8].Clearly, the changes presented here did not pose a significantthreat to balance to our cohort. Possibly, decreased stride velocityand stride length as well as increased stance time and stride widthaided the maintenance of a stable base of support minimizing therisk of falling and subsequent injury during turning. Importantly,unanticipated turns may not allow children to modulate spatio-temporal parameter responses leading to greater kinematicchanges and increased risk of injury [27].
Overall, the changes presented here reveal that turning isbiomechanically distinct from straight walking. During straightgait, based on the inverted pendulum model, motion of the COM inthe plane of progression is passively controlled by momentum andinertia [28]; however, during turning, forward progression of theCOM must be quickly halted and redirected over a relatively stablebase of support, possibly requiring greater active control from thecentral nervous system. Each turning strategy represents adifferent solution to the redirection problem with step turnsbeing more stable and spin turns possibly more economical [6]. Aninvestigation of the kinetics of turning in typically developingchildren, already underway by the present authors, may providegreater information regarding these control strategies and willprovide a complete picture of the normative changes duringturning in this population.
The investigation of turning biomechanics in children withmobility impairments, such as CP, is also warranted. Children withCP often present with impaired balance, weak hip abductors, in-toeing, and ankle contractures [29], making the aforementionedturning adaptations difficult. The inclusion of turning tasks inclinical gait analysis might help improve the assessment, diagnosis,treatment, and mobility outcomes of a variety of walking disorders,including those resulting from CP. In particular, assessing turninggait in the presence of pathology should help reveal deviations andproblems that are not obvious in straight walking.
Acknowledgments
The first author of this study is supported through funding fromthe Natural Sciences and Engineering Research Council of Canada(NSERC). We would also like to acknowledge the contribution ofGiovanni Milandri to the processing and analysis of the pilot data set.
Conflict of interest
We have no financial or personal relationships with otherpeople or organizations that could inappropriately influence (bias)our work.
P.C. Dixon et al. / Gait & Posture 38 (2013) 870–875 875
References
[1] Sedgman R, Goldie P, Iansek R. Development of a measure of turning duringwalking. In: Proceedings of Advancing Rehabilitation; 1994. p. 26–31.
[2] Glaister BC, Bernatz GC, Klute GK, Orendurff MS. Video task analysis of turningduring activities of daily living. Gait and Posture 2007;25:289–94.
[3] Lam T, Luttmann K. Turning capacity in ambulatory individuals poststroke.American Journal of Physical Medicine and Rehabilitation 2009;88:873–83.quiz 84–6, 946.
[4] Segal AD, Orendurff MS, Czerniecki JM, Schoen J, Klute GK. Comparison oftranstibial amputee and non-amputee biomechanics during a common turn-ing task. Gait and Posture 2011;33:41–7.
[5] Fuller JR, Adkin AL, Vallis LA. Strategies used by older adults to change traveldirection. Gait and Posture 2007;25:393–400.
[6] Taylor MJ, Dabnichki P, Strike SC. A three-dimensional biomechanical com-parison between turning strategies during the stance phase of walking. HumanMovement Science 2005;24:558–73.
[7] Hase K, Stein RB. Turning strategies during human walking. Journal of Neuro-physiology 1999;81:2914–22.
[8] Milandri G. Turning gait: characterisation for use in clinial gait analysis. ProjectReport. Department of Engineering Science, University of Oxford; 2011.
[9] Strike SC, Taylor MJ. The temporal-spatial and ground reaction impulses ofturning gait: is turning symmetrical. Gait and Posture 2009;29:597–602.
[10] Kadaba MP, Ramakrishnan HK, Wootten ME. Measurement of lower extremitykinematics during level walking. Journal of Orthopaedic Research 1990;8:383–92.
[11] Stebbins J, Harrington M, Thompson N, Zavatsky A, Theologis T. Repeatabilityof a model for measuring multi-segment foot kinematics in children. Gait andPosture 2006;23:401–10.
[12] Woltring HJ. A FORTRAN package for generalized, cross-validatory spline smooth-ing and differentiation. Advances in Engineering Software (UK) 1986;8:104–13.
[13] Baker R, Finney L, Orr J. A new approach to determine the hip rotation profilefrom clinical gait analysis data. Human Movement Science 1999;18:655–67.
[14] Zeni Jr JA, Richards JG, Higginson JS. Two simple methods for determining gaitevents during treadmill and overground walking using kinematic data. Gaitand Posture 2008;27:710–4.
[15] Huxham F, Gong J, Baker R, Morris M, Iansek R. Defining spatial parameters fornon-linear walking. Gait and Posture 2006;23:159–63.
[16] Hof AL. Scaling gait data to body size. Gait and Posture 1996;4:222–3.[17] Lenhoff MW, Santner TJ, Otis JC, Peterson MG, Williams BJ, Backus SI. Bootstrap
prediction and confidence bands: a superior statistical method for analysis ofgait data. Gait and Posture 1999;9:10–7.
[18] Olshen R, Biden E, Wyatt M, Sutherland D. Gait analysis and the bootstrap. TheAnnals of Statistics 1989;17:1419–40.
[19] Duhamel A, Bourriez JL, Devos P, Krystkowiak P, Destee A, Derambure P, et al.Statistical tools for clinical gait analysis. Gait and Posture 2004;20:204–12.
[20] Schwartz MH, Trost JP, Wervey RA. Measurement and management of errors inquantitative gait data. Gait and Posture 2004;20:196–203.
[21] Chau T, Young S, Redekop S. Managing variability in the summary andcomparison of gait data. Journal of Neuroengineering and Rehabilitation2005;2:22.
[22] Ramsay J, Silverman B. Functional data analysis. New York: Springer; 1997.[23] Motulsky H, Christopoulos A. Fitting curves to data using nonlinear-regres-
sion—a practical and nonmathematical approach. New York: Oxford Univer-sity Press; 2004. p. 160–66.
[24] Pataky TC. One-dimensional statistical parametric mapping in Python. Com-puter Methods in Biomechanics and Biomedical Engineering 2011;15:295–301.
[25] Roislien J, Skare O, Gustavsen M, Broch NL, Rennie L, Opheim A. Simultaneousestimation of effects of gender, age and walking speed on kinematic gait data.Gait and Posture 2009;30:441–5.
[26] Lythgo N, Wilson C, Galea M. Basic gait and symmetry measures for primaryschool-aged children and young adults whilst walking barefoot and withshoes. Gait and Posture 2009;30:502–6.
[27] Jenkyn TR, Shultz R, Giffin JR, Birmingham TB. A comparison of subtalar jointmotion during anticipated medial cutting turns and level walking using amulti-segment foot model. Gait and Posture 2010;31:153–8.
[28] Gard SA, Childress DS. What determines the vertical displacement of the bodyduring normal walking. Journal of Prosthetics and Orthotics 2001;13:64–7.
[29] Perry J, Burnfield JM. Gait analysis: normal and pathological function. 2nd ed.Thorofare, NJ: Slack Inc.; 2010. p. 345–58.